Embed Size (px)
Citation preview
Art Music and Drama Therapists
Dietitians
Physiotherapists
Orthoptists
Prosthetists and Orthotists
Occupational Therapists
Podiatrists
Paramedics
Radiographers
Speech and Language Therapists
Allied Health Professions
MSK toolkit
Maximising allied health professionalsrsquo contribution to the delivery of high quality and cost effective patient care
A guiDe fOR heALThcARe cOMMiSSiOneRS
preventionassessment
treatmentrehabilitation
re-ablementlong-term gain
how AhPs improve patient care and save the nhS money gt Click to enter toolkit
This toolkit is one of a series of toolkits developed by NHS London on behalf of the Strategic AHP Leads Group (SAHPLE)
Home MSK toolkit 2
Opening narrative
In the area of Musculoskeletal (MSK) care Allied Health Professionals (AHPs) are proactively supporting initiatives and service redesign which is evidence based and addresses the QIPP (Quality Innovation Productivity and Prevention) challenge
To bring this activity together the Strategic Health Authority Allied Health Profession Leads (SAHPLE) commissioned a project to identify clinical pathways where AHPs make a significant difference in the clinical outcomes for patients affected by MSK
AHPs include a number of professions who work both in uniprofessional teams and often in MSK care as part of a Multidisciplinary Team (MDT)
Musculoskeletal disorders (MSDs) are common and a major cause of ill health in the UK They are the single biggest cause of physical disability in the UK and can reduce quality of life impacting on family and social relations and limiting capacity to work Up to 60 of people on long term sick leave cite an MSD as the main reason (Health and Safety Executive Musculoskeletal disorders) Every year MSDs make up to 30 of GP consultations In 200910 this accounted for 21 million consultations The number of people with MSD is expected to rise with the number and proportion of older people in the population
Musculoskeletal disorders (MSDs) are problems affecting the muscles tendons ligaments nerves or other soft tissues and joints The back neck and upper limbs are particularly at risk There are many conditions including low back pain tennis elbow and carpal tunnel syndrome Acute symptoms may arise as a result of an identifiable event such as unaccustomed andor intense physical exertion resulting in pain and loss or restriction of movement for example sprains and strains Alternatively there may be a more gradual onset of symptoms with initial tingling then slight swelling or soreness which may persist and gradually worsen (ARMA 2006)
Since the DH published the published lsquoThe NHS plan ndash a plan for investmentrsquo in 2000 nurses and allied health professionals (AHPs) have increasingly adopted new roles adapting previous skills and utilising education programmes to expand their scope of practice to build services around the diverse needs of patientsDepartment of Health 2000a The NHS plan ndash a plan for investment A plan for reform London Download the report gt
Working across the whole pathway AHPs can offer at a general and advanced level significant improvements in the efficacy of services for MSD conditions including improved outcomes patient satisfaction and reduced costs by reducing referrals in primary and secondary care
For further information please contact
Lesley Johnson SHA Allied Health Professions Lead NHS London Southside 105 Victoria Street London SW1E 6QT
LesleyJohnsonlondonnhsuk
This toolkit has been endorsed by
preventiongtassessmentgt
treatmentgtrehabilitationgt
re-ablementgtlong-term gaingt
Home MSK toolkit 3
introduction
What does this toolkit do for you
This toolkit has been developed by a range of clinicians working in MSK care The information has been provided by a national collaboration of clinicians in conjunction with their professional bodies and is based on available research evidence
The work has been reviewed by a range of specialists including Sir Muir Gray Director UK NHS National Knowledge Service and NHS Chief Knowledge Officer The toolkit has been endorsed by the Professional Bodies
This toolkit provides information on the following
bull Which interventions most positively benefit patient care
bull What range of interventions over time will reap the most benefits during illness and lead to independence
bull How do the interventions match to the Outcomes Framework
bull Which interventions are able to save money to the system
bull How is the functional ability of patients enabled by using Allied Health Professionals (AHPs)
Audience
This information is aimed at those involved in commissioning or developing MSK care
The toolkit will provide an interactive method of ensuring that patient care is meeting quality standards and providing essential elements of the QIPP agenda
If you are looking to re-design or provide MSK care services this information will assist you to meet the needs of your local population
Contents
1 List of interventions by Allied Health Profession
2 A pathway graphic highlighting where each profession significantly contributes to value-for-money high quality care
3 QIPP (Quality Innovation Productivity and Prevention) ndash key facts
4 Matching interventions to the Outcomes Framework
5 Research evidence
6 Case studies
7 General information
We hope you find it valuable
Art Music and Drama Therapists Dietitians
Physiotherapists
Orthoptists
Prosthetists and Orthotists
Occupational Therapists
Podiatrists
Paramedics
Radiographers Speech and Language Therapists
Rehabilitation Re-ablement Long-term gainPrevention Assessment Treatment
patient journey
Key AHP inTeRvenTion PoinTs in THe sTRoKe PATHWAy
Click on one of the intervention stages below to find out more about AHPsrsquo input
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD Delay in diagnosis Physiotherapist Patient self-referral to physiotherapy ie the patients being able to refer themselves to a physiotherapist without the need to see the GP first enhances the patient choice and has been proved to be a highly effective and efficient use of resources This is a QIPP endorsed pathway Go to website gt
34 Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
MSD stratification Not being referred to the correct practitioner for the appropriate level of intervention
Physiotherapist A recent publication in the Lancet reported favorably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management Go to website gt
34
Home MSK toolkit 4
commissioning principles which AhPs do you need
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 5
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD requiring more complex assessment
Delay in diagnosis can mean that a short term illness can progress to a long term problem
Working for a healthier tomorrow Black report 2008
Physiotherapist
Podiatrist
Orthotist
Interface services (Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access with triage for referrals for MSK assessments and the management of chronic pain Patients can avoid secondary care waits by being managed in the community Interface services are generally run by multi-professional teams eg Advanced and general physiotherapists podiatrists and orthotists
34 A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required two wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes Download Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign gt
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)
bull Release of a Band 5 physio to other duties (pound20000)
Download AHP Service Improvement Project Compendium March 2011 gt
Persistent pain Poor quality of life Physiotherapist
Occupational therapist
Access to the full range of pain and rehabilitation services support people with persistent pain should have
3 INPUT is a pain management centre at St Thomasrsquo where patients from all over the country come to learn better ways of coping with their pain The centre offers residential pain management programmes which run throughout the year On average patients who complete treatment ndash and thatrsquos over 90 of those who are admitted onto the programme
bull can walk 50 further in 5 minutes
bull are less limited in their everyday lives (including work)
bull are more confident of managing their pain and less distressed by it
bull are using far fewer of the analgesic and psychotropic drugs they were taking before the programme
commissioning principles page 2 of 3
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 6
commissioning principles page 3 of 3
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
Overweight and obesity 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing Musculoskeletal (MSK) disorders
Dietitian
Physiotherapist
The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
3 Estimates of the direct NHS costs of treating overweight patients obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Download the National Obesity Observatoryrsquos report The Economic Burden of Obesity gt
Frail elderly prone to falling Loss of independence with potential permanent transfer from home
Occupational therapist
Physiotherapist
Paramedic
Podiatrist
All older people with recurrent falls or assessed as being at increased risk of falling should be referred to for a multidisciplinary assessment to address future risk and considered for an individualised multifactorial intervention (this would include strength and balance training home hazard assessment and intervention This is aimed at promoting independence and improving physical and psychological functioning NICE guideline CG21(2004)
135 Falls at home can lead to hip fracture which costs pound28600 or pound726m per year This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls Download the University of Birminghamrsquos report gt
Fractured neck of femur Fractured neck of femur is the most serious consequence of falls amongst the older population with high morbidity and mortality rates
Patients are likely to be malnourished on admission
Physiotherapist
Occupational therapist
Dietitian
AHPs working as part of the multidisciplinary team can provide a more co-ordinated approach which reduces length of stay mortality and readmissions
135 10 Trusts through a QIPP rapid improvement plan have reduced average length of stay to 113 days with subsequent cost savings AHPs were part of the multipdiscplinary team approach Key roles included mobilising patients within 12-18 hours of surgery and providing rehabilitation at weekends Go to website gt
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery which may lead to delayed hospital discharge slower recovery rates or even readmission
Paillaud E et al (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Download report gt
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
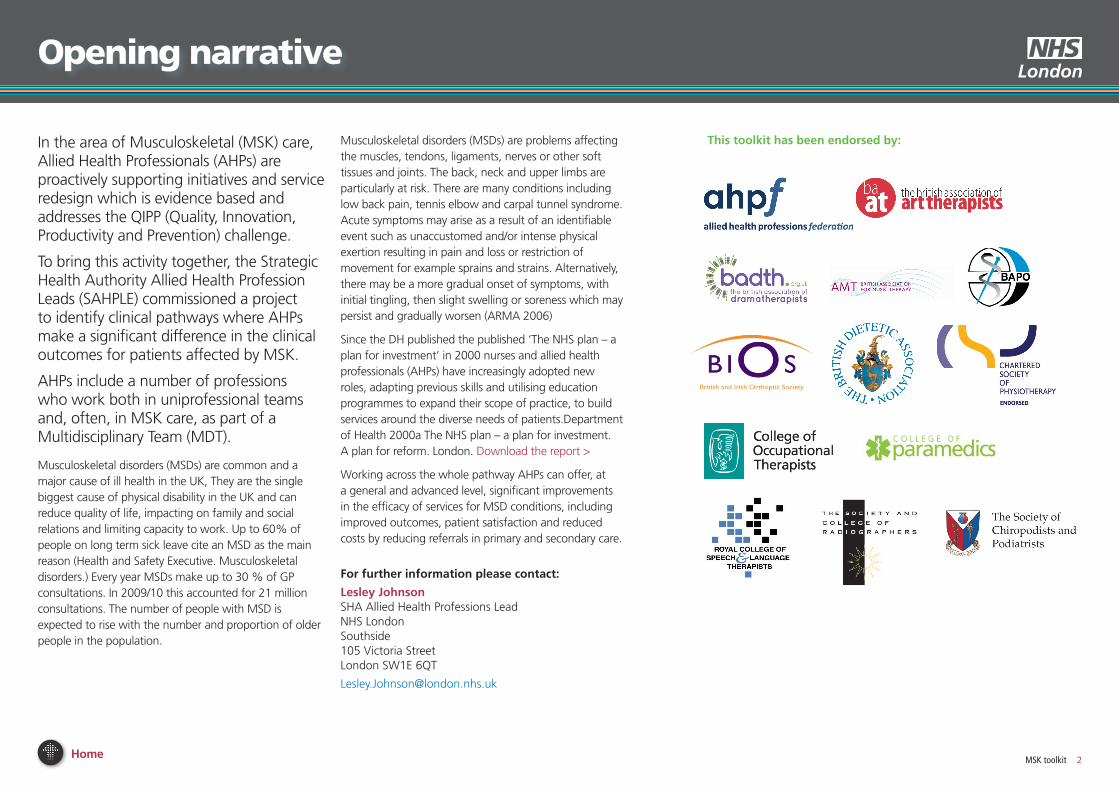
Home MSK toolkit 2
Opening narrative
In the area of Musculoskeletal (MSK) care Allied Health Professionals (AHPs) are proactively supporting initiatives and service redesign which is evidence based and addresses the QIPP (Quality Innovation Productivity and Prevention) challenge
To bring this activity together the Strategic Health Authority Allied Health Profession Leads (SAHPLE) commissioned a project to identify clinical pathways where AHPs make a significant difference in the clinical outcomes for patients affected by MSK
AHPs include a number of professions who work both in uniprofessional teams and often in MSK care as part of a Multidisciplinary Team (MDT)
Musculoskeletal disorders (MSDs) are common and a major cause of ill health in the UK They are the single biggest cause of physical disability in the UK and can reduce quality of life impacting on family and social relations and limiting capacity to work Up to 60 of people on long term sick leave cite an MSD as the main reason (Health and Safety Executive Musculoskeletal disorders) Every year MSDs make up to 30 of GP consultations In 200910 this accounted for 21 million consultations The number of people with MSD is expected to rise with the number and proportion of older people in the population
Musculoskeletal disorders (MSDs) are problems affecting the muscles tendons ligaments nerves or other soft tissues and joints The back neck and upper limbs are particularly at risk There are many conditions including low back pain tennis elbow and carpal tunnel syndrome Acute symptoms may arise as a result of an identifiable event such as unaccustomed andor intense physical exertion resulting in pain and loss or restriction of movement for example sprains and strains Alternatively there may be a more gradual onset of symptoms with initial tingling then slight swelling or soreness which may persist and gradually worsen (ARMA 2006)
Since the DH published the published lsquoThe NHS plan ndash a plan for investmentrsquo in 2000 nurses and allied health professionals (AHPs) have increasingly adopted new roles adapting previous skills and utilising education programmes to expand their scope of practice to build services around the diverse needs of patientsDepartment of Health 2000a The NHS plan ndash a plan for investment A plan for reform London Download the report gt
Working across the whole pathway AHPs can offer at a general and advanced level significant improvements in the efficacy of services for MSD conditions including improved outcomes patient satisfaction and reduced costs by reducing referrals in primary and secondary care
For further information please contact
Lesley Johnson SHA Allied Health Professions Lead NHS London Southside 105 Victoria Street London SW1E 6QT
LesleyJohnsonlondonnhsuk
This toolkit has been endorsed by
preventiongtassessmentgt
treatmentgtrehabilitationgt
re-ablementgtlong-term gaingt
Home MSK toolkit 3
introduction
What does this toolkit do for you
This toolkit has been developed by a range of clinicians working in MSK care The information has been provided by a national collaboration of clinicians in conjunction with their professional bodies and is based on available research evidence
The work has been reviewed by a range of specialists including Sir Muir Gray Director UK NHS National Knowledge Service and NHS Chief Knowledge Officer The toolkit has been endorsed by the Professional Bodies
This toolkit provides information on the following
bull Which interventions most positively benefit patient care
bull What range of interventions over time will reap the most benefits during illness and lead to independence
bull How do the interventions match to the Outcomes Framework
bull Which interventions are able to save money to the system
bull How is the functional ability of patients enabled by using Allied Health Professionals (AHPs)
Audience
This information is aimed at those involved in commissioning or developing MSK care
The toolkit will provide an interactive method of ensuring that patient care is meeting quality standards and providing essential elements of the QIPP agenda
If you are looking to re-design or provide MSK care services this information will assist you to meet the needs of your local population
Contents
1 List of interventions by Allied Health Profession
2 A pathway graphic highlighting where each profession significantly contributes to value-for-money high quality care
3 QIPP (Quality Innovation Productivity and Prevention) ndash key facts
4 Matching interventions to the Outcomes Framework
5 Research evidence
6 Case studies
7 General information
We hope you find it valuable
Art Music and Drama Therapists Dietitians
Physiotherapists
Orthoptists
Prosthetists and Orthotists
Occupational Therapists
Podiatrists
Paramedics
Radiographers Speech and Language Therapists
Rehabilitation Re-ablement Long-term gainPrevention Assessment Treatment
patient journey
Key AHP inTeRvenTion PoinTs in THe sTRoKe PATHWAy
Click on one of the intervention stages below to find out more about AHPsrsquo input
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD Delay in diagnosis Physiotherapist Patient self-referral to physiotherapy ie the patients being able to refer themselves to a physiotherapist without the need to see the GP first enhances the patient choice and has been proved to be a highly effective and efficient use of resources This is a QIPP endorsed pathway Go to website gt
34 Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
MSD stratification Not being referred to the correct practitioner for the appropriate level of intervention
Physiotherapist A recent publication in the Lancet reported favorably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management Go to website gt
34
Home MSK toolkit 4
commissioning principles which AhPs do you need
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 5
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD requiring more complex assessment
Delay in diagnosis can mean that a short term illness can progress to a long term problem
Working for a healthier tomorrow Black report 2008
Physiotherapist
Podiatrist
Orthotist
Interface services (Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access with triage for referrals for MSK assessments and the management of chronic pain Patients can avoid secondary care waits by being managed in the community Interface services are generally run by multi-professional teams eg Advanced and general physiotherapists podiatrists and orthotists
34 A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required two wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes Download Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign gt
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)
bull Release of a Band 5 physio to other duties (pound20000)
Download AHP Service Improvement Project Compendium March 2011 gt
Persistent pain Poor quality of life Physiotherapist
Occupational therapist
