Embed Size (px)
Citation preview

NeuroImage 47 (2009) 1148–1153
Contents lists available at ScienceDirect
NeuroImage
j ourna l homepage: www.e lsev ie r.com/ locate /yn img
Age-related grey matter changes in preterm infants: An MRI study
L.C. Tzarouchi a, L.G. Astrakas b, V. Xydis a, A. Zikou a, P. Kosta a, A. Drougia c,S. Andronikou c, M.I. Argyropoulou a,⁎a Department of Radiology, Medical School, University of Ioannina, 45110 Ioannina, Greeceb Department of Medical Physics, Medical School, University of Ioannina, Greecec Intensive Care Unit, Child Health Department, Medical School, University of Ioannina, Greece
⁎ Corresponding author. Fax: +30 2651097862.E-mail address: [email protected] (M.I. Argyropou
1053-8119/$ – see front matter © 2009 Elsevier Inc. Aldoi:10.1016/j.neuroimage.2009.03.072
a b s t r a c t
a r t i c l e i n f oArticle history:Received 27 November 2008Revised 17 February 2009Accepted 26 March 2009Available online 5 April 2009
Grey matter (GM) maturation has not been previously studied in healthy preterm children. The purpose ofthis study was to evaluate the age dependency of GM development in 116 GM areas in preterm subjects. Sixtyone preterm infants (corrected age: 13.7±9.92 months, gestational age: 33.4±1.9 weeks) with normalstructural appearance on MRI were included in the study. Using a T1-weighted high resolution 3D spoiledgradient echo sequence, volumes of 116 GM areas were calculated after their segmentation using the VoxelBased Morphometry Toolboxes and the Individual Brain Atlas Statistical Parametric Mapping (IBASPM) softwarepackages. Non linear regression analysis assessed age dependency of volume data for every GM area usingthe monoexponential function y=A−B⁎exp(−x/C). All supratentorial GM areas followed the mono-exponential function model reasonably well. Cerebellar structures had a poor goodness of fit. Volumeincrease of the individual GM areas followed an inferior to superior and a posterior to anterior pattern. Theputamen, thalamus, and caudate nucleus reached 99% of the final volume earlier than most cortical GM areas.The visual cortex and the postcentral and precentral cortices matured earlier than the parietal, frontal andtemporal cortices. The fronto-occipital asymmetry or torque seen in adults was observed in the preterminfants; the left occipital areas reached maturation earlier than the right, while the right prefrontal andfrontal areas matured earlier than the left. To conclude, GM development progresses in a region-specificmanner coinciding with functional, phylogenetical and regional white matter (WM) maturation.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Brain maturation follows a dynamic course, starting during fetallife and is a lifelong process (Dekaban,1978; Dobbing and Sands,1973;Kretschmann et al., 1986). Most of the progressive and regressiveevents (e.g. neuronal migration, synaptic reorganization, myelindeposition and cell death) that contribute to brain maturation takeplace during the perinatal period and the first years of life (Dobbingand Sands, 1973). Brain volume increases with age and by the age of2 years it reaches 75% of its adult weight (Dekaban, 1978;Kretschmann et al., 1986). Development of both grey (GM) andwhite matter (WM) accounts for the brain volume increase.Premature birth has been associated with complicated neonatalevents resulting in increased central nervous system (CNS) morbidity,and in particular periventricular leukomalacia (PVL) (Wood et al.,2000). Preterm infants, even those with an uncomplicated neonatalcourse, may manifest long-term neurodevelopmental deficits, includ-ing cognitive and behavioural problems (Hack et al., 2000; Marlow,2004). Evaluation of brain development, in terms of myelinationprogress and GM andWM volume changes, would permit the relating
lou).
l rights reserved.
of developmental outcomes to changes in specific anatomic struc-tures. Magnetization Transfer Imaging (MTI) evaluating Magnetiza-tion Transfer Ratio (MTR) has been used to study the progress ofmyelination in both preterm babies with an uneventful perinatalhistory and those with findings of PVL (Xydis et al., 2006a,b). Thosestudies demonstrated that myelination follows a monoexponentialfunction model. Volumetric studies evaluating GM maturation andage-related changes in full-term children included mainly subjectsaged older than 2 years (Caviness et al., 1996; Giedd et al., 1999, 1996;Reiss et al., 1996; Sowell et al., 2003). There are only few reports ofstudies assessing GM age-related changes during the first 2 years oflife in full-term babies (Gilmore et al., 2007; Matsuzawa et al., 2001;Pfefferbaum et al., 1994). Using semi-automated techniques of imagesegmentation the researchers calculated either total cortical GMvolume or GM volume of certain lobes and demonstrated that GMvolume in full-term infants increases following an exponentialfunction model (Matsuzawa et al., 2001; Pfefferbaum et al., 1994).There are no normative data regarding normal GM development inpreterm babies.
