Embed Size (px)
Citation preview

0
Afghanistan Comprehensive Health Information System
Strategic Plan 2009-2013
Implementation Plan Details of activities under each intervention

1
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
Objective 1: Enact legislation that supports improved reporting of essential health data (AS from 0.7 to 2.5)
Intervention 1: Legislation is drafted and enacted to support improved reporting from public and private sector facilities
1.1 Inventory the existing legislation about statistics
related to health from MOPH laws and regulations,
CSO and Ministry of Justice; including the review of
International Health Regulations (IHR)
1.2 Coordinate with relevant ministries (e.g. MOI, CSO,
MOF) to review, improve and enact revised or draft
new legislation and regulations to establish an
enabling legal and regulatory framework for the HIS
(including private sector reporting, & notifiable
diseases)
Inventory of current legislation
related to health reporting and
statistics; along with international
and national needs for new
legislation
Statistics Law or Law of Medicine
(as appropriate) includes
adequate language on HIS and
private sector data and reporting
requirements
Jan 09
Jan 10
Jun
Dec 09
Dec 11
MOPH Laws
and
Regulation
Office
Int’l TA (4 1-mo
visits)
Nat’l consultant
(6-month
assignment)
1.3 Coordinate with relevant ministries to develop
adequate procedures for enforcement of laws and
regulations regarding HIS
- Procedures for enforcement
- Improved registration of private
healthcare providers & reporting
of notifiable diseases by private
sector
Jan 12
Mar 12 MOPH Laws
and
Regulation
Office
Expat and
national experts
as consultants
(2 months each)
Objective 2 : To increase the % of HIS service staff with capacity in managing and performing HIS responsibilities and functions from <20% to 80%
Intervention 2.1: Include training on health information system in “in-service training” (additional program-specific training bolded w/in other interventions)
2.1.1 Clarify responsibility of MOPH central and
provincial staff with regard to HIS functions
2.1.2 Improve the TOR of individual departments with
regard to HIS and M&E
Documented list of required HIS
qualifications/skill sets
Mar 09 Jun 09 GD PP, with
support of
APHI
DG P&P
Dr Ashraf
TA (existing
JHU; Tech-
Serve; ISMPL;
EPOS support )
2.1.3 In-service Training/HR Needs Assessment related
to HIS management and use (referring to past
TRAs)
2.1.4 Update the inventory of HIS-related curriculum and
courses being conducted
2.1.5 Summarize the apparent skills and functions
development required by this HIS SP
Priority HIS in-service training
needs
Apr 09 Jul 09 APHI with
support of
HMIS, M&E;
Dr. Islam
2.1.6 Review in-service training material with all existing
training partners and coordinate the development
Updated standardized HIS
training curricula for all levels
Sept 09 Mar 10 APHI Dr. Islam Expertise (2
p/m)

2
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
of standard HIS curricula and materials based on
the defined needs (with an especial emphasis on
“Data Use” and “evidence-based decision making”
skills)
2.1.7 Define a 2-year overall HIS training plan with a
special emphasis on community, facility and
provincial levels (who and what), which confirms
sources of resource support and the responsible
departments, programs and implementers.
- A comprehensive 2-year HIS
In-service training plan
- Service implementers (NGOs
under PPA, PGC, PCH & SM)
Mar 10 May 10 APHI with the
support of
HMIS; M&E;
Dr. Islam;
2.1.8 Provide in-service training to MOPH HMIS and
M&E staff, PPHOs according to the HIS training
plan:
2.1.8.1 basic training on data use and monitoring
(Approx 34 X 9 PPHO staff)
2.1.8.2 comprehensive training including basic
epidemiology & statistics (34X1 PPHO plus one
staff per NGO and up to 30 staff at central level)
2.1.9 Organize continuing in-service learning on data
use at the health facility and provincial levels (
- Approximately 306 PPHO
staff receive basic (in-service)
training in HMIS and M&E
- Approx 104 PPHO, NGO and
Central staff receive
comprehensive HMIS course
- A strategy by which 200
health facility staff learn data
use through team processes
within their provinces every
year
Ongoing
Jan 11
Dec 10
Jan 12
HMIS HMIS;
M&E;
Funds for
training
(TechServe,
JHU, GF)
2.1.10 Sponsor 5 persons to receive short courses in
health database design and development
including TB, malaria, pharmacy, healthcare
financing, HIV programs
5 MoPH database design
specialists receive short-course
training tailored for health
purposes
Jan 10 Mar 10 HMIS DB design
expert- 2 visits
of 1-month
each;
Training costs
2.1.11 Arrange for 5 senior staff to attend CDC Field
Epidemiology short course
5 senior staff from various
programs complete CDC Field
Epid Course
Mar 10 May 10 APHI
DEWS
Costs of course
and Travel
2.1.12 Design and conduct a short field epidemiology
course
- Short Epid Course design
- 3 in-country short courses
conducted for 10 staff each
Jan 10 Jul 10 APHI TA
Training Costs
(GF Rd 8)
2.1.13 Undertake Field Epidemiology Training Program
(FETP) for 3 cohorts of 8 persons each while
- 24 selected MOPH staff
complete the FETP
2009 2011 APHI / DEWS Funds and FETP
program

3
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
institutionalizing the capacity for delivering such
training for strengthening the surveillance
system within the APHI
- FETP training is
institutionalized within the
APHS
guidance (FG Rd
8)
Intervention 2.2: Include training on health information system in “pre-service training” of health workers
2.2.1 Strengthen the existing public health
management curriculum for new MD graduates
with regard to HIS
2.2.2 Organize HIS lectures for MD students at 5
medical universities
Revised PH Management
Curriculum with new HIS
functions and material
HIS course material developed for
medical universities
Ongoing
April 10
Apr 10
Jun 10
APHI
Dr. Islam
2.2.3 Work with AK DN and public health department
of 5 universities and training schools develop HIS
courses for nursing, midwifery
HIS credit courses designed and
incorporated into the training
curriculums for nursing and WMs
Jan 11 Mar 11 APHI TA support from
AK DN (existing)
2.2.4 Work with APHI and qualified private higher
education institutions to develop HIS courses for
inclusion in MPH degree
All MPH degrees include HIS
credit courses
Jan 11 Mar 11 APHI
Objective 3 : Improve the completeness and data quality of the HMIS and harmonize indicators (80% of all health facilities and all 34 provinces have implemented the
revised HMIS by Dec 2011)
Intervention 3: Develop and implement a range of improvements to the HMIS, review of indicators and stratification, integration of data from special programs,
enhancement of data quality and scaling-up NMC at provincial level
3.1 Scale-up the nationwide implementation of National
Monitoring Checklist (NMC) and joint monitoring to
enhance HMIS data validation
3.2 Review and improve SOW of PPHO, TB, EPI DEWS and
NGOs officers regarding processes for data quality
improvement and the implementation of NMC along
with joint coordination meetings to reinforce these
responsibilities.
3.3 Ensure action plans are developed and implemented
to improve HMIS & vertical programs’ data quality
after application of NMC and vertical program
supervision; joint coordination meetings
3.4 Improve NMC/data quality database
3.5 Standardize data validation/ data quality assessment
- Strategy, procedures and
schedule for each health facility
to be visited at least once every
quarter for data validation
- consensus is created regarding
roles, responsibilities of PPHO,
TB, DEWS, EPI officers and
processes for data quality
monitoring and improvement
- Schedule and conduct of
periodic coordination meetings
conducted in each province to
reinforce these responsibilities
- Action plans for data quality
Jun 09
Jun 10
Jun 10
Jun 10
Contin’g
Contin’g
GD PP
(M&E/QA)
GD PP, HMIS,
M&E
Funding and
Facilitation
(GAVI)

