Embed Size (px)
Citation preview
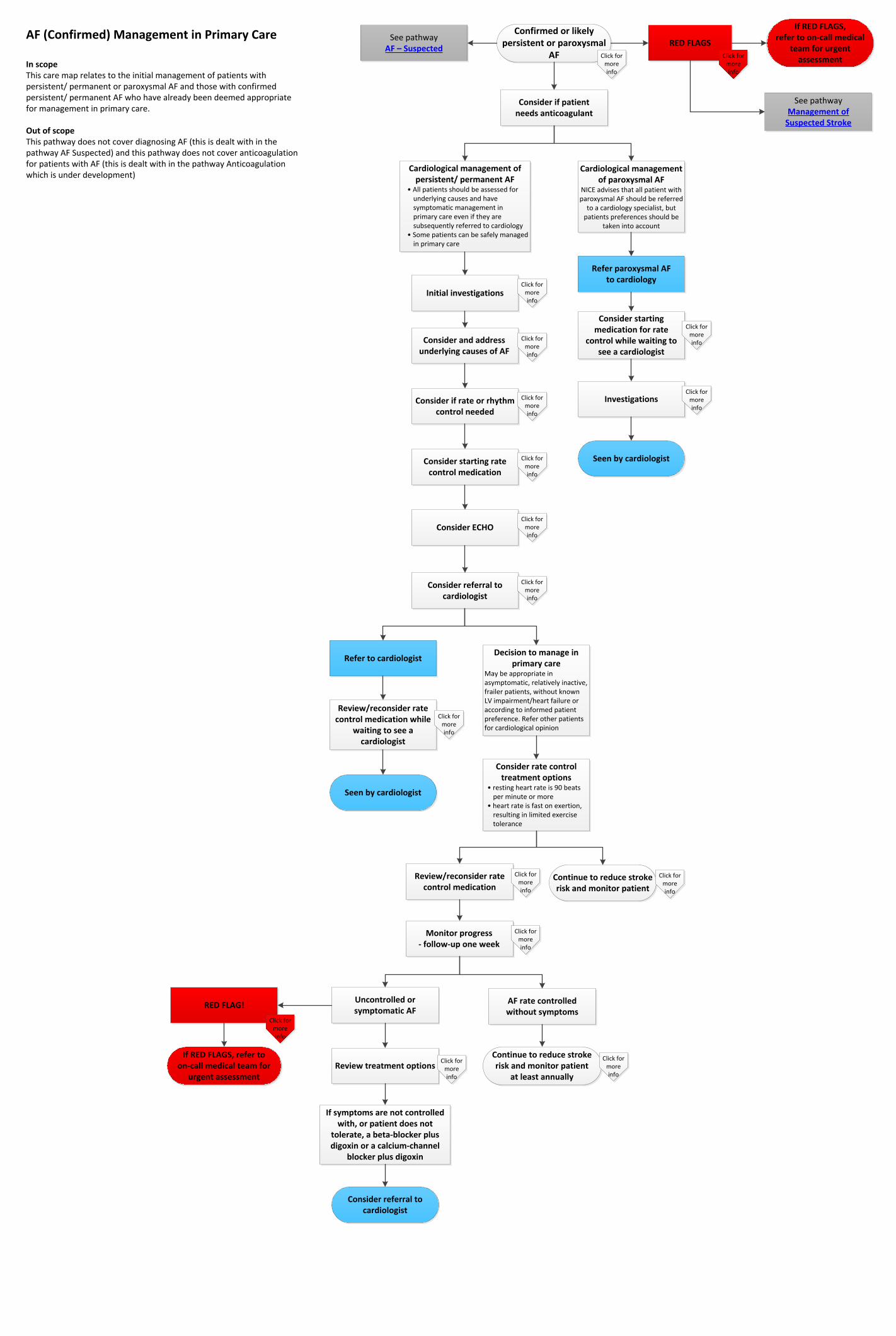
AF (Confirmed) Management in Primary Care
In scopeThis care map relates to the initial management of patients with persistent/ permanent or paroxysmal AF and those with confirmedpersistent/ permanent AF who have already been deemed appropriate for management in primary care.
