Embed Size (px)
Citation preview

Clinical Science (2013) 125, 1–17 (Printed in Great Britain) doi: 10.1042/CS20120588
Advances in our understanding of diabeticretinopathyAlan W. STITT∗, Noemi LOIS∗, Reinhold J. MEDINA∗, Peter ADAMSON† and Timothy M. CURTIS∗
∗Centre for Vision and Vascular Science, Queen’s University of Belfast, The Royal Victoria Hospital, Belfast BT12 6BA, U.K.†Ophthiris Discovery Performance Unit, GlaxoSmithKline Ophthalmology, Medicines Development Centre, Stevenage SG1 2NY, U.K.
AbstractDiabetic retinopathy remains the most common complication of diabetes mellitus and is a leading cause of visualloss in industrialized nations. The clinicopathology of the diabetic retina has been extensively studied, although theprecise pathogenesis and cellular and molecular defects that lead to retinal vascular, neural and glial celldysfunction remain somewhat elusive. This lack of understanding has seriously limited the therapeutic optionsavailable for the ophthalmologist and there is a need to identify the definitive pathways that initiate retinal celldamage and drive progression to overt retinopathy. The present review begins by outlining the natural history ofdiabetic retinopathy, the clinical features and risk factors. Reviewing the histopathological data from clinicalspecimens and animal models, the recent paradigm that neuroretinal dysfunction may play an important role in theearly development of the disease is discussed. The review then focuses on the molecular pathogenesis of diabeticretinopathy with perspective provided on new advances that have furthered our understanding of the keymechanisms underlying early changes in the diabetic retina. Studies have also emerged in the past year suggestingthat defective repair of injured retinal vessels by endothelial progenitor cells may contribute to the pathogenesis ofdiabetic retinopathy. We assess these findings and discuss how they could eventually lead to new therapeuticoptions for diabetic retinopathy.
Key words: diabetes, diabetic retinopathy, retina, visual loss
EPIDEMIOLOGY OF DIABETIC RETINOPATHY
The worldwide incidence of diabetes is set to rise dramaticallyfrom 171 million people to an estimated 366 million in 2030[1,2]. Type 1 diabetes is due primarily to autoimmune-mediateddestruction of pancreatic β-cells, which leads to insulin defi-ciency. The frequency of Type 1 diabetes is low relative to Type 2diabetes, which accounts for approximately 90 % of diabetesworldwide. The phrase ‘diabetes epidemic’ refers predominantlyto Type 2 diabetes, which is continuing to increase in both de-veloped and developing countries [3]. This increase in Type 2diabetes is mainly a consequence of increasing sedentary life-styles, poor diet and obesity. Indeed, it has been estimated thatthe prevalence of diabetes among people aged >16 years willrise by 28.3 % between 2010 and 2030, with 54.5 % of this in-
Abbreviations: AGE, advanced glycation end-product; AMD, age-related macular degeneration; BCVA, best correct visual acuity; BM, basement membrane; BP, blood pressure; BRB,blood–retinal barrier; CA, carbonic anhydrase; CSMO, clinically significant macular oedema; DCCT, Diabetes Control and Complications Trial; DMO, diabetic macular oedema; DRCR.net,Diabetic Retinopathy Clinical Research network; EDIC, Epidemiology of Diabetes Interventions and Complications; EPC, endothelial progenitor cell; EPO, erythropoietin; ERG,electroretinogram; ETDRS, Early Treatment of Diabetic Retinopathy Study; GFAP, glial fibrillary acidic protein; HbA1c, glycated haemoglobin; HMT, histone methyltransferase; IL,interleukin; IRMAs, intraretinal microvascular anomalies; NF-κB, nuclear factor κB; NPDR, non-proliferative diabetic retinopathy; Nrf2, nuclear factor erythroid 2-related factor 2; OIR,oxygen-induced retinopathy; PDGF, platelet-derived growth factor; PDR, proliferative diabetic retinopathy; PKC, protein kinase C; PKK, prekallikrein/kinin; RAGE, receptor for AGEs; RCT,randomized control trial; ROS, reactive oxygen species; RPE, retinal pigment epithelium; TNFα, tumour necrosis factor α; UKPDS, UK Prospective Diabetes Study; VEGF, vascularendothelial growth factor.
Correspondence: Professor Alan W. Stitt (email [email protected]).
crease being attributed to increased obesity [4]. The health issuesthat diabetes imposes on societal healthcare are daunting, notleast the range of debilitating complications associated with thiscondition. The macro- and micro-vascular complications arisingfrom diabetes impose an ever-increasing burden on healthcareauthorities globally.
Diabetic retinopathy is the most frequently occurring mi-crovascular complication of diabetes and, although not all pa-tients will suffer appreciable vision loss, this condition remains aleading cause of blindness. Following 20 years of diabetes, nearlyall patients with Type 1 diabetes will have at least some retino-pathy. Moreover, ∼80 % of insulin-dependent Type 2 diabeticpatients and 50 % of Type 2 diabetic patients not requiring exo-genous insulin will have retinopathy after 20 years of diabetes[5,6]. In Europe and the U.S. alone, the WHO (World Health
www.clinsci.org 1
Clin
ical
Sci
ence
ww
w.c
linsc
i.org

A. W. Stitt and others
Organization) has estimated that diabetic retinopathy accountsfor approximately 15–17 % of total blindness [7]. Worldwide,diabetic retinopathy is an even bigger problem, and a compre-hensive study by Yau et al. [8] based on 22 896 individuals from35 studies in the U.S., Australia, Europe and Asia demonstratedthat the prevalence of diabetic retinopathy was almost 35 % withincreasing risk associated with diabetes duration, higher HbA1c
(glycated haemoglobin) and hypertension. The prevalence of thesight-threatening stages typified by PDR (proliferative diabeticretinopathy) and DMO (diabetic macular oedema) was ∼7 % [8].
DMO causes more vision loss than PDR and its effectivetreatment remains a major issue for healthcare authorities. Forexample, it has been shown recently [9] that the number of peoplewith diabetes in England in 2010 was estimated to be 2 342 951of which 2 334 550 were aged >12 years. An estimated 166 325(7.12 %) had DMO in one or both eyes and, of these, 64 725 in-dividuals had clinically significant reductions in visual acuity topoorer than 6/6 in at least one eye [9]. The overall health and so-cial care costs in 2010, on the pathway from screening to rehabilit-ation and care in the home, were estimated to be £116 296 038 [9].
CLASSIFICATION OF DIABETIC RETINOPATHY
Diabetic retinopathy is largely asymptomatic and, by the timeworsening vision is experienced, pathology may be significantlyadvanced. Therefore there is a need for screening to assess thepresence and progression of the condition [10]. Various clas-sifications are used to grade the severity of diabetic retinopathy,although traditionally it is classified into two main clinical forms:NPDR (non-PDR) and PDR. The PDR stage involves the forma-tion of neovascularization that develops from the venous side ofthe retinal circulation and may penetrate the inner limiting mem-brane into the vitreous (Figure 1). Typically these new bloodvessels are fragile and leaky and, if left untreated, can becomeenveloped by fibrous connective tissue. Adhesion often occursbetween this fibrous tissue and the posterior hyaloid and result-ant traction can lead to vitreous haemorrhage and/or tractionalretinal detachment. Proliferative retinopathy occurs in approxim-ately 50 % of patients with Type 1 diabetes and in approximately15 % of patients with Type 2 diabetes who have the disease for25 years [11].
The most commonly used grading system in clinical and epi-demiological studies of diabetic retinopathy is the ETDRS (EarlyTreatment of Diabetic Retinopathy Study) scale [12], which re-lies upon a number of photographically detectable microvascularlesions as indicators of disease progression. Levels of NPDR arecharacterized by the number and severity of microaneurysms, dotand blot haemorrhages, cotton wool spots (nerve fibre layer in-farcts), venous abnormalities (beading and looping) and IRMAs(intraretinal microvascular anomalies), which are large-calibreshunt vessels within non-perfused regions of the capillary bed.PDR involves the formation of new blood vessels and is gradedaccording to the extent and location of new vessels at the opticdisc or elsewhere on the fundus and the presence or absence ofvitreous haemorrhage (Figure 1).
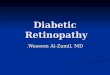
Figure 1 Fundus photographs (A and B) and fluoresceinangiogram (C) of a patient with PDR(A) Fundus photograph of the right eye of a patient with PDR. Neoves-sels in the disc and elsewhere remained active, despite panretinalphotocoagulation. A large pre-retinal haemorrhage (arrow) and markedpre-retinal fibrosis (arrow heads) can be seen. (B) Fundus photographof the right eye of a patient with PDR. Marked neovessels in the discand elsewhere are present. (C) Fundus fluorescein angiography of a pa-tient with PDR. Extensive mid-peripheral retinal ischaemia is present.Neovessels in the disc and elsewhere are seen as intense hyperfluor-escent areas.
When diabetic retinopathy affects the macula and centralvisual acuity is threatened, it is termed diabetic maculopathy.In this area of the retina, excessive vasopermeability and oed-ematous damage is referred to as DMO and is the commonestcause of blindness in diabetes [13]. Although DMO can occur atvirtually any stage of retinopathic development, it is most pre-valent during the later phases of the disease [5]. Diabetic mac-ulopathy is classified as (i) central or non-central, depending onwhether the oedema affects the centre of the fovea, (ii) focal ordiffuse, based on the extension of the area affected by the oed-ema, (iii) ischaemic or non-ischaemic, based on the preservationor involvement of the perifoveal capillary network, or (iv) mixed,when a combination of the above exists (Figure 2). Furthermore,
2 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
Figure 2 Fundus photograph (A) and optical coherence tomo-graphy (B) of a patient with NPDR(A) Fundus photograph of the right eye of a patient with NPDR andcentral involvement clinically significant macular oedema. Marked ex-udation is observed around the foveal centre. (B) Optical coherencetomography (OCT) of a patient with diabetic macular oedema. Exud-ation, demonstrating high intensity signals and shadowing (white ar-rows) and cystoid macular oedema (white arrow head), shown as areasof low-intensity signal, are observed.
diabetic maculopathy has also been classified as tractional ornot tractional depending on whether the presence of vitreoretinaltraction plays a role in its occurrence.
RISK FACTORS FOR DIABETIC RETINOPATHY
Systemic factors and retinopathyIdentifying robust risk factors for diabetic retinopathy is difficult.At present, the best advice for diabetic patients is to maintain theirglycaemic control, as indicated by HbA1c, as close to normal lim-its as possible. This was proven by DCCT (Diabetes Control andComplications Trial) for Type 1 diabetes conducted from 1983to 1993 [14], although the benefits of so-called ‘tight’ glycaemiccontrol took several years to manifest. Similarly for Type 2 dia-betes, UKPDS (UK Prospective Diabetes Study) demonstratedthat maintaining near normoglycaemia can significantly protectagainst the progression of diabetic retinopathy [15].
DCCT revealed that diabetic retinopathy can be offset withimproved glycaemic control if treatment is commenced as soonas possible after diagnosis of Type 1 diabetes. However, previousperiods of poor control are critical, as demonstrated in over 200patients from the original DCCT who were followed for a further10 years under the auspices of the EDIC (Epidemiology of Dia-betes Interventions and Complications) trial [16]. This study re-vealed that the incidence of diabetic retinopathy was significantlyless in the group initially maintained under tight glycaemic con-trol and that these benefits extended beyond the period of intens-
ive insulin therapy [16]. The patients under ‘conventional’ controlfor the first 10 years maintained a so-called ‘hyperglycaemic ormetabolic memory’ and retained a strong association with retino-pathic progression. Interestingly, the same memory phenomenonfor retinopathy was also shown nearly 20 years previously by En-german and Kern [17] in variously (insulin) controlled diabeticdogs.
Hyperglycaemia has been a focus for many studies on dia-betic retinopathy, although it is clear that dyslipidaemia is also animportant risk factor and that regulation of blood lipids shouldbe considered as an effective means to offset progression of thiscomplication. The seminal Hoorn Study identified dyslipidaemiaas a clear additional risk factor for diabetic patients [18]. Thisis also shown by clinical trials such as FIELD (Fenofibrate In-tervention and Event Lowering in Diabetes) [19] and ACCORD(Action to Control Cardiovascular Risk in Diabetes) [20], whichevaluated the role of fenofibrate and simvastatin + fenofibrate re-spectively. These drugs with proven lipidaemic control modes ofaction are effective in ameliorating the progression of diabeticretinopathy, although it should be acknowledged that HMG-CoA(3-hydroxy-3-methylglutaryl-CoA) reductase inhibitors (statins)and fenofibrates may have an impact on a range of pathogenicpathways that are independent of lipids [21,22].
UKPDS served to highlight the importance of BP (blood pres-sure) as well as hyperglycaemia in diabetic retinopathy [15,23].More recent studies, such as the META-EYE (Meta-Analysis forEye Disease) study, have demonstrated a prevalence of diabeticretinopathy among people with normal BP of 5.5 % comparedwith 10.6 % in those with hypertension (BP >140/90mmHg oralready on antihypertensive medication) [8]. It is now establishedthat patients with diabetes should avoid systemic hypertension,which exacerbates initiation and progression of retinopathy [24].