Access to the full range of pain and rehabilitation services support people with persistent pain should have
3 INPUT is a pain management centre at St Thomasrsquo where patients from all over the country come to learn better ways of coping with their pain The centre offers residential pain management programmes which run throughout the year On average patients who complete treatment ndash and thatrsquos over 90 of those who are admitted onto the programme
bull can walk 50 further in 5 minutes
bull are less limited in their everyday lives (including work)
bull are more confident of managing their pain and less distressed by it
bull are using far fewer of the analgesic and psychotropic drugs they were taking before the programme
commissioning principles page 2 of 3
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 6
commissioning principles page 3 of 3
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
Overweight and obesity 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing Musculoskeletal (MSK) disorders
Dietitian
Physiotherapist
The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
3 Estimates of the direct NHS costs of treating overweight patients obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Download the National Obesity Observatoryrsquos report The Economic Burden of Obesity gt
Frail elderly prone to falling Loss of independence with potential permanent transfer from home
Occupational therapist
Physiotherapist
Paramedic
Podiatrist
All older people with recurrent falls or assessed as being at increased risk of falling should be referred to for a multidisciplinary assessment to address future risk and considered for an individualised multifactorial intervention (this would include strength and balance training home hazard assessment and intervention This is aimed at promoting independence and improving physical and psychological functioning NICE guideline CG21(2004)
135 Falls at home can lead to hip fracture which costs pound28600 or pound726m per year This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls Download the University of Birminghamrsquos report gt
Fractured neck of femur Fractured neck of femur is the most serious consequence of falls amongst the older population with high morbidity and mortality rates
Patients are likely to be malnourished on admission
Physiotherapist
Occupational therapist
Dietitian
AHPs working as part of the multidisciplinary team can provide a more co-ordinated approach which reduces length of stay mortality and readmissions
135 10 Trusts through a QIPP rapid improvement plan have reduced average length of stay to 113 days with subsequent cost savings AHPs were part of the multipdiscplinary team approach Key roles included mobilising patients within 12-18 hours of surgery and providing rehabilitation at weekends Go to website gt
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery which may lead to delayed hospital discharge slower recovery rates or even readmission
Paillaud E et al (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Download report gt
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
preventiongtassessmentgt
treatmentgtrehabilitationgt
re-ablementgtlong-term gaingt
Home MSK toolkit 3
introduction
What does this toolkit do for you
This toolkit has been developed by a range of clinicians working in MSK care The information has been provided by a national collaboration of clinicians in conjunction with their professional bodies and is based on available research evidence
The work has been reviewed by a range of specialists including Sir Muir Gray Director UK NHS National Knowledge Service and NHS Chief Knowledge Officer The toolkit has been endorsed by the Professional Bodies
This toolkit provides information on the following
bull Which interventions most positively benefit patient care
bull What range of interventions over time will reap the most benefits during illness and lead to independence
bull How do the interventions match to the Outcomes Framework
bull Which interventions are able to save money to the system
bull How is the functional ability of patients enabled by using Allied Health Professionals (AHPs)
Audience
This information is aimed at those involved in commissioning or developing MSK care
The toolkit will provide an interactive method of ensuring that patient care is meeting quality standards and providing essential elements of the QIPP agenda
If you are looking to re-design or provide MSK care services this information will assist you to meet the needs of your local population
Contents
1 List of interventions by Allied Health Profession
2 A pathway graphic highlighting where each profession significantly contributes to value-for-money high quality care
3 QIPP (Quality Innovation Productivity and Prevention) ndash key facts
4 Matching interventions to the Outcomes Framework
5 Research evidence
6 Case studies
7 General information
We hope you find it valuable
Art Music and Drama Therapists Dietitians
Physiotherapists
Orthoptists
Prosthetists and Orthotists
Occupational Therapists
Podiatrists
Paramedics
Radiographers Speech and Language Therapists
Rehabilitation Re-ablement Long-term gainPrevention Assessment Treatment
patient journey
Key AHP inTeRvenTion PoinTs in THe sTRoKe PATHWAy
Click on one of the intervention stages below to find out more about AHPsrsquo input
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD Delay in diagnosis Physiotherapist Patient self-referral to physiotherapy ie the patients being able to refer themselves to a physiotherapist without the need to see the GP first enhances the patient choice and has been proved to be a highly effective and efficient use of resources This is a QIPP endorsed pathway Go to website gt
34 Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
MSD stratification Not being referred to the correct practitioner for the appropriate level of intervention
Physiotherapist A recent publication in the Lancet reported favorably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management Go to website gt
34
Home MSK toolkit 4
commissioning principles which AhPs do you need
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 5
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD requiring more complex assessment
Delay in diagnosis can mean that a short term illness can progress to a long term problem
Working for a healthier tomorrow Black report 2008
Physiotherapist
Podiatrist
Orthotist
Interface services (Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access with triage for referrals for MSK assessments and the management of chronic pain Patients can avoid secondary care waits by being managed in the community Interface services are generally run by multi-professional teams eg Advanced and general physiotherapists podiatrists and orthotists
34 A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required two wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes Download Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign gt
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)
bull Release of a Band 5 physio to other duties (pound20000)
Download AHP Service Improvement Project Compendium March 2011 gt
Persistent pain Poor quality of life Physiotherapist
Occupational therapist
Access to the full range of pain and rehabilitation services support people with persistent pain should have
3 INPUT is a pain management centre at St Thomasrsquo where patients from all over the country come to learn better ways of coping with their pain The centre offers residential pain management programmes which run throughout the year On average patients who complete treatment ndash and thatrsquos over 90 of those who are admitted onto the programme
bull can walk 50 further in 5 minutes
bull are less limited in their everyday lives (including work)
bull are more confident of managing their pain and less distressed by it
bull are using far fewer of the analgesic and psychotropic drugs they were taking before the programme
commissioning principles page 2 of 3
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 6
commissioning principles page 3 of 3
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
Overweight and obesity 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing Musculoskeletal (MSK) disorders
Dietitian
Physiotherapist
The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
3 Estimates of the direct NHS costs of treating overweight patients obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Download the National Obesity Observatoryrsquos report The Economic Burden of Obesity gt
Frail elderly prone to falling Loss of independence with potential permanent transfer from home
Occupational therapist
Physiotherapist
Paramedic
Podiatrist
All older people with recurrent falls or assessed as being at increased risk of falling should be referred to for a multidisciplinary assessment to address future risk and considered for an individualised multifactorial intervention (this would include strength and balance training home hazard assessment and intervention This is aimed at promoting independence and improving physical and psychological functioning NICE guideline CG21(2004)
135 Falls at home can lead to hip fracture which costs pound28600 or pound726m per year This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls Download the University of Birminghamrsquos report gt
Fractured neck of femur Fractured neck of femur is the most serious consequence of falls amongst the older population with high morbidity and mortality rates
Patients are likely to be malnourished on admission
Physiotherapist
Occupational therapist
Dietitian
AHPs working as part of the multidisciplinary team can provide a more co-ordinated approach which reduces length of stay mortality and readmissions
135 10 Trusts through a QIPP rapid improvement plan have reduced average length of stay to 113 days with subsequent cost savings AHPs were part of the multipdiscplinary team approach Key roles included mobilising patients within 12-18 hours of surgery and providing rehabilitation at weekends Go to website gt
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery which may lead to delayed hospital discharge slower recovery rates or even readmission
Paillaud E et al (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Download report gt
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
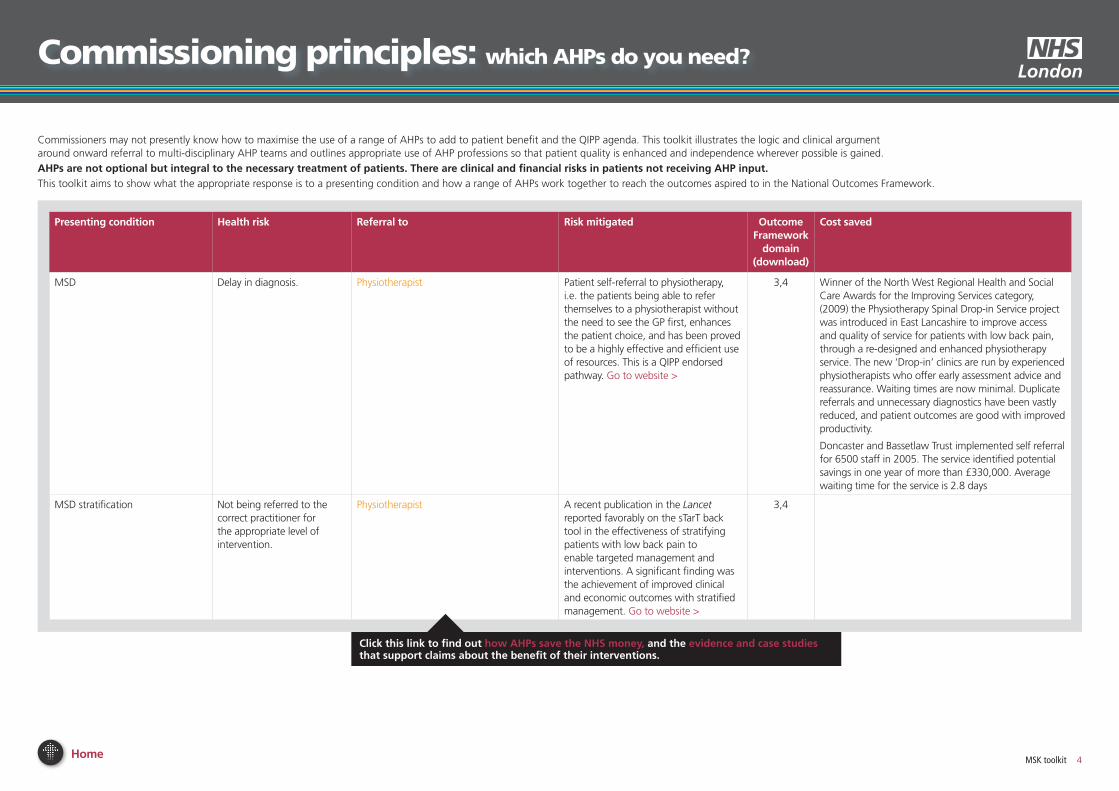
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD Delay in diagnosis Physiotherapist Patient self-referral to physiotherapy ie the patients being able to refer themselves to a physiotherapist without the need to see the GP first enhances the patient choice and has been proved to be a highly effective and efficient use of resources This is a QIPP endorsed pathway Go to website gt
34 Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
MSD stratification Not being referred to the correct practitioner for the appropriate level of intervention
Physiotherapist A recent publication in the Lancet reported favorably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management Go to website gt
34
Home MSK toolkit 4
commissioning principles which AhPs do you need
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 5
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD requiring more complex assessment
Delay in diagnosis can mean that a short term illness can progress to a long term problem
Working for a healthier tomorrow Black report 2008
Physiotherapist
Podiatrist
Orthotist
Interface services (Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access with triage for referrals for MSK assessments and the management of chronic pain Patients can avoid secondary care waits by being managed in the community Interface services are generally run by multi-professional teams eg Advanced and general physiotherapists podiatrists and orthotists
34 A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required two wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes Download Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign gt
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)
bull Release of a Band 5 physio to other duties (pound20000)
Download AHP Service Improvement Project Compendium March 2011 gt
Persistent pain Poor quality of life Physiotherapist
Occupational therapist
Access to the full range of pain and rehabilitation services support people with persistent pain should have
3 INPUT is a pain management centre at St Thomasrsquo where patients from all over the country come to learn better ways of coping with their pain The centre offers residential pain management programmes which run throughout the year On average patients who complete treatment ndash and thatrsquos over 90 of those who are admitted onto the programme
bull can walk 50 further in 5 minutes
bull are less limited in their everyday lives (including work)
bull are more confident of managing their pain and less distressed by it
bull are using far fewer of the analgesic and psychotropic drugs they were taking before the programme
commissioning principles page 2 of 3
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 6
commissioning principles page 3 of 3
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
Overweight and obesity 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing Musculoskeletal (MSK) disorders
Dietitian
Physiotherapist
The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
3 Estimates of the direct NHS costs of treating overweight patients obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Download the National Obesity Observatoryrsquos report The Economic Burden of Obesity gt
Frail elderly prone to falling Loss of independence with potential permanent transfer from home
Occupational therapist
Physiotherapist
Paramedic
Podiatrist
All older people with recurrent falls or assessed as being at increased risk of falling should be referred to for a multidisciplinary assessment to address future risk and considered for an individualised multifactorial intervention (this would include strength and balance training home hazard assessment and intervention This is aimed at promoting independence and improving physical and psychological functioning NICE guideline CG21(2004)
135 Falls at home can lead to hip fracture which costs pound28600 or pound726m per year This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls Download the University of Birminghamrsquos report gt
Fractured neck of femur Fractured neck of femur is the most serious consequence of falls amongst the older population with high morbidity and mortality rates
Patients are likely to be malnourished on admission
Physiotherapist
Occupational therapist
Dietitian
AHPs working as part of the multidisciplinary team can provide a more co-ordinated approach which reduces length of stay mortality and readmissions
135 10 Trusts through a QIPP rapid improvement plan have reduced average length of stay to 113 days with subsequent cost savings AHPs were part of the multipdiscplinary team approach Key roles included mobilising patients within 12-18 hours of surgery and providing rehabilitation at weekends Go to website gt
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery which may lead to delayed hospital discharge slower recovery rates or even readmission
Paillaud E et al (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Download report gt
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269

Home MSK toolkit 5
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
MSD requiring more complex assessment
Delay in diagnosis can mean that a short term illness can progress to a long term problem
Working for a healthier tomorrow Black report 2008
Physiotherapist
Podiatrist
Orthotist
Interface services (Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access with triage for referrals for MSK assessments and the management of chronic pain Patients can avoid secondary care waits by being managed in the community Interface services are generally run by multi-professional teams eg Advanced and general physiotherapists podiatrists and orthotists
34 A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required two wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes Download Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign gt
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)
bull Release of a Band 5 physio to other duties (pound20000)
Download AHP Service Improvement Project Compendium March 2011 gt
Persistent pain Poor quality of life Physiotherapist
Occupational therapist
Access to the full range of pain and rehabilitation services support people with persistent pain should have
3 INPUT is a pain management centre at St Thomasrsquo where patients from all over the country come to learn better ways of coping with their pain The centre offers residential pain management programmes which run throughout the year On average patients who complete treatment ndash and thatrsquos over 90 of those who are admitted onto the programme
bull can walk 50 further in 5 minutes
bull are less limited in their everyday lives (including work)
bull are more confident of managing their pain and less distressed by it
bull are using far fewer of the analgesic and psychotropic drugs they were taking before the programme
commissioning principles page 2 of 3
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Home MSK toolkit 6
commissioning principles page 3 of 3
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
Overweight and obesity 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing Musculoskeletal (MSK) disorders
Dietitian
Physiotherapist
The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
3 Estimates of the direct NHS costs of treating overweight patients obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Download the National Obesity Observatoryrsquos report The Economic Burden of Obesity gt
