Embed Size (px)
Citation preview

5328
OCTOBER 10, 1925.
An AddressON
UNUNITED FRACTURES.
Delivered at St. Bartholomew’s Hospital, London,
BY ERNEST W. HEY GROVES, M.S. LOND.,F.R.C.S. ENG.,
PROFESSOR OF SURGERY, BRISTOL UNIVERSITY.
WHEN I was a student in these revered and ancientwalls the subject of fractures received very scantattention in our surgical curriculum. Of course,necessity sometimes compelled the admission of acase of fracture of the leg bones into the wards, andthen splints were duly applied and after some weeksthe patient was sent out: what became of him wenever inquired-he did not interest us. The smartnessof a house surgeon was recognised by this among othertests-that he should avoid taking in fracture casesand, having taken them in, should hide the fact andget rid of the offending case as soon as possible. Iremember Mr. Lockwood advising us if we ever gota fracture case in private practice to pass it on to ourrival across the street, so that it might be his undoingand not ours, but beyond this, I cannot recollect anymember of the surgical staff ever taking any notice ofa fracture during my dressership. No doubt this isall changed now, and in the full illumination of theX rays the diagnosis and treatment of fractures aretaught as embodying the most important principlesof the science and art of surgery.
CAUSES OF NON-UNION.The study of a case of a fracture which has failec
to unite is one which may well absorb the interesiof the pathologist and the physician as well of thEsurgeon and the mechanic. Why does repair sometimesfail ? What determines the ordered balance betweentissue formation and tissue absorption ? What is thedifference between an osteoblast and an osteoclast ?What is the vital relation between the cells and theintercellular material of the skeleton ? Such are someof the questions which are suggested and which I findeasier to ask than to answer.Let us consider the last question a, little more
closely, for it affords a good illustration of the bafflingnature of the problem of bone pathology, and it isvery intimately connected with explaining the natureand determining the treatment of an ununitedfracture. All connective tissue and especially boneand cartilage are distinguished by the large proportionwhich the intercellular material bears to the cellularelement. Is this intercellular material living or dead ?A piece of bone is regarded as dead if it containsneither blood-vessels nor cells. But according to thisdefinition all the extra cellular material of the boneis then dead ; it is a secretion or excretion of the livingcells which can be laid down or taken up according tothe necessities of the moment.The endoskeleton of the vertebrate, like the
exoskeleton of the invertebrate, is formed by theliving tissues, but is outside them. Any piece ofhuman bone may become temporarily deprived ofits blood-supply and its cells all die, and yet in a veryshort time new blood-vessels and new cells invade thedead bone and the dry bone truly lives once again.On the other hand, a devitalised portion of bone mayremain for an indefinite time without blood and withoutcells, an indolent mass incapable of growth or repair.This, in fact, is the condition of the ends of the bonesin many cases of ununited fracture.The causes of non-union may be grouped as
follows :-
Mechanical- ]
Gap between the bone ends. Interposition of soft parts. 1Unrestricted mobility. Foreign bodies. ]
Vascular-
Sepsis, destroying the vital elements.Sclerosis, the bone canals are closed and the cells
imprisoned.Atrophy, the vital elements disappear and only an earthy
shell remains.Fibrous tissue and cartilage cover over the bone endsand so imprison the vital elements.
Disease-
Infection, pyogenic or specific, tubercle, gumma.New growth-
Fibrocystic disease, myeloma.Sarcoma, carcinoma.
Space does not permit of the discussion of each ofthese causes, and I must be content to emphasise oneor two points.
It often happens that several of these causes
cooperate. Thus, in the fracture of the neck of thefemur, it is difficult to fix the bones, and with theordinary splinting there occurs mobility, associatedwith want of apposition and the interposition of partof the capsule of the joint. The proximal fragment hasa very poor blood-supply and atrophy quickly takesplace. Again in the caseof the shaft of the FiG. 1.4"",.,"n 4-1,- 41 -, ___________________________humerus, the difficultof efficient fixation is thprime cause of thfrequent non-union. Thbone ends throw ou
granular tissue or procallus, but c o n stanmovement prevents thi;bridging the gap. Iithe meantime muscleand fascia wrap closelround the bone endsand each becomesclothed in fibrous tissueor fibro-cartilage. Theimportance of mobilityas a cause of non-unionhas been obscured bythe teaching of thosewho advocate earlymovement of a limb asconducing to rapidrestoration of function.But there is no realcon fl i c t o f opinion.Movement of the limbas a whole and of themuscles covering thefracture is good becauseit promotes vascularity.But movements of thebone ends against oneanother in the
Ununited fracture of humerus,treated by plate, wires, andscrews two years previously.(For result of grafting opera-tion, see Figs. 4 and 5.)
