Embed Size (px)
Citation preview

AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 13
• BACKGROUND Little information is available nationally about critical care units and nurses. What isknown about nurses in hospitals is generally not broken down among all the specialties.• OBJECTIVES To describe issues of workforce, compensation, and care specific to critical care units andnurses who work in them.• METHODS The American Association of Critical-Care Nurses conducted a survey of randomly selectedfacilities with critical care units in the United States. Facilities were solicited via e-mail to respond to asurvey on the World Wide Web and provide information on operations, evaluations, nursing staff reim-bursement and incentives, staffing, and quality indicators. Responding facilities also provided contactinformation for units in the facilities. Those units were surveyed about operations, acuity systems,staffing, policies on visitation and end-of-life care, administrative structure, documentation, certification,professional advancement, vacancy/floating, staff satisfaction, orientation, association membership,wages, advanced practice nursing, and quality indicators.• RESULTS The initial response rate (120 of 658 eligible facilities) was 18.2%, and 300 of 576 solicitedunits nominated by the facilities responded, yielding a 52.1% response rate for the second phase.• CONCLUSIONS These survey data define the scope and intensity of services offered and provide morespecific figures about staffing issues and unit practices than has been accessible before. Healthcareproviders may use this information for benchmarking purposes, especially for instances in which thetables provide data for each particular type of critical care unit. (American Journal of Critical Care.2006;15:13-28)
AMERICAN ASSOCIATION OF CRITICAL-CARE NURSES’NATIONAL SURVEY OF FACILITIES AND UNITS PROVIDING
CRITICAL CARE
To purchase electronic or print reprints, contact The InnoVision Group, 101Columbia, Aliso Viejo, CA 92656. Phone, (800) 809-2273 or (949) 362-2050(ext 532); fax, (949) 362-2049; e-mail, [email protected].
By Karin T. Kirchhoff, RN, PhD, and Nancy Dahl. From School of Nursing, University of Wisconsin-Madison,Madison, Wis (KTK), and Research Dimensions, Toronto, Ontario (ND).
The American Association of Critical-CareNurses (AACN) developed its national criticalcare survey to collect vital information and to
assess important US benchmarks against which hos-pitals can compare their institutions and critical careunits. The information collected is expected not onlyto inform participating institutions and the AACNabout the unmet needs in critical care units but also toprovide critical care nurses and other involved partieswith information they require to bring about thechanges needed in the workplace, in clinical practice,
and in the regulations that affect these healthcareproviders and the care of patients.
The types of data collected in this survey are notavailable elsewhere. Only recently have data fromregional or national studies specific to critical carebegun to be published. Halpern et al1 provided infor-mation on the numbers of beds in intensive care units
This AACN survey provides benchmarksagainst which hospitals and critical careunits can compare care.
Journal Club Feature
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

(ICUs) in the United States and the costs of intensivecare relative to national health expenses and the grossdomestic product. Information is not available, how-ever, about the severity of the shortage of nurses incritical care units, statistics related to quality of carein critical care units, or other important factors thatmay vary from one type of unit to another. A search ofthe Cumulative Index to Nursing and Allied HealthLiterature with the terms “nurse,” “critical care,” and“statistics” and limited to the years 2000 to 2005yielded only articles from other countries, about a sin-gle state, or articles about nurses and clinical issues.When the search was limited to US journals, only 72references were found.
Although many groups gather and publish com-prehensive statistics on hospitals and nurses in theaggregate, few separate out the data for critical careunits and critical care nurses. Reports of hospitalstatistics that include nursing issues and patient infor-mation tend to include only data combined across allunits. Rarely are the data presented according to thespecific characteristics of critical care units. It is there-fore diff icult to ascertain if the issues and eventsreported are similar in frequency in all types of units.For example, staffing statistics have not been analyzedby type of unit; no one has compared data from ICUsversus data from telemetry units versus data frompostanesthesia care units (PACUs). Until now, thesedata have not been available on a national basis—onlywithin individual hospitals.
Among the many variables included in the AACNnational critical care survey were hospital characteris-tics, unit and staff demographics, certification, formaland continuing education, leadership, decision mak-ing, patients’ outcomes, and staffing.
In addition to traditional ICUs, the study includedother areas within the hospital where acutely and criti-cally ill patients are cared for, such as progressivecare, telemetry, and step-down units. Data on thesetypes of units, their nurses, and their patients are evenscarcer because these units are still relatively newdevelopments. PACUs were also included in the sur-vey because they are an important part of the criticalcare continuum.
Planning for this survey began in the summer of2003. Data were collected from facilities in the fall of2003 and from units in the spring of 2004.
In this article, we present part of a more compre-hensive report available at www.aacn.org or by calling800-899-2226. The goal of this initial article is to pre-sent the profile of the facilities and units surveyed.Specific areas of the findings will be covered in moredepth in future articles.
MethodSample
In addition to collecting data related to the char-acteristics of critical care units and the nurses andpatients who fill the units, the survey team also soughtto learn about the facilities in which the units arehoused. Because many of the variables of interestwere hospital-wide rather than specific to a unit, thesurvey was divided and administered in 2 phases: thefacility phase and the unit phase. Contact informationfor collecting data in the unit-specific phase of thestudy was obtained during the facility phase.
Facility Phase. The survey team purchased a listof hospitals that met the survey criteria from a nation-ally recognized healthcare organization. Criteria forinvitation to participate in the survey included thepresence of one or more of the following types ofunits: ICUs (of any type), step-down units, progressivecare units, telemetry units, PACUs, and other unitswhere nursing care is provided for acutely and criti-cally ill patients.
Hospitals with fewer than 50 licensed beds wereomitted from the sample. Although these facilitiesmay be listed as having an ICU, many have only 1 or 2beds designated for stabilization of critically ill patients,and those beds are not always available. Eligible hos-pitals were then divided up into strata by number ofbeds (50-100; 101-200; 201-300; 301-500, and ≥501)and were randomly sampled across the strata. Specifi-cally, quotas were placed on the number of hospitalscontacted within various strata; that is, quotas wereplaced on hospitals with 50 to 100 operating beds, 101to 200 operating beds, and so on. This process allowedthe inclusion of more large hospitals and fewersmaller hospitals than would have been included ifproportional sampling had been used; in proportionalsampling, small hospitals would have predominated,preventing analyses of differences in hospitals withdifferent numbers of beds.
A total of 749 facilities were included in the sampleand invited to participate. During the course of the invi-tation and follow-up process, 91 facilities were deemedineligible, resulting in a final eligible sample of 658facilities. Of those eligible facilities, 120 (18.2%) par-ticipated. When the data were tabulated, they were
14 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
A profile of facilities and units surveyedis presented here. A more completereport is available at www.aacn.org.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