Frail elderly prone to falling Loss of independence with potential permanent transfer from home
Occupational therapist
Physiotherapist
Paramedic
Podiatrist
All older people with recurrent falls or assessed as being at increased risk of falling should be referred to for a multidisciplinary assessment to address future risk and considered for an individualised multifactorial intervention (this would include strength and balance training home hazard assessment and intervention This is aimed at promoting independence and improving physical and psychological functioning NICE guideline CG21(2004)
135 Falls at home can lead to hip fracture which costs pound28600 or pound726m per year This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls Download the University of Birminghamrsquos report gt
Fractured neck of femur Fractured neck of femur is the most serious consequence of falls amongst the older population with high morbidity and mortality rates
Patients are likely to be malnourished on admission
Physiotherapist
Occupational therapist
Dietitian
AHPs working as part of the multidisciplinary team can provide a more co-ordinated approach which reduces length of stay mortality and readmissions
135 10 Trusts through a QIPP rapid improvement plan have reduced average length of stay to 113 days with subsequent cost savings AHPs were part of the multipdiscplinary team approach Key roles included mobilising patients within 12-18 hours of surgery and providing rehabilitation at weekends Go to website gt
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery which may lead to delayed hospital discharge slower recovery rates or even readmission
Paillaud E et al (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Download report gt
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
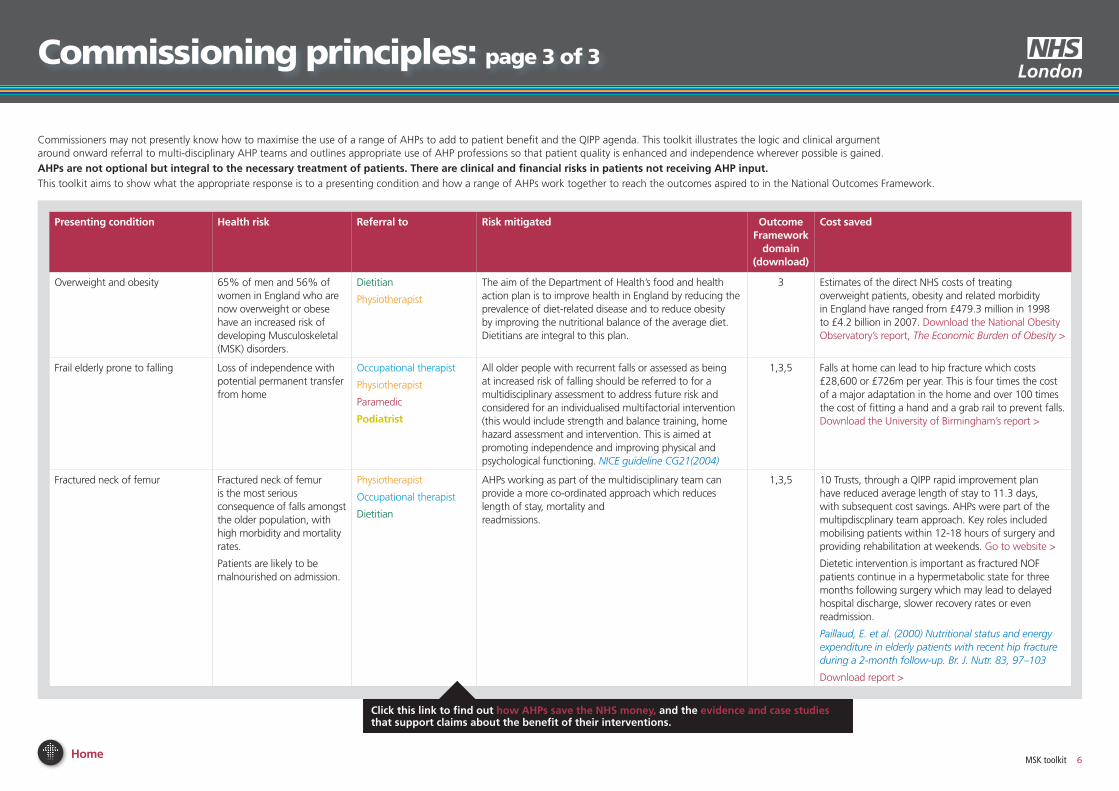
Home MSK toolkit 6
commissioning principles page 3 of 3
Commissioners may not presently know how to maximise the use of a range of AHPs to add to patient benefit and the QIPP agenda This toolkit illustrates the logic and clinical argument around onward referral to multi-disciplinary AHP teams and outlines appropriate use of AHP professions so that patient quality is enhanced and independence wherever possible is gained
AHPs are not optional but integral to the necessary treatment of patients There are clinical and financial risks in patients not receiving AHP inputThis toolkit aims to show what the appropriate response is to a presenting condition and how a range of AHPs work together to reach the outcomes aspired to in the National Outcomes Framework
Presenting condition Health risk Referral to Risk mitigated outcome Framework
domain(download)
Cost saved
Overweight and obesity 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing Musculoskeletal (MSK) disorders
Dietitian
Physiotherapist
The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
3 Estimates of the direct NHS costs of treating overweight patients obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Download the National Obesity Observatoryrsquos report The Economic Burden of Obesity gt
Frail elderly prone to falling Loss of independence with potential permanent transfer from home
Occupational therapist
Physiotherapist
Paramedic
Podiatrist
All older people with recurrent falls or assessed as being at increased risk of falling should be referred to for a multidisciplinary assessment to address future risk and considered for an individualised multifactorial intervention (this would include strength and balance training home hazard assessment and intervention This is aimed at promoting independence and improving physical and psychological functioning NICE guideline CG21(2004)
135 Falls at home can lead to hip fracture which costs pound28600 or pound726m per year This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls Download the University of Birminghamrsquos report gt
Fractured neck of femur Fractured neck of femur is the most serious consequence of falls amongst the older population with high morbidity and mortality rates
Patients are likely to be malnourished on admission
Physiotherapist
Occupational therapist
Dietitian
AHPs working as part of the multidisciplinary team can provide a more co-ordinated approach which reduces length of stay mortality and readmissions
135 10 Trusts through a QIPP rapid improvement plan have reduced average length of stay to 113 days with subsequent cost savings AHPs were part of the multipdiscplinary team approach Key roles included mobilising patients within 12-18 hours of surgery and providing rehabilitation at weekends Go to website gt
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery which may lead to delayed hospital discharge slower recovery rates or even readmission
Paillaud E et al (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Download report gt
Click this link to find out how AHPs save the nHs money and the evidence and case studies that support claims about the benefit of their interventions
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
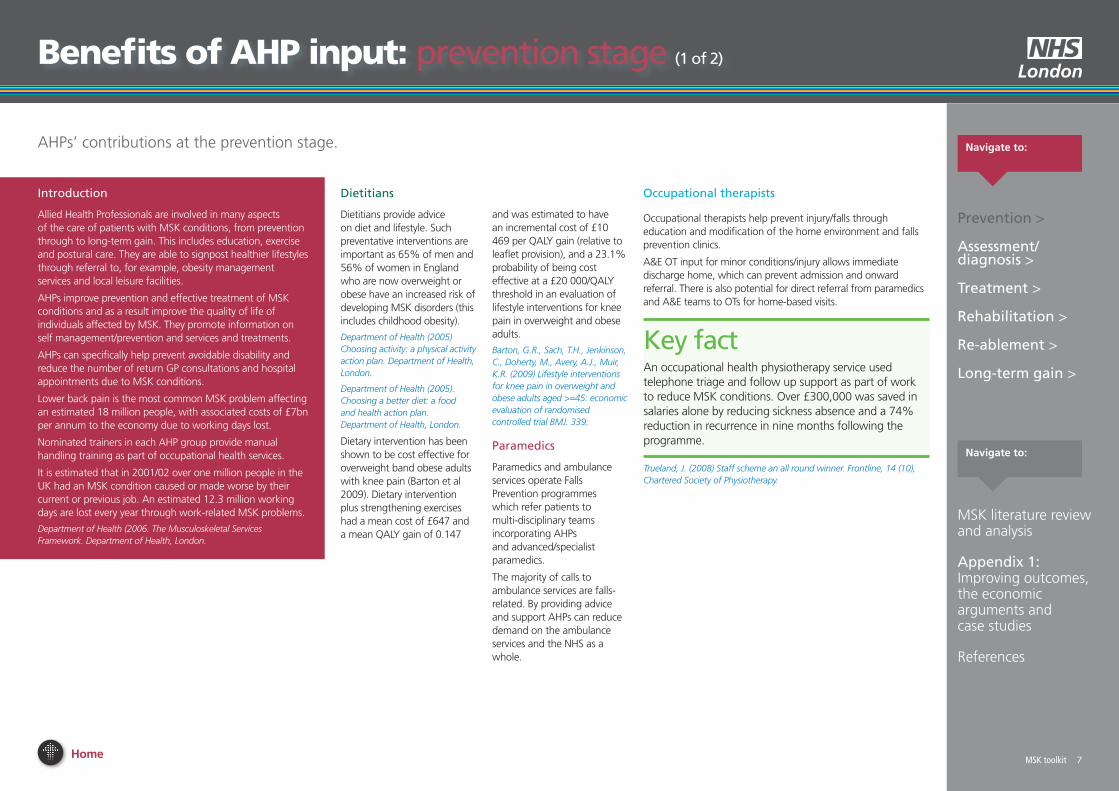
Home MSK toolkit 7
Benefits of AhP input prevention stage (1 of 2)
AHPsrsquo contributions at the prevention stage
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 7
Introduction
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self managementprevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Nominated trainers in each AHP group provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006 The Musculoskeletal Services Framework Department of Health London
Dietitians
Dietitians provide advice on diet and lifestyle Such preventative interventions are important as 65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Dietary intervention has been shown to be cost effective for overweight band obese adults with knee pain (Barton et al 2009) Dietary intervention plus strengthening exercises had a mean cost of pound647 and a mean QALY gain of 0147
and was estimated to have an incremental cost of pound10 469 per QALY gain (relative to leaflet provision) and a 231 probability of being cost effective at a pound20 000QALY threshold in an evaluation of lifestyle interventions for knee pain in overweight and obese adults
Barton GR Sach TH Jenkinson C Doherty M Avery AJ Muir KR (2009) Lifestyle interventions for knee pain in overweight and obese adults aged gt=45 economic evaluation of randomised controlled trial BMJ 339
Paramedics
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advancedspecialist paramedics
The majority of calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
Key fact An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational therapists
Occupational therapists help prevent injuryfalls through education and modification of the home environment and falls prevention clinics
AampE OT input for minor conditionsinjury allows immediate discharge home which can prevent admission and onward referral There is also potential for direct referral from paramedics and AampE teams to OTs for home-based visits
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
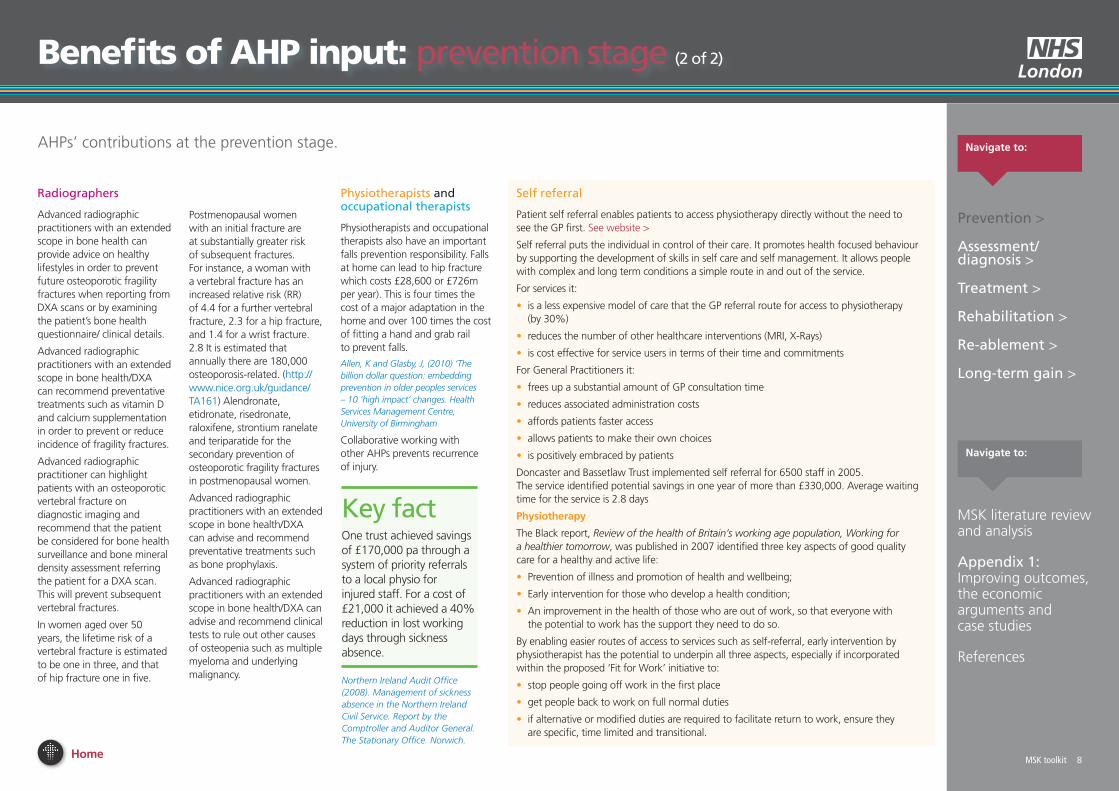
Home MSK toolkit 8
Benefits of AhP input prevention stage (2 of 2)
AHPsrsquo contributions at the prevention stage
Radiographers
Advanced radiographic practitioners with an extended scope in bone health can provide advice on healthy lifestyles in order to prevent future osteoporotic fragility fractures when reporting from DXA scans or by examining the patientrsquos bone health questionnaire clinical details
Advanced radiographic practitioners with an extended scope in bone healthDXA can recommend preventative treatments such as vitamin D and calcium supplementation in order to prevent or reduce incidence of fragility fractures
Advanced radiographic practitioner can highlight patients with an osteoporotic vertebral fracture on diagnostic imaging and recommend that the patient be considered for bone health surveillance and bone mineral density assessment referring the patient for a DXA scan This will prevent subsequent vertebral fractures
In women aged over 50 years the lifetime risk of a vertebral fracture is estimated to be one in three and that of hip fracture one in five
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
MSK toolkit 8
Postmenopausal women with an initial fracture are at substantially greater risk of subsequent fractures For instance a woman with a vertebral fracture has an increased relative risk (RR) of 44 for a further vertebral fracture 23 for a hip fracture and 14 for a wrist fracture 28 It is estimated that annually there are 180000 osteoporosis-related (httpwwwniceorgukguidanceTA161) Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend preventative treatments such as bone prophylaxis
Advanced radiographic practitioners with an extended scope in bone healthDXA can advise and recommend clinical tests to rule out other causes of osteopenia such as multiple myeloma and underlying malignancy
Physiotherapists and occupational therapists
Physiotherapists and occupational therapists also have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Collaborative working with other AHPs prevents recurrence of injury
Key fact One trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The Stationary Office Norwich
Self referral
Patient self referral enables patients to access physiotherapy directly without the need to see the GP first See website gt
Self referral puts the individual in control of their care It promotes health focused behaviour by supporting the development of skills in self care and self management It allows people with complex and long term conditions a simple route in and out of the service
For services it
bull is a less expensive model of care that the GP referral route for access to physiotherapy (by 30)
bull reduces the number of other healthcare interventions (MRI X-Rays)
bull is cost effective for service users in terms of their time and commitments
For General Practitioners it
bull frees up a substantial amount of GP consultation time
bull reduces associated administration costs
bull affords patients faster access
bull allows patients to make their own choices
bull is positively embraced by patients
Doncaster and Bassetlaw Trust implemented self referral for 6500 staff in 2005 The service identified potential savings in one year of more than pound330000 Average waiting time for the service is 28 days
Physiotherapy
The Black report Review of the health of Britainrsquos working age population Working for a healthier tomorrow was published in 2007 identified three key aspects of good quality care for a healthy and active life
bull Prevention of illness and promotion of health and wellbeing
bull Early intervention for those who develop a health condition
bull An improvement in the health of those who are out of work so that everyone with the potential to work has the support they need to do so
By enabling easier routes of access to services such as self-referral early intervention by physiotherapist has the potential to underpin all three aspects especially if incorporated within the proposed lsquoFit for Workrsquo initiative to
bull stop people going off work in the first place
bull get people back to work on full normal duties
bull if alternative or modified duties are required to facilitate return to work ensure they are specific time limited and transitional
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 9
Benefits of AhP input assessment diagnosis stage (1 of 3)
AHPsrsquo contributions at the assessmentdiagnosis stage navigate to
MSK toolkit 9
AHPs assess the care and treatment people with MSK conditions can expect This includes access to assessment of their needs diagnostics individual care plans and pain relief
All AHPs are able to undertake independent assessment of the patient and their MSD needs This is to formulate a clinical diagnosis and will form the basis of the patientrsquos treatment plan
Paramedics
A high proportion of 999 calls relate to MSK conditions and are often traumatic in origin A paramedic practitioner will assess and treat a patient and refer onwards if required This includes patients with joint back pain and mobility problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Specialist paramedics at the scene are able to administer Diazepam to help prevent spasms in lower back pain and Codydramol to help with pain management at the scene
Paramedics are able to autonomously undertake a full clinical examination of patients and determine with history the possible MSK injuries present that are not obvious
Paramedics and seniorspecialist paramedics can perform more detailed patient assessments including neuromuscular motor and sensory examinations
Occupational therapists
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph-Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun 17(2)210-28
Extended scope OT (hand therapy) has been developed at Guyrsquos and St Thomasrsquo Hospital and includes diagnosis assessment (ordering x-rays EMGs MRIs blood tests) and planning treatment up to surgery if required The patient can be seen after two weeks rather than waiting 12 weeks for a consultant appointment
Individual clinics are also offered by OTs for specific diagnostic groups ndash eg wrist problems ndash rather than general doctorrsquos clinic
ldquoThe extended scope hand therapistrsquos role has reduced consultant waiting times for selected hand and wrist diagnosis for first appointment from 10-12 weeks to two weeks and follow-up appointments from six weeks to two weeks It has also delivered cost-savings in consultant time which can now be diverted to increased surgery timerdquo
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Seniorspecialist paramedics can differentiate the patientrsquos condition which facilitates many patients being managed in the community as part of a wider primary care team
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
Seniorspecialist paramedics can also undertake a comprehensive health history including identifying red flags and in the case of back pain yellow flags Paramedics can link MSK co-morbidity to acute presentations
Continued on next page
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Physiotherapists
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
A spinal clinical assessment service assesses patients with spinal pain who have failed conservative treatment andor whose referral details indicate secondary care opinion may be necessary This service is led by extended scope physiotherapists
Sephton R Greatbatch P and Dawson J An evaluation of patients with spinal metastases initially presenting to a primary care spinal clinical assessment service NHS Knowsley
Physiotherapists are first contact practitioners who can assess diagnose and treat a patient with MSK conditions They screen for red flags ie infection and malignancy and refer to AampE
Onward referrals by physiotherapists occupational therapists and podiatrists can be made to specialists including ENT neurosurgery diabetic neuropathy clinics and vascular and rheumatology clinics
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Akbari A Mayhew A Al-Alawi MA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Through the use of ultrasound scan and differential injection therapy physiotherapists are able to make appropriate diagnoses
Home
Benefits of AhP input assessment diagnosis stage (2 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 10
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
PodiatristsPodiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
NICE recommends referral to a podiatrist for assessment and periodic review if patients have foot problems
National Institute of Clinical Excellence (2009)
The management of rheumatoid arthritis in adults
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
A recent publication in the Lancet reported favourably on the sTarT back tool in the effectiveness of stratifying patients with low back pain to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Jonathan C Hill David G T Whitehurst Martyn Lewis Stirling Bryan Kate M Dunn Nadine E Foster Kika Konstantinou Chris J Main Elizabeth Mason Simon Somerville Gail Sowden Kanchan Vohora Elaine M Hay Comparison of stratified primary care management for lowback pain with current best practice (STarT Back) a randomised controlled trial See website gt
Winner of the North West Regional Health and Social Care Awards for the Improving Services category (2009) the Physiotherapy Spinal Drop-in Service project was introduced in East Lancashire to improve access and quality of service for patients with low back pain through a re-designed and enhanced physiotherapy service The new lsquoDrop-inrsquo clinics are run by experienced physiotherapists who offer early assessment advice and reassurance Waiting times are now minimal Duplicate referrals and unnecessary diagnostics have been vastly reduced and patient outcomes are good with improved productivity
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 11Home
Benefits of AhP input assessment diagnosis stage (3 of 3)
navigate toAHPsrsquo contributions at the assessmentdiagnosis stage
MSK toolkit 11
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Diagnostic radiographers
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Diagnostic radiographers are one of the first contact practitioners when patients are referred from the Emergency Department (ED) and therefore they can use their clinical judgement to ensure correct projections are obtained in order to facilitate a definitive diagnosis The HPC (2007) Standards of Proficiency (Radiographers) states that radiographers should be able to analyse and critically evaluate the information collected They also state that the diagnostic radiographer should be ldquoable to distinguish between a disease process and traumardquo and distinguish between normal and abnormal
