Embed Size (px)
Citation preview

Agenda item 4aQuality & Clinical Governance Committee
The Trust Board received a report on the proceedings of a meeting of the Quality & ClinicalGovernance Committee. The Quality & Clinical Governance Committee considers specific caseswhere there have been problems in the care of a patient, and seeks to ensure that lessons arelearnt and service weaknesses addressed. To undertake this task effectively, the Quality &Clinical Governance Committee has to discuss cases in a level of detail that would potentiallyallow individual patients or members of staff to be identified. The Trust Board has concludedthat the publication of reports of the proceedings of the Quality & Clinical GovernanceCommittee would risk a breach of the confidentiality of a patient or a member of staff, andwould inhibit the free and frank provision of advice and exchange of views necessary for theGroup to undertake its duties effectively. In reaching this conclusion the Trust Board has takencognisance of the Data Protection Act 1998 and the Freedom of Information Act 2000, section36 (2).

1
Agenda Item 6
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
INFECTION PREVENTION & CONTROL
PURPOSE
To provide the Board with an update on the Trust’s performance in respect ofHealthcare Associated Infections.
DISCUSSION
C Difficile
In spite of an apparently improved outlook overt the last two months, C Difficile is stillone of the Trust’s most significant concerns. In the financial year to date, there havebeen 72 cases, as compared to 96 cases at the same time last year. This representsa 25% reduction, which is very a very marked change given the small variationbetween this year’s and last year’s totals in the year to date. As noted in January’sreport to the Board, however, this apparently significant improvement needs to beinterpreted with caution, for the following reasons:-
1. This is only the second month in which performance in the current year differsmarkedly from performance in the corresponding month in the previous year.
2. There were 21 cases in January 2011, which was an exceptionally highnumber, and there were 4 cases in January 2012.
3. There were 15 cases in February 2011, which again was a very high number,and there have been two cases in February 2012 to date.
4. The weather conditions this winter, taken as an average, have been milderthan last.
The Board is reminded that the target for 2012/13 is 60 cases. To achieve this targetrequires the Trust to have an average of no more than 5 cases each month. Nextyear, the financial penalties of failing to meet the target are extremely punishing,potentially leading to the imposition of a fine of £3m. The emphasis must thereforecontinue to be on implementing all relevant measures to ensure that the number ofcases is minimised. This includes implementing RCAs as soon as possible aftereach case and acting on the results, as well as maintaining all appropriate measuresimplemented to date.
Meticillin Resistant Staphylococcus Aureus (MRSA)
The target for 2011/12 is 3 cases. There have been 3 cases in the year to date. Thefirst occurred on 30th July 2011, the second on 9th November 2011 and the third on18th January 2012. In the first 2 cases, the patients had multiple risk factors and the

2
bacteraemias were judged clinically unavoidable. In the third case, the patient alsohad multiple risk factors, and whilst it does not raise issues about clinicalmanagement, it does raise issues about case management. The Medical andNursing Directors are seeing formally the consultant involved in the case. TheTrust’s target for 2012/13 is 1 clinically avoidable case. The Trust will aim to ensurethat no clinically avoidable cases occur in 2012/13 or beyond.
MRSA Screening
The objective is for the Trust to screen 100% of elective and non–elective patientsand this is consistently achieved.
Meticillin Sensitive Staphylococcus Aureus (MSSA)
Monitoring and reporting of MSSA in blood culture samples became mandatory on1st January 2011. In the year 2011/12 to date there have been 7 hospital associatedcases, with none so far in February 2012.
Preventive measures are the same as those required for protecting patients fromMRSA bacteraemia. No contractual performance measure for 2012/13 has yet beenagreed.
E.Coli Bacteraemia
E.Coli bacteraemia surveillance and reporting became mandatory from 1st June2011. No trajectories have been set for the current year, as monitoring has beenintroduced as an epidemiological measure. No Contractual Performance measurefor 2012/13 has yet been agreed.
All cases of MSSA, MRSA and E.Coli in blood cultures are subject to root causeanalysis investigation and the implementation of follow up actions as indicated.
RECOMMENDATION
The Board is asked to discuss and note the Trust’s performance and progressagainst the attached recovery plan.
Philip DylakDirector of Nursing and Infection Prevention & Control15th February 2012
3
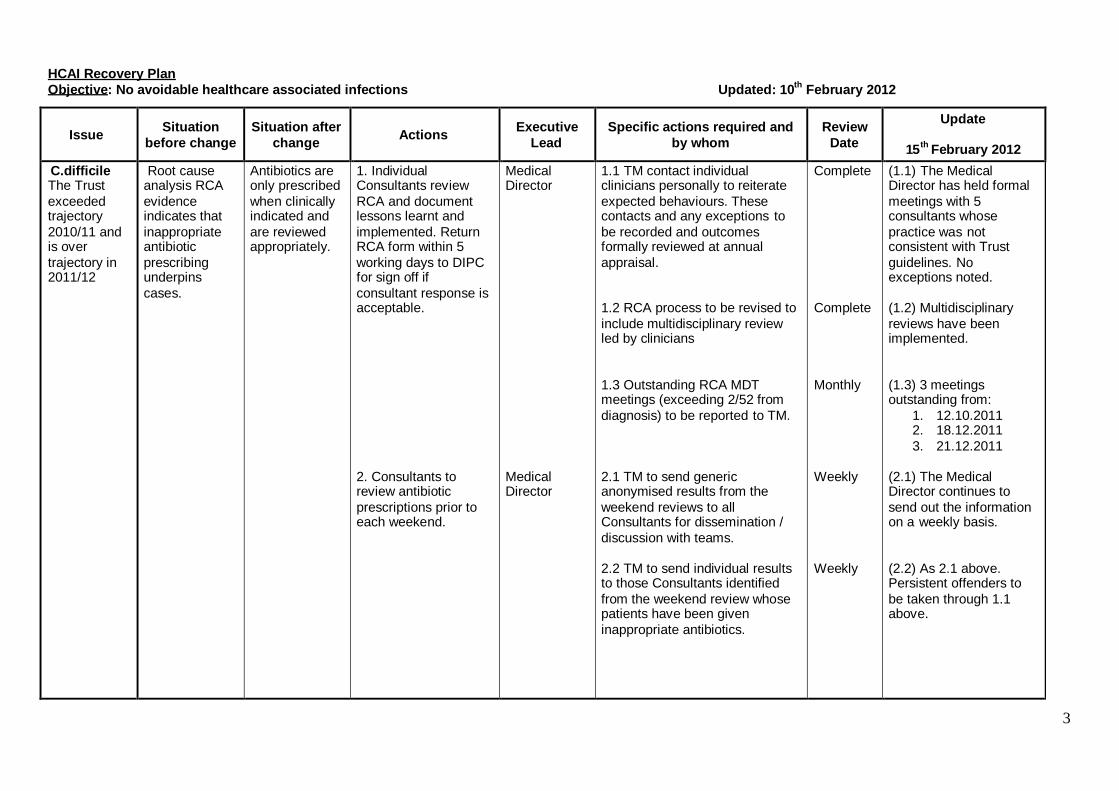
HCAI Recovery PlanObjective: No avoidable healthcare associated infections Updated: 10th February 2012
Issue Situationbefore change
Situation afterchange Actions Executive
LeadSpecific actions required and
by whomReview
Date
Update
15th February 2012
C.difficileThe Trustexceededtrajectory2010/11 andis overtrajectory in2011/12
Root causeanalysis RCAevidenceindicates thatinappropriateantibioticprescribingunderpinscases.
Antibiotics areonly prescribedwhen clinicallyindicated andare reviewedappropriately.
1. IndividualConsultants reviewRCA and documentlessons learnt andimplemented. ReturnRCA form within 5working days to DIPCfor sign off ifconsultant response isacceptable.
2. Consultants toreview antibioticprescriptions prior toeach weekend.
MedicalDirector
MedicalDirector
1.1 TM contact individualclinicians personally to reiterateexpected behaviours. Thesecontacts and any exceptions tobe recorded and outcomesformally reviewed at annualappraisal.
1.2 RCA process to be revised toinclude multidisciplinary reviewled by clinicians
1.3 Outstanding RCA MDTmeetings (exceeding 2/52 fromdiagnosis) to be reported to TM.
2.1 TM to send genericanonymised results from theweekend reviews to allConsultants for dissemination /discussion with teams.
2.2 TM to send individual resultsto those Consultants identifiedfrom the weekend review whosepatients have been giveninappropriate antibiotics.
Complete
Complete
Monthly
Weekly
Weekly
(1.1) The MedicalDirector has held formalmeetings with 5consultants whosepractice was notconsistent with Trustguidelines. Noexceptions noted.
(1.2) Multidisciplinaryreviews have beenimplemented.
(1.3) 3 meetingsoutstanding from:
1. 12.10.20112. 18.12.20113. 21.12.2011
(2.1) The MedicalDirector continues tosend out the informationon a weekly basis.
(2.2) As 2.1 above.Persistent offenders tobe taken through 1.1above.

4
3. Ensure seniormedical staff prescribein line with Trustguidance.
4. Nursing staff toinstigate Consultantreview if prescriptionexceeds 3 days.
MedicalDirector
MedicalDirector andAssociateMedicalDirectors
MedicalDirector
DIPC
3.1 TM to write policy documentto govern consultantperformance review anddescribing decision makingprocess for disciplinary action.
3.2 Antimicrobial ManagementTeam to review all prescriptionsexceeding 3 days following weekend review and report to TM. TMto record and report number ofinstances by Consultant.
3.3 TM, YS & KS to collectcontemporaneous evidence onAMT ward rounds.
3.4 Antibiotic pharmacists todesign an audit tool toencompass prescribing byConsultant, duration andindication in order thatprescribing in THFT is auditedusing a balanced approach.
4.1 DIPC instructioncommunicated to all wards.
Complete
On-going
Weekly
29th
February2012
Complete
(3.1) Policy reviewed30.11.2011.
(3.2) As 2.1 & 2.2 above.
(3.3) Medical Directorand Associate MedicalDirectors to accompanythe AMT on ward roundson a rota basis.
(3.4) Audit tool beingdrafted. 1st audit plannedfor February 2012.
(4.1) Nurses act as afailsafe to reminddoctors of the need toreview antibiotics.

5
5. Treatment protocolsfor top five presentingconditions in generalmedicine to bedeveloped.
6. Improve individualcase management toreduce transmissionby reducing severityand duration ofsymptoms and reducethe incidence ofrelapse caused byinappropriatelyprolonged treatment.
7. Update publishedclinical guideline forClostridium difficile.
MedicalDirector
MedicalDirector
DIPC
DIPC
5.1 TM to co-ordinatedevelopment of protocols for:
asymptomatic UTI, COPD cellulitis, diabetic foot ulcer pneumonia
5.2 The protocol for themanagement of diabetic footulcers to be extended to generalleg ulceration and to specificallydefine the limited role forsystemic antibiotics in this area.
6.1 YS & JD to develop ClinicalManagement Protocol forpatients with suspected/confirmed C.diff and auditcompliance.
7.1 JD review with Drs Ahmed,Shaath and Sacho
January2012
March2012
Complete
Complete
(5.1) Adopted by ClinicalCongress.Asymptomatic UTI,pneumonia and COPDcomplete.Cellulitis and diabeticfoot ulcer in progress.Also looking atOsteomyelitis as aseparate protocol. Auditson compliance to theprotocols are to beconducted.
(5.2) TM to liaise withclinician developing thediabetic foot ulcerguidance to extendaccordingly.
(6.1) ClinicalManagement Protocolimplemented 1st June2011.
(7.1) Updated guidancepublished on Intranet.

6
8. Seek additionalexternal advice.
9. Establish clinicaldialogue with primarycare colleagues.
DIPC &MedicalDirector
MedicalDirector
8.1 MD to contact wellperforming colleague Trust toobtain advice.
8.2 SHA HCAI lead to meet withMedical Director and DIPC
8.3 DIPC to contact InterimRegional Microbiologist (Dr EdKaczmarski) re investigating thebenefits of ribotyping.
9.1 Medical Director andAssociate Medical DirectorsAttend Clinical Congress Meeting
Complete
Complete
Complete
On-going
(8.1) Medical Directordiscussed successfactors and differencesin case managementwith Medical Directorfrom another Trust.Senior Infection Controlstaff also discussed theissue.
(8.2) Meeting held24.6.2011 on-goingsupport established.
(8.3) Meeting betweenDr Kaczmarski, DrSacho and lab staff tookplace on 06.12.2011.Concluded that theapproach will not have adirect bearing on theTrust’s approach as it ismore relevant tooutbreak situations, sono change made to theTrust’s plan.
(9.1) Meetings agreed.Additional meetingbetween keystakeholders (includinggeneral practitioners andhospital clinicians) tookplace on 3rd August andagreed joint workinginitiatives. The groupmet on 13th October and21st December todiscuss progress.

7
10. Initiate antibioticreview after leavingMAAU by thereceiving ward.
11. Addressinappropriateprescribing by juniordoctors
12. Implementadditional training formedical staff topromote adherence toantimicrobialprescribing policy andclinical managementprotocols.
DIPC
DIPC
DIPC
MedicalDirector
10.1 DIPC to liaise with ChiefPharmacist.
10.2 Lead pharmacist to arrangefor rapid (weekly) notification todivisions of an increase in theoverall prescribing levels withinthe Trust.
11.1 Infection Control team toidentify outliers and discuss andcorrect their practices with them.Lack of medical supervision of ajunior doctor / clinical team to behighlighted as a variable in theRCA and reported at WHE RCApanel.
12.1 AMD and infection controlteam to build training programmein liaison with undergraduate andpost graduate tutors. To reporton number (%) of eligible F1 / F2doctors who have receivedtraining on adherence to antimicrobial prescribing policy.
Ongoing
WeeklyandMonthly
Bi-monthly
Yearly(Newintake ofF1 DrseachAugust)
(10.1) Routine antibioticreview by receivingwards for all patients ontransfer.
(10.2) Lead pharmacisthas agreed a distributionprotocol with theinformation department.
(11.1) Incorporated intoRCA and individual casemanagement monitoring.
(12.1) F1 and F2 trainingestablished.24 Drs were eligible toattend training on20.07.2011 – 16 F1’s(67%) did attend.22 Drs were eligible toattend training on10.08.2011 – 21 (95%)did attend.Grand Round held on 4th
August – all grades ofstaff (23 attendees).11.12.2012 – 20 F1attendees out of apossible 23 (87%);C.difficile managementtraining.

8
13. Ensure no otherfactors may be at playin relation to the highC Diff rate.
14. Improve earlydiagnosis to facilitateprevention, andpossibly eliminatefalse positives
DIPC
DIPC
13.1 Infection control team toperform weekly checks at clinicallevel in relation to hand hygiene,environmental cleaning andpatient isolation, record andreport exceptions and remedialactions taken to DIPC for reviewat the Infection ControlCommittee. Exception reports tobe made available to thecommissioners.
14.1 Introduce 2 stage test for CDiff for trail period – move to fullimplementation if successful
14.2 Microbiology Laboratory tocomplete a 6 month audit /impact report of the 2 stage test.
14.3 KS and JD to strengthensystems enabling early riskassessment and samplecollection.
Ongoing
Complete
29th
February2012
Complete
Complete
(13.1) Routinemonitoring and “spotchecks” continue.Exception reportavailable for C. difficilecase (positive on23.11.2011).
(14.1) 2 stage testingcommenced 5th July asplanned. Evaluationreport submitted to theMedical Director andDIPC on 24.10.2011.2 stage test now fullyimplemented.
(14.2) 6 monthly Impactreport due February2012.
(14.3) Bed manager’sprotocol for GP referralupdated and circulated5th July.
JD and Manager MAU(Annmarie Daniels) havereviewed nursingassessmentdocumentation.Monitoring added to rootcause analysis process.

9
15. Reduce theincidence and impactof relapse.
16. Include andinvolve patients inantimicrobialstewardship
MedicalDirector
MedicalDirector
MedicalDirector
14.4 DIPC to enhance systemsfor early detection and monitoringof CDI sample collection.
15.1 Agree protocol to reduceinappropriate duplication oftesting in positive patients.
15.2 Monitor incidence andimpact of relapse / re-infection onoverall performance.
16.1 ICT/YS to develop patientheld Antibiotic Record to informclinicians when taking antibiotichistory and assessing risks priorto prescribing antimicrobialagents.
Complete
Ongoing
Complete
Monthly
2012/13
Trust screensaverdeveloped re stoolsample collection.
(14.4) DIPC and theAssistantDirector of Nursing metwith ward managers on04.11.11. Assessment ofpatients for symptomson admission agreed as14.3 above. Monthlymonitoring will be via theNW clinical indicators.
(15.1) Protocol agreedand implemented via ICTin hospital and TQuest(electronic laboratoryrequest system) for GPs.
Monitored on a dailybasis by the ICT.Relapse / re-infectioncases not repeat tested(within 3 month period).No relapse cases haveimpacted on Acute Trustperformance in year todate.
(16.1) Model identified.ICT to develop projectfurther.

10
17. Introduce a‘restrictive’ antibioticpolicy.
18. Review currentC.difficile processes,procedures anddocumentation takinginto account thealgorithm produced byRoyal Bolton Hospital.
MedicalDirector
DIPC &MedicalDirector
17.1 Consultant MedicalMicrobiologist and AntibioticPharmacist to change policy withan emphasis on the restriction ofAugmentin.
17.2 AMT / ICT to promote thechanges to all staff via displaystand at the Safety Day on 18th
November, on existing wardrounds, via ward pharmacist andleaflet / mail drops.
17.3 Pharmacy lead to send oute-mail to all clinicians / nurses rechanges to the policy.
18.1 IP/C Team to acquirealgorithm and review in line withour Trust procedures.
18.2 IP/C Team to update and reissue the Trust documentation forthe care and management of C.difficile patients.
18.3 Representatives from THFTto visit Bolton Hospital.
Complete
Complete
Complete
Complete
March2012
March2012
(17.1) Policy changedand uploaded onto theintranet.
(17.2) Policy changeswere promoted at theSafety Day. Ward ‘walkrounds’ and leafletdelivery took place onthe same day.
(17.3) E-mail sent on18.11.2011.
(18.1) Algorithm reviewcomplete.
(18.2) Updated Trustdocumentation to bedisseminated by 31st
March 2012.
(18.3) Visit arranged forFriday 9 th March 2012.
1
Agenda Item 7
Tameside Hospital NHS Foundation Trust
PERFORMANCE REPORT – FEBRUARY 2012
PURPOSE
To inform the Board of the Trust’s performance in respect of key national and localtargets and quality standards for the period ending January 2012.
DISCUSSION
Attached at Appendix A is the report which shows performance in month (and thepreceding months for 2011/12) for contractual performance targets and the Quality andHR metrics. This report includes a projection of performance to year end for eachindicator (along with the threshold required to meet the target).
Attached at Appendix B are the charts which show performance in graphical form forkey performance metrics.
Attached at Appendix C is the dashboard report which shows compliance with Monitortargets.
PERFORMANCE
Key Contractual Targets 2011/12 (Appendix A1)
The Trust is continuing to achieve the majority of the key performance targets in the2011/12 contract.
Although the Trust achieved the 62 day cancer target in December - with performanceof 89% (against the 85% threshold), the target was failed for Quarter 3 withperformance of 84.2%. This has resulted in the Trust attracting a further Monitorpenalty point for Quarter 3.
18 Week RTT Performance (Appendices B1 and B2)
For Admitted Patient Care 92.4% of patients were treated within 18 Weeks in January2012, which is above the operating standard of 90%. Similarly, the Trust achieved themaximum waiting time target of 95% within 23 weeks, with performance of 96.0%.
For Non Admitted Patient Care, it is anticipated that the 95% target will be met.Secondary validation is ongoing at the time of writing this report – but the actual positionwill be known by the Board meeting. A verbal update will therefore be provided.

2
Outpatient and Inpatient Service Performance (Appendix B3)
The Trust has set an internal target of a maximum waiting time of 5 weeks foroutpatients and 11 weeks for daycases/inpatients. The number of patients waiting over5 weeks for an outpatient target has decreased to 703 in January (from 996 inDecember). This is as a direct result of increased activity in January to make up for thereduced activity over the holiday period in December. For inpatient waiting lists, thenumber of patients waiting over 11 weeks has increased from 648 in December to 680in January. This is due to the fact that the Trust is continuing to tackle the longestwaiting patients (those over 18 weeks).
A&E Performance (Appendix B4)
As set out in the contract for 2011/12, the Trust needs to meet one of the patientexperience metrics, one of the timeliness metrics and both the 4 hour targets (foradmitted and non admitted patients) separately. Performance for January is detailedbelow:
Patient Experience: achieved (need to achieve at least 1 of these 2)
- Unplanned reattendances (at 7.0% against a threshold of 5%)- Patients left the department without being seen (at 3.6% against a threshold of
5%)
The Trust has undertaken a second audit of the reasons for patients returning to theEmergency Department within 7 days. Mental Health and Primary Care issues (e.g.dental pain, gout, chronic back pain) were responsible for 40% of re-attendances. Only4% of patients from the sample re-attended with the same issue that they originallypresented with. The Trust is clear that the issue can only be resolved on a healtheconomy basis and are pursuing the actions required through the Emergency CareNetwork Board.
Timeliness: achieved (need to achieve at least 1 of these 3)
- Total time in A&E under 4 hours (at 95.2% against a target of 95%)- Ambulance patients triaged within 15 minutes for 95th centile (at 15 minutes)- Median waiting time in the department for treatment of 60 minutes (at 96
minutes)
Process mapping of the 3 main streams through the Emergency Department isunderway to determine the opportunities for reducing the median waiting time.Improvement in the standard has been noted, which has been facilitated throughincreased utilisation of the REACT process within the majors stream. Work is nowongoing to increase the utilisation of this process and to enhance the time to be seen forpatients moving through the minors stream.
95% 4 hour target: failed (need to achieve both)

3
- Patients admitted within 4 hours (at 88.9% against a target of 95%)- Discharged patients seen within 4 hours (at 97.7% against a target of 95%)
The performance of the admitted patients stream is directly correlated to the significantissues experienced with delays to complex discharges and the corresponding impactupon bed availability. This issue was particularly pronounced in the first two weeks ofJanuary, when demand for inpatient capacity was significantly above the rate ofdischarges. The issue is being addressed on two main fronts:
- Analysis of medical bed capacity against demand has demonstrated a significantshortfall in capacity. The Trust is in discussions with the PCT with a view tosecuring recurrent funding for the required bed capacity as part of the 2012/13contract process.
- The National Emergency Care Intensive Support Team has recently facilitated anevent across the health economy with the objective of agreeing a strategy tosignificantly reduce the quantity of medically fit patients within the Trust.
Cancer Service Performance (Appendix B5)
In respect of two week waits, the Trust delivered performance of 98.4% in January forall urgent referrals for suspected cancer and 100% for symptomatic breast referralsagainst the 93% operating standard for both.
Reporting for the 31 and 62 day cancer treatment targets is done in arrears. ForDecember the Trust’s performance for the 31 day diagnosis to first definitive treatmenttarget was 98% (against an operating standard of 96%), 100% for thesecond/subsequent treatment for surgery (against a target of 94%) and 100% for thesecond/subsequent treatment for drug therapies (against a target of 98%).
In December, the Trust’s performance for the 62 day referral to treatment target was89% (against a standard of 85%), 100% for treatment following a referral from an NHSScreening Service (against a target of 90%) and 100% for the 62 day target for upgradeof urgency (against the target of 85%).
As previously noted, the Trust failed the Quarter 3 62 day cancer treatment target, withperformance at 84.2%. The transfer of patients requiring treatment at a tertiary centrewithin 42 days of referral is a key challenge to the Trust. A comprehensive action plan isbeing worked through, with particular attention being paid to the first 14 days fromreferral to ensure accurate diagnosis and the subsequent tracking of the patient throughtheir pathway, prior to transfer to the tertiary centre. To supplement this action plan, amember of the national Cancer Intensive Support Team was invited to review ourinternal processes and any recommendations made will be incorporated.
Diagnostics (Appendix B6)
There were 66 over 6 week waiters for Diagnostics in December. This equates to 2.2%of all diagnostic waits over 6 weeks. The reason for an increase in this target is the

