Embed Size (px)
Citation preview

Advances in Canine Cardiology
Veterinary Focus - Vol. 18(3) 2008
Richard Harvey PhD, BVSc, DVD, FIBiol, MRCVS - Editor
Biomarkers in the Diagnosis of Canine Heart Disease
Caryn Reynolds and Mark Oyama
New Echocardiographic and Doppler Techniques
Valérie Chetboul
Interventional Cardiovascular Procedures
Suzanne Cunningham and John Rush
How I Treat... Valvular Heart Disease in the Dog
Adrian Boswood
Royal Canin Viewpoint... Nutritional Management of Early Cardiac Disease: ACT with SPEED
Daniel Baker and Denise Elliott
How I Approach... Syncope in Dogs - A Syndrome, not a Disease
Marianne Skrodzki and Eberhard Trautvetter
Cut-out and Keep Guide... Electrocardiography in Dogs
Michael Johnson
Editorial Committee: Dr. Denise A. Elliott, BVSc(Hons), PhD, Dipl. ACVIM, Dipl. ACVN, Scientific Affairs, Royal
Canin, USA; Dr. Philippe Marniquet, DVM, Scientific Communication Manager, Royal Canin, France; Dr. Pauline
Devlin, BSc, PhD, Marketing Director, Royal Canin, UK; Dr. Franziska Conrad, DVM, Scientific Communications,
Royal Canin, Germany; Dr. Julieta Asanovic, DVM, Dipl. FCV, UBA, Scientific Communications, Royal Canin,
Argentina.
http://www.ivis.org/journals/vetfocus/18_3/en/toc.asp

2 / / Veterinary Focus / / Vol 18 No 3 / / 2008
IntroductionTraditionally, the evaluation of heart functionhas been accomplished by electrocardiography,radiography, and echocardiography. These testsare relatively time-consuming and expensive,and in the case of echocardiography, may not beavailable to all patients. Within the past 10 years,cardiac biomarkers, primarily cardiac troponinand natriuretic peptides, have become a mainstayfor both the diagnosis and patient monitoring inhuman heart disease. Recently, veterinary researchhas provided insight into the utility of theseblood-based cardiac biomarkers in canine andfeline patients.
A biomarker is defined as a substance elaboratedby a specific tissue that can be detected incirculation. To be clinically useful, it should bereleased in proportion to a particular diseaseprocess, and provide information regarding
presence, severity, and prognosis of the disease.Ideally, the biomarker would be stable and easyto detect with a widely available, rapid, andinexpensive assay. Biomarkers are commonly usedin veterinary patients to evaluate the function ofother organs; for example, BUN and creatinine areused to monitor kidney function, while ALT assesseshepatocellular damage. In the past, the classicenzymatic assays of cardiac disease, such as creatinekinase, lacked requisite sufficient sensitivity andspecificity for useful clinical application in dogs.In contrast, cardiac troponin and natriuretic peptidetesting appears to offer useful information in casesof canine heart disease. This review discussesavailable veterinary information regarding thesetests and potential applications.
Natriuretic peptidesChronic overstimulation of the renin-angiotensin-aldosterone system occurs with heart disease,
Caryn Reynolds, DVMMatthew J. Ryan Veterinary Hospital, School ofVeterinary Medicine, University of Pennsylvania,Philadelphia, USA
Dr. Reynolds is a Cardiology Resident at the School ofVeterinary Medicine within the University ofPennsylvania. She received her DVM from Colorado StateUniversity in 2006. Caryn Reynolds completed a SmallAnimal Medicine and Surgery internship and a CardiologyResearch internship at the Ryan Veterinary Hospital withinthe University of Pennsylvania.
Mark Oyama, DVM, Dipl. ACVIM (Cardiology)
Matthew J. Ryan Veterinary Hospital, School of Veterinary Medicine, University of
Pennsylvania, Philadelphia, USA
Dr. Oyama graduated from the University of Illinois in1994. He completed an internship at The AnimalMedical Center in NYC and then a residency in
cardiology at the University of California, Davis.Mark Oyama is currently an Associate Professor at
the Department of Clinical Sciences within theUniversity of Pennsylvania.
Biomarkers inthe diagnosis of canine
heart disease
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 3
which leads to cardiac enlargement, volumeoverload, and congestive heart failure. Thenatriuretic peptides counteract this activity bystimulating natriuresis, renal blood flow, diuresis,and vasodilation as well as enhancing diastolicheart function. Circulating atrial natriuretic peptide(ANP) and B-type natriuretic peptide (BNP) levelsare increased primarily in response to increasedmyocardial wall stress. ANP originates mainlyfrom the atria while BNP comes from both theatrial and ventricular myocytes. Both are releasedas precursor molecules then cleaved by serumproteases to form equal amounts of the activeC-terminal fragments (sometimes referred to asC-ANP and C-BNP), and an inactive N-terminalfragment (NT-proANP and NT-proBNP) (Figure 1).C-ANP and C-BNP have ultrashort half-lives,and measurement of circulating concentrationscan be difficult; NT-proANP and NT-proBNP havelonger half-lives and are more stable for collectionand sample handling, making measurement morepractical in the clinical setting. Canine-specificELISA tests for NT-proANP and NT-proBNP haverecently become available.
Currently, measurement of plasma or serumnatriuretic peptide concentrations is consideredpart of the diagnostic database for the humancardiovascular patient. In the emergency setting,NT-proBNP can be used in conjunction withphysical examination, thoracic radiography, andelectrocardiography to differentiate primaryrespiratory causes of dyspnea from congestive heartfailure (1). BNP independently predicts the riskof death or heart failure in the asymptomaticpatient, making it a valuable tool for risk assessmentand patient screening. Measurement of BNPconcentrations also helps clinicians monitor theshort-term response to congestive heart failuretherapy (2). In humans, renal function, gender,obesity, and age influence blood natriuretic levels,and must be considered when interpreting results.
Several studies have been published recentlyevaluating the utility of blood natriuretic peptides,NT-proBNP in particular, testing for dogs. Themajor indications for use are discussed below.
Diagnosis of heart diseaseBoswood, et al. reported a significant differencebetween dogs with heart disease, dogs with
heart failure, and dogs with primary respiratorydisease. Based on a cut-off value of 210 pmol/L,NT-proBNP had a positive predictive value of94% and a negative predictive value of 77% forpredicting dogs with heart disease or heart failure(3). This means that dogs with a positive testwere 94% likely to have heart disease or failurewhile dogs with a negative test were 77% likely tonot have heart disease or heart failure. In anotherstudy by Oyama, et al. (4) of 119 dogs with mitralvalve disease, 18 dogs with dilated cardiomyopathy,and 40 healthy control dogs, serum NT-proBNPdiscriminated dogs with cardiac disease fromhealthy dogs with a positive predictive value of97% and a negative predictive value of 61% whenusing a cut-off value of 445 pmol/L. In addition,it was reported that NT-proBNP was correlatedto heart rate, respiratory rate, echocardiographicheart size, and renal function. Moreover, NT-proBNP could be used to determine which dogshad clinically significant radiographic heartenlargement vs. those that did not, using a cut-offvalue of 680 pmol/L (positive predictive value,81%; negative predictive value, 86%).
The results of these studies suggest that NT-proBNPmeasurement can be utilized in conjunctionwith other diagnostic tools, including physicalexamination, radiography and echocardiography
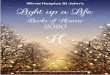
Figure 1.
NT-proBNP is formed when proBNP is cleaved by serumendopeptidases to form C-BNP. NT-proBNP is biologicallyinactive, but has greater stability than C-BNP, and becauseNT-proBNP is formed in a 1:1 proportion with C-BNP,measurement of NT-proBNP reflects the amount of biologicallyactive C-BNP that is produced in situations of underlyingheart disease.
ProBNP
NT-proBNP C-BNP
InactiveMore stable
Longer half-life
Biologically activeLess stable
Shorter half-life
Published in IVIS with the permission of the editor Close window to return to IVIS

4 / / Veterinary Focus / / Vol 18 No 3 / / 2008
to help diagnose heart disease in dogs. Thecommercial laboratory currently performingNT-proBNP assay maintains that heart diseaseis unlikely in patients with serum or plasmaNT-proBNP is ≤566 pmol/L. Prospective studiesare currently being conducted to determinewhether NT-proBNP can be used for serialmonitoring of dogs with asymptomatic mitralvalve disease to assess the risk of any individualdogs for developing actual congestive heart failuresecondary to its disease.
Etiology of respiratory signsFine, et al. (5) evaluated 46 dogs with cough orrespiratory distress and determined that dogs withcongestive heart failure had significantly highermedian NT-proBNP concentrations than thosewith respiratory disease (heart failure, median,2554 pmol/L, interquartile [25%-75%] range,1652-3476; respiratory, median, 357 pmol/L,interquartile range, [193-566]. These resultshighly support the possibility that NT-proBNPcan help determine the underlying cause ofrespiratory signs in dogs. Indeed, in a study of116 dogs presenting to referral hospitals formoderate to severe respiratory signs (i.e.,cough, wheeze, dyspnea, etc), serum NT-proBNP>1200 pmol/L had a positive predictive value of85.5% and a negative predictive value of 81.6%for distinguishing dogs with congestive heartfailure from those with signs due to primaryrespiratory disease (6). These results are similarto scientific abstracts presented by Fine, et al. andWess, et al., which show good sensitivity for thediagnosis of congestive heart failure in dogs withrespiratory disease (5,7).
Determining the cause of respiratory signs inolder, small-breed dogs in which mitral valvedisease and chronic primary respiratory diseasesoften occur concurrently can be challenging. Afinding of NT-proBNP >1200 pmol/L in thesecases can be particularly helpful if historical,physical examination, or radiographic findingsare either not available or are equivocal (8). A rapidin-hospital point-of-care test, as is available inhuman emergency hospitals, would be valuablein veterinary patients that do not tolerateradiography due to the severity of their respiratorydistress until stabilized by initial treatment. Incases of severe pulmonary disease and concurrent
pulmonary hypertension NT-proBNP can be falselyelevated and this has the potential to confoundinterpretation of the test results.
Screening for occult diseaseCurrently, diagnosis of occult DCM in dogstypically requires echocardiography and Holtermonitor, which are relatively expensive,inconvenient (with respect to the need for thedog to wear the Holter monitor for 24hrs), andnot available to all dog owners. In a study of118 Doberman Pinschers, Boxers, and GreatDanes, NT-proANP, C-BNP, and cardiac troponinwere significantly different between the 21 dogsdiagnosed with occult cardiomyopathy vs. thehealthy dogs. Of the three biomarkers, BNPhad the best sensitivity and specificity (95.2%and 61.9%, respectively) for detection of occultdisease (9).
Larger studies are currently being conducted toevaluate the utility of NT-proBNP and NT-proANPas screening tests for occult DCM. A biomarkerthat detects early cardiomyopathy in asymptomaticpatients would have substantial clinical utility.Based on the results of these studies, cut-off values,sensitivity, specificity, and positive and negativepredictive values will help determine how to usethis test in a clinical setting for predisposed dogs,such as Dobermans, Boxers, and Great Danes.
Considerations forinterpretation of result As NT-proBNP testing becomes more widelyavailable, there are some factors to considerregarding interpretation of the results. In a studycomparing normal dogs to dogs with renalazotemia (and structurally normal hearts), therenal dysfunction group had a serum meanNT-BNP level of 1069 pmol/L (range 179-2071),which was significantly elevated compared tothe normal group (mean 282 pmol/L, range 179-578 pmol/L) (10). Thus, renal dysfunction mayfalsely elevate canine NT-proBNP concentrations,as is the case in humans.
Little is known about the day-to-day variation inNT-proBNP concentrations. Theoretically, diet,water intake, and exercise could influence theNT-proBNP concentration in both healthy anddiseased dogs. In a study of weekly variation of
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 5
NT-proBNP in healthy dogs, the variability inserum and plasma NT-proBNP was as high as51% in some dogs. The degree of variation causedsome dogs to occasionally test above the currentupper reference limit of 566 pmol/L. Thus, overtlyhealthy dogs, with only mild elevation of a singleNT-proBNP test, may benefit from serial testing (11).
While NT-proBNP and NT-proANP are more stablethan their C-terminal counterpart, strict adherenceto the sample handling, storage, and shippingdirections as provided by the assay manufacturershould be followed. Plasma or serum samplesshould be separated quickly and frozen assignificant degradation of NT-proBNP occurswithin 3 to 5 hours if samples are allowed to reachtemperatures above 4° C (12).
In summary, based on the currently availableresearch, blood natriuretic peptides can be usedin conjunction with other diagnostic tools,including physical examination, radiography,and echocardiography to help diagnose heartdisease and determine the underlying causeof respiratory signs in dogs. The NT-proBNPassay may also have utility in detecting occultcardiomyopathy in asymptomatic dogs. Thecurrent recommendations indicate that heartdisease is unlikely in dogs if the NT-proBNPlevel is <566 pmol/L. In patients with respiratorysigns, an NT-proBNP greater >1200 pmol/L islikely associated with congestive heart failure.Most of the current literature involves NT-proBNPtesting, and the clinical utility of NT-proANPis slightly less clear; further studies are warrantedto determine the best way to use this test inconjunction with NT-proBNP or other cardiacbiomarkers, such as cardiac troponin.
Cardiac troponinThe troponin complex is composed of 3 subunits(cTnI, cTnT, and cTnC) that help regulate excitation-contraction coupling in the cardiac myocyte.cTnI is the inhibitory component that preventsinteraction between actin and myosin until cTnCbinds to calcium ions. Injury to the sarcomere causesdetachment of cTnI from actin and subsequentdisruption of the cellular membrane allows leakageof cTnI into the general circulation. Therefore, ahigh level of cTnI detected in serum or plasma isconsidered to be a highly sensitive and specific
indicator of myocardial cell damage and necrosis.The close homology of cTnI among mammalsallows accurate measurement in dogs and catsusing immunoassays developed for humans.
In human medicine, cardiac troponins are anintegral diagnostic criteria of acute coronarysyndromes. Elevated cTnI can be detected within3-4 hours following the onset of myocardial injuryand remain increased for 4-7 days after the initialmyocardial infarction. Chronically, heart failurepatients retain modest elevations in circulatingcTnI, which can be used to monitor progressionof disease and provides prognostic information.Elevated cTnI is associated with adverse long-termoutcome and is an independent predictor of mor-tality (13,14). It is likely that cTnI measurementin veterinary patients offers similar prognosticinformation, despite the fact that myocardialinfarction is relatively less common in dogs.
Detection of myocardialdamageCardiac troponin I immunoassays have beenvalidated in dogs (15,16). cTnI is a marker ofmyocardial necrosis and is not specific to theunderlying cause of the myocardial damage; thismeans that primary heart disease or systemicdisease that secondarily affects the heart cancause cTnI elevations. In human medicine, end-stage renal failure, sepsis, and trauma are reportedcauses of elevated values. In dogs, pyometra,gastric dilatation-volvulus (GDV), pericardialeffusion, trauma, and sepsis can cause dramaticincreases in cTnI. Myocarditis can cause 100-foldincreases in cTnI, as occurs in dogs afflicted withbabesiosis and Chagas’ disease.
Cardiac troponin can be used in conjunctionwith other diagnostics to provide prognosticinformation in cases of sepsis and GDV. In patientswith acute arrhythmias or systolic dysfunction,extreme elevation in cTnI is consistent withmyocarditis and can be a tool to monitor responseto therapy. In a small pilot study, Linklater, et al.(17) showed a decreased survival time in dogswith mitral valve disease who had elevatedcTnI and presented to the emergency hospital forcongestive heart failure. Further studies areindicated to better classify the prognostic abilityof cTnI in congenital and acquired heart disease.
BIOMARKERS IN THE DIAGNOSIS OF CANINE HEART DISEASE
Published in IVIS with the permission of the editor Close window to return to IVIS