Recent data suggests that controlling systemic modifiable riskfactors could reverse DMO. In the RISE-RIDE trial, for instance,∼18 % of patients in the sham group had visual improvementof 15 letters and ∼30 % of patients in the sham arm never re-ceived ‘rescue’ laser. The RISE and RIDE were parallel Phase IIImulti-centre double-masked sham-injection-controlled random-ized studies that aimed to evaluate the efficacy and safety of in-travitreal ranibizumab in DMO [25]. Patients (n = 759) were ran-domized to receive monthly sham injections or 0.3 mg or 0.5 mgintravitreal injections of ranibizumab. From month 3 onwards,patients were allowed to receive laser if the central foveal thick-ness was >250 μm with <50 μm change from a prior month,provided that macular laser had not been done in the previous 3months and that it was considered by the evaluating physician thatlaser would be beneficial. The primary outcome was the propor-tion of patients gaining >15 ETDRS letter score from baselineat month 24. Only 70–74 % of patients in the sham group re-ceived laser during the study period. As DMO was present in allpatients entering the study and laser treatment was the standardof care at the time the RISE and RIDE studies were initiated, itwould be expected that laser treatment would have been offeredand applied to all patients in the sham group. Although otherreasons may have accounted for the low rate of laser treatmentperformed in the sham arm, including spontaneous resolutionof DMO [26], macular ischaemia (which would be a
www.clinsci.org 3

A. W. Stitt and others
contraindication for macular laser) or end-stage disease, it ispossible that DMO may have improved or resolved in a largeproportion of patients as a result of a tighter metabolic and BPcontrol that could have been achieved as a result of patients beingenrolled in RCTs (randomized control trials) in which monthlycheck ups were being undertaken [25].
Genetic linkage to retinopathy?There have been many assessments of the role of hereditaryfactors in diabetic retinopathy (reviewed by [27]), but as yetthere is no robust indication that this complication has a geneticcomponent. This contrasts with diabetic nephropathy where someimportant associations have been highlighted in recent years [28].Candidate gene studies and GWAS (genome-wide associationstudies) may yet find genetic linkage to particular retinopathyphenotypes and onset of pathology in relation to risk factors.
On the basis of the assumption that interactions between en-vironmental factors and genetic predisposition could provide apowerful risk association to diabetic retinopathy, epigenetics hasrecently had an impact on this field. Studies on the direct and in-direct effects of epigenetics and diabetic retinopathy are a fruit-ful area of investigation, although they add a further layer ofcomplexity to the comparatively static genome. Chromatin al-terations can persist in cells for their entire lifespan, controllingcell function/dysfunction without alteration to the encoding DNAsequence. Such epigenetic changes may play a key role in retino-pathy initiation and progression. Various covalent modificationscan occur in histones such as acetylation, phosphorylation orubiquitination, but methylation via HMT (histone methyltrans-ferase) enzymes at lysine residues is probably most important inthe context of epigenetics [29]. Histone methylation at variouspromoter regions can significantly alter transcriptional regulationat defined promoters and lead to suppression or inappropriatelysustained activation of a gene sequence. With applicability todiabetic retinopathy, it has been shown that exposure of vascu-lar endothelial cells to high glucose, akin to the excursions inglycaemia observed in diabetes, induces significant epigeneticpathology [30]. Endothelial cells exposed to high glucose for16 h followed by a return to normal glucose levels for 6 daysleaves an ‘epigenetic mark’ and these cells displayed a sustainedactivation of NF-κB (nuclear factor κB) at the P65 promoter andoxidative stress responses akin to a memory phenomenon. Suchtranscriptional activation controls a range of oxidative and pro-inflammatory-linked cell responses. This has far-reaching implic-ations and demonstrates that relatively short-term high glucoseexposure induces a harmful chromatin remodelling and epigen-etic changes that could be linked to diabetic complications ingeneral and retinopathy in particular [31–33].
RETINAL VASCULAR, NEURONAL AND GLIALPATHOLOGY IN DIABETES
Pathogenic features of microvascular dysfunctionMost investigations relating to the pathogenesis of diabetic retino-pathy have focused on the vasodegenerative phase of the disease
which leads directly to areas of retinal non-perfusion and hypoxia.This often precipitates breakdown of the BRB (blood–retinal bar-rier), oedema and/or the proliferative phase of the disease. Arange of retinal microvascular abnormalities have been shown indiabetic animals (∼6 months to 4 years of diabetes duration) [34–37], but how closely these relatively short-term changes relate tohuman disease is a matter of debate.
One of the earliest histopathological changes observed indiabetic patients (and diabetic models) is thickening of the ca-pillary BM (basement membrane) [38]. This is thought to bea consequence of increased synthesis of BM components (forexample, collagen IV, fibronectin and laminin) and/or reduceddegradation by catabolic enzymes [34,39–41]. It remains uncer-tain whether BM thickening is of primary or secondary import-ance in the development of diabetic retinopathy, but it has beenspeculated that such matrix modifications may contribute to im-paired endothelial–pericyte communication, defects in capillaryautoregulation or inappropriate cell interaction with constituentBM proteins [42–45]. AGEs (advanced glycation end-products)accumulate in diabetes and these adducts precipitate enhancedcross-linking in vascular BMs with associated enhanced com-ponent gene expression, parallel reductions in BM degradability,abnormal vessel elasticity and vascular cell death [44,46–48].Inhibition of AGE formation during diabetes has been shown toprevent BM thickening in diabetic rats [34,49].
Pericytes and smooth muscle cells are among the first vascularcomponents to die during diabetic retinopathy and this occurs viaan apoptotic death mechanism [50,51]. Endothelial cells are alsodysfunctional at a similar time point, although they may havethe ability to make good the deficit, in the short-term at least.However, with prolonged exposure to the diabetic milieu, it islikely that the replicative potential of the endothelial cells willbe exhausted, as occurs in all somatic cells when their Hayflicklimit is exceeded [52,53]. Indeed, it has been shown that exposureto AGE-modified matrix proteins can induce a senescent phen-otype prematurely so that the normal Hayflick limit may not beattainable under diabetic conditions [54]. Therefore it has beenproposed that the primary defect in diabetic retinopathy lies withthe vascular endothelium and that the complication could be con-sidered to be, at least in part, an ‘endotheliopathy’ [55]. The endo-thelium is critical to normal function of other cells in the capil-lary complex [38]. The precise basis of endothelial, pericyte andsmooth muscle dysfunction in the diabetic retinal microvascu-lature in vivo remains obscure, but is most likely related to anarray of cumulative biochemical insults coupled with impairedability of the cells to repair and renew themselves. Retinal peri-cytes and smooth muscle cells are reliant on key growth/survivalfactors, such as PDGF (platelet-derived growth factor)-B [56,57],and there is selective depletion of this peptide during diabetes[58], which is closely related to acellular capillary formation[59].
Microaneurysms are hallmark lesions of diabetic retinopathy.Ophthalmoscopically, microaneurysms may appear as dark redor white spots in the fundus, whereas fluorescein angiographyreveals perfused microaneurysms as discrete hyperfluorescentspots. Clinically, many microaneurysms are sclerosed and non-perfused, whereas others can be observed as fully or partially
4 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
perfused during fluorescein angiography [60,61]. Clinicopatho-logical studies of diabetic retinopathy in which associations weremade between fluorescein angiograms and trypsin digest prepara-tions have confirmed that regions of capillary acellularity corres-ponded to non-perfused microvasculature angiographically oftendownstream from areas where microaneurysms were abundant[62]. Microaneurysms do not occur in diabetic rodents and there-fore histological studies have been limited, but it is apparent thathypertension, microvascular BM thickening, endothelial prolif-eration, thrombus formation and pericyte cell death have all beenimplicated as causal or contributory factors to formation of mi-croaneurysms [63–67]. Ultrastructurally, one of the earliest fea-tures of microaneurysms in the human diabetic retina is pericyteloss [67,68], and uncontrolled hydrostatic pressure in the capil-lary beds may also result from selective loss of smooth musclecells in the arteries and precapillary arterioles. Our group hasdemonstrated that microaneurysms occur largely on the arteri-olar side of the circulation where they often occur immediatelyupstream of large areas of capillary acellularity [38]. Early-stagemicroaneurysms may also contain large numbers of monocyteand polymorphonuclear cells [67], perhaps reflecting the pro-inflammatory state of diabetes and the role of leucocyte-mediatedcapillary occlusion in diabetic retinopathy [69].
Capillary degeneration is a central tenet of progressiveischaemia during diabetic retinopathy and degenerative vesselsare a universal finding in long-term diabetic animal models andpost-mortem specimens [38]. On trypsin digest preparations,these acellular capillaries appear as non-perfused naked BMtubes where the endothelial cells have disappeared [38]. Increas-ing closure of capillaries may be linked with cotton wool spotsin the neural retina and also the occurrence of IRMAs, whichare represented in trypsin digests by wide-calibre multicellularchannels within the capillary bed [60,62]. Although there havebeen few studies conducted on the nature of IRMAs in the dia-betic retina, it can be observed that these structures contain largenumbers of endothelial-like cells and occur in association withacellular capillaries close to the arterial side of the circulation.IRMAs show large-calibre vessels traversing ischaemic retinawith direct communication between pre-capillary arterioles andpost-capillary venules and probably represent shunt vessels andan attempt to re-vascularize the hypoxic neuropile [60,62].
Retinal neuron and glial dysfunction during diabetesAlthough vascular dysfunction and loss of perfusion remain hall-marks of diabetic retinopathy, a growing body of evidence sug-gests that neuroretinal function is also compromised during thisdisease, perhaps even before overt vessel changes [70]. Elec-trophysiological studies of patients with diabetes suggest alter-ations in the neural retina, including loss of colour vision [71]and contrast sensitivity [72], and abnormalities in the ERG (elec-troretinogram) at diabetes onset [73]. Early neuronal alterationsare also evident in experimental diabetes in rodents, includingperturbation of the retinal histaminergic system leading to in-creased apoptosis of retinal ganglion cells and cholinergic anddopaminergic amacrine cells [74–76]. Apoptotic loss of photore-ceptors has also been reported [77], corresponding to decreases
in the rod and cone components of the ERG after ∼12 weeks ofdiabetes-induction in animals [78].
Glia also show abnormalities during hyperglycaemia; in par-ticular the Muller cells which demonstrate increased expressionof GFAP (glial fibrillary acidic protein) [79] and concomitantsynthesis of glutamate (as a function of disruption of the glutam-ate transporter [80]). This may contribute to excitotoxicity andeventual depletion of retinal neurons as a component part of dia-betic retinopathy [81]. Taken together, the retinopathy literaturesuggests that neurodegeneration could constitute a significantpathophysiological defect in diabetes. It is clear that more re-search is required, especially to understand the complex interplaybetween neurons, glia and vascular components of the retina andkey elements of disease-related dysfunction on this axis. Dia-betic retinopathy may therefore be more accurately conceivedas a disease of the neurovascular unit, resulting in dysfunctionand eventual death of several of the key cells that maintain theBRB, namely pericytes, vascular endothelial cells, Muller gliaand neurons.
KEY PATHOGENIC PATHWAYS IN DIABETICRETINOPATHY
The pathogenesis of diabetic retinopathy is complex and a rangeof independent hypotheses have been proposed to explain the ad-verse effects of hyperglycaemia and dyslipidaemia, including in-creased polyol pathway flux, increased hexosamine pathway flux,increased formation of AGEs and overactivation of PKC (proteinkinase C) [82]. Although detailed discussion of these pathways isbeyond the scope of the present review, it is important to emphas-ize that these mechanisms should not necessarily be regarded asindependent phenomena. Indeed, there is some evidence that theyare linked as a direct result of hyperglycaemia-mediated over-production of superoxide by the mitochondrial-localized elec-tron transport chain [82]. This superoxide partially inhibits theglycolytic enzyme GAPDH (glyceraldehyde phosphate dehydro-genase), thereby diverting upstream metabolites from glycolysisinto the four glucose-driven signalling pathways above. Import-antly, the transketolase activator benfotiamine, which shunts hex-ose metabolism to the pentose pathway, appears to block all themajor pathways of hyperglycaemic damage and effectively pre-vents the microvascular lesions of retinopathy in diabetic animals[83]. Recent clinical studies to determine whether benfotiaminemight be useful in preventing plasma or urinary AGEs, however,have shown no benefit [84]. In addition, long-term (24 month)oral benfotiamine supplementation in Type 1 diabetic patientsshowed no change in peripheral nerve function or soluble inflam-matory biomarkers [85], although the benefits of this drug onclinical diabetic retinopathy have yet to be determined.
Changes in retinal blood flowThe earliest functional changes in NPDR which cannot be visu-alized photographically include alterations in the rate of retinalblood flow and loss of autoregulatory mechanisms for adjust-ing retinal capillary perfusion to local metabolic demand [86].
www.clinsci.org 5

A. W. Stitt and others
The retinal vasculature lacks autonomic innervation and modu-lation of blood flow through the neuropile is dependent on localsignalling mechanisms [87]. As early as the 1930s it was sug-gested that retinal blood flow was markedly altered in diabeticpatients [88]. As technology evolved there were further indic-ations that retinal vessel calibre consistently increased duringdiabetes [89,90]. Since the 1970s it has been recognized thathaemodynamic changes in the retinal vasculature could play arole in pathology and perhaps also provide an early indicator ofdiabetes-related dysfunction in the retina [91,92].
Since then various patient-based studies have shown that ret-inal haemodynamic abnormalities occur before the onset of clin-ical diabetic retinopathy [93] and progression of the disease [94–97]. For example, in diabetic patients without retinopathy, retinalarteriolar vasoconstriction and decreased total retinal blood flowhas been reported [93,98,99]. Decreased retinal blood flow dur-ing early diabetes may reduce O2 and nutrient delivery to theretinal neuropile and thereby contribute to the initial neuroglialabnormalities observed in the diabetic retina.
As the disease progresses, retinal arterioles begin to dilateand bulk retinal blood flow increases in proportion to the severityof retinopathy [100]. Indeed, enhanced blood flow may hastenthe progression of diabetic retinopathy by causing shear-stress-induced endothelial cell damage and death [86], and there hasbeen a recent trial suggesting that these changes could be re-garded as robust risk factors for retinopathy [101]. Significantly,patients with increased retinal blood flow who fail to demon-strate improvement of haemodynamic indices through normal-ization of blood glucose tend to show a more rapid progressionof the disease on follow-up [102]. Ongoing research into whatcauses changes in blood flow during various stages of diabeticretinopathy will be central to devising new ways to regulate thisabnormality. This is critical because, although blood flow changesin diabetes are widely recognized, at present there is little directevidence in the literature that such alterations contribute to patho-logy. Moreover, understanding the basic pathogenic mechanismsof what alters retinal blood flow will help link chronic hyper-glycaemia to retinal vasoconstriction and flow changes prior tothe onset of overt diabetic retinopathy.
