Embed Size (px)
Citation preview

Jonathon Burke [email protected] 200604685
Amyloid diseases: Is there light at the end of the tunnel?
Abstract Alzheimer’s disease is an ever-prevalent disease, effecting millions of people globally. In 1907 Alios Alzheimer hypothesized that amyloids play a key role in the development of Alzheimer’s via the amyloid cascade theory. Since then researchers have looked to examine and provide statistically significant data to support this hypothesis. Although there is disagreement in the exact mechanism of impact, amyloid-beta is thought to be key in Alzheimer pathology. These various mechanisms will be assessed to provide an understanding to how Alzheimer’s and amyloids are intrinsically linked. From there the question ‘is there light at the end of the tunnel?’ will be answered by looking at current developments in early detection and treatments in current research.

Introduction The impact of Alzheimer’s disease is felt not only in developed countries, but also the entire globe. There are 830’000 people suffering with Alzheimer’s in the UK alone, which has a cost of £23 billion (27). It is therefore clear why a fast and effective treatment for Alzheimer’s disease is a priority for many drug companies. To understand the treatments and future research, we will look at Alzheimer’s and the impact of beta-amyloids in the disease. From there we will look into the different approaches taken by researchers into effective treatments: from fast diagnosis to ultimately finding a cure. (26,27)
The effects of Alzheimer’s spreads past the memory loss generally associated with the disease. Cognitive functions that a healthy human takes for granted are affected at different levels depending on the patient. The degenerative disease impacts all visual and motor spatial and language skills. This over the course of the disease causes great distress to patients and family members, as not only is memory loss prevalent, but basic day-to-day skills are progressively lost. (3,5,7)
Advancing age, genetics and environmental risks are all major factors that impact on the development of Alzheimer’s disease. A.B. Graves et al, state that the major factor in development of Alzheimer’s is age. Studies suggest rates of 1-2% for 65-74 age group with these rates doubling every 5 years. This increases to 25% in 85 and over. There is conflicting data about the environmental impacts on Alzheimer’s development. It has been postulated that lower education levels and a propensity for depression can have an impact on Alzheimer’s development, although not concurrent in studies. Smoking, age of mother at birth, and certain health conditions are also believed to have an impact. It is difficult to truly assess the environmental impacts on the development of Alzheimer’s disease and therefor apart from living a healthy life, unlikely to deem credible impact on the treatment of Alzheimer’s. We can, take clear data from this aging population, which will benefit current and future Alzheimer’s research and treatment development. By doing this we can hope to learn from the effects of age on development of Alzheimer’s and therefore look to limit certain tributary steps that age effects. (3,6,7,10,13)
There has been considerable research into Alzheimer’s disease, with a common factor pointing to the impact of Amyloid’s in the development of AD. To consider if there truly is “light at the end of the tunnel’, it is beneficial to first look at amyloid pathology and its impact on AD. From there it is possible to consider how this link can be used to detect the onset of Alzheimer’s disease through early detection methods. Along with early detection mechanisms, information into the links between Ab and Alzheimer’s disease is leading to promising treatments, of which we will assess some of the current developments.

