-
8/2/2019 Airway Nightmare
1/47
AIRWAY NIGHTMARE
YUSFADZRY YUSUF
-
8/2/2019 Airway Nightmare
2/47
INTRODUCTION
Breathlessness, shortness of breath, or dyspnea isa difficult
symptom for some patients to explainand quantify.
Tend to be subjective to some individual to furtherexplain.
It can be a natural consequence of strenuousphysical
exercise.
Physiological or pathological cause in origin
-
8/2/2019 Airway Nightmare
3/47
Defined as the sensation of uncomfortable breathing.
This breathing discomfort may reflect an increasedawareness of
breathing or the sense that breathing isdifferent, difficult or
inadequate.
Several factors may operate in an individual patientto produce
breathlessness.
The clinical analysis of the breathless patientcomprises both an
assessment of the severity ofbreathlessness and identification of
its cause.
INTRODUCTION cont..
-
8/2/2019 Airway Nightmare
4/47
Begin by assessing the patients stability.
If the patient unable to talk or complete a
full sentence without pausing for a deepbreath, move quickly to
stabilize thepatient.
Return to the interview after the patient ismore
comfortable.
-
8/2/2019 Airway Nightmare
5/47
Common cause ofbreathlessness
MINUTES HOURS DAYS-WEEKS
Pneumothorax Asthma Pleural
effusionPulmonaryembolism
Pneumonia AECOAD
Pulmonaryoedema
Pulmonaryoedema
Pneumonia
Acute asthma Metabolicacidosis
Pulmonary TB
-
8/2/2019 Airway Nightmare
6/47
Anaphylaxis 50% of patient will havedyspnea associated
withanaphylaxis
Aspiration Dyspnea due to aspirationgenerally begins
abruptlywithin hours of the event
Cardiac tamponade Tamponade is associatedwith dyspnea, chest
pain &lightheadedness
-
8/2/2019 Airway Nightmare
7/47
Acutepneumonia
Prevalence of pneumonia in healthypatient with acute cough
approx- 6-7%, higher in population withcomorbid illness
Respiratorymuscleweakness
40% patient with Guillain Barre syndwill requires assisted
ventilation d/tmuscle weakness
Spontaneous
pneumothorax
The lifetime risk in men is 12% for
heavy smoker &
-
8/2/2019 Airway Nightmare
8/47
Chronic dyspnea
Cardiac: cardiomyopathies, MI, primarypulmonary hypertension,
pericardial disease.
Pulmonary: Asthma, COPD, interstitial lung
disease, chronic pneumonia, chronic pulmonaryembolism, pulmonary
neoplasm (primary/mets),pleural effusions.
Miscellaneous: Anemia, neuromuscular disorder
Psychiatric: Panic attack, anxiety disorder
-
8/2/2019 Airway Nightmare
9/47
Need intubation?.....
-
8/2/2019 Airway Nightmare
10/47
AIRWAY ASSESSMENT
Outlines of Presentation
Anatomy Terminology
History
Physical Examination Management of Difficult Intubation
-
8/2/2019 Airway Nightmare
11/47
ANATOMY I- upperrespiratory system
-
8/2/2019 Airway Nightmare
12/47
ANATOMY II- Lowerrespiratory system
-
8/2/2019 Airway Nightmare
13/47
ANATOMY III- larynx
-
8/2/2019 Airway Nightmare
14/47
ANATOMY IV
-
8/2/2019 Airway Nightmare
15/47
TERMINOLOGY I
Difficult airway is said to occurWhen one experiences difficulty
with mask
ventilation, difficulty with tracheal intubationor both
Difficult mask ventilationWhen it is not possible for the
unassisted
anaesthesiologist to maintain the SpO2>90% using 100% oxygen
and positivepressure mask ventilation in a patient
-
8/2/2019 Airway Nightmare
16/47
TERMINOLOGY II
Difficult laryngoscopyWhen it is not possible to visualize any
portion
of the vocal cords with conventionallaryngoscope
Difficult endotracheal intubation
When proper insertion of the tracheal tube
with conventional laryngoscopy requires morethan 3 attempts or
more than 10 minutes
-
8/2/2019 Airway Nightmare
17/47
HISTORY I
Taking an adequate history isnecessary to anticipate
possible
complications.