4
inclusion of the 40 neurophysiology patients in January (now included in the cohort ofdiagnostic tests which must be under 6 weeks). Actions are being taken forward to clearall patients waiting over 6 weeks across all modalities by the end of March 2012.
Infection Control Performance (Appendix B7)
There was 1 new case of MRSA in January, 4 new cases of Clostridium Difficile, 0 newcases of MSSA and 4 of E-Coli. More detail is given in the substantive agenda item.
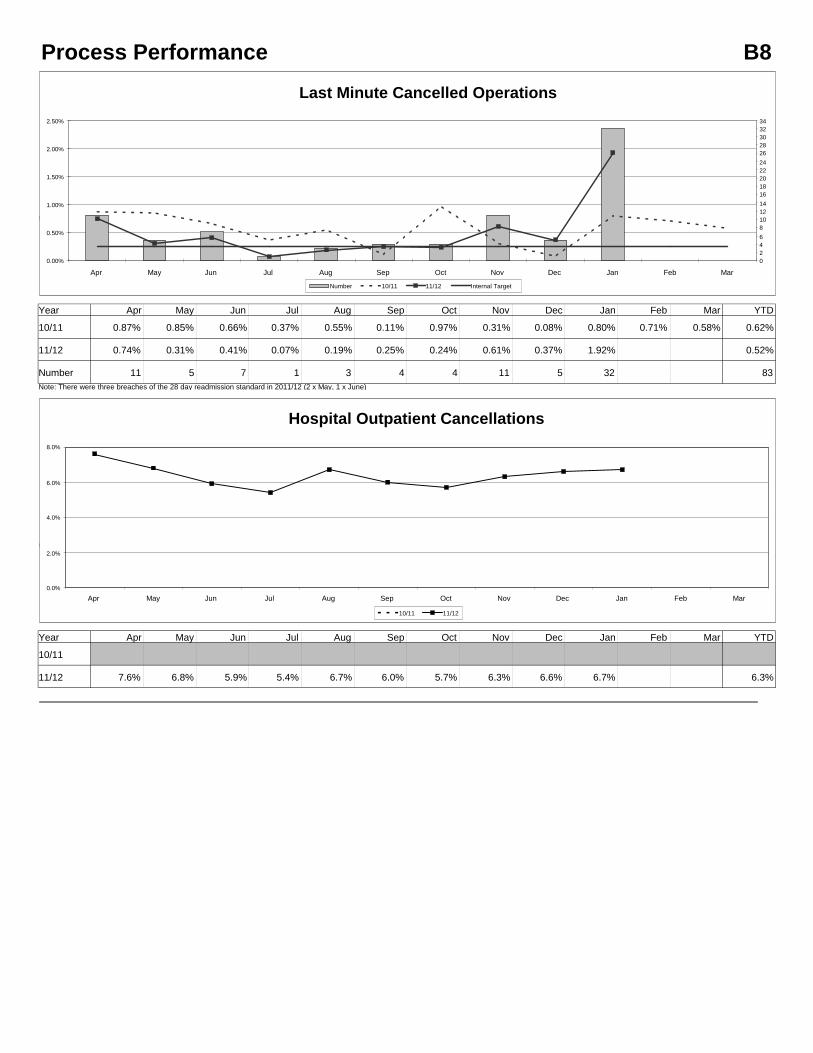
Process Performance (Appendix B8)
There were 32 last minute cancelled operations in January and hospital outpatientcancellations stood at 6.7%.
The high level of cancelled operations during January was as a result of bed capacitypressures, in particular the significant number of medically fit patients in the hospital.
CQUINs 2011/12
The key risks to securing maximum income through CQUIN performance are:
- The Urgent Care work – which is progressing well internally but reduction in theLength of Stay and utilisation of the new Ambulatory Care pathways is heavilydependent upon third parties. The assumed risk remains at £150k.
- As highlighted previously, the Trust has undertaken work to improve performanceagainst the patient experience metrics – but the results will not be known until theresults of the local and national surveys are received. The risk is still assumed tobe a loss of the CQUIN for the National Survery (£120k).
- The PCT has confirmed that, provided the Trust acheives the CQUIN target forquality of discharge summaries by the end of 2011/12, the full value of theCQUIN will be paid. It is anticipated that the 75% completeness target will beachieved which would result in payment of 40% against the CQUIN. (Anticipatedtotal loss of £145k).
- Other areas where the Trust has already failed to attract the maximum CQUINpayment include: End of Life (clinician training and patient discharges within 4hours), reduction in the number of falls, referrals to smoking cessation services,reduction in the number of caesarian sections. (metric under clinical dispute)
- Advancing Quality stretch targets, TARN (time for patient with trauma having aCT scan, and stroke (length of stay). These areas equate to a loss of circa £260kfor the year.
The Trust is anticipating achievement of approximatly 85% of the full value of theCQUINs and Quality Bonus Payment for 2012/13.

5
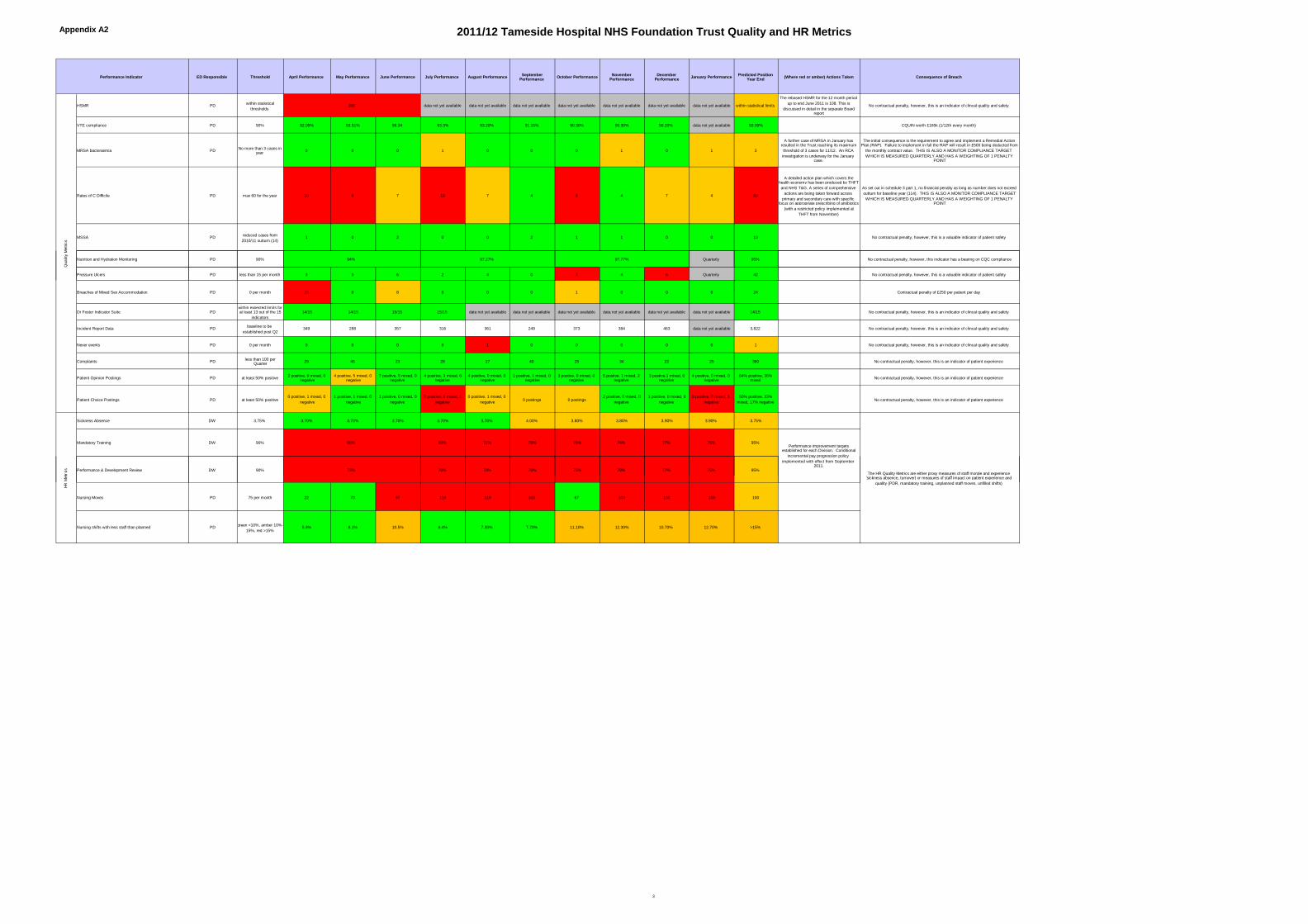
Quality Metrics (Appendix A2)
The Quality Metrics are included within the Integrated Performance Report at AppendixA2.
HR Metrics (Appendix A2)
Performance in relation to PDR and mandatory training has failed to improve in line withplan. The series of escalated actions agreed with Divisions to ensure performance hitsthe 95% target by the end of March are being closely monitored.
The number of nursing moves continues to be above target, as highlighted last month.This is largely due to the impact of ongoing capacity pressures with additional bedsopened.
Monitor Compliance (Appendix C)
Attached at Appendix C is the Monitor dashboard report. Due to the CQC warning letterand the failure of the 62 day cancer target for Quarter 3 the risk rating has risen to 6which means that the Trust has a red rating without the previous Monitor override.
RECOMMENDATION
Trust Board is asked to discuss and note the content of this report.
David Jago Paul WilliamsDirector of Finance Director of Clinical Services
15th February 2012

Appendix A1 2011/12 Tameside Hospital NHS Foundation Trust Contractual Performance Measures
Target Frequency of reporting Indicator Lead ED Responsible ThresholdApril
PerformanceMay Performance
JunePerformance
July PerformanceAugust
PerformanceSeptember
PerformanceOctober
PerfomanceNovember
PerformanceDecember
PerformanceJanuary
PerformanceYTD
Predicted YearEnd Position
Penalties in month Penalties Year to Date Actions Taken Consequence of Breach
MRSA bacteraemia Monthly PD PD No more than 3 cases in year 0 0 0 1 0 0 0 1 0 1 3 3
The initial consequence is the requirement to agree and implementa Remedial Action Plan (RAP). Failure to implement in full the RAPwill result in £500 being deducted from the monthly contract value.THIS IS ALSO A MONITOR COMPLIANCE TARGET WHICH ISMEASURED QUARTERLY AND HAS A WEIGHTING OF 1 POINT
Rates of C Difficile Monthly PD PD max 60 for the year 10 9 7 10 7 4 8 4 7 4 70 80
This target has a detailed action plan and is subject to a separate Boardreport. This continues to be monitored on a daily basis. Performance issignificantly improved in January 2012 (4 cases) compared to January
2011 (21 cases)
RTT - 95% of non admitted patients within 18.3 weeks Monthly LH/SA PW 18.3 weeks or below 18.0 18.0 18.0 18.0 18.0 18.0 18.0 18.0 18.0 18.0 18.0 18.0
RTT - 95% of admitted patients within 23 weeks Monthly SA/LH PW 23.0 weeks or below 23.0 21.9 21.3 21.8 22.6 22.0 22.9 19.8 20.0 21.5 n/a 19.0
RTT - 95% of incomplete pathways within 28 weeks Monthly SA/LH PW 28.0 weeks or below 29.3 33.7 26.1 25.8 25.3 24.5 23.2 23.4 23.4 24.7 n/a 23.0
RTT - median wait of 11.1 weeks for admitted patients Monthly SA/LH PW 11.1 weeks or below 9.4 9.3 9.1 9.0 9.0 9.4 10.3 8.9 8.5 9.2 n/a 9.0
RTT - median wait of 6.6 weeks for non admitted patients Monthly SA/LH PW 6.6 weeks or below 3.9 5.0 4.0 3.7 4.6 4.4 3.6 3.8 3.4 4.3 n/a 4.0
RTT - incomplete pathways - median wait of 7.2 weeks Monthly SA/LH PW 7.2 weeks or below 6.8 7.3 4.0 6.5 7.1 7.4 7.2 7.0 7.8 7.4 n/a 7.0
90% of admitted patients seen within 18 weeks Monthly SA/LH PW 90% 90.50% 93.10% 93.40% 93.30% 91.90% 91.90% 91.10% 94.10% 93.80% 92.30% n/a 93.00%
95% of non admitted patients seen within 18 weeks Monthly SA/LH PW 95% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% 95.00% n/a 95.00%
6 weeks maximum for diagnostic waits Monthly SA PW 0 190 110 81 60 148 9 5 6 8 66 n/a 0There is a plan in place to clear all over 6 week waiters by end March
2012
maximum 18 weeks for direct access audiology treatment (95%) Monthly SA PW 95% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
A&E - less than 5 % of reattandances within7 days Monthly LH PW Less than 5% 7.50% 7.80% 7.40% 8.00% 6.60% 7.30% 7.00% 7.10% 6.90% 7.00% 7.10% 7%Specific actions which span primary, community and secondary care are
being taken forward via the ECN as detailed in the Board report
A&E - 95% of patients seen, discharged within 4 hours Monthly LH PW 95% within 4 hours 98.10% 98.20% 98.50% 97.50% 98.50% 98.40% 97.60% 96.90% 95.90% 97.70% 97.70% 98.00%
A&E - 95% of patients seen, admitted within 4 hours Monthly LH PW 95% within 4 hours 92.50% 91.70% 93.10% 93.50% 92.30% 94.80% 93.60% 90.30% 87.90% 88.90% 91.80% 92.0%
The main issue affecting performance continues to be the high volume ofnon elective patients in the hospital - meaning that transfer of patients
from A&E into a bed is not able to take place in a sufficiently timely
fashion. The ongoing work to reduce medically fit delays continues to bethe main focus for the Trust with the PCT/CCG and TMBC
Total time spent in A&E department Monthly LH PW 95% within 4 hours 96.80% 96.70% 97.10% 96.50% 96.80% 97.50% 96.60% 95.30% 93.70% 95.20% 96.30% 96.50%
A&E - less than 5% of patients leaving the Department without being seen Monthly LH PW Less than 5% weekly 1.90% 0.90% 1.20% 5.80% 4.20% 5.00% 5.20% 4.40% 4.90% 3.60% 3.80% 4.00%
A&E - 95% of ambulance patients triaged (with pain score) within 15 minutes of arrival Monthly LH PW 95% within 15 minutes weekly 46 40 39 28 16 16 15 14 15 15 n/a 14 minutes
A&E - median waiitng time of 60 minutes from arrival to full assessment/treatment Monthly AG PW Median waiting time of 60 minutes monthly 89 83 88 118 99 110 115 115 115 96 n/a 60 minutesThe full implementation of the REACT model has now taken place,improvement and an improvement in performance can be seen in
January's reported position
Satisfaction of the Provider's obligations under the Ambulance Handover Plan Monthly LH PW25% in 15 minutes Q1, 45% Q2, 75% Q3,
95% Q484.00% 79.30% 80.10% 81.70% 84.80% 83.30% 82.40% 82.00% 76.40% 80.60% 81.80% 95.00%
Monthly withholiday of between 1% of monthly A&E contract value
with a quarterly reconiliation with 1% of actual A&E outturn value ofthe contract retained if annual performance is not met on the basisof achievement of ciompliance (all sums held returned if annualperfromance is met at year end)
% of patients seen within 2 weeks of an urgent GP referral for suspected cancer Monthly SA PW 93% 98.40% 96.90% 98.30% 97.70% 97.40% 96.10% 96.90% 95.90% 97.50% 98.40% 97.30% 98.00%
Proportion of Patients with breast symptoms where cancer not initially suspected referedto a specialist who are seen within two weeks of referral
Monthly SA PW 93% 97.50% 97.50% 96.00% 96.30% 95.30% 95.40% 94.00% 93.20% 97.40% 100.00% 96.30% 98.00%
Proportion of Patients receiving first definitive treatment for cancer within 62 days of anurgent GP referral for suspected cancer
Monthly SA PW 85% 92.30% 89.90% 87.20% 87.20% 92.00% 92.60% 85.30% 77.80% 89.00%
information notavailable until 62
days after themonth end
87.0% 85.0%
The Trust failed the 62 day cancer target for Q3 with 84.2% against atarget of 85% . In December a new reporting method came into force.
The Trust is redesigning cancer pathways and working with other Trustacross Greater Manchester to transfer patients requiring treatment at
anothet hospital within 42 days of initial diagnosis
Proportion of Patients receiving first definitive treatment for cancer within 62 days of
referral from an NHS Cancer Screening ServiceMonthly SA PW 90% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100% 100%
information notavailable until 62
days after themonth end
100.0% 100.0%
The initial consequence is the requirement to agree and implementa Remedial Action Plan (RAP). Failure to implement in full the RAPwill result in £500 being deducted from the monthly contract value.
THIS IS ALSO A MONITOR COMPLIANCE TARGET WHICH ISMEASURED QUARTERLY AND HAS A WEIGHTING OF 1 POINTEACH FOR THE 23 WEEKS ADMITTED AND 18.3 WEEKS NONADMITTED
The initial consequence is the requirement to agree and implementa Remedial Action Plan (RAP). Failure to implement in full the RAPwill result in £500 being deducted from the monthly contract value.
THE COMBINED A&E 98% TARGET IS ALSO A MONITORCOMPLIANCE TARGET WHICH HAS A WEIGHTING OF 1 POINT
The initial consequence is the requirement to agree and implementa Remedial Action Plan (RAP). Failure to implement in full the RAPwill result in £500 being deducted from the monthly contract value.
2% of the Actual Outturn Value of the service line revenue. THIS IS
ALSO A MONITOR COMPLIANCE TARGET WHICH ISMEASURED QUARTERLY AND HAS A WEIGHTING OF 1PENALTY POINT
2% of the Actual Outturn Value of the service line revenue. THIS ISALSO A MONITOR COMPLIANCE TARGET WHICH ISMEASURED QUARTERLY AND HAS A WEIGHTING OF 0.5
PENALTY POINT
1

Appendix A1 2011/12 Tameside Hospital NHS Foundation Trust Contractual Performance Measures
Target Frequency of reporting Indicator Lead ED Responsible ThresholdApril
PerformanceMay Performance
JunePerformance
July PerformanceAugust
PerformanceSeptember
PerformanceOctober
PerfomanceNovember
PerformanceDecember
PerformanceJanuary
PerformanceYTD
Predicted YearEnd Position
Penalties in month Penalties Year to Date Actions Taken Consequence of Breach
% of patients receiving first definitive treatment within one month of a cancer diagnosis(31 DAYS)
Monthly SA PW 96% 100.0% 97.8% 97.8% 95.2% 100.0% 100.0% 100.0% 100% 98%
information notavailable until 31
days after themonth end
98.9% 98.0%
2% of the Actual Outturn Value of the service line revenue. THIS ISALSO A MONITOR COMPLIANCE TARGET WHICH ISMEASURED QUARTERLY AND HAS A WEIGHTING OF 0.5PENALTY POINT
Proportion of Patients waiting no more than 31 days for second or subsequent cancertreatment - surgery
Monthly SA PW 94% 100.0% 100.0% 100.0% 90.0% 100.0% 100.0% 100.0% 100% 100%
information notavailable until 31
days after themonth end
99% 100%
Proportion of Patients waiting no more than 31 days for second or subsequent cancer
treatment - drug treatmentsMonthly SA PW 98% 100.0% 100.0% 100.0% 100.0% 100.0% 88.0% 100.0% 100% 100%
information notavailable until 31
days after themonth end
98% 98%
Proportion of patients referred to a Tertiary Centre on or before day 42 of the cancerpathway of care.
Monthly SA PW 85% 81% 81% 74% 85% 77% 85% 67% 64% 66% 52% 73% 85%The Trust continues to undertake an RCA for all delays in transfer of
patients post 42 days.No contractual penalty
Discharge summaries A&E, 90% within 2 working days Monthly TM PW 90% 83.5% 92.0% 97.8% 97.3% 97.7% 91.7% 95.2% 98.8% 98.5% 92.3% n/a 98.0%
For admitted patients, 90% of discharge summaries to be issued and sent within 3
working days.TM TM PW 90% 59.9% 77.7% 77.7% 74.0% 76.0% 85.5% 83.6% 83.0% 80.0% 82.1% n/a 90.0%
For outpatients, 90% of discharge summaries to be issued and sent within 5 workingdays.
TM TM PW 90% 68.6% 71.6% 73.5% 58.0% 62.8% 70.4% 83.6% 89.4% 85.5% 77.0% n/a 90.0%
Breaches of Mixed Sex Accommodation PD PD PD 0 per month 15 0 8 0 0 0 1 0 0 0 24 24 Financial penalty of £250 per patient per day
Provider cancellation of Elective Care operation for non-clinical reasons either before orafter Patient admission
Monthly SA PW 0 11 5 7 0 3 2 4 11 5 32 80 95The Trust continues to endeavour to ensure that patient cancellations are
minimised -high activity levels and associated bed pressures have
significantly affected the performance of this indicator in January.
No additional contract penalties (No payment for cancelledoperations initiated by Provider)
Provider cancellation of outpatient appointments Monthly SA/LH PWless than 3% of total new and follow up
attendances7.60% 6.80% 5.90% 5.40% 6.70% 6.00% 5.70% 6.30% 6.60% 6.70% 6.30% 6%
Major redesign of outpatient programme underway as part of the FinancialRecovery Plan
As per clause 32 (Performance Management) the initialconsequence is the requirement to agree and implement a RemedialAction Plan (RAP). Failure to implement in full the RAP, and subjectto there being no Excusing Notice or outstanding actions in the RAPon behalf of the Commissioner a sum of £500, shall be deducted
from the monthly contract value. The Commissioner, at its solediscretion, may also choose to issue an Exception report
As per clause 32 (Performance Management) the initialconsequence is the requirement to agree and implement a RemedialAction Plan (RAP). Failure to implement in full the RAP, and subject
to there being no Excusing Notice or outstanding actions in the RAPon behalf of the Commissioner a sum of £500, shall be deductedfrom the monthly contract value. The Commissioner, at its sole
discretion, may also choose to issue an Exception report
2% of the Actual Outturn Value of the service line revenue. THIS ISALSO A MONITOR COMPLIANCE TARGET WHICH IS
MEASURED QUARTERLY AND HAS A WEIGHTING OF 1PENALTY POINT
2
Appendix A2 2011/12 Tameside Hospital NHS Foundation Trust Quality and HR Metrics
ED Responsible Threshold April Performance May Performance June Performance July Performance August Performance SeptemberPerformance October Performance November
PerformanceDecember
Performance January Performance Predicted PositionYear End (Where red or amber) Actions Taken Consequence of Breach
HSMR PD within statisticalthresholds
data not yet available data not yet available data not yet available data not yet available data not yet available data not yet available data not yet available within statistical limits
The rebased HSMR for the 12 month periodup to end June 2011 is 108. This is
discussed in detail in the separate Boardreport
No contractual penalty, however, this is an indicator of clincal quality and safety
VTE compliance PD 90% 92.05% 93.51% 96.34 93.3% 93.20% 91.15% 90.30% 90.30% 90.20% data not yet available 93.00% CQUIN worth £165k (1/12th every month)
MRSA bacteraemia PD No more than 3 cases inyear 0 0 0 1 0 0 0 1 0 1 3
A further case of MRSA in January hasresulted in the Trust reaching its maximumthreshold of 3 cases for 11/12. An RCAinvestigation is underway for the January
case.
The initial consequence is the requirement to agree and implement a Remedial ActionPlan (RAP). Failure to implement in full the RAP will result in £500 being deducted from
the monthly contract value. THIS IS ALSO A MONITOR COMPLIANCE TARGETWHICH IS MEASURED QUARTERLY AND HAS A WEIGHTING OF 1 PENALTY
POINT
Rates of C Difficile PD max 60 for the year 10 9 7 10 7 4 8 4 7 4 80
A detailed action plan which covers thehealth economy has been produced by THFTand NHS T&G. A series of comprehensive
actions are being taken forward acrossprimary and secondary care with specific
focus on appropriate prescribing of antibiotics(with a restricted policy implemented at
THFT from November)
As set out in schedule 3 part 1, no financial penalty as long as number does not exceedoutturn for baseline year (114). THIS IS ALSO A MONITOR COMPLIANCE TARGETWHICH IS MEASURED QUARTERLY AND HAS A WEIGHTING OF 1 PENALTY
POINT
MSSA PD reduced cases from2010/11 outturn (14)
1 0 2 0 0 2 1 1 0 0 10 No contractual penalty, however, this is a valuable indicator of patient safety
Nutrition and Hydration Monitoring PD 90% Quarterly 95% No contractual penalty, however, this indicator has a bearing on CQC compliance
Performance Indicator
Qua
lity
Met
rics
108
94% 97.27% 97.77%
Pressure Ulcers PD less than 15 per month 3 3 6 2 4 0 7 4 6 Quarterly 42 No contractual penalty, however, this is a valuable indicator of patient safety
Breaches of Mixed Sex Accommodation PD 0 per month 15 0 8 0 0 0 1 0 0 0 24 Contractual penalty of £250 per patient per day
Dr Foster Indicator Suite PDwithin expected limits forat least 13 out of the 15
indicators14/15 14/15 15/15 15/15 data not yet available data not yet available data not yet available data not yet available data not yet available data not yet available 14/15 No contractual penalty, however, this is an indicator of clincal quality and safety
Incident Report Data PD baseline to beestablished post Q2
349 288 357 316 361 249 373 384 463 data not yet available 3,822 No contractual penalty, however, this is an indicator of clincal quality and safety
Never events PD 0 per month 0 0 0 0 1 0 0 0 0 0 1 No contractual penalty, however, this is an indicator of clincal quality and safety
Complaints PD less than 100 perQuarter 29 45 23 28 27 40 28 34 22 25 380 No contractual penalty, however, this is an indicator of patient experience
Patient Opinion Postings PD at least 50% positive 2 positive, 0 mixed, 0negative
4 positive, 5 mixed, 0negative
7 positive, 5 mixed, 0negative
4 positive, 3 mixed, 0negative
4 positive, 0 mixed, 0negative
1 positive, 1 mixed, 0negative
3 postive, 0 mixed, 0negative
5 postive, 1 mixed, 2negative
3 postive,1 mixed, 0negative
4 positive, 0 mixed, 0negative
64% positive, 36%mixed No contractual penalty, however, this is an indicator of patient experience
Patient Choice Postings PD at least 50% positive0 positive, 1 mixed, 0
negative1 positive, 1 mixed, 0
negative1 positive, 0 mixed, 0
negative0 positive, 0 mixed, 1
negative0 positive, 1 mixed, 0
negative 0 postings 0 postings2 positive, 0 mixed, 0
negative1 positive, 0 mixed, 0
negative0 positive, 0 mixed, 1
negative50% positive, 33%
mixed, 17% negative No contractual penalty, however, this is an indicator of patient experience
Sickness Absence DW 3.75% 3.70% 3.70% 3.70% 3.70% 3.70% 4.00% 3.80% 3.80% 3.90% 3.90% 3.75%
Mandatory Training DW 90% 60% 72% 76% 76% 74% 77% 75% 95%
Performance & Development Review DW 90% 70% 70% 70% 73% 78% 77% 75% 95%
HRM
etric
s
The HR Quality Metrics are either proxy measures of staff morale and experience(sickness absence, turnover) or measures of staff impact on patient experience and
60%
73%
Performance improvement targetsestablished for each Division. Conditional
incremental pay progression policyimplemented with effect from September
2011.
Nursing Moves PD 75 per month 22 70 97 119 119 103 67 103 130 158 100
Nursing shifts with less staff than planned PD green <10%, amber 10%-15%, red >15%
5.9% 8.1% 10.5% 6.4% 7.30% 7.70% 11.10% 12.30% 10.70% 12.70% >15%
HRM
etric
s
(sickness absence, turnover) or measures of staff impact on patient experience andquality (PDR, mandatory training, unplanned staff moves, unfilled shifts)
3