Amyloid-b pathology and Alzheimer’s disease Amyloidosis is the misfolding and accumulation of extracellular proteins that causes a specific disease. There are 27 human proteins with the ability to be amyloidogenic. There is a lot of attention paid to amyloids, as their aggregation is associated with a variety of organ illnesses. Karen E et al (10) “Amyloid is an abnormal extracellular fibrillar protein deposit in tissues”. A variety of different proteins allow varied deposition and therefore attribute to many syndromes associated to respective fibril protein precursor. In general terms, amyloid formation occurs when a peptide doesn’t acquire its functional fold allowing the ordered formation of fibrils. The likelihood for fibril formation is increased with certain in vivo factors: increase in protein concentration, unstable amyloidogenic proteins protein cleavage and age. Although there is disparity in suggested mechanism’s for Beta-amyloid pathology in Alzheimer’s disease, it is clear that is has an impact on disease development. (6,10,13,23)
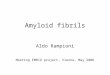
Beta amyloids are made up of 40 and 42 amyloid-b peptides (Ab 40. Ab42). B and Y secreteases allow secretion of the Ab protein precursor (APP), it does this through the B-site APP-cleaving enzyme (BACE-1). This cleavage generates an APPb (sAPPb) and a membrane-bound C-Terminal fragment of APP (CTFb). C-terminal APP is then cleaved by Y secretease forming other lengths of APP (37,38, 43). Further Ab is generated by the enzymes isomerase, glutaminylcyclase and aminopeptidase. (6,10,13)
Figure 1, APP processing to generate Amyloid-beta (amyloidogenic and non-amyloidogenic pathways)(13)

In 1907 Alios Alzheimer ‘s examination of AD brains found an accumulation of b amyloid and hyperphosphorylated tau protein. These were seen to form plaques and neurofibrillary tangles, leading to the amyloid cascade hypothesis. (10)
Figure 2, The amyloid cascade hypothesis. (10)
An increase in Ab is thought to cause a variety of neurotoxic changes: oxidative stress, fibril deposition, tau protein aggregation and inflammatory responses. (Future science editorial). Accumulation of b-amyloid in the brain parenchyma is hypothesized to be a crucial step in the onset of AD. Dominate mutations of three genes; presenilin1 (PSEN1), presenilin2 (PSEN2) and amyloid precursor protein (APP) allow this accumulation to occur. Although it is clear the relationship between cognitive decline and Ab deposition is not linear, Ab-derived diffusible ligands and soluble oligomers are proposed to account for neurotoxicity. (10) There are many ongoing studies into this hypothesis, but so far there is increasing evidence to show that the cognitive decline present in AD is caused by the accumulation of soluble oligmeric assemblies of Ab. Insoluble Ab plaques are thought to also effect cognitive function but data is not always consistent with neuronal degeneration. (13)
Since hypothesizing the amyloid cascade theory, further research into the relationship between Ab and Alzheimer’s disease has been conducted. Using modern techniques, there have been significant developments into the understanding of this relationship. Although there is ongoing debate into the exact relationship between, it is important to review the relationship’s outlined in modern scientific journals. These studies offer some insight and support for the potential mechanism of AD development via amyloid-beta deposition.

Synaptic health by signal transmission among neurons (LTP) is reduced in AD patients by accumulation of Ab. As there is a clear link between synaptotoxicity and memory loss in AD, it is thought that Ab may inhibit LTP by oligomer-targeted receptors at the synaptic plasma membrane. Snyder et al. proposes that endocytosis of N-methyl-D-aspartate (NMDA) receptors causes disturbance in calcium influx. There is interaction with receptor for advanced gylcation end (RAGE) products receptor and insulin receptor, which induces oxidative stress. Build up of reactive oxygen species (hydroxyl radical, superoxide radical etc.) leading to oxidative stress is shown to cause synaptotoxicity leading to neuronal death by Ab oligomer. A strong correlation is reported between oxidative damage levels and dementia. Varying mechanisms are proposed, “Klein and colleagues proposed that ADDLs induce LTP accompanied with oxidative damage”. It is understood that superoxide dismutase (SOD) converts superoxide radicals to hydrogen peroxide. The amount of SOD in AD brain was larger than in normal brains. K. Murakami et al found that, in mice with both AD and raised SOD levels, “Ab oligomerization associated with memory loss and synaptic loss was worsened”. This implies that there is “stimulation of the amyloidogenic pathway by cytoplasmic superoxide radicals”. (13)