Diagnostic radiographers can ensure that the radiological referral is justified in accordance with IR(ME)R (2000) Protecting
patients from exposure to unnecessary higher than deemed appropriate radiation exposures Radiographic practitioners can facilitate the use of the correct imaging modality which will provide a definitive diagnosis whilst maintaining as low a radiation dose as possible
Diagnostic radiographers assess the diagnostic image appearances to evaluate if further supplementary images are required to assist with the patientrsquos diagnosis and treatment
The HPC (2008) document Standards of conduct states that a registrant should ldquocommunicate appropriately co-operate and share your knowledge and expertise with other practitioners for the benefit of the service usersrdquo
Advanced radiographic practitioners can communicate a definitive radiological report with the referrer and share their expertise to create an accurate diagnosis
Hot reporting
Hot reporting by Advanced radiographer practitioners can ensure that patients are not unnecessarily referred to fracture clinics with false positive fractures which will increase fracture clinic capacity and reduce unnecessary resources from being inappropriately used (Berman et al (1985) first compared the accuracy of radiographers and casualty officers in detecting radiographic abnormalities and concluded that radiographers had a role to play in highlighting abnormalities This development has progressed into radiographers producing definitive radiological reports)
Hot reporting a scheme where the images are reported immediately after their acquisition is seen as the ldquogold standardrdquo (Audit Commission 2002) However as noted by Hardy et al (2008b) a large proportion of radiographer reporting is undertaken at a later date (cold reporting)
Snaith (2007) noted that the introduction of hot reporting between 9am and 5pm Monday to Friday reduced the number of patients recalled following reporting by 52 a positive improvement in patient care
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home
Benefits of AhP input treatment stage (1 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 12
Physiotherapists
Advanced practitioner physiotherapists are able to use a range of medicines supply and prescribing mechanisms ndash Patient Specific Directions (PSDs) Patient Group Directions (PGDs) and Supplementary Prescribing Department of Health (2009) Allied Health Professions prescribing and medicines supply mechanisms scoping project report Download report gt
Orthotists
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles Orthoses also provide relief from pain and prevent physical deformities from progressing
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses are the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Key fact Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
Download York Health Economics Consortium document Orthotic Service in the NHS Improving Service Provision
Key fact Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Physiotherapists are able to manage soft tissue injuries in AampE
Richardson B Shepstone L Poland F Mugford M Finlayson B and Clemence N (2005) Emergency Medicine Journal 222 (87-92) 1472-0205
Self referral into physiotherapy services provides cost efficiencies of up to pound2m compared to GP referral
Holdsworth (2007) Self referral into physiotherapy
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Key fact Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculo-skeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Podiatrists Diagnostic radiographers
Following a small study into the implementation of radiographer reporting Blakeley et al (2008) concluded that radiographer reporting alleviated the problem of long reporting times and the radiographers had comparable accuracy rates to radiologists
Snaith (2007) recognised the role of radiographers in producing an instant report on AampE examinations and demonstrated that with a care plan in place the radiographer could discharge the patient from the imaging department This was favourable to the patient and to the AampE department
Radiographers can recommend rapid referral to orthopaedic rheumatologist and other specialists for further advice and intervention if required deemed necessary
Hot reporting of pre operative chest radiographs at the time of presentation in the Emergency Department which are performed on hip fracture patients can identify any co morbidity which may contraindicate surgical intervention but will also reduce delays of patients with normal chest radiographs going to theatre
interface services (also known as Clinical Assessment and Treatment Services Tier 2 etc) provide a single point of access that includes referral management assessment screening treatment and onward referral This is an alternative to hospital based treatment for MSDs and often means that patients can avoid secondary care waits by being managed effectively in the community
Interface services are generally run by multi-professional teams eg Advanced (often known as Extended Scope Practitioners) and General Physiotherapists Podiatrists and Orthotists
The STarT Back tool has been promoted as an integral part of the MSK Interface service A recent publication in the Lancet reported favourably on its effectiveness in stratifying patients with low back pain (low medium or high risk) to enable targeted management and interventions A significant finding was the achievement of improved clinical and economic outcomes with stratified management
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home
Benefits of AhP input treatment stage (2 of 2)
navigate toAHPsrsquo contributions at the treatment stage
MSK toolkit 13
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Occupational therapists
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
OTs also maximise patientsrsquo independence and achievement of occupational performance goals in daily living work and leisure activities They provide joint protection and energy conservation advice splinting services and provide relevant equipment
Paramedics
Paramedics can in many cases make autonomous treatment and management decisions for patients with MSK presentations
Paramedics have a wide range of therapeutic options within their scope of practice which expands further for seniorspecialist paramedics Oral and parenteral medicines are available to paramedics along with non-pharmacological interventions such as positioning and splintage
Pharmacological methods authorised for paramedics are Inhalational analgesia ndash Entonox Oral analgesia ndash Paracetamol and Ibuprofen Parenteral and enteral analgesia ndash Codeine NSAIDs Morphine Sulphate IV and Morphine Sulphate Oral Solution
To aid paramedics with nausea or emesis caused by MSK injuries and pain relief anti-emetics can be administered
Splintage can be provided by Paramedics in many ways These can include rigid splints sling and support bandages pneumatic splints vacuum splints pillow and blanket splints traction splints and buddy splinting Paramedics can also immobilise the whole patient using orthopaedic stretchers vacuum mattresses and rigid collars with head support
By providing a detailed assessment and diagnosis paramedics and seniorspecialist paramedics can access specialist referral pathways
Dietitians
Dietetic intervention is important as fractured NOF patients continue in a hypermetabolic state for three months following surgery (Paillaud et al 2000) which may lead to delayed hospital discharge slower recovery rates or even readmission
A Cochrane review entitled Protein and energy supplementation in elderly people at risk from malnutrition (Milne et al 2002) underlines the need to develop a dietary intervention programme which encourages not only appropriate consumption of usual meals but also enhanced consumption of everyday food snacks between meals to optimize nutritional state
Patients with fractured NOF are likely to be malnourished on admission and to show a rapid deterioration in nutritional status during admission Energy needs were not met in up to 50 of patients Nematy (2006) demonstrated the need to screen supplement and monitor fractured NOF patients Dietetic assistants have been shown to significantly reduced patientsrsquo (women aged 65+ with non-pathological hip fracture) risk of dying during and following care in the acute trauma unit (Duncan et al 2006))
Duncan DG Beck SJ Hood K Johansen A Using dietetic assistants to improve the outcome of hip fracture ndash a randomised controlled trial of nutritional support in an acute trauma ward Age and Ageing 200635(Suppl 3)i43
Milne AC Potter J and Avenell A (2002) Protein and energy supplementation in elderly people at risk from malnutrition Cochrane Database Syst Rev 3 CD003288
Nematy M Hickson M Brynes AE Ruxton CHS Frost GS (2006) Vulnerable patients with a fractured neck of femur nutritional status and support in hospital J Hum Nut Diet 19 209-218
Paillaud E Bories PN Le Parco JC and Campillo B (2000) Nutritional status and energy expenditure in elderly patients with recent hip fracture during a 2-month follow-up Br J Nutr 83 97ndash103
Podiatrists
Tibialis Posterior Dysfunction is a progressive disorder that leads to osteoarthritic changes of the foot and ankle and disability if left untreated It is a common condition that affects up to 10 of women normally over the age of 40 Podiatrists have the ability to treat this condition in all of its stages but are especially specialised in detecting it in its early stages and preventing its progresion1 Podiatrists treat this condition by means of orthosis ankle foot orthosis immobilisation in casts bracing rehabilitation steroidal injections and surgical intervention
Plantar fasciitis is a condition that affects 10 of the adult population and is seen more and more in general practice Conservative care is the mainstay of treatment for this condition2 Podiatrists Intervene by means of tapping orthosis night splints showing exercises steroidal injection extra corporeal shock wave and in very rare cases surgical intervention Authors have correlated a linkage between increased BMI and pronated foot types with plantar fasciitis many professionals feel this condition is therefore only going to increase in the population
1 Kohls-Gatzoulis J Angel J C Singh D Haddad F Livingstone J Berry G 2004 lsquoTibialis posterior dysfunction a common and treatable cause of adult acquired flatfootrsquo British Medical Journal vol 329 pp 1328-33
2 Cole C Seto C Gazewood J Plantar fasciitis evidence-based review of diagnosis and therapy Am Fam Physician 2005722237-2242
Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269

Home
Benefits of AhP input rehabilitation stage
navigate toAHPsrsquo contributions to the rehabilitation stage
MSK toolkit 14
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
Therapists
Rheumatoid arthritis osteoarthritis and osteoporosis are associated with loss of independence sufferers require more support in the community or admission to residential care A large proportion of patients with osteoporosis and fragility fractures are directly referred to fracture liaison service within the acute setting so that their bone health can be assessed in order to prevent future osteoporotic fractures
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliamentukpacm200910cmhansrdcm100119halltext100119
Physiotherapists and Occupational Therapists can help people get back to work and can be placed in vocationaloccupational health settings
Cochrane systematic review
Prosthetists
Prosthetists provide care and advice on rehabilitation for patients who have lost or who were born without a limb fitting the best artificial replacement
Paramedics
Paramedics working in primary care in senior or specialist roles are able to give patients information on rehabilitation and recovery times (ie definitions of acute and chronic back pain)
Occupational therapists
OTs intervene in hospitals and in homes Home assessments are undertaken to optimize functional independence in the home They also focus on vocational rehabilitation and return to work undertaking work site assessments and recommending return to work programmes
Dietitians
In their Cochrane review Avenell and Handell (2010) state ldquoGiven the high numbers of hip fracture patients with prior malnutrition and the prolonged length of stay it is surprising that nutrition including the provision and uptake of basic foodstuffs is often understated or even overlooked as a component of rehabilitative care programmesrdquo
Price et al (2006) showed that dietetic intervention is cost effective with a snack based intervention providing 26 of daily energy needs the average cost of one weekrsquos supply of snacks was pound422 per participant
Eighty visits (pre-intervention assessment counselling and final assessment visits lasting approximately 30 minutes) and 42 interim visits (to deliver snacks and check adherence lasting approximately 15 minutes) were carried out by the study dietitian amounting to a total of 505 hours an average of two hours 12 min per patient over the entire four-week intervention This equates to pound3480 of a Senior I dietitianrsquos salary and is equivalent to an average of pound632 per patient per visit The travel costs associated with monitoring and delivering the snacks amounted to pound1075 equivalent to 269 miles per visit The overall cost of the intervention programme amounted to pound2129 per participant per weekly visit
Avenell A and Handoll HH (2010) Nutritional supplementation for hip fracture aftercare in older people (Review)Cochrane Database Syst Rev 2 CD001880
Price RJG McMurdo MET Anderson AS (2006) A personalized snack-based intervention for hip fracture patients development feasibility and acceptability J Hum Nut Diet 19 139-145
Physiotherapists
Health at work an independent review of sickness absence
Every year 140 million working days are lost to sickness absence much of which ends in a swift return to work However a significant number of absences last longer than they need to and each year over 300000 people fall out of work onto health-related state benefits Before reaching this point many have been long-term sick off work They have become increasingly distanced from the labour market and suffer from the reduced economic social and health status that come with being out of work This Review has been carried out to stop as many people as possible from needlessly moving away from work because of ill health and to find ways of improving the coherence effectiveness and cost of the existing system for managing sickness absence Download report gt
The AHPrsquos Assessment of Fitness for Work ndash a tool to help people to stay in work while recovering from injury or ill health
140 million working days are lost to sickness absence costing employers pound9 billion a year in sick pay associated costs plus maintaining their business while people are off sick With evidence that long periods away from work can be detrimental to an individualrsquos health the CSP has lobbied for more employers to recognise the importance of supporting employees to remain in work even when they are unable to conduct their normal duties
The AHP Assessment of Fitness for Work is an A4 document providing a tick-box for lsquocan work with adaptationsrsquorsquocanrsquot workrsquo and a space for advice on how to retain an employee in work whilst recovering from illness or injury
The tool complements the GPsrsquo Statement of Fitness for Work (DWP 2010) by providing a consistent and easy to read form for AHPs to advise emnotployees on their fitness for work and how they might be able to return to work as part of their recovery The employee is given the form to share with their employer to help plan how their recovery may continue whilst working
If the employer cannot implement the recommendations the employee can then give the form to their GP for use in completion of the Fit Note The Assessment of Fitness to Work form can therefore help GPs employees and employers to focus on what a person can do whilst using work as part of their rehabilitation rather than sign a person off to recover at home
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 15
Benefits of AhP input re-ablement stage
navigate toAHPsrsquo contributions to the re-ablement stage
MSK toolkit 15
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Occupational therapists
Occupational therapists aim to improve or maintain patientsrsquo function in work leisure self care and domestic activities social roles and psychological status and focus on helping patients regain functional levels over short periods of time A wide range of interventions are provided including joint protection assistive devices and splints They also assist with home hazard identification and modification community access and safety and transportdriving
There is good evidence for the effectiveness of comprehensive occupational therapy in rheumatoid arthritis and for joint protection and splints in rheumatoid arthritis and osteoarthritis
Vocational rehabilitation to prevent job losses in rheumatic diseases is also effective
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Paramedics
Paramedics can advise patients with acute back pain to avoid bed rest and try to live as normally as possible
Key fact Supported self management of MSK conditions leads to a 35 reduction in referral into actual services in the first place
Download Health QWest Powerpoint presentation Whatrsquos new in rehabilitation
Dietitians