4
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
incorporated in supervision programs of vertical
programs
3.6 Review, update and stratify, by health system levels,
the official set of core health indicators for use to
guide all programs and services monitoring and
reporting efforts
improvement
- Improved data quality database
- Procedures for program data
quality validation
- Revised list of core health
indicators, definitions and data
sources
Jun 10
Jun 09
May 09
July 10
Aug 09
May 09
GD PP
HMIS
GD PP
HMIS
3.7 Ensure timely evaluation of any newly introduced data
collection tool with particular emphasis on data
quality
Procedure to insure any newly
introduced data collection tools
are evaluated when designed and
after 1-year of application
ongoing Jun 09 HMIS with
support of
M&E
3.8 Organization and support of early set-up,
implementation management and monitoring of the
HIS Strategic Plan
Selection of a Mgt & Mon Officer
for HIS SP oversight (GCMU or
HMIS)
HIS Implementation Working
Group – Qtrly Progress Reports
May 09 Dec 13 60 mos Salary
7 Grp Meetings
TA 5 visits (all
GF supported)
3.9 Establish regular and systematic “pooled” analysis of
data from multiple sources to improve accuracy and
consistency of key health indicators
3.10 Incorporate appropriate measures into NGO
contracts to encourage good quality data
3.11 Provide GCMU with results of data quality
assessments as a part of NGO performance
evaluation
3.12 Insure provincial profiles and annual reports include
sections with key health indicator data benefiting
from pooled data analysis
- Add 1 Data analysis staff
- MOPH key reports include
analysis of “pooled data” from
multiple sources for key health
indicators
- Draft wording for inclusion in
NGO contracts
- Procedures for sharing results
of HMIS reporting and data
quality assessment with GCMU
- Guidance for PPHO report
preparation (Obj 17)
Apr 10
Apr 09
Apr 09
Jun 09
Jun 10 (contin’
g)
Jun 09
Jun 09
Dec 09
M&E (HMIS)
GCMU (HMIS
supt)
HMIS
HMIS
Salary for 60 M
TA 2 C make 1
visit of 2 mos
1 server, 2
comp
3.13 Assemble all recommendation for improvement of
the HMIS and its registers and records for adding
indicators, integrating data from special programs
- updated HMIS records,
registers and procedures
Apr 09 Dec 10 HMIS
throughout
Funds by BPHF
& GF round 8

5
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
and incorporating gender specificity for selected
indicators,
3.14 Revise/translate/publish new HMIS manual
3.15 Revise HMIS databases as needed
3.15 Train 1,575+ HF on revised formats
- Revised HMIS Manual
- Revised HMIS Databases
- Staff in 1,575 facilities and all
PPHOs trained in the system
Objective 4: Data warehouse functionality developed (AS rises from 1.5 to 2.5) by 2013
Intervention 4 : Develop resources, procedures and responsibilities for data warehouses at central and PPHO levels
4.1 Review existing databases, their data elements and
data dictionaries, file structure and data sources.
4.2 Identify types and sources (surveys, census, VR,
HMIS, special programs) of health-relevant data
felt to be most important for including in the initial
version of a central level health data warehouse.
4.3 Develop a composite list of priority health
indicators and data elements for which data is
needed from a variety of sources for the types of
health data identified in 4.2.
4.4 Develop the metadata dictionary for the data
categories, indicators and data elements which
clarifies data item definitions, field formats and
associated coding, along with data sources.
4.5 Design the health data warehouse architecture,
specify the database design, and record layout.
4.6 Confirm the availability of or purchase the data
management server and software
4.7 Prepare a prototype warehouse for testing with
standard and ad hoc queries, data analysis and
report preparation.
4.8 Work with the managers of the various data
sources to work out procedures for periodic data
transfer from cooperating institutions and
departments.
4.9 Train the central level data warehouse managers
Detailed description of existing
databases
List of priority types and
categories of data to be placed in
the initial data warehouse.
List of priority health indicators
and data elements
Initial health metadata dictionary
Prototype health data warehouse
for testing
Procedure for data flow and entry
into the warehouse
5 central level staff trained in
DW operations
Jan 10 Jan 11
HMIS for all
activities and
products
Dr Ashraf TA for all
activities ( 6
p/m from
TechServe, 3 2-
month
assignments for
two DW
designers )

6
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
in operating, maintaining and updating the system
4.10 Initiate the first version of the warehouse at central
level, operate for principle users and assess initial
performance.
4.11 Determine if mirror data storage or extracts are to
be implemented at the Provincial level and develop
the procedures and media for sharing the data with
PPHO.
Report of performance of the
data warehouse after 6 month of
operation
Data file extracts for use at PPHO
level
Objective 5 : Strengthen Health/statistical constituencies and coordination (AS from 1 to 3 )
Intervention 5 : Establishment of inter-ministerial (health and statistical constituencies) coordinating body for HIS, and liaison offices for coordination and sharing of
health, population and social information
5.1 Revise the SoW of the existing Inter-Ministerial
Committee on M&E to include coordination of
information systems development
The inter-ministerial committee
on M&E SoW is revised and
signed by all members and begins
coordination of information
systems, data sharing and use
Apr 09
May09
MOPH
Pol&Plan’g
Directorate
5.2 Appoint a liaison Office and Officer in the MoPH to
coordinate with other ministries and provide update
on HIS development strategies and activities
HIS Liaison Officer officially
identified
May 09 May09 MOPH
Pol&Plan’g
Directorate
5.3 Ensure timely and regular consultation and/or
decision making among the ministries and active
follow-up of decisions on data sharing
5.4 Establish regular information sharing between this I-
M C on M&E/IS and the ANDS inter-ministerial
comm..
Procedure to insure continuous
sharing of data and information,
and joint action-taking
coordinated by the Inter-
Ministerial Committee on M&I
and IS
June 09 Jun 09 Inte-
Ministerial
Committee
on M&E and
IS
Objective 6 : Census conducted in 2010 and 2020 – Enhanced use of population and vital statistics information for planning and monitoring (AS scores for use of census
and VR data raised to 3.0 (from 2 and 0 respectively)
Intervention 6.1: Promote availability and use of CSO pre-census population figures and annual population updates in planning at all levels of health service delivery
6.1.1 Improve regular communication with CSO and
advocacy by MOPH on the need for detailed and
disaggregated population data
A set of agreements with CSO
regarding:
- using a standard list of districts
including spellings and coding
- timing of release of population
Apr 09 Apr 09 HMIS