weighted to ensure that the range of facility sizesreflected the range of sizes of US hospitals in general.Both the unweighted and weighted profiles of thefacilities are listed in Table 1.
Unit Phase. Responding facilities were asked tosubmit lists of their critical care units, including pro-gressive care units, telemetry units, step-down units,and PACUs, and to provide contact information for theunit managers. The 120 responding hospitals listed576 critical care units, and the managers of those unitswere subsequently sent the unit phase of the survey.Of the 576 units invited to participate, 300 (52.1%)responded to the questionnaire. Unit data were leftunweighted because the numbers of different types ofunits in US hospitals are unknown.
InstrumentTwo instruments were used: one questionnaire for
the facility data and another for the unit data. Respon-dents to both the facility and unit questionnaires wereinstructed to report data for a full 12-month period,preferably from their most recently completed fiscal year.
Several steps were taken to improve the reliabilityand validity of the instruments. Experts in questionnairedesign and in critical care nursing and critical caremanagement designed and tested the instruments.After development of the questionnaires, experts innursing management reviewed them for correct use ofterms and generalizability across settings. Because thequestionnaires were converted to pages on the WorldWide Web, AACN staff and volunteers tested flow,handling of potential responses, and ease of use.
Facility Survey. The facility questionnaire wasadministered online, and representatives for theinvited facilities were e-mailed an invitation with alink to the survey instrument. The questions were pre-sented in a Web format, preprogrammed to allowrespondent-selected options, when appropriate, or freetext, when necessary. Facility representatives who didnot have e-mail or who preferred a paper form wereprovided with a questionnaire on paper. The surveyincluded questions on the following topics: demo-graphics about operations (14 questions), evaluations(4 questions), nursing staff reimbursement and incen-tives (7 questions), staffing (9 questions), quality indi-cators (4 questions), and information on critical careunits and contact information for critical care unitmanagers to solicit responses to the unit survey.
Unit Survey. Also administered online (with apaper option available upon request), the unit surveycontained questions on a wide array of topics: opera-tions (10 questions), acuity systems (3 questions),staffing (8 questions), policies on visitation and end-
of-life care (3 questions), administrative structure (13questions), documentation (3 questions), certification(6 questions), professional advancement (5 questions),vacancy/floating (11 questions), staff satisfaction (2questions), orientation (8 questions), associationmembership (3 questions), wages or registered nurses(RNs; 1 question), advanced practice nursing (8 ques-tions), and quality indicators (5 questions).
ProcedureAfter the facilities were randomly selected, a con-
tact person equivalent to the critical care director wasdetermined for each facility, and contact informationwas collected. E-mail invitations were sent to theseindividuals to encourage them to go to the Web sitewhere the facility questionnaire was available. Asfacility questionnaires were completed and criticalcare units and managers were specified, invitationswere sent to the unit contacts to ask them to completethe second phase, the unit questionnaire.
Follow-up was implemented by using a number ofoptions. A full-time AACN employee was dedicatedto follow up with nonrespondents in both phases ofthe survey. Special care was taken to follow up by e-mail and telephone to encourage participation or to
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 15
Table 1 Profile of facilities surveyed
Weighted
74
94
121
91
27
32322313
253218158
Percentage of 120 facilities
Feature
Organizational controlNongovernment, not for profit
Investor-owned, for profitGovernment, nonfederal hospital
Government, federal hospitalNo answer
Facility typeGeneral medical and surgical hospital
Academic medical center
SettingUrbanRuralSuburbanNo answer
Facility size* (No. of operating beds)50-100101-200201-300301-500>501
Unweighted
75
87
91
93
37
45222013
825202521
*Mean number of operating beds was 328 unweighted and 217weighted. Percentages total less than 100 because of rounding.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

determine the reason for nonresponse. Nonresponsewas a bigger factor in the facility phase of the surveythan in the unit phase. Ultimately, the sample of facil-ity responders was compared with the group of nonre-sponders to ensure that the sample of responders wasrepresentative of the randomized pool of hospitals.The research team validated that the responder facili-ties did not differ significantly from the nonresponderfacilities in terms of available data such as number ofbeds or geographic distribution.
Output from the completed questionnaires wasreviewed for consistency with expected responses, andclarification was sought for outliers. Extreme outliersin individual item responses that could not be verifiedwere removed so as not to alter reported means.
ResultsParticipating Facilities
In total, 120 respondents participated in the facilitysurvey. All participating facilities had 50 or morelicensed beds; facilities with fewer beds had beenexcluded from the study. The actual (unweighted) andweighted profiles of facilities that participated in thestudy are shown in Table 1. US hospitals in general andthe weighted data include fewer large hospitals than actu-ally participated in the study. Academic and urban hospi-tals tend to be larger than other facilities. Therefore, theirproportions were reduced accordingly when the numberof large hospitals in the weighted sample was reduced.
The weighted profile of facilities is the profile thatshould be considered when the facility findings areexamined, because the findings reflect this breakdown.According to this profile, the majority of facilities rep-resented in the data are general medical and surgicalhospitals (91%), nongovernment, not-for-profit orga-nizations (74%), from a variety of settings, with amean of 217 operating beds and 258 licensed beds.Where sample sizes allowed, differences between thevarious facility types and sizes are indicated.
Operations. Not all respondents provided informa-tion on inpatient admissions, excluding newborns butincluding neonatal and “swing” admissions and read-missions (swing beds are those that can be used to pro-vide either acute or long-term care depending on theneeds of the community or patients). Participating insti-tutions had a mean of almost 13 000 admissions peryear (Table 2). More than two thirds of respondents didnot have data available on cost per patient day or wereunable to answer the question. Of those responding, themean cost per patient day was $1883 (Table 2). Themean cost per adjusted discharge was $7333.
Evaluations. Most hospitals surveyed (80%) wereaccredited by the Joint Commission on Accreditation
of Healthcare Organizations (JCAHO). Four percentwere not accredited (16% did not provide that infor-mation). Facilities that were accredited had scored amean of 93 on their most recent JCAHO survey.
At the time of the survey, only 5% of respondinghospitals had been designated Magnet nursing ser-vices through the American Nurses CredentialingCenter’s Magnet program. Seventy-nine percent offacilities did not have Magnet-designated services, butalmost half of these (44%) said that they planned toapply for such status in the next 3 years. Mainly largerhospitals planned to apply (Table 3).
Incentives. Most hospitals offered tuition reim-bursement both to RNs for academic programs (83%)and to students in educational programs to becomeRNs (85%). Almost half of the facilities surveyed(44%) had implemented professional developmentand advancement programs for bedside nurses, pri-marily clinical ladder systems. A further 12% had pro-grams in development.
Staffing. About half of the responding institutions(52%) provided information on numbers of budgetedRN full-time equivalent (FTE) positions. Among those,
16 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Table 2 Descriptive statistics of facilities (N = 120) withcritical care units
Facility information
Inpatient admissions, excluding newborns, including neonatal and swing admissions (n = 87)
Inpatient readmissions, within 30 days (n = 45)
Inpatient days, excluding newborns, including neonatal and swing admissions (n = 87)
Discharges (n = 77)Costs, US$*
Per patient day (n = 38)Per adjusted discharge (n = 33)
Mean
12761
902
58620
11495
18837333
Median
8776
350
43151
8767
17426952
*More than two thirds of respondents did not answer this question.
Five percent of responding hospitals hadMagnet-designated nursing services,although almost half planned to apply.
Almost half had nursing developmentprograms such as a clinical ladder.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