Volumetric MRI studies assessing GM development have beenbased either on the region-of-interest (ROI) approach or morerecently on modern techniques of image segmentation and automaticvolume calculation (Caviness et al., 1996; Giedd et al., 1996;

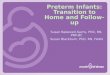
Fig. 1. (a) Parasagittal T1W scan in an 8 months old child, (b) same scan aftersegmentation of the right caudate nucleus using the IBASPM toolbox.
Fig. 2. Age-related changes of total GM volume.
1149L.C. Tzarouchi et al. / NeuroImage 47 (2009) 1148–1153
Matsuzawa et al., 2001; Peterson et al., 2000; Pfefferbaum et al., 1994;Reiss et al., 1996). Individual Brain Atlases using Statistical ParametricMapping (IBASPM) is a toolbox used for brain segmentation,individual atlas generation, labelling of 116 individual GM areas andvolume computation that permits objective measurements of regionalbrain volume (Alemán-Gómez et al., 2006). This tool has not beenused previously for the quantification ofmaturational brain changes ininfants and children.
The purpose of this study was to conduct a volumetric assessment,using IBASPM that would provide normative data on the volume of116 individual GM areas in preterm infants and to investigate the age-related changes in total GM volume and in the 116 GM areas inparticular.
Materials and methods
The study population consisted of 61 preterm infants (32males, 29females) with a mean gestational age (GA) of 33.4±1.9 weeks (range30–36 weeks), investigated at mean corrected age of 13.7±9.92 months (range 0.4–49.23 months). They had all had an uncom-plicated neonatal course, and had neurological evaluation duringregular follow up (Amiel-Tison, 2001) and had no major neurologicalproblem. Subjects with postnatal steroid exposure, or bronchopul-monary dysplasia and brain abnormalities onMRI were excluded fromthe study. Five infants had a brain MR for suspected CNS abnormality(one episode of seizure, meningoencephalitis or brain tumour) andthe rest of the population participated in an ongoing study on braindevelopment and maturation in preterm children. Local EthicalCommittee approval and written informed consent from the parentsof all subjects were obtained.
All MR examinations were performed on the same 1.5 Tesla MRunit (Gyroscan, ACS NT; Philips Medical Systems, Best, The Nether-lands) using a head coil, field of view 24 cm and 1mm×1mm×1mmresolution. The children were sedated with oral chloral hydrate (20–30 mg/kg) and the MR examinationwas performed under respiratoryand ECG monitoring. The standard imaging protocol compromised:Axial T2-weighted turbo spin-echo (TR 3.500 ms, TE 120 ms, slicethickness 5 mm, intersection gap 0.5 mm), coronal T2-weighted turbospin-echo (TR 3.500ms, TE 90ms, slice thickness 2.5 mm, intersectiongap 0 mm) and a three-dimensional spoiled gradient-echo T1-weighted (TR 25 ms, TE 4.6 ms, 6 flip angle, 2 mm gap).
Data post-processing and image analysis were performed using theVoxel Based Morphometry Toolboxes developed by the StructuralBrain Mapping Group at the University of Jena (Cuadra et al., 2005)and the IBASPM (http://www.thomaskoenig.ch/Lester/ibaspm.htm)toolboxes, both running under MATLAB 7.0 (Mathworks, Natick, MA,USA). The 3D T1-WIs were spatially segmented into GM, WM andcerebrospinal fluid (CSF) compartments and normalized to theMontreal Neurological Institute (MNI) T1 template using the VBMtoolboxes. These toolboxes allow to segment brains without braintissue probability prior maps. Instead they use prior information by
applying a Hidden Markov Random Field (HMRF) model to removeisolated voxels of one tissue class which are unlikely to be member ofthis tissue type and also to close holes in a cluster of connected voxelsof one tissue type. These algorithms have been used successfully toconstruct an infant brain template in Altaye et al. (2008). Automaticvolume computation for each tissue type into native space wasperformed with the brain computation function of IBASPM. Eachindividual grey matter voxel was labeled based on an anatomical atlasand taking into account the transformation matrix obtained in thenormalization process. An individual brain atlas was created for eachsubject consisting of 116 different GM areas. Statistical measures wereperformed for each atlas with the IBASPM volume statistic functionand the volume for the 116 areas was calculated.