There are continual studies into establishing the link between b-Amyloid and Alzheimer’s. This is because the exact method off effect and therefore positive correlations are largely hypothesized. Villemage et al (2012) and Ellis et al (2013) show an association between amyloid-b positivity and decline in episodic memory (18 &36 months) in clinically diagnosed mild cognitive impairment (MCI) patients. The cognitive decline in these otherwise healthy patients shows that Alzheimer’s related neurodegeneration could be detected with pre clinical diagnosis. To further this research, Yen Ying Lim et al (2014) proposed “all aspects of cognitive function would remain stable in healthy older adults and individuals with MCI who were Ab negative”. Healthy older adults showed no change in cognitive function, however individuals with MCI showed improvement in cognitive function. Suggesting that patients diagnosed with MCI but not Ab positive are suffering with neurological problems other than Alzheimer’s. (11,13)
Yen Ying Lim et al (2014) also hypothesized that “in healthy older adults, individuals with MCI and individuals with Alzheimer’s disease, Ab- positivity would be associated with decline in memory over 36 months”. This showed that, in amyloid-b positive healthy older adults, verbal and visual episodic memory showed a moderate decline over 36 months compare to amyloid-b negative healthy older adults. MCI amyloid-b positive patients showed a larger rate of decline in verbal and visual episodic memory when compared to Ab negative healthy older patients. Language, attention and visuospatial functions also declined in MCI Ab- positive patients. Patients with Alzheimer’s who are amyloid-b positive exhibit large cognitive function decline when compared to amyloid-b negative healthy older adults. The greatest area of decline was language and visuospatial function. (13)

Jack et al (2010,2013) proposed the pathophysiological model of Alzheimer’s disease that suggests amyloid-b accumulation slows after meeting the clinical criteria for Alzheimer’s. This means the temporal element must be considered when looking amyloid-b levels in younger adults. Yen Ying Lim et al (2014) show that cognitive decline in Ab positive Alzheimer’s patients does not plateau, but continues to decline at a similar rate to non-MCI Ab positive patients. This continual memory decline, coupled with the increase in non-memory decline, is indicative of even the earliest stages of Alzheimer’s disease. This suggests that assessing non-memory functions in Alzheimer’s disease could be beneficial for the detection of early disease development. (11,13,17)
Yen Ying Lim et al (2014) also show that there is a relationship between the amount of amyloid-b positivity and Alzheimer’s. Quantifying the relationship between Ab and Alzheimer’s development is fundamental in providing significant links. It is proposed that an SUV ratio of >1.90 is optimal for diagnosis. Therefore, in patients who are not currently clinically diagnosable as having Alzheimer’s, but have an SUV ratio of >1.90 have a higher positive predicted rate of Alzheimer’s progression. It also suggests a relationship between the amount of Ab present and cognitive decline associated with early onset Alzheimer’s. By providing doctors with a way of assessing the risk a patient has of Alzheimer’s when not showing signs of MCI, preemptive steps to actively combat the disease could be taken. (11)
It is clear that Ab pathology and Alzheimer’s disease are intrinsically linked. Poor clearance of amyloid-b precursor protein could be critical in the early development of AD, as it leads to Ab accumulation and plaque formation long before clinical diagnosis. Frontal and parietal midline structures and the default mode network (DMN) are areas of high metabolic activity and intrinsic functional connectivity. The DMN is linked to deposition of plaques due to overlap in average deposition regions with the DMN. This overlap has lead to the theory that Ab neurodegeneration in Alzheimer’s disease “occurs along network boundaries, spreading to functionally connected areas rather than to spatially contiguous but less connected neighbours”. This implies two relationships: reduction in intrinsic activity and connectivity linked to Ab, and a positive relationship between high connectivity and high Ab pathology. Nicholas Myers et al (2014) found that, in early onset Alzheimer’s disease, there were two effects of PIB-uptake on connectivity. The highest areas of connectivity showed the highest level of plaque buildup on a globular network level. On a local network level, “plaques are negatively liked with connectivity”. The observed characteristics of early onset AD, that primary sensory and sensorimotor regions are largely unaffected was supported by the observed plaque distribution in heteromodal networks. It was observed that patients with early onset AD exhibited significant level of Ab plaque formation, with the posterior DMN most affected, confirming a relationship between Ab plaque load and connectivity. This relationship supports the hypothesized statement that amyloid-b pathology has a negative impact on intrinsic connectivity, but was also seen to go past the DMN to other heteromodal networks. It is therefore possible to suggest that in the early stages of Alzheimer’s disease, Ab-pathology is linked to increased connectivity. In the later stages of AD amyloid-b pathology is linked to decreased connectivity, but it must be remembered that some areas of the brain will be affected at different rates to others. (3,14,16,20)