anotner r in tne
early period after a fracture certainly preventunion.One cause of non-union which is not uncommon is
the inefficient application of screws and plates or wirein the treatment of a fracture. This, too, has been thesubject of much misapprehension. It is commonlysaid that it is the malign influence of the foreign bodywhich has hindered the vital repair. But this is notthe case. Bones tolerate foreign bodies very kindly,provided they are fixed and give fixation. But it isthe small plate which soon works loose, or the badlyapplied wire which works the mischief, causing friction,destruction of granular tissue, and non-union. Itis easy to provide abundant proof of this both fromexperimental and clinical evidence. Fig. 1 is a goodillustration of mechanical fixation which providesthe maximum of frictional irritation with theminimum of mechanical rigidity. That there wasnothing at fault with the bone itself is provedby the kindly way it healed after a bone graft (seeFigs. 4 and 5).
p

736
VARIETIES OF NON-UNION.There are at least four different varieties of ununited
iractures, and each variety has its own structuralpeculiarity and requires special treatment. They are :-(a) Delayed Union-Mere cellular inactivity.No callus and little or no fibrous tissue.
(b) Non-union-1. Fibrous union : Fibrous tissue or fibro-cartilagebetween and connecting the bone ends.
2. Pseudarthrosis : Bone ends eburnated and covered withfibro-cartilage. A joint cavity with capsule andsynovial fluid between the ends of the bones.
3. Gap fracture : A piece of bone lost, the bone ends heldapart by the companion bone. The bone is usuallythin and atrophic.
It is not always possible to distinguish between thefirst and the second varieties-i.e., between delayedunion and fibrous union, but the other two varieties-the false joint, with its flail-like mobility, and the gapfracture-are quite distinct. In merely delayed unionthe bone’s ends are in contact, but callus does notform in such a way as to unite them. Such callus asthere is is only the internal callus which seals up each
marrow cavity. The X rays show no change in thebone except for a slight blurring of the distinctionbetween the cortical and medullary layers. It is astate of cellular indolence and inactivity, which can
Fio. 2.
In making this distinction, however, it has to be bornein mind that the one condition leads to the other, andit is therefore not always possible to draw a sharpline of demarcation between them. From a practicalpoint of view, delayed union is a condition whichcan be cured by non-operative or simple comminutionmethods, whilst true fibrous union will require openexposure with resection of the eburnated bone ends.
NON-OPERATIVE METHODS OF TREATMENT.In all doubtful cases when not more than six months
have ,elapsed since the fracture, it is worth while togive a good trial for a, period of about three monthsto non-operative methods. Such a case is oftenpresented by a fracture of the lower third of the tibia.Perhaps six months has passed since the accident,the broken bone present.s distinct mobility but notmuch pain, and the X rays show no change in thebone ends except a little rounding off of the sharpcontour. It is easy to make a mistake in such a caseby treating it as if it were a recent fracture and puttingon a plate. It may be true that if the fracture hadbeen plated in the first place union would not havebeen delayed. But the essential fact of delayedunion-viz., the cellular inactivity of the vital elementsof the bone-now dominates the situation, and mereplating is more likely to make matters worse thanbetter. To apply a plate requires that the bone ends
should be partly strippedof their vascular coveringand bored with holes, butMien Lne Dare area ana 1jue
fresh holes are covered orplugged with plate andscrews, a process whichdoes much to hinder andnothing to promote callusformation.
There are three non-
operative methods avail-able and these may be usedsingly or in combination.They are : (1) voluntarymovements, the fracturebeing protected with a
splint; (2) passive conges-tion with massage; (3) in-jection of blood or bloodproducts in and around thefracture.
In the encouragement ofactive movements the limbmust be so protected by acase-splint that absoluterigidity without lateralmovement is afforded tothe bone, whilst the jointsabove and below ‘are leftfree. The contraction ofthe muscles promotes shyperaemia and also pullsthe bones together. In thecase of the tibia the patientis made to walk, and thisis a most efficient meansof forcing the bone endstogether and so promotinga frictional stimulus tocallus formation. This typeof treatment is very prac-tical because it will enablemost patients to resumetheir active work instead ofkeeping them in prolongedinvalidity. The second non-
BFractured tibia exposed and treated by subperiosteal comminution ; inset shows jaws of
instruments used.
generally be quickened into healthy vital repair byan appropriate stimulus. In fibrous union, on theother hand, the bone ends are thickened, eburnated,and greatly increased in density as seen by the X rays.The bone ends are covered in fibrous tissue or fibro-cartilage, whilst blood-vessels and osteoblasts alike
are strangled or imprisoned in hard sclerotic bone.
operative method is the " damming and hammering" "advocated by Owen Thomas. A piece of rubbertubing is placed round the limb above and below thefracture as tightly as can be borne without alteringthe arterial pulse and so kept for several hours daily.With this is associated a heavy percussion massageof the limb aimed at promoting tissue stimulation.