A randomised controlled trial of oral nutrition supplementation following hospital discharge has been shown to increase muscle strength (Price et al 2005) in elderly people Dietetic intervention to increase nutrient intake in this vulnerable group is an important aspect of enabling the functions of daily living to be resumed following hospital discharge
Price R Daly F Pennington CR amp McMurdo ME (2005) Nutritional supplementation of very old people at hospital discharge increases muscle strength a randomised controlled trial Gerontology 51 179ndash185
Physiotherapists
The physiotherapist-led Glasgow Falls Prevention Programme sees nearly 175 patients a month in their homes to assess risk factors and intervene on modifiable risk factors Between 1998 and 2008 there was a reduction in admissions due to falls in the home of 32 falls in residential institutions of 27 and falls in the street of nearly 40 Over the same period the number of admissions for hip fractures decreased by 36 This positive trend compares with a growth of hip fracture admissions of nearly 2 in England
The potential savings from fragility fracture prevention are significant for the UK health economy Physiotherapists can lead and input into many aspects of fragility fracture and falls prevention programmes
Skelton DA Neil F NHS Greater Glasgow and Clyde strategy for osteoporosis and falls prevention 2006-2010 An evaluation 2007-2009 Glasgow Glasgow Caledonian University 2009 Go to website gt
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 16
Benefits of AhP input long-term gain
navigate toAHPsrsquo contributions to long-term gain
MSK toolkit 16
Prevention gt
Assessmentdiagnosis gt
Treatment gt
Rehabilitation gt
Re-ablement gt
Long-term gain gt
navigate to
MSK literature review and analysis
Appendix 1 Improving outcomes the economic arguments and case studies
References
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
The four objectives of delivering a falls prevention services are
bull Improving patient outcomes and efficiency of care after hip fractures through compliance with core standards
bull Responding to a first fracture and preventing the second through fracture liaison service in primary care
bull Early intervention to restore independence
bull A reduction in accidents promotion of bone health and prevention of frailty
Department of Health (2009a) Falls and fractures effective interventions in health and social care The Stationary Office London
Physiotherapists
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
Paramedics Paramedics help reduce 999 calls for MSK injuries leading to reduced numbers of people being taken to AampE
AHPs working in occupational health advice role will also keep the NHS workforce at work
Occupational therapists
Occupational therapists are key in providing aspects of vocational rehabilitation
Department for Work and Pensions and Department of Health (2008) Improving health and work Changing Lives London Department of Health and Department for Work and Pensions
Long-term OT input is likely to be required for a range of MSK conditions and OT will monitor equipment such as hoists and have ongoing input in vocational rehabilitation
Independence at home can be maintained by regular review and modification to care packages and equipmentadaptations as needed
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Diagnostic radiographers
Hip fracture best practice tariff
About 70ndash75000 hip fractures occur annually in the UK Hip fracture is the commonest reason for admission to an orthopaedic ward and is usually a rsquofragilitylsquo fracture caused by a fall affecting an older person with osteoporosis or osteopaenia
The average age of a person with hip fracture is 77 years The annual cost of medical and social care for all the hip fracture cases in the UK amounts to about pound2 billion Demographic projections indicate that the UK annual incidence will rise to 91500 by 2015 and 101000 in 2020 with an associated increase in annual expenditure that could reach pound22 billion by 2020
Mortality is high ndash about 10 of people with a hip fracture die within one month and about one third within 12 months However fewer than half of deaths are attributable to the fracture This reflects the high prevalence of comorbidity in people with hip fractures often the occurrence of fall and fracture brings to light underlying ill health This presents major
challenges to anaesthetic surgical postoperative and rehabilitative care
Using alternative radiological imaging to confirm or exclude a suspected hip fracture in patients with a normal plain radiograph httpguidanceniceorgukCG124
Alendronate etidronate risedronate raloxifene strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA161 (2011) Available from wwwniceorgukTA161
Alendronate etidronate risedronate raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended) NICE technology appraisal guidance TA160 (2011) Available from wwwniceorgukTA160
Denosumab for the prevention of osteoporotic fractures in postmenopausal women NICE technology appraisal guidance TA204 (2010) Available from wwwniceorgukTA204
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 17
MSK literature review and analysis
The Strategic Allied Health Professionals Leads Group (SAHPLE) commissioned York Health Economics Consortium (YHEC) to carry out economic analysis of the impact of AHP interventions across MSK care pathways AHP practitioners provided YHEC with a framework which highlighted a series of specific interventions by AHPs classified under six categories
bull Preventionbull AssessmentDiagnosisbull Treatmentbull Rehabilitationbull Re-ablementbull Long-term gain
introduction
YHEC reviewed literature around each of the interventions included in the framework This has been a considerable undertaking with around 30 interventions being identified We carried out broad searches for literature using databases including Medline the Cochrane Database of Systematic Reviews and NHS Evidence We sought evidence from a range of sources in the following sequence DHNHS policy documents clinical guidelines case studies published literature individual NHS organisations and expert opinion We were also provided with a range of literature references from SAHPLE which we reviewed
These searches represent an extensive but not exhaustive search of the available literature With the resources available we were not able to search other sources such as literature held by the Royal Colleges which is available for members only We contacted the Chartered Society of Physiotherapy the Royal College of Speech and Language Therapists and the College of Occupational Therapists who provided some clinical guidelines However our search is likely to have identified the highest quality evidence The view from SAHPLE is that there is more extensive literature on interventions by AHPs but that much of this is not published
our approach
YHEC has used the data obtained to present the evidence in two ways
n Examples of economic analysis across the pathways where AHPs can make a significant impact on patient care and potentially costs Three scenarios are presented below
bull Self referral into physiotherapy
bull AHP inputs to help prevent and treat MSK-related falls
bull AHP involvement in the management of low back pain
n Evidence to support the effectiveness and potential economic benefits for each of the interventions included in the SAHPLE framework This is provided at Appendix A We have colour-coded the evidence obtained to provide an indication of the level of robustness of the evidence as follows
bull Evidence supported by published study or literature in GREEN
bull Evidence supported by observational study or case study in AMBER
bull Evidence supported by clinical opinion or assumption in RED
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 18
MSK literature review and analysis
scenario 1 self referral into physiotherapy
The Chartered Society of Physiotherapy has reported that episodes of patient self-referral to physiotherapy costs 26 less compared to traditional GP referral There is also evidence of good productivity with no increase in physiotherapy workload (after an initial temporary rise due to marketing of service) Benefits include reduced investigations (X-ray and MRI scans) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society1 75 of patients who self referred did not require a prescription for medicines and they were 50 less likely to be off work for more than one month2
Findings from the research in Scotland indicated 17 lower costs for self-referral compared with GP-suggested referral and 26 lower costs compared with GP referral3
1 Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence2 Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds3 Ibid
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
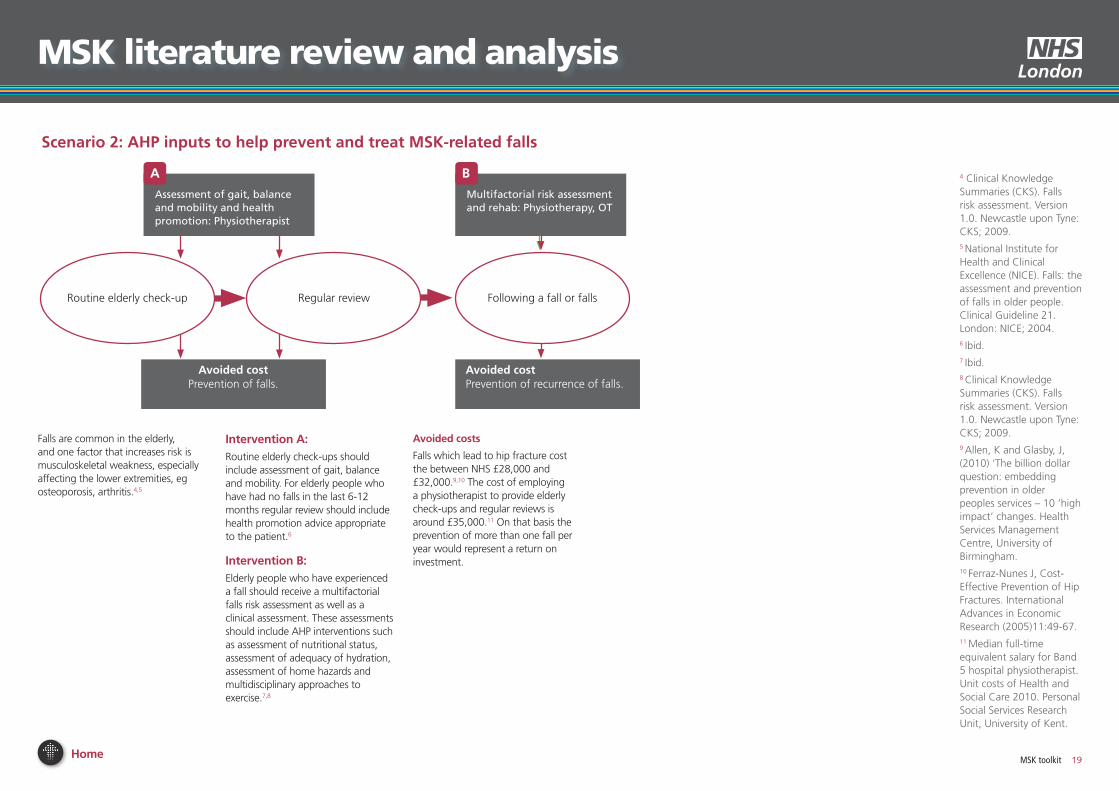
Home MSK toolkit 19
MSK literature review and analysis
Falls are common in the elderly and one factor that increases risk is musculoskeletal weakness especially affecting the lower extremities eg osteoporosis arthritis45
Multifactorial risk assessment and rehab Physiotherapy OT
B
scenario 2 AHP inputs to help prevent and treat MsK-related falls
4 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20095 National Institute for Health and Clinical Excellence (NICE) Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 20046 Ibid7 Ibid8 Clinical Knowledge Summaries (CKS) Falls risk assessment Version 10 Newcastle upon Tyne CKS 20099 Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham 10 Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-6711 Median full-time equivalent salary for Band 5 hospital physiotherapist Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
intervention ARoutine elderly check-ups should include assessment of gait balance and mobility For elderly people who have had no falls in the last 6-12 months regular review should include health promotion advice appropriate to the patient6
intervention BElderly people who have experienced a fall should receive a multifactorial falls risk assessment as well as a clinical assessment These assessments should include AHP interventions such as assessment of nutritional status assessment of adequacy of hydration assessment of home hazards and multidisciplinary approaches to exercise78
Avoided costs
Falls which lead to hip fracture cost the between NHS pound28000 and pound32000910 The cost of employing a physiotherapist to provide elderly check-ups and regular reviews is around pound3500011 On that basis the prevention of more than one fall per year would represent a return on investment
Avoided costPrevention of recurrence of falls
Avoided costPrevention of falls
Routine elderly check-up Regular review Following a fall or falls
Assessment of gait balance and mobility and health promotion Physiotherapist
A
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
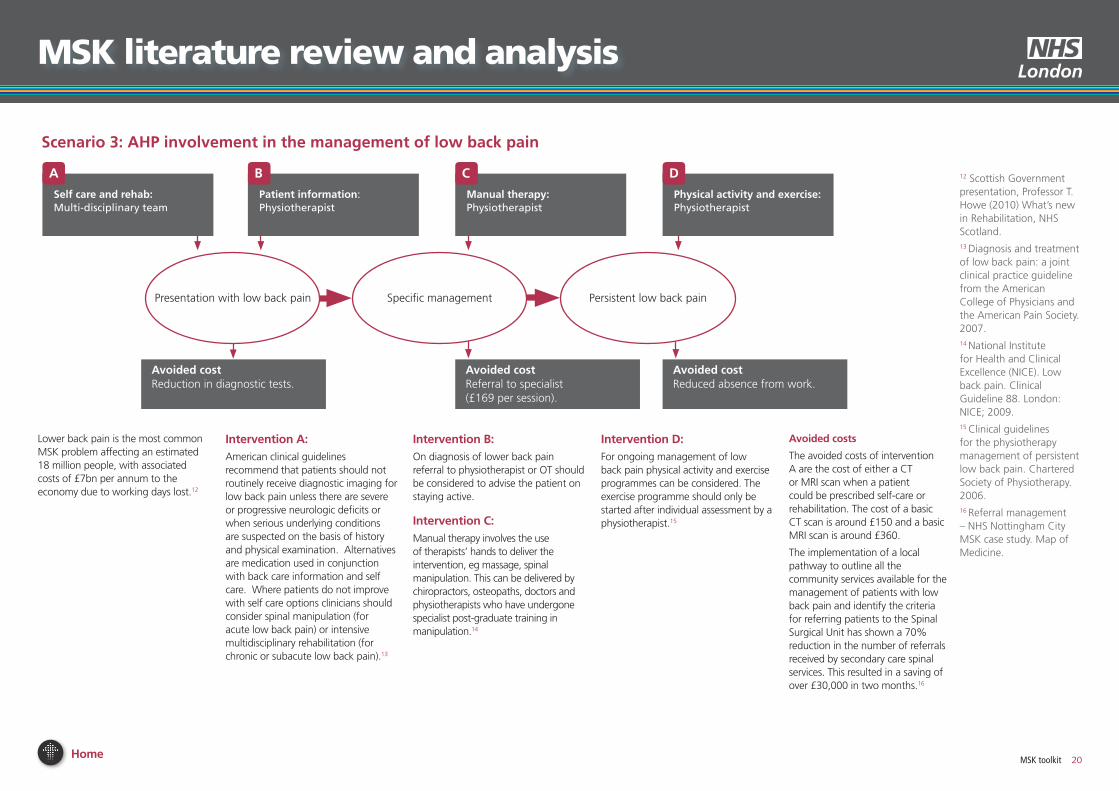
Home MSK toolkit 20
MSK literature review and analysis
scenario 3 AHP involvement in the management of low back pain
12 Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland13 Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 200714 National Institute for Health and Clinical Excellence (NICE) Low back pain Clinical Guideline 88 London NICE 200915 Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 200616 Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost12
self care and rehabMulti-disciplinary team
A
Patient information Physiotherapist
B
Avoided costReduced absence from work
Manual therapyPhysiotherapist
C
Physical activity and exercisePhysiotherapist
D
intervention AAmerican clinical guidelines recommend that patients should not routinely receive diagnostic imaging for low back pain unless there are severe or progressive neurologic deficits or when serious underlying conditions are suspected on the basis of history and physical examination Alternatives are medication used in conjunction with back care information and self care Where patients do not improve with self care options clinicians should consider spinal manipulation (for acute low back pain) or intensive multidisciplinary rehabilitation (for chronic or subacute low back pain)13
intervention BOn diagnosis of lower back pain referral to physiotherapist or OT should be considered to advise the patient on staying active
intervention CManual therapy involves the use of therapistsrsquo hands to deliver the intervention eg massage spinal manipulation This can be delivered by chiropractors osteopaths doctors and physiotherapists who have undergone specialist post-graduate training in manipulation14
intervention DFor ongoing management of low back pain physical activity and exercise programmes can be considered The exercise programme should only be started after individual assessment by a physiotherapist15
Avoided costs
The avoided costs of intervention A are the cost of either a CT or MRI scan when a patient could be prescribed self-care or rehabilitation The cost of a basic CT scan is around pound150 and a basic MRI scan is around pound360
The implementation of a local pathway to outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit has shown a 70 reduction in the number of referrals received by secondary care spinal services This resulted in a saving of over pound30000 in two months16
Avoided costReferral to specialist (pound169 per session)
Avoided costReduction in diagnostic tests
Presentation with low back pain Specific management Persistent low back pain
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
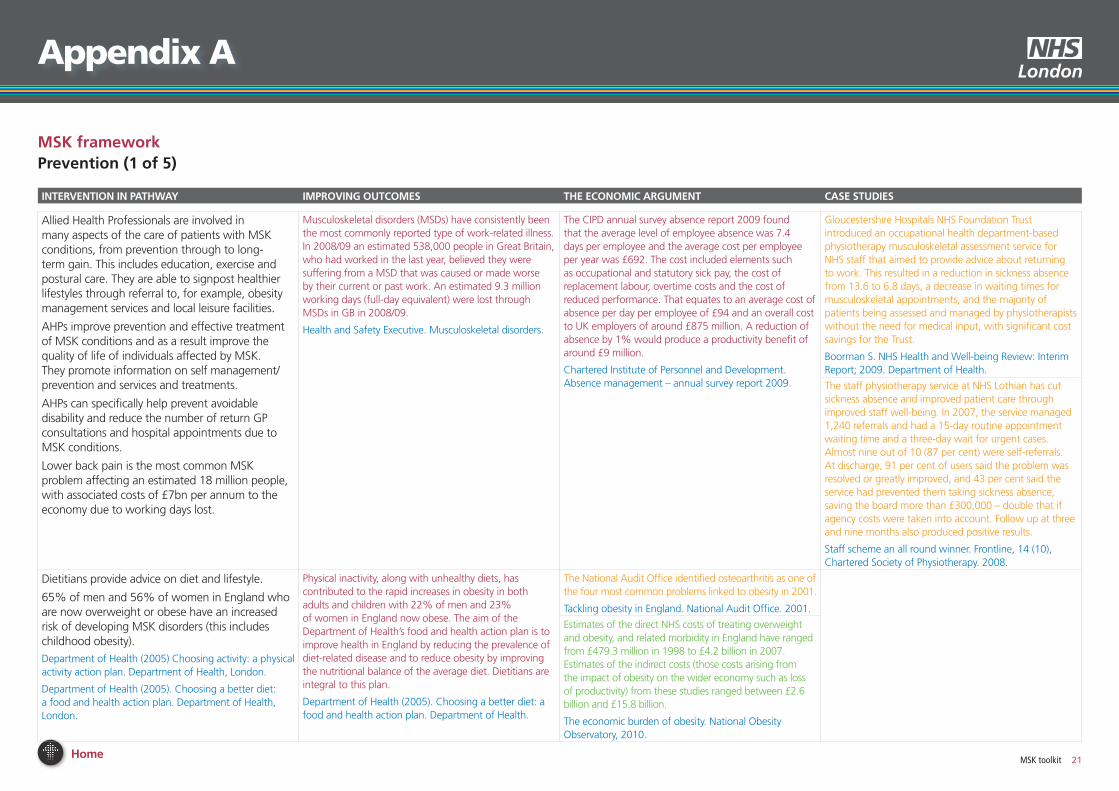
Home MSK toolkit 21
MsK frameworkPrevention (1 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Allied Health Professionals are involved in many aspects of the care of patients with MSK conditions from prevention through to long-term gain This includes education exercise and postural care They are able to signpost healthier lifestyles through referral to for example obesity management services and local leisure facilities
AHPs improve prevention and effective treatment of MSK conditions and as a result improve the quality of life of individuals affected by MSK They promote information on self management prevention and services and treatments
AHPs can specifically help prevent avoidable disability and reduce the number of return GP consultations and hospital appointments due to MSK conditions
Lower back pain is the most common MSK problem affecting an estimated 18 million people with associated costs of pound7bn per annum to the economy due to working days lost
Musculoskeletal disorders (MSDs) have consistently been the most commonly reported type of work-related illness In 200809 an estimated 538000 people in Great Britain who had worked in the last year believed they were suffering from a MSD that was caused or made worse by their current or past work An estimated 93 million working days (full-day equivalent) were lost through MSDs in GB in 200809
Health and Safety Executive Musculoskeletal disorders
The CIPD annual survey absence report 2009 found that the average level of employee absence was 74 days per employee and the average cost per employee per year was pound692 The cost included elements such as occupational and statutory sick pay the cost of replacement labour overtime costs and the cost of reduced performance That equates to an average cost of absence per day per employee of pound94 and an overall cost to UK employers of around pound875 million A reduction of absence by 1 would produce a productivity benefit of around pound9 million
Chartered Institute of Personnel and Development Absence management ndash annual survey report 2009
Gloucestershire Hospitals NHS Foundation Trust introduced an occupational health department-based physiotherapy musculoskeletal assessment service for NHS staff that aimed to provide advice about returning to work This resulted in a reduction in sickness absence from 136 to 68 days a decrease in waiting times for musculoskeletal appointments and the majority of patients being assessed and managed by physiotherapists without the need for medical input with significant cost savings for the Trust
Boorman S NHS Health and Well-being Review Interim Report 2009 Department of Health
The staff physiotherapy service at NHS Lothian has cut sickness absence and improved patient care through improved staff well-being In 2007 the service managed 1240 referrals and had a 15-day routine appointment waiting time and a three-day wait for urgent cases Almost nine out of 10 (87 per cent) were self-referrals At discharge 91 per cent of users said the problem was resolved or greatly improved and 43 per cent said the service had prevented them taking sickness absence saving the board more than pound300000 ndash double that if agency costs were taken into account Follow up at three and nine months also produced positive results
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Dietitians provide advice on diet and lifestyle
65 of men and 56 of women in England who are now overweight or obese have an increased risk of developing MSK disorders (this includes childhood obesity)
Department of Health (2005) Choosing activity a physical activity action plan Department of Health London
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health London
Physical inactivity along with unhealthy diets has contributed to the rapid increases in obesity in both adults and children with 22 of men and 23 of women in England now obese The aim of the Department of Healthrsquos food and health action plan is to improve health in England by reducing the prevalence of diet-related disease and to reduce obesity by improving the nutritional balance of the average diet Dietitians are integral to this plan