6 / / Veterinary Focus / / Vol 18 No 3 / / 2008
1. Swedberg K, Cleland J, Dargie H, et al. Guidelines for the diagnosis andtreatment of chronic heart failure: executive summary (update 2005): TheTask Force for the Diagnosis and Treatment of Chronic Heart Failure of theEuropean Society of Cardiology. Eur Heart J 2005; 26: 1115-1140.
2. Maisel A, Bhalla V, Braunwald E. Cardiac biomarkers: a contemporarystatus report. Nat Clin Pract Cardiovasc Med 2006; 3(1): 24-34.
3. Boswood A, Dukes-McEwan J, Loureiro J, et al. The diagnostic accuracy ofdifferent natriuretic peptides in the investigation of canine cardiac disease.J Small Anim Pract 2008: 49(1): 26-32.
4. Oyama M, Fox P, Rush J, et al. Clinical utility of serum N-terminal pro-B-type natriuretic peptide concentration for identifying cardiac disease indogs and assessing disease severity. J Am Vet Med Assoc 2008; 232(10):1496-1503.
5. Fine D, Declue A, Reinero C. Evaluation of circulating amino terminal-pro-B-type natriuretic peptide concentration in dogs with respiratory distressattributable to congestive heart failure or primary pulmonary disease.J Am Vet Med Assoc 2008; 232(11): 1674-1679.
6. Oyama M, Rush J, Rozanski E, et al. NT-pro-BNP assay distinguishes cardiacvs primary respiratory causes of respiratory signs in dogs (abstr) inProceedings. 26th Annu Forum Am Coll Vet Intern Med 2008.
7. Wess G, Timper N, Hirschberger J. The utility of NT-pro-BNP todifferentiate cardiac and respiratory causes of coughing or dyspnea in dogs(abstr) in Proceedings. 25th Annu Forum Am Coll Vet Intern Med 2007.
8. Fine D, DeClue A, Reinero C. Brain natriuretic peptide for discrimination ofrespiratory distress due to congestive heart failure or primary respiratorydisease (abstr) in Proceedings. 25th Annu Forum Am Coll Vet Intern Med 2007.
9. Oyama M, Sisson D, Solter P. Prospective screening for occultcardiomyopathy in dogs by measurement of plasma atrial natriureticpeptide, B-type natriuretic peptide, and cardiac troponin-I concentrations.Am J Vet Res 2007; 68(1): 42-47.
10. Schmidt M, Reynolds C, Estrada A, et al. Effect of renal dysfunction on N-terminal pro-B-type natriuretic peptide: a canine biomarker for heart disease(abstr) in Proceedings. 26th Annu Forum Am Coll Vet Intern Med 2008.
11. Kellihan H, Oyama M, Reynolds C, et al. Weekly variability of plasma andserum NT-pro-BNP measurements in normal dogs (abstr) in Proceedings.26th Annu Forum Am Coll Vet Intern Med 2008.
12. Farace G, Beardow A, Carpenter C, et al. Effect of shipping temperature oncanine N-terminal prohormone atrial natriuretic peptide and N-terminalprohormone brain natriuretic peptide (abstr) in Proceedings. 26th AnnuForum Am Coll Vet Intern Med 2008.
13. Healey J, Davies R, Smith S, et al. Prognostic use of cardiac troponin T andtroponin I in patients with heart failure. Can J Cardiol 2003; 19(4): 383-386.
14. Peacock W, DeMarco M, Fonarow M, et al. Cardiac trtoponin and outcomein acute heart failure. N Engl J Med 2008; 358: 2117-2126.
15. Schober K, Kirbach B, Oechtering G. Noninvasive assessment ofmyocardial cell injury in dogs with suspected cardiac contusion.J Vet Cardiol 1999; 1:17-25.
16. Sleeper M, Clifford C, Laster L. Cardiac troponin I in the normal dog and cat.J Vet Intern Med 2001; 15(5): 501-503.
17. Linklater A, Lichtenberger M, Thamm D, et al. Serum concentrations ofcardiac troponin I and cardiac troponin T in dogs with class IV congestiveheart failure due to mitral valve disease. J Vet Emerg Crit Care 2007; 17(3):243-249.
18. Oyama M, Sisson D. Cardiac troponin-I concentration in dogs with cardiacdiease. J Vet Intern Med 2004; 18: 831-839.
19. Baumwart R, Orvalho J, Meurs K. Evaluation of serum cardiac troponin Iconcentration in Boxers with arrhythmogenic right ventricularcardiomyopathy. Am J Vet Res 2007; 69(5): 524-528.
REFERENCES
Diagnosis of heart diseaseOyama, et al. evaluated cTnI in 269 dogs with andwithout heart disease. They reported significantelevation in cTnI in dogs with cardiomyopathy(median 0.14 ng/mL), mitral valve disease(0.11 ng/mL), and subaortic stenosis (0.08 ng/mL),compared to healthy dogs (0.03 ng/mL). Adecreased median survival time was found indogs with cardiomyopathy and cTnI greater than0.20 ng/mL (18). In Boxers with arrhythmogenicright ventricular cardiomyopathy, cardiac troponincan be elevated (19). In another study ofDobermans, Boxers, and Great Danes with occultdilated cardiomyopathy, cTnI was significantlyincreased when compared with healthy dogs(19); however, although cTnI is elevated in manyasymptomatic dogs, the lack of specificity ofthis test makes it unlikely to be useful as a stand-alone screening test. In this instance, strategies
that combine various biomarker assays, suchas testing for both cTnI and NT-proBNP mayprovide a better diagnostic tool for asymptomaticpatients. Further studies are needed to assessthe sensitivity, specificity, and predictive valueof this combination.
ConclusionCardiac biomarkers are an exciting new tool forthe diagnosis of heart disease in dogs. NT-proBNPtests can be used to help diagnose heart diseaseand distinguish cause of respiratory signs indogs. Cardiac troponin tests reflect the severityof the underlying myocardial damage, andare likely to be correlated with prognosis. Asresearch continues and these tests become morewidely used in clinical practice, other applicationssuch as risk assessment, monitoring therapy, andprognostic ability will likely be further elucidated.
BIOMARKERS IN THE DIAGNOSIS OF CANINE HEART DISEASE
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 7
IntroductionQuantitative assessment of myocardial functionis of great importance in the diagnosis, treat-ment, and management of heart diseases andalso in the understanding of their physiopathology.Standard echocardiography is commonly per-formed on both humans and small animals tonon-invasively assess myocardial function, andseveral bidimensional (2D) and M-mode measure-ments such as systolic left ventricular diameterand index volume or fractional shortening(%FS) are often used as indices of myocardialperformance. Tissue Doppler imaging (TDI) andits derived modalities, strain (St) and strain rate(SR) imaging, are newly-developed ultrasoundtechniques permitting quantitative assessmentof myocardial function by calculating myocardialvelocities in real time (1,2) and by measuringmyocardial segmental deformation (contractionor stretching) and rate of deformation (3,4),respectively. Two-dimensional speckle tracking
Valérie Chetboul, DVM, PhD, Dipl. ECVIM-CA (Cardiology)The Cardiology Unit of the National Veterinary School of Alfort, France
Dr. Chetboul graduated in Veterinary Medicine from the National Veterinary School of Alfort in 1984. She completed a postgraduate course in university teaching at the same school and is currently working as aProfessor in Small Animal Internal Medicine and Cardiology. Valérie Chetboul also belongs to a CardiologyResearch Unit (National Institute of Health and Medical Research) attached to the Paris XII University where sheis responsible for the non-invasive cardiovascular imaging in small and large animals. She was awarded herPhD in Gene therapy in the cardiology field in 2000 from the Paris XII University and became a Diplomate ofthe European College of Veterinary Internal Medicine (Cardiology section) in 1999. Dr. Chetboul was editor-in-chief of the Journal of Veterinary Cardiology (2002-2006) and is currently co-editor of the CardiovascularImaging section of the Journal.
New echocardiographicand Doppler techniques
KEY POINTS � Tissue Doppler imaging (TDI) offers a non-invasive
and sensitive Doppler analysis of regional myocardialmotion thanks to the quantification of myocardialvelocities in real time
� The main advantage of the two-dimensional color TDImode over the pulsed-wave TDI mode and the colorTDI M-mode is its ability to simultaneously quantifymyocardial velocities in several segments within 1, 2or 3 myocardial walls
� Strain and strain rate imaging are two TDI-derivedtechniques allowing quantitative assessment ofregional myocardial deformation and rate ofdeformation, respectively
� Two-dimensional speckle tracking echocardiographyis a newly-developed ultrasound technique providinga non-Doppler assessment of regional myocardialmotion, including velocity, strain and strain rate,displacement, and also amplitude of systolic rotation
Published in IVIS with the permission of the editor Close window to return to IVIS

8 / / Veterinary Focus / / Vol 18 No 3 / / 2008
echocardiography (2D STE) is an even morerecent ultrasound modality based on 2D gray-scale echocardiographic images. This non-in-vasive technique provides a new opportunity forthe non-Doppler assessment of regional myo-cardial motion, thanks to the measurement of
various myocardial parameters including velo-city, St and SR, displacement, and also ampli-tude of systolic rotation (5-7).
Tissue Doppler imagingPhysical basics of TDI are similar to those ofconventional Doppler imaging, except the factthat TDI is based on the ability of ultrasoundinstruments to eliminate Doppler informationcoming from blood flow and to keep those fromthe myocardial wall (1). In order to display thelow velocity/high amplitude Doppler signals of themyocardium and to suppress the high velocity/lowamplitude Doppler signals of blood flow, specificadjustments of Doppler setting are requiredsuch as the suppression of high-pass filters anddecrease in gain setting (1).
TDI modesThree TDI modes are available (1). The pulsed-wave TDI mode provides information on myo-cardial movements through a single sample gate, which is placed within the myocardial wallthickness to analyze its radial or longitudinalmotion (Figure 1A). With the color M-mode(Figure 1B), myocardial velocities are analyzedalong a selected single scan line, which is placedin the same manner as for conventional trans-ventricular M-mode to analyze the radial motionof the interventricular septum (IVS) or the leftventricular free wall (LVFW). Using 2D colorTDI mode (Figure 1C), real time color Doppleris superimposed on the gray-scale of 2D modeimages and the Doppler receive gain is adjusted tomaintain optimal coloring of the myocardium.One of the main advantages of 2D color TDI modeover the two others is its ability to simultaneouslyquantify myocardial velocities in several segmentswithin 1, 2 or 3 walls, thereby allowing assessmentof intra- and interventricular myocardial synchrony(Figures 2 and 3, (8)).
Left and right normal TDI myocardial velocity profiles: the normal non-uniform aspect Radial and longitudinal LVFW velocities may bequantified with correct to good repeatability andreproducibility in small animals using the rightparasternal short axis view and the left apical4-chamber view, respectively (9,10). After a shortisovolumic contraction phase (9-14), all radial and
Figure 1. The three TDI modes: the pulsed-wave mode (1A), the colorM-mode (1B) and the two-dimensional (2D) color mode (1C).
1A: The pulsed-wave TDI mode provides information onmyocardial movements through a single sample volume,which is placed within the myocardial wall thickness. Whenthe myocardium moves towards the transducer, myocardialvelocities are positive (above the baseline). Conversely,when the myocardium moves away from the transducer,myocardial velocities are negative (under the baseline).
1B: This color M-mode TDI tracing of the left ventricular free wall(radial motion) shows on the same image both systolic anddiastolic velocities within the entire wall thickness.Myocardial velocities towards the transducer are encoded inred, and those away from the transducer in blue. Using aspecific software, the mean myocardial velocity (defined asthe average of velocity values measured along each M-modescan line throughout the myocardial wall thickness) maythen be calculated throughout the whole cardiac cycle.
1C: Using the 2D color mode, myocardial velocities aresuperimposed on 2D mode images (here right parasternaltransventricular short axis view). Velocities towards thetransducer are colored in red whereas those away from thetransducer are colored in blue. Using a specific softwaremyocardial velocities may then be analyzed within one orseveral segments (see Figure 2).
LV: left ventricle.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 9
Figure 2.
Example of normal radial velocity profiles recorded within 2 segments of the left ventricular free wall using the two-dimensionalcolor TDI mode in a healthy dog (right parasternal transventricular short axis view).
This simultaneous recording of myocardial velocities in a sub-endocardial (yellow) and sub-epicardial (green) segment indicates that thesub-endocardium is moving more rapidly than the sub-epicardium in systole and also in diastole, thus defining a marked myocardialvelocity gradient throughout the whole cardiac cycle. As with the pulsed-wave TDI mode, myocardial velocities are positive when themyocardium moves towards the transducer whereas they are negative when it moves away from the transducer. Color display of velocityis superimposed on the right parasternal transventricular short axis view (left upper panel).
A: peak myocardial velocity during late diastole. AVC: aortic valve closure. AVO: aortic valve opening. E: peak myocardial velocity duringearly diastole. IVC: isovolumic contraction phase. IVR: isovolumic relaxation phase. LV: left ventricle. S: peak myocardial velocity duringsystole.
longitudinal velocity profiles include one positivesystolic wave (S), and after a short isovolumicrelaxation phase, two diastolic negative waves(E and A, respectively in early and late diastole,Figures 2 and 4). Fusion of the two negativediastolic waves E and A into one negative diastolicwave EA is often observed in the cat due to a rapidheart rate (9).
Normal radial LVFW motion is characterized bynon-uniformity (13,14), with myocardial layersmoving more rapidly in the sub-endocardiumthan in the sub-epicardium, thus creating anintra-myocardial radial velocity gradient through-out the cardiac cycle (MVG, Figure 2). Normallongitudinal myocardial motion is also character-ized by non-uniformity (9-14), with myocardialvelocities decreasing from the base to the apex,thus producing a longitudinal MVG (Figure 4). Aphysiologic heterogeneity in the longitudinalmyocardial motion has also been demonstrated inthe normal cat between the IVS and the LVFW,with higher early diastolic velocities, acceleration,
and deceleration in the former than in the latter(15). Similarly (16), longitudinal right ventricularmyocardial (RVM) velocities have been shown to behigher at the base than the apex, and also higherthan LVFW velocities of the corresponding segment(basal or apical). This additional heterogeneitymay be explained by the difference in loadingconditions between the two ventricles, andprobably also by the differing regional myocardialfiber architecture.
Factors of variationsThe main factors of variation of TDI variables arebreed, heart rate, and anesthesia. For example,in one study (13) involving a large populationof healthy dogs (n=100), a breed effect wasdemonstrated for longitudinal S wave measuredat the base. In the dog (13), a positive correlationhas been shown between heart rate and longitudi-nal S wave at the base. A similar relationshipbetween heart rate and systolic velocities has beenreported in the cat (14), involving radial sub-endocardial and sub-epicardial S waves, as well as
NEW ECHOCARDIOGRAPHIC AND DOPPLER TECHNIQUES
Published in IVIS with the permission of the editor Close window to return to IVIS