737
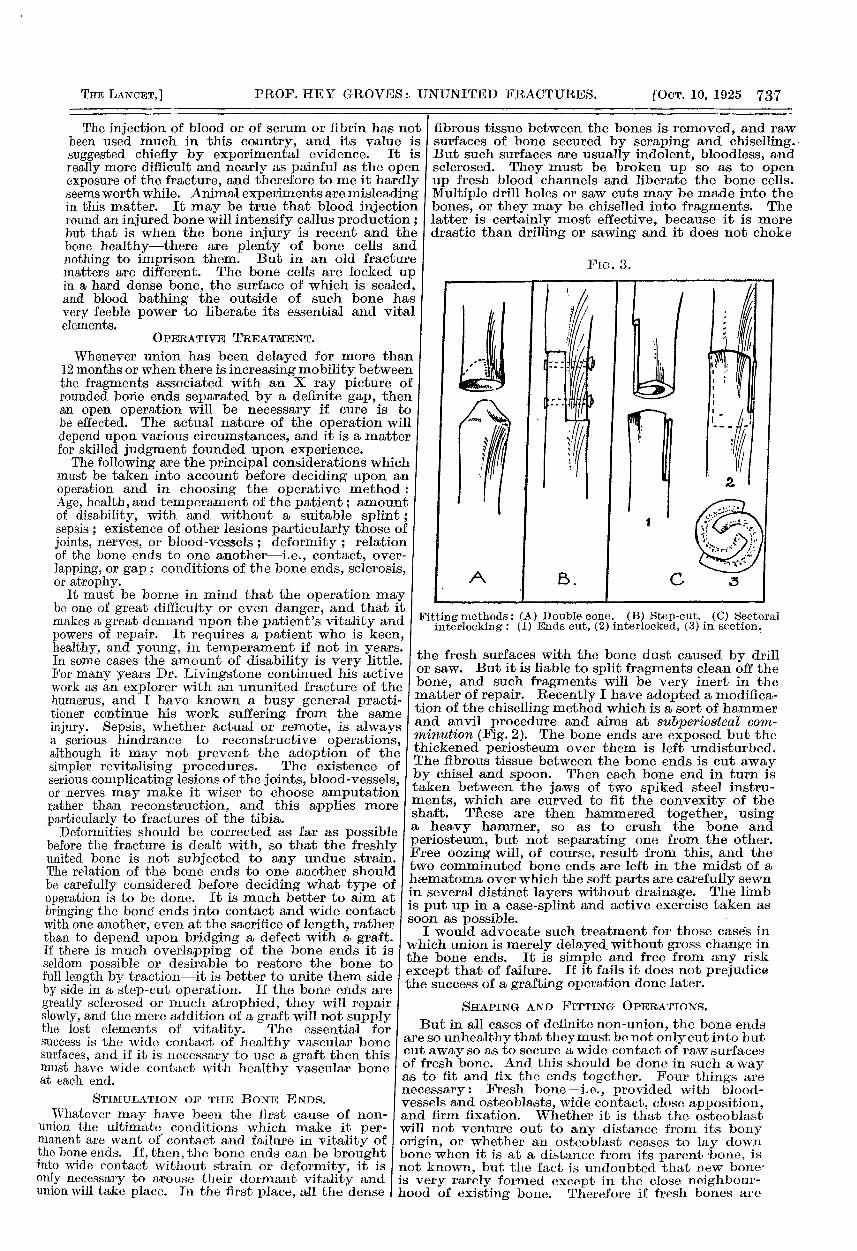
The injection of blood or of serum or fibrin has notbeen used much in this country, and its value issuggested chiefly by experimental evidence. It isreally more difficult and nearly as painful as the openexposure of the fracture, and therefore to me it hardlyseems worth while. Animal experiments are misleadingin this matter. It may be true that blood injectionround an injured bone will intensify callus production ;but that is when the bone injury is recent and thebone healthy-there are plenty of bone cells andnothing to imprison them. But in an old fracturematters are different. The bone cells are locked upin a hard dense bone, the surface of which is sealed,and blood bathing the outside of such bone hasvery feeble power to liberate its essential and vitalelements.
OPERATIVE TREATMENT.
