Embed Size (px)
Citation preview
Airway and Breathing
ETAT Module 2
Adapted from Emergency Triage Assessment and Treatment (ETAT): Manual for Participants, World Health Organization, 2005

Learning Objectives
• Accurately determine whether or not a patient’s airway is patent and adequate.
• Accurately assess the effectiveness of the patient’s breathing (oxygenation and ventilation).
• Effectively perform maneuvers to relieve choking.
• Effectively position the patient to open the airway (with and without possible cervical spine injury).
• Give supplemental oxygen.
• Effectively provide bag mask ventilation with and without airway adjuncts.
Target Audience
• Healthcare providers in any facility who are likely to manage sick patients, including physicians, nurses, and assistants.
• Teachers and trainers for healthcare professionals

Airway
Breathing
Essential assessment questions
• Is the patient breathing?
• Is the airway obstructed? Partial or complete?
• Is the patient blue?
• Does the patient have severe respiratory distress?

AB
AIRWAY BREATHING
Any positive signs
• Not breathing
• Central cyanosis (blueness)
• Severe respiratory distress
Manage
• Open airway
• Give oxygen
• Keep patient warm
Airway and breathing: overview of assessment and management

Overview of airway and breathing
• Is the airway obstructed? Is the obstruction partial or complete? – Assessment: Is there a history of choking (as with foreign body)?
• Treatment: For complete obstruction, back slaps/chest thrusts or abdominal thrusts
• Position the airway – Treatment: Chin lift
– Assessment: Is there a history of neck injury? • Treatment: Jaw thrust rather than chin lift
• Is the patient breathing? – Assessment: Look, listen, and feel
• Treatment: Bag mask ventilation
• Does the child have severe respiratory distress or cyanosis (blueness)?
Is the airway obstructed?
• Is there a history of choking? • Sudden onset of symptoms.
• Associated with eating or foreign object in mouth.
• Is the obstruction complete?
• There is no sound, even though the child is appears to be coughing or choking.
• Is the obstruction partial?
• Audible crying, coughing, or choking.
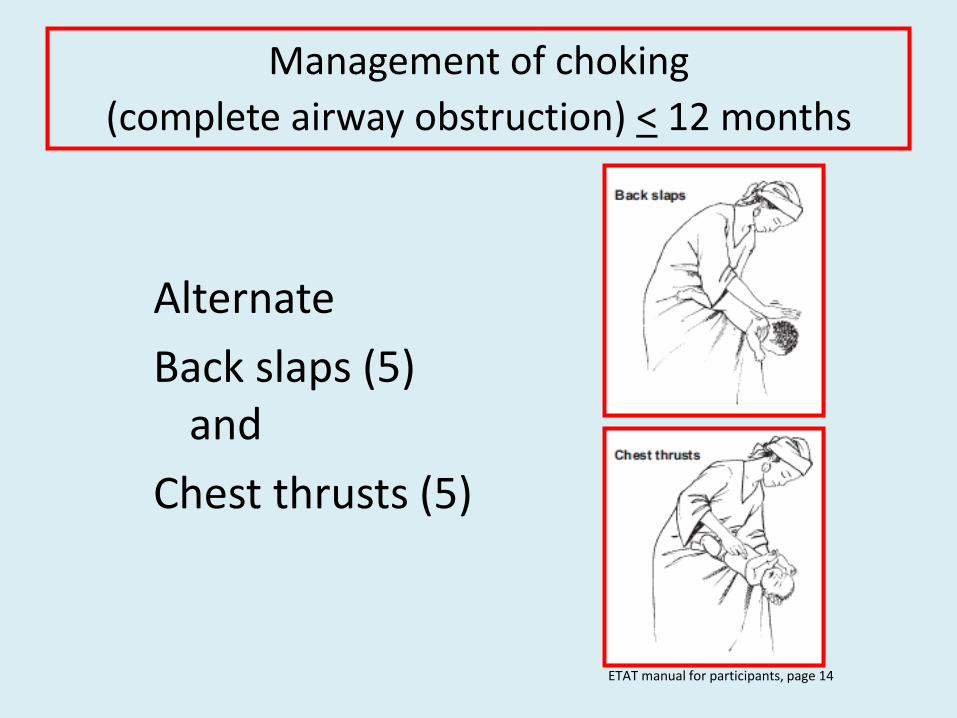
Management of choking
(complete airway obstruction) < 12 months
Alternate
Back slaps (5) and
Chest thrusts (5)
ETAT manual for participants, page 14