Out of scopeThis pathway does not cover diagnosing AF (this is dealt with in the pathway AF Suspected) and this pathway does not cover anticoagulation for patients with AF (this is dealt with in the pathway Anticoagulation which is under development)
Confirmed or likely persistent or paroxysmal
AF Click for more info
See pathway AF – Suspected
RED FLAGS
Click for more info
If RED FLAGS,refer to on-call medical
team for urgent assessment
See pathway Management of
Suspected Stroke
Consider if patientneeds anticoagulant
Cardiological management of persistent/ permanent AF
• All patients should be assessed for underlying causes and have symptomatic management in primary care even if they are subsequently referred to cardiology
• Some patients can be safely managed in primary care
Initial investigationsClick for
more info
Consider and address underlying causes of AF
Click for more info
Consider if rate or rhythm control needed
Click for more info
Consider starting rate control medication
Click for more info
Consider ECHOClick for
more info
Consider referral to cardiologist
Refer to cardiologist
Review/reconsider rate control medication while
waiting to see a cardiologist
Click for more info
Seen by cardiologist
Decision to manage in primary care
May be appropriate in asymptomatic, relatively inactive, frailer patients, without known LV impairment/heart failure or according to informed patient preference. Refer other patients for cardiological opinion
Consider rate control treatment options
• resting heart rate is 90 beats per minute or more
• heart rate is fast on exertion, resulting in limited exercise tolerance
Review/reconsider rate control medication
Click for more info
Continue to reduce stroke risk and monitor patient
Click for more info
Monitor progress - follow-up one week
Click for more info
Uncontrolled orsymptomatic AF
RED FLAG!
If RED FLAGS, refer to on-call medical team for
urgent assessmentReview treatment options
Click for more info
Consider referral to cardiologist
AF rate controlledwithout symptoms
Continue to reduce stroke risk and monitor patient
at least annually
Click for more info
Cardiological management of paroxysmal AF
NICE advises that all patient with paroxysmal AF should be referred
to a cardiology specialist, but patients preferences should be
taken into account
Refer paroxysmal AFto cardiology
Consider starting medication for rate
control while waiting to see a cardiologist
Click for more info
InvestigationsClick for
more info
Seen by cardiologist
If symptoms are not controlled with, or patient does not
tolerate, a beta-blocker plus digoxin or a calcium-channel
blocker plus digoxin
Click for more info
Click for more info
Back to pathway
Confirmed or likely persistent or paroxysmal AF
Definitions:
• Paroxysmal AF, (PAF), lasts less than 7 days, with the majority of episodes terminating within 48 hours.
• persistent AF is present when an AF episode either lasts longer than 7 days or requires termination by cardioversion
• long-standing persistent AF has lasted for 1 year or longer when it is decided to adopt a rhythm control strategy
• permanent AF is said to exist when the presence of the arrhythmia is accepted by the patient (and physician) - rhythm control interventions are, by definition, not pursued in patients with permanent AF

Back to pathway
RED FLAGS
Refer to on-call medical team for urgent assessment if the person has any of the following:
• a rapid pulse (greater than 150bpm) and/or low blood pressure (systolic blood pressure less than 90mmHg)
• loss of consciousness, severe dizziness, ongoing chest pain, or increasing breathlessness
• a complication of AF, such as stroke, transient ischaemic attack, or acute heart failure
• ongoing chest pain
Although most patients in Atrial fibrillation (AF) present without haemodynamic compromise, some are significantly compromised and require immediate hospitalisation and urgent intervention to:
• alleviate symptoms of breathlessness, chest pain, and loss of consciousness
• restore haemodynamic stability

Back to pathway
Initial investigations
NB: If referral is considered appropriate do not wait for results of investigations before referring
Consider the following routine investigations:
• full blood count (FBC) - to exclude anaemia. Haemoglobin for safety reasons and to get baseline value for future monitoring
Platelets to get a baseline value when monitoring bleeding risk.