Data analysis was conducted using SPSS 15.0 for Windows. Thenormality of distribution of parameters was assessed by theKolmogorov–Smirnov test. Nonlinear regression analysis assessedthe age dependency of GM volume for every brain area separatelyand for total GM volume. The model function used was themonoexponential y=A−B⁎exp(−x/C), where y represents thevolume at corrected age x and A, B and C were the calculatedregression parameters. According to the model parameter Arepresents the volume at the end of maturation, while parametersB and C represent the total change and the rate of change of theGM during maturation respectively. A−B represents the GM volumeat 40 weeks of gestation (corrected age=0). The 99% of the finalvolume A (0.99⁎A) or A99% was reached at the time point t(99%)and can be calculated as t(99%)=−C⁎ ln(0.01⁎A/B). Goodness of fitwas estimated using a R2 value. A two-tailed Pb0.05 was consideredstatistically significant.
Results
Figs. 1a,b demonstrate the quality of our data and the accuracy ofour registration using as example the caudate nucleus in an 8 monthsold subject.
Total GMvolume increased asymptotically, reaching99%of thefinalvalue at corrected age: 64.5 months (5.3 years, R2=0.774) (Fig. 2). Allsupratentorial GM areas followed the monoexponential functionmodel reasonably as indicated by the R2 values (Table 1). Cerebellarstructures had a poor goodness of fit.
Figs. 3 and 4 encode with colour t(99%) each GM area. Each GMarea has a different t(99%). Dark colour represents GM areas with asmall t(99%) which means areas with early maturation. Light colourrepresents GM areas with a large t(99%) meaning areas that maturedlater.

Table 1R2 values and t(99%) for each GM area.
GM area R2 t99% GM area R2 t99% GM area R2 t99% GM area R2 t99%
Precentral L 0.723 76.99 Cingulum ant L 0.498 99.75 Parietal inf L 0.564 24.50 Cerebellum crus1 L 0.458 36.13Precentral R 0.596 64.92 Cingulum ant R 0.466 86.51 Parietal inf R 0.553 49.15 Cerebellum crus1 R 0.492 57.56Frontal superior L 0.702 75.37 Cingulum mid L 0.576 83.04 Supramarginal L 0.584 48.39 Cerebellum crus2 L 0.448 39.57Frontal superior R 0.651 62.13 Cingulum mid R 0.603 52.12 Supramarginal R 0.318 29.70 Cerebellum crus2 R 0.484 73.19Frontal sup orb L 0.481 43.40 Cingulum post L 0.450 32.76 Angular L 0.523 42.58 Cerebellum 3 L 0.121 16.49Frontal sup orb R 0.635 47.96 Cingulum post R 0.402 24.62 Angular R 0.499 43.04 Cerebellum E R 0.191 20.49Frontal mid L 0.738 104.84 Hippocampus L 0.544 60.45 Precuneus L 0.603 52.25 Cerebellum 4.5 L 0.367 19.79Frontal mid R 0.572 79.54 Hippocampus R 0.573 39.95 Precuneus R 0.52 53.31 Cerebellum 4.5 R 0.37 29.35Frontal mid orb L 0.601 46.03 Parahippocampal L 0.511 27.38 Paracentral lobule L 0.678 85.54 Cerebellum 6 L 0.336 20.65Frontal mid orb R 0.661 55.00 Parahippocampal R 0.534 33.85 Paracentral lobule R 0.492 46.15 Cerebellum 6 R 0.239 37.73Frontal inf oper L 0.703 67.22 Amygdala L 0.562 31.43 Caudate L 0.583 45.15 Cerebellum 7B L 0.334 53.76Frontal inf oper R 0.618 50.01 Amygdala R 0.534 39.04 Caudate R 0.604 53.12 Cerebellum 7B R 0.297 115.31Frontal inf tri L 0.744 76.73 Calcarine L 0.561 35.11 Putamen L 0.405 41.00 Cerebellum 8 L 0.233 49.81Frontal inf tri R 0.564 56.25 Calcarine R 0.558 39.44 Putamen R 0.375 42.00 Cerebellum 8 R 0.112 68.62Frontal inf orb L 0.733 96.10 Cuneus L 0.524 38.24 Pallidum L 0.444 26.74 Cerebellum 9 L 0.238 27.56Frontal inf orb R 0.661 55.00 Cuneus R 0.532 40.77 Pallidum R 0.481 32.75 Cerebellum 9 R 0.115 28.68Rolandic oper L 0.747 85.82 Lingual L 0.572 36.70 Thalamus L 0.427 38.15 Cerebellum 10 L 0.205 19.65Rolandic oper R 0.543 49.24 Lingual R 0.601 35.48 Thalamus R 0.368 29.26 Cerebellum 10 R 0.227 28.86Sup motor area L 0.734 85.77 Occipital sup L 0.499 35.70 Heschl L 0.453 64.37 Vermis 1.2 0.15 18.08Sup motor area R 0.709 59.81 Occipital sup R 0.588 57.99 Heschl R 0.56 75.17 Vermis 3 0.218 15.35Olfactory L 0.295 32.66 Occipital mid L 0.409 33.96 Temporal sup L 0.598 71.00 Vermis 4.5 0.303 19.09Olfactory R 0.342 29.70 Occipital mid R 0.642 52.16 Temporal sup R 0.447 46.89 Vermis 6 0.305 17.17Frontal sup med L 0.765 252.93 Occipital inf L 0.608 37.51 Temporal pole sup L 0.751 117.94 Vermis 7 0.371 26.05Frontal sup med R 0.741 81.18 Occipital inf R 0.661 47.30 Temporal pole sup R 0.677 119.53 Vermis 8 0.316 27.12Frontal mid orb L 0.707 106.51 Fusiform L 0.552 34.10 Temporal mid L 0.544 59.93 Vermis 9 0.242 22.75Frontal mid orb R 0.698 54.36 Fusiform R 0.637 45.08 Temporal mid R 0.542 53.51 Vermis 10 0.116 20.90Rectus L 0.638 50.28 Postcentral L 0.654 68.68 Temporal pole mid L 0.553 64.37Rectus R 0.62 55.35 Postcentral R 0.455 51.34 Temporal pole mid L 0.567 43.76Insula L 0.72 161.95 Parietal sup L 0.422 40.32 Temporal inf L 0.656 52.46Insula R 0.762 137.16 Parietal sup R 0.461 43.85 Temporal inf R 0.59 40.26