10 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Figure 4. Example of normal longitudinal velocity profiles recorded within 2 segments of the left ventricular free wall using thetwo-dimensional color TDI mode in a healthy dog (left apical 4-chamber view).
This simultaneous recording of myocardial velocities in a basal (yellow) and apical (green) segment indicates that the base ismoving more rapidly than the apex in systole and also in diastole, thus defining a myocardial velocity gradient throughout thewhole cardiac cycle. Color display of velocity is superimposed on the left apical 4-chamber view (left upper panel).
A: peak myocardial velocity during late diastole. AVC: aortic valve closure. AVO: aortic valve opening. E: peak myocardialvelocity during early diastole. IVC: isovolumic contraction phase. IVR: isovolumic relaxation phase. LA: left atrium. LV: left ventricle.S: peak myocardial velocity during systole.
Figure 3. Example of interventricular dyssynchrony assessed by the two-dimensional color TDI mode in a dog with dilated cardiomyopathy.
The longitudinal velocity profiles obtained from 3 basal segments of the left ventricular free wall (LVFW, red), the interventricular septum(IVS, green), and the right myocardial wall (RVMW, yellow) show a delayed peak systolic LVFW velocity (arrows) compared with the2 others. Color display of velocity is superimposed on the left apical 4-chamber view (left upper panel).
S: peak myocardial velocity during systole. LA: left atrium. LV: left ventricle. RA: right atrium. RV: right ventricle.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 11
NEW ECHOCARDIOGRAPHIC AND DOPPLER TECHNIQUES
longitudinal annular and basal S waves. Onestudy performed on healthy dogs (10) showedthat anesthesia significantly decreases both radialand longitudinal myocardial velocities, up to 60%compared to values measured in awake animals.
Current applications of the TDItechnique TDI offers a non-invasive, sensitive, and quanti-tative analysis of regional myocardial motion.One of the major applications of the TDI techniqueis the detection of slight myocardial alterationsthat are equivocal or even not apparent usingconventional ultrasound techniques. Using adog model of dilated cardiomyopathy (DCM),our group demonstrated (17) that TDI is moresensitive than conventional echocardiographyin detecting preclinical regional myocardialabnormalities before occurrence of left ventriculardilation and overt systolic dysfunction (Figure 5).Similarly, in a feline model of hypertrophic cardio-
myopathy, TDI has been shown to consistentlydetect LVFW dysfunction despite the absence ofmyocardial hypertrophy in affected males and incarrier females (18).
TDI may also be used to accurately investigatemyocardial dysfunction associated with heartdiseases, thus providing new insights in theunderstanding of their pathophysiology. Forexample, diastolic dysfunction has traditionallybeen thought to be the only abnormality incats with HCM. One study using the 2D colorTDI mode showed that systolic dysfunction is anadditional component of myocardial alteration(19). Such a systolic dysfunction is characterizedby a decrease in longitudinal systolic velocitiesand gradients (despite normal or increasedfractional shortening) and the high prevalenceof post-systolic contraction waves (Figure 6).A recent study performed by another group usingthe pulsed-wave TDI mode confirmed these
Figure 5.
Example of abnormal radial velocity profiles recorded within 2 segments of the left ventricular free wall using the two-dimensionalcolor TDI mode in a young Golden Retriever dog with muscular dystrophy (right parasternal transventricular short axis view).
The sub-endocardial (yellow) and sub-epicardial (green) velocity profiles are nearly superimposed in systole, thus indicating a verylow systolic myocardial velocity gradient (double arrows, for comparison see normal radial velocity profiles in Figure 2). This TDIsystolic dysfunction was not detected using conventional echocardiography (fractional shortening of 38%, i.e., within the normalranges). Color display of velocity is superimposed on the right parasternal transventricular short axis view (left upper panel).
A: peak myocardial velocity during late diastole. AVC: aortic valve closure. AVO: aortic valve opening. E: peak myocardialvelocity during early diastole. IVC: isovolumic contraction phase. IVR: isovolumic relaxation phase. LV: left ventricle. RV: right ventricle.S: peak myocardial velocity during systole.
Published in IVIS with the permission of the editor Close window to return to IVIS

12 / / Veterinary Focus / / Vol 18 No 3 / / 2008
results, demonstrating a systolic impairmentalong the longitudinal axis of the LVFW in catswith HCM (15).
Another important TDI application is the assess-ment of a treatment effect on myocardial function.For example, our group has recently used the TDItechnique to demonstrate the beneficial regionalsystolic myocardial effect of non-cultured skeletalmuscle cell transplantation in an animal modelof non-ischemic DCM (20).
Strain and strain rate imaging St and SR imaging are two TDI-based techniquesthat complete the TDI analysis by measuringmyocardial segmental deformation and rate ofdeformation, respectively. Both Doppler techniqueshave been shown to be repeatable and reproduciblemethods for assessing systolic radial and longi-tudinal LVFW function, and also systolic longi-
tudinal function of the IVS and the RVM in theawake dog (4). Myocardial St represents the de-formation of a myocardial segment over time(3,4) and is expressed as the % of change fromits original dimension (Figure 7A). MyocardialSR is the temporal derivative of St (3,4) and ismeasured in s-1 (Figure 7B). SR describes the rateof myocardial deformation, that is, how quickly
Figure 6. Example of abnormal longitudinal velocity profiles recordedwithin 2 segments of the left ventricular free wall using thetwo-dimensional color TDI mode in a cat with hypertrophiccardiomyopathy (left apical 4-chamber view).
Note that E is lower than A in the basal segment (yellow curve),thus confirming a diastolic dysfunction. Moreover, the apicalvelocity curve (green curve) shows post-systolic contraction waves(green arrows), which were confirmed using strain imaging.
A: peak myocardial velocity during late diastole. E: peakmyocardial velocity during early diastole. S: peak myocardialvelocity during systole.
Figure 7. Example of normal regional radial strain (7A) and strain rate (7B)profiles recorded within the left ventricular free wall in a healthydog (right parasternal transventricular short axis view).
The radial strain profile (expressed in %) is positive and maximalin end-systole (arrows), and then decreases during diastole, thusconfirming a regional systolic expansion (i.e., thickening) and adiastolic compression (i.e., shortening), respectively (7A). Thestrain rate profile (expressed in s-1) is positive during systole (SRS)indicating a regional thickening and then features 2 negativediastolic peaks during early filling and atrial contraction (SRE andSRA) corresponding to a biphasic thinning phase. Color display ofstrain and strain rate are superimposed on the right parasternaltransventricular short axis views (left upper panels of Figures 7Aand 7B, respectively). Strain length = 12 mm. Region of interestsize = 3/3 mm.
AVC: aortic valve closure. AVO: aortic valve opening. LV: leftventricle.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 13
NEW ECHOCARDIOGRAPHIC AND DOPPLER TECHNIQUES
Figure 8.
Example of an abnormal regional longitudinal strain profile recorded within the right ventricular myocardial wall in a dog withpulmonary arterial stenosis (left apical 4-chamber view).
The longitudinal strain profile is negative, thus confirming a regional compression (i.e., myocardial shortening) during systole. However,the maximal negative strain value is measured after T wave on the ECG tracing, i.e., in diastole instead of systole. These post-systoliccontraction waves (PSC) confirm a marked right myocardial systolic dysfunction. This systolic dysfunction is also characterized by apeak systolic strain (arrows) lower than the published reference ranges (4). Color display of velocity is superimposed on the leftventricular 4-chamber view (left upper panel). Strain length = 12 mm. Region of interest size = 6/3 mm.
AVC: aortic valve closure. AVO: aortic valve opening. RA: right atrium. RV: right ventricle.
a myocardial segment shortens or lengthens.Therefore, compared to TDI, St and SR imagingoffer true measures of local myocardial deform-ation, thereby separating active from passivemyocardial motion (3,4). Conversely, myocardialvelocities assessed by TDI do not discriminatebetween actively contracting myocardium andpassive motion due to heart translation andtethering effects. Regional systolic St and SR havealready been shown to be powerful and sensitivenon-invasive indices of myocardial contractility(Figure 8), and these indices have also beensuggested to be sensitive and effective measures ofmyocardial synchrony (3,8).
However, St and SR imaging present severalmajor limitations resulting in a high risk of mis-interpretation. These include angle dependency(as for the TDI technique), a low signal to noise ratio(particularly for SR imaging), and many types ofartifacts due to stationary reverberations, drop-out zones, and low lateral resolution. Theseartifacts may create false regional myocardial
akinesia or dyskinesia. St and SR curves shouldtherefore always be interpreted carefully by atrained observer while taking into account both thealignment with the ultrasound beam and the locationof the sample area throughout the cardiac cycle.Myocardial segments with obvious artifacts shouldalways be excluded from post-processing analysis.
Two-dimensional speckletracking echocardiography2D STE is the most recent ultrasound techniquedeveloped in cardiology to assess regionalmyocardial function concomitantly in severalsegments (5-7). The 2D STE principle is based onthe formation of speckle patterns due to reflection,scattering, and interferences between tissueand ultrasound beams in routine grayscale 2Dechocardiographic images (5-7). These specklesappear as small, bright elements homogeneouslydistributed within the myocardium on 2D modeimages. They represent natural acoustic tissuemarkers that can be tracked from frame to framethroughout the cardiac cycle. Thus 2D STE allows
Published in IVIS with the permission of the editor Close window to return to IVIS

14 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Figure 9. Example of normal left ventricular (LV) rotation profiles recorded within 6 apical myocardial segments using two-dimensionalspeckle tracking echocardiography in a healthy dog (right parasternal apical short axis view).
The software algorithm has automatically defined 6 equidistant myocardial segments within the interventricular septum and theLV free wall. Figure 9 shows on the right the 6 corresponding LV apical rotation versus time curves, and the orange dotted line theaveraged LV rotation versus time curve of the 6 segments. As seen from the apex, the 6 myocardial segments go through ahomogenous systolic wringing motion with an initial clockwise rotation (negative rotation) followed by a dominantcounterclockwise rotation (positive rotation). This may also be observed on 2D color-coded views (left) showing a clockwise (red)and then counterclockwise (blue) rotation in early and end-systole (ES), respectively.
a non-Doppler assessment of regional myocardialmotion (velocity, rotation, St, and SR) by filteringout these random speckles, and then performingautocorrelations to evaluate the motion of stablestructures.
One of the major advantages of 2D STE comparedto the Doppler-based techniques, such as TDI orTDI-derived techniques (St and SR imaging), is itsindependence of both cardiac translation andinsonation angle. When the latter are used, anincorrect alignment between the ultrasound beamand the myocardial wall motion may lead tosubstantial errors (underestimation of velocity,St, and SR), which is not the case with 2D STE.Another advantage of 2D STE is that it offers directmeasures of myocardial displacement, whereaswith Doppler-based techniques, all measurementsare done in reference to an external point, e.g., thetransducer.
Our group has shown that 2D STE is a repeatableand reproducible method for assessing radial LV
St and SR in the awake dog. Moreover, thesenon-Doppler measurements correlate well withthose obtained by the TDI-based techniques,at least in normal myocardial segments (6).However, which of these techniques is actuallythe best (particularly the most sensitive forthe detection of myocardial dysfunction) stillremains unknown.
Another study (7) demonstrated that 2D STEprovides also a repeatable and reproducible non-invasive assessment of the systolic LV wringingmotion in the awake dog (Figure 9). Peak LVbasal and apical systolic rotations and systolicglobal LV torsion, defined as apical rotationrelative to the base, have been shown to bealtered in dogs with hypokinesia (7). Similaralterations of the LV systolic wringing motionalso have been identified in humans with variousheart diseases (DCM and myocardial infarction)and could contribute to a certain extent to thereduction in stroke volume in these pathologicsettings.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 15
1. Chetboul V. Tissue Doppler Imaging: a promising technique forquantifying regional myocardial function. J Vet Cardiol 2002; 4: 7-12.
2. Uematsu M, Miyatake K, Tanaka N, et al. Myocardial velocity gradientas a new indicator of regional left ventricular contraction: detection bya two-dimensional tissue Doppler imaging technique. J Am Coll Cardiol1995; 26: 217-223.
3. D’hooge J, Heimdal A, Jamal F, et al. Regional strain and strain ratemeasurements by cardiac ultrasound: principles, implementation andlimitations. Eur J Echocardiography 2000; 1: 154-170.
4. Chetboul V, Carlos Sampedrano C, Gouni V, et al. Ultrasonographicassessment of regional radial and longitudinal systolic function inhealthy awake dogs. J Vet Intern Med 2006; 20: 885-893.
5. Helle-Valle T, Crosby J, Edvardsen T, et al. New noninvasive method forassessment of left ventricular rotation: speckle trackingechocardiography. Circulation 2005; 112: 3149-3156.
6. Chetboul V, Serres F, Gouni V, et al. Radial strain and strain rate bytwo-dimensional speckle tracking echocardiography and the tissuevelocity based technique in the dog. J Vet Cardiol 2007; 9: 69-81.
7. Chetboul V, Serres F, Gouni V, et al. Non-invasive assessment of systolicleft ventricular torsion by 2-dimensional speckle tracking imaging in theawake dog: repeatability, reproducibility, and comparison with tissueDoppler imaging variables. J Vet Intern Med 2008; 20: 885-893.
8. Estrada A, Chetboul V. Tissue Doppler evaluation of ventricularsynchrony. J Vet Cardiol 2006; 8: 129-137.
9. Chetboul V, Athanassiadis N, Carlos Sampedrano C, et al.Quantification, repeatability, and reproducibility of feline radial andlongitudinal left ventricular velocities by tissue Doppler imaging.Am J Vet Res 2004; 65: 566-572.
10. Chetboul V, Athanassiadis N, Carlos Sampedrano C, et al. Assessmentof repeatability, reproducibility, and effect of anesthesia ondetermination of radial and longitudinal left ventricular velocities viatissue Doppler imaging in dogs. Am J Vet Res 2004; 65: 909-915.
11. Koffas H, Dukes-McEwan J, Corcoran BM, et al. Peak mean myocardialvelocities and velocity gradients measured by color M-mode tissueDoppler imaging in healthy cats. J Vet Intern Med 2003; 17: 510-524.
12. Gavaghan BJ, Kittleson MD, Fisher KJ, et al. Quantification of leftventricular diastolic wall motion by Doppler tissue imaging in healthycats and cats with cardiomyopathy. Am J Vet Res 1999; 60: 1478-1486.
13. Chetboul V, Carlos Sampedrano C, Concordet D, et al. Use ofquantitative two-dimensional color tissue Doppler imaging forassessment of left ventricular radial and longitudinal myocardialvelocities in dogs. Am J Vet Res 2005; 66: 953-961.
14. Chetboul V, Carlos Sampedrano C, Tissier R, et al. Quantitativeassessment of velocities of the annulus of the left atrioventricular valveand left ventricular free wall in healthy cats by use of two-dimensionalcolor tissue Doppler imaging. Am J Vet Res 2006; 67: 250-258.
15. Koffas H, Dukes-McEwan J, Corcoran BM, et al. Pulsed tissue Dopplerimaging in normal cats and cats with hypertrophic cardiomyopathy.J Vet Intern Med 2006; 20: 65-77.
16. Chetboul V, Carlos Sampedrano C, Gouni V, et al. Quantitativeassessment of regional right ventricular myocardial velocities in awakedogs using Doppler tissue imaging: repeatability, reproducibility, effectof body weight and breed, and comparison with left ventricularmyocardial velocities. J Vet Intern Med 2005; 19: 837-44.
17. Chetboul V, Escriou C, Tessier D, et al. Tissue Doppler imaging detectsearly asymptomatic myocardial abnormalities in a dog model ofDuchenne's cardiomyopathy. Eur Heart J 2004; 25: 1934-1939.
18. Chetboul V, Blot S, Carlos Sampedrano C, et al. Tissue Dopplerimaging for detection of radial and longitudinal myocardialdysfunction in a family of cats affected by dystrophin-deficienthypertrophic muscular dystrophy. J Vet Intern Med 2006; 20: 640-647.
19. Carlos Sampedrano C, Chetboul V, Gouni V, et al. Systolic and diastolicmyocardial dysfunction in cats with hypertrophic cardiomyopathy orsystemic hypertension. J Vet Intern Med 2006; 20: 1106-1115.
20. Borenstein N, Chetboul V, Bruneval P, et al. Non-cultured celltransplantation in an ovine model of non-ischemic heart failure.Eur J Cardiothorac Surg 2007; 31: 444-451.
NEW ECHOCARDIOGRAPHIC AND DOPPLER TECHNIQUES
REFERENCES
Similarly to the other three ultrasound methods, 2DSTE presents several technical limitations, includ-ing the failure to obtain reliable STE measure-ments mostly because of reverberation artifactsand drop-outs, and also because of the use of short-axis images (6). Regarding the latter, longitudi-nal myocardial motion may cause speckles to movein or out of the image plane, thereby decreasingthe reliability and the possibility of the speckletracking process.
ConclusionThe recent development of Doppler imagingtechniques, such as TDI, St and SR imaging, offersa new opportunity for the non-invasive assessmentof regional myocardial function in small animals.
The non-Doppler technique, 2D STE, may providea complement or alternative to the TDI and TDI-based techniques to quantify myocardial synchronyand also to assess the complex pattern of regionalmyocardial motion including the LV wringingmotion. The combined use of these imagingindices, whose repeatability and reproducibilityare adequate for routine clinical use, providesadditional information beyond that obtained fromconventional echocardiography. Further studiesare now required in large populations of diseasedpatients to determine the comparative clinicalrelevance of these new imaging variables, and theirpotential additive value with regards to prognosisand therapeutic implications.
Published in IVIS with the permission of the editor Close window to return to IVIS