The effect of amyloid-beta on Alzheimer’s is seen in a variety of areas. A decrease in synaptic activity by neuronal decay leads to an overall decrease in memory. Evidence to show this is linked to Ab oligomer accumulation suggests that amyloidosis is impactful in MCI related to Alzheimer’s disease. This synaptic decay is seen to be more prominent in areas of high metabolic activity such as the DMN. This suggests that areas of higher intrinsic functional connectivity are prone to greater levels of synaptoxicity and therefore exhibit the strongest impact of Ab aggregation. It can be seen that an overall increase in the amount of amyloid-beta accumulation correlates with the onset of AD, and that the amount of Ab present is proportional to the development of observed Alzheimer’s disease. This accumulation is seen to effect both memory and on memory areas of cognitive function, with visuospatial and attention functions also effected. Although the above studies present the effect of amyloid deposition with different mechanisms, they all show the same underlining problem; that amyloid deposition impacts on brain function in AD patients. The variety of hypotheses open up many avenues for future research into both the stated relationship, and to future treatments for Alzheimer’s disease. (1,3,14,16,20) Early detection In a clinical setting, it is regularly observed that a patient is exhibiting some, but not all signs of Alzheimer’s development, before a full clinical diagnosis can be achieved. It is often the case that the impact of Alzheimer’s is too far onset by the time full clinical diagnosis is accomplished. For there to be ‘light at the end of the tunnel’, a combination of approaches to tackling Alzheimer’s disease could be taken. If it is possible to assess and diagnose AD development prior to current clinical diagnosis, more time can be given to patient and doctor to effectively treat the disease. Studies into the development of the disease and identification methods offer potential into possible steps for quick diagnosis. It is important to assess any relationships between amyloid-b pathology and the reduction in cerebral blood flow in Alzheimer’s patients. This is because rate of cerebral blood flow and effects on locations within the brain, may have an impact on future treatments that target Ab fibrils. There is also observed relationships between rate of CBF and metabolic activity of the brain, indicating brain activity. Miklas mattsson et al (2014) found that ‘brain amyloid-b load was associated with reduced CBF in poro-parietal regions across all subjects”. CBF in Ab positive patients was reduced when compared to Ab negative patients. It was also found that the effects of Ab load differed between CBF and volume, suggesting “Ab has a stronger association with brain function than with structure in mild disease stages, but larger associations with structure in advanced stages”. Lowered CBF in temporo-parietal and frontal regions in AD patients was found which supports Alsop et al (2010) findings. Miklas mattsson et al (2014) observed “reduced CBF in several AD related brain regions regardless of cognitive status”. This supports the hypothesis that Ab positive subjects have Ad pathology, but also that MCI early and late have varying level of AD pathology. The positive correlation between higher amyloid-b load and increased CBF in several brain regions in AD patients was found. This increase in perfusion is suggested to be a compensation for Ab neurotoxicity. The generally accepted hypothesis that AD starts with Ab pathology in healthy adults, following a progression of neurodegradation, reduced brain activity and clinical symptoms is supported by Miklas mattson et al (2014). By dividing groups into Ab load and then