• blood urea and electrolytes, calcium, magnesium, to exclude electrolyte disturbances, which may precipitate AF
• creatinine and eGFR
• thyroid function tests
• chest radiography - to investigate a suspected lung abnormality, e.g. lung cancer, or detect heart failure
NB: additional tests are needed prior to anticoagulation:
• Clotting studies
• LFTs
Back to pathway
Consider and address underlying causes of AF
• often caused by co-existing medical conditions - both cardiac and non-cardiac
• common cardiac causes include:
• ischaemic heart disease - specifically mitral valve disease
• hypertension
• sick sinus syndrome
• pre-excitation syndromes, e.g. Wolff-Parkinson-White
• less common cardiac causes include:
• cardiomyopathy or hear muscle disease
• pericardial disease, including effusion and constrictive pericarditis
• atrial septal defect
• atrial myxoma
• non-cardiac causes include:
• acute infections, especially pneumonia
• electrolyte depletion
• lung carcinoma
• other intrathoracic pathology, e.g. pleural effusion
• pulmonary embolism
• thyrotoxicosis
Risk factors include:
• increasing age:
• the prevalence of AF roughly doubles with each advancing decade of age, from 0.5% at age 50-59 years to almost 9% at age 80-89 years
• AF is very uncommon in infants and children, unless concomitant structural or congenital heart disease is present
• diabetes mellitus (DM)
• hypertension
• valve disease
• surgery, especially cardiothoracic operations such as thoracotomy and coronary artery bypass graft
• lifestyle factors, such as:
• excessive alcohol consumption
• excessive caffeine consumption
• emotional or physical stress

Back to pathway
Consider if rate or rhythm control needed
When to offer rate or rhythm control
Rate control:
Offer rate control as the first-line strategy to people with atrial fibrillation, except in people:
• whose atrial fibrillation has a reversible cause
• who have heart failure thought to be primarily caused by atrial fibrillation
• with new-onset atrial fibrillation
• with atrial flutter whose condition is considered suitable for an ablation strategy to restore sinus rhythm
• for whom a rhythm control strategy would be more suitable based on clinical judgement
Rhythm control:
Consider pharmacological and/or electrical rhythm control for people with atrial fibrillation whose symptoms continue after heart rate
has been controlled or for whom a rate-control strategy has not been successful.
NB: rhythm control strategies are usually initiated in secondary care and a blood clot must be excluded via ECHO prior to initiation.
Back to pathway
Consider starting rate control medication
Rate control
Offer either a standard beta-blocker (that is, a beta-blocker other than sotalol) or a rate-limiting calcium-channel blocker (diltiazem (off-label) or verapamil) as initial monotherapy to people with atrial fibrillation who need drug treatment as part of a rate control strategy.
Base the choice of drug on the person's symptoms, heart rate, comorbidities and preferences when considering drug treatment.
Consider digoxin monotherapy for people with non-paroxysmal atrial fibrillation only if they are sedentary.
If maximally tolerated monotherapy with a rate-limiting calcium-channel blocker (diltiazem (off-label) or verapamil) or a beta-blocker does not fully control symptoms, and if continuing symptoms are thought to be due to poor ventricular rate control, consider adding in digoxin.
If maximally tolerated monotherapy with digoxin does not fully control symptoms, and if continuing symptoms are thought to be due to poor ventricular rate control, consider adding in a rate-limiting calcium-channel blocker (diltiazem (off-label) or verapamil) or a beta-blocker.
https://cks.nice.org.uk/atrial-fibrillation
Do not offer amiodarone for long-term rate control.