16 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Suzanne Cunningham, DVM, Dipl. ACVIM(Cardiology)Department of Clinical Sciences, Tufts CummingsSchool of Veterinary Medicine, North Grafton, USA
Dr. Cunningham is a Clinical Professor of Cardiology atTufts Cummings School of Veterinary Medicine in NorthGrafton, MA. She received her DVM from CornellUniversity in 2003 and completed a Small AnimalMedicine internship, and residency in Cardiology at Tufts Cummings School of Veterinary Medicine. Suzanne Cunningham recently became a Diplomate of the American College of Veterinary Internal Medicinein Cardiology. Her current research interests includeinterventional cardiology and investigation of noveltherapies for cardiomyopathy and congestive heart failure.
John Rush, DVM, MS, Dipl. ACVIM(Cardiology), Dipl. ACVECC
Department of Clinical Sciences, Tufts Cummings,School of Veterinary Medicine, North Grafton, USA
Dr. Rush is Professor at the Tufts Cummings School ofVeterinary Medicine in North Grafton, MA. He is a
Diplomate of the American College of Veterinary InternalMedicine in Cardiology and also a Diplomate of the
American College of Veterinary Emergency and CriticalCare. He obtained his DVM and Master’s Degree from
the Ohio State University, completed an internship at theAnimal Medical Center in New York, and did a residency
at the University of Wisconsin-Madison. Dr. Rush has anumber of publications in the fields of cardiology and
emergency and critical care medicine.
Interventionalcardiovascular
procedures
IntroductionThe advent of minimally invasive, catheter-basedinterventions has revolutionized the treatment ofcardiovascular disease in people and transcatheterinterventions are becoming more commonplace inveterinary medicine. Transcatheter proceduresallow for the correction of several congenital andacquired cardiac defects without the attendantmorbidity and mortality associated with surgery.Since the first balloon valvuloplasty was performedin a Bulldog in 1980, the scope of interventionalprocedures has expanded to include myriad noveltechniques. Interventional procedures are nowcommonly used for the successful treatment ofpatent ductus arteriosus, pulmonic stenosis, atrio-ventricular valve stenoses, vascular stenoses, atrialand ventricular septal defects, heartworm disease,and life-threatening bradyarrhythmias, conditionsthat were once treatable only with considerablesurgical morbidity and mortality. The focus of
this paper is to introduce the most common inter-ventional procedures available for the treat-ment of congenital and acquired cardiovasculardiseases in companion animals.
Patent ductus arteriosusPatent ductus arteriosus (PDA) is one of the mostcommon congenital heart defects in the dog, butis uncommon in the cat. Failure of ductus closureresults in left-to-right shunting with resultantpulmonary overcirculation, cardiac enlargement,pulmonary vascular injury, and congestive heartfailure (CHF) that typically develops by one yearof age. Typical diagnostic findings in left-to-rightshunting PDA include a continuous cardiac mur-mur at the left heart base and hyper-dynamicarterial pulses. Thoracic radiographs demonstratepulmonary overcirculation. Echocardiographicfindings typically reveal a volume overload tothe left heart and continuous turbulent blood flow
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 17
Figure 1.
Stainless steel embolization coils of varying sizes. Thrombus formation is stimulated by the synthetic Dacron fibers embedded within the coils.
in the main pulmonary artery originating fromthe junction of the ductus arteriosus. Due to thehigh likelihood of progression to CHF, closure ofthe PDA is recommended in virtually all cases.
Transcatheter PDA occlusion provides a minimallyinvasive alternative to open surgical ligation,circumventing the need for thoracotomy and itsattendant surgical morbidity. While successfulin experienced hands, surgical PDA ligationvia thoracotomy carries the risk of catastrophichemorrhage due to tearing of the ductus andsurgical mortality has been reported to rangefrom 4 to 10%. Transcatheter PDA occlusion maybe achieved by coil embolization or deploymentof various self-expanding devices designed forhuman patients (1) or dogs (2).
Coil occlusion entails the transcatheter delivery ofembolization coils into the ductal lumen (Figure 1).The coils are made of metal (e.g., stainless steela)and are manufactured to retain a helical structureafter deployment from the catheter. Enmeshedwithin the coils are synthetic Dacron fibers,which stimulate thrombus formation. The PDAis most commonly accessed from the ascendingaorta using femoral arterial access. Selectiveangiography allows delineation of ductal anatomyand measurement of the minimal ductal diameterto determine the feasibility of coil occlusion andallow selection of appropriately sized coils. Whendeployed within the target vessel, the resultingthrombus formation results in occlusion of ductalflow (Figure 2). Successful coil deployment istypically achieved in 85-90% of coil embolizationattempts, with complete occlusion of ductal flowoccurring in at least 60% of patients assessed oneyear after occlusion (3). Dogs with persistent flowthrough the PDA following coil occlusion generallyhave hemodynamically insignificant residual shuntvolumes and infrequently require a second proce-dure to achieve complete occlusion (3). Risks in-herent in coil embolization include hemorrhage,great vessel perforation, infection, hemolysis andmost commonly, embolization of coils to thepulmonary or systemic circulation. Pulmonaryembolization of 1-2 small to medium sized coils isgenerally well-tolerated and retrieval of coils inthe pulmonary circulation is generally unnecessaryand ill-advised. Successful coil embolization ofPDA from a retrograde transvenous approachhas also been described in the cat (4).
Coil embolization is more difficult to achievein dogs with large PDA and those that lack a
Figure 2.
Lateral selective angiograms in a young female Papillon with apatent ductus arteriosus (PDA). In the left hand panel contrast isinjected in the descending aorta and blood flow is documentedthrough the PDA and into the main pulmonary artery. Theangiogram in the right hand panel was obtained followingdeployment of a coil in the PDA and confirms complete occlusionof ductal flow.
Published in IVIS with the permission of the editor Close window to return to IVIS

18 / / Veterinary Focus / / Vol 18 No 3 / / 2008
narrowing at the junction of the ductus and thepulmonary artery. Coil occlusion of PDA measuring>0.5 cm in minimal ductal diameter has been dis-couraged by some veterinary cardiologists. Variousself-expanding devices allowing transcatheterocclusion of large PDA have been devised for usein human patients and a canine-specific deviceb hasrecently become commercially available (Figure 3).Initial experience with this device has been verypromising, with successful occlusion of large PDAand immediate complete occlusion rates reportedat 94% (2) (Figure 4), compared to immediateocclusion rates of 34% with coil embolizationtechniques (3).
Pulmonic stenosisPulmonic stenosis, another common congenitalcardiac defect in the dog, may occur at subvalvular,valvular or supravalvular locations. Valvularstenosis, characterized by dysplastic pulmonaryvalve leaf lets that are thickened, fused andimmobile, is the most common manifestationof the disease and is also the most amenable toballoon valvuloplasty. Dogs with pulmonic stenosistypically exhibit a loud systolic ejection murmur atthe left heart base and variable degrees of rightventricular (RV) hypertrophy. Disease severityis gauged by the Doppler echo-derived pressuregradient across the pulmonic valve, in combinationwith the degree of RV hypertrophy, right atrial
enlargement, tricuspid valve regurgitation, and thepresence or absence of either cardiac arrhythmiasor clinical signs. Dogs with gradients acrossthe pulmonic valve of <50 mmHg are typicallyconsidered to have mild disease and may remainasymptomatic without intervention. However, dogswith severe disease (Doppler gradient >100 mmHg)are likely to manifest signs of right-sided CHF,arrhythmias, syncope or sudden death, warrantingpreemptive treatment with surgery or valvuloplasty.Balloon valvuloplasty is the current treatment ofchoice in these dogs to prevent or ameliorateclinical signs.
Pulmonic balloon valvuloplasty entails inflationof a balloon dilation catheter engaged withinthe pulmonary annulus at the level of stenosis(Figure 5). The balloon size is dictated by thediameter of the pulmonary annulus and aorta andthe balloon width chosen is typically 1.2 to 1.4times the diameter of the pulmonary annulus, orthe approximate diameter of the normal aorticannulus (5). In smaller dogs it may be difficult topass an introducer or dilation catheter of sufficientdiameter through the jugular or femoral vein and adouble balloon procedure may be elected wherebytwo smaller balloon catheters from both the jugularand femoral locations are inflated simultaneouslyto allow for a greater effective balloon diameter (5).
The best candidates for valvuloplasty are those dogswith dysplastic pulmonary valve leaflets and anormal pulmonary annulus size. Dogs with a fibrous
Figure 3.
A self-expanding multi-layered nitinol mesh device used forocclusion of patent ductus arteriosus (PDA) is shown fullydeployed from the delivery catheter. During actual deployment,the delivery catheter is advanced through the aorta and PDA andpositioned in the main pulmonary artery. The flat distal disc isfirst deployed into the pulmonary artery, and then the deliverycatheter is gently retracted into the PDA to engage the distal discwith the pulmonary ostium of the PDA. The proximal disc is thendeployed within the ductal lumen and the device is then releasedfrom the delivery cable.
Figure 4.
Post-operative right lateral thoracic radiograph of an adult femaleSpringer Spaniel with cardiac enlargement and patent ductusarteriosus (PDA). A double-disc nitinol mesh canine ductalocclusion device has been deployed within the PDA. This dog hadcomplete elimination of PDA flow and resolution of congestiveheart failure following device placement.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 19
subvalvular ring and those with concurrent hypo-plasia of the pulmonary annulus (characterizedby an aorta-to-pulmonary artery ratio of >1.2)may have a more uncertain outcome (6). Bulldogs,Boxers and other breeds (e.g. Beagle, Bichon Frisé)may have pulmonic stenosis complicated by thepresence of an abnormal coronary artery (the R2Acoronary anomaly), in which a single right coronaryartery gives rise to a branch that encircles the RVoutflow tract, and balloon valvuloplasty of thislesion may result in fatal hemorrhage secondary toavulsion of the circumpulmonary coronary artery(7). Up to 20% of dogs with pulmonic stenosis mayhave a concurrent atrial septal defect or patentforamen ovale, which can result in hypoxemia dueto increased right-to-left shunting during balloonvalvuloplasty. In order to identify these potentialcomplicating lesions, cardiac and coronary anatomyshould be carefully scrutinized by echocardiographyand/or selective angiography prior to balloonvalvuloplasty. The overall reported success rate ofthe procedure exceeds 90%, resulting in a 46%immediate mean reduction in pressure gradient andsustained clinical improvement in 80% of previouslysymptomatic dogs (8).
Subaortic stenosisAortic stenosis most often results from subvalvularobstruction secondary to a ridge of fibrous tissue inthe left ventricular outflow tract. Valvular aorticstenosis is uncommon in the dog. Typical clinicalfindings include a loud systolic ejection qualitymurmur heard well at the left and right heartbase, weak arterial pulses, and a prominent leftventricular (LV) apical impulse. The stenoticlesion results in a pressure overload to the LVand characteristic echocardiographic findings ofconcentric LV hypertrophy often associated withhyperechoic regions of the papillary muscles andsubendocardium, a reflection of tissue hypoxia,ischemia, and resultant fibrosis. This myocardialinjury and hypoxia may also result in electrocardio-graphic abnormalities such as LV enlargementpatterns, ST segment depression and ventriculararrhythmias. The severity of subaortic stenosis(SAS) is also categorized, in part, according to themeasured echocardiographic Doppler gradientacross the aortic valve. Severely affected dogs withtransvalvular aortic pressure gradients exceeding 80to 100 mmHg may develop cardiac arrhythmias,bacterial endocarditis of the aortic valve, syncope,left-sided CHF or sudden death. The natural historyof subaortic stenosis includes sudden death in at least1 out of 5 severely affected dogs, and the averagesurvival time of dogs with severe SAS has beenreported to range from 19 months to 56 months (9).
Balloon valvuloplasty is less successful in thetreatment of aortic stenosis compared to pulmonicstenosis. Although the procedure may yield animmediate reduction in the aortic outflow gradient,one retrospective analysis of severely affected dogsshowed no difference in survival times betweendogs treated with valvuloplasty compared to thosemanaged medically with atenolol, a beta-blocker(9). Reasons for the failure of valvuloplasty toconsistently benefit dogs with severe SAS arepoorly understood, but a report of dogs withSAS undergoing open surgical resection of thesubaortic fibrous ring also failed to show anybenefit of this procedure on survival times (10).
To date, there have been no studies to establishwhether earlier intervention at several months ofage, or combined valvuloplasty and beta-blockertreatment would improve clinical outcomes. Thus,while many cardiologists routinely administer
Figure 5.
Lateral fluoroscopic images during pulmonic balloon valvuloplastyof a 7-month-old female Boxer with valvular pulmonic stenosis. Atransesophageal echo (TEE) probe is evident within the esophagusand the round structure in the lower left hand corner of the imageis a dime used to standardize cardiac measurements. A guidewirecan be seen traversing the right atrium and right ventricle andentering the main pulmonary artery. The balloon dilation catheteris positioned across the region of the stenotic pulmonic valve inboth figures. In the left hand panel the indentation noted in thepartially inflated balloon is created by the stenotic pulmonaryvalve leaflets. In the right hand panel the balloon is fully inflatedand the indentation in the balloon is no longer apparent. Valvularstenosis was successfully relieved with a 65% reduction intransvalvular pressure gradient following 3 sequential ballooninflations.
INTERVENTIONAL CARDIOVASCULAR PROCEDURES
Published in IVIS with the permission of the editor Close window to return to IVIS