7
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
datasets every year
- regular sharing of population
information with MOPH
- assistance with resolving
discrepancies with previous
datasets
- assistance with district
boundaries and administrative
divisions of the country
6.1.2 Make available user-friendly disaggregated pre-
census population figures for planning by MOPH
departments and partners
6.1.3 Annually update HMIS database population
tables and linkages
- District level population
breakdown by age, gender
incorporated into HMIS and
readily available to central and
provincial planners.
- All programs have access to
most updated population data
with sufficient disaggregation
(age, gender)
Apr 09 Apr 09 HMIS
6.1.4 Support CSO in implementing census in 2010 Recommendation to CSO about
possible health questions in the
Census
Agreement on the involvement of
PPHOs, HFs & CHWs in the
conduct of the census
Jan 10 Mar 10 HMIS
Intervention 6.2: Support the development, availability and use of vital registration data by the MoPH and its partners
6.2.1 Oversee development and piloting of the
Demographic Surveillance System (DSS) by the
MOPH
6.2.2 Expand the number of DSS sites
6.2.3 Develop a plan with CSO, MOI/VR, DSS
contractor and MOPH concerned departments
ensuring the sustainability of DSS including
availability of resources at provincial level to
- DSS is established and running
(with at least one complete
year data on a key set of
indicators in the pilot
provinces)
- DSS rollout/scale-up plan
- DSS sustainability plan and
recommendations for the
Mar 09 Sep11 HMIS Dr. Ashraf Funds
(GAVI-HSS)

8
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
maintain DSS MoPH
6.2.4 Coordinate with MOI for sharing (supporting
registration and receiving information)
information on Vital Registration
- An agreement with MOI
regarding vital registration
system and data including: linking
with DSS, sharing of VR data
available with MOI
- Procedure for providing VR data
inputs of birth and death
registration from health facilities
Jan 10 Jun 10 HMIS
Objective 7: Comprehensive, multi-year survey plan is in place and updated biannually
Intervention 7: Prepare and implement a multi-year plan for health surveys that insures timely, efficient availability of priority qualitative and quantitative indicators
(reducing survey overlaps and gaps)
7.1 Designate the M&E Directorate as responsible for
overseeing the MoPH health survey program, activity
and donor support, and for reviewing proposals for
all new surveys to determine their justification
7.2 Every two years, review the list of all key health
indicators used by MOPH departments and partners
(following on the creation of the meta data dictionary
as part of data warehousing.)
- Designation and MoPH-wide
acknowledgement of survey
oversight responsibility.
- A procedure for submitting
and approving proposals for
surveys
- Key indicator list and Meta-
data dictionary reviewed and
updated every two years,
published and widely
disseminated among MOPH
departments and partners
Apr 09
Apr 09
May 09
Apr 09
Apr 09
July 09
P&P Dir
M&E
M&E
7.3 Create and maintain an inventory of ongoing and
planned surveys including timeline of important
survey schedules and report due dates
7.4 Develop a comprehensive multi-year plan for health
related surveys in close coordination with CSO and
the inter-ministerial M&E/IS Coordination Committee
for fulfilling timely measurement of the full list of key
health indicators.
- An updated inventory and
schedule of planned health
surveys and special studies
- multi-year plan for population-
based surveys approved by
Executive Board and Inter-
Ministerial M&E/IS Coordination
Committee
May 09 Sep 09 M&E with
support of
MOPH
Research
Depart
Data
repository
officer at
M&E
Funding and TA
(GF)
7.5 Plan for staff within the MOPH to technically oversee - one focal point in each Mar 09 Dec 10 APHI Funding and TA

9
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
the design, management and analysis of population
based surveys and health studies including studies
and research
7.6 Obtain 4 scholarships for biostatistics and
demography
department qualified in survey
and health study design.
- Two masters level graduates
focused on biostatistics and 2 on
demography
for in-service
training (GAVI
and GF)
Four
scholarships
Objective 8: Integrated, multi-level health M&E activities, including an M&E Plan for Community-based health care carried out by all facilities and 40% of communities
Intervention 8.1: Strengthen coordinated monitoring and evaluation of all health activities integrating data from vertical programs, HMIS and DEWS, along with
relevant survey data
8.1.1 Review and coordinate M&E strategies and plans
for programs across MoPH departments
8.1.2 Identify data sources in all MoPH programs and
their links with HMIS for essential data elements
and indicators
8.1.3 Establish quarterly meetings of M&E focal points
from each department at central and provincial
levels to increase coordination and identify M&E
issues.
8.1.4 Add one position at PPHO to support use of data
for service M&E
8.1.5 Train staff in each MoPH Directorate and PPHO
on basic and comprehensive data analysis and
use, and analytical report writing.
8.1.6 Establish procedures for increased number of joint
monitoring visits by PPHCCs and train the
members as a team to used the findings more
effectively for local problem-solving,
Procedure for M&E Dir to sign off
on M&E plans for all major
policies, strategies and programs
Meta-data dictionary includes
updated mapping of sources of
key indicators (within Obj 4)
M&E information sharing through
4 quarterly meetings
AHMIS Officers in 34 PPHOs
68 staff in PPHOs and 20 staff in
General Directorate of health
services are trained
Increased no. and coverage of
JMVs by 50% to 4 per year per
province
Efficient NMC data flow
established for all provinces in
two directions
Oct 09
Apr 09
Mar 09
Apr 09
Apr 09
May 09
Apr 09
Contin’g
Dec 09,
updateannual
Apr 09
Dec 10
Dec 10
May 09
Jun 09
M&E
APHI Res
Dept
M&E
HMIS
M&E
M&E
M&E
Funding for
salaries (GF)
Funding
Tech Advisors
(GF)
Funding (GAVI)
Intervention 8.2 : Develop and pilot a new innovative approach to monitoring of health service by involvement of the community
8.2.1 Advocate for an enhanced approach for monitoring
of health services by community
Support of the M&E/IS IMCC Jul 09 Dec 09 M&E Dept