VV J.H.::i.l1tJ V tJ.1." 11111V11 Ki3 AJGG11 UC-LcfyC J.VJ.- 111V1 V’ V11G411
12 months or when there is increasing mobility betweenthe fragments associated with an X ray picture ofrounded bone ends separated by a definite gap, thenan open operation will be necessary if cure is tobe effected. The actual nature of the operation willdepend upon various circumstances, and it is a matterfor skilled judgment founded upon experience.The following are the principal considerations which
must be taken into account before deciding upon anoperation and in choosing the operative method :Age, health, and temperament of the patient; amountof disability, with and without a suitable splint;sepsis ; existence of other lesions particularly those ofjoints, nerves, or blood-vessels ; deformity ; relationof the bone ends to one another-i.e., contact, over-lapping, or gap ; conditions of the bone ends, sclerosis,or atrophy.
It must be borne in mind that the operation mabe one of great difficulty or even danger, and that imakes a great demand upon the patient’s vitality anpowers of repair. It requires a patient who is keerhealthy, and young, in temperament if not in year:In some cases the amount of disability is very littlEFor many years Dr. Livingstone continued his activwork as an explorer with an ununited fracture of thhumerus, and I have known a busy general practitioner continue his work suffering from the saml
injury. Sepsis, whether actual or remote, is alwaysa serious hindrance to reconstructive operationsalthough it may not prevent the adoption of th<simpler revitalising procedures. The existence ojserious complicating lesions of the joints, blood-vesselsor nerves may make it wiser to choose amputationrather than reconstruction, and this applies moreparticularly to fractures of the tibia.Deformities should be corrected as far as possible
before the fracture is dealt with, so that the freshlyunited bone is not subjected to any undue strain.The relation of the bone ends to one another shouldbe carefully considered before deciding what type ofoperation is to be done. It is much better to aim atbringing the bone ends into contact and wide contactwith one another, even at the sacrifice of length, ratherthan to depend upon bridging a defect with a graft.If there is much overlapping of the bone ends it isseldom possible or desirable to restore the bone tofull length by traction-it is better to unite them sideby side in a step-cut operation. If the bone ends aregreatly sclerosed or much atrophied, they will repairslowly, and the mere addition of a graft will not supplythe lost elements of vitality. The essential forsuccess is the wide contact of healthy vascular bonesurfaces, and if it is necessary to use a graft then thismust have wide contact with healthy vascular boneat each end.
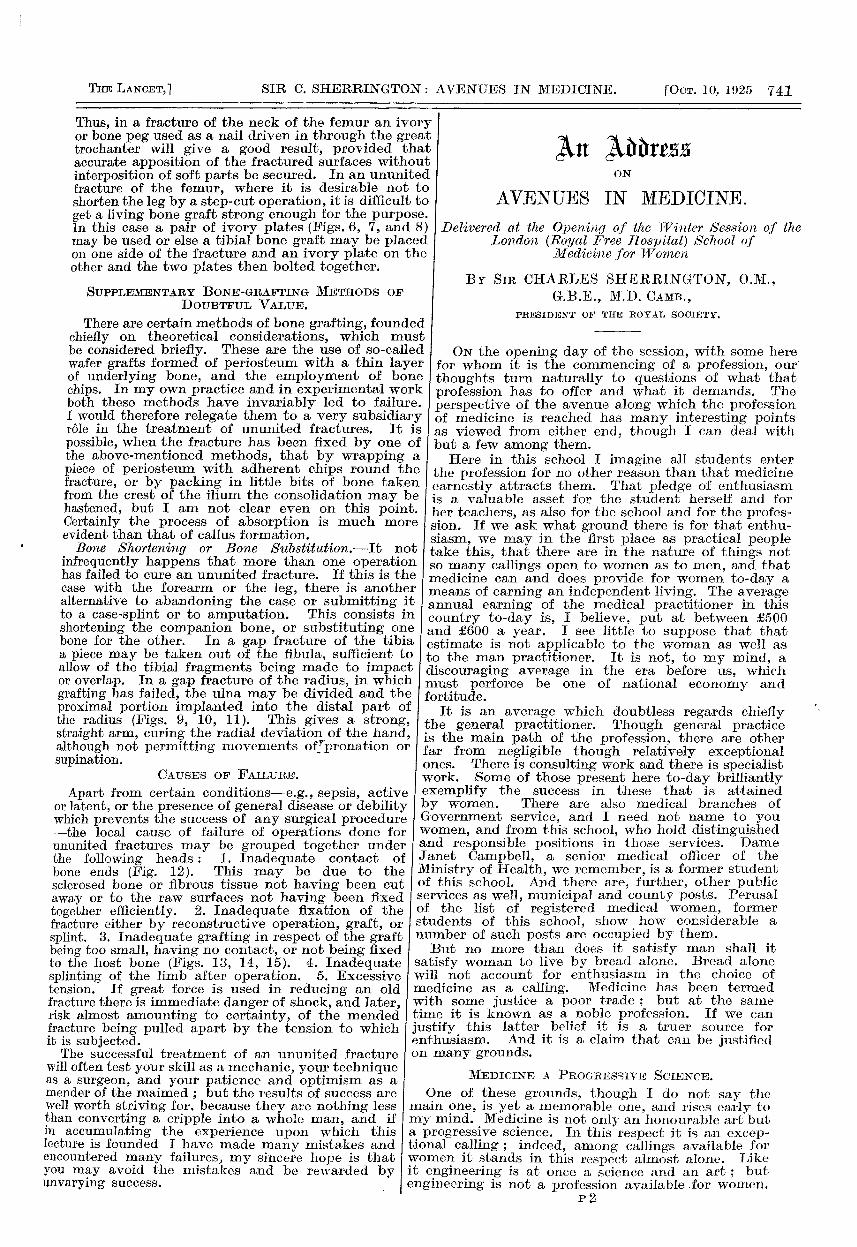
STIMULATION OF TIIE BONE ENDS.Whatever may have been the lirst cause of non-
union the ultimate conditions which make it per-manent are want of contact and failure in vitality ofthe bone ends. If, then, the bone ends can be broughtinto wide contact without strain or deformity, it isonly necessary to arouse their dormant vitality andunion will take place. In the first place, all the dense