20 / / Veterinary Focus / / Vol 18 No 3 / / 2008
atenolol to affected dogs, it has also been ourpractice to selectively choose certain dogs foraortic balloon valvuloplasty. Those dogs with acomponent of valvular aortic stenosis, and thosewith a thin fibrous subaortic ring and limitedmuscular hypertrophy of the interventricularseptum are offered balloon valvuloplasty, andwe are much more likely to be enthusiasticabout the procedure in young dogs, before markedremodeling and fibrosis of the left ventricle havedeveloped. In our experience, it is easier to engagethe subaortic ring if 2 smaller balloons are usedrather than trying to relieve the obstruction with asingle balloon. Balloon dilation of the aortic valve isassociated with greater risk and often results inmore serious arrhythmia than that encounteredduring pulmonic balloon valvuloplasty.
Atrial septal defectsAtrial septal defects (ASD) are relatively un-common defects, though a genetic predispositionhas been noted in the Boxer, Doberman Pinscher,Samoyed and Standard Poodle. Typical physicalexamination findings accompanying ASD mayinclude a systolic ejection murmur of functionalpulmonic stenosis and fixed splitting of thesecond heart sound. Though small ASD may behemodynamically insignificant, large left-to-right shunting defects may result in right-sidedvolume overload with attendant right atrial and
ventricular enlargement, pulmonary hypertension,increased right atrial filling pressures, and theeventual development of right-sided CHF. Surgicalcorrection of ASD requires cardiopulmonary bypassand is associated with significant risk and expense.Successful transcatheter closure of secundum ASDshas been reported in the dog using a self-expandingdouble-disk septal occluder devicec (11,12) (Figure6). Transthoracic and transesophageal echocardio-graphic assessment of ASD anatomy are crucial indetermining the size and location of the defect andensuring that there is a sufficient rim of interatrialseptal tissue to support the device while avoidinginterference with surrounding cardiac structures.Animals with Eisenmenger’s physiology, characteri-zed by severe pulmonary hypertension and a largeright-to-left-shunting atrial or ventricular septaldefect, are not candidates for surgical or trans-catheter closure of the defect.
Ventricular septal defectsVentricular septal defects (VSD) are amongst themost common congenital defects in the cat, and apredisposition for VSD has been described in theEnglish Springer Spaniel, Keeshound and EnglishBulldog. Ventricular septal defects are associatedwith a loud systolic heart murmur, often mostprominent on the right chest wall at the right cranialsternal border. The degree of cardiomegaly andpulmonary overcirculation accompanying VSDdepends upon the size of the defect and the relativecompliance of the right and left ventricles. Smallrestrictive VSD are often hemodynamicallyunimportant and may be well-tolerated for the lifeof the animal. However large defects may resultin considerable left-to-right shunting with left-sided volume overload and chamber enlargement,pulmonary vascular damage, and left-sided CHF.Surgical palliation of large VSD may includecorrection of the defect under cardiopulmonarybypass or circumferential banding of the mainpulmonary artery to reduce the volume of left-to-right shunting. The surgical risk to the patient andthe post-operative discomfort of thoracotomy maybe reduced if the repair can be accomplishedwith a percutaneous approach.
Transcatheter occlusion of suitable defects is thetreatment of choice for human patients with VSDand has been described in the dog. Catheter-basedocclusion of small VSD in the dog has been reported
Figure 6.
Right parasternal long axis transthoracic echocardiographic viewfrom a dog with an atrial septal defect (ASD). An atrial septaloccluder device has been positioned across the interatrial septumand can be noted as the bright hyperechoic double disc structurebetween the right atrium (RA) and left atrium (LA). LV = leftventricle, RV = right ventricle. Picture courtesy of Texas A&MUniversity.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 21
using detachable embolization coils (13). Largenonrestrictive VSD located an adequate distancefrom the aortic valve in the muscular septum may becandidates for VSD occlusion with a double-diskseptal occluderd (14) (Figure 7). Transesophagealechocardiography is necessary to determine thefeasibility of VSD occlusion with a percutaneousdevice. Unfortunately, VSD located high in themembranous septum are both more common indogs and cats and more difficult to treat, since theopen device may interfere with either aortic ortricuspid valve function. A membranous VSDoccluder has recently been designed for use inhuman patients, and this device may prove to beapplicable to a larger number of veterinary patients.Ventricular septal defect occlusion with the currentlyavailable VSD occlusion device sizes is not feasiblein the cat.
Tricuspid stenosisTricuspid stenosis is an uncommon congenitaldefect characterized by a diastolic pressure gradientbetween the right atrium and ventricle, right atrialenlargement, atrial arrhythmias and eventual right-sided congestive heart failure. Tricuspid valvestenosis typically accompanies tricuspid dysplasia,a heritable disorder in the Labrador Retriever. Inthe absence of concurrent valvular insufficiency,affected dogs often have soft or absent cardiacmurmurs and the disease may go unnoticed untilclinical signs develop. Percutaneous balloonvalvuloplasty of the tricuspid valve with a singleor double balloon procedure (Figure 8) may beaccomplished by jugular or femoral venousaccess and valvuloplasty may result in a significantreduction in the pressure gradient across the valve,with attendant improvements in hemodynamicsand clinical signs (15).
Mitral stenosisMitral valve dysplasia and stenosis (MS) is anuncommon congenital defect with breedpredilections in the Newfoundland and Bull Terrier.Affected dogs typically exhibit signs of exerciseintolerance, syncope and congestive heart failureand most dogs with MS do not survive beyond 2-3 years of age (16). Percutaneous mitral valvuloplastyis the treatment of choice for human patients withsymptomatic MS. This procedure is more difficultto accomplish than other valvuloplasties due tothe need for trans-septal puncture to access theleft atrium, and has only been reported once inthe dog (17). Valvular and supravalvular mitralstenosis have also been described in the cat butmitral valvuloplasty has not been described inthis species.
Figure 8.
Lateral fluoroscopic images of a young Labrador Retrieverwith tricuspid dysplasia and valvular tricuspid stenosis. Balloonvalvuloplasty was performed on the stenotic tricuspid valveutilizing a double balloon technique. Two guidewires are evidentwithin the cranial vena cava, right atrium, right ventricle andpassing into the pulmonary artery. Two balloon dilation cathetershave been passed over the guidewires and are seen positionedacross the tricuspid orifice. In the left hand panel, a waist createdby the stenotic tricuspid valve leaflets is seen across the mid-portion of the simultaneously inflated balloons. In the right handpanel the balloons are fully inflated and resolution of the balloonwaist demonstrates effective dilation of the stenosis.
Figure 7.
Right lateral thoracic radiograph of a dog 1 year followingpercutaneous device occlusion of a muscular VSD. The VSDocclusion device can be seen deployed across the interventricularseptum. Picture courtesy of Dr. Marco Margiocco.
INTERVENTIONAL CARDIOVASCULAR PROCEDURES
Published in IVIS with the permission of the editor Close window to return to IVIS

22 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Cor triatriatumCor triatriatum dexter and cor triatriatum sinisterare characterized by a perforate or imperforatefibrous membrane partitioning the respective rightor left atrium into a proximal and distal atrialchamber. Clinical manifestations depend on thelocation of the membrane and the size of thecommunication between the proximal and distalchambers. The resultant increase in filling pressurein the proximal chamber results in signs of CHF.Cor triatriatum dexter may be palliated by percutan-eous balloon dilation of the anomalous membraneto reduce the pressure gradient between theproximal and distal chambers of the right atrium(18). Balloon dilation of cor triatriatum sinisteris also feasible with transseptal puncture to accessthe left atrium, but has not been described incompanion animals.
Congenital and acquired cavalstenosisVena caval stenosis or stricture formation may occuras a congenital defect or may be acquired secondaryto endothelial injury from cardiovascular devicesor central venous catheters. The functional conse-quences of caval stenosis depend on the locationand severity of the stenosis, and percutaneoustreatment of symptomatic stenoses may be achievedwith balloon angioplasty or intravascular stenting.
Congenital stenosis of the caudal vena cava andBudd-Chiari syndrome caused by an intraluminalfibrous membrane has been described in the cat(19). Affected cats often develop severe ascitesdue to impedance of venous return from the caudalvena cava. In one report, treatment of an affectedcat with balloon dilation and endovascular stentplacement failed to resolve the cat’s ascites and wasassociated with a poor outcome (19). However,the authors have performed successful balloondilation of an obstructive intraluminal mem-brane in the caudal vena cava of one cat thatpresented with severe refractory ascites, result-ing in complete resolution of clinical signs thathad persisted for greater than 15 months (Figure9). We have also performed successful balloonvenoplasty in two dogs with cranial vena cavasyndrome and pleural effusion due to acquiredstenosis and thrombosis of the cranial vena cavasecondary to transvenous pacemaker leads.
Supraventricular tachycardiaassociated with accessory pathwaysAccessory atrioventricular (AV) conductionpathways, or bypass tracts, are abnormal electricalcommunications across the fibrous skeletonthat normally serves to electrically isolate theatria and ventricles. The accessory pathway mayfunction as one limb of a rapid, narrow complextachyarrhythmia circuit termed orthodromicatrioventricular reciprocating tachycardia (OAVRT).Vagal maneuvers and adenosine, both effectivein human patients with OAVRT, are generallyineffective in terminating OAVRT in the dog andthe response of reciprocating tachycardias toantiarrhythmic drug therapy is inconsistent,with affected dogs often becoming refractoryto previously effective antiarrhythmic strategies.Unrelenting tachycardia results in reduced cardiacoutput and will eventually result in the develop-ment of tachycardiomyopathy and congestiveheart failure if left untreated.
Radiofrequency catheter ablation utilizes analternating electrical current to induce thermaldamage to the accessory pathway and is thestandard of care for human patients withmacroreentrant tachycardias. The procedure is alsohighly effective for eliminating accessory pathwayconduction in the dog (20) however it is onlyperformed in a limited number of specializedcenters due to the need for highly specialized
Figure 9.
Selective venogram of a young castrated male domestic shorthaired cat with Budd-Chiari syndrome and massive ascitessecondary to an obstructive membrane within the caudal venacava at the level of the diaphragm. In the left hand panel thecatheter has been advanced from the femoral vein and positionedin the caudal vena cava just caudal to the diaphragm. Contrast isseen to fill the dilated cava and only a small stream of contrastcan be seen passing through the membrane and into the cavacranial to the diaphragm (c). In the right hand panel a balloonhas been advanced across the membrane and is inflated. Ascitesresolved following balloon dilation of the stenosis in this cat.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 23
equipment and expertise. Electroablation entailsthe placement of several multipolar electrodecatheters into the right atrium, followed byelectrical mapping to determine the exact locationof the accessory pathway. Radiofrequency energyis then delivered to the accessory pathway throughthe catheter tip electrode, resulting in thermal-induced damage to the pathway and ablation ofimpulse conduction. Electroablation is also used forthe treatment of atrial fibrillation and atrial flutterin human patients and has potential for greaterapplication for treatment of these arrhythmias inthe dog.
Bradyarrhythmias and cardiacpacingHigh degree second-degree and third-degreeatrioventricular (AV) block are associated withsigns of exercise intolerance, syncope, cardiacenlargement, and a high incidence of suddencardiac death (21). Pacemaker therapy is the onlytreatment effective in alleviating clinical signsand prolonging survival in affected dogs, andpacemaker implantation is the current standard ofcare for patients with high grade AV block, atrialstandstill, and sick sinus syndrome. Since theadvent of epicardial pacing in the dog in 1967,transvenous pacing has become widespread andhas largely replaced the surgical placement ofepicardial leads in dogs (Figure 10).
Permanent transvenous cardiac pacing can beachieved using a wide variety of pacing modalities,including the use of one or more pacemakerleadwires. Single-chamber permanent transvenouspacing is used most frequently in the dog and isachieved by passing the leadwire through a vein,usually the jugular vein, and advancing the leadthrough the right atrium and into the rightventricle. Most pacemaker lead systems now allowfor active fixation of an endocardial lead in the rightventricular myocardium, reducing the chancefor leadwire dislodgement. The pulse generator isimplanted beneath the skin, and the pacing modeand rate, amplitude and pulse width of the pacingstimulus, and a variety of more advanced featurescan be subsequently adjusted via an externalprogrammer. Many pacemakers have a sensor thatdetects vibration and allows for rate modulationwith increased activity. Although a variety ofcomplications can occur following pacemakerimplantation, such as lead fracture or dislodge-ment, infection, battery failure or developmentof congestive signs in patients with intercurrentstructural cardiac disease, the vast majority of dogs(over 90%) do well and never have recurrenceof clinical signs related to the cardiac brady-arrhythmia (22). The average survival of dogsfollowing pacemaker implantation is at least 2 yearsand many dogs live in excess of 3 to 5 years afterpacemaker implantation (21,22).
Dual chamber physiologic pacing allows forpreservation of atrioventricular synchrony and isutilized extensively in human patients, althoughit is associated with increasing pacemakerprogramming complexity. Acute beneficial hemo-dynamic and neurohormonal changes have beendemonstrated with physiologic pacing modalitiesin the dog (23) but the long-term benefits of dualchamber pacing in veterinary patients remainuncertain. Implantable cardioverter defibrillators(ICD) are devices used extensively in humanpatients to prevent sudden cardiac death secondaryto life-threatening tachyarrhythmias such asventricular tachycardia and fibrillation. Suddenarrhythmic cardiac death is encountered frequentlyin some dog breeds (e.g., Boxer, DobermanPinscher) and ICD technology has great potentialapplication in these patients, however the currentICD devices designed for humans are not well-adapted to use in the dog (24).
Figure 10.
Right lateral thoracic radiograph of an elderly female CockerSpaniel with high-grade second-degree AV block followingpermanent transvenous pacemaker implantation. The pacing leadcan be seen passing through the cranial vena cava and rightatrium into the right ventricular apex where it is actively fixatedinto the right ventricular myocardium.
INTERVENTIONAL CARDIOVASCULAR PROCEDURES
Published in IVIS with the permission of the editor Close window to return to IVIS