comparing within the diagnostic groups, they were able to determine a reduction in CBF for early and late MCI and Alzheimer’s patients. From this it could be possible to isolate Ab positive Alzheimer’s patients in people with varying cognitive decline. (11,12,14,16) Another consideration by Miklas mattson et al (2014) is the varying association between Ab pathology, CBF and structural measurements. Ab load was associated to reduced CBF, but a small/positive impact on grey matter volume. However, when compared with Ab positive late MCI or Alzheimer’s patients, the effects of Ab on structure were more significant. There were greater reductions in brain volume than CBF, which support assessments of advanced stages of the disease. Negligible differences in early MCI support the hypothesis that synaptic loss is a primary step in Alzheimer’s disease development. Synaptic loss causes an overall reduction in brain activity, which can be seen in a reduction of CBF. From Miklas mattsson et al (2014) it is possible to postulate that early onset Alzheimer’s may be represented by a reduction in CBF before grey matter reduction. This opens up the possibility for doctors to diagnose high-risk patients based on CBF far sooner than if they were assessing grey matter atrophy. The accumulation of amyloid-b is also considered an early indicator of Alzheimer’s disease. Through combined use of PET and CSF biomarkers, it is now possible to visualize fibrillar Ab plaques in the brain. 11C-pittsburgh compound B (PIB) is regularly used as it has been heavily studied, showing detection of Ab fibrils with high accuracy. The use of PET with PIB has shown high retention of the biomarker in AD brains, as well as MCI patients prior to Alzheimer’s development. The use of other biomarkers is a key area of development for AD diagnosis. 18F-florbetapir and 11C-PIB have shown promising associations, and offer benefits over 11C-PIB. 18F amyloid tracers have the potential to be more suitable for clinical usage, as they have a longer half-life, allowing greater distance between cyclotron and hospital. They also require a shorter scan time (10 min) compared to 11C-PIB (60-90 min). (11,12,14,16) Ruiqing Ni et al (2013) assessed the use of 3H-PIB as a suitable biomarker. Using the frontal cortex as a region with high amyloid and hippocampus with low amyloid load. High and low affinity sites in the frontal cortex and hippocampus were observed in AD patients, compared to only low affinity sites in normal patients. A common high affinity binding site for PIB in AD brains were also observed. The ratios of high to low in the frontal cortex was 6:1, hippocampus 3:1 and this has been attributed to more high affinity sites in the frontal cortex. Tracer retention was observed in small amounts of the control, which lends itself the effects of age. Although low affinity sites aren’t imaged using current techniques, they could have an impact on Ab aggregation and overall development of Ab pathology in the brain. From the findings, Ruiqing Ni Et al (2013) propose a multi-binding site model (1,2 &3). When considering early detection, it is important to make sure that all variables between patients and AD models are considered. Nicholas Myers et al (2014) ‘analyzed the within subject relationship between amyloid-b pathology and functional connectivity”. By creating this model, future research can be carried out to further the hypothesized model, and so allow a greater understanding between the links. If supporting data is found, it could yield a strong boost to early detection and quantization of the development of the disease in patients. It could also yield future developments in biomarkers for early detection. (11,13,14,15)

By combining a greater understanding into the expected pathological development of Ab aggregation in Alzheimer’s disease patients, with more effective tracers and modern imagining techniques, there could be ‘light at then end of the tunnel’ for early detection. It is feasible for researchers to be able to develop a clear early detection system for the development of AD in patients exhibiting some cognitive impairment. Treatments For there to truly be ‘light at the end of the tunnel’, effective treatments for Alzheimer’s disease are needed. Due to the high cost involved, pharmaceutical companies at great risk undertake drug development. According to alzforum, there are 44 amyloid-related therapies listed. Of these 44, 12 are discontinued and 3 are inactive. Although there is great risk involved at a drug failing, pharma companies invest heavily due to the potentially lucrative business in successfully developing an effective treatment. Amyloid-b immunotherapy is researched as a potential treatment for AD. There are currently 2 passive immunotherapy treatments at stage 3 of clinical trials: Gantenerumab and Solanezumab. Although active immunization is successful in lowering Ab oligomer levels, there are significant safety concerns associated with this method. The removal of both pathological and non-pathological Ab is thought to be the reason for this, and as the function non-pathological Ab is not fully understood, it should be avoided in current techniques. Passive immunization, through the regular administration of antibodies could therefore be an option for AD treatment. This method allows the use of antibodies that work against specific conformations of Ab, of which there are over 600 currently listed. Presuming that the antibodies can cross the blood brain barrier, two mechanisms for the antibodies are suggested. Binding of antibodies