Inflammation and diabetic retinopathyOver recent years there has been considerable focus on the roleof inflammation in diabetic retinopathy [103]. The aberrant ex-pression of pro-inflammatory cytokines within the neural retinaand up-regulation of adhesion molecules on the microvasculatureleading to leukostatic responses have been linked to both theneurovascular dysfunction and formation of acellular capillar-ies [104]. Recent evidence suggests that leukocytes may act-ively damage the retinal vascular endothelium [105,106]. GlobalmRNA expression profiling has highlighted altered expression ofpro-inflammatory cytokines and inter-related pathways not onlyin the retinal vessels [107], but also in the neuroglia [108]. There isundoubtedly a complex milieu of dysregulated pro-inflammatoryfactors evident in diabetic retina such as IL (interleukin)-1α, IL-1β, IL-6 and TNFα (tumour necrosis factor α) [103].
Although microglia and infiltrating monocytes are recognizedas central to inflammatory CNS (central nervous system) patho-
logy, the role of these cells in diabetic retinopathy is considerablyless well understood. A number of in vitro studies and in vivoinvestigations of animal models and human post-mortem speci-mens indicate that activation of retinal microglia could play animportant regulatory role in diabetes-mediated retinal inflamma-tion [109] by modulating cytokine expression [110] and otherpathologic responses [111]. Monocytes that infiltrate the retinaand are distinct from microglia have not been adequately studiedin diabetic retinopathy even though they reside in proximity toblood vessels (perivascular macrophages) or within various layersof the neuropile [112]. Monocytes and microglia have importantroles in retinal homoeostasis, but they are also central to neuro-inflammation and these have been shown to increase in diabetes,in both humans and animal models [113–115].
Our group has studied the role of RAGE (receptor for AGEs)in the context of diabetic retinopathy and inflammation. RAGEis a component of the innate immune system and is a signallingreceptor for various ligands, including AGEs, S100B, HMGB-1 (high-mobility group box-1), amyloid-β and Mac-1 [116].Ligand-binding and signal transduction activates transcriptionof NF-κB and induction of adhesion molecules, cytokines and/oroxidative stress. In the retina, RAGE is expressed by many cells,although the highest expression levels are in Muller glia [117].S100B is neurotrophic at low levels [118], although up-regulationoccurs in the Muller glia of diabetic animal models where itcan induce inflammatory cytokine expression [119]. Blockade ofRAGE may be a useful therapeutic strategy. For example, it hasbeen shown that the soluble RAGE fragment (known as sRAGE)can prevent Muller cell dysfunction [117] during diabetes andretinal capillary leukostasis in AGE-infused (non-diabetic) mice[120]. Importantly, RAGE antagonists can prevent acellular capil-lary formation in diabetic mice [121], underscoring the potentialfor this receptor as a target for preventing inflammatory pathologyin diabetic retinopathy.
VEGF (vascular endothelial growth factor) anddiabetic retinopathyVascular permeability in the retina is controlled by the innerBRB, formed by the intra-retinal microvasculature and the outerBRB formed by the RPE (retinal pigment epithelium). The RPEacts as barrier limiting the passage of solutes and fluids betweenthe choroidal stroma and the outer retina, while the retinal vas-culature directly regulates flux into and out of the inner retina.The BRB is formed by tight junctions between adjacent cellswhich effectively blocks paracellular vascular permeability (i.e.the transport of substances between cells). Several tight junctionproteins, including transmembrane proteins, such as occludin andthe claudin family, and the membrane-associated protein zonulaoccludens, contribute to the formation of the BRB [122].
In diabetes, the inner BRB is compromised and macromolec-ules leak from the intraretinal vasculature into the interstitialspaces of the surrounding retina. In humans, MRI (magnetic res-onance imaging) assessment of the retina shows an early stagepermeability that occurs in advance of clinically recognizablediabetic retinopathy [123,124]. In animal models, increased ret-inal vascular permeability occurs shortly after diabetes onset,with a >60 % increase in permeability to fluorescein-conjugated
6 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
albumin after only 4 weeks of diabetes [122]. It has also beenrecognized that the outer BRB is dysfunctional in diabetic retino-pathy and it seems likely that leakage from the choriocapillaristhrough the RPE [125], perhaps in unison with impaired fluidclearance by this layer, may also contribute to oedematous changein the retina as diabetes progresses [126]. Fluid normally movesfrom the retina to the choroid largely due to the osmotic pres-sure exerted by the proteins in the choroidal stroma. In diabetes,breakdown of the outer BRB allows protein to leak into the sub-retinal space and thereby reduces the osmotic pressure gradient.Leakage and impaired fluid clearance are therefore most likelyintimately linked to one another. Vascular leakage leads to DMOwith or without cystoid degenerative changes, photoreceptor at-rophy and an irreversible loss of central vision, although it isunclear whether this is related to a persistent vascular leakage orrather an acute wholesale breakdown of the BRB. It has also beensuggested that Muller cell swelling could contribute significantlyto oedematous changes in the diabetic retina [127].
CURRENT TREATMENTS OPTIONS FORDIABETIC RETINOPATHY
At present there are few measures available to prevent diabeticretinopathy beyond maintenance of tight glycaemic control [14],cessation of smoking [128], BP control [86] and correction of dys-lipidaemia [129]. Beyond control of systemic factors, laser photo-coagulation, intravitreal anti-VEGF drugs and intravitrealcorticosteroids are the principal therapies to reduce sight-threatening DMO. Laser photocoagulation and vitreoretinal sur-gery are the main treatments for PDR.
Treatments for DMOMacular laser photocoagulationETDRS demonstrated the value of laser photocoagulation in thetreatment of clinically significant diabetic macular oedema [12].Although laser reduced the risk of moderate visual loss by 50 %,after 3 years of follow-up <3 % of patients had visual acuity im-provement by >15 letters. In ETDRS, although the diagnosis ofCSMO (clinically significant macular oedema) was made basedon clinical examination, laser treatment was guided by fluoresceinangiography. Hence, traditionally, laser was applied with a viewto preventing or slowing visual acuity deterioration rather than anattempt to restore vision. More recent data from RCTs suggeststhat laser treatment can actually improve vision in a relativelyhigh percentage of patients. Thus, in the DRCR.net (DiabeticRetinopathy Clinical Research network) study comparing triam-cinolone with laser in patients with DMO, an improvement of>10 letters was achieved in 32 % of patients at 2 years in thelaser group; the probability of improvement was similar in naıveeyes and in those that had received >3 bouts of laser therapy[130]. Interestingly, FFA (fundus fluorescein angiography) wasnot undertaken to guide laser treatment. Very similar results wereobtained in a more recent study also conducted by the DRCR.netstudy and which compared ranibizumab combined with promptor deferred laser with prompt laser alone and with prompt laser
combined with triamcinolone in patients with centre-involvedDMO [131]. In this study, a visual acuity improvement of >10letters was achieved in 35 % of patients at 2 years in the laserarm. The above data suggests that laser treatment can success-fully improve vision in a proportion of patients with DMO.
Anti-VEGF therapiesBRB compromise and overt DMO during diabetic retinopathyhas been closely linked to VEGF overexpression within the ret-ina. This peptide is elevated in the ocular fluid of diabetic patients[132] and in the retina of diabetic animals before the appear-ance of observable retinopathy [133]. Laser photocoagulation re-duces retinal VEGF [134] and is an effective treatment [130,135].Furthermore, recently conducted RCTs have demonstrated thatanti-VEGF drugs can reduce/eliminate DMO and improve vision[25,131,136,137]. It should be noted, however, that in most RCTsonly around 50 % of patients experienced clinically meaningfulimprovements in vision and in a similar number retinal thicknessreturns to normal levels [131,136]. Interestingly, not all patientswith DMO respond to VEGF blockade and it is worth noting thata recent pharmacogenetics study in AMD (age-related maculardegeneration) patients suggested that variation in nucleotide poly-morphisms [tSNPs (tagging single nucleotide polymorphisms)]in the VEGFA gene were associated with responsiveness to anti-VEGF therapy [138]. It remains unknown whether this also ap-plies to patients with DMO.
Several RCTs have demonstrated the clinical efficacy of in-travitreal anti-VEGF treatment in DMO. The DRCR.net study(n = 854 eyes; n = 691 patients) [131] showed superiority inthe primary outcome [mean change in BCVA (best correctvisual acuity) at 1 year] in patients treated with ranibizumaband prompt (3–10 days after ranibizumab treatment) or de-ferred (�24 weeks following ranibizumab) laser compared withthose treated with prompt laser + sham injection or promptlaser + triamcinolone injection. In this study, the percentage ofpatients receiving at least one session of focal/grid laser treat-ment in the ranibizumab + deferred laser group increased from28 % in the first year to 42 % in the second year (extension ofthe trial) [131], indicating that laser treatment was still requiredto control patients longer term. The READ-2 (Ranibizumab forEdema of the mAcula in Diabetes) (n = 126 patients; primary out-come, mean change in BCVA at 6 months) [139] and RESTORE(n = 354 patients; primary outcome, mean average change inBCVA from baseline to months 1–12) [136] randomized pa-tients to ranibizumab alone, ranibizumab + laser or laser aloneand found greater visual acuity improvement in patients in theranibizumab groups. The RESOLVE (n = 151 patients; primaryoutcome, mean average change in BCVA from baseline to months1–12) [140] and RISE-RIDE (n = 377 and n = 382 for RISE andRIDE respectively; primary outcome, proportion of patients with�15 letters at month 24) [139] randomized patients to ranibizu-mab or sham and, similarly, found better visual acuity outcomes inpatients treated with the former. Rescue laser was allowed in thesetrials in ranibizumab and sham groups and was used in ∼35 %and ∼5 % of patients in sham and ranibizumab groups in RE-SOLVE and in 70–74 % and 20–40 % of patients in sham andranibizumab groups in RISE-RIDE. It is important to note that in
www.clinsci.org 7

A. W. Stitt and others
all of the above studies with one exception (RESOLVE), at best,only ∼50 % of patients treated with ranibizumab responded tothis treatment with an improvement of �10 letters.
An RCT, BOLT (Bevacizumab Or Laser Therapy) (n = 80patients; main outcome, difference between groups on BCVAat 1 year) [141] compared bevacizumab with laser photocoagu-lation in the treatment of patients with DMO and also foundgreater BCVA improvements in patients receiving bevacizumab.A further larger study, but with short follow-up, DA VINCI(n = 221 patients; main outcome, mean change in BCVA at 6months) [142] compared macular laser photocoagulation withfour regimes of a fusion protein (‘VEGF-trap’) (0.5 mg or 2 mgevery 4 weeks, 2 mg every 4 weeks for 3 months and then every8 weeks, 2 mg every 4 weeks for 3 months and then as needed)and found all VEGF-trap arms superior to laser.
Steroid treatmentTriamcinolone, dexamethasone and fluocinolone have been usedin the treatment of patients with DMO. Several RCTs have com-pared triamcinolone with laser photocoagulation and laser hasbeen shown to be superior. DRCR.net, however, found that,in pseudophakic eyes, visual acuity improvement in thetriamcinolone + prompt laser group appeared comparable withthat in ranibizumab groups (also see the section on anti-VEGFtherapies above) [131]. Triamcinolone + prompt laser appearedalso more cost-effective than ranibizumab + prompt or deferredlaser for pseudophakic patients [143].
Intravitreal DXM (dexamethasone), at a dose of 700 μg, usingan intravitreal drug delivery system was found to be superiorto no treatment short-term in an RCT that randomized patientsto 350 μg, 700 μg or no treatment (n = 171 patients; primaryoutcome, proportion of eyes that achieved an improvement inBCVA of �10 letters or more from baseline at day 90) [144].
The FAME (Fluocinolone Acetonide in Diabetic Macular Ed-ema) trial compared fluocinolone (0.2 μg/day or 0.5 μg/day) withsham treatment (n = 956; main outcome, percentage of patientswith �15 letter improvement at 2 years) [145] in patients withDMO. Rescue laser was allowed in all groups. Fluocinolone wasfound to be superior to sham, but side effects including cataract,increased intraocular pressure and glaucoma, occurred as a resultof the treatment with fluocinolone. Rescue laser was performedin ∼37 % and 59 % of fluocinolone-treated and sham-treated eyesrespectively.
Treatments for PDRIn contrast with DMO, treatment advancements in the manage-ment of PDR have been more restricted. PRP (panretinal photo-coagulation) remains the mainstay treatment for PDR, althoughvitreoretinal surgery is used now in earlier stages (rather thanas a treatment of last resort). Indeed, recent data supports bet-ter visual and anatomical outcomes and decreased complicationsof vitrectomy in patients with diabetic retinopathy (DMO/PDR)compared with earlier data published by DRVS (Diabetic Ret-inopathy Vitrectomy Study) [146]. RCTs have suggested less ret-inopathy progression in patients receiving intravitreal anti-VEGFor triamcinolone with prompt/deferred macular laser [131], in-travitreal anti-VEGF alone [25,140], or oral fenofibrate [147]
and, thus, these treatments may reduce the number of patientsreaching the proliferative stage. Further management options forestablished PDR are, nonetheless, very much needed.