Appendix CTameside Hospital NHS Foundation TrustMonitor Performance Management Dashboard
Performance to 31 January 2011
MONITOR Service Performance: Governance Risk Rating December data for 3,4 and 5
Targets as per Compliance Framework January Penalty Points To DateWeight Met/Not Met Q1 Q2 Q3 Q4
National Indicators1 Infection Control: MRSA Bacteraemia 1.0 0.0 0.0 0.02 Infection Control: Clostridium Difficile Infections 1.0 O 1.0 1.0 1.03 Cancer: 31 Day Diagnosis to Treatment for First Definitive Treatment 0.5 0.0 0.0 0.04 Cancer: 31 Day Diagnosis to Treatment for Second or Subsequent Treatment 1.0 0.0 0.0 0.05 Cancer: 62 Days to Treatment from GP Urgent Referral O 0.0 0.0 1.0
Cancer: 62 Days to Treatment from Screening Service Referral 0.0 0.0 0.06 Cancer: Two Week Wait from GP Urgent Referral 0.0 0.0 0.0
Cancer: Two Week Wait from GP Symptomatic Breast Referral 0.0 0.0 0.07 RTT: 95th percentile for Non-Admitted Patients within 18.3 Weeks 1.0 0.0 0.0 0.08 RTT: 95th percentile for Admitted Patients within 23 Weeks 1.0 0.0 0.0 0.09 A&E: 95% Total Time in A&E Four Hours or Less (replaces all other A&E metrics) 1.0 0.0 0.0 0.010 Stroke Care: Stroke Indicator (construction to be confirmed) 0.5 n/a11 Learning Disabilities: Access to Healthcare 0.5 0.0 0.0 0.0
Third Parties1 CQC: Moderate Concerns 1.0 - 0.0 0.0 0.02 CQC: Major Concerns 2.0 - 0.0 0.0 0.03 CQC: Regulatory Action - Compliance 2.0 - 2.0 2.0 0.04 CQC: Regulatory Action - Enforcement 4.0 O 0.0 0.0 4.05 NHSLA: Minimum CNST Level 1 2.0 - 0.0 0.0 0.06 Mandatory Services: Failure / Risk of Failure to Deliver 4.0 - 0.0 0.0 0.0
Service Performance Score 3.0 3.0 6.00-0.5 Green; 1-1.5 Amber/Green; 2-3.5 Amber/Red; 4+ Red Amber/Red Amber/Red Red
Governance Risk Rating (Overriding Rules) RED RED RED
1.0
0.5


18 / 23 Week RTT Performance Appendix B1
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
11/12 95.0% 95.8% 96.0% 95.5% 95.3% 95.4% 95.0% 97.1% 96.6% 96.0% 95.8%Target 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 93.8% 94.7% 96.0% 94.6% 95.9% 93.7% 92.9% 87.1% 90.1% 90.6% 77.9% 78.8% 90.5%
11/12 90.6% 93.1% 93.4% 93.3% 91.9% 92.4% 91.1% 94.1% 93.7% 92.4% 92.6%
Target 0.90 0.90 0.90 0.90 0.90 0.90 0.90 0.90 0.90 0.90 0.90 0.90Within 18 3667 1483 1428 1657 1196 1440 2367 2571 2330 2538 2233 3298
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 96.5% 96.3% 96.1% 97.0% 96.5% 95.6% 95.5% 94.1% 95.4% 95.1% 95.0% 90.0% 95.3%
11/12 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.0% 95.2% 95.0% 95.0%Target 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95Within 18 3667 1483 1428 1657 1196 1440 2367 2571 2330 2538 2233 3298Over 18 0 40 78 136 93 247 438 542 649 764 647 285Total 3667 1523 1506 1793 1289 1687 2805 3113 2979 3302 2880 3583
18 Weeks RTTPercentage Seen within 18 Weeks - Admitted Patients
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Target
18 Weeks RTTPercentage Seen within 18 Weeks - Non Admitted Patients
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Target
23 Weeks RTTPercentage Seen within 23 Weeks - Admitted Patients
60%
70%
80%
90%
100%
Apr Ma Ju Jul Au Se Oc No De Ja Fe Ma
11/12 Target

Outpatient and Inpatient Service Performance B3
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 3,803 3,968 3,845 3,987 4,178 4,090 4,178 3,771 3,543 3,796 3,885 4,532 3,965 10/11 13 35 25 45 110 135 96 89 110 281 242 195 115
11/12 4,613 4,280 4,094 4,232 4,305 3,916 3,838 3,783 3,503 3,443 4,001 11/12 314 199 196 127 79 74 116 62 66 51 128
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 877 977 819 879 1,338 1,227 1,046 987 1,332 1,199 1,131 1,333 1,095 10/11 4.9 4.6 4.7 4.6 4.6 5.6 5.3 5.1 5.1 5.9 5.4 5.4 5.1
11/12 1,559 1,244 1,087 1,026 1,074 1,083 951 893 996 703 1,062 11/12 5.1 6.3 5.7 5.3 5.3 5.3 4.9 5.3 4.9 5.3 5.2
Note: During 2011/12 - 414 patients waited longer than the national 13 week guarantee (93 x April, 88 x May, 92 x June, 53 x July, 19 x August, 8 x September, 16 x October, 14 x November, 13 x December, 18 x January)
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 2,471 2,478 2,387 2,395 2,394 2,466 2,667 2,853 2,961 3,097 3,028 2,806 2,667 10/11 17 4 0 7 8 10 23 101 170 317 329 284 106
11/12 2,623 2,619 2,546 2,702 2,561 2,744 2,559 2,595 2,717 2,783 2,645 11/12 281 246 240 212 240 208 215 241 213 202 230
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 253 223 154 174 240 291 399 512 759 854 842 608 442 10/11 5.9 6.0 5.8 5.5 5.6 6.2 5.5 6.1 6.4 7.0 8.1 8.6 6.3
11/12 586 551 577 531 590 589 577 565 648 680 589 11/12 7.0 8.4 7.7 8.3 7.0 7.8 7.1 6.8 6.8 6.8 7.3
Note: During 2011/12 - 1389 patients waited longer than the national 26 week guarantee (152 x April, 177 x May, 168 x June, 116 x July, 139 x August, 119 x September, 122 x October, 128 x November, 139 x December, 129 x January)
Total (New) Outpatient Waiting List
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
5,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12
Outpatient Waits 11+ Weeks
0
50
100
150
200
250
300
350
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12
Outpatient Waits 5+ Weeks
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12
Outpatient Mean Waiting Times
0
2
4
6
8
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12
IP/DC Waits 20+ Weeks
0
50
100
150
200
250
300
350
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Num
ber
10/11 11/12
IP/DC 11+ Weeks
0
100
200
300
400
500
600
700
800
900
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Num
be
r
10/11 11/12
IP/DC Mean Waiting Times
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Num
be
r
10/11 11/12
Total Inpatient / Day Case Waiting List
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Num
ber
10/11 11/12

A&E Clinical Quality Indicators B4
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 97.9% 98.3% 98.6% 98.8% 98.1% 98.8% 97.9% 97.9% 95.9% 95.4% 96.3% 95.4% 98.7% 10/11 94.9% 95.0% 96.0% 97.2% 95.0% 96.1% 95.1% 94.8% 90.7% 87.5% 91.6% 90.6% 93.5%
11/12 96.8% 96.7% 97.1% 96.5% 96.8% 97.5% 96.9% 95.2% 93.7% 95.2% 96.4% 11/12 92.5% 91.7% 93.1% 93.5% 92.3% 94.8% 93.6% 90.3% 88.0% 88.9% 91.8%
Standard 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 Standard 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 98.8% 99.2% 99.3% 99.3% 99.0% 99.5% 98.9% 98.9% 97.8% 98.3% 98.2% 97.0% 98.7% 10/11 7.3% 7.0% 7.1% 7.9% 7.1% 6.7% 7.5% 7.1% 7.4% 7.5% 7.2% 7.7% 7.3%
11/12 98.1% 98.2% 98.5% 97.5% 98.5% 98.4% 97.6% 96.9% 96.0% 97.7% 97.7% 11/12 7.2% 7.4% 7.0% 8.0% 6.6% 7.3% 7.0% 7.1% 6.9% 7.0% 7.1%
Standard 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 Standard 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 10/11
11/12 2.2% 1.3% 1.7% 5.9% 4.2% 5.0% 5.2% 4.4% 4.9% 3.6% 3.8% 11/12 46 40 39 28 16 16 15 14 15 15
Standard 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 0.05 Standard 15 15 15 15 15 15 15 15 15 15 15 15
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 10/11
11/12 89 83 88 118 99 110 115 114 115 96 11/12 65.9% 72.2% 73.8% 70.3% 57.9% 79.9% 80.0% 83.1% 80.8% 81.2% 74.4%
Standard 60 60 60 60 60 60 60 60 60 60 60 60 Standard 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95 0.95
Under 4 Hour Waits in A&E
91.0%
92.0%
93.0%
94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Standard
Unplanned Reattendance Rate
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Standard
Total Time in A&E(Patients Admitted)
82.0%
84.0%
86.0%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Standard
Total Time in A&E(Patients Not Admitted)
92.0%
93.0%
94.0%
95.0%
96.0%
97.0%
98.0%
99.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Standard
Left Without Being Seen
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Standard
Initial Assessment Within 15 Minutes of Arrival (AmbulanceCases)
0
5
10
15
20
25
30
35
40
45
50
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Min
utes
10/11 11/12 Standard
Treatment Within 60 Minutes of Arrival
0
20
40
60
80
100
120
140
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Min
utes
10/11 11/12 Standard
Data Completeness - Treatment Times
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12 Standard

Cancer Service Performance - NHS Cancer Plan B5
September 2004 September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 94.3% 96.8% 96.3% 98.1% 99.1% 98.5% 99.4% 97.6% 96.7% 96.7% 96.0% 97.6% 96.0% 10/11 90.3% 98.8% 90.8% 93.1% 93.3% 98.5% 91.8% 94.2% 98.6% 90.2% 94.1% 96.4% 40.0%
11/12 98.4% 96.9% 98.3% 97.6% 97.3% 96.1% 96.9% 95.9% 97.5% 98.4% 97.3% 11/12 97.5% 97.5% 96.0% 96.3% 95.3% 95.4% 93.9% 93.2% 97.4% 100.0% 96.3%
Breaches 7 14 8 11 13 17 15 21 12 7 125 # Breaches 2 2 4 3 5 3 6 5 2 0 32
Threshold 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% Threshold 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
September 2004 September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 98.4% 97.3% 100.0% 100.0% 97.8% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 99.5% 10/11 77.8% 100.0% 100.0% 83.3% 92.9% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 97.5%
11/12 100.0% 97.8% 97.8% 95.2% 100.0% 100.0% 100.0% 100.0% 98.2% 98.9% 11/12 100.0% 100.0% 100.0% 90.0% 100.0% 100.0% 100.0% 100.0% 100.0% 98.5%
Breaches 0 1 1 2 0 0 0 0 1 5 # Breaches 0 0 0 1 0 0 0 0 0 1
Threshold 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% Threshold96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96%
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 10/11 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 81.8% 88.9% 100.0% 95.5%
11/12 92.3% 89.9% 87.2% 87.7% 92.0% 92.6% 85.3% 77.8% 89.0% 88.3% 11/12 100.0% 100.0% 100.0% 75.0% 100.0% 100.0% 100.0% 100.0% 100.0% 98.6%
Breaches 2.5 3.5 3.0 3.5 3.5 3.0 5.0 9.0 5.0 38.0 # Breaches 0.0 0.0 0.0 0.5 0.0 0.0 0.0 0.0 0.0 0.5
THFT /Shared
0 / 5 0 / 7 1 / 4 0 / 7 3 / 1 0 / 6 5 / 0 9 / 0 5 / 0 23 / 30THFT /Shared
0 / 0 0 / 0 0 / 0 0 / 1 0 / 0 0 / 0 0 / 0 0 / 0 0 / 0 0 / 1
Threshold 0.85 0.85 0.85 0.85 0.85 0.85 0.85 0.85 0.85 0.85 0.85 0.85 Threshold 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
Note: From January 2009 the 'Clock Rules' governing cancer waiting times were changedNote: From 01/11/2011 62 day breaches are automatically reallocated to referring trust if referred to Tertiary Centre after Day 42
Cancer: Two Week Waits (Standard 93%)
7
14
8
11
13
17
15
21
12
7
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
5
10
15
20
25
Breaches 10/11 11/12 Threshold
Cancer: 31 Days - Diagnosis to Treatment (Standard 96%)
0
1 1
2
0 0 0 0
1
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
1
2
3
4
5
6
7
8
9
10
Breaches 10/11 11/12 Threshold
Cancer: Two Week Waits: Symptomatic Breast(Standard 93%)
2 2
4
3
5
3
6
5
2
00.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
2
4
6
8
10
12
Breaches 10/11 11/12 Threshold
Cancer: 31 Days - Diagnosis to Start of Second / SubsequentTreatment (Standard 94% - 98%)
0 0 0
1
0 0 0 0 00.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar0
1
2
3
4
5
6
7
8
9
10
Breaches 10/11 11/12 Threshold
Cancer: 62 Days - Upgrade of Urgency (Standard 85%)
0.0 0.0 0.00.5
0.0 0.0 0.0 0.0 0.00.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
1
2
3
4
5
6
7
8
9
10
Breaches 10/11 11/12 Threshold
Cancer: 62 Days - Referral to Treatment (Standard 85%)
2.5
3.53.0
3.5 3.53.0
5.0
9.0
5.0
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
1
2
3
4
5
6
7
8
9
10
Breaches 10/11 11/12 Threshold

Diagnostic Service Performance B6
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 11 1 0 0 1 0 1 0 10 12 25 27 7
11/12 15 3 0 0 3 0 0 0 1 0 2
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Ave
10/11 415 322 122 104 111 254 217 233 260 190 151 127 209
11/12 190 110 81 60 148 9 5 6 8 66 68
Diagnostic Waits 13+ Weeks: Key Tests
0
5
10
15
20
25
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12
Diagnostic Waits 6+ Weeks: Key Tests
0
50
100
150
200
250
300
350
400
450
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12

Infection Control Performance B7
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 0 0 0 0 1 1 0 0 0 0 0 1 3
11/12 0 0 0 1 0 0 0 1 0 1 3
Trajectory 1 0 0 0 1 0 0 0 1 0 0 0 3
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 9 9 5 9 8 8 8 4 8 21 15 10 114
11/12 10 9 7 10 7 4 8 4 7 4 70
Trajectory 7 6 5 7 6 5 5 4 3 5 4 3 60
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
MSSA 1 0 2 0 0 2 1 1 0 0 7
E.Coli 0 4 3 3 5 2 5 1 2 4 29
MRSA Bacteraemia(Meticillin Resistant Staphylococcus Aureus)
0
2
4
6
8
10
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Month
Num
ber
10/11 11/12 Trajectory
Clostridium Difficile Infections
0
10
20
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Month
Num
ber
10/11 11/12 Trajectory
MSSA Bacteraemia and E. Coli(Meticillin Sensitive Staphylococcus Aureus and Escherichia Coli)
0
2
4
6
8
10
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Month
Num
ber
MSSA E.Coli
Process Performance B8
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11 0.87% 0.85% 0.66% 0.37% 0.55% 0.11% 0.97% 0.31% 0.08% 0.80% 0.71% 0.58% 0.62%
11/12 0.74% 0.31% 0.41% 0.07% 0.19% 0.25% 0.24% 0.61% 0.37% 1.92% 0.52%
Number 11 5 7 1 3 4 4 11 5 32 83Note: There were three breaches of the 28 day readmission standard in 2011/12 (2 x May, 1 x June)Internal Target 0.25% 0.25% 0.25% 0.25% 0.25% 0.25% 0.25% 0.25% 0.25% 0.25% 0.25% 0.25%
September 2004
Year Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
10/11
11/12 7.6% 6.8% 5.9% 5.4% 6.7% 6.0% 5.7% 6.3% 6.6% 6.7% 6.3%
Last Minute Cancelled Operations
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0246
8101214
1618202224
2628303234
Number 10/11 11/12 Internal Target
Hospital Outpatient Cancellations
0.0%
2.0%
4.0%
6.0%
8.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
10/11 11/12

1
Agenda item 8
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
FINANCE AND ACTIVITY REPORT
JANUARY 2011
PURPOSE
The purpose of this report is to advise the Board on the financial position of the Trustand overall activity levels for the period ending 31st January 2011.
DISCUSSION
This report reflects a revised format in order to communicate key messages moreclearly. The graphs have been populated with future month’s plans, but these maychange as CIPs are posted.
In month the table below and the attached Appendix A, have been amended to takeout restructuring costs from the normalised surplus/deficit reported position.
Summary Position
Key Financial Metrics: Month 10
CurrentMonth Plan
£000
CurrentMonthActual£000
CurrentMonth
Variance£000
YTD Plan
£000
YTD Actual
£000
YTDVariance
£000
FY Plan
£000
ForecastOutturn
£000
Income 12,220 12,908 688 116,659 118,500 1,840 140,578 142,784Expenditure (10,895) (11,593) (697) (113,531) (114,151) (621) (135,667) (137,396)EBITDA 1,325 1,315 (9) 3,129 4,348 1,220 4,912 5,388Financing (841) (796) 45 (8,171) (8,343) (173) (9,834) (10164)Exceptional Items 0 228 228 (2,633) (2,235) 398 (3,914) (3,744)Net (Deficit) Surplus 484 747 263 (7,675) (6,230) 1,445 (8,837) (8,520)Exceptional Items 0 (228) 228 (2,633) (2,235) 398 (3,914) (3,744)Normalised(Deficit)Surplus
484 519 35 (5,042) (3,995) 1,047 (4,923) (4,776)
Overall Financial RiskRating(FRR)
2 2 - 2 2
Capital expenditure 90 80 10 3,060 2,319 742 3,993 3,328Cash 1,608 9,407 7,799 226 6,990CIP 1,371 1,241 (129) 6,641 6,851 210 9,395 9,395
In January the Trust is reporting a net normalised surplus of £519k, against aplanned surplus of £484k, resulting in the Trust being ahead of plan by £35k in themonth. Cumulatively at the end of January the reported deficit position is £3,995k.This continues to be an improved position on plan at month 10 by some £1,047k.
This position results in the Trust having an overall financial risk rating (FRR) of 2,which is in line with the plan set of 2.

2
Income
In the month of January clinical income has over-performed by £709k, materiallydriven by over-performance on other income (£257k), non-elective in patients(£162k) elective in patients (£157k), and outpatients (£140k), offset by under-performance on A&E (£9k). (Table 1 below). In the month of January, contractincome was above plan by £475k, as detailed on Appendix G, which means thatthere has been a £234k gain on income relating to activity in previous months. Itshould be noted that the December activity was only 75% coded as previouslyreported and as such there have been gains on the fully coded data.
Actual performance against the Trusts income plan by point of delivery and bycommissioner is detailed in Appendices C1 and G.
Table 1:- NHS Clinical Income
Elective activity is below plan by 14 spells in January, with an associated incomeloss of £10k in the period. (Table 2 below). Elective inpatient income is down onplan by £92k, excess bed day by £4k, offset by day cases being ahead of plan by£86k. Elective inpatient activity is down on plan by 55 spells, offset by an over-performance on day cases by 41 spells. It should be noted that eight operationswere cancelled in the month due to a lack of beds, which will reduce the levels ofelective income.
Within the in month position Trauma & Orthopaedics is behind plan by £49k,Gynaecology is also below plan by £42k, whilst General Medicine is ahead of planby £29k.