to Ab complex induces phagocytosis, and the antibodies prevent that aggregation of Ab. The use of conformation specific antibodies to attack different lengths of Ab is an option for treatment. Antibody A11 reacts with several types of Ab but doesn’t recognize Ab fibrils. This is useful as it is binding to Ab intermediates, which could allow active combating of Ab oligomers before fibril formation. Further development of A11 to be an antibody for annular protofibrillar oligomer (aAPF) extends the applications of A11. OC antibody has the opposite effect of A11; it recognizes only amyloid-b fibrils. As previously stated, increased levels of fibrillar Ab oligomers are found in the brains of AD patients, indication a clear use for OC antibody. However no significant difference in prefibrillar Ab oligomer was found, meaning the use of stage 1 A11 could be largely ineffective. There are, however, raised levels of aDPF in the CBF pre-clinical diagnosis for AD. This opens up the use of stage 2 A11 as a biomarker for aAPF. (3,5,13,26)
As it is known that Ab-42 ADDLs cause oxidative stress and synaptoxicity, the formations of relevant antibodies could yield positive effects. Anti-ADDls antibody (Nu-1) allows the discrimination between Alzheimer’s and non-Alzheimer’s brain. Nu-1 has been shown to “significantly rescue Ab-42 induced LTP inhibition as well as ROS”. Further development of NU-1 to combat localized ADDLs and so to inhibit dendritic spine reduction has yielded further positive results. Globular Ab-42 oligomers have been shown to “inhibit spontaneous synaptic function”. The antibody A-887755 has shown to only recognize globular Ab-42 oligomer and not monomer or fibril plaque formations. This allowed induced synpatoxicity to be neutralized

allowing an improvement in novel object recognition. The use of A-887755 in passive immunization was also found to improve overall cognitive function and increased synaptic density. With the observed dangers in plaque removals, these antibodies could offer a safe alternative to other AD treatments. Toxic conformers of Ab-42 are thought to occur through an oxidation in a peptide in the oligomer. Although it is thought that this oxidation can occur at various turns, oxidation at Met35 (turn 22,23) forms toxic Ab-42. These toxic oligomers have observed synaptoxity and therefore offer an option for treatment to negate their effect in AD. A developed antibody, 11A1, has shown the ability to recover neurotoxicity and inhibit cytotoxicity. 11A1 did this by detecting the related toxic Ab-42 oligomers stopping aggregation and neurotoxicity. It has also been observed that 11A1 also recognized intracellular Ab, this staining occurred in both AD and non-AD brains. The isolation of intracellular Ab in non-AD brains by 11A11 has lead to the possibility of pre AD detection. NU-1 also showed intracellular Ab staining. Although it is unclear how deposition of intracellular Ab-42 occurs, its potential as antibody target should not be ignored. (3,5,13,26) As well as environmental factors, genetic variation is a risk factor for the onset of AD. Variation in the APOE gene increase disease risk as normally functioning APOE helps in the formation of HDls, which aid in the degradation of soluble Ab. Agonists of APOE receptors “also act on macrophages and microglia” to form alternative active sites and promote phagocytosis. It is fair to assume that expression of these agonists could aid Ab clearance and therefore alleviate AD risk. Paige E. Cramer et al (2014) identified that RXR agonist would allow APOE expression, which, in turn, would aid Ab clearance and promote phagocytosis. Bexarotene (RXR agonist) lowered Ab levels in the CBF within 6 hours and offered a 25% reduction at 24 hours. Further reduction was seen over a 70-hour period, with a return to normal levels after 84 hours. With continual dosage, a 30% reduction in soluble Ab levels and 40% in insoluble Ab was observed. Similar results were expressed in later stages of AD, suggesting that bexarotene works across all stages of AD. As was previously suggested, soluble Ab deposition has a negative effect on MCI through impairment o synaptic function. Beraxotene exhibited restoration of cognitive function, memory and improvements to impaired olfactory systems. (1,4,6,9,18)