1150 L.C. Tzarouchi et al. / NeuroImage 47 (2009) 1148–1153
The volume increase of the individual GM areas followed aninferior to superior and a posterior to anterior order pattern. Theputamen, thalamus, and caudate nucleus reached A99% earlier thanmost cortical GM areas. The visual cortex and postcentral andprecentral cortices reached A99% earlier than the temporal andother parietal and frontal cortices. A pattern of GM maturationconsistent with fronto-occipital asymmetry or torque was observed.The right frontal regions reached maturation earlier than the left,while the left occipital regions reached maturation earlier than theright (Figs. 3, 4).
Fig. 3. Shows in axial plane with colour scale the t(99%) for each individual GM area. Dark cVolume increases in a posterior to anterior pattern.
Discussion
In this study an automated method for brain segmentation andvolume calculation was used in order to evaluate normal GMdevelopment in preterm infants. The main finding was an increase intotal and regional GM volume in preterm babies that followed amonoexponential function model. Regional GM maturation tookplace in order from inferior to superior and from posterior toanterior. The basal ganglia matured earlier than the cortex while themotor, sensory and visual cortices matured before the prefrontal
olour encodes areas of early maturation; light colour encodes areas of late maturation.

Fig. 4. Demonstrates in sagittal plane with colour scale the t(99%) for each individual GM area. Dark colour encodes areas of early maturation; light colour encodes areas of latematuration Volume increases in a caudal to cephalad pattern.
1151L.C. Tzarouchi et al. / NeuroImage 47 (2009) 1148–1153
cortex. A pattern of maturation consistent with fronto-occipitalasymmetry was observed.
Cross-sectional volumetric studies in full-term babies have shownthat total GM volume increases with age from birth until the age of4–6 years (Matsuzawa et al., 2001; Pfefferbaum et al., 1994).Matsuzawa et al. (2001) studied a series of full-term children agedfrom one month to 10 years using a semi-automated method ofimage segmentation, and found an exponential increase of GMvolume up until the age of 2 years, followed by a more gradualexpansion. Pfefferbaum et al. (1994) evaluated GM development infull-term subjects aged 3 months to 30 years and demonstrated thatGM volume peaked around the age of 4 years. The present study inagreement with these reports, demonstrated that in preterm infantsthe total GM volume increases with age following a monoexponentialfunction model. However, total GM volume increase reached aplateau by the age of 5.9 years, time point different from that foundin studies of full-term children. Previous volumetric MRI studiescomparing GM volume between full-term and preterm infants (bothhealthy and preterms with PVL were included) have showndecreased total and regional GM volume in preterm subjects duringchildhood and adolescence (Nosarti et al., 2002; Peterson et al., 2003,2000). These studies used the region-of-interest method but alsoautomatic techniques of image segmentation and volume calculation.The more protracted time scale of GM development found in ourstudy may account for the decreased GM volume of preterms whencompared to full-term subjects. GM maturation in the intrauterineenvironment is genetically controlled and well protected while inpreterm birth it is exposed to several environmental factors that mayinfluence normal development (Peterson et al., 2003). There arestudies in preterms (without and with PVL) that correlate factors likethe degree of immaturity, intrauterine growth restriction, exposure todexamathasone and broncopulmonary dysplasia with altered GMvolume when compared to full-term children (Inder et al., 2005;Murphy et al., 2001; Thompson et al., 2007). Some of these factorsmay influence GM development even in preterms with uneventfulneonatal courses resulting in low maturational rate.