, fibrous tissue between the bones is removed, and rawsurfaces of bone secured by scraping and chiselling.But such surfaces are usually indolent, bloodless, andsclerosed. They must be broken up so as to openup fresh blood channels and liberate the bone cells.Multiple drill holes or saw cuts may be made into thebones, or they may be chiselled into fragments. Thelatter is certainly most effective, because it is moredrastic than drilling or sawing and it does not choke
Frc. 3.
Fitting methods : (A) Double cone. (B) Step-cut. (C) Sectoralinterlocking : (1) Ends out, (2) interlocked, (3) in section.
the fresh surfaces with the bone dust caused by drill’or saw. But it is liable to split fragments clean off thebone, and such fragments will be very inert in thematter of repair. Recently I have adopted a modifica-tion of the chiselling method which is a sort of hammerand anvil procedure and aims at subperiosteal com-minution (Fig. 2). The bone ends are exposed but thethickened periosteum over them is left undisturbed.The fibrous tissue between the bone ends is cut awayby chisel and spoon. Then each bone end in turn istaken between the jaws of two spiked steel instru-ments, which are curved to fit the convexity of theshaft. Tnese are then hammered together, usinga heavy hammer, so as to crush the bone andperiosteum, but not separating one from the other.Free oozing will, of course, result from this, and thetwo comminuted bone ends are left in the midst of ahasmatoma over which the soft parts are carefully sewnin several distinct layers without drainage. The limbis put up in a case-splint and active exercise taken assoon as possible. ’
I would advocate such treatment for those cases inwhich union is merely delayed without gross change inthe bone ends. It is simple and free from any riskexcept that of failure. If it fails it does not prejudicethe success of a grafting operation done later.
SHAPING AND FITTING OPERATIONS.
But in all cases of definite non-union, the bone endsare so unhealthy that they must be not only cut into butcut away so as to secure a wide contact of raw surfacesof fresh bone. And this should be done in such a wayas to fit and fix the ends together. Four things arenecessary: Fresh bone-i.e., provided with blood-vessels and osteoblasts, wide contact, close apposition,and firm fixation. Whether it is that the osteoblastwill not venture out to any distance from its bonyorigin, or whether an osteoblast ceases to lay downbone when it is at a distance from its parent bone, isnot known, but the fact is undoubted that new bone-is very rarely formed except in the close neighbour-hood of existing bone. Therefore if fresh bones are

738
fitted and fixed firmly together they will unite intoone solid bone, whereas if they are in loose appositionthey will only become tied together by fibrous union.
FIG. 4. FIG. 5.
FIG. 4.-Fractured humerus (same ease as Fig. 1) treated byautogenous intramedullary graft fixed by " split-and-thrust "method. One month after operation.
FIG. 5.-Same case as Fig. 4. Two years later.
A good illustration may be given from the joinery Iof a cabinet maker or carpenter. In such work alljoining is done by accurate fitting. If glue is used,it is only to fix accurately apposed surfaces and not
FIG. 7.