A problem with delivering treatments for Alzheimer’s is getting the drug across the blood brain barrier in the correct dose. Nanoparticles offer an interesting area of research for drug developers to combat this issue. They offer the possibility to not only deliver a range of drugs, but also have the ability to provide the drug for a sustained period of time. Juliana B. Hoppe et al (2013) approach the use of nanoparticles with curcumain, which is understood to have neuroprotective effects. The use of lipid core-nanocapsules coated in polysorbate 80 to enhance the brain delivery of the drug. An appeal to nanoparticles is there ability to provide a therapeutic dose to the target with decreased amount of administered drug. The dose necessary for nanoencapsulated was 20fold lower than that of free curcumin. Exhibiting a higher concentration (2.5 times) in cerebral tissue over free drug and a longer mean residence time (14 times) than that of the free drug. The ability to provide a specific drug, in smaller administered doses for a longer duration, could open up possibilities past the administration of curcumin. LNC’s also seem to avoid side effects over a 28 day treatment, due to being non-toxic and reduced dosage. Both nanoencapsulated and free curcumin were seen to be active in preventing

inflammation, tau hyperphosphorylation, behavioral impairments (seen to be associated with Ab aggregation) and signal disturbances. It is hypothesized that the hippocampal region is crucial in AD patients, and therefore synaptic loss correlates to cognitive impairment. It was observed that curcumin, in both forms, acted against Ab related synaptocicity due to raised synaptophysin levels. Ab is also thought to trigger microglial cells, which are active in neurodegeneration by phagocytizing after synaptic rewiring and release of proinflamatory cytokines. Both forms of Curcumin were seen to decrease microglial activation, but only LNC reduced levels of cytokines in the hippocampus. This is hypothesized to be caused by LNC’s greater bio-distribution throughout the brain. BDNF/neurotrophins are noted to decrease with an increase in proinflammatory chemicals. Curcumin was seen to rescue and then up-regulate BDNF levels in the hippocampus, which leads some way to explaining the cognitive improvements exhibited. BDNF acts through the AKt pathway to maintain neuronal health; Ab in AD brains directly impacts this. One such component of AKT pathway is GSK-3b, which has roles in tau phosphorylation and cytokine production. Treatment with curcumin stabilized phosphorylation and inhibits GSK-3b. (8,17,24,25,26) Tau protein phosphorylation, and neurodegeneration by Ab is key in AD pathology. Hyperphosporylation of the tau protein causes reduction in microtubule affinity. Detachment of microtubules disrupts axon transport resulting in synaptic degeneration. There is one treatment for tau phosphorylation in phase 3 clinical trial; TRx0237. It is a small molecule treatment that is already approved for treatment of malaria and methemoglobinemia. (8,13,17,24,25,26) Conclusions With Alzheimer’s having a large, cross-population impact, both researchers and pharmaceutical companies are searching for the ‘light at the end of the tunnel’. Research is continual into understanding the link between Alzheimer’s disease and amyloid-beta aggregation. Although there is not currently a unanimously agreed single mechanism for the link between the two, it is possible that there are a number of different pathways that Alzheimer’s disease goes down in relation to Ab accumulation. By taking a step back and assessing all these avenues, there may be a possibility of finding common ground between all these hypotheses. The chance of decreasing diagnosis time offers a unique opportunity to the treatment of Alzheimer’s. By isolating a patient as being high risk/early onset then a patient is open to treatment a lot earlier. This may allow more effective therapy and potential to overcome the disease before lasting synaptic damage is done. A major risk with late detection is that brain atrophy is past the point of acceptable recovery, therefore emphasis on early detection is key to there being ‘light at the end of the tunnel’. Combining this early detection with treatments in development could be a fruitful path for overall treatment. Immunotherapy and Ab clearance offer future generations a real chance of overcoming Alzheimer’s. This review set out to see if there was truly ‘light at the end of the tunnel’; with current research and future developments in both techniques and understanding, science offers a real opportunity for this life changing disease to be beaten.

References 1. Algamal, M. et al. Mapping the Interactions between the Alzheimer's A beta-Peptide and Human Serum Albumin beyond Domain Resolution. Biophysical Journal. 2013, 105(7), pp.1700-1709.
2. Brinton, R.D. Neurosteroids as regenerative agents in the brain: therapeutic implications. Nature Reviews Endocrinology. 2013, 9(4), pp.241-250.
3. Buxbaum, J.N. and Linke, R.P. A Molecular History of the Amyloidoses. Journal of Molecular Biology. 2012, 421(2–3), pp.142-159.
4. Cramer, P.E. et al. ApoE-Directed Therapeutics Rapidly Clear beta-Amyloid and Reverse Deficits in AD Mouse Models. Science. 2012, 335(6075), pp.1503-1506.
5. Fernandez-Busquets, X. Amyloid fibrils in neurodegenerative diseases: villains or heroes? Future Medicinal Chemistry. 2013, 5(16), pp.1903-1906.
6. Gillmore, J.D. and Hawkins, P.N. Pathophysiology and treatment of systemic amyloidosis. Nat Rev Nephrol. 2013, 9(10), pp.574-586.