How to perform back slaps
• Lay infant on your arm or thigh with head down.
• Give 5 blows to back with heel of hand.
ETAT manual for participants, page 14

How to perform chest thrusts
• From the back slap position, turn the infant over, keeping the head down.
• With two fingers, perform 5 chest thrusts in the midline just below the nipple line.
Circulation 2005;112:IV-156

Back slap chest thrust sequence for choking child < 12 months
• Infant with a history of choking is not breathing. • Deliver 5 back thrusts. • Assess breathing. • Obstruction persists, deliver 5 chest thrusts. • Assess breathing. • Obstruction persists, check mouth and remove any visible
foreign body. • Assess breathing. • Obstruction persists. • Continue to deliver alternating back slaps and chest thrusts,
checking the mouth after each series of chest thrusts.
Demonstration
Choking manoeuveres for infants
< 12 months
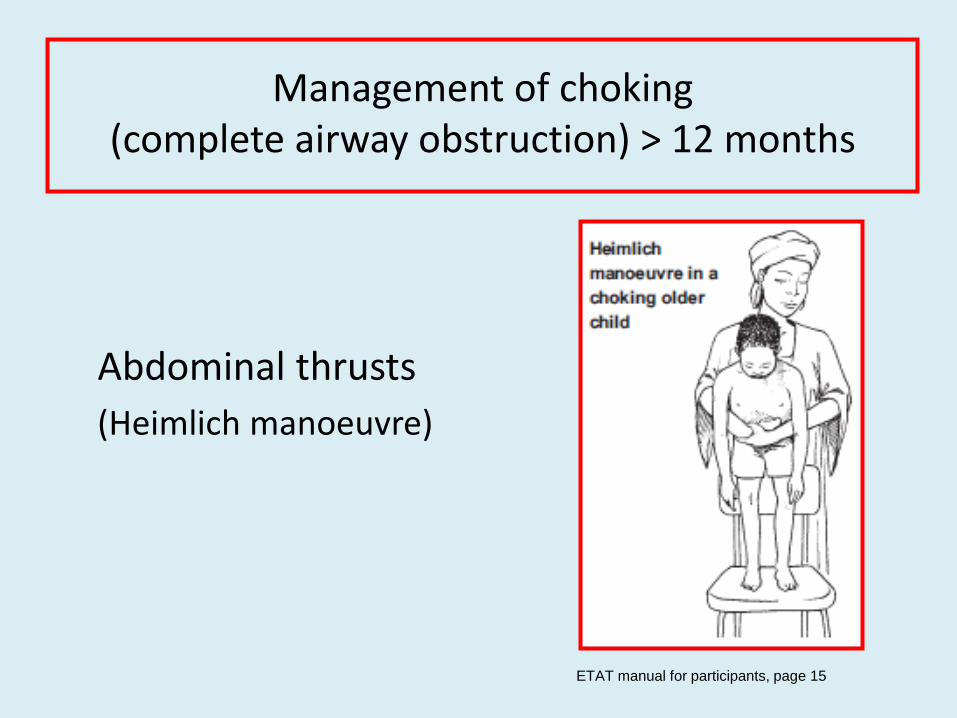
Management of choking
(complete airway obstruction) > 12 months
Abdominal thrusts
(Heimlich manoeuvre)
ETAT manual for participants, page 15

How to perform abdominal thrusts
• Go behind patient.
• Pass your arms around the patient’s body.
• Immediately below the patient’s sternum, make a fist with one hand and place the other hand over it.
• Pull inward and upward into the patient’s abdomen.
• Repeat this manoeuvere 5 times.
• If obstruction persists, check the patient’s mouth and remove visible obstructions.
www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18153.j