-
8/2/2019 Airway Nightmare
18/47
HISTORY II
Condition that may associated with difficultairway included
Obesity Pregnancy and labour
Increased risk of laryngeal eodema in preeclamsia
Anatomical abnormalities
Microanathia Macroglossia
Congenital syndromes (eg: Pierre-Robin, Treacher-Collin)
Burn contracture involving the head and neck
-
8/2/2019 Airway Nightmare
19/47
Pierre Robin syndrome
Pierre Robin syndrome is a condition
present at birth marked by a very small
lower jaw (micrognathia).
The tongue tends to fall back and
downward (glossoptosis) and there is cleft
soft palate.
-
8/2/2019 Airway Nightmare
20/47
Treacher Collins Syndrome
Treacher Collins Syndrome, alsocalled mandibulofacial
dysostosis,affects the head and face.Characteristics include:
down-slanting eyes
notched lower eyelids
underdevelopment or absenceof cheekbones and the side walland
floor of the eye socket
lower jaw is often small andslanting
forward fair in the sideburnarea
underdeveloped, malformedand/or prominent ears
-
8/2/2019 Airway Nightmare
21/47
HISTORY III
Evidence of airway obstruction
Tumour or oedema involving upper airway
Large goitre
Acute epiglottitisMaxillofacial injury
Airways burns
Cervical spine problem
Fracture-dislocation or subluxation orcervical spine
Ankylosing spondylitis, rheumatoid arthritis
-
8/2/2019 Airway Nightmare
22/47
HISTORY IV
History of upper airway compromise duringsleep
History of radiotherapy head and neckregion
History of difficult intubation duringprevious anaesthetics
-
8/2/2019 Airway Nightmare
23/47
HISTORY V
Past Medical HistoryBronchiol Asthma
COPDElectrolytes imbalance
Myasthenia gravis
HPT
DM
Allergy HistoryDrugs/food
-
8/2/2019 Airway Nightmare
24/47
PHYSICAL EXAMINATION I
Body weight and general status
Expect difficulty in
obese patients (body weight > 90kg or >
20% above ideal weight)Pregnant ladies particularly those in
third
trimester of pregnancy
-
8/2/2019 Airway Nightmare
25/47
PHYSICAL EXAMINATION II
Inspection in anterior and lateralviews
Inspect the facial features for bony or
soft tissue abnormalities:Small receding chin,
Mandibular or maxillary fractures, tumourand oedema
xam ne e nec or swe ng go re
-
8/2/2019 Airway Nightmare
26/47
xam ne e nec or swe ng, go re,scarring, tracheal deviation
and
position of thyroid cartilage
-
8/2/2019 Airway Nightmare
27/47
Inspection in anterior and
-
8/2/2019 Airway Nightmare
28/47
Inspection in anterior andlateral views
Noted the pattern of respiration forpresence of stridor,
tachypnoea,
respiratory distress and paradoxicalrespiration.
-
8/2/2019 Airway Nightmare
29/47
PHYSICAL EXAMINATION III
Mouth Opening
Modified Mallampati Classification
Inter-incisor gap (expect difficulty if< 3cm) Any intra oral
cavity swelling:
Eg ; adenotonsillar hypertrophy.