the numbers of total budgeted RN FTEs ranged up to1000 or more; most facilities (64%) had fewer than300 positions. The median number of budgeted RNFTE positions was 214, and the mean was 332. Thetotal number of unfilled budgeted RN FTE positionswas up to 100 or more; most hospitals (64%) had fewerthan 30 unfilled positions. The median and mean num-bers of unfilled positions were 21 and 36, respectively.The means for total and unfilled budgeted positionswere slightly higher than the medians because somehospitals had many positions. The mean vacancy rate,calculated by dividing the mean number of unfilledpositions (36) by the mean number of budgeted RNpositions (332), was 10.8%.
Among the 51 facilities that provided informa-tion, the total number of RN staff who had terminatedemployment during a 12-month period (including vol-untary and involuntary termination) was up to 150 ormore. The median number of terminations was 31,and the mean number was 53 (the mean is higherbecause a few hospitals had high termination levels).Respondent hospitals reported a mean turnover rate of11.8%. The mean turnover rate was calculated by
dividing the mean number of terminations (53) by themean number of RNs on the payroll (449).
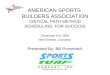
Almost two thirds of respondents did not havedata available on the number of days needed to fill a
vacant RN position or were unable to answer the ques-tion. Answers varied among those who responded, butit took a mean of 59 days (median 54 days) to fill avacancy (Figure 1).
Most facilities surveyed (64%) did not have a col-lective bargaining unit representing their nursing staff.
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 17
Table 3 Facilities’ plans for Magnet-designated nursing services
Facility has Magnet-designated service
Facility plans to apply for Magnet designation
Facility size, No. of beds
<300(n = 65)
3
39
>301(n = 55)
10
63
Academic(n = 44)
10
44
General medical/surgicalhospital (n = 111)
4
43
Urban(n = 54)
9
58
Suburban/ rural (n = 50)
4
45
Facility type Setting
Status of facility
Percentage of responding facilities
Hospitals reported a nursing vacancy rateof 10.8% and a turnover rate of 11.8%.
Figure 1 Number of days required to fill a vacant position for a registered nurse.
*Questionnaire included a “data not available” response option that was combined with “no answer” responses in the data.
Percentage of 120 facilities
0 20 40 60 80 100
Data not available/no answer*
Among those answering (n = 45)
<30 days
30-44 days
45-59 days
60-89 days
90-119 days
>120 days
Most hospitals (64%) did not have acollective bargaining unit representingtheir nursing staff.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

Twenty-two percent of hospitals did have collectivebargaining units, half with mandatory (closed-shop)membership.
Participating UnitsCritical care units were defined as any unit in
which acute and critically ill patients received care. Inthis survey, the 3 prevalent types of critical care units,ICUs, PACUs, and progressive care units, were stud-ied (Table 4). From the 120 responding facilities, 300critical care units participated in the survey. A littlemore than half of the units in this study were tradi-tional ICUs. The unit results were not weighted toreflect hospitals nationwide, because the proportionsof critical care units across US hospitals in general arenot well known. Therefore, we caution that the totalresults for each question are skewed to the activities ofthe more dominant units in the sample. (For example,the total results are somewhat more representative ofthe activities of recovery room/PACUs, medical-surgi-cal ICUs, and combined intensive/coronary care unitsand less representative of the activities of trauma unitsand burn ICUs). Differences between ICUs (total) andprogressive care units (total) and PACUs specificallyare discussed throughout this section, because theirsample sizes were large enough for categorical analy-sis. The sample sizes for the other individual unitswere too small for such analysis.
The unit findings also often varied, depending onthe size of the unit or the size or location of the hospi-tal the unit was in (eg, urban, suburban, or rural hospi-
tals). Significant differences are noted. Table 5 showsrelationships between the types of units in a hospitaland the unit’s size. Of note, in this table, smaller units(12-29 operating beds) are predominantly ICUs.
The larger units with 30 beds or more were mainlyprogressive care units. For this reason, smaller units andICUs often had common patterns throughout the find-ings. The same was true of larger units and progressivecare units.
Operations. Almost half (46%) of the critical careunits in the study had fewer than 15 operating beds;the largest concentration of units (30% of units) had10 to 14 beds. Overall, the mean unit size was 19operating beds (median 16 beds; Figure 2).
Almost two thirds of the units provided informa-tion on their admissions. Overall, the number of criti-cal care admissions varied widely from less than 250to 5000 or more. Critical care units had a mean ofabout 2000 admissions during a 12-month period, but,half of the units had fewer than 1000 admissionsannually.
More than three quarters of units did not provideinformation on readmissions, an important indicatorof quality of care. Perhaps the respondent did not haveaccess to the information or that information was notcollected in the unit. Of the units for which informa-tion was provided, 38% had had no readmissionswithin 48 hours during the preceding 12-month period.Among the few remaining respondents, the number ofreadmissions within 48 hours varied widely from 1 to50 or more during a 12-month period. The mediannumber of readmissions was 4, and the mean was 16
18 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Table 4 Critical care units represented in this report
Type of critical care unit
Intensive care unitsMedical-surgicalCombined intensive/coronary careCardiovascular/surgicalCoronary careNeonatalPediatricMedicalSurgicalNeuro-neurosurgicalTraumaBurn
Postanesthesia care units/recovery roomsProgressive care units
TelemetryStep-downIntermediate careProgressive care
Other types of critical care unitsNo answer
Percentage oftotal sample
(N = 300 units)
5388755444322
10301276543
Table 5 Percentages of each unit type among small, medium,and large units*
Type of unit
Intensive care unitsMedical-surgicalCombined intensive/ coronary care
NeonatalProgressive care units
TelemetryStep-down
Small<12
(n = 84)
827
11
11352
Medium12-29
(n = 150)
70119
52576
Large>30
(n = 57)
2642
12703518
Unit size, No. of beds
*Numbers in table are percentages of each type of unit in each unitsize range. For example, 82% of small (<12 bed) units are intensivecare units. Percentages do not total 100. All other units representedin this study and listed in Table 4 are equally prevalent amongsmaller and larger units. A bold number within a category (eg,within Unit size) is significantly higher than nonbold numberswithin the same category. An italic number is significantly higherthan nonitalic numbers, but significantly lower than bold numbers.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