10
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
8.2.2 Assemble lessons learned in monitoring from NGO
experiences in insecure areas (eg. AHDS)
Documented lessons learned Jan 10 Jun 10 M&E Dept
8.2.3 Develop strategies, guidelines and tools for
engaging communities in service monitoring
Official strategy and tool for
community service monitoring
Jul 10 Dec 10 M&E Dept
8.2.4 Pilot test Community monitor and roll out Improved CM and rollout
schedule
Jan 11 Mar 11 M&E Dept
Objective 9: Improved tracking of health sector inputs including health financing (AS 1.0 to 3.0), human resources and commodities (AS from 0 to 3)
Intervention 9.1 : Support improved tracking of health system finances including program budgets and expenditures at the central and provincial levels, and establish a
system of National Health Accounts
9.1.1 Assess the need and define the purposes of the
health financing system and information support
Need Assessment Paper on HCF
and FM data including NHA
Mar 09 Apr 09 HF Dept
Technical
Advisors
9.1.2 Specify the types of financial management data in
AFMIS and the BPHS and EPHS requirements
Short Report of financial data
requirements
Mar 09 Apr 09 HF Dept
Tech Advisors
9.1.3 HCF Department and the M&E Directorate
develop an action plan and design criteria for
tracking of finances by using AFMIS at the central
(ongoing) and provincial level
Action Plan for developing the
financial tracking system
Mar 09 Apr 09 HF Dept
TA
9.1.4 Develop procedures and a Manual for AFMIS AFMIS Procedures and
Operations Manual
Jun 09 May10 HF Dept Technical
advisor (EPOS)
9.1.5 Increase demand for and use of better health
financing information (sources, expenditures) for
planning by program and provincial health
directors; Develop guidelines and manuals and
train staff for linking national planning and
program budgeting
Procedures and Guidelines May10 Dec 10 Policy and
Planning
Directorate
TA
9.1.6 Develop a list of analyses from the NHA literature
that need to be developed for Afghanistan.
9.1.7 Develop guidelines and an implementation
activity plan for establishment of NHA, insuring
links to policy and decision making
9.1.8 Assess data sources and staff capacity available to
contribute to the establishment of National
Health Accounts
Report of national capacity to
develop NHA
NHA Implementation Plan
Jan 11
Apr 11
Jun 11
Mar 11
Jun 11
Jun 11
HF Dept
HF Dept
HF Dept
Short term
experts for all
activities (6 1-
month visits by
2 experts)
(EPOS, USAID)

11
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
9.1.9 Undertake the funding, allocation and utilization
studies and accounts design work needed to
establish the NHA
9.1.10 Define data flow mechanisms to support National
Health Accounts
9.1.11 Test the first version of the NHA with data from
the funding, allocation and utilization study
9.1.12 Train 6 staff in the operations, maintenance and
use of the NHAs system
Data flow design
Functional NHA within the HF
system
6 staff trained in the generation
of NHA reports
Jul 11
Jan 12
Mar 12
Mar 12
Dec 11
Mar 12
June12
May12
HF Dept
HF Dept
HF Dept
HF Dept
Intervention 9.2: Establish a drug management information system (DMIS) at central and provincial level as an enhanced tracking system for pharmaceuticals
procurement, importation, storage, distribution and rational use of medicine
9.2.1 Based on the pharmaceutical review, prepare an
action plan for developing the DMIS
9.2.2 Agree upon core indicators for the DMIS
9.2.3 Standardize the list of drugs to be imported
9.2.4 Computerize the current system of drugs
importation
9.2.5 Compile and disseminate information on drugs
importing at the central level for forward planning
9.2.6 Develop procedures for a coordinated drug
procurement system and tracking of drugs
9.2.7 Develop a Drug Management Information System
(DMIS) database for tracking and managing drug
supply systems (including cost) for public sector;
reflecting coordinated procurement procedures
DMIS development plan
List of core Drug management
indicators
Standard list of drugs for
importation
A program for modest tracking of
drugs ordered, cleared, received
and distributed, by funding
source
Standard report on drug
importation process and results
Procedures for procurement and
tracking described
First version of an operating DMIS
Apr 09
Jul 09
Jul 09
Sep 09
Sep 09
Jun 09
Feb 10
Sep 09
Sep 09
Sep 09
Sep 10
Dec 09
Jan 10
Feb 11
GDPA
GDPA
GDPA
GDPA
GDPA
GDPA (Cent
WH)
GDPA (Cent
WH)
TA 3-week visit
(SPS & TS))
(same as above)
TA (TechServe)
TA 2 visits for 3
weeks
TA (3 visits for 3
weeks)
Computers, LAN
9.2.8 Include requirements in NGO contracts to report
details of drugs received and cost
9.2.9 Breakdown BPHS, EPHS and national hospitals
drug requests and utilization within a periodic
report
Definition of drug reporting
requirements for NGO contracts
Report of drug utilization by level
of service (health center,
provincial hospitals, central
hospitals)
Apr 09
Jul 09
Jun 09
Sep 09
GDPA +
GCMU
TA (TS, 1 visit
for 2 weeks of
SPS)
9.2.10 Review and update standardized forms for Formats for drug management in Sep 09 Nov 09 GDPA/API TA (EC, TS, 1