Department of Health (2005) Choosing a better diet a food and health action plan Department of Health
The National Audit Office identified osteoarthritis as one of the four most common problems linked to obesity in 2001
Tackling obesity in England National Audit Office 2001
Estimates of the direct NHS costs of treating overweight and obesity and related morbidity in England have ranged from pound4793 million in 1998 to pound42 billion in 2007 Estimates of the indirect costs (those costs arising from the impact of obesity on the wider economy such as loss of productivity) from these studies ranged between pound26 billion and pound158 billion
The economic burden of obesity National Obesity Observatory 2010
Appendix A
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 22
Appendix A
MsK frameworkPrevention (2 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists provide manual handling training as part of occupational health services
It is estimated that in 200102 over one million people in the UK had an MSK condition caused or made worse by their current or previous job An estimated 123 million working days are lost every year through work-related MSK problems
Department of Health (2006) The Musculoskeletal Services Framework Department of Health London
The Department of Health Musculoskeletal Services Framework includes an emphasis on the prevention of injury through occupational health services This includes primary prevention through accident prevention occupational health advice and healthy workplace initiatives
Department of Health (2006) The Musculoskeletal Services Framework
One Trust achieved savings of pound170000 pa through a system of priority referrals to a local physio for injured staff For a cost of pound21000 it had achieved a 40 reduction in lost working days through sickness absence
Northern Ireland Audit Office (2008) Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General The stationary office Norwich
An occupational health physiotherapy service used telephone triage and follow up support as part of work to reduce MSK conditions Over pound300000 was saved in salaries alone by reducing sickness absence and a 74 reduction in recurrence in nine months following the programme
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
Occupational health guidelines for the management of low back pain at work found that there is limited evidence but general consensus that joint employer-worker initiatives can reduced the number of reporting back injuries and sickness absences
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 23
Appendix A
MsK frameworkPrevention (3 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists and occupational therapists have an important falls prevention responsibility Falls at home can lead to hip fracture which costs pound28600 or pound726m per year) This is four times the cost of a major adaptation in the home and over 100 times the cost of fitting a hand and a grab rail to prevent falls
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
Each year 35 of over-65s experience one or more falls Between 10 and 25 of such fallers will sustain a serious injury A local authority and PCT population of 300000 may currently include 45000 people aged over 65 Of these 15500 will fall each year 1100 of whom wiIl sustain a fracture 360 to the hip
Based on NICE guidelines and population modelling amongst a population of 300000 around 10000 people per year who fall should receive a falls assessment with a further 5000 potentially requiring a brief screening of gait and balance
Department of Health Falls and fractures ndash Effective interventions in health and social care (2009)
Research highlights potential for reducing costs and achieving significant health benefits within older populations Prevention of hip fractures seems to be cost effective because it dominates a situation without any prevention This implies a reduction in the total costs for society and an improvement in quality of life and life expectancy
A fall at home that leads to a hip fracture cost the state pound25424 on average in 2000 or pound726 million in total Applying inflation to adjust those figures to 2010 prices would give a cost per hip fracture of pound32929 and a total cost of pound984 million This takes into account hospital costs ambulance costs social care costs GP costs outpatient costs and travel costs to outpatients This is 45 times the average cost of a major housing adaptation and over 100 times the cost of fitting hand and grab rails to prevent falls
Ferraz-Nunes J Cost-Effective Prevention of Hip Fractures International Advances in Economic Research (2005)1149-67
Calderdale PCT was one of the first local trusts to create a specific falls prevention team The team consists of four falls prevention workers and is led by a clinical specialist The workers co-ordinate personalised falls prevention services for older people across health and social care With the ultimate goal of preventing falls and reducing hospital admissions in this area key activities are
bull Raising public awareness of falls and how to prevent them
bull Case identification of older people at risk of fallsbull Detailed screening case management and referral to
appropriate servicesbull Provision of information and advice to older peoplebull Provision of strength and balance improvement groups
in local community settings and tailored exercise plans within older peoplersquos homes
Trueland J (2008) Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy
A range of AHPs help assist in reducing falls including occupational therapists These services include specific exercise programmes and safety awareness around the home There have been reported success rates of over a 50 reduction of subsequent falls for those receiving these types of interventions The cost of fractures following a fall in the elderly is significantly high and is borne by both health and social care Key objectives for developing falls prevention services include early intervention to restore independence and preventing frailty promoting bone health and reducing accidents all of which involve AHPs
Prevention of Falls Key facts College of Occupational Therapists
GPs can refer people for a falls risk assessment The falls prevention service will assess what may make people likely to fall and agree an individual action plan to reduce falling risk This could include strength and balance exercises home checks for hazards investigating continence problems checking eyesight and medicines and showing how to get up safely following a fall
Staying Steady Improving your strength and balance Age UK (2010)
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 24
Appendix A
MsK frameworkPrevention (4 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists podiatrists orthotists and occupational therapists also prevent the recurrence of injury and advise on community equipment and Telecare to help maintain an individualrsquos independence
The NHS in Scotland has established a pathway to prevent and manage falls by older people in the community Some of the key actions requiring the involvement of occupational therapists include providing community-based services to support safety at home and in the wider community and ensuring that older people identified as having a high risk of falling are offered a multi-factorial assessment to identify contributory risk factors
NHS Quality Improvement Scotland Up and about ndash Pathways for the prevention and management of falls and fragility fractures (2010)
In 1999 in the UK there were 647721 AampE attendances and 204424 admissions to hospital for fall-related injuries to people aged 60 years and over The total cost to the UK government from falls in those aged 60 and over was pound981 million 59 of this cost was incurred by the NHS and the remainder by the Personal Social Services for long term care Uplifted for inflation the total cost would be pound1286 billion
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
OTs in Central Aberdeenshire are involved in falls prevention and management in a number of settings OT assessment and intervention is provided as part of a 14-week multi-factorial falls programme offered at a number of NHS and community venues in the area A comprehensive OT assessment which includes the use of the standardised tools to identify environmental issues and assess cognition and perception ascertains the individualrsquos needs Tailored interventions to improve strength stamina and confidence and to provide advice on lifestyle management and energy conservation are offered Consideration is given to any equipment needs for function and safety OTs in the community also carry out initial falls risk assessments For patients admitted to hospital following a fall the process starts with an initial assessment by the ward OT and is continued following discharge until goals have been achieved All OT staff have access to a local resource which provides information on the care pathway for the prevention and management of falls and has been developed based on good practice and guidelines from the College of Occupational Therapy NICE and NHS Grampian
Heywood F and Turner L Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence (2007)
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 25
Appendix A
MsK frameworkPrevention (5 of 5)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Paramedics and ambulance services operate Falls Prevention programmes which refer patients to multi-disciplinary teams incorporating AHPs and advanced specialist paramedics
Many of the calls to ambulance services are falls-related By providing advice and support AHPs can reduce demand on the ambulance services and the NHS as a whole
The role of the paramedic has shifted from its focus on basic first aid and patient transportation to include higher levels of patient care and the treatment of a wide range of conditions Many paramedics have undertaken additional training and moved into specialist practitioner roles combining extended nursing and paramedic skills and supporting the first contact needs of patients in unscheduled care Specialist practitioners are primarily employed by ambulance service trusts and undertake a range of activities including carrying out and interpreting diagnostic tests undertaking basic procedures and assessments of patients with long-term conditions in their homes and prescribing a wider range of medications
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
Research suggests that specialist practitioners have had a significant positive impact on emergency servicesrsquo workloads leading to reductions in referrals to other health professionals and the use of emergency transport and in associated costs
The indications are that the specialist practitioner model delivered through the 999 service may yield cost savings of approximately pound291 per patient This saving comes primarily from lower staff costs at incident avoided Emergency Department attendances and lower use of non-inpatient follow-up services
However the validity of this finding and its generalisability to other models of care need to be confirmed in a larger study
S Mason et al Effectiveness of emergency care practitioners working within existing emergency service models of care Emerg Med J 2007
A falls and fracture prevention protocol for older people presenting at AampE following a fall was set up in AampE at the Royal infirmary Edinburgh to identify patients aged over 65 who require a falls prevention assessment following discharge from AampE after presentation with a fall
Those with recurrent falls andor who present with gait and balance problems on the Get Up and Go test are referred by an Accident and Emergency-based Occupational Therapist either to their local Community Falls service or if there are significant ongoing medical issues to a Day Hospital
wwwfallspathwaynhshealthqualityorg gt
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 26
Appendix A
MsK frameworkAssessmentDiagnosis (1 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Patients are referred to occupational therapists from orthopaedics rheumatology pain and occupational health services for hand conditions These patients are often assessed and a diagnosis made They are triaged accordingly for appropriate treatment
For carpal tunnel syndrome OTs provide hand assessment and undertake nerve conduction studies They can reduce waiting times for neurophysiological studies
Muller M Tsui D Schnurr R Biddulph- Deisroth L Hard J MacDermid JC (2004) ldquoEffectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic reviewrdquo Journal of hand therapy Apr-Jun17(2)210-28
Without triage to OT carpal tunnel patients group can experience long waits for orthopaedic consultant clinics Patients are often then referred on to OT services to be managed through a recognised pathway for treatment This delay in treatment can have a direct impact on the symptoms quality of life and work capacity of this patient group If patients are triaged by OTs it can lead to the following benefits
bull Patients see the most appropriate professional in a timely manner
bull Patients can be discharged from surgery quickerbull There can be earlier diagnostic testingbull OTs can refer direct to an ultrasound clinicbull Better utilisation of OT skills and appointmentsbull Reduction in waiting times for carpal tunnel patientsbull Increased consultant outpatient clinic capacitybull Utilisation and development of OT specialist skills to
deliver more timely and appropriate patient care
wwwimprovingnhsscotlandscotnhsuk gt
In the USA health care costs for carpal tunnel syndrome are estimated to be from $5000 per case for conservative treatment to $60000 for surgical interventions In the United States carpal tunnel release is one of the most common hand and wrist surgeries performed with approximately 400000 conducted per year In the workplace it results in lost days of productivity and wages high health care costs and constitutes a significant proportion of workersrsquo compensation claims
Muller M et al (2004) Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Journal of hand therapy Apr-Jun17(2)210-28
In NHS Dumfries and Galloway a protocol has been put in place to ensure that carpal tunnel patients are seen by an OT The OT takes the referral from the triage box and the patient is examined for carpal tunnel syndrome The diagnosis is either confirmed or an alternative diagnosis is given and the patient then follows the appropriate pathway relevant to their condition There has been a reduction in waiting times for patients from a minimum of 16 weeks wait for an outpatient appointment with a consultant and an appointment with an OT to a four to six week wait to see an OT in first instance with immediate implementation of treatment pathway
wwwimprovingnhsscotlandscotnhsuk gt
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 27
Appendix A
MsK frameworkAssessmentDiagnosis (2 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Diagnostic radiographers undertake X rays MRI and other radiographic investigations The majority of people with a MSK condition will need at least one type of imaging procedure to aid diagnosis Radiographers are able to use X rays as a diagnostic tool
Berman et al Hughes et al
Research evidence shows that given sufficient training and resources health staff can undertake many extended practices showing clear benefits in training AHPs to undertake specific tasks traditionally performed by medical practitioners Trained radiographers are able to use X-rays as a diagnostic tool but further research is needed to systematically evaluate the impact of extended roles on health outcomes
Department of Health Briefing Paper ndash Extending the practice of allied health professionals in the NHS March 2006
The difference in hourly cost of a reporting radiographer and a radiologist is around pound120 based on the cost of a radiographer at the mid-point of Agenda for Change Band 7 and a consultant radiologist
The potential saving from substituting radiographers for radiologists is only a realisable cash saving to the hospital if they subsequently reduce the number of radiologists they employ It is more likely that this will be an opportunity cost saving ie the freeing up of this resource in the form of time available to radiologists to carry out other work
A hot reporting service was implemented in AampE from 9-5 Monday to Friday This required 2 wte substantive advanced practitioner posts paid for through backfill posts This has led to a decrease in the number of misinterpretations and clinical management changes
Pinderfields General Hospital Wakefield ndash Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign
Service improvement in radiology should lead to benefits for patients (eg shorter waiting times for examinations and results increased patient safety) organisations (eg efficient cost effective services lower DNA rates shorter waiting times)
Staffing implications for improved radiology services include advanced practice such as
bull Radiographers perform barium enemas and other fluoroscopic procedures
bull Radiographer reporting (Plain films selected CT selected MR fluoroscopic procedures)
bull Protocol driven radiographer-led exams eg IVUs DEXA Nuclear Medicine
bull Radiographer and sonographer vetting of requestsbull Radiographers andor radiology nurses perform
selected interventional procedures (for example central line placement breast biopsy) or sedation
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269

Home MSK toolkit 28
Appendix A
MsK frameworkAssessmentDiagnosis (3 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists assess and diagnose foot and ankle pathologies to maintain and enhance locomotive function of the feet and legs alleviate pain and reduce the impact of disability