(the mean was skewed high because a few critical careunits had high numbers of readmissions).
Among the 59% of respondents who providedinformation, numbers of inpatient days for their unitswere as high as 10 000 or more in a 12-month period.The median number of inpatient days was 3708, andthe mean was 4808 (the mean was skewed slightlyhigher than the median because some units had verylarge numbers of inpatient days).
Seventy percent of respondents provided informa-tion on the mean length of stay in their units. In mostcritical care units (74%), the length of stay was between2 and 5 days. The longest stays were in larger criticalcare units (20% of patients in the largest units stayedfor ≥11 days versus 2% in the smaller units) and inurban hospitals (which are more likely to have thelarger critical care units; Table 6). Table 6 also showshow numbers of operating beds, admissions, and inpa-tient days varied depending on unit size and hospitalsetting. Naturally, larger units had more operating beds,admissions, and inpatient days; mean values amongsmaller and larger units are shown in the table.
Hospital size had little relation to the number ofbeds in a unit, except in the smallest hospitals. Smallhospitals (101-200 operating beds) had a mean of 15beds per critical care unit. Larger hospitals had amean of 20 or 21 beds per critical care unit, regardlessof whether the facility had 201 to 300 beds, 301 to500 beds, or more than 500 beds.
Acuity Systems. Forty-two percent of critical careunits in the study used a formal acuity system. Formalacuity systems were more prevalent in the largest hos-pitals (>500 beds) and urban hospitals (which tendedto be the larger ones). A wide variety of systems were
in place. In about 7 in 10 critical care units surveyed,respondents had seen an increase in patients’ acuity inthe preceding year or had perceived that acuity at thetime of patients’ transfer or discharge was higher thanit had been 1 year earlier.
Respondents from the larger units (12 or more oper-ating beds) and urban/suburban hospitals were mostlikely to have noticed these changes in acuity (althoughurban facilities were less likely than suburban facili-ties to have experienced higher-acuity transfers/dis-charges). Increases in patients’ acuity were reportedequally in ICUs, progressive care units, and PACUs.But, progressive care units (and ICUs, directionally)were more likely than PACUs to see patients beingtransferred or discharged with higher acuity (Table 7).
The same trend was evident in terms of “chroniccritical care” patients. Almost half of units (45%) hadseen an increase in the percentage of longer-termchronic critical care patients who could not be placedelsewhere (eg, patients receiving long-term mechanicalventilation, patients with complex wound management,and patients in stable condition who were receivingintravenous vasoactive medications). Again, thisincrease had occurred more in urban and suburbanhospitals than in rural facilities. Respondents fromunits in smaller hospitals (up to 300 operating beds)and the largest hospitals (>500 beds) were more likelyto have noticed an increase than were respondentsfrom mid-sized facilities (301-500 beds; Figure 3).
Staffing. In most of the critical care units surveyed(73%), the nurse manager or assistant nurse managercoordinated staffing. A few facilities coordinated staffingeither through a staff-run scheduling committee or astaff nurse coordinator; these methods of coordinating
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 19
Percentage of 300 units
0
Percentage of units*Adult Recovery/
intensive Progressive postanesthesiacare care care
No. of beds (n = 118) (n = 90) (n = 31)
<12 38 12 39
12-29 58 42 52
>30 4 44 10
Mean 15 26 16
20 40 60 80 100
<10 beds
10-14 beds
15-19 beds
20-29 beds
30-39 beds
>40 beds
No answer
Figure 2 Total number of operating beds in the unit.
* A bold number within a category (eg, within intensive care) is significantly higher than nonbold numbers in other units (eg, progressive care).Numbers of units do not total 300 because of “no answer” responses, units unspecified, and exclusion of atypical units (eg, neonatal and pedi-atric intensive care units).
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

were more prevalent among smaller or rural hospitalsor government nonfederal hospitals (as opposed tonongovernment, not-for-profit centers).
Respondents were asked which factors they consid-ered in determining the number of nurses needed fortheir basic staffing plans. Of the 4 factors listed in thesurvey, the most commonly considered factor (by 88%
of respondents) was the expected patient census. Theneed for specialized skills (eg, balloon pumps, dialysis)and the skill mix of the staff ranked next in importance.A formal acuity system had the lowest priority.
The few PACUs were less inclined than ICUs andprogressive care units to select any of the 4 factors.Smaller units (up to 29 operating beds) were more
20 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Table 6 Unit statistics by type of facility and unit*Unit size, No. of beds
<12
(n = 84)
8
(n = 45)
1140
(n = 56)
2039
(n = 57)
584024
Unit statistic
No. of operating beds<107-1112-29>30Mean
No. of admissions, mean
No. of inpatient days, mean
Length of stay, days
<44-10>11Mean
18
(n = 97)
2229
(n = 94)
4429
(n = 108)
5337106.5
>30
(n = 57)
39
(n = 28)
2996
(n = 35)
9276
(n = 39)
4931207
Urban
(n = 198)
620482520
(n = 114)
2120
(n = 114)
4856
(n = 137)
4642126
Suburban
(n = 46)
226657
17
(n = 30)
1696
(n = 26)
4877
(n = 34)
682665
Rural
(n = 47)
1528451116
(n = 36)
1969
(n = 33)
4073
(n = 34)
652695
Setting
* This table includes results from 4 questions. The total numbers of respondents for each question are shown in parentheses. Most numbers inthe body of the table are percentages of respondents reporting that statistic. The 4 rows of mean values are actual numbers of that statisticrather than percentages of respondents. A bold number within a category (eg, within Unit size, Setting) is significantly higher than nonboldnumbers within the same category. An italic number is significantly higher than nonitalic numbers, but significantly lower than bold numbers.
12-29
(n = 150)
Table 7 Perceived changes in patients’ acuity in the preceding year by type of facility
Percentage of all units or facilities responding*
Unit type
Recovery/postanesthesia
care(n = 31)
682606
58366
Progressivecare
(n = 90)
771823
78176
Adultintensive
care(n = 118)
692542
70282
Patients’ acuity hadIncreasedStayed the sameDecreasedNo answer
Were patients being transferred or dischargedwith higher acuity?
YesNoNo answer
Unit size, No. of beds
<12(n = 84)
573346
58366
Setting
12-29(n = 150)
752131
73261
>30(n = 57)
771922
74252
Urban(n = 198)
712333
65332
Suburban(n = 46)
782200
85132
Rural(n = 47)
553266
66286
* A bold number within a category (eg, within Unit type, Unit size, Setting) is significantly higher than nonbold numbers within the samecategory.
Change
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