The actual shaping of the bones after sclerotic tissuehas been cut away should be adapted to the conditionof the bones, the shape of the fracture, and the advisa-
FiG. 6. FrG. 8.
FIG. 6.-Ununited fracture of femur treated 12 months pre-viously by inadequate plating.
FIG. 8.-Same case as Fig. 6. After operation, by a pair ofivory plates, bolted together.
bility of shortening the bone. Thus transversefractures may be shaped as a double cone and fixed bya peg or a plate (Fig. 3, A). Oblique fractures may bestep-cut so as to give a wide overlapping and fixed by
bolts or bands (Fig. 3, B).Sectlon through Femur Or an atrophic bone may
have a piece taken out ofits circumference and thenbe made to interlock withits fellow by engaging oneedge of each bone in themarrow cavity of the other,a device which may bedescribed as sectoral inter-locking (Fig. 3, c).
It will be noted that allthese reconstructive opera-tions involve the shorten-ing of the bone. This isof no great importance inthe humerus. In the femurit is better to have a shortstrong leg than an ununitedfracture. It is wise not toattempt full elongation ofthe thigh bone. It may begiven one week’s tractionby a 25 lb. weight appliedby a transfixion pin, andthen at the operation thebone should be joined withsome overlapping. It isdangerous on account ofshock to pull the leg outto its full length, and it isfatal to the fixation if itbe put up under strongtension. In the forearmand lower leg the fittingoperations usually involvean osteotomy of the com-
Pratt-Lowmans’ self retaining retrators.Same case as Fig. 6. Operation by bolting on pair of ivory plates.
fill up cracks or deficiencies. No more should beasked of the reparative callus than a carpenter asksof his glue-i.e., to knit together surfaces which trulyfit and are firmly fixed. I
panion bone. Having fitted the ends together theycertainly should be fixed. Such fixation may be bymetal bolts, ivory screws, bands, or wire, or in manycases tendon ligatures, silkworm gut, or stout silk will

739
suffice. If metal fixation can be dispensed with, so Imuch the better, but it is absurd to make the non-useof metal sutures a guiding maxim of bone surgery.Having fixed the fitted bones together by propersutures the limb is immobilised by an external splintor plaster-of-Paris.To recapitulate the essential points. Secure fresh I
bone by cutting away the unhealthy ends ; provide Iwide contact of the freshbone surfaces by accuratefitting; ensure close con-tact by proper sutures ofwhich the metal bandsand bolts are the mostreliable; and get properprolonged fixation by anexternal splint whichmust be worn for threemonths at least.
BONE-GRAFTINGOPERATIONS.
The ideal and obviousmethod of treating un-
united fractures is byputting in a bone graft.But it is well at the outsetto realise that this methodhas very definite limita-uons, ana mat tne conuinons ior success are veryexact.A piece of bone cut from the living bone of the
Ipatient is endowed with very limited vitality. It has Iliving bone-cells, but for the most part these are
locked up in the depth of the dense skeletal tissue.It has blood channels cut off from the active circula- Ition, and it has a strong rigid frame which can be used ias an internal splint or strut, whilst this framework isporous and is thus capable of acting as a scaffold workinto which new bone tissue may penetrate from
11
Gap fracture of radius resulting from gunshot injury in which bone graftinghad twice failed.
neighbouring active bone. It has no power of inde-pendent growth, and if it is placed in any living tissueother than the skeleton it rapidly withers away. Its Ipower of producing new bone is very limited, and bymany authorities is considered non-existent. When Iused to repair a defect in a long bone it can act infour ways. First, as an internal fixation splint ; Isecond, as a strut by which continuity being restored
to t broken bone, the latter is provided with afunctional stimulus ; third, as a scaffold, in and aroundwhich new bone is built up ; and fourth, as a sourceof new bone. The functions of the graft as an agent offixation and osteo-conduction are clear and obvious,whilst that of osteogenesis is problematical. But apiece of dead bone will carry out the function offixation and conduction, and it often becomes a
FIG. 10.
Same case as Fig. 9 after transplanting ulna into radius.
question whether it is worth while using living bone
just for the sake of its osteogenetic power. If a gap hasto be bridged, then living bone must be used for thegraft, but if the pieces of the broken bone can bebrought into contact and the graft buried in livingbone, then dead bone may be used, and should be used,if greater strength is demanded than can be providedby a live graft.Exactly the same principles apply to the fitting and
fixing of a graft as have been laid down for the fittingand fixing of the bone ends of an ununited fracture.
FIG. 11.
Same case as Figs. 9 and 10.X rays three years later.Strong working hand.