Age-related GM volume increase reflects dynamic changes of acomplex architecture, consisting of neurons with their dendritic andsynaptic processes, of glia (i.e. myelin) and vasculature (Ramakers,2005). Neuronal proliferation and migration to the cerebral cortexare already completed by the 24th week of gestation (Rakic, 1988).Thus GM volume increase after this time point is mainly related tothe axonal growth and development of new synapses. Histological
studies demonstrated that synaptogenesis and axonal outgrowthstart as soon as neurons have stopped migrating and continuethrough lifespan reaching a plateau at different time depending onbrain region (Huttenlocher, 1979; Huttenlocher and Dabholkar,1997).
Regional specificity was observed during brain maturation con-cerning the 116 individual GM areas. GM areas matured throughoutthe brain from inferior to superior and from posterior to anterior.Occipital and parietal regions matured earlier than the frontal andprefrontal regions. Regional differences in synaptogenesis as indicatedby histological studies might explain this pattern of different regionalGM maturation. Indeed, in the visual cortex synaptic overproductionreaches a maximum at 3–4 months of age, while in the prefrontalcortex the peak occurs at 4–5 years (Huttenlocher, 1979; Huttenlocherand Dabholkar, 1997). A similar spatial pattern of age-related changeshas been reported in white matter tracts. Indeed histopathologic andMRI studies have shown that white matter volume increase andmyelination progress follow an inferior to superior and posterior toanterior pattern (Barkovich et al., 1988; Gilmore et al., 2004; Neil et al.,2002; Xydis et al., 2006b). Close interactions between GM and WMmaturation during brain development could explain these similarpatterns of age-related changes.
GM maturation progresses in a localized, region-specific mannercoinciding with functional maturation (Kagen, 2005). Regionsassociated with more basic functions such as primary motor cortexdevelop earlier compared with regions that are responsible of morecomplex and integrative functions like prefrontal cortex (Kagen,2005). In this study motor, sensory and visual cortex reachedmaturation earlier than prefrontal cortex reflecting the rapid devel-opment of visual and sensory-motor functions compared with theexecutive functions of the prefrontal cortex. Similar findings weredemonstrated by volumetric MRI studies in full terms evaluated forGM maturation at the neonatal period but also later at adolescence(Gilmore et al., 2007; Gogtay et al., 2004).
The basal ganglia, part of the telencephalon, are phylogeneticallymore primitive regions than the more advanced cortical regions. Anearlier maturation of the basal ganglia has been demonstrated bySPECT and perfusion studies in full-term infants (Chiron et al., 1992;Takahashi et al., 1999; Tokumaru et al., 1999). These studies showedincreased Cerebral Blood Flow (rCBF) and uptake 123I-IMP in the basalganglia compared to cortical regions. These findings reflect functionaland anatomical maturation in the basal ganglia (Chiron et al., 1992;Takahashi et al., 1999; Tokumaru et al., 1999). Consistent with these

1152 L.C. Tzarouchi et al. / NeuroImage 47 (2009) 1148–1153
studies maturation of the basal ganglia preceded cortical maturationin our study.
The cerebral hemispheres are structurally and functionally asym-metric (Toga and Thompson, 2003). “Brain torque” or “fronto-occipitalasymmetry” is a well-documented asymmetry pattern of hemisphericvolume distribution. The occipital and frontal lobes are leftwardly andrightwardly asymmetric, respectively. Postmortem, CT and MRIstudies evaluating brain width from the midline to the outer borderin the occipital and frontal lobe have demonstrated the presence ofbrain torque in adult brains (Chiu and Damasio, 1980; Kertesz et al.,1990; LeMay, 1976). More recently, manual and automated MRIvolumetric studies in adults have shown that increased GM and WMvolume in the corresponding areas are responsible for brain torque(Good et al., 2001; Watkins et al., 2001). In the present study GMmaturation followed a clock-wise pattern e.g. right frontal regionsreached maturation earlier than the left, while left occipital regionsreached maturation earlier than the right, which is consistent withbrain torque asymmetry. Cerebral asymmetry patterns observed inadults are attributable to genetic factors that operate early from thefetal life but also to environmental influences that may alter geneticprogramming (Sun et al., 2005). Children born preterm are at risk ofdisruption of the normal cerebral development and their brainsundergo an extended period of postnatal stress (Peterson et al., 2003;Thompson et al., 2007). It has been suggested that postnatal stressmay influence the development of adult patterns of asymmetry(Carrion et al., 2001). Our study shows that in preterm born childrenwith uncomplicated neonatal course the development of adultpatterns of asymmetry is preserved. Consistent with our findings arecent study in a 14-year-old child born preterm found the normaladult pattern asymmetries (Lancefield et al., 2006).