24 / / Veterinary Focus / / Vol 18 No 3 / / 2008
1. Smith PJ, Martin MW. Transcatheter embolisation of patent ductus arteriosususing an Amplatzer vascular plug in six dogs. J Small Anim Pract 2007; 48:80–86.
2. Nguyenba TP, Tobias AH. Minimally invasive per-catheter patent ductusarteriosus occlusion in dogs using a prototype duct occluder. J Vet InternMed 2008; 22: 129-134.
3. Campbell FE, Thomas WP, Miller SJ, et al. Immediate and late outcomes oftransarterial coil occlusion of patent ductus arteriosus in dogs. J Vet InternMed 2006; 20: 83–96.
4. Schneider M, Hildebrandt N. Transvenous embolization of the patent ductusarteriosus with detachable coils in 2 cats. J Vet Intern Med 2003; 17: 349-353.
5. Estrada A, Moïse NS, Renaud-Farrell S. When, how and why to perform adouble ballooning technique for dogs with valvular pulmonic stenosis.J Vet Cardiol 2005; 7: 41–51.
6. Bussadori C, DeMadron E, Santilli RA, et al. Balloon valvuloplasty in 30 dogswith pulmonic stenosis: Effect of valve morphology and annular size oninitial and 1-year outcome. J Vet Intern Med 2001; 15: 553-558.
7. Buchanan JW. Pathogenesis of single right coronary artery and pulmonicstenosis in English Bulldogs. J Vet Intern Med 2001; 15: 101-104.
8. Stafford-Johnson M, Martin M. Results of balloon valvuloplasty in 40 dogswith pulmonic stenosis. J Small Anim Pract 2004; 45: 148-153.
9. Meurs KM, Lehmkuhl LB, Bonagura JD. Survival times in dogs with severesubvalvular aortic stenosis treated with balloon valvuloplasty or Atenolol.J Am Vet Assoc 2005; 227: 420-424.
10. Monnet E, Orton EC, Gaynor JS. Open resection for subvalvular aorticstenosis in dogs. J Am Vet Med Assoc 1996; 209: 1255-1261.
11. Sanders RA, Hogan DF, Green III HW, et al. Transcatheter closure of anatrial septal defect in a dog. J Am Vet Assoc 2005; 227: 430-434.
12. Gordon SG, Miller MW. Percutaneous ASD repair in dogs. In: ProceedingsAmerican College of Veterinary Internal Medicine Forum, Seattle, WA, 2007.
13. Fujii Y, Fukuda T, Machida N, et al. Transcatheter closure of congenitalventricular septal defects in 3 dogs with a detachable coil.J Vet Intern Med 2004; 18: 911–914.
14. Margiocco ML, Bulmer BJ, Sisson DD. Percutaneous occlusion of amuscular ventricular septal defect with an Amplatzer® Muscular VSDoccluder. J Vet Cardiol 2008; 10: 61-66.
15. Kunze CP, Abbott JA, Hamilton SM, et al. Balloon valvuloplasty forpalliative treatment of tricuspid stenosis with right-to-left atrial-levelshunting in a dog. J Am Vet Assoc 2002; 220: 491-496.
16. Lehmkuhl LB,Ware WA, Bonagura JD. Mitral stenosis in 15 dogs.J Vet Intern Med 1994; 8: 2-17.
17. Oyama MA, Weidman JA, Cole SG. Calculation of pressure half-time.J Vet Cardiol 2008; 10: 57-60.
18. Johnson MS, Martin M, De Giovanni JV, et al. Management of cortriatriatum dexter by balloon dilatation in three dogs. J Small Anim Pract2004; 45: 16-20.
19. Holt D, Saunders HM, Aronson L. Caudal vena cava obstruction and ascitesin a cat treated by balloon dilation and endovascular stent placement.Vet Surg 1999; 28: 489-495.
20. Wright KN, Knilans TK, Irvin HM. When, why, and how to perform cardiacradiofrequency catheter ablation. J Vet Cardiol 2006; 8: 95-107.
21. Wess G, Thomas WP, Berger DM. Applications, complications, andoutcomes of transvenous pacemaker implantation in 105 dogs (1997-2002).J Vet Intern Med 2006; 20: 877-884.
22. Johnson MS, Martin MWS, Henley W. Results of pacemaker implantationin 104 dogs. J Small Anim Pract 2007; 48: 4-11.
23. Bulmer BJ, Sisson DD, Oyama MA, et al. Physiologic VDD versusnonphysiologic VVI pacing in canine 3rd-degree atrioventricular block.J Vet Intern Med 2006; 20: 257-271.
24. Nelson OL, Lahmers S, Schneider T, et al. The use of an implantablecardioverter defibrillator in a boxer dog to control clinical signs ofarrhythmogenic right ventricular cardiomyopathy. J Vet Intern Med 2006;20: 1232-1237.
REFERENCES
Additional interventional proceduresand future directions Many other minimally invasive therapies arecurrently employed for the treatment of acquiredcardiovascular disease in small animals. Theseinclude transjugular heartworm removal forpatients with advanced heartworm disease,catheter placement for local thrombolytic therapy,thrombectomy for the treatment of arterial andvenous thromboembolism, endomyocardial biopsytechniques, and pulmonary artery catheterizationfor measurement of cardiac output, pulmonaryartery and pulmonary capillary wedge pressures.
Mitral regurgitation secondary to endocardiosisis the most common cardiac disease of dogs andthe most important cause of CHF. Despite recentadvances in medical therapy, the average survival
of dogs with CHF is still less than 1-year afterdiagnosis. Various percutaneous techniques areunder investigation for the treatment of mitralregurgitation in human patients, many ofthem employing animal models. A successfulpercutaneous therapy for mitral regurgitationwould have a tremendous impact for the treat-ment of endocardiosis in the dog.
Interventional cardiology is a developing fieldthat has yet to reach its full potential in veterinarymedicine. Catheter-based procedures have resultedin successful alternatives to reduce surgicalmorbidity and mortality in small animal patients.As the technology advances we will continue todevelop novel strategies for the minimally invasivetreatment of congenital and acquired cardiovasculardisease in companion animals.
Footnotes:a Cook Stainless Steel Embolization Coils, Cook Medical Inc, Bloomington, IN
b Amplatz Canine Duct Occluder (ACDO), Infiniti Medical, Malibu, CA c Amplatzer Septal Occluder, AGA Medical Corp, Golden Valley, MN
d Amplatzer Muscular VSD occluder, AGA Medical Corp, Golden Valley, MN
INTERVENTIONAL CARDIOVASCULAR PROCEDURES
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 25
Acquired valvular heart disease in the dog isthe most common cause of heart diseaseand heart failure in the canine population
(1). Valvular heart disease in the dog is usually achronic degenerative condition which is knownby various terms including endocardiosis andmyxomatous mitral valve disease. The disease mostcommonly affects the mitral valve and results in thedevelopment of mitral regurgitation. This mitralregurgitation leads to an increased volume ofblood being pumped by the left ventricle due tothe proportion of each ventricular ejection that goesback into the left atrium. Chronically this results inincreased left ventricular and left atrial size and, insome affected animals, results in the developmentof clinical signs of heart failure. It typically affectsolder small breed dogs although certain breeds of
dog, particularly Cavalier King Charles Spaniels,appear to have a higher prevalence of disease andan earlier onset of both disease and clinical signs.
In patients that are regularly examined byveterinarians the characteristic left-sided systolicmurmur of mitral insufficiency is usually the firstclinical abnormality identified. The developmentof a murmur often precedes the development ofclinical signs by many years. In the SVEP study(2) Cavalier King Charles Spaniels with a heartmurmur and no cardiac enlargement had a medianperiod of well over three years before developingsigns of heart failure. In a recent paper Borgarelli,et al. (3) showed that in a more mixed populationof asymptomatic dogs with mitral regurgitationfewer than 50% of the dogs died as a consequenceof their disease during the period of follow-up.Thus in some cases mitral valve disease can be arelatively benign slowly progressive conditionthat does not progress sufficiently to lead to thedevelopment of clinical signs. In others the diseasemay progress to the point where clinical signs ofheart failure result. The challenge for the clinicianfaced with patients with this disease is to establisha diagnosis of the disease, recognize at which stageof this progressive disease the patient in questioncurrently resides and to appropriately and optimallytreat those patients that require treatment.
A diagnosis of mitral regurgitation can be suspectedin any dog with a left apical systolic murmur, parti-cularly if it is a small breed dog. There are somelarge breed dogs that are affected by primarymitral valve disease but this is a rarer form of thedisease. Large breed dogs with primary valvulardisease may have a slightly different course ofdisease compared to small breed dogs (4).
Adrian Boswood, MA, VetMB, DVC,Dipl. ECVIM (Cardiology), MRCVSDepartment of Veterinary Clinical Sciences, The Royal Veterinary College, London, UKDr. Boswood graduated from The University of Cambridgein 1989. In 1990, following a period in general practice, he joined the Royal Veterinary College as an intern andremained at the Royal Veterinary College ever since wherehe is now a Senior Lecturer. Adrian Boswood’s mainclinical interest is in medical cardiology and his researchinterests are in cardiac biomarkers and valvular heartdisease of dogs.
Valvular heart disease in the dog
HOW I TREAT...
Published in IVIS with the permission of the editor Close window to return to IVIS

26 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Confirmation of the diagnosis of primary valvulardisease requires two-dimensional and Dopplerechocardiography but the clinical presentation isso typical, and the disease so common, that thisis not a test that is necessary to perform in everycase. Thoracic radiographs are particularly use-ful for determination of the stage of disease bydemonstrating the presence or absence of cardio-megaly and the presence or absence of left-sidedcongestive heart failure (Figure 1).
Left apical systolic murmurs may also be caused bycongenital heart disease and mitral regurgitationsecondary to other causes including dilatedcardiomyopathy and bacterial endocarditis. Theseconditions are however less commonly encounteredand tend to occur in different types of dog.
For the purposes of this article, I will discuss onlythe chronic management of patients with heartfailure and not describe the acute management ofpatients with sudden onset of severe heart failure.The UK trade names and doses of all the drugsmentioned appear in Table 1. I will divide patientsinto four stages and discuss the treatment optionsthat are appropriate at each stage in the light ofwhat I consider to be current best evidence.
These stages are as follows:• Early disease: the patient without clinical signs
and without significant cardiomegaly.• Moderately progressed disease: A patient without
overt clinical signs but with evidence ofcardiomegaly implying the necessity to adapt tothe increased volume of blood being encounteredby both the left atrium and ventricle.
• Heart failure: A patient that has developed signsof congestive heart failure as a consequence oftheir mitral valve disease. Typically the first signsof heart failure will be left-sided failure and willinclude pulmonary congestion and edema.
• Refractory heart failure: A patient that hasredeveloped clinical signs despite receivingtherapy for heart failure.
Treatment of the patient withmitral regurgitation according tothe stage of diseaseEarly diseaseThere is little evidence to suggest the benefit of anytherapy in the early stages of mitral valve disease.Two published studies have evaluated the efficacyof treatment with angiotensin converting enzymeinhibitors (ACEI) in this population (2,5). Thesestudies produced conflicting results. The study byKvart, et al. was a double-blind placebo controlledprospective study performed only in Cavalier KingCharles Spaniels (2). This study suggested thatthere was no benefit of administration of ACEI indogs prior to the onset of clinical signs irrespectiveof whether there was any cardiomegaly. The morerecent study by Pouchelon, et al. (5) is a retrospec-tive study conducted in a small but more hetero-geneous population of dogs (Editor’s note: 141dogs). The conclusion of the paper was that Bena-zepril administered in dogs with early diseasemay be of benefit in dogs of breeds other thanCavalier King Charles Spaniels. The fact that thiswas a retrospective, unblinded study with a lowevent rate (a low number of animals in the studyreached the endpoints of cardiac death or onsetof heart failure) and with different median follow-up periods for the treated and untreated groupsmean that the conclusions should be interpretedwith some caution. I would regard their conclu-sions as generating a useful hypothesis thatshould be tested in future in a placebo controlled,double-blind study and I am not yet convinced ofthe value of early therapy in this group.
Figure 1.
A lateral thoracic radiograph from a dog with advancedmitral valve disease. There is marked cardiomegaly withcraniocaudal widening of the cardiac silhouette and dorsaldisplacement of the trachea. The lung fields are diffuselyopacified by the presence of an alveolar pattern indicatingthe presence of pulmonary edema, in this case secondary toleft-sided congestive heart failure. This is a severe exampleof the radiographic changes that can be associated withadvanced mitral valve disease.
HOW I TREAT...
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 27
My approach to this population of dogs is notto intervene pharmacologically but to adviseand educate the client. If the animal is overweightthen weight control is important. Continuingto regularly exercise the patient is in my opinionprobably of benefit. There is no convincingevidence to suggest a benefit of sodium restrictionat this stage of the disease. Clients should beadvised about the signs that might indicatethe development of heart failure and the necessityfor treatment; such as exercise intolerance,increased respiratory rate and effort, cough,lethargy and unexplained weight loss. Regularre-examination of these patients may help pick upearly signs of clinical deterioration and will alsoreassure the client that one is not simply ignoringthe presence of a clinically significant disease.Client reassurance is important at the early stage ofthe disease because over-stressing the likelihoodof development of problems in the near future maycause unnecessary worry. Many dogs remain at the
early stage of mitral valve disease for many yearsand some will succumb to non-cardiac diseasebefore they have ever had the opportunity todemonstrate signs of heart failure.
Moderately progressed diseaseTwo studies have evaluated the effects of ACEI indogs with cardiomegaly prior to the onset of signs ofheart failure these are the SVEP study (2) andthe VETPROOF study (6). Both of these studiesevaluated the effect of treatment prior to theonset of clinical signs in dogs with mitral valvedisease. Some of the dogs in the SVEP study hadcardiomegaly and left atrial enlargement was one ofthe inclusion criteria for the VETPROOF study –therefore all the dogs in this study had some degreeof cardiac enlargement. Again these studies appearto generate conflicting conclusions. The SVEPstudy showed no benefit of ACEI therapy withrespect to delaying the onset of heart failure inCavalier King Charles Spaniels. The VETPROOF
Table 1. Proprietary names and doses of drugs
Generic drug name
Enalapril
Benazepril
Pimobendan
FrusemideFurosemide
Spironolactone
Digoxin
Amlodipine
Hydralazine
Sildenafil
Theophylline
Etamiphylline Camsylate
Terbutaline
Butorphanol
Codeine
Dose and frequency (These doses may differ fromthose given in the data sheet)
0.5 mg/kg s.i.d.-b.i.d.
0.25-0.5 mg/kg s.i.d.-b.i.d.
0.2-0.6 mg/kg/day divided into two doses
1-2 mg/kg b.i.d. initially increasing to a maximum of4 mg/kg t.i.d.
1-3 mg/kg b.i.d.
0.22 mg/m2 b.i.d. check trough (8 hour post pill)serum digoxin levels after 5-7 days to ensuretherapeutic and not excessive concentrations havebeen achieved
0.05-0.1 mg/kg s.i.d.-b.i.d.
0.5-3.0 mg/kg b.i.d.-t.i.d. (start with low dose andtitrate to effect with blood pressure monitoring)
0.5-3.0 mg/kg s.i.d.-t.i.d.
20 mg/kg s.i.d.
10–33 mg/kg t.i.d. (according to data sheet)
1.25-5 mg/dog b.i.d.-t.i.d.
0.5 mg/kg b.i.d.-q.i.d.
0.5-2 mg/kg b.i.d.
Proprietary names and doses ofdrugs described in the text. Thedoses may differ from those given inthe data sheets. No responsibility is accepted foradverse reactions to the drugs givenat the dosages recommended andveterinarians are recommended tocross reference to other sources (e.g.BSAVA Small Animal Formulary)prior to administration.
Abbreviations used: s.i.d. oncedaily, b.i.d. twice daily, t.i.d. threetimes daily, q.i.d. four times daily,mg milligram, kg kilogram, m2 metersquared.
VALVULAR HEART DISEASE IN THE DOG
Published in IVIS with the permission of the editor Close window to return to IVIS