likely than large units to take into account the need forspecialized skills. Formal acuity systems were more ofa priority to urban hospitals, where these systems weremore established, than to suburban/rural facilities.Still, acuity systems had the lowest priority evenamong urban hospitals (Table 8).
The majority of respondents thought that thestaffing had not been optimal up to 25% of the time interms of the match between patients’ acuity and thenurses’ skill level or mix.
Nine percent of critical care units participating inthe study had recently been required to close beds formore than 30 days because of insufficient numbers ofRNs. This finding was consistent among all types andsizes of units.
Overall, most critical care units (71%) had a pol-icy that patients being transported out of the unit mustbe accompanied by a unit nurse. The number of trans-ports of patients out of the unit for tests or proceduresvaried considerably and depended on the unit.
Respondents were asked what they used whenthey needed to adjust staffing to manage sudden oremergency admissions or sudden increases in patients’acuity. Of the 7 options given in the survey, the mostcommonly used strategies (used by 70% of units ormore) were calling in regular staff RNs on their days
off, calling in regular staff RNs early, and jugglingcurrent RN staff to make do. Borrowing (“floating”)RNs from other critical care areas was the next-most-used alternative (by just more than half of the units).Floating RNs from other noncritical areas was theleast favored option.
The predominant way that units in the study man-aged floating among their staff was via cluster unitfloating; staff were required to float, but in a desig-nated unit only (55% of units). Among the remainingunits, 2 practices were equally prevalent: in open units(23%), staff were required to float to any unit withinthe facility; in closed units (19%), staff were notrequired to float outside of their unit. The strategiesused to manage sudden or emergency situations or tomanage floating varied considerably by type of unitand hospital. Progressive care units were less likelythan ICUs and PACUs to use on-call systems and weremore likely to float RNs from non–critical care areas.
ICUs and progressive care units were more likelythan PACUs to use several different approaches formanaging sudden admissions or increases in patients’acuity. They were more likely than PACUs to call inregular staff RNs on their days off, to float RNs fromother critical care areas, or to use agency nurses. Thereasons were not addressed in the survey. This findingmay be linked to the fact that the few PACU nurses inthe study used other strategies that were not listedamong the options for that item. Or, perhaps PACUsdid not adjust staffing for sudden situations to thesame degree that ICUs and progressive care units did.
Similarly, rural hospitals were less likely thanurban or suburban hospitals to use many of the strate-gies listed. Again, the reasons for this finding were notaddressed in the survey. Perhaps fewer rural hospitals
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 21
Most respondents thought that thestaffing had not been optimal up to25% of the time in terms of the matchbetween patients’ acuity and thenurses’ skill level or mix.
Figure 3 Percentage of 300 respondents who had perceived changes in the number of long-term “chronic critical care” patients inthe preceding year.
* Bold numbers within a category (eg, facility size, setting) are significantly higher than nonbold numbers in the same category.
Decreased
Stayed the same
Increased
No answer
Feature of Percentage of facility respondents*
Size, No. of beds101-200 52201-300 50301-500 31>500 54
SettingUrban 48Suburban 50Rural 26
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

than urban/suburban hospitals had increases in theacuity of patients or in the number of patients requir-ing long-term chronic critical care. Or, perhaps ruralhospitals used other approaches that were not listed inthe questionnaire. Or, perhaps they did not need tomake staffing adjustments to the same degree as urbanand suburban hospitals did.
Visitation Policies. In the survey, respondentswere asked what their unit’s family visitation policywas and were given 3 alternatives to select from, withan option to write in another response (these otherresponses were quite diverse). The 3 family visitationpolicies given were as follows: open on a scheduledbasis only, open except for rounds and/or changes inshift reports, and open at all times.
Family visitation policies varied considerably byunit type and size. Units that were open on a sched-uled basis only (eg, hourly, every 2 hours for a speci-fied time, or some other schedule) were almost alwaysICUs or progressive care units; very few respondentsfrom PACUs reported having this policy (Figure 4).
Policies varied even within unit type. Most ICUswere open on a scheduled basis only (44%). But, ICUsalso commonly had a policy of being open except forrounds and/or changes in shift reports (31%). The per-centage of progressive care units that were open at alltimes (36%) did not differ significantly from the per-centage that were open on a scheduled basis only (34%).Not surprisingly, most (84%) of the few PACUs in this
study used some other family visitation policy thanthe 3 just listed (Figure 4). Smaller units (<30 operat-ing beds) were more likely than large units to have apolicy of being open except for rounds and/or changesin shift reports. Larger units (≥30 beds) were morelikely than other units to be open at all times.
End-of-Life Care. Respondents were also askedwhat policies they initiated for managing patientswhen the goals of care changed from aggressive careto comfort care. Again, they were given 3 alternativesto select from, with an option to write in anotherresponse (these other responses varied widely). The 3comfort care policies that they were given were pallia-tive care standards, end-of-life care standards, andhospice services in the unit.
Comfort care policies varied considerably by typeof unit. Progressive care units (86%) and ICUs (75%)were most likely to have comfort care policies.Among both progressive care units and ICUs that didhave policies, palliative care standards and end-of-lifecare standards were equally prevalent. Progressivecare units were more likely than ICUs to also imple-ment hospice services in the units (Figure 5). MostPACUs (71%) did not have comfort care standards orthose policies were not applicable to their units. Thosethat did have policies tended to use policies that dif-fered from the policies listed in the questionnaire.
In terms of facility types, smaller hospitals (101-300 operating beds) were more likely to use hospiceservices in the unit than were larger hospitals. Urbanand rural facilities were most likely to initiate palliativecare standards, whereas suburban hospitals imple-mented a variety of approaches. Nongovernment, not-for-profit institutions were less likely than government,nonfederal facilities to have any comfort care policies.
Overall, about 1 in 4 critical care units reportedusing some type of end-of-life protocol, and this find-
22 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Most intensive care units were openfor family visitation on a scheduledbasis only; larger units were more likelyto be open all the time.
Table 8 Factors considered in determining the number of nurses needed for basic staffing plan by type of facility and unit
Percentage of units or facilities responding*
Unit type
Recovery/postanesthesia
care(n = 31)
8432261023
Progressivecare
(n = 90)
9049602820
Adultintensive
care(n = 118)
9085642514
Factor considered
Expected patient censusSpecialized skills neededSkill mix of nursesFormal acuity systemOther
Unit size, No. of beds
<12(n = 84)
8671602913
Setting
12-29(n = 150)
8973592517
>30(n = 57)
9140653228
Urban(n = 198)
8769623316
Suburban(n = 46)
9465501720
Rural(n = 47)
8557641728
* A bold number within a category (eg, within Unit type, Unit size, Setting) is significantly higher than nonbold numbers within the samecategory.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