Cerebellar GM areas did not fit the monoexponential functionmodel used it the present study. Data from cerebellar GM areas had agreat variability and age-related changes could not be described by thefunctional model that was used. GM maturational processes in thecerebellar cortex are complex. The developing cerebellar cortexconsists of several molecular layers (Purkinje cell sheet, molecularlayer, external and internal granular layer). Formation and migrationof Purkinje cells take place early in gestation, but granule cells are stillgenerated in the external granular layer and migrate through themolecular layer into the internal granular layer during postnatal life(Millen and Gleeson, 2008; Riedel et al., 1989; Triulzi et al., 2005).Growth in volume of the external and internal granular layers reflectschanges in cell number whereas volume changes in the Purkinje cellsheet and molecular layer correspond to increases in neuropil (Millenand Gleeson, 2008; Riedel et al., 1989; Triulzi et al., 2005). Thus duringpostnatal development of the cerebellum all stages of neuronaldevelopment from cell generation to final differentiation can beobserved and probably a more complicated statistical model wouldexplain age-related changes in cerebellar GM areas.
To conclude, this study provides normative data for GMmaturationin preterm born children during the first years of life. Higher-orderassociation areas mature after the lower-order sensorimotor regions.The adult pattern of cerebral asymmetry is preserved in preterm bornchildren suggesting that the genetic programming is preserveddespite the postnatal stress that they are subject.
References
Alemán-Gómez, Y., Melie-Garcia, L., Valdés-Hernandez, P.A., 2006. IBASPM: toolbox forautomatic parcellation of brain structures.12th Annual Meeting of the Organizationfor Human Brain Mapping, Florence, Italy.
Altaye, M., Holland, S.K., Wilke, M., Gaser, C., 2008. Infant brain probability templates forMRI segmentation and normalization. Neuroimage 43, 721–730.
Amiel-Tison, C., 2001. Clinical assessment of the infant nervous system. In: Levene, M.I.,Chervenak, F.A.,Whittle, M. (Eds.), Fetal and Neonatal Neurology and Neurosurgery.Churchill Livingstone, London, pp. 99–120.
Barkovich, A.J., Kjos, B.O., Jackson Jr., D.E., Norman, D., 1988. Normal maturation of theneonatal and infant brain: MR imaging at 1.5 T. Radiology 166, 173–180.
Carrion, V.G., Weems, C.F., Eliez, S., Patwardhan, A., Brown,W., Ray, R.D., Reiss, A.L., 2001.Attenuation of frontal asymmetry in pediatric posttraumatic stress disorder. Biol.Psychiatry 50, 943–951.
Caviness Jr., V.S., Kennedy, D.N., Richelme, C., Rademacher, J., Filipek, P.A., 1996. Thehuman brain age 7–11 years: a volumetric analysis based on magnetic resonanceimages. Cereb. Cortex 6, 726–736.
Chiron, C., Raynaud, C., Maziere, B., Zilbovicius, M., Laflamme, L., Masure, M.C., Dulac, O.,Bourguignon, M., Syrota, A., 1992. Changes in regional cerebral blood flow duringbrain maturation in children and adolescents. J. Nucl. Med. 33, 696–703.
Chiu, H.C., Damasio, A.R., 1980. Human cerebral asymmetries evaluated by computedtomography. J. Neurol. Neurosurg. Psychiatry 43, 873–878.
Cuadra, M.B., Cammoun, L., Butz, T., Cuisenaire, O., Thiran, J.P., 2005. Comparison andvalidation of tissue modelization and statistical classification methods in T1-weighted MR brain images. IEEE Trans. Med. Imaging 24, 1548–1565.
Dekaban, A.S., 1978. Changes in brainweights during the span of human life: relation ofbrain weights to body heights and body weights. Ann. Neurol. 4, 345–356.
Dobbing, J., Sands, J., 1973. Quantitative growth and development of human brain. Arch.Dis. Child 48, 757–767.
Giedd, J.N., Blumenthal, J., Jeffries, N.O., Castellanos, F.X., Liu, H., Zijdenbos, A., Paus, T.,Evans, A.C., Rapoport, J.L., 1999. Brain development during childhood andadolescence: a longitudinal MRI study. Nat. Neurosci. 2, 861–863.