SHORTCOMINGS OF CURRENT THERAPYAND POTENTIAL NEW AVENUES
The approaches described above are focused on end-stage diseaseand carry significant sight-threatening side effects. Importantly,they do not address the early and potentially reversible failure ofretinal perfusion [148]. The use of VEGF-neutralizing antibod-ies, crossing over from success in treating wet AMD, has shownsignificant benefit, although the effects are short-lived and requiremultiple intravitreal injections [131,136,149]. Although hopeful,inhibition of VEGF bioactivity is end-stage and is not withoutdrawbacks. For example, there have been concerns raised thatsuch therapy could compromise retinal neuroglial and residentmicrovascular survival [150–154]. In addition, there have beenclinical reports that some patients with diabetic retinopathy mayrespond poorly to VEGF inhibition and it could even be associ-ated with poor visual outcomes [155,156]. Although anti-VEGFtherapy has revolutionized ophthalmic care, there is a need forcaution surrounding long-term use of these approaches [157]. Inthe context of diabetic retinopathy, this is an increasing concern.For this reason, the development of therapies capable of prevent-ing or slowing the onset and progression of diabetic retinopathyremain a priority.
It is clear that many other pathogenic mechanisms besidesVEGF are involved and play an important role in diabetic ret-inopathy, including PDR and DMO. A multitude of new ap-proaches based on retinal glial, neuronal and vascular patho-physiology during diabetes are being developed. However, manytherapeutic strategies are simply attempting more convenient orbetter-tolerated ways of having an impact on the VEGF pathway.Consequently therapeutics targeted at non-VEGF mechanismsare perhaps the more interesting and offer the greatest hope fora wider treatment response in DMO patients or additional thera-peutic benefit in an adjunctive treatment setting with anti-VEGFs(see below).
Therapeutics with proven efficacy in other diseases may proveuseful in diabetic retinopathy. One such cellular mechanism ofsignificant interest in diabetes is oxidative stress. Nrf2 (nuclearfactor erythroid 2-related factor 2) is a transcription factor thatplays key roles in controlling the expression of antioxidant anddetoxification genes, and mice deficient in Nrf2 are more vulner-able to oxidative damage especially in tissues with high oxygenconsumption, such as the retina. Nrf2 has been reported to be as-sociated with the altered inflammatory status present in chronicobstructive airway disease [158–161] and, indeed, bardoloxone(Reata), an Nrf-2 activator which progressed to a significant stageof development, but was later terminated, was shown to improveglomerular filtration in type 3b-4 chronic kidney disease asso-ciated with Type 2 diabetes in Phase II clinical studies [162].An additional approach which is currently being targeted at thetreatment of diabetic retinopathy is NOX-2 inhibitors (part of the
8 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
NADPH oxidase system), whose major function is to generateROS (reactive oxygen species) as part of the respiratory burst.In spite of the fact that nephritic vasculopathy is the targeted in-dication, there is significant pre-clinical evidence to support theutility of these molecules in the treatment of diabetic retinopathy.ROS formation is correlated with diabetes-induced retinal vas-cular injury and overexpression of VEGF [163] and can lead toactivation of the polyol pathway, AGE formation, RAGE induc-tion and activation of the PKC and hexosamine pathways [31].Up-regulation of NADPH oxidase activity or ROS productionalso correlates with increases in VEGF in rat models of Type 2diabetes [164–166]. Inhibiting NADPH oxidase activity can limitretinal leukostasis [167] and reduced BRB integrity secondary tohyperglycaemia [168]. These approaches may have an ability tohave an impact on diabetic retinopathy at all stages. There is alsoa considerable body of emerging evidence that local inflamma-tion has a significant impact on disease and a myriad of cytokines,including TNFα, have been implicated in PDR and DMO. How-ever, small experimental medicine studies using intravitreal neut-ralizing anti-TNFα antibodies have shown little benefit in DMOpatients refractory to anti-VEGF therapy.
Other therapeutics may arise from novel non-biased genomicand proteomic screens in the context of diabetic retinopathy. Onesuch example focuses on the involvement of extracellular CA(carbonic anhydrase), which is up to 15-fold higher in the vit-reous of individuals with PDR compared with that in vitreousof non-diabetic individuals [169]. Intravitreal injection of CA-Istimulated an increase in retinal vascular permeability to a sim-ilar magnitude to that shown for VEGF. CA-I increases retinalvascular permeability by elevating the vitreal pH, leading to ac-tivation of the PKK (prekallikrein/kinin) pathway, and this hasopened up therapeutic opportunities for inhibitors or antagonistsof the kallikrein system which could be useful as an adjunct tolaser photocoagulation or anti-VEGF agents. Indeed, in a pilotstudy, the CA-1 inhibitor acetazolamide has been shown to im-prove visual outcomes in patients with DMO [170]. Inhibitorsof PKK are being developed which will be initially targeted atintravitreal use, but could probably be developed further as oralmedications if initial studies show promising results.
THE DIFFICULTY OF EXPLORING NEWAVENUES
Despite the possibility of significant drawbacks associated withlong-term intravitreal anti-VEGF use in diabetic retinopathy,these agents now represent the effective standard of care forregulatory authorities. Consequently, when considering a newtherapeutic strategy for diabetic retinopathy, it is important tounderstand whether the targeted mechanism is likely to be in-dependent of VEGF, or simply work via a mechanism whichultimately suppresses VEGF. If the action of the therapeutic is tosimply have an impact on the VEGF pathway or VEGF levels,then it is unlikely that this treatment, however dosed, will be su-perior to intravitreal anti-VEGF therapies in responsive patients.This situation will significantly have an impact on the likeli-
hood of successful development since reduction of treatmentburden is often not an acceptable regulatory endpoint in someregions. Consequently, the new therapeutic has to demonstratenon-inferiority to intravitreal anti-VEGF therapy or increased ef-ficacy in an adjunctive treatment setting. The situation is easierwhen the targeted therapeutic is clearly independent of VEGFsince all marketed anti-VEGF therapeutics show similar effic-acy, suggesting that additional suppression of this pathway isincapable of translating into greater efficacy and only additionalindependent mechanisms can probably deliver improved efficacy.An example of this situation has been demonstrated with PKKinhibitors. Vitreal samples from DMO patients were observed tohave high PKK or high VEGF levels or a combination of both. In-terestingly, human vitreous with either high PKK or high VEGFwere both able to increase retinal vascular permeability wheninjected into mouse eyes and such effects were inhibited by bra-dykinin antagonists or anti-VEGF antibodies respectively. Whenthe opposite experiment was performed attempting to block PKKsamples with anti-VEGF antibodies and VEGF samples withbradykinin antagonists, there was no impact on the ability ofthe human vitreal samples to stimulate retinal vascular permeab-ility in the mouse [171]. This was a clear demonstration of aVEGF-independent pathway and may explain why a significantproportion of DMO patients do not respond adequately to anti-VEGF therapeutics and require additional treatment strategies tobe conceived.
REGENERATIVE MEDICINE AND DIABETICRETINOPATHY
Our own group and others have recently focused on the possibilitythat vascular regeneration could be beneficial for diabetic retino-pathy. Indeed, if the ischaemia that drives DMO and PDR canbe contained or reversed, then this could become an exciting andviable therapeutic option. Such an approach is commonplace inother non-retinal systems where the growth of new blood vesselscan be stimulated to promote regeneration in ischaemic tissues[172]. Reparative angiogenesis in the retina is also a realisticoption. Most of these studies have used OIR (oxygen-inducedretinopathy) [173] in neonatal mice as a model system for regulat-ing intra- and pre-retinal neovascularization. Our laboratory hasused several approaches to achieve effective re-vascularizationof the ischaemic retina, including treatment with an agonist pep-tide that promotes vascular endothelial cell substrate attachment[174–176], genetic knockout or pharmacological inhibition ofTNFα [177], treatment with low-dose simvastatin [178] or use ofa human cell-derived recombinant EPO (erythropoietin) [179].The Smith laboratory has also demonstrated that early-stage de-livery of recombinant EPO to the OIR model can prevent vascularand neural degeneration and hypoxia-induced neovascularization[180]. With respect to EPO, we have also recently shown that anEPO-receptor analogue can effectively regenerate defunct acel-lular capillaries in the diabetic retina with a suggestion that thiscould be linked to increased mobilization and incorporation ofvascular progenitor cells [181].
www.clinsci.org 9

A. W. Stitt and others
Figure 3 Schematic diagram highlighting the complex pathogenesis of diabetic retinopathy and a range of points thatmay be addressed by novel therapeutic interventionACE, angiotensin-converting enzyme; Ang, angiotensin; DME, DMO; PEDF, pigment epithelium-derived factor.
Possibilities for cell therapyEPCs (endothelial progenitor cells) are circulating bone-marrow-derived cells with the ability to differentiate into mature func-tional endothelial cells and repair vessel integrity [182]. This isparticularly relevant for diabetic retinopathy which is associatedwith an accelerated loss of endothelial cells and capillary occlu-sion. Although there is no consensus as to a definite vasoreparat-ive or antigenic phenotype for EPCs, it is generally accepted thatthese cells are capable of differentiating into endothelial cellsand integrating into vascular structures [183]. EPCs normallyonly constitute 0.01 % of circulating cells, but, in response togrowth factors and cytokine gradients secreted from sites of in-jury, inflammation or ischaemia, they are recruited to damagedvasculature [183–185].
Diabetes alters EPC number and function and poor glycaemiccontrol is associated with lower circulating levels of EPCs[186,187], and cells isolated from diabetic donors show signi-ficantly impaired vasoreparative potential [188] and are suscept-ible to premature senescence [189]. Such EPC dysfunction hasbeen reported in patients with Type 1 diabetes [190] and alsoType 2 diabetes [191]. The depressed EPC function is negativelyassociated with severity of vascular complications. Indeed, EPCdysfunction has been implicated in a range of cardiovascular dis-orders, including coronary artery disease, myocardial infarctionand microvasculopathies [192].
In contrast with many other vascular beds, EPC therapy forthe retina has received comparatively less attention. Beginningwith the first report that adult HSCs (haematopoietic stem cells)
10 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
contribute significantly to neovascularization in the ischaemicretina [193], other reports have demonstrated that intravitreal de-livery of EPCs (and related cells) can repair the ischaemic retina[194–198]. These studies show the potential of EPC therapy forischaemic retinopathies, but they also highlight the need for amore thorough characterization of EPC subsets so that the pre-cise fate and utility of delivered cells can be determined withoutthe potential to evoke unwanted responses. This is especiallyimportant in the context of a complex milieu, such as diabetes,which is known to alter EPC phenotype [199]. Nevertheless,when the molecular nature and precise function of EPCs is fullyresearched, vascular cell therapy has potential to translate to theclinical realm and patients with diabetic retinopathy could benefitfrom the remarkable regenerative potential of these cells.
The differentiation potential of MSCs (mesenchymal stemcells) and multipotent adult progenitor cells into mural cells suchas smooth muscle and pericytes has been reported [200,201].Pericytes are crucial for capillary integrity, so if EPC therapy isever to be used for diabetic patients it will be essential to alsoachieve adequate pericyte coverage on intra-retinal vessels. It hasbeen reported that human pluripotent stem cells differentiate tomesodermal precursors that can be expanded to produce cellswith a pericyte phenotype expressing CD146/NG2/PDGFR-β(PDGF-receptor-β) [202]. Implantation of these cells into a mur-ine model of ischaemic limb injury induces vascular regeneration[202]. It has also been shown that human saphenous-vein-derivedpericyte precursors have prolonged therapeutic benefit in a modelof myocardial infarction [203]. This is an interesting and import-ant area for diabetic retinopathy research, since pericyte death isa hallmark lesion of this condition. The ability to regenerate thesecells in the early stages of disease would be a signal advance andthis is being actively pursued by our group.
SUMMARY
Diabetic retinopathy is a multifactorial condition arising fromthe complex interplay between biochemical and metabolic ab-normalities occurring in all cells of the retina. Identification ofa precise pathogenesis that links the progressive neuroglial andmicrovascular damage occurring in the diabetic retina remainsa valid but somewhat elusive goal. Nevertheless, over the com-ing years continued progress is anticipated in our understandingof the molecular and cellular basis of diabetic retinopathy. Weare also entering a new exciting era in which the first pharma-cological treatments based on an understanding of the causativemechanisms of diabetic retinopathy may soon become available(Figure 3). These will include vascular and neuroprotection ther-apies that can halt the progression of retinopathy in the earlystages. There are also exciting possibilities of harnessing repar-ative cells and thereby regenerating retina after retinopathy hasalready become established. In view of the complexity of diabeticretinopathy, it seems likely that combinatory therapy will be re-quired with pathways targeted in different cell types at differentstages of the disease process. With genome-wide assessments
for patients becoming a possibility, the likelihood is that highlytailored pharmacogenetic approaches will be most efficacious.
FUNDING
Our own work was supported by Fight for Sight (UK), the Sir Ju-les Thorn Trust, Medical Research Council, European Union (FP-7),British Heart Foundation, Biotechnology and Biological SciencesResearch Council, Royal Society and Juvenile Diabetes ResearchFoundation.