3
Table 2: - Elective Activity
Non-elective activity has under-performed by 27 spells in the period. (Table 3below). It has over-performed by 559 spells year to date, with an associated incomeunder-performance in the period of £65k once the threshold and re-admissionsadjustments are taken into account (detailed in Table 5). This is materially due tounder-performance in the period on non-elective excess bed day’s of £92k, non-elective admissions of £38k, offset by over-performance on critical care of £64k.However, within this General Medicine has under-performed by £282k, and GeneralSurgery £37k. This is offset by an over-performance in Paediatrics of £75k, with theother main offset being against the threshold and re-admissions.
Table 3: - Non-Elective Activity

4
Outpatient activity is ahead of plan by 971 attendances in January equating to anover-performance against the income plan of £89k in the period. (Table 4 below).First attendances have under-achieved plan by £31k, whilst follow up activity hasover-performed by £40k and outpatient procedures by £80k.
Across all points of delivery both the Emergency Division £172k (0.4%) and ElectiveServices Division £970k (3.0%) are over achieving against their income targets yearto date (excluding non-recurrent funding, threshold and re-admissionslosses).However, Women and Children’s are below plan by £694k (4.1%) year todate (detailed in Appendix G). This is materially driven by under performance onObstetrics £379k, Gynaecology £351k, and Neonatal critical care £137k.
The over-performance against other income relates mainly to £273k of income whichrelates to bids submitted and approved by NHS Tameside & Glossop.
Accident and Emergency attendances are below plan by 308 attendances in theperiod and this equates to income being below planned levels by £22k.
Table 4: - Outpatient Activity including Outpatient Procedures
Table 5 below summarises the cumulative impact of the non-elective threshold andre-admission penalties on the Trusts income plan.
Table 5: Non Elective Activity; Threshold and Re-Admissions Penalties
Annual EstimatedImpact
CumulativeM10Estimated Impact
Cumulative M10Actual Penalty Applied
Variance
£’000 £’000 £’000 £’000EL Readmissions -340 -282 -171 111NEL Readmissions -755 -626 -275 351NEL threshold -1,073 -1,062 -1,482 -420Total -2,168 -1,970 -1,928 42
Over performance against the 2008/09 outturn levels as previously reported ispayable at 30% of tariff. It should be noted that in November the threshold value fell

5
as a result of the activity on the short stay admissions unit coming out of thethreshold as it is no longer being paid for under PbR. Cumulatively to January theTrust “lost” £1,482k of income on this basis as activity was in excess of the thresholdagainst a planned loss of £1,062k resulting in a downside of a further £420k. This ishowever an improvement on the December position by some £56k.
Table 5 details the ongoing contract penalties. It should be noted however, that thedata in the above table excludes any penalties for re-admissions to other hospitals.
The income for CQUIN at month 9 reflects the achievement of 82% (£1,258k) of thetotal 1.5% planned value year to date. The income for Quality Bonus Payment (QBP)has been reduced from 93% last month to 87.4% (£1,986k) of plan to reflect latestestimates of performance.
PFI transitional income is below plan by £137k in month and £1,287k year to date.As previously reported this under-performance against plan is matched by under-spends on PFI pay and non-pay.
Expenditure
Operating expenses are above plan by £697k in January, £621k year to date(Appendix D & F).
Pay is above plan by £486k in the month, £278k year to date. (Table 6 below). TheTrust would expect to be overspent in the period by circa £270k, to reflect the bidsfunded by the PCT, as this is covered by other income being above plan. In additionthe pay CIP has under-achieved in the period by £133k, and as such the Trust wouldexpect to be above plan by £403k. Pay expenditure in the period has risen to £8mcompared with the December spend of £7.75m
Medical pay has over spent by £62k in the period. The underlying expenditure onmedical staff in January (£2,546k) is slightly above average levels to date (£2,532),but is against a reducing budget in order to deliver CIP. In month the medical CIPplanned target across all work streams was £334k, and the Trust has delivered£384k against the plan. The key issues driving this level of performance arediscussed in more detail in Appendix H.
Cumulatively, medical pay has under-spent by £446k, of which £578k is due tobelow planned use of the WLI reserve up to month 05, reflecting improvedproductivity. CIP has also contributed to the under spend as £561k has been postedagainst medical staffing over the levels planned, with £541k being derived from VATsavings on medical agency staff due to the reduced levels of agency use, comparedto 2010/11. However, these areas of over-performance are off set by overspends inEmergency Services of £865k, of which £286k relates to A&E, and overspends inElective Services of £283k. These overspends are due partially to the use of agencymedical staff.
Nursing has overspent by £457k in the period, £1,831k year to date. Actualexpenditure on nursing has increased by £120k on levels in December, mainly dueto increased expenditure on payroll of £49k, agency staff of £41k and bank staff of£30k. The current overspend has been driven by the cost of opening escalation bedswith £100k being incurred in January, £1,117k year to date. In January an additional32 escalation beds have been open on average across the month, equating to 984

6
bed days, compared with 22 in December. The Trust would expect to be overspenton nursing by a further £178k in the month, as this is matched by additional fundingfrom the PCT.
In addition to this £165k of the nursing overspend has been driven by non delivery ofthe nursing CIP (a ward closure), which relates to the inability to deliver the capacitymanagement schemes due to the high level of non-elective admissions.
Excluding these factors there is an underlying over spend on nursing of £14k in themonth.
Other pay has under-spent by £33k in the month, and is under-spent £983k year todate. Year to date £363k of the under spend is due to over-achievement of CIPagainst the planned profile to January.
Although overall pay is broadly over plan at the end of January by £278k,Emergency services are above plan by £1,416k year to date (of which £865k was onmedical staffing) and Elective Services above plan by £570k year to date (of which£283k was on medical staffing). Prior to September an element of these overspendswas as a result of waiting lists initiatives. However, since September the waiting listreserve has been allocated out to divisions non-recurrently after finalising in yearcapacity and demand work.
Non-pay costs are above plan by £212k in January; and £343k year to date. Themain drivers of the in month position relates to general supplies and services £210k,which is due to non-delivery of CIP, and clinical supplies & services £125k.
Table 6:- Pay Expenditure
In month 10 the drugs reported position is an overspend of £41k, with a year to dateoverspend of £293k. (Table 7 below). PbR drugs income in the period is £112kahead of the income plan, and as such the Trust underlying in month position is anunder spend of £71k. Year to date PbR drug income is above plan by £321kmaterially explaining the above plan performance.

7
Table 7: Drugs Expenditure
The other main non-pay overspend is on clinical supplies and services which hasoverspent by £125k. (Table 8 below). The main driver of the overspend is onmedical and surgical equipment of £62k, but £38k, of this is driven by undeliveredCIP. The remaining £24k is activity driven with the escalation beds which are open.The other main driver is orthopaedic implants which has overspent by £57k in themonth, which is activity led. Although the orthopaedic activity is down the case mixundertaken in the period is richer, with an over performance on implant work in theperiod.
Table 8: - Clinical Supplies & Services Expenditure

8
Financing Costs
Depreciation is above planned levels by £8k in the period, whilst interest receivablehas overachieved by £3k. PDC Dividend now reflects the estimate submitted to theDepartment of Health for payment in March, any difference applicable at year endwill be a debtor or creditor, in the March position. Both dividends and depreciationreflect the estate revaluation effective from the 1st January 2012.
Risk Rating
The overall Financial Risk Rating (FRR) (Appendix B) for the month is 2, in line withthe plan set of 2. The key metrics driving the overall FRR is detailed below.
Risk Rating Metric JanuaryPlan
JanuaryActual
EBITDA Margin % 2.68% = 2 3.67% = 2EBITDA, % Achieved of Plan 93.6% = 4 138.99% = 5Return on Capital Employed -5.22% = 1 -0.07% = 2I&E Surplus Margin (%) -4.30% = 1 -3.37% = 1Liquid Ratio (days) -4.23 days = 1 -0.22 days = 1
The liquid ratio remains ahead of plan by 4 days.
At the EBITDA level which drives a number of the financial metrics, the Trust isreporting a surplus of £4,348k, which is ahead of plan by £1,220k, resulting in theEBITDA margin being 3.67% against the planned 2.68%.
CIPs
The Trust has set a CIP target of £9.4m for the year. The monthly planned profile ofCIPs as applied to the budget is shown below.
Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 TotalIncome 0 0 4 8 8 22 63 63 72 72 72 72 458Pay Costs 132 109 103 172 225 388 664 773 804 893 893 893 6,048Drug Costs 4 4 18 29 32 36 36 36 36 36 36 36 337Clinical Supplies & Services 29 29 32 33 40 47 67 69 72 73 74 81 645Other Costs(excl. depreciation) 64 46 47 39 68 76 78 299 297 297 297 300 1,908
229 187 203 281 373 569 908 1,240 1,281 1,370 1,372 1,382 9,395
Cumulative to the end of January the Trust has formally recorded CIP delivery of£6,851k against a profiled figure of £6,641k which results in an over-achievement of£210k. Of the savings achieved to date £1,797k has been achieved non-recurrentlywith £5,054k being recurrent. In terms of recurrent CIP delivery to the end of Januarythe Trust is behind the planned profile submitted to Monitor by £1,588k. The impacton the financial plan for 2012/13 has been factored in to the Trusts plans aspreviously discussed. Year to date £8.66m of the £9.4m target has been achieved.
The table below identifies the CIP posted by month and identifies if it is recurrent ornon-recurrent.

9
April May June July Aug Sept Oct Nov Dec Jan Feb March TotalCIP Planned (229) (187) (203) (281) (373) (569) (908) (1,240) (1281) (1,370) (1,372) (1,382) (9,395)CIP AchievedRecurrently
95 162 285 287 555 491 607 824 824 922 744 749 6,546
CIP Achievednon-recurrently
93 236 119 157 109 129 247 130 258 319 157 157 2,111
Total CIPAchieved
188 398 404 444 663 621 854 955 1,082 1,241 901 906 8,657
CIP Variance (41) 210 201 163 290 52 (55) (286) (198) (129) (472) (475) (738)
A detailed update on CIP performance can be found at Appendix H.
Key Risks
Key risks to the delivery of the Trusts’ financial plan remain,
Delivery of a challenging Cost Improvement Programme totalling £9.4m, (andincreased quarter 4 profile).
CQUIN total income of £1.5m with a challenging performance trajectory todeliver across the schemes agreed with NHS Tameside & Glossop.
QBP income of £2.7m required to be delivered.
Continued over performance on emergency admission generating 30% oftariff or no income, but at premium costs.
If KPI’s for stroke are not achieved at year end the PCT will require theadditional funding received to be returned a risk of £303k.
Penalties at year end greater than those currently being catered for.
These risks will continue to be assertively managed.
Conclusion
At the end of January the Trust’s position is ahead of the planned trajectory with acumulative normalised income and expenditure deficit of £3.99m against a planneddeficit of £5.04m and a risk rating of 2 for the year to date. Whilst the Trust is aheadof its plan, given the profile of CIP work streams and below plan performance sinceOctober, the key challenge is to ensure delivery of productivity and efficiency savingsagainst a challenging level of monthly savings required in the last quarter of thefinancial year of over £1.4m per month.
RECOMMENDATION
The Board is requested to discuss and note the contents of this report.
David JagoDirector of Finance16 February 2012

Cumulative Cumulative
FINANCE DASHBOARD AS AT 31ST JANUARY 2012
-2000
-1500
-1000
-500
0
500
1000
Sur
plu
s/(D
efic
it)£
000
Month
Monthly Surplus/(Deficit)
Plan Actual
-
100
200
300
400
500
600
700
800
900
£000
Month
Capital Programme
Plan Actual
Cash BalancesKey MeasuresCumulative
PlanCumulative
Actual Variance£000 £000 £000
EBITDA 3,129 4,348 1,220Net Surplus/(Deficit) (7,675) (6,230) 1,445Net Surplus/(Deficit) before Exceptional Items (5,042) (3,995) 1,047CIP 6,641 6,850 210
Margins Annual PlanCumulative
Actual Variance% % %
EBITDA Margin % 3.50% 3.67% 0.17%EBITDA % Achieved of Plan 93.60% 138.99% 45.39%I&E Surplus Margin % -3.50% -3.37% 0.13%
Financial Risk Rating Year-to-Date 1.75 1.85
a) Non-achievement of current and future years cost improvement plans (CIPs) resulting in a potential deficit and a reduction in cash balances.
b)c) Inability to reduce the use of escalation beds thereby negating the impact of previous CIP programmes, and incurring escalation costs possibly at premium ratesd) Continuing staffing overspends within Accident and Emergency due to the inability to recruit to the vacant posts.e) PCT demand management initiatives are effective resulting in the Trust having to make a further savings.f)g) PCT Targets and penalties missed or applied
Key Risks
Sustainability of growth in contracted activity levels for non-elective and outpatients.
Management of capacity and the achievement of 18 week targets whilst, minimising premium cost lists to ensure positive EBITDA growth, and remaining within the undingenvelope identified.
-2000
-1500
-1000
-500
0
500
1000
Sur
plu
s/(D
efic
it)£
000
Month
Monthly Surplus/(Deficit)
Plan Actual
-
100
200
300
400
500
600
700
800
900
£000
Month
Capital Programme
Plan Actual
-1,0002,0003,0004,0005,0006,0007,0008,0009,000
10,000
£000
Month
Cash Balances
Plan Actual

Appendix A
Budget Actual Variance Budget Actual Variance Annualbudget
£000 £000 £000 £000 £000 £000 £000
IncomeClinical Income 11,029 11,738 709 106,105 108,530 2,426 127,520Research & Development 9 13 4 91 129 37 110Education & Training 298 438 140 3,001 3,322 322 3,598Other Clinical & other non-clinical income 573 546 (27) 5,618 5,960 342 6,768PFI Specific Income (transitional) 310 173 (137) 1,844 558 (1,287) 2,583
0Total Income 12,220 12,908 688 116,659 118,500 1,840 140,578
ExpenditurePay Costs (7,515) (8,001) (487) (78,883) (79,284) (401) (93,937)Pay Costs - PFI transitional (8) (7) 1 (250) (127) 124 (275)Non-pay cost (incl internal recharges) (2,849) (3,198) (349) (30,761) (32,271) (1,510) (36,676)PFI Specific Expenditure - UP (221) (220) 1 (2,090) (2,083) 6 (2,518)PFI Specific Expenditure - transitional (302) (167) 136 (1,547) (386) 1,161 (2,261)
Total Costs (10,895) (11,593) (697) (113,531) (114,151) (621) (135,667)
EBITDA 1,325 1,315 (9) 3,129 4,348 1,220 4,912EBITDA as a % of Income 10.84% 10.19% -0.65% 2.68% 3.67% 0.99% 3.49%
INCOME & EXPENDITURE REPORT JANUARY 2012
In Month Year to Date
Technical ItemsProfit/(loss) on asset disposal 0 0 0 0 0Exceptional income ( fixed asset impairment) 0 0 0 0 0 0 0Exceptional costs ( fixed asset impairment) 0 0 0 (1,500) (1,500) 0 (2,781)Restructuring Costs 0 228 228 (1,133) (735) 398 (1,133)Plus Income from Donated Depreciation/Assets 17 0 (17) 173 20 (154) 209Less Total Depreciation (438) (447) (8) (4,308) (4,412) (104) (5,184)Plus Total Interest Receivable 3 6 3 30 49 19 36Plus income from Impairment 0 0 0 0 0 0 0Less Total Interest Payable 0 0 0 0 0 0 0Less Total Interest payable on loans and leases - PFI (258) (258) 0 (2,437) (2,437) 0 (2,936)
Less Total Interest payable on loans and leases - Finance Leases (0) (0) 0 (3) (3) 0 (4)
PFI Contingent Rent (31) (31) 0 (292) (292) 0 (352)Less Other Finance Cost - Unwinding Discount (1) (1) 0 (13) (13) (1) (15)Less PDC Dividend (132) (64) 68 (1,322) (1,255) 67 (1,587)
Net Surplus/(deficit) 484 747 263 (7,675) (6,230) 1,445 (8,837)
For InformationNet Surplus/(deficit) before exceptional items 484 519 35 (5,042) (3,995) 1,047 (4,923)

Risk Rating Metrics Annual Budget Year to DateEBITDA Margin % 3.50% 3.67%EBITDA, % Achieved of Plan 93.60% 138.99%
Return on Capital Employed -0.3% -0.07%I&E Surplus Margin (%) -3.50% -3.37%Liquid Ratio (days) -5.30 0
Weighted Risk Rating 1.75 1.85
Risk Rating Metrics Scoring Annual Budget Year to DateEBITDA Margin % 2 2EBITDA, % Achieved of Plan 4 5Return on Capital Employed 2 2
I&E Surplus Margin (%) 1 1Liquid Ratio (days) 1 1
Weighted Risk Rating 1.75 1.85
Appendix B
RISK RATING METRICS - JANUARY 2012
Weighted Risk Rating Metrics Annual Budget Year to DateEBITDA Margin % 0.5 0.5
EBITDA, % Achieved of Plan 0.4 0.5Return on Capital Employed 0.4 0.4I&E Surplus Margin (%) 0.2 0.2
Liquid Ratio (days) 0.25 0.25
Weighted Risk Rating 1.75 1.9

Appendix C1
Budget Actual Variance Budget Actual VarianceAnnualbudget
£000 £000 £000 £000 £000 £000 £000
Clinical Income by typeElective 1,700 1,858 157 17,159 17,369 210 20,558Non-Elective 4,424 4,586 162 40,637 40,948 311 48,970Outpatient 2,266 2,406 140 22,483 23,115 631 27,013A&E 640 632 -9 6,320 6,324 4 7,538Other 1,998 2,255 257 19,505 20,775 1,269 23,441
Total 11,029 11,738 709 106,105 108,530 2,426 127,520
Clinical Income by CommissionerTameside PCT 9,540 10,088 548 91,771 93,241 1,469 110,251Manchester PCT 412 460 48 4,008 4,148 140 4,806Oldham PCT 598 680 82 5,861 5,953 92 7,027Stockport PCT 92 166 74 893 1,032 139 1,071All other contracts PCTs (less than £1m) 388 345 -43 3,570 4,157 587 4,366
In Month Year to Date
INCOME REPORT JANUARY 2012
All other contracts PCTs (less than £1m) 388 345 -43 3,570 4,157 587 4,366
Total 11,029 11,738 709 106,105 108,530 2,426 127,520
Other income:Research & Development 9 13 4 91 129 37 110Education & Training 298 438 140 3,001 3,322 322 3,598Other clinical & other non-clinical income 573 546 -27 5,618 5,960 342 6,768PFI Specific Income - Transitional 310 173 -137 1,844 558 (1,287) 2,583
Total 1,191 1,170 -21 10,555 9,969 (585) 13,058
Total Income 12,220 12,908 688 116,659 118,500 1,840 140,578
Activity (Spells)Activity (Spells)Elective 1,575 1,561 -14 16,088 15,601 (487) 19,236Non Elective 2,514 2,487 -27 23,360 23,919 559 28,104Outpatients (including outpatient procedures) 18,200 19,171 971 180,624 185,023 4,399 217,004A&E Attendances 6,439 6,131 -308 63,567 62,866 (701) 75,822
Total Activity 28,728 29,350 622 283,638 287,409 3,771 0 340,166

APPENDIX D
ANALYSIS OF EXPENDITURE
AnnualBudget Actuals Variance Budget Actuals Variance Budget£000's £000's £000's £000's £000's £000's £000's
Expenditure
Pay Costs:-Medical (2,485) (2,546) (62) (25,764) (25,318) 446 (31,160)Nursing (2,799) (3,257) (457) (29,712) (31,542) (1,831) (34,967)Other (2,231) (2,198) 33 (23,407) (22,424) 983 (27,809)PFI Transitional Pay (8) (7) 1 (250) (127) 124 (275)
Total Pay Costs (7,523) (8,008) (486) (79,133) (79,411) (278) (94,212)
Non-Pay Costs:-
In Month Year-to-Date
EXPENDITURE REPORT JANUARY 2012
Non-Pay Costs:-Drugs (483) (524) (41) (4,567) (4,860) (293) (5,520)Clinical Supplies & Services (713) (837) (125) (7,849) (8,454) (605) (9,419)General Supplies & Services (211) (421) (210) (3,770) (4,279) (509) (4,232)Establishment Expenses (105) (127) (21) (1,083) (1,057) 25 (1,309)Other Establishment Costs (372) (402) (30) (3,731) (3,891) (160) (4,480)Premises & Fixed Plant (594) (670) (76) (5,808) (5,774) 34 (6,972)Other (372) (218) 154 (3,954) (3,956) (2) (4,744)PFI - UP (221) (220) 1 (2,090) (2,083) 6 (2,518)PFI - Transitional Costs (302) (167) 136 (1,547) (386) 1,161 (2,261)
Total Non-Pay Costs (3,373) (3,584) (212) (34,398) (34,740) (343) (41,455)Total Expenditure (10,895) (11,593) (697) (113,531) (114,151) (621) (135,667)
The above table excludes expenditure on technical items as detailed in Appendix A such as depreciation, dividends and exceptional items.

Budget Actual Variance Budget Actual VarianceAnnualBudget
£000 £000 £000 £000 £000 £000 £000Emergency services
Pay Costs (2,637) (2,770) (132) (25,243) (26,658) (1,416) (30,449)Drug Costs (0) 0 0 (1) 0 1 (2)Clinical Supplies & Services (129) (130) (0) (1,226) (1,343) (117) (1,482)Other Costs(excl. depreciation) (111) (117) (7) (1,130) (1,305) (176) (1,359)Total (2,877) (3,016) (139) (27,600) (29,307) (1,707) (33,292)
Elective ServicesPay Costs (1,877) (1,915) (38) (18,961) (19,531) (570) (22,716)Drug Costs (0) 0 0 (1) 0 1 (2)Clinical Supplies & Services (386) (465) (79) (4,111) (4,322) (210) (4,975)Other Costs(excl. depreciation) (72) (66) 5 (779) (770) 9 (933)Total (2,334) (2,446) (112) (23,852) (24,622) (770) (28,625)
Women and Children servicesPay Costs (1,312) (1,287) 25 (13,054) (12,782) 272 (15,672)Clinical Supplies & Services (33) (38) (5) (361) (457) (97) (435)Other Costs(excl. depreciation) (29) (48) (19) (304) (402) (97) (367)Total (1,374) (1,374) 1 (13,719) (13,641) 78 (16,474)
0 0Diagnostic and Therapeutic services
Pay Costs (1,031) (1,027) 5 (10,330) (10,105) 225 (12,471)
APPENDIX F
DIVISIONAL EXPENDITURE REPORT JANUARY 2012
In month Year to Date
Pay Costs (1,031) (1,027) 5 (10,330) (10,105) 225 (12,471)Drug Costs (471) (524) (52) (4,369) (4,861) (492) (5,163)Clinical Supplies & Services (210) (210) 1 (2,164) (2,055) 109 (2,607)Other Costs(excl. depreciation) (132) (120) 12 (1,324) (1,376) (51) (1,591)Total (1,845) (1,881) (35) (18,188) (18,397) (209) (21,833)
Pay Costs (289) (296) (7) (2,944) (2,909) 35 (3,527)Clinical Supplies & Services (3) (3) 0 (37) (33) 3 (44)Other Costs(excl. depreciation) (794) (880) (86) (8,155) (7,995) 160 (9,832)Total (1,086) (1,179) (93) (11,136) (10,937) 199 (13,403)
PFIPay Costs (8) (7) 1 (250) (127) 123 (275)Clinical Supplies & Services 0 0 0 0 0 0 0Other Costs(excl. depreciation) (560) (420) 140 (4,009) (2,723) 1,287 (5,226)Total (569) (427) 142 (4,260) (2,850) 1,410 (5,501)
CorporatePay Costs (368) (707) (338) (8,351) (7,300) 1,051 (9,102)Drug Costs (11) 0 11 (196) 1 197 (352)Clinical Supplies & Services 49 8 (41) 50 (243) (293) 125Other Costs(excl. depreciation) (480) (571) (91) (6,282) (6,856) (574) (7,209)Total (810) (1,270) (460) (14,779) (14,398) 381 (16,538)
Trust TotalPay Costs (7,523) (8,008) (486) (79,133) (79,411) (278) (94,212)Drug Costs (483) (524) (41) (4,567) (4,860) (293) (5,520)Clinical Supplies & Services (713) (837) (125) (7,849) (8,454) (605) (9,419)Other Costs(excl. depreciation) (2,176) (2,224) (45) (21,982) (21,427) 555 (26,515)Grand Total (10,895) (11,593) (697) (113,531) (114,151) (621) (135,667)
Non clinical and Facilities includingIT and information

Directorate and POD Budget Actual Variance Budget Actual VarianceAnnualBudget
£000 £000 £000 £000 £000 £000 £000Emergency servicesElective Inpatients/PSD 209 238 29 2,325 2,378 53 2,743Non-Elective Inpatients 2,390 2,267 (123) 22,437 22,819 382 26,885Adult Critical Care 450 492 42 4,441 4,199 (243) 5,298Excess Bed Days 297 204 (93) 2,790 2,811 20 3,347Outpatients 771 737 (33) 7,542 7,727 185 9,082Outpatient Procedures 22 39 18 157 176 19 200Accident & Emergency 652 630 (22) 6,366 6,324 (42) 7,598Cardiac Rehab Contract 19 28 9 193 184 (10) 232Other - T&G Funding 64 0 (64) 193 0 (193) 321Other- CRI 4 4 0 39 38 (1) 46Total 4,878 4,640 (238) 46,483 46,655 172 55,754
Elective servicesElective Inpatients/PSD 1,190 1,203 12 11,848 12,296 448 14,228
Non-Elective Inpatients 849 838 (10) 7,895 8,371 476 9,483Excess Bed Days 70 39 (32) 665 462 (203) 798
Outpatients 996 1,005 9 9,889 9,730 (159) 11,880Outpatient Procedures 125 177 52 1,204 1,573 369 1,453Audiology 94 98 4 939 978 39 1,127
CONTRACT INCOME ANALYSIS - JANUARY 2012
APPENDIX G
In month Year to Date
Audiology 94 98 4 939 978 39 1,127Total 3,325 3,359 35 32,440 33,410 970 38,969
Women & ChildrensElective Inpatients/PSD 287 242 (46) 2,858 2,581 (277) 3,432Non-Elective Inpatients 852 878 27 8,515 8,245 (270) 10,157Paediatric Critical Care 175 197 22 1,727 1,590 (137) 2,060Excess Bed Days 22 31 8 215 192 (22) 256Outpatients 365 368 4 3,628 3,575 (53) 4,357Outpatient Procedures 15 18 3 147 213 66 177Other 0 0Total 1,715 1,734 18 17,091 16,397 (694) 20,440
Diagnostic & TherapeuticsDirect Access 334 379 45 3,321 3,445 125 3,988Outpatients 12 11 (1) 119 120 1 143Total 346 390 44 3,440 3,565 125 4,131
OtherEmergency Threshold Income Reduction (16) 45 61 -1,062 -1,482 (421) (1,073)EL readmissions (31) (7) 24 -282 -171 111 (340)NEL readmissions (69) 9 78 -626 -275 351 (755)Planned OP Coding Changes 9 0 (9) 18 91 73 36CIP Planned Overperform at spec level (49) 0 49 -242 0 242 (331)Non-Activity Based/TEL 922 1,335 413 8,845 10,341 1,496 10,689Total 765 1,381 616 6,651 8,504 1,852 8,226
Grand Total 11,029 11,504 475 106,105 108,530 2,426 127,520
NB ~ Appendix G in month actual income reflects the estimated income of activity for the month reported, this differs from Appendices C and A which
reports both the estimated income for the month and also the difference between the previous months' uncoded estimate and the coded position.
DJ – 16.2.12
Appendix H
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
Financial Recovery Plan
2011/12 Savings Plan
Month 10 cumulative CIP delivery totals £6.85m against a plan of £6.64m. Theconfirmed savings figure for 2011/12 remains at £9.4m (with the Waiting List moniesincluded). The recurrent cumulative figure to date is £5.05m, which is £1.59m behindthe recurrent plan. Failure to deliver the level of CIP required recurrently impactsadversely on the financial plan set for 2012/13.An assessment of the shortfall againstthe planned full year effect of £14.6m has been incorporated into the refreshedfinancial plan for 2012/13 based on performance at the end of month 10.
65 projects are now confirmed green for delivery in 2011/12. The key risk remainingis around the final execution phase of the administration/clerical project. Thesesavings will be finalised once the individual consultations have reached a conclusionwith regards to “buy out” of pay protection.
The business case with regards to “E-Rostering” has recently been approved atTrust Executive Group (TEG).This is an enabler to the key efficiency project tofacilitate delivery of the planned reduction in usage of bank and agency staff andsubstantive pay bill.
2 schemes are being brought forward from 2012/13 to 2011/12 with a value of £70k.Monthly budget reviews are continuing which is ensuring close monitoring ofexpenditure against plan to identify where further reductions can be made.
Implementation costs for the 2011/12 savings programme are currently forecast tofall below the plan set of £1.1m based on information provided these are more likelyto come in at circa £0.7m.
2012/13 Savings Plan
The 12/13 savings plan development process continues to increase the clarity androbustness around specific projects. A total of £6.3m has been currently identified interms of the total scheme value. This represents 52% of the total current estimatedrequirement for 2012/13.
In addition divisions have been targeted to deliver tactical savings of some£2.6m.The PMO is continuing to work with project leads to develop robust projectplans for these schemes and to identify further schemes to reach the required circa£12m target.
The planning for 2012/13 and detailed review of CIP programme is the subject of aseparate Board Seminar discussion on the 28th February 2012.