Demonstration
Choking manoeuveres for
children > 12 months

Positioning the airway
• The most common cause of upper airway obstruction is the tongue.
• Use chin lift for patients without concern for neck trauma.
ETAT manual for participants, page 15
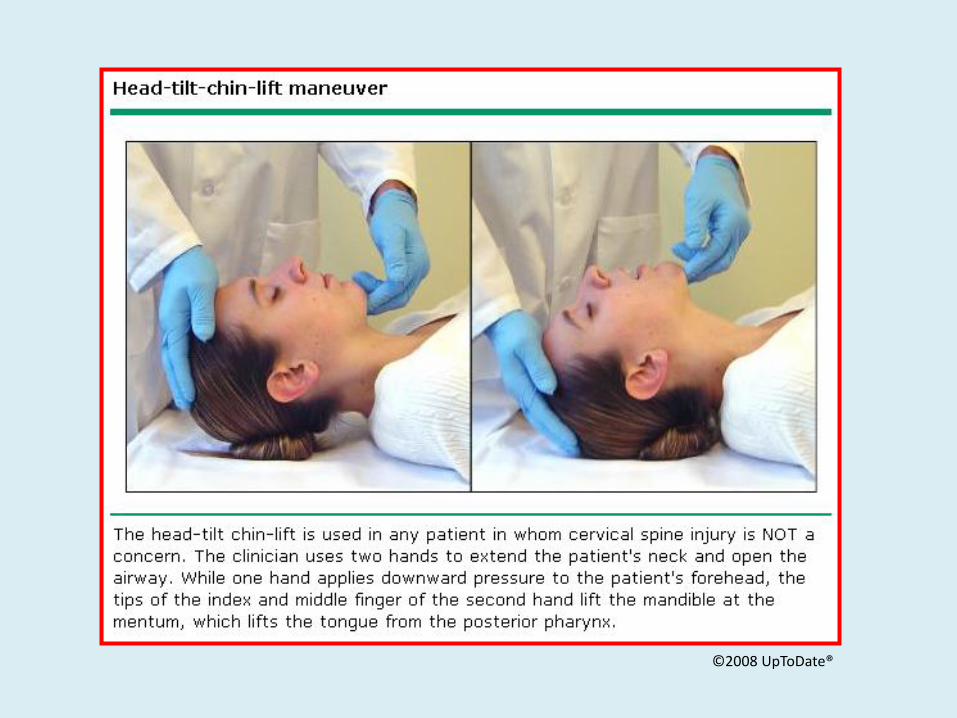
©2008 UpToDate®
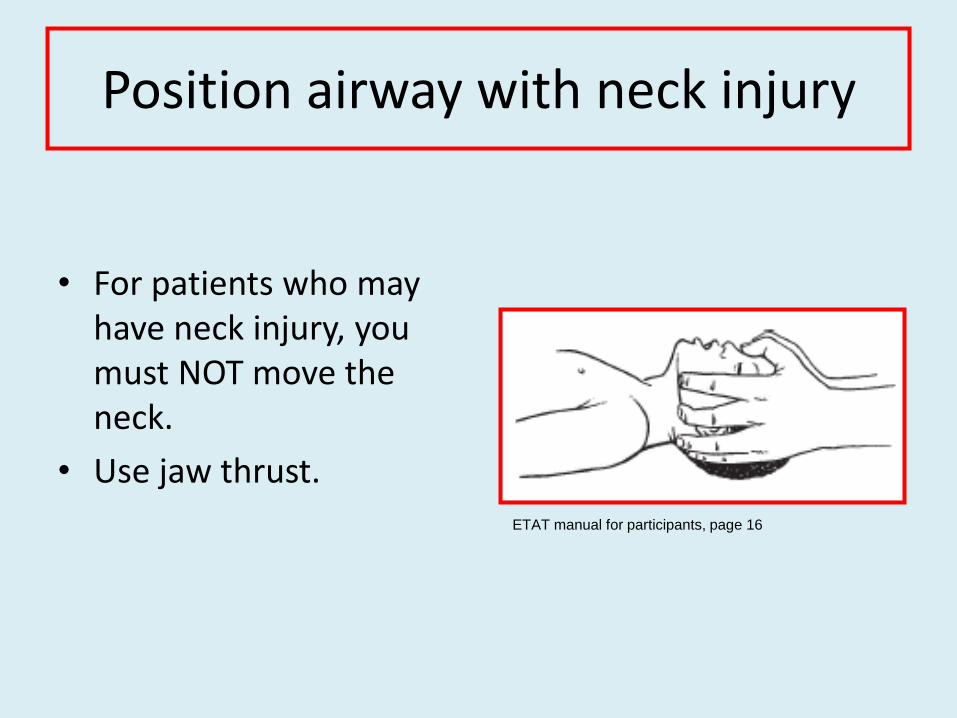
Position airway with neck injury
• For patients who may have neck injury, you must NOT move the neck.
• Use jaw thrust.
ETAT manual for participants, page 16
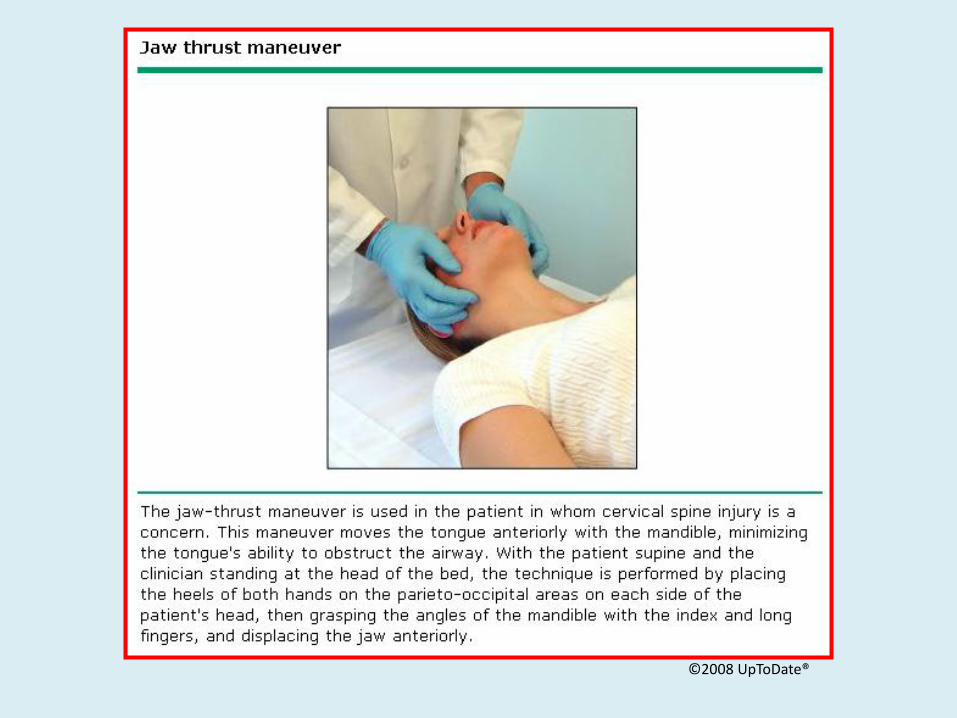
©2008 UpToDate®