28 / / Veterinary Focus / / Vol 18 No 3 / / 2008
HOW I TREAT...
study did not show a significant effect of Enalaprilon the primary endpoint of the study which wastime to onset of congestive heart failure. Lookingat a secondary combined endpoint of all causemortality and onset of heart failure they appearedto show a significant difference after excludingthose dogs that succumbed in the first 60 days ofthe study. This was not a pre-planned analysis butgenerates a fascinating hypothesis that there maybe a non-cardiac beneficial effect on survival. Thecombination of results from these two studies is notenough to currently convince me of the benefit oftherapy even in dogs with cardiomegaly at the timeof diagnosis.
It is worth pointing out that only ACEI have beenevaluated as potentially beneficial treatment priorto the onset of clinical signs in large well conductedstudies. There are of course other candidates forearly treatment that have not been evaluated asrigorously and all that one can say with respect toother therapy is “we don’t know”. It may be in thefuture that some therapy is proved to be beneficialat this stage in the disease but at the moment if weare to practice “evidence-based medicine” there isinsufficient evidence of a convincing benefit oftherapy for me to advocate its use.
A recent, as yet unpublished study, has claimed abenefit of Spironolactone prior to the onset ofsigns of heart failure however the absence of fulldisclosure of the results of this study throughpublication precludes further evaluation of thisclaim and it has not as yet changed my practice ofnot treating these patients.
Again my management of patients and theirowners at this stage of the disease consists ofeducation and monitoring. It is important thatsigns of heart failure are recognized as and whenthey occur so that treatment can be introducedwhen it is known to be effective. Clients can beinstructed in how to take a respiratory rate at homeand should also be advised to look out for subtlesigns of intolerance of exercise. Having said thisit is still the case that many dogs with mitralregurgitation and cardiomegaly live for yearsbefore developing signs of heart failure so over-stressing the likelihood of development of signsmay lead to anxiety on the part of clients andplenty of “false alarms”.
Onset of heart failureThe onset of congestive heart failure is bestdocumented with thoracic radiographs. When apatient has developed signs of congestive heartfailure secondary to mitral valve regurgitation thereis convincing evidence of benefit of therapy bothin terms of improvement of quality of life and,with some treatments, prolongation of life. Severalcontrolled studies have been conducted from whichvalid conclusions on which to base our therapy canbe drawn. There are multiple studies that havedemonstrated the benefits of ACEI in the treatmentof dogs with mitral valve disease. The LIVE study(7) and the BENCH study (8) were two of the earlierstudies published. These showed that compared toplacebo ACEI prolonged survival of dogs in heartfailure when added to standard therapy of diureticsplus in some cases digoxin and other drugs. Thesestudies both enrolled populations of dogs includingthose with mitral regurgitation. A sub-analysis ofthe LIVE study (7) showed benefit specifically in thegroup with mitral regurgitation. Thus ACEI arebetter than placebo in the treatment of dogs in heartfailure secondary to mitral valve disease.
More recently Pimobendan has been shown tobe efficacious. Mitral valve disease studies havedemonstrated improvements in quality of lifeand time to events such as hospitalization areimproved with Pimobendan (9). The VetSCOPEstudy suggested that the beneficial effects ofPimobendan may exceed those of ACEI (10)although substantial debate remained after theconclusion of this study. The recently reportedQUEST study (11), a positive controlled, single-blind, prospective study comparing Benazeprilto Pimobendan concluded that the benefits ofPimobendan exceeded those of Benazepril (andby inference probably other ACEI) with a 91%prolongation of the time to reach a composite end-point of death, euthanasia for cardiac reasons ortreatment failure (Figure 2). This study suggeststhat if either an ACEI or Pimobendan is to be usedin isolation, in conjunction with diuresis and othertreatments, then Pimobendan is the preferredagent. What it does not enable us to conclude iswhether not the combination of an ACEI andPimobendan will be better still. There is also recent,as yet unpublished, evidence of a benefit ofSpironolactone in dogs with mitral regurgitationand signs of heart failure.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 29
0
0
100
10
20
30
40
50
60
70
80
90
100
200 300 400 500 600 700 800 900 1000 1100
The way I treat patients at this stage dependsto some extent on client preference and thefeasibility of administering multiple medicationsin these patients. The optimum treatment couldconsist of up to four medications. What is not indoubt is the necessity for the administration ofFrusemide to patients with congestive heartfailure. Therefore the two, three and four drugregimes would be:
• Frusemide plus Pimobendan• Frusemide plus Pimobendan plus ACEI; or• Frusemide plus Pimobendan plus ACEI plus
Spironolactone.
Where minimum therapy is dictated for eitherfinancial reasons or risks of poor compliance thenthe two drug regime will suffice. Optimal therapymay involve administration of either the three orfour drug regime although evidence of additionalbenefit of these therapies when added to the twodrug regime is currently lacking. However, theopinion is widely held among cardiologists thatthere are additional benefits.
Refractory heart failureOnce a patient is receiving optimal therapyfollowing the onset of signs of heart failure thereis often a period of several months when the patientis fairly stable and compensates for their heartfailure (provided they continue to receive theirtreatment). Unfortunately, for most dogs therereaches a point where their clinical signs returndespite receiving treatment and modificationof treatment is necessary. Modification shouldconsist of optimization of doses of drugs alreadybeing received plus the addition of further treat-ment. In this late stage of disease there is a lackof evidence of efficacy of any particular therapy anda plethora of individual opinion. If a patient is onlyreceiving two or three of the drugs outlined in thedifferent regimes above I would add the othersto ensure that all four of Frusemide, Pimobendan,an ACEI and Spironolactone are being receivedby the patient. In addition to this combinationthere is the option to add further diuretics, furthervasodilators and/or Digoxin to the treatment;the latter particularly where patients have atrialfibrillation.
Figure 2.
Kaplan Meier survival analysis from the QUEST study. The median time to reaching the primary endpoint was 267 days in thePimobendan group compared to 140 days in the Benazepril group suggesting a 91% prolongation of time to cardiac death,euthanasia for cardiac reasons or treatment failure in the group receiving Pimobendan.
Log-Rank Test, P=0.0099
Pimobendan group267 days, IQR 122-523 days
Benazepril group140 days, IQR 67-311 days
Dog
s re
mai
nin
g in
stu
dy (
%)
Time (Days)
VALVULAR HEART DISEASE IN THE DOG
Published in IVIS with the permission of the editor Close window to return to IVIS

30 / / Veterinary Focus / / Vol 18 No 3 / / 2008
I undertake the following modifications to treat-ment:• Increase the Frusemide dose and frequency up
to a maximum of 4 mg/kg three times daily. • Maximize the Spironolactone dose up to
2-3 mg/kg twice daily. • Double the frequency of the ACEI administration
(going from once daily to twice daily).
After this one can consider addition of furtherdiuretics, particularly thiazide diuretics as these actelsewhere within the nephron (sequential nephronblockade) and further vasodilators includingAmlodipine and Hydralazine. If patients developsigns of right-sided congestive heart failure thesemay be secondary to the development of pulmonaryhypertension. Some authors have advocated theuse of Sildenafil in these circumstances (12).
There are many risks associated with the admin-istration of multiple drugs to patients with advancedvalvular heart disease; the most frequently seencomplications include compromised renal func-tion and electrolyte disturbances (13). I wouldrecommend checking a biochemistry profile inpatients with mitral regurgitation prior to intro-duction of treatment and 7-10 days after anysignificant modification to therapy. In the laterstages of disease it is almost inevitable that somedegree of azotemia will develop. Provided this ismodest then therapy can be continued but in somecircumstances the creation of concurrent renaldysfunction can be a limiting factor in the abilityto administer further therapy.
Ultimately the majority of patients that developsigns of heart failure secondary to mitral re-gurgitation will succumb to their disease (75%of dogs in the QUEST study reached the primaryendpoint (11)), despite further attempts at therapy.In many cases it is necessary to consider euthanasiaand the decision to undertake this should be in-formed by the quality of life enjoyed by the patienton treatment and client preferences.
Additional problemsThere are two problems relating to the aboveclassification. One is the artificial sense of certaintyit creates about dogs fitting into one of thecategories rather than hovering on the boundaries.The second problem relates to the clinical sign of
intractable coughing that occurs in many dogswith valvular heart disease.
Any type of categorization of disease artificiallydivides a continuous spectrum of patients intoa series of apparently distinct categories. There isoften a problem with dogs lying on the boundariesbetween categories. There is an artificial level ofcertainty associated with a patient either havingor not having signs of heart failure. In some patientsit is difficult to judge, for instance in patientswith moderate to marked intolerance of exercise,or patients with evidence of a mild interstitial lungpattern radiographically: are these patients in heartfailure or not? It may be that in the future the useof biomarkers may help us to distinguish dogsthat are more or less likely to be showing signs ofheart failure and NTproBNP appears promising inthis respect (14,15). See also first paper in thisissue by M. Oyama and C. Reynolds. Sometimeshowever it is necessary to consider, where clinicalsigns and radiography or echocardiographysuggest the disease is advanced, the introductionof empirical therapy to see if signs will improve.This strategy can sometimes be fraught withuncertainty because concurrent disease couldbe responsible for the signs that might eitherimprove in response to the same therapy or simplyresolve with time. Thus an apparent response totherapy is a tenuous reason to condemn a dog tolifelong therapy. It is very unlikely that a dogwith a relatively quiet heart murmur that doesnot have evidence of cardiac enlargement will beshowing any clinical signs as a consequence oftheir disease.
Coughing is one very specific clinical sign in dogswith mitral valve disease that may be a consequenceof the disease but not necessarily a sign of heartfailure. It is widely believed that the cough indogs with mitral valve disease, which frequentlyprecedes signs of heart failure, is due to thephysical size of the enlarged left atrium leadingto compression of the left mainstem bronchus.In this circumstance treatment aimed at controllingsigns of congestive heart failure may not lead toa resolution of the signs of coughing becausethey do not necessarily reduce the size of the leftatrium. Various strategies have been suggestedin these patients in an effort to improve signs.These can all be tried in these patients but,
HOW I TREAT...
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 31
1. Buchanan JW. Prevalence of Cardiovascular Disorders. In: Fox PR, SissonD, Moise NS, eds. Textbook of Canine and Feline Cardiology. Philadelphia:Saunders, W.B.; 1999: 457-470.
2. Kvart C, Haggstrom J, Pedersen HD, et al. Efficacy of enalapril forprevention of congestive heart failure in dogs with myxomatous valvedisease and asymptomatic mitral regurgitation. J Vet Intern Med 2002;16: 80-88.
3. Borgarelli M, Savarino P, Crosara S, et al. Survival characteristics andprognostic variables of dogs with mitral regurgitation attributable tomyxomatous valve disease. J Vet Intern Med 2008; 22: 120-128.
4. Borgarelli M, Zini E, D'Agnolo G, et al. Comparison of primary mitral valvedisease in German Shepherd dogs and in small breeds. J Vet Cardiol 2004;6: 27-34.
5. Pouchelon JL, Jamet N, Gouni V, et al. Effect of benazepril on survivaland cardiac events in dogs with asymptomatic mitral valve disease: Aretrospective study of 141 cases. J Vet Intern Med 2008; 22: 905-914.
6. Atkins CE, Keene BW, Brown WA, et al. Results of the veterinary enalapriltrial to prove reduction in onset of heart failure in dogs chronically treatedwith enalapril alone for compensated, naturally occurring mitral valveinsufficiency. J Am Vet Med Assoc 2007; 231: 1061-1069.
7. Ettinger SJ, Benitz AM, Ericsson GF, et al. Effects of enalapril maleateon survival of dogs with naturally acquired heart failure. The Long-TermInvestigation of Veterinary Enalapril (LIVE) Study Group. J Am Vet MedAssoc 1998; 213: 1573-1577.
8. BENCH, Pouchelon JL, Martignoni L, et al. The effects of benazepril onsurvival times and clinical signs of dogs with congestive heart failure:Results of a multicenter, prospective, randomized, double-blinded,placebo-controlled, long-term clinical trial. J Vet Cardiol 1999; 1: 7-18.
9. Smith PJ, French AT, Van Israel N, et al. Efficacy and safety of pimobendanin canine heart failure caused by myxomatous mitral valve disease.J Small Anim Pract 2005; 46: 121-130.
10. Lombard CW, Jons O, Bussadori CM. Clinical efficacy of pimobendanversus benazepril for the treatment of acquired atrioventricular valvulardisease in dogs. J Am Anim Hosp Assoc 2006; 42: 249-261.
11. Häggström J, Boswood A, O'Grady M, et al. Effect of pimobendan versusbenazepril hydrochloride on survival times in dogs with congestive heartfailure due to naturally occurring myxomatous mitral valve disease:Results of the QUEST study. J Vet Intern Med 2008 Jul 11 (in press).
12. Bach JF, Rozanski EA, MacGregor J, et al. Retrospective evaluation ofsildenafil citrate as a therapy for pulmonary hypertension in dogs.J Vet Intern Med 2006; 20: 1132-1135.
13. Boswood A, Murphy A. The effect of heart disease, heart failure anddiuresis on selected laboratory and electrocardiographic parameters indogs. J Vet Cardiol 2006; 8: 1-9.
14. Boswood A, Dukes-McEwan J, Loureiro J, et al. The diagnostic accuracyof different natriuretic peptides in the investigation of canine cardiacdisease. J Small Anim Pract 2008; 49: 26-32.
15. Oyama MA, Fox PR, Rush JE, et al. Clinical utility of serum N-terminalpro-B-type natriuretic peptide concentration for identifying cardiac diseasein dogs and assessing disease severity. J Am Vet Med Assoc 2008; 232:1496-1503.
16. Troughton RW, Frampton CM, Yandle TG, et al. Treatment of heart failureguided by plasma aminoterminal brain natriuretic peptide (N-BNP)concentrations. The Lancet 2000; 355: 1126-1130.
17. Lainchbury JG, Troughton RW, Frampton CM, et al. NTproBNP-guideddrug treatment for chronic heart failure: design and methods in the"BATTLESCARRED" trial. Eur J Heart Fail 2006; 8: 532-538.
VALVULAR HEART DISEASE IN THE DOG
despite the use of many or all of these, the coughfrequently proves unresponsive to treatment.Strategies for treatment include:• Bronchodilation: Theophylline, Etamiphylline
and Terbutaline could be considered.• Management changes: Weight loss, avoidance of
smoky dusty environments, use of a harnessrather than a collar to prevent further irritationto the airways.
• Introduction of low doses of vasodilators ordiuretics: the rationale behind this approach isto try to physically reduce left atrial size.
• Cough suppressants: Butorphanol or Codeinecan be used intermittently to suppress the coughwhen it is particularly problematic.
• Anti-inflammatory medication: some authorsadvocate the use of intermittent low dosecorticosteroids or steroids by inhaler in thesecircumstances.
Future directionsOne recent exciting development that may havesignificant ramifications for the identification andmanagement of heart disease in dogs with mitral
valve disease (and other cardiac diseases) is thedevelopment of assays for cardiac biomarkers(See article on page 2). The measurement ofNTproBNP seems particularly promising. Severalrecent studies have outlined the value of thismarker in the identification of patients withheart disease and heart failure (14,15). In humanpatients assessment of biomarkers can assist inboth the identification of patients with moreadvanced disease and decisions with regard totheir therapy. There are also prognostic impli-cations of elevated levels of NTproBNP in humanpatients; preliminary data from dogs would alsosuggest that there is a strong predictive associationbetween NTproBNP concentration and outcome.
It is conceivable that in future we may be able toinitiate therapy with more confidence in patientswith mitral valve disease that have elevatedconcentrations of NTproBNP. The potential forspecifically targeting a reduction of natriureticpeptide concentrations in humans is already beingexplored (16,17) and this is an avenue worthy offurther evaluation in dogs.
REFERENCES
Published in IVIS with the permission of the editor Close window to return to IVIS