1
Agenda Item 9
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
STATEMENT OF POSITION REPORT
MONTH 10 – JANUARY 2012
PURPOSE
The purpose of this report is to advise the Board of the performance on key elements ofthe Trust’s Statement of Position, which underpins the income and expenditure position.
DISCUSSION
This report provides the Board with the Statement of Position for the period ended 31January 2012, together with details of capital expenditure.
Statement of Position (See Appendix A)
Overall, in the month of January the total assets of the Trust have increased by £0.7mto £46.1m against the December figure of £45.4m.
Total net current assets/liabilities (working capital) have moved from net currentliabilities of £8.66m at the end of December, to net current liabilities of £7.71m at theend of January, a decrease in liabilities of £0.94m in the month.
Capital Expenditure (See Appendix B)
Appendix B provides details of the capital programme for 2011/12, detailing expenditureincurred to date, including accruals, against the planned capital spend, per scheme.
The plan submitted to Monitor detailed a capital programme totalling £3.99m during2011/12.
Capital expenditure year to date is £2.32m against the original plan to Monitor of£3.06m, resulting in an under-spend of £742k, which is 24.25% less than the plan. Thecriterion for assessing financial control requires capital spend to fall within the range of75% - 125% of the planned profiled budget on a cumulative basis.
Appendix B includes a forecast outturn position, and a movement from the originalMonitor plan. The forecast identifies a reduction in outturn spend of £665k, forecastingtotal capital spend for 2011/12 at £3.33m.
Estate Schemes are under-spent by £397k against the plan. The enabling schemes tovacate Darnton building are under-spending by £457k to plan. It is expected that theseschemes will continue to under-spend in 2011/12 with an overall forecast of £341kunder-spend against the estates schemes.

2
There is an under-spend of £80k against the conditions and statutory complianceschemes. This is mainly due to the under-spend of £34k on the Ladysmith fire dampersand pipes scheme and £25k on the nurse call systems programme.
IM&T Schemes are under-spent by £172k against plan. This is mainly due to threeschemes – Wireless Data and Voice, and software rollouts for the Switchboard Consoleand Digital Dictation. The plan had expected all of these schemes to have started, butto date only £15k has been spent against the Digital Dictation scheme. The IM&Tschemes have been reviewed, and it is now expected that these schemes will have ayear end under-spend of £356k, relating mainly to reduced spend on the PACS refreshand slippage on schemes into 2012/13.
Medical equipment schemes are under-spending by £94k. To date £73k expenditurerelates to purchases of equipment for Theatres. It is expected that a further £332k, willbe spent during the remainder of the financial year, creating an overspend of £39k.
The Trust had been expecting to receive £850k, from the sale of Hyde hospital. This isnow expected to slip into 2012/13 financial year. The loss of this income to fund thecapital programme is being offset by the forecast reduction in expenditure of £665k.
Current Assets
Total current assets have increased in the period by £0.57m giving a balance of£16.9m. This is due to an increase of £264k against trade and other receivables and acash increase of £299k.
The increase relating to trade and other receivables relates to accrued NHS income of£145k which is expected from various PCTs, whilst £157k relates to an increase of theVAT debtor.
In the period, cash and cash equivalent balances have increased by £299k, giving acash balance of £3.6m, and an investment balance of £5.8m at the end of January.
The table below details the Trust investment portfolio as at the end of January:-
Bank Account Type % Rate £mBarclays Instant Access 0.70% £2.0Lloyds 2 month fixed 0.70% £2.0
Santander Instant Access 0.80% £1.8
Due to the reduction of the rates being offered, the investment placed with Lloyds hasbeen increased by £200k, increasing the overall investment portfolio to £5.8m. At theend of January the Trust has 62% of the cash in higher interest accounts. This is toensure the Trust continues to generate the maximum levels of interest receivable on itscash balances. It is expected that these investments will remain in place until the 31March 2012.

3
Appendix C compares the actual cash balances throughout the year against theplanned cash position included in the Monitor Plan. The cash balance at the end ofJanuary is £9.4m, this is £7.8m above the plan of £1.6m. Cash is in excess of plan, dueto the improved EBITDA position compared with plan of £1.4m and the improvedworking capital compared to plan of £6.0m. The improvement of working capital ismaterially driven by increased accruals and deferred income compared to plan.
The plan submitted to Monitor was reporting a year end cash position of £226k. TheTrust has now revised the year end cash balance forecast and is now forecasting abalance of £7m on the 31st March 2012 utilising a range of upside and downsideassumptions as contained in the submitted and refreshed recovery plan.
The Trust produces a 13 week cash flow forecast, which monitors closely the cashbalances to ensure sufficient funds are available. The graph below details the 13 weekcash flow forecast balances compared to the Monitor cash flow plan, for the period 13th
February 2012 to 11th May 2012.
The Trust has a working capital facility of £10m with Barclays Bank, but does notcurrently expect to utilise this facility during 2011/12. From discussions with BarclaysBank following delivery of plan at the end of quarter 3 an extension proposal would besubmitted to the Treasury team. The Trust has requested an update followingsubmission of quarter three performance.
Current Liabilities
In the period, current liabilities have decreased by £0.4m, giving total current liabilities of£24.6m. There has been an increase of Trade and Other Payables of £1.82m and adecrease of Other Liabilities of £2.2m.
Non NHS trade creditors have increased in the month by £1.8m. This is due to anincrease in invoices processed in January, which had previously accrued in December.
01,0002,0003,0004,0005,0006,0007,0008,0009,000
10,00011,00012,00013,00014,00015,00016,00017,00018,000
£00
0
Week
13 Week Cashflow Forecast - v - Monitor Plan
13 week cashflow Monitor Plan

4
Other Liabilities have decreased by £2.2m, relating mainly to the decrease of accrualsand deferred income.
Accruals have decreased by £1.3m. The majority of this relates to charges that hadbeen accrued in December, but have now been invoiced and are now trade creditors.
Deferred income has decreased by £987k. This relates to the release of £372k ofdeferred income which was received from Tameside PCT in December. Also, £236khas been released for MADEL income and £138k for HIT Transitional funding.
Conclusion
During January, the total value of the Trust’s assets employed increased by £747k. Netcurrent liabilities have decreased by £944k. The plan set for liquidity at the end ofJanuary was (4.23) days, whilst the actual achieved is (0.23) days, so the Trust remainsahead of plan by some 4 days.
The plan for net current liabilities was (£10.2m) against the actual for January of(£7.7m), an over-achievement of £2.5m.
RECOMMENDATION
The Board is requested to note and discuss the contents of this report.
David JagoDirector of Finance16 February 2012

Appendix ATAMESIDE HOSPITAL NHS FOUNDATION TRUST
Column A Column B Column C Column D Column E
PeriodEnding 31st
Mar 2011£'000s
PeriodEnding 30thDecember
2011 £'000s
PeriodEnding 31st
January 2012£'000s
Movement inthe monthDec 2011 -Jan 2012
£'000
MovementYTD 2011/12
£'000
Non Current Assets
Property, plant and equipment 73,578 72,126 71,836 (290) (1,742)PFI: Property, plant and equipment 38,543 39,361 39,280 (81) 737
Trade and Other Receivables> Accrued Income (CRU Income grt than 1 yr) 807 662 836 174 28> Prepayments - PFI Related 353 784 740 (45) 386
Total Non Current Assets 113,281 112,933 112,692 (242) (590)
Current AssetsInventories - Stock - Finished Goods 1,346 1,434 1,442 8 96
Trade & Other Receivables:-> NHS Trade Receivables 963 2,151 2,282 132 1,319> Non NHS Trade Receivables 83 122 142 20 59> Other Receivables 512 307 515 208 3> Accrued Income 898 931 884 (47) (14)> Prepayments - Non PFI Related 686 1,365 1,316 (49) 630
Non-Current Assets held for sale and assets indisposal groups 904 928 928 0 24
Cash 7,641 3,491 3,591 100 (4,050)Investments 1 5,618 5,816 199 5,815
Total Current Assets 13,035 16,347 16,918 571 3,883
STATEMENT OF POSITION 2011/12
Total Current Assets 13,035 16,347 16,918 571 3,883
Current LiabilitiesTrade & Other Payables:-> NHS Trade Creditors (1,645) (2,007) (2,063) (55) (417)> Non NHS Trade Creditors (2,659) (3,498) (5,286) (1,788) (2,627)> Other Creditors (3,584) (3,835) (3,884) (49) (300)> Capital Creditors (865) (581) (506) 75 359
Other Liabilities:-> Accruals (3,967) (6,366) (5,125) 1,241 (1,158)> Deferred Income (3,139) (6,751) (5,765) 987 (2,626)>Finance Leases (43) (36) (35) 1 8>PFI Leases (807) (1,080) (1,080) 0 (273)>PDC Dividend Creditor 0 (469) (533) (64) (533)
Provisions (469) (380) (354) 26 116
Total Current Liabilites (17,179) (25,003) (24,631) 373 (7,451)
Net Current Assets/Liabilities (4,144) (8,656) (7,713) 944 (3,568)
Non Current Liabilities
Other Financial Liabilities:-> Finance Leases (34) (9) (6) 2 28> PFI Leases (56,085) (58,213) (58,142) 71 (2,057)
Provisions (624) (674) (701) (27) (77)
Total Non Current Liabilities (56,742) (58,895) (58,849) 46 (2,107)
TOTAL ASSETS EMPLOYED 52,395 45,384 46,131 747 (6,264)
Financed By Taxpayers EquityPDC 53,168 53,168 53,168 0 (0)Revaluation Reserve 18,733 18,549 18,549 0 (184)Donated Asset Reserve 1,207 0 0 0 (1,207)I&E Reserve 7,586 7,586 7,586 0 0I&E Reserve 2008/09 124 124 124 0 0I&E Reserve 2009/10 (4,245) (4,245) (4,245) 0 0I&E Reserve 2010/11 (24,179) (22,822) (22,822) 0 1,357I&E Reserve 2011/12 0 (6,977) (6,230) 747 (6,230)I&E Reserve 2011/12 0 (6,977) (6,230) 747 (6,230)
TOTAL TAXPAYERS EQUITY 52,395 45,384 46,131 747 (6,264)

APPENDIX B
CAPITAL MONITORING REPORT - JANUARY 2012
Ref Scheme Description
ANNUALPLAN TOMONITOR
£'000
REVISEDFORECAST
OUTURNCPEC28.1.12£'000
MOVEMENTORIGINALMONITORPLAN TOREVISED
FORECASTOUTURN
£'000
PLAN TOJANUARY
£'000
ACTUAL TOJANUARY
£'000
VARIANCETO PLAN
£'000
ESTATES SCHEMES
1 Redevelopment of Accident and Emergency 1,112 1,087 25 1,112 1,087 252 PFI Infrastructure Variations 241 221 20 241 221 203 Refrigerated Merchandiser 18 16 2 18 14 44 Enabling Schemes to vacate Darnton Building - W30 250 25 225 250 27 2235 Enabling Schemes to vacate Darnton Building - Scan Van 250 20 230 250 16 2346 DSEU Single Gender Compliance 25 25 0 25 19 67 MAU Move 100 111 (11) 80 111 (31)8 A&C Review 0 150 (150) 0 84 (84)
SUB TOTAL ESTATES SCHEMES 1,996 1,655 341 1,976 1,579 397
CONDITIONS & STATUTORY COMPLIANCE
9 Provision for Conditions & Statutory Compliance 202 280 (78) 97 108 (11)10 Drainage And Access Darnton Road 10 2 8 10 2 811 Ladysmith Fire Dampers and Pipes (ph3 and 4) 232 198 34 232 198 3412 Nurse call to Hartshead Theatre 0 (5) 5 0 (5) 512 Energy Management 50 50 0 30 40 (10)13 Fire and Safety slipped from 2010/11 15 24 (9) 15 24 (9)14 Ladysmith Ramped Fire Escape 10 5 5 10 4 615 VIE - Third Supply Source (no longer required planning permission received) 10 0 10 10 0 1016 Nurse Call Systems Programme 40 20 20 40 15 2517 Hartshead Plates 7 9 (2) 7 9 (2)
2011/12 2011/12
17 Hartshead Plates 7 9 (2) 7 9 (2)18 Fire and Safety forward programme 2011/12 50 35 15 50 26 2419 HV Sub 2 Charlsworth 21 22 (1) 21 22 (1)
SUB TOTAL CONDITION AND STATUTORY SCHEMES 647 640 7 522 442 80
IM&T SCHEMES
20 Provision for General IM&T Equipment 200 147 53 110 61 4921 Positive Patient Blood Tracking - Phase 2 68 70 (2) 68 70 (2)22 PACS - Refresh 498 253 245 0 (0) 023 Maternity IT System 60 52 8 60 52 824 Wireless Data and Voice 66 16 50 66 0 6625 Switchboard Console - Software roll out 27 0 27 27 0 2726 Software for Digital Dictation roll out Trust Wide (storage & software) 35 65 (30) 35 15 2027 Bedside Information System - RENAL 30 25 5 30 25 5
SUB TOTAL IM&T SCHEMES 984 628 356 396 224 172
MEDICAL EQUIPMENT SCHEMES
28 Provision for General Medical Equipment 350 389 (39) 150 73 7829 Echo Machines and Archiving Facility 16 16 0 16 0 16
SUB TOTAL MEDICAL EQUIPMENT SCHEMES 366 405 (39) 166 73 94
TOTAL CAPITAL EXPENDITURE 3,993 3,328 665 3,060 2,319 742
VARIANCE TO MONITOR PLAN 665 17% 742 24%
Financed By:-
1Assets Held for Sale - Hyde Hospital - Offer accepted for £850k with cost this willgive a net receipt of £750k. Shortfall of £100k possible fund from PFITransitional
850 850 0
2 Capital Receipt - sale of small piece of land - No longer able to sell 0 0 0
3 Transitional Income (as I&E Surplus) to fund enabling schemes to vacateDarnton building
500 269 231
4 Unspent/(over spent) Internally Generated Resources b/fwd (968) (968) 0
5Internally Generated Resources (Risk when site revalued in Sept 11, mayreduce)
3,454 3,454 0
Anticipated Capital Resource 2011/12 3,836 3,605 231Anticipated Capital Resource 2011/12 3,836 3,605 231
UNDER / (OVER) COMMITMENT - CUMULATIVE (157) 277 (434)

APPENDIX C
ForecastOutturn2011/12
MonitorPlan
2011/12
MovementRevisedPlan toMonitor
Plan 11/12£'000
Q1 2011/12£'000
Q2 2011/12£'000
Q3 2011/12£'000
January2011£'000
YTD 2011£'000
February2012 £'000
March2012 £'000 Total £'000 Total £'000 Total
£'000
Operating Surplus/(deficit) after tax (2,703) (3,849) (425) 747 (6,230) 1,445 (547) (1,439) (8,216) (8,837) 621
Non Cash flows in operating surplus/(deficit)Depreciation and Amortimisation 1,317 1,314 1,334 447 4,412 104 447 233 5,092 5,184 (92)Impairment losses/(reversals) 0 1,500 0 0 1,500 0 0 1,281 2,781 2,781 0PDC Dividend 397 325 468 65 1,255 (68) 126 126 1,506 1,587 (81)Gain/loss on disposal of property, plant and equipment 0 0 0 0 0 0 0 0 0 0 0Other increases/(decreases) to reconcile to profit/(loss) fromoperation items 710 844 832 281 2,667 138 251 269 3,187 3,048 139Non-Cash flows in operating surplus/(deficit) total 2,424 3,983 2,634 793 9,834 175 824 1,908 12,566 12,600 (34)
Operating Cash Flows before movement in working capital (279) 134 2,209 1,540 3,604 1,620 277 469 4,349 3,763 586
Increase/(Decrease) in working capital(Increase)/Decrease in inventories 23 (46) (65) (8) (96) (116) 0 100 4 24 (20)(Increase)/Decrease in NHS Trade Receivables (2,826) 1,650 (11) (132) (1,319) (1,485) 150 500 (669) 319 (988)(Increase)/Decrease in Non NHS Trade Receivables (88) 27 22 (20) (59) (59) 0 100 41 0 41(Increase)/Decrease in other receivables 110 (48) 143 (208) (3) (9) 0 0 (3) (46) 43(Increase)/Decrease in accrued income (377) 199 145 47 14 199 0 50 64 (101) 165(Increase)/Decrease in prepayments (245) (288) (146) 49 (630) (27) 0 50 (580) 12 (592)(Increase)/Decrease in Non Current Assets held for sale (16) (4) (4) 0 (24) (24) 0 24 0 0 0Increase/(Decrease) in Trade Creditors 565 766 (133) 1,843 3,041 2,391 (100) (100) 2,841 650 2,191Increase/(Decrease) in Other Creditors 267 65 (81) 49 300 300 0 2,850 3,150 0 3,150
Cashflow Statement 2011/12
Actual 11/12
YTD Apr-Jan varianceto plan £'000
as per 13 week cashforecast
Increase/(Decrease) in Other Creditors 267 65 (81) 49 300 300 0 2,850 3,150 0 3,150Increase/(Decrease) in accruals 1,942 (686) 1,143 (1,241) 1,158 2,095 10 (481) 687 (966) 1,653Increase/(Decrease) in Deferred Income (exl Donated Assets) 4,136 (718) 194 (987) 2,625 2,817 (720) (2,422) (518) (1,473) 956Increase/(Decrease) in provisions (48) (75) 84 1 (38) (39) 0 50 12 0 12Increase/(Decrease) in other - Other Financial Liabilities 0 0 0 0 0 0 0 0Increase/(Decrease) in working capital total 3,443 842 1,291 (607) 4,969 6,043 (660) 721 5,030 (1,581) 6,611
Net cash inflow/(outflow) from operating activities 3,164 976 3,500 933 8,573 7,663 (383) 1,190 9,379 2,182 7,197
Net cash inflow/(outflow) from Investing activiesProperty, plant and equipment (626) (789) (829) (75) (2,319) 741 (526) (483) (3,328) (3,993) 665Property, plant and equipment - non -maintenance expenditure 0 0 0 0 0 (155) (155) (310) 0 (310)Increase/(decrease) in Capital Creditor (575) 284 7 (75) (359) 200 (100) (100) (559) (509) (50)Proceeds from sale of assets 0 0 392 0 392 (512) 0 0 392 904 (512)Proceeds on current asset investments 0 0 0 0 0 0 0 0Proceeds on current asset investments 0 0 0 0 0 0 0 0Other cashflows from investing activities 0 0 0 0 0 0 0 0Net cash inflow/(outflow) from Investing activies - Total (1,201) (505) (430) (150) (2,286) 429 (781) (738) (3,805) (3,598) (207)
Net cash inflow/(outflow) before financing 1,963 471 3,070 783 6,287 8,092 (1,164) 452 5,574 (1,416) 6,990
Net cash inflow/(outflow) from Financing activitiesPublic Dividend Capital Received 0 0 0 0 0 0 0 0Public Dividend Capital Repaid 0 0 0 0 0 0 0 0PDC Dividends paid 0 (722) 0 0 (721) 73 0 (783) (1,504) (1,587) 83Interest element of finance lease rental payments - other 0 0 0 0 0 0 0 0Interest element of finance lease rentals on balance sheet (772) (809) (861) (289) (2,731) 1 (271) (288) (3,290) (3,293) 3Capital element of finance lease rental payments - other - PFI Prepayments 0 (279) (152) 45 (386) (386) (50) (50) (486) 0 (486)Capital element of finance lease rental payments - on balance sheet (200) (208) (223) (74) (705) (0) (70) (75) (850) (851) 1Interest received on cash and cash equivalent 12 15 16 6 49 19 2 2 53 36 17Increase/(decrease) in non-current payables 0 0 0 0 0 0 0 0(Increase)/decrease in non-current receivables 571 (293) (132) (174) (28) 0 (41) (82) (151) (307) 156Net cash inflow/(outflow) from Financing activities - Total (389) (2,296) (1,352) (486) (4,522) (293) (430) (1,276) (6,227) (6,002) (225)
Net increase/(decrease) in cash and cash equivalents 1,574 (1,825) 1,718 297 1,765 7,799 (1,594) (823) (653) (7,418) 6,764
Opening cash and cash equivalents 7,642 9,216 7,391 9,109 7,642 0 9,407 7,813 7,642 7,642 0
Closing cash and cash equivalents 9,216 7,391 9,109 9,407 9,407 7,799 7,813 6,990 6,990 226 6,764Monitor Plan 11/12 5,811 1,692 1,692 1,608 1,608 1,645 226 226 226 0Variance to Monitor Plan 11/12 3,405 5,699 7,417 7,799 7,799 7,799 6,168 6,764 6,764 0 6,764Variance to Monitor Plan 11/12 3,405 5,699 7,417 7,799 7,799 7,799 6,168 6,764 6,764 0 6,764

1
Agenda Item 10
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
CHIEF EXECUTIVE’S REPORT
PURPOSE
To draw the Board’s attention to key issues.
RECOMMENDATION
The Trust Board is asked to discuss and note the contents of the attached report.
Christine GreenChief Executive14 February 2012

2
Annex 1
1. Quarterly Cleanliness Compliance
The cleaning services provided by MITIE are continually assessed by inspectionsundertaken jointly by MITIE and Trust staff. The areas are classified in four riskcategories, in accordance with national standard specifications. The pass score andthe scores achieved for November, December 2011 and January 2012 are shown inthe table below.
Risk Category Pass Score Nov2011 Score
Dec2011 Score
Jan2012 Score
Very High Risk 98% 99% 99% 99%High Risk 95% 97% 97% 97%Significant Risk 85% 94% 95% 95%Low Risk 75% 95% 88% Nil
Each room is assessed against more than 20 detailed criteria, and the room scoresare averaged to provide the overall performance score. The pass score is thepercentage score the contractor must achieve to avoid any financial penalties in theirmonthly payment from the Trust, and it is clear that the required level of performanceis being achieved.
The score for low risk areas remains lower than for other risk categories, reflectingagreed and appropriate reductions in cleaning frequency in those areas. Howeverthe scores remain within an acceptable range and the performance in these areascontinues to be closely monitored. Formal cleaning audits in low risk areas now onlytake place quarterly, therefore no figures are returned for low risk areas in January2012.
2. Revalidation of Medical Practitioners
Planning is under way to introduce revalidation for licensed doctors towards the endof 2012. Doctors will revalidate usually every five years by having annual appraisalsthat are based on the General Medical Council’s core guidance for the medicalprofession, Good Medical Practice. Revalidation is intended to give furtherassurance to patients, employers and other health professionals that doctors are upto date and fit to practise. It will contribute to improving the quality of care receivedby patients by ensuring doctors practise in an environment with a strong focus oneffective clinical governance and medical human resource management.
NHS Foundation Trust’s, are expected to ensure they have robust systems in placeto support doctors with revalidation. These systems include providing effectiveannual appraisals for all licensed doctors practising in their organisations and strongsystems of clinical governance.
In accordance with the Medical Profession (Responsible Officers) Regulations 2010which came into force on 1 January 2011 the Trust has appointed Tariq Mahmoodas the “Responsible Officer”. The regulations place a statutory duty on “ResponsibleOfficers” to ensure doctors are appraised annually and to investigate (and refer to