Demonstration
Positioning the airway
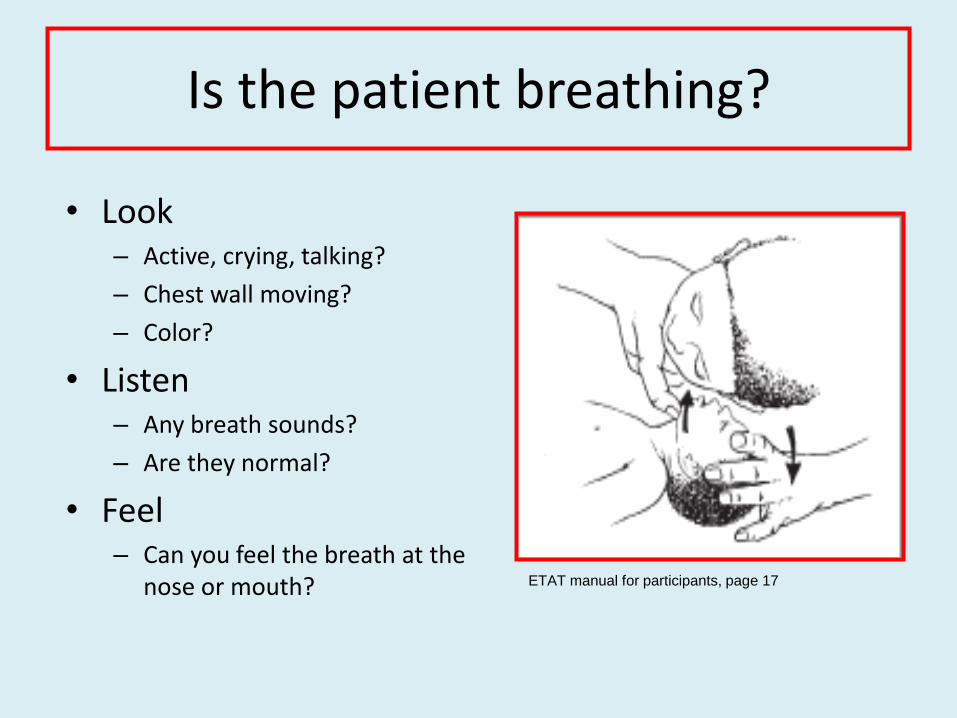
Is the patient breathing?
• Look – Active, crying, talking?
– Chest wall moving?
– Color?
• Listen – Any breath sounds?
– Are they normal?
• Feel – Can you feel the breath at the
nose or mouth? ETAT manual for participants, page 17