ing was consistent across most types of units andfacilities studied. The one exception was among urbanhospitals, where an end-of-life protocol was somewhatmore prevalent than it was in suburban facilities.
Administrative Structure. Slightly more than halfof the units (55%) surveyed had formalized shared
governance through written bylaws and staff-directedcommittees, mostly at a facility-wide level. Units witha formalized structure were more likely to be PACUs(particularly when compared with progressive careunits), rural hospitals, and smaller units with fewerthan 30 operating beds.
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 23
Figure 4 Family visitation policy.
* A bold number within a category (eg, within Unit type, Unit size) is significantly higher than nonbold numbers within the same category. Num-bers of units do not total 300 because of “no answer” responses, units unspecified, and exclusion of atypical units (eg, neonatal and pediatricintensive care units).
Percentage of 300 units
0 20 40 60 80 100
Open on scheduledbasis only
Open except forrounds/shift changes
Open at all times
Other
No answer
Adultintensive
care(n = 118)
44
31
14
9
2
Unit type
Unit size, No. of bedsProgressivecare
(n = 90)
34
8
36
19
3
Recovery/postanesthesia
care(n = 31)
3
0
7
84
6
12-29(n = 150)
35
26
20
19
0
>30(n = 57)
32
9
35
23
2
<12(n = 84)
31
25
18
20
6
Percentage of responding units*
Figure 5 Services initiated when goals changed to comfort care.
Totals exceed 100% because of multiple mentions.
* A bold number within a unit (eg, within intensive care) is significantly higher than nonbold numbers in other units. An italic number is signifi-cantly higher than nonitalic numbers, but significantly lower than bold numbers. Numbers of units do not total 300 because of “no answer”responses, units unspecified, and exclusion of atypical units (eg, neonatal and pediatric intensive care units).
Percentage of 300 units
0 20 40 60 80 100
Palliative care standards
End-of-life care standards
Hospice services in the unit
Physician writes orders
Transfer to appropriate unit
Other
None
Not applicable
No answer
Adultintensive
care(n = 118)
53
46
14
4
5
11
23
0
2
Percentage of units that initiated each service*
Progressivecare
(n = 90)
56
42
27
2
1
14
11
0
3
Recovery/postanesthesia
care(n = 31)
3
3
0
0
7
39
45
26
10
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

Documentation. Overall, 42% of the critical careunits surveyed used an electronic documentation sys-tem. These units were more likely to be ICUs and pro-gressive care units, smaller hospitals (up to 300operating beds), suburban hospitals, and nongovern-ment, not-for-profit hospitals. The majority of criticalcare nurses (83%) could access the Internet in theirunits as a resource for their nursing practice. Nurses inlarge hospitals (>500 operating beds), mid-sized hospi-tals (201-300 beds), and mid-sized units (12-29 beds)had even greater Internet access than did other nurses.
Recognition. Nursing recognition awards werepresented in 84% of the units in the study. The awardswere often presented on multiple levels, usuallyincluding the facility level (62% of respondents), butnurses were also commonly awarded at the nursingdepartment (41%) and unit levels (39%).
Nursing recognition awards had a variety offorms, depending on what nurses were being recog-nized for. Public acknowledgment was an often-usedreward across different activities. Many facilitiesrewarded a particular achievement in several ways. Asindicated in Table 9,
• Almost all facilities rewarded nurses for years ofservice at the facility, usually via public acknowledg-ment or a gift (about two thirds of facilities) or oftenwith a letter (30%).
• About three quarters of facilities recognizednurses for certification, mostly through public acknowl-edgment (42% of facilities) or bonuses (25%).
• About half to two thirds of facilities rewardednurses for volunteer and research/scholarly activities,respectively, again usually through public acknowl-edgment.
• About 7 in 10 facilities did not recognize associ-ation membership at all. (Smaller units and suburban/rural hospitals were less likely to reward membershipthan were larger units with ≥30 beds and urban hospi-
tals.) Similarly, about 8 in 10 facilities surveyed offeredno financial support for association membership, andthis finding was consistent across all types and sizesof facilities.
Professional Advancement. Most of the hospitalsin the study (84%) offered financial support to nursesfor continuing education. This support most often wasin the form of paid registration or paid time off forlocal or regional/national meetings (in about twothirds of units).
Progressive care nurses were less likely than ICUor PACU nurses to receive support for continuing edu-cation. The same was true for nurses in governmentnonfederal hospitals, compared with nurses in non-government not-for-profit facilities. Small to mid-sized units (≤29 operating beds) were more likely thanlarge units to offer paid time off for meetings.
Filling Vacancies. The total number of budgetedRN FTE positions in the critical care units in therecent months before the survey was up to 50 or more(mean 34 positions). The total number of open/unfilledbudgeted RN FTE positions (excluding contract) wasup to 10 or more. But 40% of units had minimal num-bers of unfilled positions. Specifically, 19% had nounfilled positions and 21% had 1 or 2 open positions.On average, units had 4 open/unfilled positions.
The mean vacancy rate was 11.8%. This rate wasslightly higher than the 10.8% vacancy rate reportedfacility-wide. The vacancy rate was calculated bydividing the mean number of unfilled positions (4) bythe mean total number of budgeted RN positions (34).
The actual total number of RNs (individuals) inthe units was up to 70 or more; about half of the unitshad between 20 and 49 RNs. The mean number ofindividuals working in the units was 38. Total num-bers of RN FTEs working in the units seemed lowerthan the total number of RNs working there; this find-ing was not surprising because of the number of part-
24 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Table 9 Percentages of 300 units responding in which nurses were recognized for activities*
Recognition
Public acknowledgmentBonusPlaqueLetterGiftNoneOtherNo answer
Certification
422513122
23114
Associationmembership
13213
<1†
65118
Research/scholarly activities
473291
31165
Volunteer activities
3131
101
42175
Years of serviceat facility
61101130634
143
*Totals exceed 100% because of multiple mentions.†Less than 1⁄2 of 1%.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