12
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
managing drug supply in hospitals and
warehouses
9.2.11 Training of central and provincial level staff in
managing drug supply
hospitals and warehouses.
75 staff trained in the drug
management system at NGO,
PPHO and Central level
Jan 10
Jul 10
visit of 3 weeks
–SPS)
9.2.12 Plan for dissemination of information on drugs to
professionals and the public through the
operation of a Drug Information Center
Drug Information Center Jan 11 Jan 12 GDPA TA (2 visits of 3
weeks – SPS)
Intervention 9.3 : Further develop data management for Human Resources, including training, private providers and CHWs
9.3.1 Based on the HR assessment, review existing
efforts and develop an action plan for better
tracking HR workforce
9.3.2 Improve coordination with civil services for
exchange of requirements
National Action Plan for HR
management
List of items needed by CS DB &
realigned MoH HR Database
Under-
way
Mar 09
Jun 09
Apr 09
HR
HR
TA (2 visits of 3
weeks)
9.3.4 Decentralize HR database to provincial level
9.3.5 Prepare a training plan for and conduct capacity
building of HR staff at the province level
9.3.6 Explore ways to PRR the HR position in the
provinces
Strategy/Plan for procedurizing
Provincial HR DBs
Training Plan for PPHO staff
Approved HR positions at PPHO
Jan 10
Jan 10
Mar 10
Mar 10
HR
Training Costs
(EC, Continued)
9.3.7 APHI/HMIS Develop specifications for Training
database in coordination with HR
Specifications for Training data
base
Mar 09 May 09 APHI w/
HMIS
TA (TS)
9.3.8 Develop procedures for maintaining the HR
training database by programs for regular update
Procedures for maintaining HR
training database
May 09 Aug 09 APHI w/ HMIS TA (TS)
9.3.9 develop a CHW module for the HR database
9.3.10 Pilot the database and prepare guidelines
CHW Module of HR database
Guidelines
Mar10 Jun 10 CBHC TA (TS GAVI)
Forms
Objective 10: 80% of facilities receive maternal death notifications and conduct investigations
Intervention 10: Develop procedures for improving maternal and neonatal death notification from health facilities and for investigation of causes
10.1 Prepare procedural guidelines for instituting
maternal and neonatal death notification from
communities
� Review existing tools (Care International)
� draft or revise new tools
� prepare data flow
Draft Procedure manual for
maternal and neonatal death
notification and investigation
(verbal autopsy)
Jan 10 Sep 10 RH with the
support of
HMIS
TA 2 pers/mo
Funding
13
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
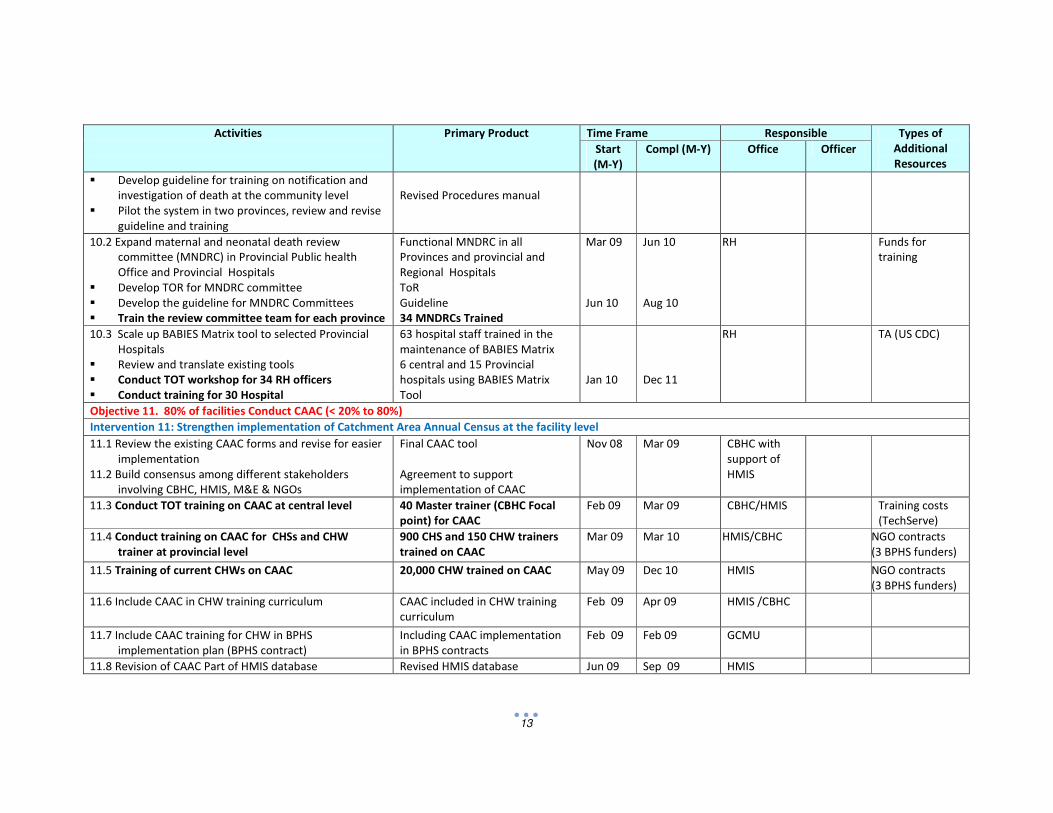
� Develop guideline for training on notification and
investigation of death at the community level
� Pilot the system in two provinces, review and revise
guideline and training
Revised Procedures manual
10.2 Expand maternal and neonatal death review
committee (MNDRC) in Provincial Public health
Office and Provincial Hospitals
� Develop TOR for MNDRC committee
� Develop the guideline for MNDRC Committees
� Train the review committee team for each province
Functional MNDRC in all
Provinces and provincial and
Regional Hospitals
ToR
Guideline
34 MNDRCs Trained
Mar 09
Jun 10
Jun 10
Aug 10
RH
Funds for
training
10.3 Scale up BABIES Matrix tool to selected Provincial
Hospitals
� Review and translate existing tools
� Conduct TOT workshop for 34 RH officers
� Conduct training for 30 Hospital
63 hospital staff trained in the
maintenance of BABIES Matrix
6 central and 15 Provincial
hospitals using BABIES Matrix
Tool
Jan 10
Dec 11
RH
TA (US CDC)
Objective 11. 80% of facilities Conduct CAAC (< 20% to 80%)
Intervention 11: Strengthen implementation of Catchment Area Annual Census at the facility level
11.1 Review the existing CAAC forms and revise for easier
implementation
11.2 Build consensus among different stakeholders
involving CBHC, HMIS, M&E & NGOs
Final CAAC tool
Agreement to support
implementation of CAAC
Nov 08 Mar 09 CBHC with
support of
HMIS
11.3 Conduct TOT training on CAAC at central level 40 Master trainer (CBHC Focal
point) for CAAC
Feb 09 Mar 09 CBHC/HMIS Training costs
(TechServe)
11.4 Conduct training on CAAC for CHSs and CHW
trainer at provincial level
900 CHS and 150 CHW trainers
trained on CAAC
Mar 09 Mar 10 HMIS/CBHC NGO contracts
(3 BPHS funders)
11.5 Training of current CHWs on CAAC 20,000 CHW trained on CAAC May 09 Dec 10 HMIS NGO contracts
(3 BPHS funders)
11.6 Include CAAC in CHW training curriculum CAAC included in CHW training
curriculum
Feb 09 Apr 09 HMIS /CBHC
11.7 Include CAAC training for CHW in BPHS
implementation plan (BPHS contract)
Including CAAC implementation
in BPHS contracts
Feb 09 Feb 09 GCMU
11.8 Revision of CAAC Part of HMIS database Revised HMIS database Jun 09 Sep 09 HMIS

14
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
11.9 Deliver learning opportunities on better use of CAAC
data at health facility level (as a part of data use
enhancement and calculation of coverage rates)
34 Provincial HMIS officer and 50
NGOs HMIS officers participate in
learning opportunities
Feb 10 Apr 10 CBHC w/
support of
HMIS
Objective12: Further Strengthen DEWS at the provincial and central level
Intervention 12: Further development of DEWS – Assessment scores for Mapping (III.D.1.3), diagnosis, analysis and response (III.D.2), HW knowledge of standard case
definitions (III.D.2.2) and % outbreaks supported with lab results (III.D.2.5) are all raised from 1.0 to 3.0 by 2013.
12.1 Establish effective coordination between DEWS,
special disease programs, HMIS/ M&E, PPHOs and
district officers including the integration of special
disease surveillance functions
12.2 Clarify DEWS info flow to departments and
programs in central level (including the Emergency
Response Program) in order they regularly receive
DEWS data and summaries
12.3 Develop procedure for linking geographic outbreak
mapping with action planning for preventive
activities at the central and provincial levels (as part
of annual and PI planning in Objective 18)
Procedures for integration of
surveillance functions and joint
disease data analysis
Official mechanism for sharing
DEWS information with all health
programs
Procedure for linking geographic
outbreak analysis and planning
prevention activities
Jun 09
Aug 09
Aug 09
Aug 09
Dec 09
Dec 09
DEWS w/
support of
HMIS
Funds and TA (4
TA visits of 3
weeks each) for
all activities
(from GF)
12.4 Develop DEWS database to be consistent with and
linked to other MOPH databases (through MoPH
data warehouse – Objective 4)
DEWS database linked to MoPH
data warehouse
Ma 09 Aug 09 HMIS TA (GF)
Objective 13 : All reports and surveys provide gender-specific data as appropriate by end 2010
Intervention 13 : Enhance the generation of gender-specific data and indicators (within routine registers, records reports and surveys)
13.1 Review and define which key indicators require
gender breakdown in data recording and report
preparation (as a part of Objective 3)
13.2 Engage ERB in the enforcement of compliance with
gender data standards for all surveys and
assessment
13.3 Revise HMIS procedures and formats to provide
gender-specific data where necessary and provide
on-site mentoring (as a part of Objective 3)
List of indicators that require
gender specificity
Procedure for ERB oversight of
gender-specific monitoring of
diseases and services
All surveys and data collection
registers and records support
gender disaggregation of data for
the indicators specified in 13.1
Ongoing Jun 09 HMIS with
support of
Gender Dept