Giedd, J.N., Snell, J.W., Lange, N., Rajapakse, J.C., Casey, B.J., Kozuch, P.L., Vaituzis, A.C.,Vauss, Y.C., Hamburger, S.D., Kaysen, D., Rapoport, J.L., 1996. Quantitative magneticresonance imaging of human brain development: ages 4–18. Cereb. Cortex 6,551–560.
Gilmore, J.H., Lin, W., Prastawa, M.W., Looney, C.B., Vetsa, Y.S., Knickmeyer, R.C.,Evans, D.D., Smith, J.K., Hamer, R.M., Lieberman, J.A., Gerig, G., 2007. Regionalgray matter growth, sexual dimorphism, and cerebral asymmetry in the neonatalbrain. J. Neurosci. 27, 1255–1260.
Gilmore, J.H., Zhai, G., Wilber, K., Smith, J.K., Lin, W., Gerig, G., 2004. 3 Tesla magneticresonance imaging of the brain in newborns. Psychiatry Res. 132, 81–85.
Gogtay, N., Giedd, J.N., Lusk, L., Hayashi, K.M., Greenstein, D., Vaituzis, A.C., Nugent III,T.F., Herman, D.H., Clasen, L.S., Toga, A.W., Rapoport, J.L., Thompson, P.M., 2004.Dynamic mapping of human cortical development during childhood throughearly adulthood. Proc. Natl. Acad. Sci. U. S. A. 101, 8174–8179.
Good, C.D., Johnsrude, I., Ashburner, J., Henson, R.N., Friston, K.J., Frackowiak, R.S.,2001. Cerebral asymmetry and the effects of sex and handedness on brainstructure: a voxel-based morphometric analysis of 465 normal adult humanbrains. Neuroimage 14, 685–700.
Hack, M., Taylor, H.G., Klein, N., Mercuri-Minich, N., 2000. Functional limitations andspecial health care needs of 10- to 14-year-old children weighing less than750 grams at birth. Pediatrics 106, 554–560.
Huttenlocher, P.R., 1979. Synaptic density in human frontal cortex — developmentalchanges and effects of aging. Brain Res. 163, 195–205.
Huttenlocher, P.R., Dabholkar, A.S., 1997. Regional differences in synaptogenesis inhuman cerebral cortex. J. Comp. Neurol. 387, 167–178.
Inder, T.E., Warfield, S.K., Wang, H., Huppi, P.S., Volpe, J.J., 2005. Abnormal cerebralstructure is present at term in premature infants. Pediatrics 115, 286–294.
Kagen, J.H.N. (Ed.), 2005. A Young Mind in a Growing Brain.Kertesz, A., Polk, M., Black, S.E., Howell, J., 1990. Sex, handedness, and the morphometry
of cerebral asymmetries on magnetic resonance imaging. Brain Res. 530, 40–48.Kretschmann, H.J., Kammradt, G., Krauthausen, I., Sauer, B., Wingert, F., 1986. Brain
growth in man. Bibl. Anat. 28, 1–26.Lancefield, K., Nosarti, C., Rifkin, L., Allin, M., Sham, P., Murray, R., 2006. Cerebral
asymmetry in 14 year olds born very preterm. Brain Res. 1093, 33–40.LeMay, M., 1976. Morphological cerebral asymmetries of modern man, fossil man, and
nonhuman primate. Ann. N. Y. Acad. Sci. 280, 349–366.Marlow, N., 2004. Neurocognitive outcome after very preterm birth. Arch. Dis. Child
Fetal Neonatal. Ed. 89, F224–F228.Matsuzawa, J., Matsui, M., Konishi, T., Noguchi, K., Gur, R.C., Bilker, W., Miyawaki, T.,
2001. Age-related volumetric changes of brain gray and white matter in healthyinfants and children. Cereb. Cortex 11, 335–342.
Millen, K.J., Gleeson, J.G., 2008. Cerebellar development and disease. Curr. Opin.Neurobiol. 18, 12–19.
Murphy, B.P., Inder, T.E., Huppi, P.S., Warfield, S., Zientara, G.P., Kikinis, R., Jolesz, F.A.,Volpe, J.J., 2001. Impaired cerebral cortical gray matter growth after treatment withdexamethasone for neonatal chronic lung disease. Pediatrics 107, 217–221.
Neil, J., Miller, J., Mukherjee, P., Huppi, P.S., 2002. Diffusion tensor imaging of normal andinjured developing human brain — a technical review. NMR Biomed. 15, 543–552.
Nosarti, C., Al-Asady, M.H., Frangou, S., Stewart, A.L., Rifkin, L., Murray, R.M., 2002.Adolescents whowere born very preterm have decreased brain volumes. Brain 125,1616–1623.