REFERENCES
1 Rathmann, W. and Giani, G. (2004) Global prevalence ofdiabetes: estimates for the year 2000 and projections for2030. Diabetes Care 27, 2568–2569
2 Derakhshan, R., Arababadi, M. K., Ahmadi, Z., Karimabad, M.N., Salehabadi, V. A., Abedinzadeh, M., Khorramdelazad, H.,Balaei, P., Kennedy, D. and Hassanshahi, G. (2012) Increasedcirculating levels of SDF-1 (CXCL12) in type 2 diabetic patientsare correlated to disease state but are unrelated topolymorphism of the SDF-1beta gene in the Iranian population.Inflammation 35, 900–904
3 Lam, D. W. and LeRoith, D. (2012) The worldwide diabetesepidemic. Curr. Opin. Endocrinol. Diabetes Obes. 19, 93–96
4 Holman, N., Forouhi, N. G., Goyder, E. and Wild, S. H. (2011)The Association of Public Health Observatories (APHO) DiabetesPrevalence Model: estimates of total diabetes prevalence forEngland, 2010–2030. Diabetic Med. 28, 575–582
5 Klein, R., Klein, B. E. and Moss, S. E. (1989) The Wisconsinepidemiological study of diabetic retinopathy: a review.Diabetes Metab. Rev. 5, 559–570
6 Romero-Aroca, P., Sagarra-Alamo, R., Basora-Gallisa, J.,Basora-Gallisa, T., Baget-Bernaldiz, M. and Bautista-Perez, A.(2010) Prospective comparison of two methods of screening fordiabetic retinopathy by nonmydriatic fundus camera. Clin.Ophthalmol. 4, 1481–1488
7 Resnikoff, S., Pascolini, D., Etya’ale, D., Kocur, I.,Pararajasegaram, R., Pokharel, G. P. and Mariotti, S. P. (2004)Global data on visual impairment in the year 2002. Bull.WorldHealth Organ. 82, 844–851
8 Yau, J. W., Rogers, S. L., Kawasaki, R., Lamoureux, E. L.,Kowalski, J. W., Bek, T., Chen, S. J., Dekker, J. M., Fletcher, A.,Grauslund, J. et al. (2012) Global prevalence and major riskfactors of diabetic retinopathy. Diabetes Care 35, 556–564
9 Minassian, D. C., Owens, D. R. and Reidy, A. (2012) Prevalenceof diabetic macular oedema and related health and social careresource use in England. Br. J. Ophthalmol. 96, 345–349
10 Jones, S. and Edwards, R. T. (2010) Diabetic retinopathyscreening: a systematic review of the economic evidence.Diabetic Med. 27, 249–256
11 Klein, R., Klein, B. E., Moss, S. E., Davis, M. D. and DeMets, D.L. (1984) The Wisconsin epidemiologic study of diabeticretinopathy. II. Prevalence and risk of diabetic retinopathy whenage at diagnosis is less than 30 years. Arch. Ophthalmol. 102,520–526
12 Early Treatment Diabetic Retinopathy Study Research Group(1991) Early photocoagulation for diabetic retinopathy. ETDRSreport number 9. Ophthalmology 98, 766–785
13 Joussen, A. M., Smyth, N. and Niessen, C. (2007)Pathophysiology of diabetic macular edema. Dev.Ophthalmol.39, 1–12
www.clinsci.org 11

A. W. Stitt and others
14 Diabetes Control and Complications Trial Research Group(1993) The effect of intensive treatment of diabetes on thedevelopment and progression of long-term complications ininsulin-dependent diabetes mellitus. N. Engl. J. Med. 329,977–986
15 UK Prospective Diabetes Study Group (1998) Effect of intensiveblood-glucose control with metformin on complications inoverweight patients with type 2 diabetes (UKPDS 34). Lancet352, 854–865
16 The Writing Team for the Diabetes Control and ComplicationsTrial/Epidemiology of Diabetes Interventions and ComplicationsResearch Group (2003) Sustained effect of intensive treatmentof type 1 diabetes mellitus on development and progression ofdiabetic nephropathy: the Epidemiology of DiabetesInterventions and Complications (EDIC) study. JAMA, J. Am.Med. Assoc. 290, 2159–2167
17 Engerman, R. L. and Kern, T. S. (1987) Progression of incipientdiabetic retinopathy during good glycemic control. Diabetes 36,808–812
18 van Leiden, H. A., Dekker, J. M., Moll, A. C., Nijpels, G., Heine,R. J., Bouter, L. M., Stehouwer, C. D. and Polak, B. C. (2002)Blood pressure, lipids, and obesity are associated withretinopathy: the hoorn study. Diabetes Care 25, 1320–1325
19 Keech, A., Simes, R. J., Barter, P., Best, J., Scott, R., Taskinen,M. R., Forder, P., Pillai, A., Davis, T., Glasziou, P. et al. (2005)Effects of long-term fenofibrate therapy on cardiovascularevents in 9795 people with type 2 diabetes mellitus (the FIELDstudy): randomised controlled trial. Lancet 366, 1849–1861
20 Ismail-Beigi, F., Craven, T., Banerji, M. A., Basile, J., Calles, J.,Cohen, R. M., Cuddihy, R., Cushman, W. C., Genuth, S., Grimm,R. H. et al. (2010) Effect of intensive treatment ofhyperglycaemia on microvascular outcomes in type 2 diabetes:an analysis of the ACCORD randomised trial. Lancet 376,419–430
21 Sen, K., Misra, A., Kumar, A. and Pandey, R. M. (2002)Simvastatin retards progression of retinopathy in diabeticpatients with hypercholesterolemia. Diabetes Res. Clin. Pract.56, 1–11
22 Wong, T. Y., Simo, R. and Mitchell, P. (2012) Fenofibrate: apotential systemic treatment for diabetic retinopathy? Am. J.Ophthalmol 154, 6–12
23 UK Prospective Diabetes Study Group (1998) Tight bloodpressure control and risk of macrovascular and microvascularcomplications in type 2 diabetes: UKPDS 38. Br. Med. J. 317,703–713
24 Chaturvedi, N., Sjolie, A. K., Stephenson, J. M., Abrahamian,H., Keipes, M., Castellarin, A., Rogulja-Pepeonik, Z. and Fuller,J. H. (1998) Effect of lisinopril on progression of retinopathy innormotensive people with type 1 diabetes. EURODIABControlled Trial of Lisinopril in Insulin-Dependent DiabetesMellitus. Lancet 351, 28–31
25 Nguyen, Q. D., Brown, D. M., Marcus, D. M., Boyer, D. S., Patel,S., Feiner, L., Gibson, A., Sy, J., Rundle, A. C., Hopkins, J. J.et al. (2012) Ranibizumab for diabetic macular edema: resultsfrom 2 phase III randomized trials: RISE and RIDE.Ophthalmology 119, 789–801
26 Romero-Aroca, P. (2010) Targeting the pathophysiology ofdiabetic macular edema. Diabetes Care 33, 2484–2485
27 Schwartz, J. A., Lantis, II, J. C., Gendics, C., Fuller, A. M.,Payne, W. and Ochs, D. (2012) A prospective, non comparative,multicenter study to investigate the effect of cadexomer iodineon bioburden load and other wound characteristics in diabeticfoot ulcers. Int. Wound J., doi: 10.1111/j.1742-481X.2012.01109.x
28 Doria, A. (2010) Genetics of diabetes complications. Curr.Diab. Rep. 10, 467–475
29 Cooper, M. E. and El-Osta, A. (2010) Epigenetics: mechanismsand implications for diabetic complications. Circ. Res. 107,1403–1413
30 El-Osta, A., Brasacchio, D., Yao, D., Pocai, A., Jones, P. L.,Roeder, R. G., Cooper, M. E. and Brownlee, M. (2008) Transienthigh glucose causes persistent epigenetic changes and alteredgene expression during subsequent normoglycemia. J. Exp.Med. 205, 2409–2417
31 Giacco, F. and Brownlee, M. (2010) Oxidative stress anddiabetic complications. Circ. Res. 107, 1058–1070
32 Villeneuve, L. M. and Natarajan, R. (2010) The role ofepigenetics in the pathology of diabetic complications. Am. J.Physiol. Renal Physiol. 299, F14–F25
33 Kadiyala, C. S., Zheng, L., Du, Y., Yohannes, E., Kao, H. Y.,Miyagi, M. and Kern, T. S. (2012) Acetylation of retinal histonesin diabetes increases inflammatory proteins: effects ofminocycline and manipulation of histone acetyltransferase(HAT) and histone deacetylase (HDAC). J. Biol. Chem. 287,25869–25880
34 Stitt, A., Gardiner, T. A., Alderson, N. L., Canning, P., Frizzell, N.,Duffy, N., Boyle, C., Januszewski, A. S., Chachich, M., Baynes,J. W. and Thorpe, S. R. (2002) The AGE inhibitor pyridoxamineinhibits development of retinopathy in experimental diabetes.Diabetes 51, 2826–2832
35 Kern, T. S. and Engerman, R. L. (1995) Vascular lesions indiabetes are distributed non-uniformly within the retina. Exp.Eye Res. 60, 545–549
36 Kern, T. S. and Engerman, R. L. (1996) A mouse model ofdiabetic retinopathy. Arch. Ophthalmol. 114, 986–990
37 Engerman, R. L. and Kern, T. S. (1995) Retinopathy in animalmodels of diabetes. Diabetes Metab. Rev. 11, 109–120
38 Gardiner, T. A., Archer, D. B., Curtis, T. M. and Stitt, A. W.(2007) Arteriolar involvement in the microvascular lesions ofdiabetic retinopathy: implications for pathogenesis.Microcirculation 14, 25–38
39 Stitt, A. W., Anderson, H. R., Gardiner, T. A. and Archer, D. B.(1994) Diabetic retinopathy: quantitative variation in capillarybasement membrane thickening in arterial or venousenvironments. Br. J. Ophthalmol. 78, 133–137
40 Ljubimov, A. V., Burgeson, R. E., Butkowski, R. J., Couchman, J.R., Zardi, L., Ninomiya, Y., Sado, Y., Huang, Z. S., Nesburn, A.B. and Kenney, M. C. (1996) Basement membraneabnormalities in human eyes with diabetic retinopathy. J.Histochem. Cytochem. 44, 1469–1479
41 Roy, S., Maiello, M. and Lorenzi, M. (1994) Increasedexpression of basement membrane collagen in human diabeticretinopathy. J. Clin. Invest. 93, 438–442
42 Beltramo, E., Pomero, F., Allione, A., D’Alu, F., Ponte, E. andPorta, M. (2002) Pericyte adhesion is impaired on extracellularmatrix produced by endothelial cells in high hexoseconcentrations. Diabetologia 45, 416–419
43 Padayatti, P. S., Jiang, C., Glomb, M. A., Uchida, K. and Nagaraj,R. H. (2001) High concentrations of glucose induce synthesisof argpyrimidine in retinal endothelial cells. Curr. Eye Res. 23,106–115
44 Stitt, A. W., Hughes, S. J., Canning, P., Lynch, O., Cox, O.,Frizzell, N., Thorpe, S. R., Cotter, T. G., Curtis, T. M. andGardiner, T. A. (2004) Substrates modified by advancedglycation end-products cause dysfunction and death in retinalpericytes by reducing survival signals mediated byplatelet-derived growth factor. Diabetologia 47, 1735–1746
45 Roy, S., Tonkiss, J. and Roy, S. (2010) Aging increases retinalvascular lesions characteristic of early diabetic retinopathy.Biogerontology 11, 447–455
46 Kalfa, T. A., Gerritsen, M. E., Carlson, E. C., Binstock, A. J. andTsilibary, E. C. (1995) Altered proliferation of retinalmicrovascular cells on glycated matrix. Invest. Ophthalmol.Visual Sci. 36, 2358–2367
47 Boyd-White, J. and Williams, Jr, J. C. (1996) Effect ofcross-linking on matrix permeability. A model for AGE-modifiedbasement membranes. Diabetes 45, 348–353
12 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
48 Mott, J. D., Khalifah, R. G., Nagase, H., Shield, III, C. F.,Hudson, J. K. and Hudson, B. G. (1997) Nonenzymaticglycation of type IV collagen and matrix metalloproteinasesusceptibility. Kidney Int. 52, 1302–1312
49 Gardiner, T. A., Anderson, H. R. and Stitt, A. W. (2003) Inhibitionof advanced glycation end-products protects against retinalcapillary basement membrane expansion during long-termdiabetes. J. Pathol. 201, 328–333
50 Gardiner, T. A., Stitt, A. W., Anderson, H. R. and Archer, D. B.(1994) Selective loss of vascular smooth muscle cells in theretinal microcirculation of diabetic dogs. Br. J. Ophthalmol. 78,54–60
51 Mizutani, M., Kern, T. S. and Lorenzi, M. (1996) Accelerateddeath of retinal microvascular cells in human and experimentaldiabetic retinopathy. J. Clin.Invest. 97, 2883–2890
52 Hayflick, L. (1965) The limited in vitro lifetime of human diploidcell strains. Exp. Cell Res. 37, 614–636
53 Linskens, M. H., Harley, C. B., West, M. D., Campisi, J. andHayflick, L. (1995) Replicative senescence and cell death.Science 267, 17
54 Chen, J., Brodsky, S. V., Goligorsky, D. M., Hampel, D. J., Li, H.,Gross, S. S. and Goligorsky, M. S. (2002) Glycated collagen Iinduces premature senescence-like phenotypic changes inendothelial cells. Circ. Res. 90, 1290–1298
55 Khan, Z. A., Farhangkhoee, H. and Chakrabarti, S. (2006)Towards newer molecular targets for chronic diabeticcomplications. Curr. Vasc. Pharmacol. 4, 45–57