15
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
13.4 Strengthen coordination and links between the
MOPH and other sectors for expanding the
generation and use of gender-specific health data
(as part of activities supporting Objective 5)
Coordinated activities for
strengthening gender-specific
monitoring and reporting on the
agenda of IMC – M&E/IS
May 09 May 09 M&E w/
Gender Dept
13.5 Ensure presentation of key health indicators with
appropriate gender breakdown
Main MOPH information products
such as Health Factsheet, report
on MDGs, ANDS progress reports
& MOPH/PPHO annual reports
include gender breakdown of key
indicators
Ongoing May 09 M&E w/
Gender Dept
13.6 Orient Gender Dep. staff on existing indicators and
available sources of gender information (BSC, HHS,
HMIS, census)
Inclusion of gender-specific data
analysis and reporting
(Related to activities under
objectives 3 and 18)
May 09 HMIS with
support of
Gender Dept,
M&E
Objective 14 : At least 90% of private facilities and practitioners are registered and at least 50% are regularly reporting through HMIS by end 2013
Intervention 14 : Establish, supported by legislation, private health provider registration and reporting procedures (including qualified practitioners, pharmacies,
private clinics & hospitals, diagnostic centers and laboratories)
14.1 Review and update existing regulations on
registering and reporting by private for-profit
facilities
Report of strengths and gaps in
current legislation and
regulations
Oct 09 Dec 09 GD SP, w/
Laws/Regs
14.2 Conduct a national survey to inventory active
private health facilities
Inventory of private health
facilities
Sep 10 Dec 10 GD SP w/ L&R funding (34
survey teams)
14.3 Develop a strategy and guidelines for registering
private providers, and for their reporting through
the HMIS
14.5 Review SOW of involved MOPH departments
(including PPHOs) to clarify who will be responsible
for managing and monitoring the registration of
private providers
14.6 Build the capacity of the designated MOPH officers
responsible for managing and monitoring the
registration and reporting of private practitioners
A procedure for registration and
reporting of private providers
with unique ID codes, and for
their HMIS reporting
Designation of responsible
officers for managing registration
of PP and reflection in their SoWs
40 central and PPHO staff trained
in the registration and monitoring
of private practitioners
Jan 10
Mar 10
Jun 10
Dec 10
Jun 10
Oct 10
GD SP w/ L&R
and HMIS
GD of SP- L&R
GD SP w/
HMIS
HMIS
Funds for
training (2 2-day
workshops)

16
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
14.7 Provide database support for proper registration of
private practitioners and facilities
Data base of private practitioners
and facilities
Mar 10 Jun 10 TA 1 p/m
TechServe)
14.8 Establish formats and procedures for monitoring
and reporting selected indicators of performance
of private providers
(Development of quality standards and monitoring for
private practitioners appears under Obj 15)
Private Provider performance
monitoring procedures and
report formats, presented at
national level at least annually
Jan 12 Mar 12 HMIS w/ GD
SP
TA (1 visit of 4
weeks)
Objective 15 : 40 % of facilities are monitoring quality of care by 2013
Intervention 15.1: Establish a quality measurement and assurance system for all levels health care, public and private (indicators, tools and procedures)
15.1.1 Review past and current quality assurance and
monitoring approaches and tools including FFSDP,
Balanced Scorecard, the JHPIEGO Quality
Assurance Tool, and the NMC Checklist to assess
current QA efforts and products.
15.1.2 Determine the office and staff to be responsible
for developing and managing the health care
quality assurance program and the offices to be
closely collaborating
15.1.3 Develop the capability of the staff assigned to QA
functions at central level
15.1.4 Define the set of procedures and tools to be used
in the Health Care QA program
15.1.5 Design the data repository for holding the results
of quality monitoring for reference and trend
analysis by facility, NGO, provincial and central
level
15.1.6 Design the analysis and report formats for
reflecting trends and current deficiencies in
quality of care at various service levels
Summary of current QA efforts
and results including the current
coverage with these practices
Office and staff designated to
develop and manage the QA
program, and the collaborating
offices
6 central staff to be oriented in
the process of designing and
implementing the QA scheme
Guideline and compendium of QA
tools to be used in health clinic
and hospital settings
Data repository for QA
monitoring results
Procedures and formats for
analyzing and reporting trends in
quality of care
May 09 Dec 09
All products
M&E/QA
(eventually
the unit
assigned for
QA
responsibility)
with support
of HMIS Unit
for all
activities
ST Technical
Advisor (1 3-
week visit)
STTA (2 visits of
3-weeks each)
Intervention 15.2 : Standardize hospital patient records and develop hospital service(quality) monitoring procedures
15.2.1 Develop national policy for hospital medical Medical records policy On-going Aug 09 HC GD

17
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
records
15.2.2 Review and update the existing hospital data
recording system including the redesign of a
standard patient record, along with the review
and selection of a minimum set of hospital
(EPHS) performance indicators
Updated hospital data recording
system focused on monitoring
patient care according to
minimum performance indicators
Sep 10 Jun 11 Dir of
Curative
Services
STTA (two visits
of 4 weeks
each)
15.2.3 Establish essential elements/standards of
medical record keeping at hospitals to help
improve the quality of recording and data
(initially for provincial hospitals then for national
hospitals at a later stages)
- Essential standards of medical
record keeping at hospitals
defined
- 34 provincial & 6 national
hospitals have implemented the
revised recording system
May 10
Dec 13
Dir of
Curative
Services
15.2.4 Develop Hospital Medical Record data base HMR Database On-going Aug 09 Health CGD
Intervention 15.3: Design and implement procedures for monitoring quality of hospital services
15.3.1 Develop hospital monitoring checklist (HMC) Hospital Monitoring Checklist Aug 09 Jul 10 M&E Dept STTA (two visits
of 4 weeks
each) 15.3.2 Review and finalize standards and tools for
quality assessment for hospitals both public and
private
Hospital quality standards and
measurement tools
Jan 10 Jul 10 M&E Dept
Objective 16 : Timely estimates of priority indicators are provided for stewardship – one MMR estimate during the period plus AS for Maternal Mortality (V.A.3.7), Child
Mortality (V.A.1.7) and Child malnutrition (V.A.5.5) rise from 0 to 3.0 by 2013
Intervention 16.1: Develop a methodology and plan for measuring MMR
16.1.1 Strongly support the ongoing MOPH senior
leadership efforts to select the most cost
effective methodology for estimating MMR and
advocate the development of a multi-year plan
for MMR assessments in Afghanistan
Decision regarding who will
conduct MMR survey with what
methodology
Under-
way
Jun 09 APHI w/
support of
M&E & RH
Depts
TA (2 visits of 3
weeks each)
(USAID, UNICEF)
16.1.2 Coordinate with CSO and other ministries with
regard to getting approvals for the conduct of
the MMR survey
CSO’s active support for the
survey is confirmed
Under-
way
Jul 09 M&E supp’d
by RH Dept
16.1.3 Oversee the selection of the survey
implementers and conduct of the MMR survey
One nationally representative
measurement of MMR
Jan 10 Jun 10 M&E/ RH
Dept
Funding for
survey costs
Intervention 16 .2: Design coordinated interventions for assessing child mortality including Demographic Surveillance System (DSS) and MICS

