Embed Size (px)
Citation preview

Alvaro Coronado

57d old female with one day with fever at home (101,5).
Mild runny nose, no cough, no vomiting.
Mild diarrhea for 3 days non bloody.
Normal feedings: 2oz every 2-3 hours.
No sick contacts

ER: T102.2, HR 125, RR36, Sat99%Normal PE.
CBC: WBC 16.4 (2%bands, 53% segm 14%lymph), Hgb 8.1, Hct 26.9, Platelet count 485 / BCx
UA: WBC 7, RBC 0, Epi Cells 1, Bacteria few, LE TR, nitrite neg, protein neg, Spec. Gravity
1.011 / Ucx
LP: Glu56, WBC 0, RBC 533/ CSF Cx
Started on Ceftriaxone 100mg/Kg/day divided q12hrs

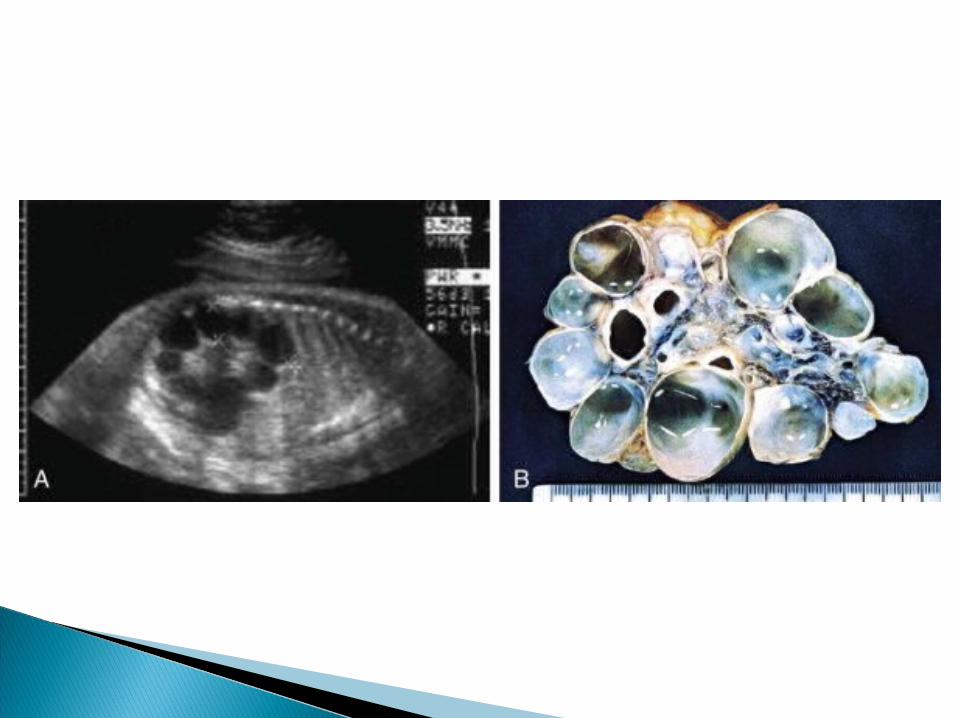
PMH: Fetal US: R Polycystic kidneyNormal NB course. Repeated US, nuclear scan:
- R multicystic dysplastic kidney, non functional .
Started on amoxicillin prophilaxis for 2 weeks.

Gaining weight, normal growingNo surgeriesFMHx negative, no kidney diseasesSH lives with parents and sister (3yo)
NKDA, no medications

No fever during admission, normal PO. No new symptoms.
Vitals: T98.6, HR144, RR38, Sat 100PE unchanged, normal PE.Plan: RSV and FLU (negative)BMP
135
5
109
22
6
0.3
73
9.5

On 1st day of admission urine culture positive (24hrs):
E. Coli 50000 – 100000 cfuOn 2nd day E. Coli resistant to Ampicillin and
intermediate to Ampicillin/clavunalate
US Mild fullness L renal pelvis, Atrophic R kidney with cyst
BCx, CSFCx negative at 48hrs Patient sent home with Keflex FU at Renal in Jacobi

Agenesia: associated with other congenital anomalies (VATER).
Think in newborns with single umbilical artery!!
Agenesia ≠ Aplasia If kidney not seen in US consider a Nuclear
Scan to look for ectopic kidney.