Is there increased work of breathing?
• Can child talk or nurse?
• Signs of distress
– Anxious
– Nasal flaring
– Indrawing of chest • Between the ribs
• Below the breast bone
PALS: Rapid Cardiopulmonary Assessment, American Heart Association 2001
What is the rate and pattern of breathing?
• Too fast
• Too slow
• Agonal breathing: irregular, slow
• Abnormal patterns – Deep, slow (as with acidosis)
– Irregular (as with brain abnormalities)
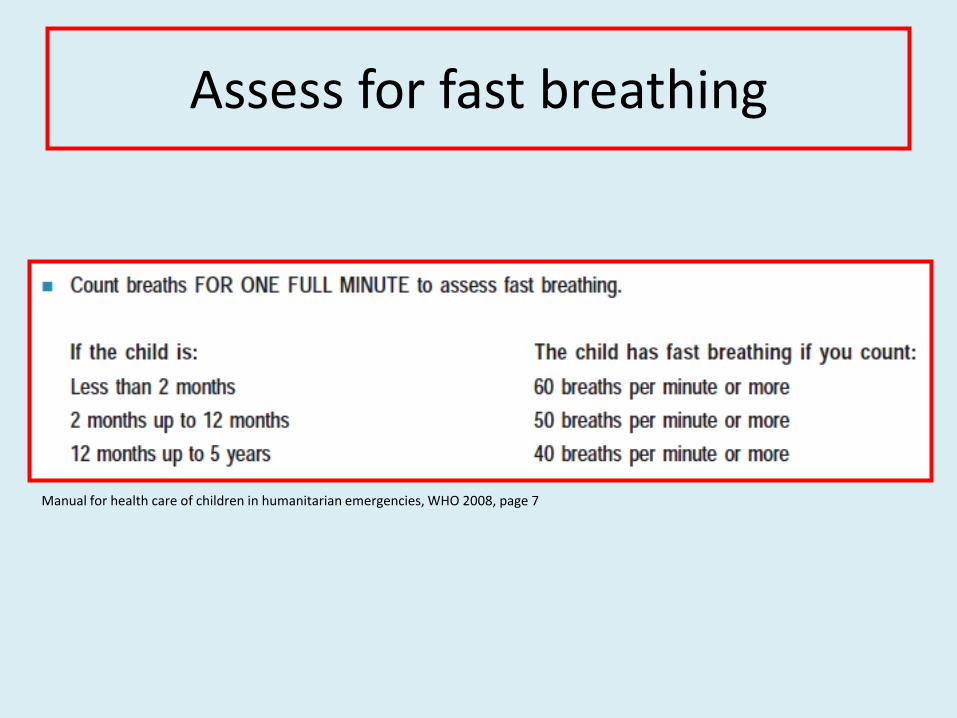
Assess for fast breathing
Manual for health care of children in humanitarian emergencies, WHO 2008, page 7

Are there abnormal sounds?
• Stridor: upper airway obstruction (foreign body, croup)
• Wheezing: lower airway obstruction (bronchospasm)
• Grunting: increased end expiratory pressure (pneumonia)

Who needs oxygen?
• Any patient with airway or breathing problems
• Patients with shock
• Children with severe anemia (< 5 gm Hb)
– They will not show cyanosis

www.cdc.gov/niosh/fire/images
Oxygen sources
Refillable cylinders Oxygen concentrator
• Portable • Require reliable oxygen source to refill • Flammable hazard
• Can supply 95% oxygen • Requires electricity • Requires maintenance