Back to pathway
Consider ECHO
Perform transthoracic echocardiography (TTE) in people with atrial fibrillation:
• for whom a baseline echocardiogram is important for long-term management
• for whom a rhythm-control strategy that includes cardioversion (electrical or pharmacological) is being considered
• in whom there is a high risk or a suspicion of underlying structural/functional heart disease (such as heart failure or heart murmur) that influences their subsequent management (for example, choice of antiarrhythmic drug or anticoagulant)
• in whom refinement of clinical risk stratification for antithrombotic therapy is needed

Back to pathway
Consider referral to cardiologist
· Any known valve disease
· Patient has a murmur and does not have a prosthetic heart valve
· Patient is symptomatic EHRA class 2 or above (breathless, palpitations, reduced exercise tolerance) despite rate control
· Has known impaired LV function
· New ischaemic heart disease is suspected
· If ablation or cardioversion could be considered i.e. in younger active patients in whom the long-term implications of AF and subsequent
anticoagulation are significant
NB: intervention with ablation or cardioversion is more likely to be successful in early stages after diagnosis
Consider referral to cardiologist
· Any known valve disease
· Patient has a murmur and does not have a prosthetic heart valve
· Patient is symptomatic EHRA class 2 or above (breathless, palpitations, reduced exercise tolerance) despite rate control
· Has known impaired LV function
· New ischaemic heart disease is suspected
· If ablation or cardioversion could be considered i.e. in younger active patients in whom the long-term implications of AF and subsequent
anticoagulation are significant
NB: intervention with ablation or cardioversion is more likely to be successful in early stages after diagnosis

Back to pathway
Continue to reduce stroke risk and monitor patient at least annually
At least annual review of CHA2DS2VASc and HAS-BLED scores are needed with review of symptoms, blood pressure and appropriate treatment and life-style advice to prevent stroke and referral to consultant cardiologist where appropriate.
Do not offer antithrombotic therapy to people aged under 65 years with atrial fibrillation and no risk factors other than their sex (that is, very low risk of stroke equating to a CHA2DS2VASc score of 0 for men or 1 for women).
Reviewing established atrial fibrillation (AF):
• check for ongoing symptoms, both at rest and upon exercise
• assess heart rate
• check for complications of AF and assess blood pressure - identify and manage existing heart failure or hypertension
• review the patient's medication:
• if patient is currently taking anticoagulants, reassess risk of bleeding, including risk of falls
• check compliance and identify and manage drug interactions and complications, such as dyspepsia with aspirin
• give advice on known drug interactions and which drugs should be avoided with anticoagulants

Back to pathway
Monitor progress - follow-up one week
Follow-up within 1 week:
• Check whether the patient is tolerating the medication - if the patient is unable to tolerate the current medication, prescribe an alternative
• Review symptoms, heart rate, and blood pressure
Check for ongoing symptoms, both at rest and upon exercise
• assess heart rate and assess blood pressure
• check for complications of AF - identify and manage existing heart failure or hypertension
• review the patient's medication:
• if patient is currently taking an anticoagulant, reassess risk of bleeding, including risk of falls
• check compliance and identify and manage drug interactions and complications
• give advice on known drug interactions and which drugs should be avoided with aspirin or warfarin
Back to pathway
Review treatment options
If the patient's symptoms and/or heart rate are not controlled, consider increasing the dose to control symptoms.
If the patient is taking the maximum drug dose, consider combining drug treatments:
• to control symptoms during normal activities only, offer a beta-blocker or calcium-channel blocker (diltiazem (off-lable use) or verapamil) with digoxin
• to control symptoms during normal activities and during exercise, offer a calcium-channel blocker (diltiazem or verapamil) with digoxin
• if the patient is already taking a beta-blocker, it may be more practical to add in digoxin first, and if symptoms are still not controlled, then switch the beta-blocker with a calcium-channel blocker
Do not initiate a combination of a beta-blocker and a rate-limiting calcium-channel blocker in primary care





