Musculoskeletal biomechanics is an important component of podiatry practice and involves multi and interdisciplinary work across primary secondary and tertiary care This collaboration can extend to hospital prosthetists and orthotists in surgical appliance and therapeutic footwear provision
The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Many podiatry patients present with pain caused by biomechanical problems which can involve the foot knee hip and lower back affecting gait These symptoms are often part of a multi-pathological problem exacerbated by diseases such as the many forms of arthropathies and diabetes The most cost effective and appropriate intervention to treat and prevent these symptoms is by the provision of foot orthoses which modify or correct the biomechanical problem Many types of foot orthoses can be provided by podiatrists according to patient needs and the presenting condition Foot orthoses can range from a simple heel raise or cushioning insoles through to complex bespoke devices which are made to prescription to alleviate symptoms or provide function realignment and change of gait
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Podiatrists provide assessment treatment and patient advice in order to reduce the long-term and potentially very serious problems that can result including amputation Podiatric intervention with such patients can reduce amputation rates by 40
J Needle et al The allied health professions and health promotion a systematic literature review and narrative synthesis NIHR 2011
In 2007 Stockport PCT piloted a joint podiatry and physiotherapy clinic Two sessions per week respectively of a physiotherapistrsquos time and a podiatristrsquos time were focussed on this new service provision Patients selected were those in greatest clinical need and who would benefit from joint and holistic assessment Discussions were also held with referrers such as GPs consultants health visitors and colleagues to establish two way pathways to enable referrals to and from the service when necessary There was improved liaison with diagnostic services such as imaging established a seamless service for diagnostic tests
Outcomes from the pilot were
bull A reduction in the paediatric physiotherapy waiting list from two years to six weeks
bull A reduction in the number of appointments for patients who are already attending many such appointments from multiple services
bull An increase in skills for both podiatrist and physiotherapist from learning outcomes whilst working jointly which cascades to departmental staff
bull There were no direct cost savings but a more efficient use of funding resulted in improved outcomes for patients
A significant saving to patients was experienced as they attended far fewer appointments which resulted in lower personal cost and less inconvenience
Department of Health (2006) The Musculoskeletal Services Framework
The cost of amputation is estimated at up to pound65000
Hutton and Hurry 2009 Orthotic Service in the NHS Improving Service Provision York Health Economics Consortium pg 12 - 13
It is estimated that up to 30 of all GP consultations are about musculoskeletal complaints
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 29
MsK frameworkAssessmentDiagnosis (4 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Podiatrists are able to request blood tests and scans and interpret the results to assist in obtaining a diagnosis They also request and interpret advanced vascular investigations These extended scope roles have led to reductions in waiting times for patients and more efficient use of resources
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare Department of Health London
Using podiatrists in diagnostic activity can help to reduce waiting times for patients and therefore help to improve their outcomes
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
The Bolton musculoskeletal clinical and treatment service has created a one-stop shop for patients referred for an orthopaedic surgical opinion who previously would have waited an average of six months for assessment followed by a further average of six months on the surgical waiting list
A triage service managed by orthopaedic advanced practitioners with extended scope skills (podiatrists and physiotherapists) assesses (including by carrying out X-rays and other clinical tests) and refers patients for surgery or conservative management If surgery is recommended the patient is given a lsquofitness for surgeryrsquo assessment and information to help them decide if they want to proceed on the same day Those who are offered conservative treatment can see a physiotherapist on the same day The use of advanced practitioners with extended scope skills has reduced the waiting time for an assessment to less than a week and the whole patient journey has reduced from an average of one year to below 18 weeks The one-stop shop offers patients an assessment test results and an opinion in one appointment with quicker access to further management
Department of Health (2008) Framing the contribution of allied health professionals delivering high quality healthcare
Community AHP MSK pathways reduce variation in practice and provide effective and sustainable care for patients with MSK conditions This is achieved through self referral evidence based triage protocols and single system MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
In Barnet MSK therapy services were improved by self-referral condition specific pathways and reduced waits This has improved services for patients and achieved savings
AHP Service Improvement Project Compendium March 2011
Productivity in Barnet improved when MSK therapy services were redesigned through
bull Improved DNA rates (pound20000)bull Release of a Band 5 physio to other duties (pound20000)
AHP Service Improvement Project Compendium March 2011
A multidisciplinary Tier 2 MSK triage interface service comprising extended scope podiatrists and physiotherapists set up in South Manchester reduced referrals to secondary care by 85 and reduced waiting times for patients to two weeks Cost per case has also reduced
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Home next
Appendix A
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 30
Appendix A
MsK frameworkAssessmentDiagnosis (5 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapists assess and diagnose patients using a range of techniques including imaging and blood tests and can triage lists for surgery
The present model of MSK care is a pathway where patients present at their GP and are then referred to secondary care and an orthopaedic waiting list Around 70 of patients referred do not require surgical intervention but their referral to a waiting list means that they are not being actively managed and there is no improvement in their functional capacity Low back pain is the most common MSK problem affecting an estimated 18 million people across the UK with associated costs of pound7 billion per year to the economy due to working days lost
The development of a community AHP MSK service can help to reduce variation in practice and provide effective and sustainable care for patients with MSK conditions The service is staffed by AHPs across all disciplines and allows for self referral across all MSK services evidence-based triage protocols and single system community MSK teams
Scottish Government presentation Professor T Howe (2010) Whatrsquos new in Rehabilitation NHS Scotland
The cost per patient per week for attendance at an outpatient clinic is pound150 The cost per patient per week for extended scope physiotherapy (ESP) services is around pound45 An average caseload of 30 patients in an orthopaedic clinic costs around pound4500 a week or pound234000 per year The average cost per week for ESP for the same caseload is around pound1350 or pound70000 per year
Research in Scotland found that self-referral to physiotherapy services could save the NHS in Scotland around pound2 million per year compared to GP referral and GP-suggested referral With ten times the population in England there could be potential for up to pound20 million savings per year
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Data confirms that of the patients referred into secondary care by the North Kirklees MSK service between 78 and 95 undergo surgery confirming only appropriate patients are referred on to consultants
Creaghan C (2009) Performance review of the North Kirklees MSK service 200809
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 31
Appendix A
MsK frameworkAssessmentDiagnosis (6 of 6)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Physiotherapists providing a second opinion before referring or enhancing services provided before a referral can improve the referral process
Physiotherapists have been shown to be as effective as post-fellowship junior doctors and clinical assistant orthopaedic surgeons in the assessment and management of new referrals to orthopaedic outpatients Physiotherapy involvement leads to lower indirect hospital costs
Physiotherapists and orthopaedic surgeons make similar diagnoses and have similar levels of accuracy in making clinical diagnosis for non-complex conditions of the knee and shoulder
Akbari A Mayhew A Al-AlawiMA Grimshaw J Winkens R Glidewell E Pritchard C Thomas R and Fraser C (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
Daker-White G Carr AJ Harvey I Woolhead G Bannister G Nelson I and Kammerling M (1999) A randomised controlled trail Shifting boundaries of doctors and physiotherapists in orthopaedic outpatient departments Journal of Epidemiology and Community Health Vol 5310
Aiken AB Harrison MM and Hope J (2009) Role of the advanced practice physiotherapist in decreasing surgical wait times Healthcare Quarterly 123 (80-83)
Research has found that some patients may be referred to a specialist inappropriately or not be referred when they should have or when they were referred have unnecessary tests or procedures Providing a second opinion before referring or enhancing the services provided before a referral (eg providing access to a physiotherapist) may improve the referral process
A study examined the effects of requiring an rsquoin housersquo second opinion prior to referral General practitioners considering referral arranged for the patient to see a different partner in the same practice for an independent assessment They found that approximately 70 of patients having an in-house second opinion were judged to need referral to the same hospital discipline immediately (630) or within 12 months (98) Patients referred in-house were more likely to report themselves as satisfied with their care
Akbari et al (2008) Interventions to improve outpatient referrals from primary care to secondary care Cochrane database of systematic reviews Issue 4
With an ageing population locally the Leicester Leicestershire and Rutland Planned Care Board identified musculoskeletal conditions as an area of high priority with variations in care pathways and patient outcomes Audits of individual patientsrsquo case notes identified that much of the variation in care arose from a lack of consistent access to support services such as Orthotics or Physiotherapy and a lack of consensus about expected pathways of care A group of some 50 clinicians from primary and secondary care (including GPs Consultants and Allied Health Professionals) developed a comprehensive set of local Musculoskeletal Referral Guidelines A baseline audit suggested that by implementing standard local pathways the Trusts could expect up to 4150 fewer first Orthopaedic outpatient appointments across the region and improved quality and equity for patients who are directed to the right place first time
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
NHS Nottingham City decided to develop a local pathway that would clearly outline all the community services available for the management of patients with low back pain and identify the criteria for referring patients to the Spinal Surgical Unit The clinical pathway development work was undertaken by the already established pathway steering group which included a Specialist Physiotherapist Since the launch of the pathway in June 2010 there has already been a 70 reduction in the number of referrals received by secondary care spinal services in Nottingham City This has resulted in a saving of over pound30000 in the first two months based on known expenditure from the previous year and on the cost of referrals after the pathway was published which dropped significantly
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 32
Appendix A
MsK frameworkTreatment (1 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Orthotists design and fit orthoses (braces etc) which provide support to a part of a patientrsquos body to compensate for paralysed muscles They also provide relief from pain and prevent physical deformities from progressing
Around 75 of patients attending an orthotic clinic in secondary care have a chronic condition with only 25 being acute or new patients
In Stockport an MSK podiatry service was set up with two podiatrists Money saved as a result of all orthotic devices being made in-house by technicians were between pound11-42 per device compared to pound70-200 per device when outsourced Patients also had significantly faster access to orthotics under this arrangement (the average time is two weeks from diagnosis)
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010)A guide to the benefits of podiatry to patient care
Podiatrists treat foot and ankle pathologies This includes the ability to undertake nail and soft tissue surgery and administration of local anaesthetics
Foot orthoses is the most cost effective and appropriate intervention to treat and prevent pain caused by biomechanical problems involving the foot knee hip and lower back affecting gait
Direct management of podiatric surgery within primary care (as opposed to the acute setting) significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay This is equivalent to 45000-60000 procedures nationally Elective foot surgery provided in the community setting by a podiatry team in South Derbyshire offered substantial cost savings over orthopaedics provided in an acute unit
The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
Direct management of podiatric surgery within primary care rather than the acute setting significantly reduces costs of each procedure 50-60 of foot cases which could be suitable for day case surgery are performed with an inpatient stay Day case podiatric surgery under local anaesthesia could undertake 45-60000 in-patient procedures nationally One primary care trust in Rotherham produced savings of pound300000 per annum against tariff and realised benefits within two years In Kent where there is a much larger podiatric surgery service savings of pound450000 have been achieved
wwwlibrarynhsukqipp ViewResourceaspxresID=330594 gt
Footwear is likely to be regarded as an important consideration in the clinical management of many foot disorders and the development of key criteria for the assessment of footwear by experts from the footwear industry together with expert podiatrists should enable the construction of a widely applicable tool in this evaluation
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 33
Appendix A
MsK frameworkTreatment (2 of 4)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Extended scope physiotherapy practitioners undertake prescribing
Present orthopaedic outpatient clinic appointments cost a total of pound18000 per month based on a cost of pound150appointment and 30 patients per clinic per week The total cost of an extended scope practitioner is pound5400 per month based on a rate of pound45 per appointment
Research in Scotland indicates that patient self referral to physiotherapy provides cost efficiencies compared to GP referral This could amount to a saving of pound2 million per year for Scotland
The additional costs of the 7 day service at Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust is around pound200000
The cost savings achieved were due to the reductions in LOS Improved patient throughput enabled the closure of beds and resultant necessary cost savings to the Trust (cost savings calculated using the NHS Institute figure of pound225 per bed day)
bull 1st Year ndash 2007 - Average LOS reduction from 78 days to 55 This resulted in a saving of 4000 bed days and over pound1 million
bull 2009 -10 - 1633 bed days saved from the previous year with an additional pound367000 saved upon the recurrent savings
bull 2010-12 - Predicted to save another 588 bed days pound132300
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Royal Bournemouth amp Christchurch Hospitals NHS Foundation Trust reduced hospital Length of Stay without compromising patient outcomes through the introduction of an Enhanced Recovery Program which included numerous Therapy initiatives in addition to improved MDT working across the whole Orthopaedic service
This has included the introduction of a 7 Day Orthopaedic Therapy service
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 34
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Self referral into physiotherapy services has a number of patient benefits including
bull high levels of service-user satisfaction and confidence
bull a more responsive and attractive service to patients with acute conditions affording them wider access
bull empowering patients to self-careself-manage to meet their needs
bull lower levels of work absence