Oxygen delivery systems
• Nasal prongs
• Blow by
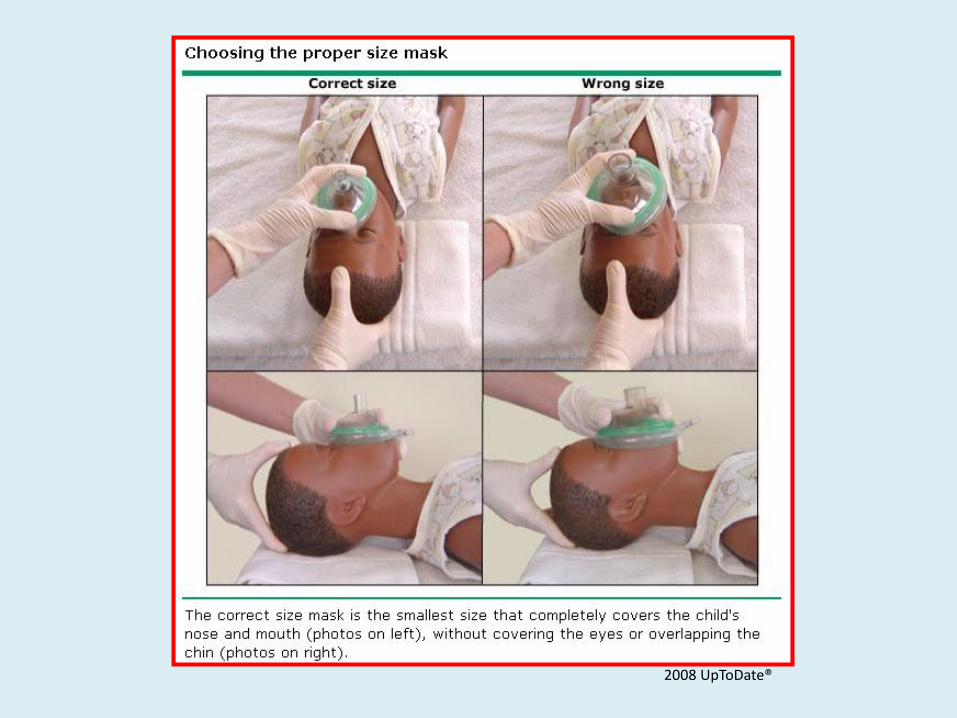
• Mask
– Simple
– Non-rebreather
ETAT manual for participants, page 21