time staff (fewer units had ≥50 RN FTEs). But thesenumbers should be viewed with some discretionbecause 20% of the units did not provide informationon RN FTEs. Thirty-four percent of units used RNFTEs that were contract staff (including travelers andlocal external agencies).
Slightly more than half of the units surveyed(52%) reported that their numbers of budgeted RNpositions had not changed since the previous 12-month period. Twenty-seven percent of units, however,had experienced an increase in the number of bud-geted positions; these were more likely in suburbanfacilities than in urban/rural ones. The number of bud-geted RN positions had decreased among 17% ofunits, particularly units in larger hospitals (the numberof positions in smaller hospitals was more likely tohave remained unchanged).
The turnover rates for ICUs, progressive care units,and PACUs were 11.2%, 13.3%, and 6.5%, respectively.
Turnover rates were determined by dividing the meannumber of terminations by the mean number of RNson the unit’s payroll.
More than half of the respondents did not havedata available on the number of days required to fill avacant RN position in their units or were unable toanswer the question. Among those who providedinformation, it took a mean of 66 days to fill a vacantpost, although some units required more than 120days. Progressive care units (mean 90 days), followedby ICUs (mean 62 days), took the longest to f illvacancies. PACUs were able to fill vacant RN posi-tions quickly in comparison (mean 33 days).
Orientation Programs. About 8 in 10 units in thestudy reported having clinical rotations of not-yet-licensed students in their units and hiring newlylicensed RNs (Table 10).
Respondents from more than 80% of units reportedhaving standardized orientation programs for all
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 25
Table 10 Orientation to critical care by unit type and facility size*
Unit type
Recovery/postanesthesia
care(n = 31)
61
32
65
71
7266
233
36
90
68
94
7351313266
Progressivecare
(n = 90)
83
90
89
93
6392316107
87
74
94
1243181674
Adultintensive
care(n = 118)
85
82
85
88
41919232312
88
69
96
11311720183
Not-yet-licensed students have a clinical rotation on unit
Unit hires newly licensed registered nurses
Newly licensed registered nursesA standardized program is used for all
orientees
Preceptors are assigned to each orientee
Mean length of orientation, days<3030-5960-8990-119>120No answer
New-hire experienced registered nursesA standard program is used for all
orientees
Components are individualized for each nurse
Preceptors are assigned to each orientee
Mean length of orientation, days<1515-3031-4546-60>60No answer
Facility size,No. of beds
Total(N = 300)
82
80
84
88
62819191613
88
71
96
10351618164
101-200(n = 46)
59
63
72
78
43515131122
83
57
94
1741152
177
>201(n = 244)
87
85
87
91
62719201810
89
74
97
9341621164
* A bold number within a category (eg, within Unit type, Facility size) is significantly higher than nonbold numbers within the same category.
Orientation
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

newly licensed RNs and for all newly hired experi-enced RNs. Almost all units assigned preceptors to allorientees. In most units, components of the orientationwere individualized for each newly hired experiencedRN. But, individualization was not quite as commonlypracticed as were implementing standardized pro-grams and assigning preceptors (Table 10). ICUs andprogressive care units and larger hospitals (>200 beds)were more likely to have orientation programs in placefor newly licensed RNs.
Almost all units, including recovery room/PACUs,had standardized orientation programs for newly hiredexperienced RNs. But larger hospitals were morelikely to have individualized components for eachexperienced nurse.
The orientation programs for newly licensed RNsrange varied considerably in length; some exceeded 120days. The median length was 60 days, and the meanlength was 80 days (the mean was skewed higher by afew facilities that had lengthy programs). The longestorientation programs were more likely to be run byICUs; a higher proportion of progressive care units thanICUs had programs that lasted only 30 to 59 days.(Many of the few PACUs in this study did not provideinformation, making any comparisons difficult.)
Orientation programs for newly hired experiencedRNs were shorter than such programs for newly licensedRNs. Some programs lasted more than 60 days; morethan one third of programs lasted between 15 and 30days. The mean duration of an orientation programwas 45 days. Again, the longest programs were morelikely to be conducted by ICUs and also PACUs; ahigher proportion of progressive care units had pro-grams that lasted 30 days or less. Larger facilities(>200 operating beds) and urban and rural hospitalswere also more likely than other hospitals to runlonger programs for newly hired experienced RNs.
Wages. Survey respondents reported that the meanhourly wage of RNs employed in the unit at entry levelwas $21. The entry-level wage paid most often was $18to $19 per hour (27% of units). With 10 years of experi-ence, the mean hourly wage of RNs increased to $27(with most nurses earning between $22 and $29).
Wage rates were the same among nurses whoworked in ICUs, progressive care units, and recoveryrooms/PACUs. Government nonfederal hospitals paidhigher wages than did nongovernment, not-for-profitinstitutions. Hospitals with 201 to 300 operating bedspaid the lowest wages.
Entry-level wages were the same among smalland large units and among urban, suburban, and ruralhospitals. However, more of a wage discrepancy wasapparent among experienced nurses. With 10 years of
experience, RNs in large units earned more than didthose in the smallest units (<12 beds). ExperiencedRNs in urban and suburban facilities earned higherwages than did those in rural hospitals.
Advanced Practice Nursing. Forty-two percent ofcritical care units surveyed had hospital-employed clini-cal nurse specialists allocated to their units. In almostall cases, one clinical nurse specialist was assigned tothe unit. Far fewer units (16%) had been allocated hos-pital-employed nurse practitioners, especially smallerunits. It was more often the larger units (≥30 operatingbeds) that were assigned nurse practitioners. The num-ber of nurse practitioners assigned to a unit variedamong the small number of units that had them.
A greater proportion of ICUs and progressive careunits than PACUs had clinical nurse specialistsassigned to them. Units in larger hospitals (>300 oper-ating beds), urban hospitals, and academic medicalcenters (which tended to be larger), and governmentnonfederal facilities were more likely than units inother institutions to have a clinical nurse specialist.We found no significant relationship between the sizeof a unit and the presence of a clinical nurse specialist.
Most clinical nurse specialists earned an hourlywage at entry level of between $24 and $34, for amean wage of $29 per hour. With 10 years of experi-ence, the mean hourly wage for clinical nurse special-ists had increased to $34 (with wages mostlyconcentrated between $26 and $34 per hour). Thenumber of respondents providing information aboutnurse practitioners’ wages was too small for analysis.
ConclusionMore details about facilities and units serving criti-
cally ill patients are now available as a result of theAACN national critical care survey. We have moreinformation about the scope and intensity of servicesoffered and more specific figures about staffing issuesand unit practices than has been accessible before.Healthcare providers can use this information forbenchmarking purposes, especially in instances inwhich the tables provide the information for the sametype of critical care unit. The methods for obtaining thisinformation have now been tested, and adjustments canbe made to increase response rates in future surveys.
26 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Almost half of the units had a clinicalnurse specialist allocated to their unit,whereas only 16% had been allocatednurse practitioners.
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