18
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
16.2.1 Oversee the design and further implementation
of Demographic Surveillance System
Expanded implementation of the
DSS See activity 8.2.1
Under-
way
Jun 10 M&E Funds (GAVI,
JHU)
16.2.2 Coordinate with UN partners and CSO on
including child mortality assessments in
upcoming MICS or MMR survey
Choice of survey and technically
sound measurement of child
mortality
Under-
way
Jun 09 M&E
16.2.3 Support refinement and scale-up of Catchment
Area Annual Census (CAAC) specially in insecure
areas and assure that CAAC data is used for
generating better estimates of child mortality at
provincial and national levels
CAAC implemented nationwide
(see objective 11)
Apr 09 Dec 10 HMIS
Intervention 16.3: Devise an approach for assembling and integrating morbidity data from various sources (DEWS, HMIS, prevalence and household surveys) for 12 key
communicable diseases
16.3.1 Convene the disease control group to confirm
the list of key communicable diseases for which
morbidity data from various sources will be
drawn on for periodically updating morbidity
rates
16.3.2 Determine for each disease the primary routine
sources of morbidity (case data)
16.3.3 Confirm case definitions for each disease
16.3.4 Determine the level of the services at which
multiple sources of case data are to be
integrated into a total case and morbidity rate
(probably the PPHO)
16.3.5 Devise a case identification number and method
for detecting duplicate reports for use at the
program and facility levels
16.3.6 Devise the format of the periodic report of CD
morbidity, the frequency of reporting and the
data files for maintaining the consolidated
reports.
Confirmed list of communicable
diseases whose morbidity rates to
be continuously monitored
List of CD case data sources
Confirmed case definitions and
site of case confirmations
Defined level of data integration
and report preparation
Procedure for case identification
and avoidance of duplication
reporting
CD Morbidity report format and
frequency of dissemination
Data base for morbidity data
Apr 09
Apr 09
May 09
Apr 09
Jun 09
Jul 09
May 09
May 09
Jun 09
May 09
Jul 09
Sep 09
DEWS w/
support of
HMIS
DEWS
DEWS
DEWS w/
support of
HMIS
DEWS w/
support of
HMIS
DEWS w/
support of
HMIS
Intervention 16.4: Devise cost-effective method for estimating prevalence of NCDs, including diabetes, hypertension, disability and mental health problems

19
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
16.4.1 Ensure that information on disability is collected
and analyzed as part of MICS in 2009
16.4.2 Design and implement special surveys to assess
prevalence of mental health problems, diabetes
and hypertension
Disability questions and
indicators included in the 2009
MICS
Surveys designed and conducted;
prevalence estimates available
Feb 09
Mar 11
Apr 09
Sep 11
Disability
Dept
GD Health
Care
TA (UNICEF)
TA (3 STTA
visits for 4
weeks each)
Intervention 16.5: Devise cost-effective methodology for measuring and monitoring <5 severe malnutrition at the provincial level, including tools development
16.5.1 Assist the Nutrition Department in analysis and
dissemination of existing information on severe
and chronic malnutrition
16.5.2 Establish coordination, data sharing and joint
work with CSO and NRVA for assessment of
malnutrition on a regular basis
16.5.3 Review and standardize existing tools for
malnutrition monitoring at the facility and
community levels
Malnutrition indicators and data
from existing sources
Agreed assessment approach and
data sources
Community Growth Monitoring
System
Dec 08
Mar 09
Mar 10
Feb 09
Sep 10
Sep 10
Nutrition
Dept
Nutrition
Dept
Nutrition
Dept
TA (2 visits of 3
weeks each)
UNICEF
Objective 17: All central Directorates & PPHOs produce annual reports including core health indicators by 2013 (AS VI.B.1 rises from 2 to 3)
Intervention 17: Streamline and enhance the quality of and broaden targeted distribution of health and service at central and provincial level, including results
conferences and PR events.
17.1 Assist provinces to focus on a manageable number
indicators supporting MOPH national strategies for
provincial planning and ongoing performance
improvement (These activities are undertaken as
part of Objectives 3 and 18)
As a part of the HMIS
improvement effort and data use
for provincial planning and
monitoring, core sets of
indicators exist for the central
and provincial levels
Apr 09 Dec 09 M&E w/
support of
HMIS
17.2 Design analytical reports of key indicators /results
with each directorate at the central level and for
PPHO at the province level
Standard recommended reports
of indicator levels and trends for
use at the central and provincial
levels
Jun 09 Dec 09 M&E w/
support of
HMIS
TA (1 visit for 3
weeks –
TechServe)
17.3 Coordinate among APHI, Tech-Serve, EC and decide
on a standard report writing course to be provided to
designated MOPH M&E staff
Joint decision by MOPH and
partners on the selected report
writing course
Dec 09 Jan 10 APHI (M&E)

20
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
17.4 Sponsor report writing courses for at least one
person per department/province with an emphasis
on analytical skills
60 staff complete the course, 2
staff of each department, 3
courses of 20 participants
Mar 10 Dec 10 APHI (M&E) TA (2 visits of 3
weeks)
Funding
17.5 Define a health information dissemination strategy
and key information products of MOPH around the
revised MOPH objectives and programs and establish
dissemination system for updates on core national
health indicators (addressing progress of main MOPH
strategies)
Health Information Dissemination
Strategy
List and definition of information
products (including reports)
linked with main MOPH strategies
Info dissemination strategy
(including bi-direction flow of
information products, frequency.
Jan 10 Jun 10 GD PP; M&E TA (2 STTA visits
of 2 weeks each
- Techserve)
17.6 Establish coordination between planning
department, program budgeting, ANDS & GDPP for
developing standardized national reports
Lead department for developing
HNSS report is identified
Jan 10 Mar 10 Planning
Directorate
(M&E)
17.7 Further develop annual Results Conferences at
MOPH to share and analyze progress/challenges
for making strategic policy decisions Review timing
of Results Conference/ Strategy Retreat to better
align it with planning/budgeting cycle of MOPH (by
CGHN and TAG). Link with provincial coordination
meetings
Content further organized around
implementation of national
strategies; agendas and style of
conferences further improved
Link with and provides inputs to
annual provincial coordination
meetings
Under-
way
Dec 2013 M&E w/
support of
HMIS and
DEWS
17.8 Standardize and maintain provincial health profiles
and link with integrated (provincial) planning (see
also activity 6.3)
Standard format developed for
provincial health profiles in
support of provincial plans
Aug 09 Dec 09 P&P Dir
Objective 18: Thirty-four PPHOs give evidence of data use for provincial planning, resource allocation and performance improvement; 75% of HF have periodic data use
sessions
Intervention 18: Develop guidance for and implement team approaches in using routine and survey data at central, PPHO, NGO and facility levels, including the weekly
“watch” of health events, performance monitoring, annual provincial planning and resource allocation and Performance Improvement planning
18.1. Improve availability of Balanced Score Card (BSC),
HMIS and DEWS data in a user friendly format at
various levels, but especially the provincial level
Electronic and hard copy of data
with appropriate level of
breakdown and reporting
features available at central,
provincial and health facility level
Jun 09 Dec 09 M&E w/
support of
HMIS and
DEWS