Patient not breathing: needs ventilation
Bag Mask Ventilation
2008 UpToDate®
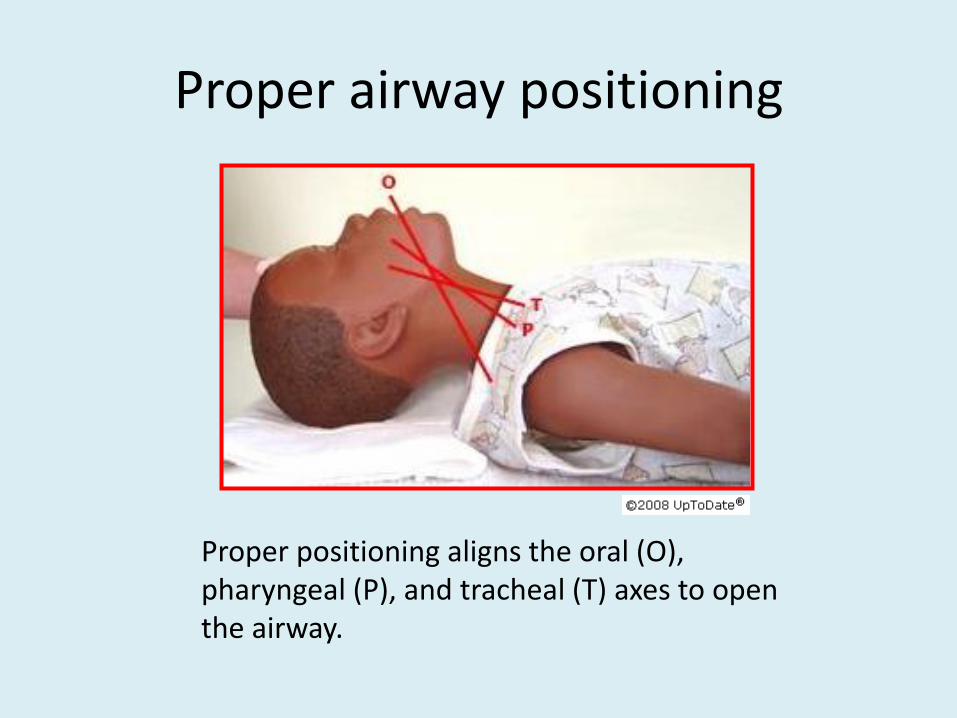
Proper airway positioning
Proper positioning aligns the oral (O), pharyngeal (P), and tracheal (T) axes to open the airway.
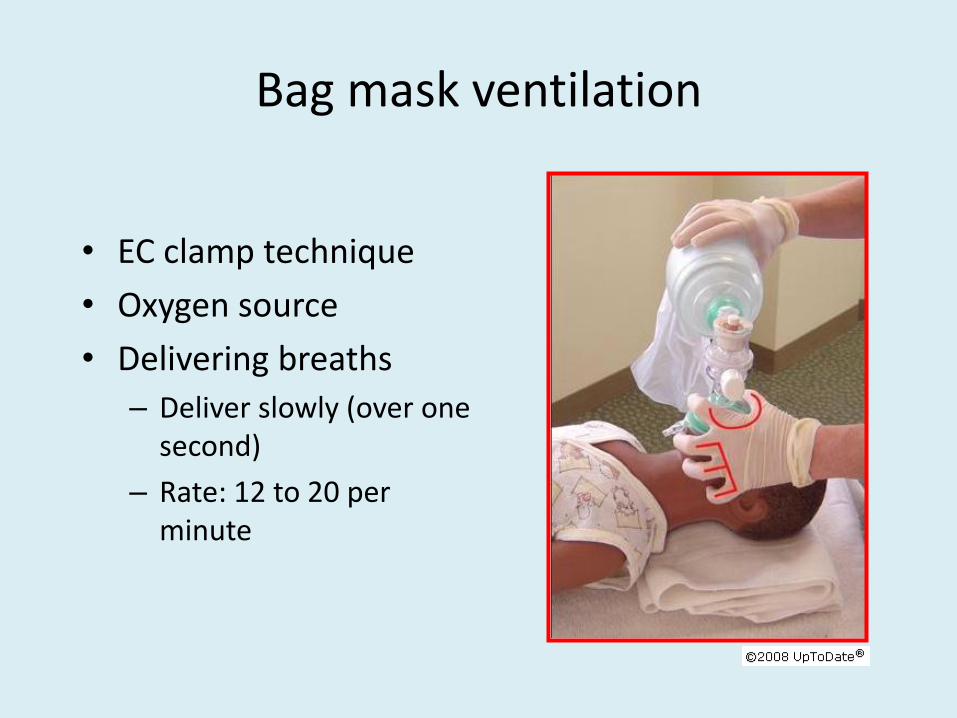
Bag mask ventilation
• EC clamp technique
• Oxygen source
• Delivering breaths
– Deliver slowly (over one second)
– Rate: 12 to 20 per minute

Airway adjuncts Oral airway Nasal airway
• Can only be used in unconscious patients. • Tongue can be inadvertently pushed into the hypopharynx, causing obstruction.
• Can be used for conscious patients.

Demonstration
Bag Mask Ventilation

When management resources are limited
• Use guidelines from Integrated Management of Childhood Illness (IMCI).
• IMCI chartbook uses the same assessment and classification principles as ETAT.
• Management recommendations emphasize recognizing patients that should be stabilized and transferred.

ABCD
• Severe disease OR
• Local bacterial infection
Positive sign
• Not feeding well OR
• Convulsion OR
• Rapid breathing OR
• Severe chest indrawing OR
• Fever OR low temperature
• Poorly responsive
Manage • Keep patient warm
(skin to skin)
• Give first dose of antibiotic
• Refer urgently to hospital
Assessment and classification: IMCI under 2 months
AB
AIRWAY BREATHING
Positive signs
• Cyanosis
• Chest indrawing
• Stridor at rest
Manage • Keep patient warm
• Give first dose of antibiotic
• Refer urgently to hospital
Airway and breathing: IMCI 2 months to 5 years

Summary
Obstructed airway
Not breathing
Hypoxia
Severe respiratory distress
Choking manoeuvers
Give oxygen
Give oxygen, Ventilate
Ventilate