56 Fruttiger, M. (2002) Development of the mouse retinalvasculature: angiogenesis versus vasculogenesis. Invest.Ophthalmol. Visual Sci. 43, 522–527
57 Hoffmann, J., Feng, Y., vom Hagen, F., Hillenbrand, A., Lin, J.,Erber, R., Vajkoczy, P., Gourzoulidou, E., Waldmann, H., Giannis,A. et al. (2005) Endothelial survival factors and spatialcompletion, but not pericyte coverage of retinal capillariesdetermine vessel plasticity. FASEB J. 19, 2035–2036
58 Cox, O., Stitt, A. W., Simpson, D. A. and Gardiner, T. A. (2003)Sources of PDGF expression in murine retina and the effect ofshort-term diabetes. Mol. Vision 10, 665–672
59 Hammes, H. P., Lin, J., Renner, O., Shani, M., Lundqvist, A.,Betsholtz, C., Brownlee, M. and Deutsch, U. (2002) Pericytesand the pathogenesis of diabetic retinopathy. Diabetes 51,3107–3112
60 Kohner, E. M. and Dollery, C. T. (1970) Fluorescein angiographyof the fundus in diabetic retinopathy. Br. Med. Bull. 26,166–170
61 Kohner, E. M. and Henkind, P. (1970) Correlation of fluoresceinangiogram and retinal digest in diabetic retinopathy. Am. J.Ophthalmol. 69, 403–414
62 Bresnick, G. H., Davis, M. D., Myers, F. L. and de Venecia, G.(1977) Clinicopathologic correlations in diabetic retinopathy. II.Clinical and histologic appearances of retinal capillarymicroaneurysms. Arch. Ophthalmol. 95, 1215–1220
63 Amemiya, T. and Bhutto, I. A. (2001) Retinal vascular changesand systemic diseases: corrosion cast demonstration. Ital. J.Anat. Embryol. 106, 237–244
64 Baskin, E., Balkanci, F., Cekirge, S., Sener, C. and Saatci, U.(1999) Renal vascular abnormalities in Bardet-Biedl syndrome.Pediatr. Nephrol. 13, 787–789
65 Ishikawa, K., Uyama, M. and Asayama, K. (1983) Occlusivethromboaortopathy (Takayasu’s disease): cervical arterialstenoses, retinal arterial pressure, retinal microaneurysms andprognosis. Stroke 14, 730–735
66 Tolentino, M. J., Miller, J. W., Gragoudas, E. S., Jakobiec, F. A.,Flynn, E., Chatzistefanou, K., Ferrara, N. and Adamis, A. P.(1996) Intravitreous injections of vascular endothelial growthfactor produce retinal ischemia and microangiopathy in an adultprimate. Ophthalmology 103, 1820–1828
67 Stitt, A. W., Gardiner, T. A. and Archer, D. B. (1995) Histologicaland ultrastructural investigation of retinal microaneurysmdevelopment in diabetic patients. Br. J. Ophthalmol. 79,362–367
68 Yanoff, M. (1966) Diabetic retinopathy. N. Engl. J. Med. 274,1344–1349
69 Miyamoto, K., Khosrof, S., Bursell, S. E., Rohan, R., Murata, T.,Clermont, A. C., Aiello, L. P., Ogura, Y. and Adamis, A. P. (1999)Prevention of leukostasis and vascular leakage instreptozotocin-induced diabetic retinopathy via intercellularadhesion molecule-1 inhibition. Proc. Natl. Acad. Sci. U.S.A.96, 10836–10841
70 Antonetti, D. A., Barber, A. J., Bronson, S. K., Freeman, W. M.,Gardner, T. W., Jefferson, L. S., Kester, M., Kimball, S. R.,Krady, J. K., LaNoue, K. F. et al. (2006) Diabetic retinopathy:seeing beyond glucose-induced microvascular disease.Diabetes 55, 2401–2411
71 Roy, M. S., Gunkel, R. D. and Podgor, M. J. (1986) Color visiondefects in early diabetic retinopathy. Arch. Ophthalmol. 104,225–228
72 Sokol, S., Moskowitz, A., Skarf, B., Evans, R., Molitch, M. andSenior, B. (1985) Contrast sensitivity in diabetics with andwithout background retinopathy. Arch. Ophthalmol. 103, 51–54
73 Yonemura, D., Aoki, T. and Tsuzuki, K. (1962) Electroretinogramin diabetic retinopathy. Arch. Ophthalmol. 68, 19–24
74 Barber, A. J., Lieth, E., Khin, S. A., Antonetti, D. A., Buchanan,A. G. and Gardner, T. W. (1998) Neural apoptosis in the retinaduring experimental and human diabetes. Early onset andeffect of insulin. J. Clin. Invest 102, 783–791
75 Gastinger, M. J., Singh, R. S. and Barber, A. J. (2006) Loss ofcholinergic and dopaminergic amacrine cells instreptozotocin-diabetic rat and Ins2Akita-diabetic mouseretinas. Invest. Ophthalmol. Visual Sci. 47, 3143–3150
76 Martin, P. M., Roon, P., Van Ells, T. K., Ganapathy, V. and Smith,S. B. (2004) Death of retinal neurons in streptozotocin-induceddiabetic mice. Invest. Ophthalmol. Visual Sci. 45, 3330–3336
77 Park, S. H., Park, J. W., Park, S. J., Kim, K. Y., Chung, J. W.,Chun, M. H. and Oh, S. J. (2003) Apoptotic death ofphotoreceptors in the streptozotocin-induced diabetic rat retina.Diabetologia 46, 1260–1268
78 Phipps, J. A., Fletcher, E. L. and Vingrys, A. J. (2004)Paired-flash identification of rod and cone dysfunction in thediabetic rat. Invest. Ophthalmol. Visual Sci. 45, 4592–4600
79 Mizutani, M., Gerhardinger, C. and Lorenzi, M. (1998) Mullercell changes in human diabetic retinopathy. Diabetes 47,445–449
80 Puro, D. G. (2002) Diabetes-induced dysfunction of retinalMuller cells. Trans. Am. Ophthalmol. Soc. 100, 339–352
81 Lieth, E., Barber, A. J., Xu, B., Dice, C., Ratz, M. J., Tanase, D.and Strother, J. M. (1998) Glial reactivity and impairedglutamate metabolism in short-term experimental diabeticretinopathy. Diabetes 47, 815–820
82 Brownlee, M. (2001) Biochemistry and molecular cell biology ofdiabetic complications. Nature 414, 813–820
83 Hammes, H. P., Du, X., Edelstein, D., Taguchi, T., Matsumura, T.,Ju, Q., Lin, J., Bierhaus, A., Nawroth, P., Hannak, D. et al.(2003) Benfotiamine blocks three major pathways ofhyperglycemic damage and prevents experimental diabeticretinopathy. Nat. Med. 9, 294–299
84 Alkhalaf, A., Kleefstra, N., Groenier, K. H., Bilo, H. J., Gans, R.O., Heeringa, P., Scheijen, J. L., Schalkwijk, C. G., Navis, G. J.and Bakker, S. J. (2012) Effect of benfotiamine on advancedglycation endproducts and markers of endothelial dysfunctionand inflammation in diabetic nephropathy. PLoS ONE 7, e40427
85 Fraser, D. A., Diep, L. M., Hovden, I. A., Nilsen, K. B., Sveen, K.A., Seljeflot, I. and Hanssen, K. F. (2012) The effects oflong-term oral benfotiamine supplementation on peripheralnerve function and inflammatory markers in patients withtype 1 diabetes: a 24-month, double-blind, randomized,placebo-controlled trial. Diabetes Care 35, 1095–1097
www.clinsci.org 13

A. W. Stitt and others
86 Kohner, E. M., Patel, V. and Rassam, S. M. (1995) Role ofblood flow and impaired autoregulation in the pathogenesis ofdiabetic retinopathy. Diabetes 44, 603–607
87 Delaey, C., Boussery, K. and Van, d.V. (2000) A retinal-derivedrelaxing factor mediates the hypoxic vasodilation of retinalarteries. Invest. Ophthalmol. Visual Sci. 41, 3555–3560
88 Wagener, H. P., Story, D. T. D. and Wilder, R. M. (1934) Retinitisin diabetes. N. Engl. J. Med. 211, 1131–1137
89 Ballantyne, A. J. and Loewenstein, A. (1943) The pathology ofdiabetic retinopathy. Trans. Ophthalmol. Soc. 63, 95–113
90 Skovborg, F., Nielsen, A. V., Lauritzen, E. and Hartkopp, O.(1969) Diameters of the retinal vessels in diabetic and normalsubjects. Diabetes 18, 292–298
91 Kohner, E. M., Hamilton, A. M., Saunders, S. J., Sutcliffe, B. A.and Bulpitt, C. J. (1975) The retinal blood flow in diabetes.Diabetologia 11, 27–33
92 Kohner, E. M. (1993) The retinal blood flow in diabetes.Diabetes Metab. 19, 401–404
93 Bursell, S. E., Clermont, A. C., Kinsley, B. T., Simonson, D. C.,Aiello, L. M. and Wolpert, H. A. (1996) Retinal blood flowchanges in patients with insulin-dependent diabetes mellitusand no diabetic retinopathy. Invest. Ophthalmol. Visual Sci. 37,886–897
94 Clermont, A. C., Aiello, L. P., Mori, F., Aiello, L. M. and Bursell,S. E. (1997) Vascular endothelial growth factor and severity ofnonproliferative diabetic retinopathy mediate retinalhemodynamics in vivo: a potential role for vascular endothelialgrowth factor in the progression of nonproliferative diabeticretinopathy. Am. J. Ophthalmol. 124, 433–446
95 Clermont, A. C., Brittis, M., Shiba, T., McGovern, T., King, G. L.and Bursell, S. E. (1994) Normalization of retinal blood flow indiabetic rats with primary intervention using insulin pumps.Invest. Ophthalmol. Visual Sci. 35, 981–990
96 Cunha-Vaz, J. G., Fonseca, J. R., de Abreu, J. R. and Lima, J. J.(1978) Studies on retinal blood flow. II. Diabetic retinopathy.Arch. Ophthalmol. 96, 809–811
97 Yoshida, A., Feke, G. T., Morales-Stoppello, J., Collas, G. D.,Goger, D. G. and McMeel, J. W. (1983) Retinal blood flowalterations during progression of diabetic retinopathy. Arch.Ophthalmol. 101, 225–227
98 Ciulla, T. A., Harris, A., Latkany, P., Piper, H. C., Arend, O.,Garzozi, H. and Martin, B. (2002) Ocular perfusionabnormalities in diabetes. Acta Ophthalmol. Scand. 80,468–477
99 Klein, R., Klein, B. E., Moss, S. E., Wong, T. Y., Hubbard, L.,Cruickshanks, K. J. and Palta, M. (2003) Retinal vascularabnormalities in persons with type 1 diabetes: the WisconsinEpidemiologic Study of Diabetic Retinopathy: XVIII.Ophthalmology 110, 2118–2125
100 Schmetterer, L. and Wolzt, M. (1999) Ocular blood flow andassociated functional deviations in diabetic retinopathy.Diabetologia 42, 387–405
101 Klein, R., Myers, C. E., Lee, K. E., Gangnon, R. and Klein, B. E.(2012) Changes in retinal vessel diameter and incidence andprogression of diabetic retinopathy. Arch Ophthalmol 130,749–755
102 Grunwald, J. E., Riva, C. E., Baine, J. and Brucker, A. J. (1992)Total retinal volumetric blood flow rate in diabetic patients withpoor glycemic control. Invest Ophthalmol.Visual Sci. 33,356–363
103 Tang, J. and Kern, T. S. (2011) Inflammation in diabeticretinopathy. Prog. Retin. Eye Res. 30, 343–358
104 Joussen, A. M., Poulaki, V., Le, M. L., Koizumi, K., Esser, C.,Janicki, H., Schraermeyer, U., Kociok, N., Fauser, S., Kirchhof,B. et al. (2004) A central role for inflammation in thepathogenesis of diabetic retinopathy. FASEB J. 18, 1450–1452
105 Talahalli, R., Zarini, S., Tang, J., Li, G., Murphy, R., Kern, T. S.and Gubitosi-Klug, R. A. (2013) Leukocytes regulate retinalcapillary degeneration in the diabetic mouse via generation ofleukotrienes. J. Leukocyte Biol. 93, 135–143
106 Li, G., Veenstra, A. A., Talahalli, R. R., Wang, X., Gubitosi-Klug,R. A., Sheibani, N. and Kern, T. S. (2012) Marrow-derived cellsregulate the development of early diabetic retinopathy andtactile allodynia in mice. Diabetes 61, 3294–3303
107 Gerhardinger, C., Dagher, Z., Sebastiani, P., Park, Y. S. andLorenzi, M. (2009) The transforming growth factor-β pathway isa common target of drugs that prevent experimental diabeticretinopathy. Diabetes 58, 1659–1667
108 Brucklacher, R. M., Patel, K. M., Vanguilder, H. D., Bixler, G. V.,Barber, A. J., Antonetti, D. A., Lin, C. M., Lanoue, K. F., Gardner,T. W., Bronson, S. K. and Freeman, W. M. (2008) Wholegenome assessment of the retinal response to diabetesreveals a progressive neurovascular inflammatory response.BMC Med. Genomics 1, 26
109 Zeng, H. Y., Green, W. R. and Tso, M. O. (2008) Microglialactivation in human diabetic retinopathy. Arch. Ophthalmol.126, 227–232
110 Budzynski, E., Wangsa-Wirawan, N., Padnick-Silver, L., Hatchell,D. and Linsenmeier, R. (2005) Intraretinal pH in diabetic cats.Curr. Eye Res. 30, 229–240
111 Kuiper, E. J., Witmer, A. N., Klaassen, I., Oliver, N.,Goldschmeding, R. and Schlingemann, R. O. (2004) Differentialexpression of connective tissue growth factor in microglia andpericytes in the human diabetic retina. Br. J. Ophthalmol. 88,1082–1087
112 Xu, H., Chen, M. and Forrester, J. V. (2009) Para-inflammationin the aging retina. Prog. Retin. Eye Res. 28, 348–368
113 Barber, A. J., Antonetti, D. A., Kern, T. S., Reiter, C. E., Soans,R. S., Krady, J. K., Levison, S. W., Gardner, T. W. and Bronson,S. K. (2005) The Ins2Akita mouse as a model of early retinalcomplications in diabetes. Invest. Ophthalmol. Visual Sci. 46,2210–2218