3
the GMC where necessary) any concerns about a doctor’s fitness to practise. The“Responsible Officer” makes the revalidation recommendations to the GMC aboutdoctors working in the Trust.
The Medical Director and HR Director have been charged with developing a systemto ensure all doctors are systematically revalidated. A further report will be providedto the Board in August 2012.
3. Medical Director
Tariq Mahmood’s appointment as Medical Director has been extended for a furtherthree years. This follows an open and transparent process through which allconsultant medical staff were invited to express an interest in the position if they toowished to be considered.
4. Emergency Planning
The Trust has put in place a number of measures to ensure it remains in a state ofpreparedness for emergencies and unplanned events, and to discharge its legalobligations in respect of the Civil Contingencies Act, 2004. The programme of workis coordinated by the Emergency Planning Group, which meets every quarter andreports to the Risk Management and Corporate Governance Committee. TheCommittee works to an annual plan, which covers the updating of BusinessContinuity Plans, guideline and policy development, training events and incidentsimulations.
Since the last report, the Trust’s Executive Directors, any of whom could be calledupon to assume the role of Hospital Control Centre Manager in a major incident,have been “walked through” the Trust’s plan by the Director of Nursing in theHospital Control Centre in Werneth House. Every such exercise identifies potentialmodifications and improvements, and in this case a requirement for updated I.T. andtelecoms equipment was identified. The Trust has also sent staff to a Burns exerciseat the University Hospital of South Manchester and this identified a number oftraining needs for the hospital, which are the subject of specific action.
At the request of the Greater Manchester Resilience team, the Trust has made somemodifications to its Major Incident Plan in response to the possibility of receiving highprofile casualties during the period of the Olympic Games.
5. Annual Plan
As the Board is aware Foundation Trusts are required to develop an Annual Plan forsubmission to Monitor. Monitor use the Trust’s forward planning data to inform theTrust’s risk rating in relation to finance, governance and mandatory services.Clearly, the Annual Plan acts as a vehicle to progress the Trust’s strategic directionand goals.
In 2011/12 the Trust’s Annual Plan comprised of six main sections included in atemplate provided by Monitor. The table below provides a description of the 6

4
sections. Although Monitor has yet to advise the approach for 2012/13, it is unlikelyto be significantly different.
Section Description1 Strategy The Trust’s current position and vision
The Trust’s strategy over the next 3 years Key priorities
2 Externalenvironment
Summary of national & local key external impacts
3 Summaryfinancialcommentary
A summary of the current financial state of the trust Key assumptions made in compiling the financial plan A synopsis of the material changes over the three
years of the plan4 Trust plans
Financial plans Income Service developments Activity and costs Workforce Capital programmes (including estates strategy)
Clinical plans Quality accounts Measures to improve clinical quality Safeguarding patient safety
Other priorities Other strategic priorities not covered in the sectionsabove
5 Regulatoryrequirements
Current and future regulatory risks
6 Leadership &Governance
Key leadership and governance priorities
The Annual Plan for 2012/13 is due to be submitted to Monitor by 31st May 2012. Itis therefore proposed that the Annual Plan forms the basis of a joint Council ofGovernors and Trust Board Seminar once a substantial portion of work has beencompleted and endorsed by the Trust Executive. The Board Seminar scheduled for18 April would be ideal, as this would be prior to the final approval of the Annual Planat the May meetings of both the Board and the Council.
6. Greater Manchester Cluster Integrated Plan
Having reviewed the Greater Manchester Cluster’s Operating Plan for 2012/13 whichincludes local commissioning plans the following information is of particular interestto the Trust.
Key areas of service focus include:
- Improving performance – 18 weeks, A&E, HCAI, Cancer

5
- Service realignment across Greater Manchester – the “safe and sustainable”strategy
- Clinical strategy. Service transformation, e.g. Pathology, End of Life Care,Acute Oncology and Urgent Care
- Development of Clinical Commissioning Groups
- Shadow form for Health and Wellbeing Boards from April 2012
- QIPP - with required savings of £369m across GM from 2011-15 (NHS T&G£22.2m)
The Financial issues as they relate to T&G PCT indicate a 3 year financial plan withtotal growth £113m (2012/13 £43.1m). The PCT’s plan shows growth of £11m, arecurrent surplus of £8.1m, lodgements of £3m. It also indicates a QUIPP of £4.8mwith a risk contingency £11m against it.

1
Agenda Item 12
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
CQC ACTION PLANS
PURPOSE
To provide the Board with an update on progress against the Trust’s two CQC actionplans.
DISCUSSION
The Board is aware of the two action plans which the Trust has been required toproduce. One of these is in response to the CQC report (Annex 1) and the other inresponse to the Warning Letter (Annex 2). Both plans are attached, and have beenupdated as at 16 February, 2012. The Board will recall discussing and endorsingboth items at the January Board meeting.
The action plans are by intention relatively brief summary documents, so thefollowing narrative identifies key changes and developments undertaken in responseto the plans. The Board will recall that an underlying objective is to change theculture to become more proactive and less reactive, and so that staff at all levels ofthe organisation feel empowered and recognise and accept a level of responsibilityand autonomy commensurate with their position. The action plans also go beyondthe immediate implications of the CQC Report and Warning Letter, as it is clearlyessential to secure permanent and effective change.
As the action plan produced in response to the CQC report (Annex 1) subsumeseverything which is in the plan produced in response to the warning letter (Annex 2),the narrative which follows focusses on the former item. Evidence relating to theprogress made against the plan will be available for perusal by Board members. Alist of evidence generated to date is given at Appendix A to this report.
Narrative
Outcome 4: Care and welfare of people who use services
Four senior nurses from the University Hospital of South Manchester (UHSM)undertook a review of ward practices within the hospital on 10 February 2012.Verbal feedback was given and written feedback will also be provided. The briefverbal feedback indicated that care observed was good, with a supportive teamethic. The quality of documentation was also reported to be good, with consistentand appropriate follow through of actions identified as necessary. The team felt thatward staff now understand the importance of effective documentation andrecommended that the daily documentation audits which had been taking place inresponse to outcome 16 could be reduced to weekly, so that this does not becomecounter - productive.

2
The team also observed that there is scope for further rationalisation of nursingdocumentation (as in all health care settings), and that staff have embraced theenhanced autonomy they have for issues such as discharge arrangements andundertaking and acting on ward documentation audits.The UHSM nurses also noted and commented on the levels of bed occupancy andbed pressures in the hospital, commending the nursing response. The Board isreminded that securing a recurrent bed base consistent with the numbers and needsof the patients using the hospital is a key contractual objective in the Trust’snegotiations with the Commissioner for 2012/13.
Outcome 5: Meeting nutritional needs
As noted in the action plans, the Trust has provided a “Back to Basics” EducationalProgramme for all Ward Managers. This concluded on 8 February, 2012 and WardManagers are expected to cascade the training to their junior staff. The Back toBasics Training is an important part of the cultural change which the Trust seeks toachieve, and covered the following:-
Effective patient assessment and care planning Documentation to a high professional standard Confidentiality and storage of healthcare records Medicines Management Expectations of ward managers in their leadership role
The first four parts were delivered by internal Trust staff, whilst the fifth was deliveredby an external training manager and took the form of a learning day away from theclinical area.
Outcome 9 – Management of Medicines
The measures required to ensure the safety and security of medicines across thehospital site, and to ensure that an up to date copy of a medicines reference bookknown as the British National Formulary were implemented with immediate effect.The effectiveness of the measures is monitored by ward staff, the hospital’s wardpharmacists, and the Executive Directors via the Ward Sponsorship process (seeOutcome 16 below).
Outcome 13: Staffing
The additional demands on the hospital’s in - patient beds and the Trust’s goal ofminimising nursing redundancies has meant that this has been a challenging area inrecent months. As the final redundancy figure is now known, interviews wereconducted on 16 February, 2012 and all vacant established posts have beensuccessfully recruited to.
In addition, the Board is aware that securing a recurrent bed base is a significantcontractual objective, in order to reduce the risks and interruptions in the continuity of

3
care which may be associated with the short term opening and closing of beds usingnon – recurrent funding. The changes proposed for the MAAU are dependent uponthe provision of additional recurrent funding from the PCT as part of the 2012/13contract settlement.
Outcome 16: Assessing and monitoring the quality of service provision
A number of important actions have been taken in response to this outcome. Thisincludes daily ward led “learning audits” of nursing records in all areas, which havenow been reduced to weekly, as indicated above. These audits are supplementedby additional audits by Matrons and Divisional Nurse Managers.
Director “Sponsorship” of wards has also been introduced, in which each Directortake a special interest in a group of wards, visiting at least one each week to checkcompliance with CQC standards and outcomes. As well as providing support toclinical areas, this has also identified a number of areas in which individual areasneed to improve to maintain compliance with CQC outcomes, for exampleincomplete documentation, poorly coordinated escalation area, drug trolley notsecured to the wall, out of date signage and information. The principle has beenextended to the Non - Executive Directors, who, like the Executive Directors willcease using the IHI model and instead use a checklist which relates to CQCoutcomes. Use of the new checklist for NEDs begins with their next set of wardvisits.
The direct linking of audit and assessment processes to CQC outcomes is furtherdeveloped via the replacement of the Matrons’ Round audits with the CQC outcomesbased “Essential Standards of Quality and Safety” framework. This will be used toassess compliance with outcomes and reinforce the accountability which individualward managers and nurses hold for the quality of service in their area. This wasdescribed in some detail at the January Board. All clinical areas will have undergonean audit using this tool by the end of February 2012.
The Director of Nursing has met with RSM Tenon, Internal Auditors, to agreeprocesses which will provide an early view on the sustainability of the changes madein respect of documentation and audit, supplemented by a follow up audit later in theyear. The first stage of the audit process will commence on 28 February, 2012.
Outcome 21: Records
The measures required to ensure the appropriate access to healthcare records wereimplemented with immediate effect, with a number of wards fitting additional doorlocks or purchasing lockable storage trolleys for notes. Compliance is monitored byward staff, and the Executive Directors via the Ward Sponsorship process (seeOutcome 16 above).
CONCLUSION
Good progress is being made against all aspects of the plans, in line with theprescribed timescales.

4
RECOMMENDATION
The Board is asked to discuss and note progress against the attached action plans,and in particular to determine whether any additional measures are required toprovide assurance to the Board about the changes made and their sustainability.
Philip DylakDirector of Nursing16 February, 2012

5
Appendix A
List of evidence generated to date
Outcome 4: Care and welfare of people who use services
Visit programme.
Report on visit – anticipated week commencing 27 February.
Outcome 5: Meeting nutritional needs
“Back to Basics” programme materials
Back to Basics attendance log
Outcome 9: Management of Medicines
Feedback reports from Executive Director sponsorship visits.
Compliance reports – Pharmacy Department
Purchase orders – additional equipment and locks
Pharmacy process for ensuring wards copies of BNF are up to date
Outcome 13 – Staffing
Trust operational standard supernumerary status
Ward budgeting exercise documentation
Staffing plan, MAAU
MAAU to AAU conversion plan
Revised documentation – MAAU
Corporate Risk Register
Outcome 16: Assessing and monitoring the quality of service provision
Records of daily learning audits

6
DNM/Matron monthly audit reports
Executive Director reports – ward sponsorship visits, and documentation evidencingfollow up actions
RSM Tenon Audit Schedule
Essential Standards of Quality and Safety Framework (reports to be available fromall areas by end of February 2012)
Outcome 21: Records
Executive Director reports – ward sponsorship visits, and documentation evidencingfollow up actions in relation to appropriate storage of health records

1
Action Plan Produced in Response to CQC Report

2
ANNEX 1 - ACTION PLAN PRODUCED IN RESPONSE TO CQC REPORT – UPDATED 16 FEBRAURY 2012 (v 1.2)
CQC FINDING OBJECTIVES ACTIONS AND ACCOUNTABLE OFFICER TIMESCALE ANDPOSITION AT 16FEBRUARY, 2012
Outcome 4: Care and welfare of people who use services
There were a number ofinconsistencies and inaccuracies inthe records. This meant that peoplewere not put on the correct carepathways or did not have theequipment needed to prevent falls.
Patients who were at risk of fallshad no clear plans in place tomanage these risks. Assessmentswere not complete or reviewedwhen required and some wereinconsistent with other informationabout the patient
Consistency between thepatient assessment, theplan of care, the patientdocumentation and anyfollow up actions required.
The ward has fullydocumented the degree offalls risk for all eligiblepatients and all relevantadditional information.
Any information on “whiteboards” (e.g. falls ornutrition risk) is consistentwith the warddocumentation
Director of Nursing has met with Director of Nursing fromUHSM to agree a process whereby senior nurses fromUHSM will review patient documentation in use atTameside Hospital FT, to ensure that patient assessmentis carried out correctly, documented appropriately, and thatany patient risks identified are followed through properly.
The UHSM nurses will also conduct focus groups withnursing staff to obtain their views on compliance issuesand how they can be resolved.
The UHSM nurses will report their findings to the Directorof Nursing and further actions will be determineddepending on the outcome.
(See also actions in respect of outcome 5).
Accountable OfficerPhilip Dylak, Director of NursingLiz Penny, Matron, Support to Director of Nursing
Four Senior nurses fromUniversity Hospitals ofSouth Manchester workedwith the hospital 10February, 2012. Verbalfeedback given – writtenfeedback to be produced.
Action plan will be updatedon receipt of the feedback.
Outcome 5: Meeting nutritional needs
Accurate and up to date records ofhow much people ate and drankwere not always kept.
Weights and body mass indexes(BMI) were not being accuratelyrecorded and updated.
Records did not always confirmthat appropriate action was being
Ward staff “own” the issueof accurate recording of allpatient data, includingnutritional and hydrationintake and output. Therecords are complete andconsistent with patientneed.
“Back To Basics” Educational Programme for WardManagers which will then be cascaded to other membersof the ward team and will include:-
Effective patient assessment and careplanning
Documentation to a high professionalstandard
Confidentiality and storage of healthcarerecords
Medicines Management
Programme commencedweek commencing 23January 2012 andcompleted 8 February 2012.

3
taken in response to weight loss orpoor appetite.
Expectations of ward managers in theirleadership role
(See also actions in respect of outcome 4).
Accountable OfficerPhilip Dylak, Director of NursingDavid Wilkinson, Director of Human Resources
Outcome 9: Management of medicines
Medicines were seen not to besecured appropriately. Weobserved on one ward, during ourvisit, that an unlocked drug trolleywas left in a clinic room.
On one nurse station we found a2009 copy of the British NationalFormulary (BNF).
Medicines to be storedsafely and appropriately inall areas.
Sources of reference usedat ward level to be currentand appropriate
All staff have been reminded that this is a disciplinaryoffence. Checks on existing medicines security measureshave been carried out in all parts of the hospital andadditional measures put in place where required.
The nurse who left a drug trolley unlocked at the time ofthe CQC visit has been identified and disciplinaryproceedings implemented.
Ward managers and their staff have been reminded thatthey will be held fully accountable for breaches and thatany member of staff leaving a trolley unlocked will bedisciplined.
Pharmacy Department will also monitor compliance withthis requirement via their ward audits and routine visits.
Each area has checked and removed any out of datecopies of BNF.
The Pharmacy Dept. will issue copies of the BNF to wardstwice each year and ward pharmacists will check thecurrency of BNFs used in clinical areas on their wardvisits.Issues also monitored via Executive Director sponsorshipwalk rounds.
Accountable OfficerPhilip Dylak, Director of NursingKaran Shingler, Alice Baxter, Lesley Tones, StephenMcLaughlin, Karen Rowland - Divisional Nurse ManagersTony Sivner, Chief Pharmacist
All measures implementedand follow up arrangementsin place.
No additional actions atpresent.

4
Outcome 13: Staffing
The Trust’s operational standarddocumented that band 7 staffshould undertake a minimum of 2by 7.5hr shifts per weeksupernumerary status. During ourvisit some staff told us thatsupernumerary time was notprotected and was sometimes usedto cover staff absences.
During our visit we observed thatone ward had a staffingestablishment for 39 beds. Thisestablishment did not take intoaccount two additional four bedbays or attending to up to eightpatients accommodated in sit outareas. Staff also told us that it wasdifficult to identify any time for teammeetings to discuss and sharelearning from incidents.
Each area covered by theoperational standard tohave 2 supernumerary daysward leader per week.
Establishment of MAAU tomatch workload.
MAAU ward leaders toensure staff have breaksand receive updates
Divisional Nurse Manager for the area concerned hasreiterated this requirement and is monitoring it.
Trust committed to maintaining at least 0.4 wte in wardbudgets to enable this standard to be met in the areas towhich the standard applies.
Accountable OfficerPhilip Dylak, Director of NursingKaran Shingler, DNM
Trust has agreed increase to nursing workforce in MAAU.Agreed changes will be implemented according to plan aspart of wider actions to redesignate MAAU as an AcuteAdmissions Unit (AAU). This change will recognise theunit’s role in accepting all medical and appropriate surgicaladmissions, and the medical and nurse staffing will beadjusted accordingly. The Unit will work to an agreeddesignated number of beds and assessment bays. Therewill be zero tolerance for expansion of the Unit beyond itsestablished configuration.Investigation of the arrangements for breaks, training etcon MAAU indicated that improved organisation couldensure the standards are met The required changes havebeen implemented and will be monitored by the Matronand Divisional Nurse Manager.
Accountable OfficerPhilip Dylak, Director of NursingTariq Mahmood, Medical Director & Paul Williams, Directorof Clinical Services
To ensure that the level of detail recorded in nursingrecords is consistent with the time the patient will spend inthe unit and to reduce the burden of unnecessarydocumentation on unit staff, MAAU documentation has
Ward budgeting exerciseincorporates thisrequirement. Somedifficulty in achievingsupernumerary status dueto bed pressures andholding vacancies – as thefinal redundancy figure isnow known, restriction lifted,interviews conducted 16Feb 2012, and vacantestablished posts recruitedto.
The target date forimplementing the changesis the end of May 2012. TheTrust needs to finalise thefinancial implications withPCT as part of its contractnegotiations for 2012/13.
Further work to beundertaken in respect of theplan.
Review complete. TrustDocument Assurance Grouphas commenced year longproject to review all nursing

5
been reviewed and rationalised.
Accountable OfficerPhilip Dylak, Director of NursingNasrin Khadim, Assistant Director of Nursing
and midwiferydocumentation in use in theTrust – due to complete midFebruary 2013. Followingfeedback from the UHSMnurses, the pace of changewill be accelerated andthere will be greater wardstaff participation in anumber of sub groupsassociated with the process.
During our visit we reviewed theaccident and emergency serviceredesign programme. The trust hadcarried out a quality and safetyimpact assessment beforeimplementing the changes. Anumber of key risks were identifiedduring the assessment process. Itwas not clear from the documentsprovided by the trust how thesewould be monitored and managed.
Clear pathway for managingrisk related to CIP schemes.
Any issues would be dealt with via the Executive DeliveryGroup, which meets weekly under the chairmanship of theChief Executive. Significant issues would be dealt with viathe usual managerial routes, as appropriate, and would beadded to the divisional or corporate risk register.However, the process of Quality Impact Assessment,which occurs three times in the life of each project, shouldensure that risks are identified and mitigated in a timelymanner.
Accountable OfficerTariq Mahmood, Medical DirectorPhilip Dylak, Director of NursingDavid Jago, Director of Finance
Structures and processeswell established
Issue added to CorporateRisk Register at lastiteration (February 2012)
Outcome 16: Assessing and monitoring the quality of service provision
The Trust’s audit and monitoringsystems still lack sufficient rigor toidentify and escalate risk issues.The (documentation) audit showed97% compliance. We reviewed therecords and found that fallsassessment documentation hadbeen completed incorrectly on anumber of occasions.
There were a number ofinconsistencies in the quality of thecompletion of nutritional screeningtools.
Full congruity between auditresults and quality/contentof patient records.
All patient records completeand consistent.
Following meetings between the Director of Nursing andthe Divisional Nurse Managers, Matrons and WardManagers, daily “learning audits” of nursing records havebeen initiated in all areas.
The audits are conducted by the ward manager, with thefocus on the quality and logic of the record.
Should it be found that a record identifies a patient risk(e.g. nutrition, falls, pressure ulcers) which is not followedup, the ward manager will educate the member of staff,pursuing other options if this does not elicit the requiredbehaviour.
System and processesintroduced, and reportingsystem put in place.
Daily audits were completeduntil 10 February, 2012 –with reports to Director ofNursing. Following theirvisits to ward areas, UHSMnurses assessed thatnurses at ward level have“got the message” regardingdocumentation and have

6
The ward managers report on a daily basis to their DNMs,who in turn report to the Director of Nursing. DivisionalNurse Managers and Matrons are also undertaking weeklyaudits to provide additional assurance. Similar principleswill be introduced for the other clinical staff groups workingin the Diagnostic and Therapeutic Division.
Accountable OfficerPhilip Dylak, Director of NursingKaran Shingler, Alice Baxter, Lesley Tones, StephenMcLaughlin, Karen Rowland - Divisional Nurse ManagersTony Sivner, Chief Pharmacist
Director “Sponsorship” of wards scheme introduced inwhich each Director take a special interest in a group ofwards, visiting at least one each week to checkcompliance with CQC standards and outcomes.The Director of Nursing has provided a visiting schedule toprovide structure for the Directors when they undertaketheir visits, and a means of feeding back theirobservations.(NB this supplements the existing and well establishedprogramme of patient safety walkrounds)
Accountable OfficerMel Laskey, Director of Strategy & Performance
To provide additional external perspectives regardingprocesses of care and compliance with CQC outcomesTameside LINk has agreed to use future formal visits tothe hospital to help the Trust in assessing compliance withCQC outcomes.
Accountable OfficerPhilip Dylak, Director of NursingChristine Green, Chief Executive
Director of Nursing has met with Director of Nursing fromLiverpool Heart & Chest Hospital to gain an understanding
recommended reduction infrequency to weekly –implemented 10 February2012.
Reports provided to Directorof Nursing and issues fedback to clinical areas asappropriate. NED visitingschedule adapted toincorporate assessment ofCQC outcomes –programme to commence23 February 2012.
Trust currently finalisingarrangements for a furthermeeting with LINk at whichthis will be one of the issuesdiscussed
Director of Nursing has metwith Senior Nurse

7
During our visit we observed thatmedicines were not securedappropriately, on one ward. We
Medicines to be storedsafely and appropriately inall areas.
of how they use the ESQS (Essential standards of Qualityand Safety) framework to assess compliance withoutcomes and reinforce the accountability which individualward managers and their staff hold for the quality ofservice in their area. This approach will be adopted by theTrust, replacing the existing system of Matron’s RoundsAudits, which has been in use for some time.
Accountable OfficerPhilip Dylak, Director of NursingLiz Penny, Matron, Support to Director of Nursing
Director of Nursing has met with Internal Audit to agreeprocesses which will provide an early view on the changesmade in respect of documentation and audit,supplemented by a follow up audit later in the year.Accountable OfficerPhilip Dylak, Director of NursingDavid Jago, Director of Finance
Personal Responsibility Framework to be implemented forward and shift leaders
Accountable OfficerPhilip Dylak, Director of NursingKerry Lyons, Quality Nurse
Consultant led documentation reviews and medical staffrefresher training on documentation.
Accountable OfficerTariq Mahmood, Medical Director
Please see actions in respect of outcome 9.
Managers, 8 February 2012to agree process. The firstassessment will beundertaken in all areasbefore end of February,2012, with aim for fullimplementation by end ofMarch 2012.
Specification produced byInternal Audit – actions tobe undertaken 28 February,2012.
Aim is to produce andimplement by end ofFebruary 2012.
Medical Director to presentplan to March 2012 meetingof Clinical GovernanceAccountability Committeeon how the reviews will becarried out and how therefresher training will beprovided.