The report of self-referral pilots to musculoskeletal physiotherapy supported findings of research in Scotland Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Holdsworth L Webster V McFadyen A lsquoWhat are the costs to NHS Scotland of self-referral to physiotherapy Results of a national trialrsquo Physiotherapy 2007 97(1) 3ndash11
An episode of patient self-referral versus traditional GP referral costs 25 less There is also evidence of good productivity with no increase in physiotherapy workload after initial temporary rise (due to marketing of service) and cuts out one stage in the current patient pathway Benefits include reduced investigations (X-ray and MRI) prescribing and the cost of medical consultation without any increase in physiotherapy contact numbers Benefits to patients include reduced overall costs associated with attending for medical consultations and reduced time off work which also benefits employers and the wider society
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral to physiotherapy has proven to be clinically successful and cost effective Patients who self referred themselves to physiotherapists during the self referral pilots (between 2006-2008 across NHS sites) showed a reduction in the need for investigations and prescribing 75 of patients who self referred not requiring a prescription for medicines were 50 less likely to be off work for more than one month
Department of Health (2008) Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
Doncaster and Bassetlaw Hospitals NHS Trust conducted a pilot to evaluate the benefits of providing an OH physiotherapy service for the trustrsquos staff 55 of staff referrals utilised the self-referral pathway During the evaluation period the average referral rate was 64 cases a month 448 for the seven-month evaluation period which equates to 768 per year
Of the total 55 per cent accessed the service through self referral negating the need to take time off to see a GP 18 per cent were referred by the OH department 12 per cent by their manager and 5 per cent by other unspecified routes The trust estimates that based on a D grade staff nurse earning pound87 per day the fast track service has the potential to make savings For example if each member of staff who referred over a 12 month period reduced their absence by one day then pound66816 would be saved (pound87 x 768 staff) If five days were saved per referral then the saving would be pound334080 (pound87 x 768 staff x 5 days)
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Appendix A
MsK frameworkTreatment (3 of 4)
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
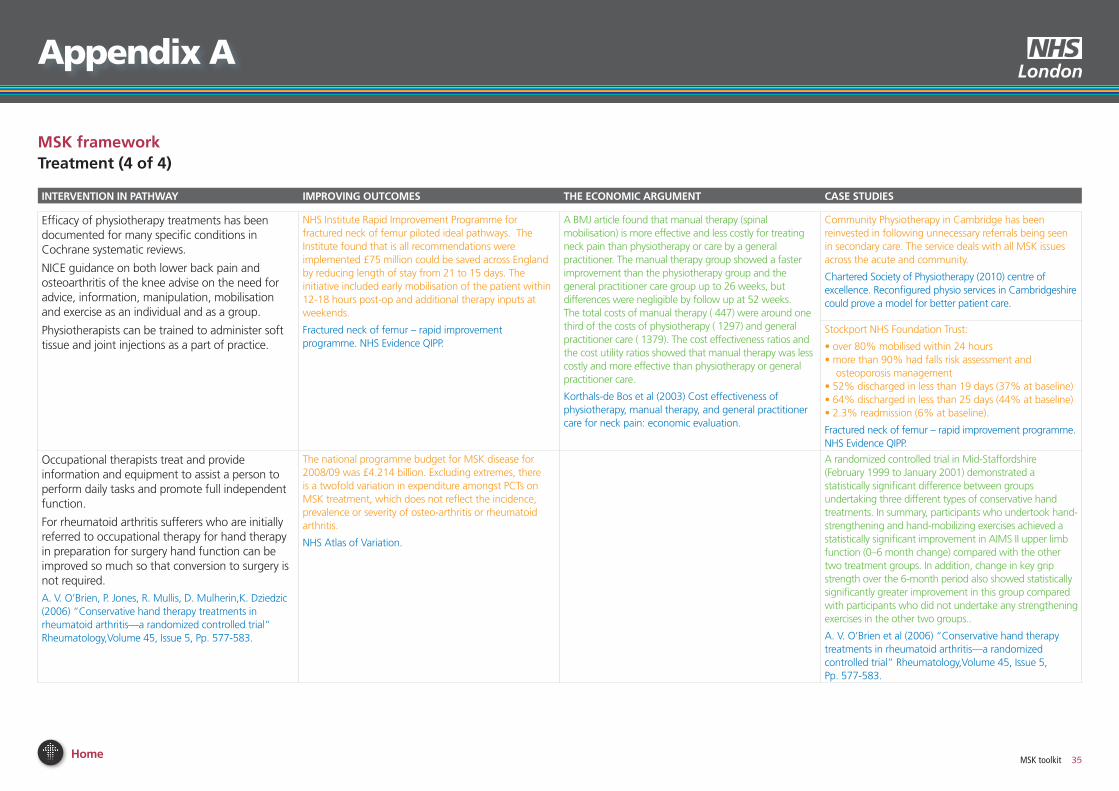
Home MSK toolkit 35
Appendix A
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
Efficacy of physiotherapy treatments has been documented for many specific conditions in Cochrane systematic reviews
NICE guidance on both lower back pain and osteoarthritis of the knee advise on the need for advice information manipulation mobilisation and exercise as an individual and as a group
Physiotherapists can be trained to administer soft tissue and joint injections as a part of practice
NHS Institute Rapid Improvement Programme for fractured neck of femur piloted ideal pathways The Institute found that is all recommendations were implemented pound75 million could be saved across England by reducing length of stay from 21 to 15 days The initiative included early mobilisation of the patient within 12-18 hours post-op and additional therapy inputs at weekends
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
A BMJ article found that manual therapy (spinal mobilisation) is more effective and less costly for treating neck pain than physiotherapy or care by a general practitioner The manual therapy group showed a faster improvement than the physiotherapy group and the general practitioner care group up to 26 weeks but differences were negligible by follow up at 52 weeks The total costs of manual therapy (euro447) were around one third of the costs of physiotherapy (euro1297) and general practitioner care (euro1379) The cost effectiveness ratios and the cost utility ratios showed that manual therapy was less costly and more effective than physiotherapy or general practitioner care
Korthals-de Bos et al (2003) Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation
Community Physiotherapy in Cambridge has been reinvested in following unnecessary referrals being seen in secondary care The service deals with all MSK issues across the acute and community
Chartered Society of Physiotherapy (2010) centre of excellence Reconfigured physio services in Cambridgeshire could prove a model for better patient care
Stockport NHS Foundation Trust
bull over 80 mobilised within 24 hoursbull more than 90 had falls risk assessment and
osteoporosis managementbull 52 discharged in less than 19 days (37 at baseline) bull 64 discharged in less than 25 days (44 at baseline)bull 23 readmission (6 at baseline)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Occupational therapists treat and provide information and equipment to assist a person to perform daily tasks and promote full independent function
For rheumatoid arthritis sufferers who are initially referred to occupational therapy for hand therapy in preparation for surgery hand function can be improved so much so that conversion to surgery is not required
A V OrsquoBrien P Jones R Mullis D MulherinK Dziedzic (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
The national programme budget for MSK disease for 200809 was pound4214 billion Excluding extremes there is a twofold variation in expenditure amongst PCTs on MSK treatment which does not reflect the incidence prevalence or severity of osteo-arthritis or rheumatoid arthritis
NHS Atlas of Variation
A randomized controlled trial in Mid-Staffordshire (February 1999 to January 2001) demonstrated a statistically significant difference between groups undertaking three different types of conservative hand treatments In summary participants who undertook hand-strengthening and hand-mobilizing exercises achieved a statistically significant improvement in AIMS II upper limb function (0ndash6 month change) compared with the other two treatment groups In addition change in key grip strength over the 6-month period also showed statistically significantly greater improvement in this group compared with participants who did not undertake any strengthening exercises in the other two groups
A V OrsquoBrien et al (2006) ldquoConservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trialrdquo RheumatologyVolume 45 Issue 5 Pp 577-583
MsK frameworkTreatment (4 of 4)
Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269

Home MSK toolkit 36
Appendix A
MsK frameworkRe-ablement (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
One review suggests that a process of reablement was able to reduce the need for home care by 28
Kent J et al (2000) External evaluation of the home care re-ablement pilot project De Montfort University Leicester
Norfolk first support a home care reablement service reduced care hours for those going on to longer term support by 90 23 ceased using the services as they no longer required it and there was a large reduction in the average weekly hours of support required for service users
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham (Norfolk county council re-ablement scheme)
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
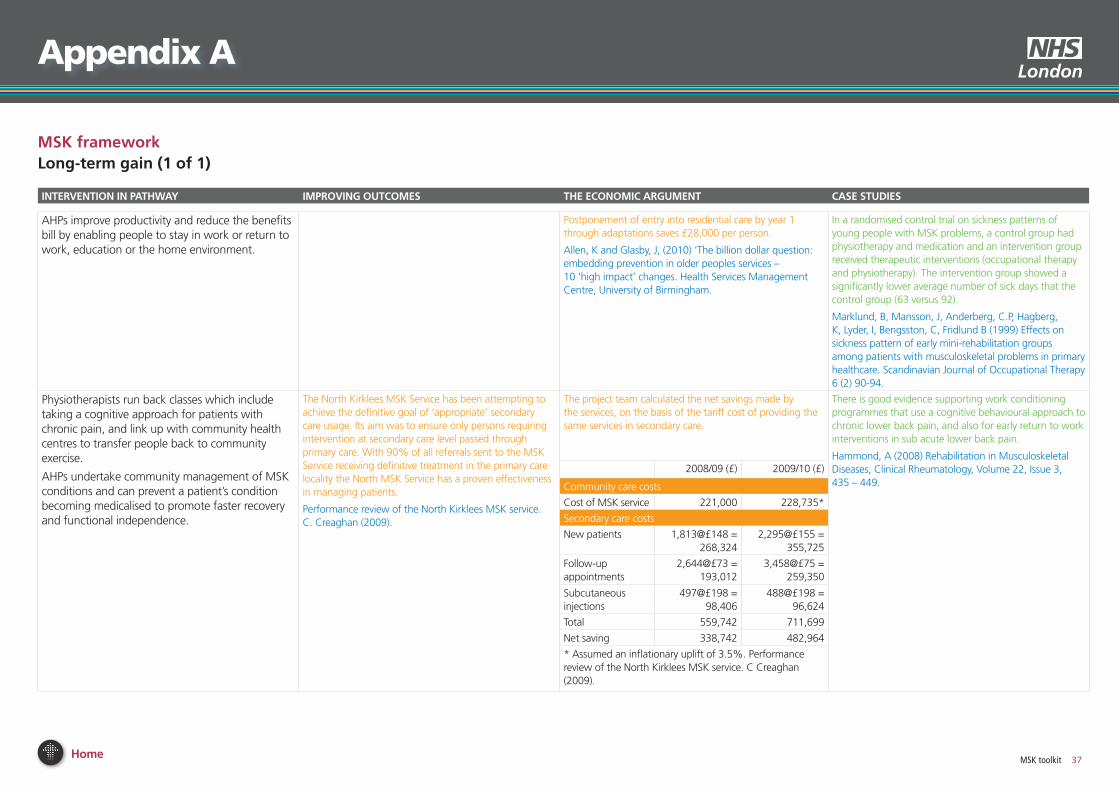
Home MSK toolkit 37
Appendix A
MsK frameworkLong-term gain (1 of 1)
inTeRvenTion in PATHWAy iMPRoving ouTCoMes THe eConoMiC ARguMenT CAse sTuDies
AHPs improve productivity and reduce the benefits bill by enabling people to stay in work or return to work education or the home environment
Postponement of entry into residential care by year 1 through adaptations saves pound28000 per person
Allen K and Glasby J (2010) lsquoThe billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Health Services Management Centre University of Birmingham
In a randomised control trial on sickness patterns of young people with MSK problems a control group had physiotherapy and medication and an intervention group received therapeutic interventions (occupational therapy and physiotherapy) The intervention group showed a significantly lower average number of sick days that the control group (63 versus 92)
Marklund B Mansson J Anderberg CP Hagberg K Lyder I Bengsston C Fridlund B (1999) Effects on sickness pattern of early mini-rehabilitation groups among patients with musculoskeletal problems in primary healthcare Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Physiotherapists run back classes which include taking a cognitive approach for patients with chronic pain and link up with community health centres to transfer people back to community exercise
AHPs undertake community management of MSK conditions and can prevent a patientrsquos condition becoming medicalised to promote faster recovery and functional independence
The North Kirklees MSK Service has been attempting to achieve the definitive goal of lsquoappropriatersquo secondary care usage Its aim was to ensure only persons requiring intervention at secondary care level passed through primary care With 90 of all referrals sent to the MSK Service receiving definitive treatment in the primary care locality the North MSK Service has a proven effectiveness in managing patients
Performance review of the North Kirklees MSK service C Creaghan (2009)
The project team calculated the net savings made by the services on the basis of the tariff cost of providing the same services in secondary care
There is good evidence supporting work conditioning programmes that use a cognitive behavioural approach to chronic lower back pain and also for early return to work interventions in sub acute lower back pain
Hammond A (2008) Rehabilitation in Musculoskeletal Diseases Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
200809 (pound) 200910 (pound)
Community care costs
Cost of MSK service 221000 228735
Secondary care costs
New patients 1813pound148 = 268324
2295pound155 = 355725
Follow-up appointments
2644pound73 = 193012
3458pound75 = 259350
Subcutaneous injections
497pound198 = 98406
488pound198 = 96624
Total 559742 711699
Net saving 338742 482964
Assumed an inflationary uplift of 35 Performance review of the North Kirklees MSK service C Creaghan (2009)
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 38
References
economic scenarios
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health 2008
Falls risk assessment Version 10 Clinical Knowledge Summaries (CKS) Newcastle upon Tyne CKS 2009
Falls the assessment and prevention of falls in older people Clinical Guideline 21 London NICE 2004
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Unit costs of Health and Social Care 2010 Personal Social Services Research Unit University of Kent
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T
Howe (2010) NHS Scotland
Diagnosis and treatment of low back pain a joint clinical practice guideline from the American College of Physicians and the American Pain Society 2007
Low back pain Clinical Guideline 88 London NICE 2009
Clinical guidelines for the physiotherapy management of persistent low back pain Chartered Society of Physiotherapy 2006
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Prevention
Musculoskeletal disorders Health and Safety Executive
Absence management ndash annual survey report 2009 Chartered Institute of Personnel and Development
NHS Health and Well-being Review Interim Report 2009 Boorman S Department of Health
Staff scheme an all round winner Frontline 14 (10) Chartered Society of Physiotherapy 2008
Choosing activity a physical activity action plan Department of Health (2005) London
Choosing a better diet a food and health action plan Department of Health (2005) London
Tackling obesity in England National Audit Office 2001
The economic burden of obesity National Obesity Observatory 2010
The Musculoskeletal Services Framework Department of Health (2006)
Occupational health guidelines for the management of low back pain at work evidence review G Waddell and A Burton Occupational Medicine 512 124-135 2001
Management of sickness absence in the Northern Ireland Civil Service Report by the Comptroller and Auditor General Northern Ireland Audit Office (2008)
Falls and fractures ndash Effective interventions in health and social care Department of Health (2009)
Prevention of Falls Key facts College of Occupational Therapists
Staying Steady Improving your strength and balance Age UK (2010)
Cost-Effective Prevention of Hip Fractures Ferraz-Nunes J International Advances in Economic Research (2005)1149-67
Better outcomes lower costs ndash Implications for health and social care budgets of investment in housing adaptations improvements and equipment a review of the evidence Heywood F and Turner L (2007)
Up and about ndash Pathways for the prevention and management of falls and fragility fractures NHS Quality Improvement Scotland (2010)
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Effectiveness of emergency care practitioners working within existing emergency service models of care S Mason et al Emerg Med J 2007
wwwfallspathwaynhshealthqualityorg
AssessmentDiagnosis
wwwimprovingnhsscotlandscotnhsuk
Effectiveness of hand therapy interventions in primary management of carpal tunnel syndrome a systematic review Muller M et al (2004) Journal of hand therapy Apr-Jun17(2)210-28
Briefing Paper ndash Extending the practice of allied health professionals in the NHS Department of Health March 2006
Service Improvement for Radiologists a signposting document summarising service improvement methodology and benefits NHS Radiology Service Improvement Team 2007
Radiographer-led hot reporting in AampE Modernising Radiology Services ndash A practical guide to redesign Pinderfields General Hospital Wakefield
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
The Musculoskeletal Framework ndash A joint responsibility doing it differently Department of Health 2006
The allied health professions and health promotion a systematic literature review and narrative synthesis J Needle et al NIHR 2011
Orthotic Service in the NHS Improving Service Provision Hutton and Hurry 2009 York Health Economics Consortium
Framing the contribution of allied health professionals delivering high quality healthcare Department of Health (2008) London
Whatrsquos new in Rehabilitation Scottish Government presentation Professor T Howe (2010) NHS Scotland
AHP Service Improvement Project Compendium March 2011
Coordinated integrated and fit for purpose ndash A delivery framework for adult rehabilitation in Scotland NHS Scotland 2007
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Interventions to improve outpatient referrals from primary care to secondary care Akbari A et al (2008) Cochrane database of systematic reviews Issue 4
A randomised controlled trail Shifting boundaries of doctors and physiotherapists
in orthopaedic outpatient departments Daker-White G et al (1999) Journal of Epidemiology and Community Health Vol 5310
Role of the advanced practice physiotherapist in decreasing surgical wait times Aiken AB et al (2009) Healthcare Quarterly 123 (80-83)
Reducing health inequalities ndash Leicestershire MSK services case study Map of Medicine
Referral management ndash NHS Nottingham City MSK case study Map of Medicine
Treatment
Example of service improvement project in MSK podiatry services in Stockport 2009 The Society of Chiropodists and Podiatrists (2010) A guide to the benefits of podiatry to patient care
A guide to the benefits of podiatry to patient care The Society of Chiropodists and Podiatrists (2010)
Expert group criteria for the recognition of healthy footwear W Vernon et al British Journal of Podiatry (2007)
wwwlibrarynhsukqipp
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269
Home MSK toolkit 39
References
Self referral pilots to musculoskeletal physiotherapy and the implications for improving access to other AHP services Department of Health Leeds
7 day orthopaedic therapy service Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust
Patient referral to musculoskeletal physiotherapy Chartered Society of Physiotherapy NHS Evidence
Maximising the role of physiotherapists in delivering occupational health services Briefing 44 Chartered Society of Physiotherapy (2008)
Fractured neck of femur ndash rapid improvement programme NHS Evidence QIPP
Cost effectiveness of physiotherapy manual therapy and general practitioner care for neck pain economic evaluation Korthals-de Bos et al (2003)
NHS Atlas of Variation
Conservative hand therapy treatments in rheumatoid arthritismdasha randomized controlled trial A V OrsquoBrien et al (2006) Rheumatology Volume 45 Issue 5 Pp 577-583
Rehabilitation
House of Commons Hansard Debates 19th January 2010 wwwpublicationsparliament
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Preventing and reducing admissions through AampE departments Key facts College of Occupational Therapists
Re-ablement
External evaluation of the home care re-ablement pilot project Kent J et al (2000) De Montfort University Leicester
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Long-term gain
The billion dollar question embedding prevention in older peoples services ndash 10 lsquohigh impactrsquo changes Allen K and Glasby J (2010) Health Services Management Centre University of Birmingham
Effects on sickness pattern of early mini-rehabilitation
groups among patients with musculoskeletal problems in primary healthcare Marklund B et al (1999) Scandinavian Journal of Occupational Therapy 6 (2) 90-94
Performance review of the North Kirklees MSK service 200809 Creaghan C (2009)
Rehabilitation in Musculoskeletal Diseases Hammond A (2008) Clinical Rheumatology Volume 22 Issue 3 435 ndash 449
Department of Health gateway Reference 17269