Potter Syndrome: Bilateral renal Agenesia
Potter facies Oligohydramnios Die after delivery because of
hypoplastic lungs Potter phenotype include different
kinds of renal anomalities


AR disorder with incidence of 1:10000 to 40000
Enlarged kidney with cysts between functional nephrons. Leads to fibrosis and tubular atrophy resulting in renal failure
Also Liver fibrosis (behaves like congenital hepatic fibrosis)
Abnormal fibrocystin (gene PKHD1)

Clinical presentation: Bilateral flank masses, respiratory
problems, oligohydramnios, pulmonary hypoplasia, resp. distress…
Hypertension Initial renal function normal in 20-30% Liver failure with portal HTNUS:No cysts. Enlarged kidneys,
hyperechogenic with poor corticomedullary differentiation.


Treatment: supportive. Ventilation in neonatal period. Management of hypertension, electrolytes and renal failure.
Prognostic: 30% die in the neonatal period.If they survive the first year the 15yr survival is 70-80%.

Most common hereditary kidney disease: 1/500-1000
Genes: PKD1 (80%) and PKD2 (20%) Bilateral enlarged kidneys with medullar
and cortical cysts Clinical manifestations in 4th or 5th
decade of life. Some symptoms in children are
hematuria, flank pain, abdominal masses, HTN and UTI

US: bilateral enlarged kidney and cysts. Early phase can be normal size and some changes are only unilateral (like MCKD)

Systemic: cysts in liver, pancreas, spleen and ovaries.
Intracranial aneurysm, prevalence of 5%.
Mitral valve prolapse in 12% of children Renal cell carcinoma has been reported
in association with ADPCKDDiagnosis: Enlarged kidneys in patient with first
degree affected relative. Findings will appear later.
Treatment: supportive. HTN: use ACE-I.

Renal dysgenesis: dysplastic, hypoplastic (hypodysplastic) and cystic.
Dysplasia: focal/diffuse primitive structures
Cystic dysplasia / Multicystic dysplasia
Unilateral 1/2000 – 4000 newborns

TGF – β and IGF – 2 (?)

Most common cause of abdominal mass in newborns
Contralateral hydronephrosis in 5-10% of patients.
Nuclear SCAN (?): non functioning VCUG (?): 15% have reflux Complete involution at 5 to 7 yo

17 cases MCKD 10w/ and 7w/o obstruction Pathology of fetuses –
immunohistochemistry TGF-2 absent and IGF-2 overexpressed in
MCKD

A review of the literature: involution rates 19–73%, Compensatory hypertrophy of the
contralateral kidney occurs from 24–81%
Estimated glomerular filtration rates (GFRs)range from 86–122 ml/min/1.73 m3 BSA

Management and etiology of the unilateral multicystic dysplastic kidney: a review. David S. Hains. Pediatr Nephrol (2009) 24:233–241

Of the 50 patients, 19 underwent nephrectomy, and the other 31 were conservatively managed with clinical and US or scan follow-up
Mean FU time 6 years. No complications, normal creatinine and urea in both groups

58 patients with MCKD Compare US (retrospective) and MRI
(prospective), only 1 nuclear scan…?????!?!??!?!

Case report:2mo F, MCKD, non functioning, HTN (on atenolol)
After the nephrectomy remained normotensive FU 1 year
Hypothesis: remaining functional cells produce renin

14 patients went to minimal invasive retroperitoneoscopic nephrectomy at 23mo not seen by US. No complications
Total involution in all the cases.

200 patients, 5 had infundibular stenosis with reflux. (20 years)
Consider to be an expected malformation part of the disease spectrum
Wilm´s tumor: no need for surveillance. (L3) Hypertension: nephrectomy to be consider
after other causes have been excluded. (L3) “complex” MCKD close FU to renal function,
“simple” normal life (L3) VUR more risk. UTI more risk in “complex”
MCKD (L3)

Recommendations: Correct dx: US / Nuclear scan +/- (Gr. A) Clinical judgement before doing VCUG (Gr.
D) “complex” vs “simple” (Gr. B) - Complex: BP!!! / UTI (prophylaxis??!?) - Simple: FU with US 12 and 24 mo to check
contralateral kidney
Multicystic dysplastic kidney in the neonate: the role of the urologist, Karen Psooy, MD, FRCSC.Can Urol Assoc J
2010;4(2):95-7





