8
observed that the staff seemedunaware that safe storageprocedures were being breached.
We found that medical recordswere not stored securely in two ofthe areas we visited.
During our visit we observed thatone ward, which had recentlyrelocated, had a staffingestablishment for 39 beds. Thisestablishment did not take intoaccount that there were twoadditional four bed bays, in the newlocation, and up to eight patientsaccommodated in sit out areas.Staff on this ward were extremelybusy and told us that it was difficultto identify any time for teammeetings to discuss and sharelearning from incidents.
The trust provided a report, whichdetailed the implications of thetrusts financial recovery plan. Thereport set out the proposals foreighteen workstreams to meet costimprovement programme targets.
During our visit we reviewed theaccident and emergency serviceredesign programme. The trust hadcarried out a quality and safetyimpact assessment beforeimplementing the changes. Anumber of potential negativeimpacts were identified during theassessment process. It was notclear from the documents providedby the trust how these would bemonitored, managed and reviewed
Records are accessible tostaff who need them andare kept secure from thosewho do not.
Establishment of MAAU tomatch workload.
MAAU ward leaders toensure staff have breaksand receive updates
Clear pathway for managingrisk related to CIP schemes.
Please see actions in respect of outcome 21 (third action)
Please see actions in respect of outcome 13 (secondaction)
Please see actions in respect of outcome 13 (third action)

9
as the changes progressed.
Outcome 21: Records
A small number of records (casenotes) had not been signed anddated.
Assessments for risk of falling andnutrition screening tools had notbeen completed accurately in anumber of cases.
Medical records were not storedsecurely in two of the areas wevisited.
Complete and accuratecase notes for all patients
Consistency between thepatient assessment, theplan of care, the patientdocumentation and anyfollow up actions required.
Records are accessible tostaff who need them andare kept secure from thosewho do not.
The Medical Director has reminded medical staff of theirroles and responsibilities in respect of this key professionalrequirement. Medical Director to identify and implementprocesses for ensuring ongoing compliance
Accountable OfficerTariq Mahmood, Medical Director
Please see actions in respect of outcomes 4, 5 and 16
Checks have been carried out in all parts of the hospitaland additional measures put in place where required - anumber of wards have purchased additional locks and/ordocument trolleys to ensure appropriate levels of security.
A specific issue which gave rise to this problem in MAAUhas been addressed.
The issue is monitored via the Executive Sponsorshipward visits.
Accountable OfficerPhilip Dylak, Director of NursingTariq Mahmood, Medical Director
Key action implemented.Medical Director planningConsultant leddocumentation reviews andmedical staff refreshertraining on documentationas per actions in respect ofOutcome 16
All relevant actions havebeen implemented, andmonitoring systems put inplace.

1
Action Plan in Response to CQC Warning Letter

2
Action Plan in Response to CQC Warning Letter - Version 1.2
OBJECTIVES ACTIONS/ACCOUNTABLE OFFICER TIMESCALE AND POSITION AT 16FEBRUARY 2012
1. Assuring the quality of the nursing record, to ensure patient risk is properly identified and acted upon
To refresh and provide newchallenge within the organisationby obtaining external professionalinput.
To use these external sources aspart of the process of addressspecific issues of compliance withdocumentation standards
Director of Nursing has met with Director of Nursing from UHSM toagree a process whereby senior nurses from UHSM will reviewpatient documentation in use at Tameside Hospital FT, to ensurethat patient assessment is carried out correctly, documentedappropriately, and that any patient risks identified are followedthrough properly.
The UHSM nurses will also conduct focus groups with nursing staff toobtain their views on compliance issues and how they can beresolved.
The UHSM nurses will report their findings to the Director of Nursingand further actions will be determined depending on the outcome.
Accountable OfficerPhilip Dylak, Director of NursingLiz Penny, Matron, Support to Director of Nursing
Four Senior nurses fromUniversity Hospitals of SouthManchester worked with thehospital 10 February, 2012.Verbal feedback given – writtenfeedback to be produced.
Action plan will be updated onreceipt of the feedback.
To ensure that there is no lack ofclarity about the leadership roleof ward managers or thestandards for which they andtheir staff are accountable.
To achieve cultural changewhereby “ownership” for issuesat clinical level, and theassociated accountability clearlylie with “shop floor” staff
“Back To Basics” Educational Programme for Ward Managers whichwill then be cascaded to other members of the ward team and willinclude:-
Effective patient assessment and care planning Documentation to a high professional standard Confidentiality and storage of healthcare records Medicines Management Expectations of ward managers in their leadership
role
Programme commenced weekcommencing 23 January 2012 andcompleted 8 February 2012.

3
Implement Personal Responsibility Framework for ward and shiftleaders
Accountable OfficerPhilip Dylak, Director of NursingDavid Wilkinson, Director of Human ResourcesKerry Lyons, Quality Nurse
Consultant led documentation reviews and medical staff refreshertraining on documentation
Accountable OfficerTariq Mahmood, Medical Director
Framework to be devised by 10February, 2012, and rolled out toeach area by 29 February, 2012
Medical Director to present planto March 2012 meeting of ClinicalGovernance AccountabilityCommittee on how the reviewswill be carried out and how therefresher training will beprovided.
2. Ensuring audit accurately reflects compliance and provides a realistic view of the level compliance
To ensure that each nursingrecord accurately identifies andresponds to patient needs, andthat audits of these recordsaccurately reflect the level ofcompliance.
Following meetings between the Director of Nursing and theDivisional Nurse Managers, Matrons and Ward Managers, daily“learning audits” of nursing records have been initiated in all areas.
The audits are conducted by the ward manager, with the focus on thequality and logic of the record. Should it be found that a recordidentifies a patient risk (e.g. nutrition, falls, pressure ulcers) which isnot followed up, the ward manager will educate the member of staff,pursuing other options if this does not elicit the required behaviour.
The ward managers report on a daily basis to their DNMs, who in
Daily audits were completed until10 February, 2012 – with reportsto Director of Nursing. Followingtheir visits to ward areas, UHSMnurses assessed that nurses atward level have “got themessage” regardingdocumentation and haverecommended reduction infrequency to weekly –implemented 10 February 2012.

4
turn report to the Director of Nursing. Divisional Nurse Managersand Matrons are also undertaking weekly audits to provide additionalassurance. Similar principles will be introduced for the other clinicalstaff groups working in the Diagnostic and Therapeutic Division.
Accountable OfficerPhilip Dylak, Director of NursingKaran Shingler, Alice Baxter, Lesley Tones, Stephen McLaughlin,Karen Rowland - Divisional Nurse Managers
Review outputs from the processat Senior Nurse and MidwiferyManagers’ Group monthly.
To provide additional externalperspectives regarding processesof care and compliance with CQCoutcomes
Tameside LINk has agreed to use future formal visits to the hospitalto help the Trust in assessing compliance with CQC outcomes.
Accountable OfficerPhilip Dylak, Director of NursingChristine Green, Chief Executive
Trust currently finalisingarrangements for a furthermeeting with LINk at which thiswill be one of the issues discussed
Action plan to be updated onreceipt.
To identify and implementappropriate means of assessingcompliance with key clinicalstandards and outcomes, usingexternal professional input overthe longer term
Director of Nursing has met with Director of Nursing from LiverpoolHeart & Chest Hospital to gain an understanding of how they use theESQ (Essential standards of Quality and Safety) framework to assesscompliance with outcomes and reinforce the accountability whichindividual ward managers and their staff hold for the quality ofservice in their area.
This approach will be adopted by the Trust, replacing the existingsystem of Matron’s Rounds Audits, which has been in use for sometime.
Accountable OfficerPhilip Dylak, Director of NursingLiz Penny, Matron, Support to Director of Nursing
Director of Nursing has met withSenior Nurse Managers, 8February 2012 to agree process.The first assessment will beundertaken in all areas before endof February, 2012, with aim forfull implementation by end ofMarch 2012.
5
To provide additional assurancesthat that system and processchanges being made in relation todocumentation of planned careare appropriate and will besustained
Director of Nursing has met with Internal Audit to agree processeswhich will provide an early view on the effectiveness of changesmade, with follow up audit later in the year so that sustainability canbe assured
Accountable OfficerPhilip Dylak, Director of NursingDavid Jago, Director of Finance
Specification produced by InternalAudit – actions to be undertaken28 February, 2012.
3. Ensuring medicines are safely and appropriately stored
Zero tolerance for unlocked drugtrolleys
All staff have been reminded that this is a disciplinary offence.
Checks on existing medicines security measures have been carriedout in all parts of the hospital and additional measures put in placewhere required.
The nurse who left a drug trolley unlocked at the time of the CQCvisit has been identified and disciplinary proceedings implemented.
Ward managers and their staff have been informed that they will beheld fully accountable for breaches and that any member of staffleaving a trolley unlocked will be disciplined
Pharmacy Department will also monitor compliance with thisrequirement via their ward audits and routine visits.
Accountable OfficerPhilip Dylak, Director of NursingKaran Shingler, Alice Baxter, Lesley Tones, Stephen McLaughlin,Karen Rowland - Divisional Nurse Managers
All measures implemented
The issue is monitored via theExecutive Sponsorship ward visitswhich take place weekly on asample basis.

6
4. Ensuring healthcare records are accessible but secure in the clinical area
Records are accessible to staffwho need them and are keptsecure from those who do not.
Checks have been carried out in all parts of the hospital andadditional measures put in place where required - a number of wardshave purchased additional locks and/or document trolleys to ensureappropriate levels of security.
A specific issue which gave rise to this problem in MAAU has beenaddressed.The Medical Director has reminded medical staff of their roles andresponsibilities in respect of this key professional requirement.
Accountable OfficerPhilip Dylak, Director of NursingTariq Mahmood, Medical Director
All measures implemented
The issue is monitored via theExecutive Sponsorship ward visits.
The issue is monitored via theExecutive Sponsorship ward visitswhich take place weekly on asample basis.
5. Matching workload and staffing on the Medical Assessment and Admissions Unit
Ensure staffing is consistent withworkload.
As part of the Trust’s Time to Care programme, the Trust isaccelerating plans to redesignate MAAU as an Acute Admissions Unit(AAU). This involves increasing the bed complement from 39 to 52.
This change will recognise the unit’s role in accepting all medical andappropriate surgical admissions, and the medical and nurse staffingwill be adjusted accordingly. The Unit will work to an agreeddesignated number of beds and assessment bays (52). There will bezero tolerance for expansion of the Unit beyond its establishedconfiguration.
To ensure that the level of detail recorded in nursing records isconsistent with the time the patient will spend in the unit and toreduce the burden of unnecessary documentation on unit staff,review and rationalise MAAU documentation
The target date for implementingthe staffing changes is the end ofMay 2012 and AAU changes bythe end of June, The Trust needsto finalise the financialimplications with PCT as part of itscontract negotiations for2012/13, a key objective of whichis to increase the recurrent bedbase.
Review complete. TrustDocument Assurance Group hascommenced year long project toreview all nursing and midwiferydocumentation in use in the Trust

7
Accountable OfficerPhilip Dylak, Director of NursingTariq Mahmood, Medical Director & Paul Williams, Director ofClinical Services
– due to complete mid February2013. Following feedback fromthe UHSM nurses, the pace ofchange will be accelerated andthere will be greater ward staffparticipation in a number of subgroups associated with theprocess.

1
Agenda Item 13
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
MEDICAL DIRECTOR’S DIGNITY IN CARE REPORT
Purpose
To present an audit of medical staff leave over the 2011 Christmas holiday period aspart of the 2011/12 Medical Directors Dignity in Care (DIC) programme.
Discussion
The DIC Programme 2011/12 assessed 4 key areas of consultant professional practicewith a view to providing guidance on best practice, developing policies to incorporatethis guidance and implementing the policies to manage behaviour:
- consultant leave- senior medical staff cover over public holidays- recommended numbers of consultants away at any one time- consultant ward rounds
Whilst these behaviours are to be expected all year round, it was felt important to auditthis over the critical Christmas holiday period. There is evidence to suggest thatsignificant depletion of senior medical staff can occur during the Christmas and NewYear bank holiday period due to extensive use of annual leave resulting in increasedrisk to patients. This is particularly the case for adult medicine where the clinical activityand admission rates can be very high.
Planning and managing medical staff leave for Christmas 2011 was more structuredand timely than in 2010. All consultants were written to by the medical director askingfor their support in ensuring implementation of best practice. Consultants were asked to:
- review their own patients just before the Christmas leave began (Friday 23rdDecember) and ensure that all patients under their care had management plansreviewed and an effective hand over to the on-call teams.
- review patients on the first day back from leave even if their formal ward roundwasn’t scheduled for that day.
- ensure best practice with respect to numbers of consultants away at any onetime with particular reference to the 28-30th December 2011 (i.e. normal workingdays).

2
Audit of consultant leave over Christmas 2011
Table 1 shows the bank holidays over the Christmas period. In the planning phase, itwas anticipated that strategic leave taking on December 23, 28, 29 and 30 could resultin a significant depletion of consultants. By taking these 4 days as annual leave, staffcould be off for 11 consecutive days. This was witnessed to some extent in 2010.
Table 1; Bank Holidays, Christmas 2011
As demonstrated in Table 2 consultants complied well with the recommendations forconsultant leave.
Table 2; Numbers of consultants on leave at any one time (December; 23, 28, 29 and30)
Department Total No. ofconsultants indepartment
Recommended No.of consultants onleave at any onetime
Actual No. ofconsultants on leaveat any one time
Surgery 8 3 3-4O&G 9 3 1-2Paediatrics 9 3 1-2Adult medicine 17 5-6 3-6Orthopaedics 9 3 3-4Radiology 8 3 3A&E 7 3 2Anaesthetics 16 5-6 4-8
Additional consultant cover
In adult medicine, additional consultant cover was provided over the extended bankholiday period to support the on-call teams. This ensured timely discharge of patientsand enhanced patient safety.
Fri 23rd DecemberSat 24th
Sun 25th
Mon 26th Bank holidayTues 27th Bank holidayWed 28th
Thurs 29th
Fri 30th
Sat 31st
Sun 1st
Mon 2nd Bank holidayTues 3rd

3
Medical Directors Dignity in care programme 2012/13
At the last board the new DIC programme was agreed and involves implementation ofcare bundles and improvements in medical record keeping and clinical documentation.Work on these programmes has begun and details will be provided to the May Board.
Conclusion
Effective management of leave and the provision of additional consultant supportresulted in a satisfactory level of medical cover over the Christmas holiday period.
Recommendation
The board is requested to note the contents of this report
Tariq MahmoodMedical Director16 February 2012

1
Agenda Item 14
NHS STAFF SURVEY 2010 - FINAL PROGRESS REPORT
PURPOSE
To update the Board on the actions and progress following the 2010 Annual NHS StaffSurvey.
DISCUSSION
Trust Board members will recall from previous Board Reports that, overall, the 2010NHS Staff Survey showed a distinct improvement from 2009, with nine key result areas(out of 38) seeing a statistically significant improvement and no areas with a statisticallysignificant deterioration.
The annual NHS Staff Survey is one way staff can give their views to inform actionswhich will address inconsistencies and improve working lives and patient care. Thesurvey results for 2010 were structured around the staff pledges contained within theNHS Constitution.
Updates on the corporate-level actions identified from this year’s Staff Survey are givenbelow – the Divisional-level actions are being progressed through the “SmallConversations approach” introduced last year as part of the Everyone Matters atTameside programme.
Corporate-level Actions
Continued implementation of Everyone Matters at Tameside OD Programme anddelivery of the full action plan arising from the Phase 2 Big Conversations
There has been continued implementation of the Everyone Matters at Tamesideprogramme throughout 2011/12, as Board will be aware from the quarterly updatesprovided by the Chief Executive.
One of the key actions has been the revision of the Staff Charter, which was launchedat a specific event on 13th December 2011. At the event, the Trust Chair, ChiefExecutive, Non-Executive Director chair of the Everyone Matters Steering Group, StaffGovernors and Staffside Chair all formally signed up to the Staff Charter on behalf oftheir respective constituencies – a review of how the Trust is delivering against itsspecific responsibilities under the staff charter is shortly to be undertaken at a TrustBoard Seminar.
A Staff Charter Toolkit has also been developed to support managers, Staff Governorsand Trade Union representatives in utilising the Staff Charter as part of the DivisionalSmall Conversations.
2
Following receipt of the recommendations from the Big Conversation Phase Two, a BigConversation Action Group has been established to progress workstreams in relation toFeedback, Staff Engagement, Internal Communication, Performance, Coaching, 360appraisal, Back to the Floor and Listening.
A full report will be presented to the Everyone Matters Steering Group in March 2012.
The Everyone Matters at Tameside programme has so far been effective in increasinglevels of staff engagement, with the focus for 2012/13 on:
Delivery of the Big Conversation Action Group recommendations and action plan Promotion and use of the Staff Charter Promotion and use of the Values & Behaviours leaflet Promotion and use of a Personal Responsibility Framework
Revised Mandatory Training process
A Mandatory Training Workbook was introduced in Autumn 2010, in order to reduce thereliance on classroom-based teaching and support the move to annual mandatoryupdates.
An e-learning version of the Mandatory Training Workbook went live in November 2011.The electronic version features competency testing at the start of each section – it onlyrequires individuals to complete the full module if the competency test is failed to furtherstreamline the process. The electronic version is also automatically linked to the ESRsystem, reducing data input requirements and improving the accuracy of reporting.
The paper workbook is to be phased out by the end of March 2012 - all staff will beexpected to complete their update electronically from April onwards.
Introduction of Conditional Incremental Progression
In order to improve mandatory training and PDR compliance rates, conditionalincremental progression was introduced with effect from 13th September 2011. Fromthis date, only those employees who are compliant with both PDR and MandatoryTraining receive their annual pay increment.
Overall compliance rates for mandatory training and PDR has been increasing sinceSeptember – whilst the rise in compliance has been rising steadily, this is as a result ofmanagers focusing their attention on the staff that are due to receive their incrementsrather than those whose mandatory training/PDR has expired. The impact of this will belessened as the incremental year moves on.
To date, less than 20 employees have had their incremental progression withheld.

3
With effect from 1st April 2012, it is intended to extend the conditional incremental policyto cover attendance, conduct and capability.
Review of Reward & Recognition Schemes
As part of the Everyone Matters approach, staff opinions have been gathered on thecurrent processes for formal and informal reward and recognition schemes (e.g.Chairman’s Prize, Excellence in Care awards, Long Service Awards, 100% AttendanceAwards, etc).
The report has highlighted that whilst some changes should be made to the formalschemes, it is informal reward/recognition where the attention needs to focus. This willbe picked up with Divisional Teams through the Staff Charter.
The formal schemes are currently being reviewed in light of the report outcomes.
Leadership & Management Development
The OD Strategy is currently being revised to ensure that it fully addresses the Trust’sorganisational objectives. A team-based leadership development programme is beingdeveloped to incorporate the following elements:
Team development Developing financial skills Developing people management skills Developing performance and programme management skills Developing service improvement and redesign skills Developing a customer care environment Developing a personal accountability culture
Full review of internal communications systems
As part of the Communications Strategy approved in 2010, an internal communicationsreview has commenced. A revised Team Brief system was introduced in August 2011to improve delivery of key messages through verbal briefings and to ensure 2-wayfeedback – an interim review of the new process has been undertaken in order toensure that it is effective.
A mini-survey for staff on the Trust’s formal communications systems was undertakenthrough Staff Matters in the Summer – the feedback gathered is being used to improvethe existing communication methods, particularly Staff Matters, Staff Online Forum andthe Executive Director Surgeries.

4
Equality Act training
The implications and expectations of the Equality Act are now embedded in themandatory annual update for all employees, either through workbook, e-learning ortaught course. Training on Analysis of Effect (replacing Equality Impact Assessments) isbeing delivered to managers from February 2012 onwards.
The 2012/13 Operating Framework highlights the need for all NHS organisations todeliver against the Public Sector Equality Duties, particularly the recording of progressthrough the Equality Delivery System. E&D training is a key component of this and thetraining programme for 2012/13 is currently being developed.
Enhanced PDR process for managers
The Enhanced PDR for managers at band 7 and above has been a component in thedevelopment of the Performance and Development Plan (PDP). This requires theappraiser and the appraisee to assess the individual’s contribution to the CorporateObjectives, achievement of objectives and goals and modelling the Trust Values.
From early 2012, a quality assurance system has been introduced to undertake samplereviews of the full PDR documentation and short online surveys on the quality andimpact of the PDR being sent to the reviewer and the reviewee.
Framework for linking corporate objectives to individual objectives through Divisional,Departmental and Team objectives
The PDP Documentation includes the requirement for managers to make explicit linksto the Corporate Objectives when setting objectives at Divisional, Specialty/Team andindividual level, so that all objectives map into one or more of the Corporate Objectives.
Implementation of the Fit for 2012 campaign (including Tameside 200)
One of our biggest actions this year has been the continued development of Happy,Healthy, Safe through the Tameside 200 programme, with over 200 employeesundertaking periodic lifestyle/health checks and fitness testing in the run up to the 2012Olympic Games.
All participants in the Tameside 200 campaign are required to sign up to at least onecommitment to improve their health and wellbeing – this vary from a major organisedactivity (e.g. GM Run, GM Swim, Manchester – Blackpool cycle ride, etc) to moreinformal activities (e.g. pledges to lose weight, participation in on-site Zumba classes,team games, etc).

5
There is particular interest in walking, cycling and swimming and those who haveexpressed an interest have been put in contact with each other, together with volunteerswho have offered to help organise specific activities.
As a result of this initiative, the Trust has been awarded the Inspire Mark, a nationallyrecognised endorsement of organisations supporting and promoting the health of theirworkforce.
Revise and relaunch the Attendance Management Policy
The policy has now been revised and is shortly to be approved and launched. Therevised policy and associated actions will ensure that the Trust maintains its position ofbetter than average levels of attendance in the North-West.
Continued implementation of Board to Ward activities
There are already well-established systems in place for Executive and Non-ExecutiveDirector visits to clinical areas, as part of the Patient Safety Walkarounds and the Backto the Floor activities.
Zero Tolerance campaign to address physical and verbal abuse against staff
A comprehensive action plan has been developed - actions include re-establishing thePolice Room in A&E and a publicity campaign to deter violence and aggression againststaff.
The Violence & Aggression Policy is in the process of being revised, with a majorcampaign on security and personal safety planned to coincide with Security Awarenessweek in September.
Feedback has been sought directly from Nursing staff as to their concerns and theirperceptions of effective action from the Trust in maintaining their safety.
A display on the recent Trust Safety Day on security and personal safety was held inconjunction with GMP. A supporting article is to go in the next Staff Matters and thecampaign is highlighted during the Mandatory Conflict Resolution Training.
2011 Staff Survey
The 2011 NHS Staff survey closed in December. The final NHS Survey report for 2011is expected in March 2012.

6
Board should be aware that the timing of the staff survey coincided with the end of theworkforce consultation and start of the implementation phases for the 2011/12 CIPschemes, which will undoubtedly impact on the results.
The survey and findings action plan will be submitted to the Board in April.
RECOMMENDATION
The Board is requested to discuss and note of this report.
David WilkinsonDirector of Human Resources20th February 2012

1
Agenda Item 15
Tameside Hospital NHS Foundation Trust
Risk Management and Health & Safety ReportOctober – December 2011 (Quarter 3)
PURPOSE
To inform the Board of the Trust’s performance in relation to a number of key riskmanagement and health and safety indicators for this quarter.
DISCUSSION
The information in the annex to this report is reviewed in depth by the RiskManagement Committee and is appended for information. The following paragraphshighlight the main trend data in the annexed report:-
1. Total Incidents Reported
A total of 1235 incidents were reported in this quarter which is an increase from theprevious quarter’s total of 997. During the quarter, the Security Department began torecord incidents on the Trust’s main incident system, whereas previously they hadbeen recorded on a stand - alone system. It was expected that this would lead to anincrease in reported incidents, but the threshold for reporting also appears to havechanged. The Risk Management and Security Departments are working together toensure that there is clarity over what constitutes an incident, what should bereported, and the correct processes for doing so.
2. Incidents Requiring Police Attendance
A total of 45 incidents required police assistance during this quarter, which is anincrease from the previous quarter’s total of 31.
3. Reporting of Injuries and Diseases Dangerous Occurrence Regulations(RIDDOR)
Five RIDDOR incidents were reported in the quarter. The number of incidents whichoccur is too small to allow any trend to be identified.
4. Health & Safety Executive Inspections and Visits
No HSE inspections were carried out on site in the quarter.
5. Serious Clinical Incidents (Red incidents)
During Quarter 3, three reported incidents were confirmed as “red” by the Qualityand Clinical Governance Committee.