That is to say, wide contact with live bone, firmfixation, and efficient immobilisation. And if thegraft is used to bridge a gap it must be as stout andas strong as the bone it has to replace.An autogenous graft is usually cut from the inner
surface and crest of the tibia, which in an adult iscapable of providing a piece of bone 8 in. long, in.wide, and in. thick. A motor-driven circular saw

740
cuts the graft quickly, neatly, and with precision,and I have seen no evidence that the use of this instru-ment produces any interference with the vitality ofthe graft. It is not essential to take periosteum withthe graft, although I think it is an advantage, becausethe attached membrane will help as a medium ofvascuiar ex-
change betweenthe graft andthe tissues ofthe bed intowhich it is laid.
The fitting ofthe graft intothe broken bonemay be carriedout in variousways, driving itinto the marrowcavity, em-bedding it inthe surface, or
by combining these methods, placing one end in themedullary canal, and fixing the other in a slot cutin the cortex.
Intramedullary Grafting.-If a bone graft of suitablesize and shape be driven into the marrow cavity of atubular bone it will rapidly become consolidated withthe latter. I think this admits of no doubt, and yetintramedullary grafting has fallen into undeserveddisrepute because of the technical difficulty of placing
FiG. 13.
Fractured radius resulting from gunshot Same case as Fig. 13 with graft of adequate Same case as Figs. 13 and 14.injury. Shows graft too small, no contact, size and fixation. Two years later.and no fixation.
the graft tightly in each fragment. This can beaccomplished in various ways. The graft can be driventhrough the end of the bone so as to nail one fragmentto the other. This is possible for a fracture near eitherextremity of the humerus or for one at the proximalend of the femur or ulna. Or it may be driven intoone fragment, whilst the other fragment is split toreceive it and then tied together with wire or silk(Figs. 4 and 5). In dealing with a gap fracture, the graft
is shaped like a cricket bail, one end being driveninto one fragment whilst the other is manoeuvred intoposition by angulating the other fragment out of thewound and slowly straightening the bone whilst thegraft is engaged in its cavity. Or the graft may bemade in two pieces, one is driven into the marrow
Specimen from the Museum of the Royal College of Surgeons (a femur whichhas been grafted). This specimen shows (1) no contact between mainfragments ; (2) inadequate size of graft; (3) inadequate fixation.
cavity of each fragment, and the two grafts are thenfixed together. Of these various devices the thrust-and-split method is the most satisfactory, because itgives the greatest contact between the graft and thehost bone.
Cortical Inlay Grafting.—In this method a slot iscut in the surface of both fragments of the fracture,and into this slot is fixed a graft which is made tofit accurately into the slot. The actual fitting is
facilitated by using anFIG. 14. aluminium plate as a..
template to measure the.size both of the slot andthe graft. It necessitatesa very free exposure ofthe broken bone, becauseat least one-third of itslength should be involved
FIG. 15.
in the grafting operation in order to give strength andrigidity. It is particularly suited for the tibia or oneof the forearm bones, because it supports one sidewhilst the other side is held by the companion bone.The graft is fixed in its bed by accurate fitting, bysewing the soft parts over it, or by bone nails or screws.
Use of Beef Bone or Ivory Pegs or Plates.-If thegraft has to be buried in living bone then a strongdead graft is often better than a weak living one
741
Thus, in a fracture of the neck of the femur an ivoryor bone peg used as a nail driven in through the greattrochanter will give a good result, provided thataccurate apposition of the fractured surfaces withoutinterposition of soft parts be secured. In an ununitedfracture of the femur, where it is desirable not toshorten the leg by a step-cut operation, it is difficult toget a living bone graft strong enough for the purpose.In this case a pair of ivory plates (Figs. 6, 7, and 8)may be used or else a tibial bone graft may be placedon one side of the fracture and an ivory plate on theother and the two plates then bolted together.
SUPPLEMENTARY BONE-GRAFTING METHODS OFDOUBTFUL VALUE.
There are certain methods of bone grafting, foundedchiefly on theoretical considerations, which mustbe considered briefly. These are the use of so-calledwafer grafts formed of periosteum with a thin layerof underlying bone, and the employment of bonechips. In my own practice and in experimental workboth these methods have invariably led to failure.I would therefore relegate them to a very subsidiaryr6le in the treatment of ununited fractures. It ispossible, when the fracture has been fixed by one ofthe above-mentioned methods, that by wrapping apiece of periosteum with adherent chips round thefracture, or by packing in little bits of bone takenfrom the crest of the ilium the consolidation may behastened, but I am not clear even on this point.Certainly the process of absorption is much moreevident than that of callus formation.Bone Shortening or Bone Substitution.-It not
infrequently happens that more than one operationhas failed to cure an ununited fracture. If this is thecase with the forearm or the leg, there is anotheralternative to abandoning the case or submitting itto a case-splint or to amputation. This consists inshortening the companion bone, or substituting onebone for the other. In a gap fracture of the tibiaa piece may be taken out of the fibula, sufficient toallow of the tibial fragments being made to impact or overlap. In a gap fracture of the radius, in whichgrafting has failed, the ulna may be divided and theproximal portion implanted into the distal part ofthe radius (Figs. 9, 10, 11). This gives a strong, 1straight arm, curing the radial deviation of the hand, ialthough not permitting movements of pronation or fsupination. ,-
CAUSES OF FAILURE.