This article offers a broad overview of the find-ings, and additional articles are planned that willfocus more closely on specific areas of the findings,for example, the similarities and differences we vali-dated between ICUs and progressive care units.
The full report of f indings from the AACNnational critical care survey is available throughAACN at www.aacn.org or by calling 800-899-2226.
ACKNOWLEDGMENTSMi-Kyung Song and Rick Voland assisted with initial data analysis, and Elfa Gretars-dottir assisted with preparation of the tables and figures.
Commentary by Mary Jo Grap (see shaded boxes).
REFERENCE1. Halpern NA, Pastores SM, Greenstein RJ. Critical care medicine in the
United States 1985-2000: an analysis of bed numbers, use, and costs. CritCare Med. 2004;32:1254-1259.
AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1 27
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

28 AMERICAN JOURNAL OF CRITICAL CARE, January 2006, Volume 15, No. 1
Study Synopsis: This study reports on the findings ofAACN’s national critical care survey, which was developedto provide information focusing on critical care nursing,including issues related to workforce, compensation, andcare issues specific to critical care units and nurses. Descrip-tive survey information was obtained from 300 critical careunits of 120 hospitals nationwide. Participants completedfacility and unit survey questionnaires that assessed informa-tion on operations, staffing, quality indicators, acuity sys-tems, administrative structure, and other aspects of nursingpractice. Responding facilities include academic and generalmedical and surgical hospitals in urban, suburban, and ruralsettings with from 50 to more than 500 beds. The results ofthe survey provide important information on acute and criti-cal care nursing practice including staffing, documentationsystems, shared governance, wages, and nursing recognitionawards; unit characteristics include orientation programs,family visitation policies, end-of-life protocols, and charac-teristics of patients such as length of stay and acuity levels.The results of the national survey provide data on facilitiesand units serving critically ill patients that were not previ-ously known. Additionally, the survey results offer importantinformation on critical care practices that can be used forbenchmarking purposes.
A. Description of the Study• What were the objectives of the research?• What specific information was collected on facility
and unit practices?
B. Literature Evaluation• What previous research has been conducted
evaluating critical care practices?• What contributions does the current study make to
the research literature?
C. Sample• How were specific units and hospitals identified
for study participation?
D. Methods and Design• What specific instruments were used in the study?• How were the instruments developed and tested? • What was the procedure used to contact sites and
obtain survey responses?
E. Results• How did the respondents compare to national
facilities with respect to size and geographic location?
• Why was a weighted profile developed?• What were important facility-based findings?• What were important unit-based findings?
F. Clinical Significance• What are implications of the survey for critical
care nursing?
Information From the Authors: Karin Kirchhoff, RN,PhD, lead author of this journal club article, provided addi-tional information about the study. She relates “AACN wasthe initiator of this research effort. We developed the topicsto be covered and the questions to be used. This paperreports on the major findings of the study.”
Kirchhoff adds that the study results have importantimplications for critical care nursing. She states “The datacan be useful for benchmarking. For example, the studyprovides information on what units are doing about travelingwith patients for procedures—whether it is a common prac-tice, and if not, what could we do instead?”
Kirchhoff reports that additional information on thestudy is available. She relates “The full study report is avail-able from AACN. There are many data tables that provideadditional study information.” She adds “Another use for thestudy data is to query the results as issues arise in the unit sothat you can see what others might have thought of, forinstance with respect to nursing staffing, or what units havein place for EOL [end-of-life] issues.”
Implications for Practice: This national survey provideshelpful information on facilities and units providing care tocritically ill patients. The study findings provide information toinstitutions as well as to the critical care community on aspectsof critical care nursing, unit, and facility practices. Kirchhoffhighlights the significance of the national AACN survey andadds “This is the first report of some of these variables by typeof unit. Also the inclusion of other units such as PACUs[postanesthesia care units] gives us a better idea of how thepatient transitions and what the issues are there.”
Journal Club feature commentary is provided by Ruth Kleinpell.
In a journal club, research articles are reviewed and critiqued. General and specific questions help to aid journal club par-ticipants in probing the quality of the research study, the appropriateness of the study design and methods, the validity of theconclusions, and the implications for practice.
When critically appraising this issue’s AJCC journal club article, “American Association of Critical-Care Nurses’National Survey of Facilities and Units Providing Critical Care,” consider the questions and discussion points listed below.
JOURNAL CLUB ARTICLE DISCUSSION POINTS
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from

Karin T. Kirchhoff and Nancy DahlProviding Critical CareAmerican Association Of Critical-Care Nurses' National Survey of Facilities and Units
http://ajcc.aacnjournals.org/Published online Copyright © 2006 by the American Association of Critical-Care Nurses
13-28 15 2006;Am J Crit Care
http://ajcc.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ajcc.aacnjournals.org/subscriptions/Subscription Information
http://ajcc.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ajcc Submit a manuscript
http://ajcc.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
. 532. Fax: (949) 362-2049. Copyright ©2016 by AACN. All rights reserved(AACN) published bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. The American Journal of Critical Care is an official peer-reviewed journal of the American Association of Critical-Care Nurses
by AACN on August 21, 2018http://ajcc.aacnjournals.org/Downloaded from