2
6. Examples of actions taken as a result of an incident
This section provides the above summary.
7. Complaints Received
During October-December 2011, 85 complaints were received. This is in line withestablished trends.
8. Claims Received
There have been 22 new claims received, a slight increase as compared to theprevious quarter.
9. Multi Agency Child Protection Reviews
There have been no new serious case reviews during this quarter.
RECOMMENDATION
The Board is asked to discuss and note the content of this report.
Philip DylakDirector of NursingFebruary 15, 2012

3
Annex to Risk Management and Health & Safety ReportOctober-December 2011 (Quarter 3)
1. Total Incidents Reported
1.1 Summary of all Incidents
The following table summarises all incidents reported during the quarter, and in theprevious four quarters. Each incident type is discussed further in the report. Theincrease in incident reports received is largely due to changes in the reporting ofsecurity incidents.
Incident Type Oct-Dec 10
Jan-Mar11
Apr-Jun 11
Jul-Sep 11
Oct-Dec 11
Contractor\ Non TrustEmployee
2 2 0 2 2
Other (not related to specificperson)
35 26 36 48 35
Patient 946 1049 911 812 895Staff 113 136 125 126 284
Visitor 4 4 5 9 19Total 1100 1217 1077 997 1235
1.2 Severity of all Incidents
This section in the report provides numbers of incidents by grade. The majority ofincidents that are recorded are of a low grading. Three incidents during this periodwere reported to StEIS.
Quarter /Year
Number of incidentsVeryLow
Low Moderate High Totals
Oct-Dec 10 3 1088 6 3 1100Jan-Mar 11 57 1139 19 2 1217Apr-Jun 10 161 899 15 2 1077Jul-Sep 11 5 978 10 4 997Oct-Dec 11 37 1181 14 3 1235
1.3 Patient Accidents/Incidents
During Quarter 3, 895 incidents were reported which related to a specific patient(incidents relate to both the patient’s episode of care and to any incidents whichinvolve a specific patient’s medical records). This is an increase on the last quarterbut is within the established range of values.
The table overleaf identifies the number and type of patient incidents in this quarterand in the previous four quarters. Patient slips, trips and falls increased slightly inthe last quarter but still show a tangible overall reduction. An extensive work plan

4
has been implemented via the Trust’s Safety Express Group to reduce the numberand severity of these falls and this continues to be monitored closely.
The Board has previously been advised that the apparently high number ofspecimen errors is related to very diligent reporting of any situation in which threefully consistent patient identifiers do not accompany a sample sent to the lab foranalysis. The figure of 174 reports is therefore very positive, given the 120,000specimens processed during the quarter. The figure has reduced further for thisquarter and is the lowest value recorded in the period covered by the report.Continuing compliance to the zero tolerance policy on specimen samples should seethis figure continue to decrease.
There was an increase in the number of reported absconds or self - discharges. Theincrease is marked, and was further investigated by the Risk ManagementDepartment. There were two main reasons for the increase. Firstly, one patient leftthe ward on a number of occasions. Secondly, during the quarter, the SecurityDepartment began to record incidents on the Trust’s main incident system, whereaspreviously they had been recorded on a stand - alone system. It was expected thatthis would lead to an increase in reported incidents, but the threshold for reportingalso appears to have changed. The Risk Management and Security Departmentsare working together to ensure that there is clarity over what constitutes an incident,what should be reported, and the correct processes for doing so.
Patient Accidents/Incidents
Patient Accident / IncidentType
Oct-Dec10
Jan-Mar 11
Apr-Jun 11
Jul-Sep 11
Oct-Dec11
Absconded/Self Discharge 14 15 19 13 61Accidental Injury 20 26 14 13 13Assault: physical & verbal 5 4 9 17 9Blood products 5 1 2 4 1Bullying & Harassment -- -- -- -- --Consent / Communication 31 33 30 22 31COSHH -- 1 -- -- --Documentation 43 48 66 79 66Diagnosis -- -- -- -- --Dispensing Error -- -- -- 3 --Equipment 24 27 16 5 8Failure to follow procedures 10 11 12 5 7Fire 2 -- -- -- --Impact/Collisions -- 1 1 --Infection Control (HCAI Deaths) -- -- -- --Manual Handling -- -- -- 1Maternity Incident 9 14 26 40 43Medical Care 21 38 53 44 31Medication Error 16 25 22 21 16Medical Equipment 1 16 7 6 16Nursing Care 24 41 31 26 14Other 47 17 11 37 35Patient Transfers 31 27 25 20 20

5
Pre-existing Condition 5 28 23 10 32Pressure ulcers hosp acquired(grade 3\4)
-- -- 1 1 --
Pressure ulcers (non hospital) * -- -- -- -- --Safeguarding Adults 32 28 24 14 8Security 8 2 7 16 34Self Injury/suicide 2 -- 2 2 6Sharps/Needlestick -- 2 -- 1 1Slips/Trips/Falls 301 342 273 224 267Smoking -- 1 2 1 1Specimen Error 295 302 235 187 174
Total 946 1049 911 812 895
1.4 Slip, trips and falls
The table above indicates that the overall number of falls was 267. The vast majorityof slip/trips/falls incidents were graded low or very low. There were also two highgraded falls, which have been discussed by the Quality and Clinical GovernanceCommittee. All high and moderate falls incidents are subject to a full Root CauseAnalysis investigation. Actions implemented from RCA investigations have beendesigned to ensure that A&E and MAAU are working to Trust policy and procedurewith respect to the Trust falls programme, “Falls are Everybody’s Business”.
1.5 Staff Accidents / Incidents
A total of 284 staff accidents or incidents were reported during Quarter 3, ascompared to 126 for the previous quarter. The number of physical or verbal assaultsrecorded increased during this quarter. This was an expected increase due tochanges in the way the Security Department record incidents, as noted in paragraph1.3 above.
Staff Accident \IncidentType
Oct-Dec 10
Jan-Mar11
Apr-Jun 11
Jul-Sept
11
Oct-Dec 11
Accidental Injury 16 18 22 15 19Assault: physical & verbal 47 61 44 46 145Bullying & Harassment 2 -- -- 2 3Communication\Consent 1 1 -- 1 4COSHH 3 2 -- 1 1Documentation 1 3 13 5 2Equipment 3 2 2 5 1Failure to Follow Procedures 2 5 1 1 3Fire -- -- -- -- 1Impact \Collisions 1 10 4 2 1Manual Handling 10 5 6 2 10Medical Equipment 1 1 -- -- --Nursing Care -- -- -- -- --Other (Minor) 5 -- 1 3 6Pre-existing condition -- -- 2 -- 5

6
Security 2 1 8 10 64Sharps \Needlestick 8 14 16 25 14Slips\Trips\Falls 9 12 6 8 5Smoking -- 1 -- -- --Specimen Error 2 -- -- -- --Total 113 136 125 126 284
1.6 Visitor/Non-Trust Employee Accident/Incidents
A total of 19 accidents or incidents were reported which related to a visitor or non -Trust employee. The data is summarised in the following table, and the value isslightly higher than the previous quarters. This has been attributed to more diligentreporting by the Security Department.
Visitor \ Non Trust EmployeeIncident Type
Oct-Dec10
Jan-Mar11
Apr-Jun11
Jul-Sept11
Oct-Dec11
Accidental Injury 2 1 1 1 1Assault: Physical or verbal 2 2 5COSHHEquipment 1Failure to follow proceduresImpact\ Collisions 1 1Manual HandlingOther 2Pre-existing condition 1 2 1 1Security 1 2 8Sharps\Needlestick 2Slips\trips\falls 1 4
Total 4 4 5 11 19
1.7 Other accident/Incidents (not related to a specific person)
There were 35 incidents in this category, which records “other” accidents or incidentsnot related to a specific patient, staff member, and visitor or non – Trust employee.These incidents are summarised in the table which follows, along with data for theprevious four quarters. No particular trend has been identified within the data but aslight decrease is noted.
Other Accidents /Incidents(not related to a specificpatient, staff or visitor)
Oct-Dec10
Jan-Mar11
Apr– Jun11
Jul-Sept11
Oct-Dec11
Assault (physical & verbal) 1 -- --Blood products -- -- --Communication/Consent -- -- 2 -- 1COSHH 1 -- --Dispensing error -- -- --Documentation 3 -- 2 2Equipment 16 6 10 7 2Failure to follow procedures 4 3 7 1 2Fire -- -- --

7
Impact/collision -- -- 1 1Medical Equipment 1 2 5 8 6Maternity -- -- 1Manual handling -- -- --Medical Care -- -- --Medication error -- 1 1 2 1Nursing Care -- 1 3Other 5 5 7 5Patient transfer -- 1 --Security 3 3 2 5 8Sharps/Needlestick 1 4 6 9 8Specimen Error -- -- --Waste Disposal -- -- 1 2 1Totals 35 26 36 48 35
1.8 Violence and Aggression Incidents
A total of 159 incidents involving violence and aggression were recorded during thisquarter. This is an expected increase on previous quarters and is also a result ofchanges in the reporting arrangements within the Security Department. The rise inreported physical assaults has been investigated further by the Risk Managementand Security Departments, and appears to be due to a change in the definitions usedby the Security Department. Many of the assaults were not intentionally aggressivebut reflected the patients’ condition. There was no serious or significant outcomefrom any of the incidents. Nevertheless, trends will be monitored closely over thecoming quarters. The table which follows summarises data for quarter 3 and theprevious four quarters. Physical assaults accounted for 65 of the incidents, whilstverbal assaults accounted for the other 94.
Physical assaults Verbal assaultsOct-Dec10
Jan-Mar11
Apr-Jun11
Jul-Sept11
Oct-Dec11
Oct-Dec10
Jan-Mar11
Apr-Jun11
Jul-Sept11
Oct-Dec11
Patient topatient
1 2 -- -- 5 -- 1 1 2 2
Patient tostaff
26 27 7 7 57 9 14 3 63 71
Staff to Staff -- -- -- -- 1 5 6 -- 1Visitor to staff -- -- -- -- 1 3 5 -- 3 16Visitor topatient
-- -- -- -- -- 2 -- -- 4
Patient tovisitor
-- 1 -- 1 1 -- -- -- 2 --
Other 3 3 -- -- -- 4 4 -- --Total 30 33 7 8 65 23 30 4 70 94

8
The “Tackling Violence & Aggression Policy” is available on the Trust website andprovides procedures which enable managers and staff to reduce risk and deal withactual and threatened aggression. All staff in patient facing roles are expected toattend conflict resolution training as part of their mandatory training requirements.
2. Incidents Requiring Police Attendance
A total of 45 incidents required police assistance during this quarter. This is a slightincrease on the previous months but remains in line with previous quarters. Thefollowing table identifies the number of incidents requiring police attendance for thelast and previous four quarters.
3. Reporting of Injuries and Diseases Dangerous Occurrence Regulations(RIDDOR)
The Trust is required to report to the Health and Safety Executive all incidents andaccidents leading to any injury resulting in an individual being incapacitated orunable to work for over 3 days, as well as incidents which give rise to death, majorinjuries, and dangerous occurrences. The manager of the area in which theRIDDOR event occurs is responsible for undertaking an investigation andimplementing any training programmes or process improvements required to preventa recurrence. In such cases, managers work closely with the Occupational HealthDepartment and the Risk Management Department. The table which follows showsthe number of RIDDOR incidents reported during quarter 3 compared with theprevious four quarters. All the RIDDOR concerns for this quarter were reported dueto being an over 3 day injury, and no major injuries were reported.
No. of RIDDOR incidents reportedQuarter Staff Contracto
rPatient Visitor Total
OCT-DEC 10 4 -- -- -- 4JAN-MAR 11 9 -- -- -- 9APR-JUN 11 8 -- 1 -- 9JUL-SEPT 11 4 -- 1 -- 5OCT-DEC 11 5 -- -- -- 5
4. Health & Safety Executive Inspections and Visits
No HSE inspections were carried out on site in the quarter.
Oct-Dec 10
Jan-Mar11
Apr-Jun 11
Jul-Sept 11
Oct-Dec 11
38 45 35 31 45

9
5. Serious Clinical Incidents (Red incidents)
Red incident figures are not included in this report until the Quality and ClinicalGovernance Committee has both confirmed the grading of red and determined thatthe final investigation report with action plan meets the standards required by theCommittee. The table which follows is updated as these processes are completed.The Committee closely monitors the progress of each investigation, ensuring thatevery action is complete before ratifying the report for closure. Some incidents areinitially reported as “red”, but on investigation turn out to be of a lower grade. Otherreported incidents may be upgraded to “red” on further investigation. Thesedecisions are made by the Medical Director and the Director of Nursing. At the endof each year, the actual figure for red incidents is reconciled in light of any re-designations which may occur.
Red incidents are fully investigated by multidisciplinary teams led by a trainedinvestigator. The investigation team is appointed by the Director of Nursing and theMedical Director. A recent review of the RCA investigators log has led to a revisionof the internal RCA course and a decision to offer training to Clinical Leads and theAssociate Medical Directors. The number of confirmed “red” incidents in this andthe previous four quarters are given in the following table which follows –
Quarter / Year Red Incidents StEIS recordedOCT-DEC 10 3 -JAN-MAR 11 1 1APR-JUN 11 2 -JUL-SEPT 11 3 5OCT-DEC 11 3 3
The table above also includes “STEIS” reportable incidents. These are incidentswhich must be reported to the “Strategic Executive Information System”, a nationalrequirement, with arrangements devolved to PCTs.
6. Examples of actions taken as a result of an incident:-
Listed below are a number of examples of actions taken following an incident:-
A new scheduling tool has been ordered which will provide a more robustbooking system and reduce the number of incidents reported by DSEU inwhich patients had been scheduled at the wrong time or for the wrongprocedures.
An IV fluid bag was found to have an unexplained leak. The item wasquarantined and the circumstances fully investigated in case malicioustampering had occurred. No contaminant was found and staff were praised bythe police for their quick action. It was later found that only the bag had beenquarantined, and not the full giving set. Staff will be now made aware that incases of suspected contamination the full set of equipment must bequarantined.

10
A new clinical guideline has been developed for ‘Tapping AscitesParacentesis’
After an incident was reported regarding the inappropriate disposal ofconfidential waste following the relocation of offices, the Director of Nursingsent out an e-mail to all Managers reminding them if their obligation underInformation Governance of the correct procedures to be followed.
An audit of theatre compliance with the WHO checklist for correct site surgerywas commissioned – no specific issues were identified.
Individual accountability is being stressed in respect of failure to comply withfalls standards
Matrons are reporting on “frequent fallers” on a monthly basis
7. Complaints Received
The Trust has been working to develop divisional management and accountability forcomplaints rather than a corporate structure. The policy for the management ofcomplaints was revised in November 2011 to reflect the revised structures and thedivisions now investigate and respond to their own complaints in line with the policyupdates. The work of the corporate complaints team now comprises the elements ofthe policy that delivers compliance with the Trust policy for the managementtimeframes and action plans developed by the divisions. The corporate team willensure that the divisional implementation of actions is complete and lessons learnedare disseminated. Templates have been developed and are now being sent out tothe divisions.
During October - December 2011, 85 complaints were received. This is a decreasefrom 96 in the previous quarter. The number of complaints varies, and rises and fallsof this degree should not be seen as indicative of any trend. Of the 85 complaints,66 met the target of 25 day response and agreed extension which gives a totalresponse rate of 78% for this reporting period.
Quarter /Year
No. ofcomplain
ts
No. met 25days &
agreed extn
% met 25 days& agreed extn
OCT-DEC10 94 46 49%JAN-MAR 11 80 47 59%
APR-JUNE 11 97 65 67%JUL-SEP 11 96 74 77%OCT-DEC 11 85 66 78%
The table which follows compares the number of complaints by quarter:-
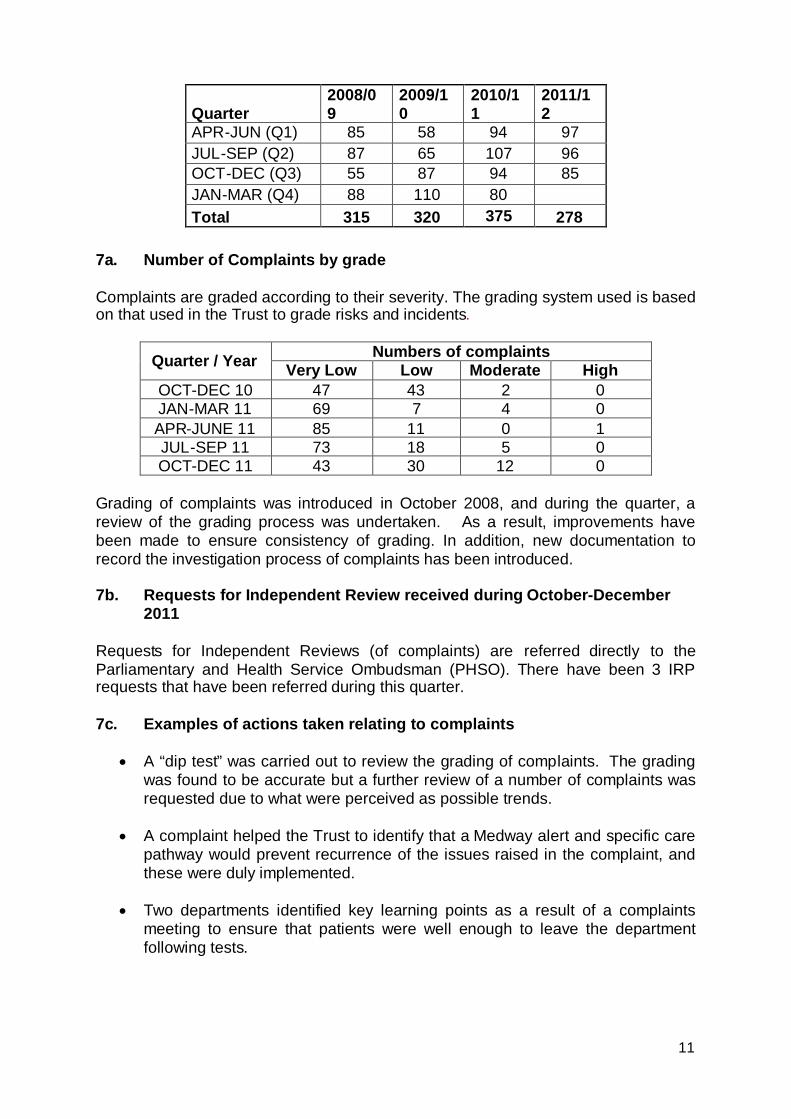
11
Quarter2008/09
2009/10
2010/11
2011/12
APR-JUN (Q1) 85 58 94 97JUL-SEP (Q2) 87 65 107 96OCT-DEC (Q3) 55 87 94 85JAN-MAR (Q4) 88 110 80Total 315 320 375 278
7a. Number of Complaints by grade
Complaints are graded according to their severity. The grading system used is basedon that used in the Trust to grade risks and incidents.
Quarter / Year Numbers of complaintsVery Low Low Moderate High
OCT-DEC 10 47 43 2 0JAN-MAR 11 69 7 4 0APR-JUNE 11 85 11 0 1JUL-SEP 11 73 18 5 0OCT-DEC 11 43 30 12 0
Grading of complaints was introduced in October 2008, and during the quarter, areview of the grading process was undertaken. As a result, improvements havebeen made to ensure consistency of grading. In addition, new documentation torecord the investigation process of complaints has been introduced.
7b. Requests for Independent Review received during October-December2011
Requests for Independent Reviews (of complaints) are referred directly to theParliamentary and Health Service Ombudsman (PHSO). There have been 3 IRPrequests that have been referred during this quarter.
7c. Examples of actions taken relating to complaints
A “dip test” was carried out to review the grading of complaints. The gradingwas found to be accurate but a further review of a number of complaints wasrequested due to what were perceived as possible trends.
A complaint helped the Trust to identify that a Medway alert and specific carepathway would prevent recurrence of the issues raised in the complaint, andthese were duly implemented.
Two departments identified key learning points as a result of a complaintsmeeting to ensure that patients were well enough to leave the departmentfollowing tests.

12
8. Claims
The table which follows provides an overview of claims received during Quarter 2compared to the previous four quarters.
Quarter /Year
ClinicalNegligence
PublicLiability
EmployersLiability
VehicleAccidents
Totals
OCT-DEC10
9 2 2 1 14
JAN-MAR11
14 3 2 -- 19
APR-JUN11
14 2 4 0 20
JUL-SEPT11
13 1 3 0 17
OCT-DEC11
16 2 3 1 22
9. Multi Agency Child Protection Reviews
There are no new Serious Case Reviews to report for this quarter.
Philip DylakDirector of Nursing15 February 2012

1
Agenda Item 16
TAMESIDE HOSPITAL NHS FOUNDATION TRUST
NATIONAL SERVICE FRAMEWORKS AND THE NATIONAL CANCER PLAN
PURPOSE
To apprise the Board of progress in respect of the National Cancer Plan and theNational Service Frameworks (NSF) for Older People and Children, Young People &Maternity Services.
DISCUSSION
a) NSF for Older People
The Trust addressed the requirements within this document by developing acomprehensive framework encompassing work groups in the key areas of rootingout age discrimination, person centred care, intermediate care, general hospital care,stroke, falls, mental health for older people and the promotion of health and activelife in old age. These standards have now been firmly embedded into operatingprocesses and nursing governance structures (e.g. the North West Care Indicatormetric set).
This NSF has now been largely superseded by new requirements which address inmore detail issues concerning stroke and dementia. The Trust has utilised non-recurrent funding from the PCT to open an acute stroke ward which accepts directreferrals from the Emergency Department. This has significantly improved ourperformance against national indicators in a short time span, examples include:
Time spent on a dedicated stroke ward – 77% (previously 36%) Swallow Screen within 24 hours of admission – 82% (previously 45%) Aspirin within 24 hours of hospital admission – 82% (previously 33%)
The Trust is negotiating the continuation of funding for this unit as part of thecontractual settlement for 2012/13 and would anticipate further improvements inthese indicators.
The Trust has established a joint Strategy Implementation Group withCommissioners in response to the national dementia strategy. The key issues for theTrust are:
- development of an explicit care pathway for the management and care ofpatients with dementia.
- delivery of a formative training programme for staff in caring for patients withdementia.

2
- development of a centre of excellence in dementia care
- enhancing in-reach services in liaison with the Mental Health Trust.
- establishing collaborative working with Commissioners and the Mental HealthTrust to streamline Dementia care and service provision.
An action plan to achieve these objectives is operational under the guidance of theDirector of Nursing, and reports to TEG. It is proposed to substitute the NSF OPupdates to the Board with the dementia workstream. Stroke issues are addressed inthe Boards performance report.
b) Children, Young People and Maternity Services
i) Children
The development of child appropriate environments continues to be central to fullimplementation of this NSF.
Following transfer of paediatric services to Hartshead South in November 2010,improved compliance was achieved. The two main non paediatric service providers(Orthopaedic and ENT) have since relocated into the children’s area. This has nowallowed the organisation to achieve the target of 95% compliance of all childrenaccessing care in child friendly areas. The only areas not achieving this separationare the dermatology clinic and the BCG clinic. Options to address this are beingworked through in order to achieve total compliance with the standard. All children’ssurgical lists are conducted in accordance with the NSF standard and operate fromthe paediatric area.
The three Advanced Paediatric Nurse Practitioners in A&E continue to provideproactive care in avoiding unnecessary admissions of children from the A&Edepartment. These staff are a central feature of the new paediatric A&E department,completed in January 2012.
ii) Maternity Services
A key priority for maternity services remains the recognition and management ofwomen with mental health problems throughout their pregnancy. The perinatal mentalhealth pathway has now been launched, with maternity representation led by thespecialist midwife for vulnerable families. Good progress has been made and midwiveshave accessed training to ensure successful implementation.
Multi agency working continues with the ‘early attachment service’ to recognise andwork with families at risk of poor attachment and bonding, in particular with teenageparents.
Maternity services recognise the importance of routine enquiry for domestic abuse inpregnancy and have organised and participated in inter-agency training by the IDVA(independent domestic violence advocate) service.

3
Breast feeding remains a key priority and all necessary staff have an induction to thepolicy in the first week of employment and relevant staff attend a Trust two daybreast-feeding programme. Paediatric medical staff are trained in order to ensurecontinuity of care on the inpatient ward as well as on NICU.
c) The Cancer Plan
The main areas of interest to the Board in respect of Cancer Services include:-
i) Peer Review
All cancer tumour sites are now subject to annual self assessment against publishedcancer standards. In 2011 the Trust had external visits for Upper GI, Colorectal andHead & Neck. A series of actions were required as a result of these audits, which arebeing implemented. The Trust has been notified that only Acute Oncology will besubject to external Peer Review in 2012.
ii) Acute Oncology Services
The Cancer Network has produced a framework for the provision of an AcuteOncology service within each DGH. This is designed to rapidly respond to patientsattending A&E Departments with complications relating to their cancer treatment, inaddition to signposting previously undiagnosed patients to the most appropriatecancer pathway. Evidence from a pilot scheme indicates that this early interventionfrom specialist oncology support will reduce length of stay in addition to improvingoutcomes. Non-recurrent funding has been provided to the Trust to enablerecruitment to a full-time Advanced Nurse Practitioner and administrative support. Akey element of this service will be the daily presence of a visiting oncologist from theChristie Hospital. The Cancer Network are working closely with the Christie to securethis capacity.
iii) Palliative Care
The Trust does not currently have a Consultant in Palliative Medicine. A freshattempt at recruitment is currently in process. The Trust is also exploring improvedmedical support to this critical area with the medical lead at Willow Wood Hospice.
RECOMMENDATION
The Board is asked to:-
i. note the Trust’s current position against the two National Service Frameworksand also the Cancer Strategy
ii. endorse the proposal to substitute in future reports to Board the NSF OlderPeople section with the dementia workstream.
Paul WilliamsDirector of Clinical Services14th February 2012





