21
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
18.2. Strengthen evidence-based decision making skills in
MOPH Director Generals and Deputy Minister with
the expanded provision of quantified evidence and
the use of tools such as Executive Dashboards
Procedures and guidance for
preparing quantitative monitoring
and evidence for key policy-level
decision making forums including
CGHN and TAG
Jan 10 May 10 M&E w/
support of
HMIS; DEWS
and APHI
TA (1 visit for 1
month)
18.3. Develop and test training/learning materials and
guidelines for use of data for monitoring,
assessment and performance improvement at all
levels, which include the use of the HMIS, Balanced
Scorecard, and NMC, DEWS and quality
measurement and assurance.
• Annual-biannual planning and resource allocation
• “Weekly Watch” health and service monitoring
• Team service performance assessment and
improvement processes
• Facility data use sessions
18.4 Develop a roll-out plan and initiate implementation
of data use activities cited in 18.3
Procedures, tools and formats
within user-friendly guidelines for
use of data at provincial and
facility levels
Initial application of data use
activities has taken place in all 34
provinces
Jun 09
Jun 10
Jun 10
Jun 12
HMIS Technical
support (6 TA
visits of 3 weeks
each –Tech
Serve, EC, JHU)
TA support (6 3-
week visits
Funding
Objective 19 : A robust performance measurement system is in place to support Results-Based Financing (RBF) by January 2010
Intervention 19: Review existing, design improved, and assess pilot applications of service measurement methods in support of the RBF initiative
19.1 Review existing practices in community and
facility level service performance measurement
(LQAS by TechServe, Balanced Score Card, NMC,
etc.)
19.2 Provide input to the RBF design committee on
appropriate mechanism for monitoring service
performance at facility and community level
19.3 Map all donor interventions that may influence
service performance for use in choosing areas for
performance monitoring
19.4 Ensure adequate resources for the measurement
aspects of RBF including staff, training, equipment
and management capacity
Choice of practical RBF service
performance monitoring and
assessment approach
Procedures performance
monitoring at facility and
community levels
Map of all donor support to
services enhancement
Resources mobilized for service
monitoring in RBF areas
May 09
Jul 09
Jul 09
Jul 09
Sep 09
Jul 09
Nov 09
Aug 09
Jul 09
Sep 10
GCMU with
support from
M&E
TA (WB, Tech
Serve, EC)

22
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
19.5 Oversee the conduct of the 3rd
party monitoring of
service performance
19.6 Evaluate the pilot phase and provide the ministry
with lessons learned in RBF performance
monitoring.
Performance monitoring
conducted in initial RBF provinces
Decision on monitoring approach
for roll-out.
Oct 10
Dec 10
Funds (WB,
Norway)
Objective 20 : Data support developed for specific new strategies and services
Intervention 20.1: Develop procedures for collecting data on gender-based violence through appropriate mechanisms
20.1.1 Assist Gender Dept to coordinate with MoWA and
other ministries on how to be notified about and
monitor gender-based violence
20.1.2 Design a procedure for GV notification and
investigation between PPHOs and MoWA
provincial directors, including a procedure for
health service to report evidence of gender-based
violence
20.1.3 Obtain information and coordinate with planned
gender household surveys by MoWA
A system of regular exchange of
routine and survey data on
gender-based violence between
MoPH and MoWA is established
Procedure for GV notification and
investigation established
Results of Gender household
surveys available w/ each
province
Apr 10
Jun 10
Apr 09
Jun 10
Sep 10
May 09
Gender Dept
MoPH
Intervention 20.2: Facilitate development and maintenance of recording and reporting of services related to HIV/AIDS including drug users (as a part of overall HMIS
improvement and integration of data from special programs
20.2.1 Develop a standardized data collection system to
record and collect essential information on
health services on HIV/AIDS including drug users
20.2.2 Integrate the HIV/AIDS data system into the
HMIS
20.2.3 Scale up newly developed HIV/AIDS routine data
collection system
HIV/AIDS data recording and
reporting system
Elements of the HIV data within
HMIS reporting system and DB
Data system extended to all
central and provincial hospitals
May 09 May 10 NACP w/
support of
HMIS
TA and funds
(WB AHAPP)
Intervention 20.3: Develop recording and reporting of blood screening services (as a part of overall HMIS improvement and integration with the hospital data system
development)
20.3.1 Develop a standardized data collection system to
record and collect essential information on blood
screening services
Blood screening data system
Selected data elements and
Jun 09 Jun 11 Blood Bank ,
HMIS
TA and funds
(WB AHAPP)

23
Activities
Primary Product Time Frame Responsible Types of
Additional
Resources
Start
(M-Y)
Compl (M-Y) Office Officer
20.3.2 Integrate the blood screening data into the HMIS
20.3.3 Expand the blood screening service data to all
central and provincial hospitals
indicators added to the HMIS
System implemented in all central
and provincial hospitals
Intervention 20.4: Develop and maintain recording and reporting system for emergency preparedness and for monitoring the effects of disasters, and the services
delivered for the affected populations.
20.4.1 Coordinate with DEWS and Emergency
Preparedness and Response Dept to develop a
an emergency response data system
20.4.2 Review and confirm a list of notifiable diseases,
and other conditions prevalent as result disasters
and emergencies
20.4.3 Revise notifiable disease format as
needed for use in emergencies
20.4.4 Set up procedures for enabling notification of
health problems and monitoring response
actions during disasters and emergencies
20.4.5 Identify the department at the central level and
focal points at provincial level for managing
outbreak data collection and data transfer during
emergencies and disasters
Emergency and Disaster
Information System which
monitors persons whose health is
affected and the response and
services provided
• List of diseases and
conditions to be notified
• Procedures for notification
and monitoring of response
• Designation of responsible
offices for data
management at central and
provincial level
Sep
2009
Mar 2010 ERP TA (4 visits of 3
weeks)
Funding needed
for
communications





