Peterson, B.S., Anderson, A.W., Ehrenkranz, R., Staib, L.H., Tageldin, M., Colson, E., Gore, J.C., Duncan, C.C., Makuch, R., Ment, L.R., 2003. Regional brain volumes and their laterneurodevelopmental correlates in term and preterm infants. Pediatrics 111,939–948.
Peterson, B.S., Vohr, B., Staib, L.H., Cannistraci, C.J., Dolberg, A., Schneider, K.C., Katz, K.H.,Westerveld, M., Sparrow, S., Anderson, A.W., Duncan, C.C., Makuch, R.W., Gore, J.C.,Ment, L.R., 2000. Regional brain volume abnormalities and long-term cognitiveoutcome in preterm infants. Jama 284, 1939–1947.
Pfefferbaum, A., Mathalon, D.H., Sullivan, E.V., Rawles, J.M., Zipursky, R.B., Lim, K.O.,1994. A quantitative magnetic resonance imaging study of changes in brainmorphology from infancy to late adulthood. Arch. Neurol. 51, 874–887.
Rakic, P., 1988. Specification of cerebral cortical areas. Science 241, 170–176.Ramakers, G.J., 2005. Neuronal network formation in human cerebral cortex. Prog. Brain
Res. 147, 1–14.

1153L.C. Tzarouchi et al. / NeuroImage 47 (2009) 1148–1153
Reiss, A.L., Abrams, M.T., Singer, H.S., Ross, J.L., Denckla, M.B., 1996. Brain development,gender and IQ in children. A volumetric imaging study. Brain 119 (Pt 5), 1763–1774.
Riedel, A., Klekamp, J., Harper, C., Kretschmann, H.J., 1989. Morphometric study on thepostnatal growth of the cerebellum of Australian aborigines and Caucasians. BrainRes. 499, 333–343.
Sowell, E.R., Peterson, B.S., Thompson, P.M., Welcome, S.E., Henkenius, A.L., Toga, A.W.,2003.Mapping cortical change across the human life span. Nat. Neurosci. 6, 309–315.
Sun, T., Patoine, C., Abu-Khalil, A., Visvader, J., Sum, E., Cherry, T.J., Orkin, S.H.,Geschwind, D.H., Walsh, C.A., 2005. Early asymmetry of gene transcription inembryonic human left and right cerebral cortex. Science 308, 1794–1798.
Takahashi, T., Shirane, R., Sato, S., Yoshimoto, T., 1999. Developmental changes ofcerebral blood flow and oxygen metabolism in children. AJNR Am. J. Neuroradiol.20, 917–922.
Thompson, D.K., Warfield, S.K., Carlin, J.B., Pavlovic, M., Wang, H.X., Bear, M., Kean, M.J.,Doyle, L.W., Egan, G.F., Inder, T.E., 2007. Perinatal risk factors altering regional brainstructure in the preterm infant. Brain 130, 667–677.
Toga, A.W., Thompson, P.M., 2003. Mapping brain asymmetry. Nat. Rev. Neurosci. 4,37–48.
Tokumaru, A.M., Barkovich, A.J., O'Uchi, T., Matsuo, T., Kusano, S., 1999. The evolution ofcerebral blood flow in the developing brain: evaluation with iodine-123 iodoam-phetamine SPECT and correlation with MR imaging. AJNR Am. J. Neuroradiol. 20,845–852.
Triulzi, F., Parazzini, C., Righini, A., 2005. MRI of fetal and neonatal cerebellardevelopment. Semin. Fetal. Neonatal. Med. 10, 411–420.
Watkins, K.E., Paus, T., Lerch, J.P., Zijdenbos, A., Collins, D.L., Neelin, P., Taylor, J., Worsley,K.J., Evans, A.C., 2001. Structural asymmetries in the human brain: a voxel-basedstatistical analysis of 142 MRI scans. Cereb. Cortex 11, 868–877.
Wood, N.S., Marlow, N., Costeloe, K., Gibson, A.T., Wilkinson, A.R., 2000. Neurologicand developmental disability after extremely preterm birth. EPICure Study Group.N. Engl. J. Med. 343, 378–384.
Xydis, V., Astrakas, L., Drougia, A., Gassias, D., Andronikou, S., Argyropoulou, M., 2006a.Myelination process in preterm subjects with periventricular leucomalaciaassessed by magnetization transfer ratio. Pediatr. Radiol. 36, 934–939.
Xydis, V., Astrakas, L., Zikou, A., Pantou, K., Andronikou, S., Argyropoulou, M.I., 2006b.Magnetization transfer ratio in the brain of preterm subjects: age-related changesduring the first 2 years of life. Eur. Radiol. 16, 215–220.