114 Rungger-Brandle, E., Dosso, A. A. and Leuenberger, P. M. (2000)Glial reactivity, an early feature of diabetic retinopathy. Invest.Ophthalmol. Visual Sci. 41, 1971–1980
115 Zeng, X. X., Ng, Y. K. and Ling, E. A. (2000) Neuronal andmicroglial response in the retina of streptozotocin-induceddiabetic rats. Visual Neurosci. 17, 463–471
116 Zong, H., Ward, M. and Stitt, A. W. (2011) AGEs, RAGE, anddiabetic retinopathy. Curr. Diabetes Rep. 11, 244–252
117 Barile, G. R., Pachydaki, S. I., Tari, S. R., Lee, S. E., Donmoyer,C. M., Ma, W., Rong, L. L., Buciarelli, L. G., Wendt, T., Horig, H.et al. (2005) The RAGE axis in early diabetic retinopathy. Invest.Ophthalmol. Visual Sci. 46, 2916–2924
118 Donato, R. (2001) S100: a multigenic family ofcalcium-modulated proteins of the EF-hand type withintracellular and extracellular functional roles. Int. J. Biochem.Cell Biol. 33, 637–668
119 Zong, H., Ward, M., Madden, A., Yong, P. H., Limb, G. A., Curtis,T. M. and Stitt, A. W. (2010) Hyperglycaemia-inducedpro-inflammatory responses by retinal Muller glia are regulatedby the receptor for advanced glycation end-products (RAGE).Diabetologia 53, 2656–2666
120 Moore, T. C., Moore, J. E., Kaji, Y., Frizzell, N., Usui, T., Poulaki,V., Campbell, I. L., Stitt, A. W., Gardiner, T. A., Archer, D. B. andAdamis, A. P. (2003) The role of advanced glycation endproducts in retinal microvascular leukostasis. Invest.Ophthalmol. Visual Sci. 44, 4457–4464
121 Li, G., Tang, J., Du, Y., Lee, C. A. and Kern, T. S. (2011)Beneficial effects of a novel RAGE inhibitor on early diabeticretinopathy and tactile allodynia. Mol. Vision 17, 3156–3165
122 Erickson, K. K., Sundstrom, J. M. and Antonetti, D. A. (2007)Vascular permeability in ocular disease and the role of tightjunctions. Angiogenesis. 10, 103–117
123 Trick, G. L., Edwards, P. A., Desai, U., Morton, P. E., Latif, Z. andBerkowitz, B. A. (2008) MRI retinovascular studies in humans:research in patients with diabetes. NMR Biomed. 21,1003–1012
14 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
124 Trick, G. L., Liggett, J., Levy, J., Adamsons, I., Edwards, P.,Desai, U., Tofts, P. S. and Berkowitz, B. A. (2005) Dynamiccontrast enhanced MRI in patients with diabetic macularedema: initial results. Exp. Eye Res 81, 97–102
125 Simo, R., Villarroel, M., Corraliza, L., Hernandez, C. andGarcia-Ramirez, M. (2010) The retinal pigment epithelium:something more than a constituent of the blood-retinal barrier:implications for the pathogenesis of diabetic retinopathy. J.Biomed. Biotechnol. 2010, 190724
126 Xu, H. Z. and Le, Y. Z. (2011) Significance of outer blood-retinabarrier breakdown in diabetes and ischemia. Invest.Ophthalmol. Visual Sci. 52, 2160–2164
127 Krugel, K., Wurm, A., Pannicke, T., Hollborn, M., Karl, A.,Wiedemann, P., Reichenbach, A., Kohen, L. and Bringmann, A.(2011) Involvement of oxidative stress and mitochondrialdysfunction in the osmotic swelling of retinal glial cells fromdiabetic rats. Exp. Eye Res. 92, 87–93
128 Schram, M. T., Chaturvedi, N., Schalkwijk, C., Giorgino, F.,Ebeling, P., Fuller, J. H. and Stehouwer, C. D. (2003) Vascularrisk factors and markers of endothelial function asdeterminants of inflammatory markers in type 1 diabetes: theEURODIAB Prospective Complications Study. Diabetes Care 26,2165–2173
129 Chowdhury, T. A., Hopkins, D., Dodson, P. M. and Vafidis, G. C.(2002) The role of serum lipids in exudative diabeticmaculopathy: is there a place for lipid lowering therapy? Eye16, 689–693
130 Aiello, L. P., Edwards, A. R., Beck, R. W., Bressler, N. M., Davis,M. D., Ferris, F., Glassman, A. R., Ip, M. S. and Miller, K. M(2010) Factors associated with improvement and worsening ofvisual acuity 2 years after focal/grid photocoagulation fordiabetic macular edema. Ophthalmology 117, 946–953
131 Elman, M. J., Aiello, L. P., Beck, R. W., Bressler, N. M., Bressler,S. B., Edwards, A. R., Ferris, III, F. L., Friedman, S. M.,Glassman, A. R., Miller, K. M. et al. (2010) Randomized trialevaluating ranibizumab plus prompt or deferred laser ortriamcinolone plus prompt laser for diabetic macular edema.Ophthalmology 117, 1064–1077
132 Aiello, L. P., Avery, R. L., Arrigg, P. G., Keyt, B. A., Jampel, H. D.,Shah, S. T., Pasquale, L. R., Thieme, H., Iwamoto, M. A. andPark, J. E. (1994) Vascular endothelial growth factor in ocularfluid of patients with diabetic retinopathy and other retinaldisorders. N. Engl. J. Med. 331, 1480–1487
133 Sone, H., Kawakami, Y., Okuda, Y., Sekine, Y., Honmura, S.,Matsuo, K., Segawa, T., Suzuki, H. and Yamashita, K. (1997)Ocular vascular endothelial growth factor levels in diabetic ratsare elevated before observable retinal proliferative changes.Diabetologia 40, 726–730
134 Lip, P. L., Belgore, F., Blann, A. D., Hope-Ross, M. W., Gibson, J.M. and Lip, G. Y. (2000) Plasma VEGF and soluble VEGFreceptor FLT-1 in proliferative retinopathy: relationship toendothelial dysfunction and laser treatment. Invest.Ophthalmol. Visual Sci. 41, 2115–2119
135 Beck, R. W., Edwards, A. R., Aiello, L. P., Bressler, N. M., Ferris,F., Glassman, A. R., Hartnett, E., Ip, M. S., Kim, J. E. andKollman, C. (2009) Three-year follow-up of a randomized trialcomparing focal/grid photocoagulation and intravitrealtriamcinolone for diabetic macular edema. Arch. Ophthalmol.127, 245–251
136 Mitchell, P., Bandello, F., Schmidt-Erfurth, U., Lang, G. E.,Massin, P., Schlingemann, R. O., Sutter, F., Simader, C., Burian,G., Gerstner, O., Weichselberger, A. and group, R. s. (2011) TheRESTORE study: ranibizumab monotherapy or combined withlaser versus laser monotherapy for diabetic macular edema.Ophthalmology 118, 615–625
137 Nguyen, Q. D., Shah, S. M., Khwaja, A. A., Channa, R., Hatef,E., Do, D. V., Boyer, D., Heier, J. S., Abraham, P., Thach, A. B.et al. (2010) Two-year outcomes of the ranibizumab for edemaof the mAcula in diabetes (READ-2) study. Ophthalmology 117,2146–2151
138 Abedi, F., Wickremasinghe, S., Richardson, A. J., Makalic, E.,Schmidt, D. F., Sandhu, S. S., Baird, P. N. and Guymer, R. H.(2013) Variants in the VEGFA gene and treatmentoutcome after anti-VEGF treatment for neovascularage-related macular degeneration. Ophthalmology, 120,115–121
139 Nguyen, Q. D., Shah, S. M., Heier, J. S., Do, D. V., Lim, J.,Boyer, D., Abraham, P., Campochiaro, P. A. and Group, R.-S.(2009) Primary end point (six months): results of theRanibizumab for Edema of the mAcula in diabetes (READ-2)study. Ophthalmology 116, 2175–2181
140 Massin, P., Bandello, F., Garweg, J. G., Hansen, L. L., Harding,S. P., Larsen, M., Mitchell, P., Sharp, D., Wolf-Schnurrbusch, U.E., Gekkieva, M., Weichselberger, A. and Wolf, S. (2010) Safetyand efficacy of ranibizumab in diabetic macular edema(RESOLVE Study): a 12-month, randomized, controlled,double-masked, multicenter phase II study. Diabetes Care 33,2399–2405
141 Michaelides, M., Kaines, A., Hamilton, R. D., Fraser-Bell, S.,Rajendram, R., Quhill, F., Boos, C. J., Xing, W., Egan, C., Peto, T.et al. (2010) A prospective randomized trial of intravitrealbevacizumab or laser therapy in the management of diabeticmacular edema (BOLT study) 12-month data: report 2.Ophthalmology 117, 1078–1086
142 Do, D. V., Schmidt-Erfurth, U., Gonzalez, V. H., Gordon, C. M.,Tolentino, M., Berliner, A. J., Vitti, R., Ruckert, R., Sandbrink,R., Stein, D. et al. (2011) The DA VINCI Study: phase 2 primaryresults of VEGF Trap-Eye in patients with diabetic macularedema. Ophthalmology 118, 1819–1826
143 Dewan, V., Lambert, D., Edler, J., Kymes, S. and Apte, R. S.(2012) Cost-effectiveness analysis of ranibizumab plusprompt or deferred laser or triamcinolone plus prompt laserfor diabetic macular edema. Ophthalmology 119,1679–1684
144 Haller, J. A., Kuppermann, B. D., Blumenkranz, M. S., Williams,G. A., Weinberg, D. V., Chou, C. and Whitcup, S. M. (2010)Randomized controlled trial of an intravitreous dexamethasonedrug delivery system in patients with diabetic macular edema.Arch. Ophthalmol. 128, 289–296
145 Campochiaro, P. A., Brown, D. M., Pearson, A., Ciulla, T., Boyer,D., Holz, F. G., Tolentino, M., Gupta, A., Duarte, L., Madreperla,S. et al. (2011) Long-term benefit of sustained-deliveryfluocinolone acetonide vitreous inserts for diabetic macularedema. Ophthalmology 118, 626–635
146 Arrigg, P. G. and Cavallerano, J. (1998) The role ofvitrectomy for diabetic retinopathy. J. Am. Optom. Assoc. 69,733–740
147 Keech, A. C., Mitchell, P., Summanen, P. A., O’Day, J., Davis, T.M., Moffitt, M. S., Taskinen, M. R., Simes, R. J., Tse, D.,Williamson, E. et al. (2007) Effect of fenofibrate on the need forlaser treatment for diabetic retinopathy (FIELD study): arandomised controlled trial. Lancet 370, 1687–1697
148 Spranger, J., Mohlig, M., Osterhoff, M., Buhnen, J., Blum, W. F.and Pfeiffer, A. F. (2001) Retinal photocoagulation does notinfluence intraocular levels of IGF-I, IGF-II and IGF-BP3 inproliferative diabetic retinopathy-evidence for combinedtreatment of PDR with somatostatin analogues andretinal photocoagulation? Horm. Metab. Res. 33,312–316
149 Campochiaro, P. A., Hafiz, G., Channa, R., Shah, S. M., Nguyen,Q. D., Ying, H., Do, D. V., Zimmer-Galler, I., Solomon, S. D.,Sung, J. U. and Syed, B. (2010) Antagonism of vascularendothelial growth factor for macular edema caused by retinalvein occlusions: two-year outcomes. Ophthalmology 117,2387–2394
150 Benjamin, LE, Hemo, I and E, K. (1998) A plasticity window forblood vessel remodelling is defined by pericyte coverage of thepreformed endothelial network and is regulated by PDGF-B andVEGF. Development 125, 1591–1598
www.clinsci.org 15

A. W. Stitt and others
151 Nishijima, K., Ng, Y. S., Zhong, L., Bradley, J., Schubert, W., Jo,N., Akita, J., Samuelsson, S. J., Robinson, G. S., Adamis, A. P.and Shima, D. T. (2007) Vascular endothelial growth factor-A isa survival factor for retinal neurons and a criticalneuroprotectant during the adaptive response to ischemicinjury. Am. J. Pathol. 171, 53–67
152 Saint-Geniez, M. and D’Amore, P. A. (2004) Development andpathology of the hyaloid, choroidal and retinal vasculature. Int.J. Dev. Biol. 48, 1045–1058
153 Saint-Geniez, M., Maharaj, A. S., Walshe, T. E., Tucker, B. A.,Sekiyama, E., Kurihara, T., Darland, D. C., Young, M. J. andD’Amore, P. A. (2008) Endogenous VEGF is required for visualfunction: evidence for a survival role on muller cells andphotoreceptors. PLoS ONE 3, e3554
154 D’Amore, P. A. (2007) Vascular endothelial cell growth factor-A:not just for endothelial cells anymore. Am. J. Pathol. 171,14–18
155 Chung, E. J., Freeman, W. R. and Koh, H. J. (2008) Visual acuityand multifocal electroretinographic changes after arteriovenouscrossing sheathotomy for macular edema associated withbranch retinal vein occlusion. Retina 28, 220–225
156 Chung, E. J., Hong, Y. T., Lee, S. C., Kwon, O. W. and Koh, H. J.(2008) Prognostic factors for visual outcome after intravitrealbevacizumab for macular edema due to branch retinal veinocclusion. Graefes Arch. Clin. Exp. Ophthalmol. 246,1241–1247
157 Kim, L. A. and D’Amore, P. A. (2012) A brief history of anti-VEGFfor the treatment of ocular angiogenesis. Am. J. Pathol. 181,376–379
158 Goven, D., Boutten, A., Lecon-Malas, V., Marchal-Somme, J.,Amara, N., Crestani, B., Fournier, M., Leseche, G., Soler, P.,Boczkowski, J. and Bonay, M. (2008) Altered Nrf2/Keap1-Bach1equilibrium in pulmonary emphysema. Thorax 63, 916–924