Apart from certain conditions-e.g., sepsis, activeor latent, or the presence of general disease or debilitywhich prevents the success of any surgical procedure-the local cause of failure of operations done forununited fractures may be grouped together underthe following heads: 1. Inadequate contact ofbone ends (Fig. 12). This may be due to thesclerosed bone or fibrous tissue not having been cutaway or to the raw surfaces not having been fixedtogether efficiently. 2. Inadequate fixation of thefracture either by reconstructive operation, graft, orsplint. 3. Inadequate grafting in respect of the graftbeing too small, having no contact, or not being fixedto the host bone (Figs. 13, 14, 15). 4. Inadequatesplinting of the limb after operation. 5. Excessivetension. If great force is used in reducing an oldfracture there is immediate danger of shock, and later,risk almost amounting to certainty, of the mendedfracture being pulled apart by the tension to whichit is subjected.The successful treatment of an ununited fracture
will often test your skill as a mechanic, your techniqueas a surgeon, and your patience and optimism as amender of the maimed ; but the results of success arewell worth striving for, because they are nothing lessthan converting a cripple into a whole man, and ifin accumulating the experience upon which thislecture is founded I have made many mistakes andencountered many failures, my sincere hope is thatyou may avoid the mistakes and be rewarded byunvarying success.
An AddressON
AVENUES IN MEDICINE.
Delivered at the Opening of the Winter Session of theLondon (Royal Free Hospital) School of
Medicine for Women
BY SIR CHARLES SHERRINGTON, O.M.,G.B.E., M.D. CAMB.,
PRESIDENT OF THE ROYAL SOCIETY.
ON the opening day of the session, with some here, for whom it is the commencing of a profession, our’
thoughts turn naturally to questions of what thatprofession has to offer and what it demands. Theperspective of the avenue along which the professionof medicine is reached has many interesting pointsas viewed from either end, though I can deal withbut a few among them.Here in this school I imagine all students enter
the profession for no other reason than that medicineearnestly attracts them. That pledge of enthusiasmis a valuable asset for the student herself and forher teachers, as also for the school and for the profes-sion. If we ask what ground there is for that enthu-siasm, we may in the first place as practical peopletake this, that there are in the nature of things notso many callings open to women as to men, and thatmedicine can and does provide for women to-day ameans of earning an independent living. The averageannual earning of the medical practitioner in thiscountry to-day is, I believe, put at between £500and jE600 a year. I see little to suppose that thatestimate is not applicable to the woman as well asto the man practitioner. It is not, to my mind, adiscouraging average in the era before us, whichmust perforce be one of national economy andfortitude.
It is an average v-hich doubtless regards chtelly’ the general practitioner. Though general practice
is the main path of the profession, there are other,
far from negligible though relatively exceptionalones. There is consulting work and there is specialistwork. Some of those present here to-day brilliantlyexemplify the success in these that is attained
by women. There are also medical branches ofGovernment service, and I need not name to youwomen, and from this school, who hold distinguishedand responsible positions in those services. DameJanet Campbell, a senior medical officer of theMinistry of Health, we remember, is a former studentof this school. And there are, further, other publicservices as well, municipal and county posts. Perusalof the list of registered medical women, formerstudents of this school, show how considerable a
number of such posts are occupied by them.But no more than does it satisfy man shall it
satisfy woman to live by bread alone. Bread alonewill not account for enthusiasm in the choice ofmedicine as a calling. Medicine has been termedwith some justice a poor trade ; but at the sametime it is known as a noble profession. If we canjustify this latter belief it is a truer source forenthusiasm. And it is a claim that can be justifiedon many grounds.
MEDICINE A PROGRESSIVE SCIENCE.One of these grounds, though I do not say the
main one, is yet a memorable one, and rises early tomy mind. Medicine is not only an honourable art buta progressive science. In this respect it is an excep-tional calling ; indeed, among callings available forwomen it stands in this respect almost alone. Likeit engineering is at once a science and an art ; butengineering is not a profession available .for women.
r3