7. Holroyd, S. and Shepherd, M.L. Alzheimer's Disease: A Review for the Ophthalmologist. Survey of Ophthalmology. 2001, 45(6), pp.516-524.
8. Hoppe, J.B. et al. Free and nanoencapsulated curcumin suppress beta-amyloid-induced cognitive impairments in rats: Involvement of BDNF and Akt/GSK-3 beta signaling pathway. Neurobiology of Learning and Memory. 2013, 106, pp.134-144.
9. Knowles, J.K. et al. A small molecule p75(NTR) ligand prevents cognitive deficits and neurite degeneration in an Alzheimer's mouse model. Neurobiology of Aging. 2013, 34(8), pp.2052-2063.
10. Karran, E. et al. The amyloid cascade hypothesis for Alzheimer’s disease: an appraisal for the development of therapeutics. Nature. 2011, 10, pp, 698-712.
11. Lim, Y.Y. et al. Effect of amyloid on memory and non-memory decline from preclinical to clinical Alzheimer's disease. Brain. 2014, 137, pp.221-231.
12. Mattsson, N. et al. Association of brain amyloid-beta with cerebral perfusion and structure in Alzheimer's disease and mild cognitive impairment. Brain. 2014, 137, pp.1550-1561.
13. Murakami, K. Conformation-specific antibodies to target amyloid beta oligomers and their application to immunotherapy for Alzheimer's disease. Bioscience Biotechnology and Biochemistry. 2014, 78(8), pp.1293-1305.
14. Myers, N. et al. Within-patient correspondence of amyloid-beta and intrinsic network connectivity in Alzheimer's disease. Brain. 2014, 137, pp.2052-2064.
15. Ni, R.Q. et al. Amyloid tracers detect multiple binding sites in Alzheimer's disease brain tissue. Brain. 2013, 136, pp.2217-2227.

16. Philibert, K.D. et al. Identification and characterization of Abeta peptide interactors in Alzheimer's disease by structural approaches. Frontiers in aging neuroscience. 2014, 6, p.265.
17. Poojari, C. Aggregation of Amyloids at Biomembranes and its Implications in Alzheimer’s Disease and Type II Diabetes. Biophysical Journal. 2013, 104(2), pp.592A-592A.
18. Ramanan, V.K. et al. APOE and BCHE as modulators of cerebral amyloid deposition: a florbetapir PET genome-wide association study. Molecular Psychiatry. 2014, 19(3), pp.351-357.
19. Roberts, B.R. et al. The role of metallobiology and amyloid-ss peptides in Alzheimer's disease. Journal of Neurochemistry. 2012, 120, pp.149-166.
20. Rosales-Corral, S.A. et al. Alzheimer's disease: pathological mechanisms and the beneficial role of melatonin. Journal of Pineal Research. 2012, 52(2), pp.167-202.
21. Saito, S. and Ihara, M. New therapeutic approaches for Alzheimer's disease and cerebral amyloid angiopathy. Frontiers in aging neuroscience. 2014, 6, p.290.
22. Shojaei, F. et al. Biochemical and immunological aspects of protein aggregation in neurodegenerative diseases. Journal of the Iranian Chemical Society. 2014, 11(6), pp.1503-1512.
23. Tharp, W.G. and Sarkar, I.N. Origins of amyloid-beta. Bmc Genomics. 2013, 14, p.15.
24. Wang, Q.M. et al. De Novo Design of Self-Assembled Hexapeptides as beta-Amyloid (A beta) Peptide Inhibitors. Acs Chemical Neuroscience. 2014, 5(10), pp.972-981.
25. Wu, J. et al. Activation of the CB2 receptor system reverses amyloid-induced memory deficiency. Neurobiology of Aging. 2013, 34(3), pp.791-804.
26. Alzforum. Therapeutics 2014. [Online]. 2014. [Accessed 12 February 2015]. Available from: http://www.alzforum.org/therapeutics
27. Alzheimer’s Research UK. Facts and Stats 2014. [Online]. 2014. [Accessed 10 January 2015]. Available from: http://www.alzheimersresearchuk.org/about-dementia/facts-stats/