Dentition
Protruding incisors, loose or missing teeth Orthodontic work
with cap, crown or dentures
Position of lower teeth in relation to upperteeth
-
8/2/2019 Airway Nightmare
30/47
PHYSICAL EXAMINATION IV
Neck Movement Neck movement-flexion,extension,rotation
Excluded cervical spondylosis- any pain in theneck, or
neurological symptoms in the arm
Thyromental distance- Should be > 6.5cm. Ifless expect
difficulty
Sternomental distance >12.5cm, If less,expect
difficulty
-
8/2/2019 Airway Nightmare
31/47
PHYSICAL EXAMINATION V
Indirect laryngscope
Relevant in laryngael tumour or thyroidenlargement scheduled for
surgery
Radiological examination Chest x-ray
Cervical x-ray
To look for fracture dislocation of cervicalspines
Modified Mallampati
-
8/2/2019 Airway Nightmare
32/47
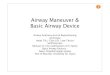
Modified MallampatiClassification
Mallampati reported a correlation between the visibility
oforopharyngeal structures and the degree of difficulty ofglottic
exposure on direct laryngoscope
Laryngoscopy was difficult in Class III and IV
The test is performed at the patients bedside with the
patientsitting up and the observer at eye level. The patient is
askedto open the mouth fully and protrude the tongue.
Visualization and identification of pharyngeal structures ismade
without phonation.
Modified Mallampati Classification
-
8/2/2019 Airway Nightmare
33/47
Modified Mallampati Classification
Class I: Soft palate, uvula,tonsillar pillars visibleClass II:
Soft palate, uvula visible, tonsillar pillars notvisible
Class III: Only soft palate visibleClass IV: No pharyngeal
structures except hard palate
visible
-
8/2/2019 Airway Nightmare
34/47
Cormack and LehaneClassification
Grade I Visualization of the entire laryngeal aperture Grade II
Visualization of the posterior portion of laryngeal
aperture Grade III Visualization of the tip of epiglottis Grade
IV Visualization of the soft palate only
In Grade III and IV, intubation is considered to be
difficult
-
8/2/2019 Airway Nightmare
35/47
MANAGEMENT
MANAGEMENT OF KNOWN DIFFICULTAIRWAY
Inform senior colleague, specialistin charge and discuss
optionsavailable for patient
Regional anaesthesia Local anaesthesia
GA with spontaneous respiration via facialmask or laryngeal mask
airway
-
8/2/2019 Airway Nightmare
36/47
MANAGEMENT
Ensure Empty Stomach anddecreased gastric acidity Implementation
of fasting guidelines
Use antacids or H2 receptor antagonist
Inform surgeon about Potential airway problem
Option of tracheostomy
-
8/2/2019 Airway Nightmare
37/47
MANAGEMENT
Difficult Intubation Equipment
should be checked and there arein good working order
Laryngoscopes of different
-
8/2/2019 Airway Nightmare
38/47
Laryngoscopes of differenttypes and sizes
ET tubes with various types
-
8/2/2019 Airway Nightmare
39/47
ET tubes with various typesand sizes
Stylet and gum elastic bougie
-
8/2/2019 Airway Nightmare
40/47
Stylet and gum elastic bougie
Laryngeal mask airway (LMA) of various
-
8/2/2019 Airway Nightmare
41/47
Laryngeal mask airway (LMA) of varioussizes, intubating LMA, LMA
Proseal,
Trachlight,
-
8/2/2019 Airway Nightmare
42/47
Ambu bag
Airway adjunct such as
-
8/2/2019 Airway Nightmare
43/47
Airway adjunct such as
oesohageal-tracheal Combitube,
laryngeal tube
Fibreoptic laryngoscope and its
accesories
Invasive means of airway:cricothyrotomy or minitracheostomy
-
8/2/2019 Airway Nightmare
44/47
MANAGEMENT
Preoxygenation with 100%oxygen for 3-5 minutes prior toinduction
of anaesthesia
Establish monitors consisting ECG, BP,pulse oximetry,
capnography,
-
8/2/2019 Airway Nightmare
45/47
MANAGEMENT
Ensure that the intubating conditionare optimal
Sniffing the morning air position
-
8/2/2019 Airway Nightmare
46/47
MANAGEMENT
Consider using alternativelaryngoscope blade andhandle
Macoy blade to retract the
epiglottis
Straight blade in patient withreceding chin, prominentincisors
or if epiglottis is long
and floppy
Short handle in a patient withshort neck and pendulousbreast
-
8/2/2019 Airway Nightmare
47/47
ThankYou..