159 Malhotra, D., Thimmulappa, R., Navas-Acien, A., Sandford, A.,Elliott, M., Singh, A., Chen, L., Zhuang, X., Hogg, J., Pare, P.et al. (2008) Decline in NRF2-regulated antioxidants in chronicobstructive pulmonary disease lungs due to loss of its positiveregulator, DJ-1. Am. J. Respir. Crit. Care Med. 178, 592–604
160 Malhotra, D., Thimmulappa, R., Vij, N., Navas-Acien, A.,Sussan, T., Merali, S., Zhang, L., Kelsen, S. G., Myers, A.,Wise, R. et al. (2009) Heightened endoplasmic reticulumstress in the lungs of patients with chronic obstructivepulmonary disease: the role of Nrf2-regulated proteasomalactivity. Am. J. Respir. Crit. Care Med 180, 1196–1207
161 Suzuki, M., Betsuyaku, T., Ito, Y., Nagai, K., Nasuhara, Y., Kaga,K., Kondo, S. and Nishimura, M. (2008) Down-regulatedNF-E2-related factor 2 in pulmonary macrophages of agedsmokers and patients with chronic obstructive pulmonarydisease. Am. J. Respir. Cell Mol. Biol. 39, 673–682
162 Pergola, P. E., Krauth, M., Huff, J. W., Ferguson, D. A., Ruiz, S.,Meyer, C. J. and Warnock, D. G. (2011) Effect of bardoxolonemethyl on kidney function in patients with T2D and Stage 3b-4CKD. Am. J. Nephrol. 33, 469–476
163 Kowluru, R. A. and Zhong, Q. (2011) Beyond AREDS: is there aplace for antioxidant therapy in the prevention/treatment of eyedisease? Invest. Ophthalmol. Visual Sci. 52, 8665–8671
164 Ellis, E. A., Grant, M. B., Murray, F. T., Wachowski, M. B.,Guberski, D. L., Kubilis, P. S. and Lutty, G. A. (1998) IncreasedNADH oxidase activity in the retina of the BBZ/Wor diabetic rat.Free Radical Biol. Med. 24, 111–120
165 Ellis, E. A., Guberski, D. L., Somogyi-Mann, M. and Grant, M. B.(2000) Increased H2O2, vascular endothelial growth factor andreceptors in the retina of the BBZ/Wor diabetic rat. Free RadicalBiol. Med. 28, 91–101
166 Ellis, E. A., Guberski, D. L., Hutson, B. and Grant, M. B. (2002)Time course of NADH oxidase, inducible nitric oxide synthaseand peroxynitrite in diabetic retinopathy in the BBZ/WOR rat.Nitric Oxide 6, 295–304
167 Chen, P., Guo, A. M., Edwards, P. A., Trick, G. and Scicli, A. G.(2007) Role of NADPH oxidase and ANG II in diabetes-inducedretinal leukostasis. Am. J. Physiol. Regul. Integ. Comp. Physiol.293, R1619–R1629
168 Al-Shabrawey, M., Rojas, M., Sanders, T., Behzadian, A.,El-Remessy, A., Bartoli, M., Parpia, A. K., Liou, G. and Caldwell,R. B. (2008) Role of NADPH oxidase in retinal vascularinflammation. Invest. Ophthalmol. Visual Sci. 49, 3239–3244
169 Gao, B. B., Clermont, A., Rook, S., Fonda, S. J., Srinivasan, V.J., Wojtkowski, M., Fujimoto, J. G., Avery, R. L., Arrigg, P. G.,Bursell, S. E. et al. (2007) Extracellular carbonic anhydrasemediates hemorrhagic retinal and cerebral vascularpermeability through prekallikrein activation. Nat. Med. 13,181–188
170 Giusti, C., Forte, R., Vingolo, E. M. and Gargiulo, P. (2001) Isacetazolamide effective in the treatment of diabetic macularedema? A pilot study. Int. Ophthalmol. 24, 79–88
171 Kita, T., Clermont, A. C., Fujisawa, K., Ishibashi, T., Aiello, L. P.and Feener, E. P. (2012) Identification of a VEGF-independentand plasma kallikrein-kinin-dependent pathway of retinalvascular permeability in diabetic macular edema. Invest.Ophthalmol. Visual Sci. 2431, A526
172 Carmeliet, P. (2004) Manipulating angiogenesis in medicine. J.Intern. Med. 255, 538–561
173 Smith, L. E., Wesolowski, E., McLellan, A., Kostyk, S. K.,D’Amato, R., Sullivan, R. and D’Amore, P. A. (1994)Oxygen-induced retinopathy in the mouse. Invest. Ophthalmol.Visual Sci. 35, 101–111
174 Stitt, A. W., McKenna, D., Simpson, D. A., Gardiner, T. A.,Harriott, P., Archer, D. B. and Nelson, J. (1998) The 67-kdlaminin receptor is preferentially expressed by proliferatingretinal vessels in a murine model of ischemic retinopathy. Am.J. Pathol. 152, 1359–1365
175 Donaldson, E. A., McKenna, D. J., McMullen, C. B., Scott, W.N., Stitt, A. W. and Nelson, J. (2000) The expression ofmembrane-associated 67-kDa laminin receptor (67LR) ismodulated in vitro by cell-contact inhibition. Mol. Cell. Biol. Res.Comm. 3, 53–59
176 McKenna, D. J., Simpson, D. A., Feeney, S., Gardiner, T. A.,Boyle, C., Nelson, J. and Stitt, A. W. (2001) Expression of the67 kDa laminin receptor (67LR) during retinal development:correlations with angiogenesis. Exp. Eye Res. 73, 81–92
177 Gardiner, T. A., Gibson, D. S., de Gooyer, T. E., de la Cruz, V. F.,McDonald, D. M. and Stitt, A. W. (2005) Inhibition of tumornecrosis factor-α improves physiological angiogenesis andreduces pathological neovascularization in ischemicretinopathy. Am. J. Pathol. 166, 637–644
178 Medina, R. J., O’Neill, C. L., Devine, A. B., Gardiner, T. A. andStitt, A. W. (2008) The pleiotropic effects of simvastatin onretinal microvascular endothelium has important implicationsfor ischaemic retinopathies. PLoS ONE 3, e2584
179 McVicar, C. M., Colhoun, L. M., Abrahams, J. L., Kitson, C. L.,Hamilton, R., Medina, R. J., Durga, D., Gardiner, T. A., Rudd, P.M. and Stitt, A. W. (2010) Differential modulation ofangiogenesis by erythropoiesis-stimulating agents in a mousemodel of ischaemic retinopathy. PLoS ONE 5, e11870
180 Chen, J., Connor, K. M., Aderman, C. M. and Smith, L. E.(2008) Erythropoietin deficiency decreases vascular stability inmice. J. Clin. Invest. 118, 526–533
181 McVicar, C. M., Hamilton, R., Colhoun, L. M., Gardiner, T. A.,Brines, M., Cerami, A. and Stitt, A. W. (2011) Intervention withan erythropoietin-derived peptide protects against neuroglialand vascular degeneration during diabetic retinopathy. Diabetes60, 2995–3005
182 Thum, T., Fraccarollo, D., Schultheiss, M., Froese, S., Galuppo,P., Widder, J. D., Tsikas, D., Ertl, G. and Bauersachs, J. (2007)Endothelial nitric oxide synthase uncoupling impairs endothelialprogenitor cell mobilization and function in diabetes. Diabetes56, 666–674
16 C© The Authors Journal compilation C© 2013 Biochemical Society

Advances in our understanding of diabetic retinopathy
183 O’Neill, C. L., O’Doherty, M. T., Wilson, S. E., Rana, A. A., Hirst,C. E., Stitt, A. W. and Medina, R. J. (2012) Therapeuticrevascularisation of ischaemic tissue: the opportunities andchallenges for therapy using vascular stem/progenitor cells.Stem Cell Res. Ther. 3, 31
184 Hibbert, B., Olsen, S. and O’Brien, E. (2003) Involvement ofprogenitor cells in vascular repair. Trends Cardiovasc. Med. 13,322–326
185 Stitt, A. W., O’Neill, C. L., O’Doherty, M. T., Archer, D. B.,Gardiner, T. A. and Medina, R. J. (2011) Vascular stem cellsand ischaemic retinopathies. Prog. Ret. Eye Res. 30, 149–166
186 Kusuyama, T., Omura, T., Nishiya, D., Enomoto, S., Matsumoto,R., Takeuchi, K., Yoshikawa, J. and Yoshiyama, M. (2006)Effects of treatment for diabetes mellitus on circulatingvascular progenitor cells. J. Pharmacol. Sci. 102, 96–102
187 Fadini, G. P., Sartore, S., Albiero, M., Baesso, I., Murphy, E.,Menegolo, M., Grego, F., Vigili de Kreutzenberg, S., Tiengo, A.,Agostini, C. and Avogaro, A. (2006) Number and function ofendothelial progenitor cells as a marker of severity for diabeticvasculopathy. Arterioscler. Thromb. Vasc. Biol. 26, 2140–2146
188 Tepper, O. M., Galiano, R. D., Capla, J. M., Kalka, C., Gagne, P.J., Jacobowitz, G. R., Levine, J. P. and Gurtner, G. C. (2002)Human endothelial progenitor cells from type II diabetics exhibitimpaired proliferation, adhesion, and incorporation intovascular structures. Circulation 106, 2781–2786
189 Ingram, D. A., Lien, I. Z., Mead, L. E., Estes, M., Prater, D. N.,Derr-Yellin, E., DiMeglio, L. A. and Haneline, L. S. (2008) In vitrohyperglycemia or a diabetic intrauterine environment reducesneonatal endothelial colony-forming cell numbers and function.Diabetes 57, 724–731
190 Loomans, C. J., de Koning, E. J., Staal, F. J., Rookmaaker, M.B., Verseyden, C., de Boer, H. C., Verhaar, M. C., Braam, B.,Rabelink, T. J. and van Zonneveld, A. J. (2004) Endothelialprogenitor cell dysfunction: a novel concept in the pathogenesisof vascular complications of type 1 diabetes. Diabetes 53,195–199
191 Egan, C. G., Lavery, R., Caporali, F., Fondelli, C., Laghi-Pasini, F.,Dotta, F. and Sorrentino, V. (2008) Generalised reduction ofputative endothelial progenitors and CXCR4-positive peripheralblood cells in type 2 diabetes. Diabetologia 51, 1296–1305
192 Shantsila, E., Watson, T. and Lip, G. Y. (2007) Endothelialprogenitor cells in cardiovascular disorders. J. Am. Coll. Cardiol.49, 741–752
193 Grant, M. B., May, W. S., Caballero, S., Brown, G. A., Guthrie, S.M., Mames, R. N., Byrne, B. J., Vaught, T., Spoerri, P. E., Peck,A. B. and Scott, E. W. (2002) Adult hematopoietic stem cellsprovide functional hemangioblast activity during retinalneovascularization. Nat. Med. 8, 607–612
194 Dorrell, M. I., Otani, A., Aguilar, E., Moreno, S. K. andFriedlander, M. (2004) Adult bone marrow-derived stem cellsuse R-cadherin to target sites of neovascularization in thedeveloping retina. Blood 103, 3420–3427
195 Caballero, S., Sengupta, N., Afzal, A., Chang, K. H., Li Calzi, S.,Guberski, D. L., Kern, T. S. and Grant, M. B. (2007) Ischemicvascular damage can be repaired by healthy, butnot diabetic, endothelial progenitor cells. Diabetes 56,960–967
196 Medina, R. J., O’Neill, C. L., Humphreys, M. W., Gardiner, T. A.and Stitt, A. W. (2010) Outgrowth endothelial cells:characterization and their potential for reversing ischemicretinopathy. Invest. Ophthalmol. Visual Sci. 51,5906–5913
197 Medina, R. J., O’Neill, C. L., O’Doherty, T. M., Knott, H.,Guduric-Fuchs, J., Gardiner, T. A. and Stitt, A. W. (2011) Myeloidangiogenic cells act as alternative M2 macrophages andmodulate angiogenesis through interleukin-8. Mol. Med. 17,1045–1055
198 Otani, A., Kinder, K., Ewalt, K., Otero, F. J., Schimmel, P. andFriedlander, M. (2002) Bone marrow-derived stem cells targetretinal astrocytes and can promote or inhibit retinalangiogenesis. Nat. Med. 8, 1004–1010
199 Awad, O., Jiao, C., Ma, N., Dunnwald, M. and Schatteman, G. C.(2005) Obese diabetic mouse environment differentially affectsprimitive and monocytic endothelial cell progenitors. Stem Cells23, 575–583
200 Crisan, M., Yap, S., Casteilla, L., Chen, C. W., Corselli, M.,Park, T. S., Andriolo, G., Sun, B., Zheng, B., Zhang, L. et al.(2008) A perivascular origin for mesenchymal stem cells inmultiple human organs. Cell Stem Cell 3, 301–313
201 Quevedo, H. C., Hatzistergos, K. E., Oskouei, B. N.,Feigenbaum, G. S., Rodriguez, J. E., Valdes, D., Pattany, P. M.,Zambrano, J. P., Hu, Q., McNiece, I. et al. (2009) Allogeneicmesenchymal stem cells restore cardiac function in chronicischemic cardiomyopathy via trilineage differentiating capacity.Proc. Natl. Acad. Sci. U.S.A. 106, 14022–14027
202 Dar, A., Domev, H., Ben-Yosef, O., Tzukerman, M., Zeevi-Levin,N., Novak, A., Germanguz, I., Amit, M. and Itskovitz-Eldor, J.(2012) Multipotent vasculogenic pericytes from humanpluripotent stem cells promote recovery of murine ischemiclimb. Circulation 125, 87–99
203 Katare, R., Riu, F., Mitchell, K., Gubernator, M., Campagnolo, P.,Cui, Y., Fortunato, O., Avolio, E., Cesselli, D., Beltrami, A. P.et al. (2011) Transplantation of human pericyte progenitor cellsimproves the repair of infarcted heart through activation of anangiogenic program involving micro-RNA-132. Circ. Res. 109,894–906
Received 30 October 2012/19 December 2012; accepted 22 January 2013
Published on the Internet 13 March 2013, doi: 10.1042/CS20120588
www.clinsci.org 17












![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://img.dokumen.tips/doc/110x75/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)