32 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Accurate and timely diagnosis of earlystage (Class 1 & 2, Table 1) cardiacdisease historically has been difficult.
Most patients show no outward evidence of beingsick. Owners themselves usually do not reportclinical signs related to a cardiac abnormalityuntil later stages occur. Typical treatment of earlystage cardiac disease has largely focused onbenign neglect with subsequent monitoring ofthe patients cardiac rate, rhythm, size andassociated clinical signs at six to twelve monthintervals. The question that must be asked is a topicof much debate within the veterinary community.“If a patient shows no outward clinical signs
associated with a disease, such as early cardiacdisease, what if anything should be done clinicallyto aid in the improvement of the animal’s health”?
Through the collaboration with some of the worldsleading cardiologists and nutritionists in conjunc-tion with the innovative research performed atRoyal Canin and the WALTHAM Centre for PetNutrition, we now realize the beneficial effects ofimplementing early nutritional support in patientsfaced with cardiac abnormalities. Nutrition by itselfcan have profound beneficial effects at minimizingmetabolic disturbances, while at the same timeimproving the patients over all quality of life.
Daniel Baker, DVMScientific Communications, Royal Canin USA
Dr. Baker graduated from the University ofMassachusetts-Amherst with a Bachelor of Sciencedegree in biology with Honors in 1999. As anundergraduate he was one of the eighteen membersfrom around the world who took part in the East/Westmarine biology program at Northeastern University,allowing students to compare and contrast marine floraand fauna in three distinct parts of the world. Danielreceived his DVM degree from Ross University in 2003having completed his clinical year at the University ofMinnesota. Following graduation he worked as a smallanimal clinician for 4 years. During this time he focusedmainly in the area of emergency and critical basedmedicine. Daniel is currently a member of the ScientificCommunications team for Royal Canin USA.
Denise Elliott, BVSc (Hons), PhD, Dipl. ACVIM, Dipl. ACVN
Scientific Affairs, Royal Canin USA
Dr. Elliott received her degree in Veterinary medicinewith honors from the University of Melbourne in 1991.
After completing an internship in Small AnimalMedicine and Surgery at the University of Pennsylvania,Denise completed a residency in Small Animal Internal
Medicine and Clinical Nutrition at the University ofCalifornia-Davis. Denise became a Diplomate of theAmerican College of Internal Veterinary Medicine in
1996 and the American College of Veterinary Nutritionin 2001. She received her PhD in Nutrition from the
University of California-Davis in 2001, for her work onmultifrequency bioelectrical impedance analysis in
healthy cats and dogs. Denise is currently the Directorof Scientific Affairs for Royal Canin USA.
Nutritional managementof early cardiac disease:
ACT with SPEED
ROYAL CANIN VIEWPOINT
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 33
Cardiac disease is now the second leading causeof death in dogs. Chronic valvular disease (CVD)accounts for approximately 75% of these caseswhile dilated cardiomyopathy (DCM) is responsiblefor 10-15% of cases observed. Over the past decademore advanced diagnostic tools such as: electro-cardiography (ECG), Holter monitoring andechocardiography are now available to the generalpractitioner. This allows for early diagnosis andsubsequent intervention of early cardiac disease.
Nutrition’s primary role in the prevention andtreatment of cardiac disease is multimodal.Through the use of key nutrients, dietaryintervention seeks to provide optimal amountsof energy, minimize oxidative stress, reduceinflammation, balance electrolytes and ultimatelyto improve cardiac performance. Through the useof the ACT with SPEED acronym we can betterunderstand each key nutrients role in slowingthe progression of heart disease.
ACTArginine, an essential amino acid, is the precursorfor endogenously synthesized nitric oxide. Nitricoxide is well known for its role as an endothelium-derived relaxation factor, which in turn isresponsible for maintaining normal vascular tone(1). Endothelial dysfunction has been linked, inhumans and dogs, with congestive heart failure
(CHF) (2). Arginine supplementation appears toimprove cardiac output in patients with cardiacdisease by positively inf luencing preload andafterload (CO = HR x contractility x preload/afterload).
Carnitine, a quaternary amine, is composed of twoessential amino acids, lysine and methionine. It iscommonly found concentrated in both skeletal andcardiac muscle. L-carnitine (the biologically activeform) is critical for oxidation of fatty acids withinmitochondria. It serves as a transport shuttle offatty acids from outside the mitochondria intothe inner membrane and in turn is a key componentin the regulation of the citric acid cycle (3).L-carnitine is also responsible for transportingmetabolic waste products out of the mitochondriathat might otherwise become cardiotoxic.L-carnitine is normally provided to the animal insufficient amounts through intestinal absorption orfollowing hepatic and renal synthesis. In certainbreeds (Boxers, Doberman Pinschers and AmericanCocker Spaniels) there have been reportedmyocardial carnitine deficiencies (4,5). In a greatmany of these cases plasma carnitine levels werewithin normal limits. These findings suggest amembrane transport defect may be presentpreventing L-carnitine from entering into themyocardial cells from the plasma. Providingoptimal amounts of carnitine in the diet mayimprove overall myocardial function.
Taurine, a non-essential amino acid in the dog,is well known for its powerful antioxidant effectsthroughout the body. Taurine also is a key nutrientin the treatment of certain cardiomyopathies (6-8).Recent evidence also suggests that feeding certainlamb-based diets and severely protein restricteddiets, may lead to marked taurine deficiencieswith associated clinical signs (9-10). Breedassociated deficiencies (e.g. American CockerSpaniel, Portuguese Water dog) have manifestedthemselves in the form of dilated cardiomyopathy.Clinical improvement has resulted in severalcases where the proper taurine levels were presentwithin the diet (5-11). Taurine has also provento have positive iontropic effects in animals withexperimentally induced heart failure (12). Thissuggests taurine supplementation may provebeneficial in patients with cardiac disease withouttrue taurine deficiencies.
Table 1. Classification of heart disease
Grade
Class I
Class II
Class III
Class IV
Clinical description
No limitation of physical activity. Ordinary physical activity does not causeundue fatigue, palpitation, or dyspnea.
Slight limitation of physical activity.Comfortable at rest, but ordinary physicalactivity results in fatigue, palpitation, ordyspnea.
Marked limitation of physical activity.Comfortable at rest, but less than ordinaryactivity causes fatigue, palpitation, ordyspnea.
Unable to carry out any physical activitywithout discomfort. Symptoms of cardiacinsufficiency at rest. If any physical activityis undertaken, discomfort is increased.
Published in IVIS with the permission of the editor Close window to return to IVIS

34 / / Veterinary Focus / / Vol 18 No 3 / / 2008
With
SPEEDSodium restriction has long been thought of asthe nutritional mainstay of treating cardiacdisease. While sodium restriction has its placeadjunctively along side additional nutritionalmodalities, it is the degree of sodium restrictionbased on the severity of cardiac disease presentthat must be taken into account. Indeed, sodiumrestriction that is too severe early on in thedisease process may lend itself to an exaggeratedresponse by the renin-angiotensin aldosteronesystem (13-18). This can exacerbate clinicalsigns and the progression of the disease itself.The advent of angiotensin converting enzyme(ACE) inhibitors has further decreased the needfor severe sodium restriction in most patients(19). Based on our current understandingof sodium’s relationship to cardiac physiologyduring certain stages of cardiac disease, tailoringthe degree of sodium restriction is of the utmostimportance.
Protein restriction has erroneously worked itsway into the management of cardiac disease.Many of today’s diets are formulated on the anti-quated thought process that protein restrictionlends itself to reduced metabolic stress on thekidneys and liver (20). No known peer reviewedpublications exist proving this hypothesis.What’s worse is that protein restricted diets favorthe development of cardiac cachexia. This in turnwill lead to the perception by the owner of a poor
quality of life and likely hasten euthanasia. Cardiacdiets should contain optimal amounts of highlydigestible proteins that allow for the preservationof lean body mass.
Energy requirements in patients with cardiacdisease should be considered with both thepatients’ body condition score (BCS) and degreeof cardiac cachexia (Table 2) in mind. The goalshould be to manage caloric intake to preventboth obesity and emaciation while preservinglean body mass. Special focus needs to be placedon patients with poor BCS and/or cachexiaalready prevalent. Poor doing is often associatedwith anorexia in patients with cardiac disease.A recent study revealed the daily caloric intakein dogs with dilated cardiomyopathy was 72-84%of their expected daily energy requirements (21).Nutrient profiles therefore need be formulatedwith nutrients that are highly digestible andreadily bioavailable.
Eicosapentaenoic acid (EPA)
&
Docosahexaenoic acid (DHA) are essentiallong chain fatty acids derived from marinesources that provide profound anti-inflammatoryeffects throughout the body but especially with-in the heart. Studies have revealed that dogswith congestive heart failure have decreasedconcentrations of plasma EPA/DHA in comparisonwith healthy dogs (21). Their combined effectstarget the reduction of pro-inflammatory mediatorsactions on the cardiac infrastructure (21).Supplementation with marine derived omega-3fatty acids have also been shown to improve cardiaccachexia scores in dogs with cardiac disease. Arecent study revealed that EPA/DHA from fishoils given over a six-week period may decrease theseverity and frequency of arrhythmias in Boxerswho suffer from Arrhythmogenic Right VentricularCardiomyopathy (ARVC) (22).
Several other key nutrients related to the heartshould be taken into consideration. For example,vitamin E has positive effects on inhibiting lipidperoxidation of the cellular membranes of cardiaccells. Vitamin E can be looked at as a biomarker ofoxidative stress. In patients with heart disease, low
Cachexiascore
0
1
2
3
4
Description
Good muscle tone with no evidence ofmuscle wasting
Early, mild muscle wasting, especially in thehindquarters and lumbar region
Moderate muscle wasting apparent in allmuscle groups
Marked muscle wasting as evidenced byatrophy of all muscle groups
Severe muscle wasting
*Modified from Freeman (29).
Table 2. Cachexia scoring system
ROYAL CANIN VIEWPOINT
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 35
1. Palmer RM, Ferrige AG, Moncada S. Nitric oxide release accounts forthe biological activity of endothelium-derived relaxing factor.Nature 1987; 327: 524-526.
2. Wang J, Yi GH, Knecht M, et al. Physical training alters the pathogenesis ofpacing-induced heart failure through endothelium-mediated mechanismsin awake dogs. Circulation 1997; 96: 2683-2692.
3. Rebouche CJ, Paulson DJ. Carnitine metabolism and functions in humans.Annu Rev Nutr 1986; 6: 41-66.
4. Keene BW. L-carnitine deficiency in canine dilated cardiomyopathyIn: R. W. Kirk and J. D. Bonagura, eds. Current veterinary therapy XI.Philadelphia: W. B. Saunders Co, 1992; 780-783.
5. Kittleson MD, Keene B, Pion PD, et al. Results of the multicenter spaniel trial(MUST): taurine- and carnitine-responsive dilated cardiomyopathy inAmerican Cocker Spaniels with decreased plasma taurine concentration.J Vet Intern Med 1997; 11: 204-211.
6. Kramer GA, Kittleson MD, Fox PR, et al. Plasma taurine concentrations innormal dogs and in dogs with heart disease. J Vet Intern Med 1995; 9: 253-258.
7. Alroy J, Rush JE, Freeman LM, et al. Inherited infantile dilatedcardiomyopathy in dogs: genetic, clinical, biochemical and morphologicfindings. J of Med Genet 2000; 95: 57-66.
8. Freeman LM, Rush JE, Brown DJ, et al. Relationship between circulatingand dietary taurine concentrations in dogs with dilated cardiomyopathy.Vet Ther 2001; 2: 370-378.
9. Torres CL, Fascetti AJ, Rogers QR. Taurine and sulphur amino acid status indogs fed dry commercial poultry-by-product meal or lamb meal diets.J Vet Int Med 2000; 14: 364.
10. Sanderson SL, Gross KL, Ogburn PN, et al. Effects of dietary fat andL-carnitine on plasma and whole blood taurine concentrations andcardiac function in healthy dogs fed protein-restricted diets. Am J Vet Res2001; 62: 1616-1623.
11. Gavaghan B, Kittleson MD. Dilated cardiomyopathy in an AmericanCocker Spaniel with taurine deficiency. Aust Vet J 1997; 75: 862-868.
12. Elizarova EP, Orlova TR, Medvedeva NV. Effects on heart membranesafter taurine treatment in rabbits with congestive heart failure.Arzneimittelforschung 1993; 43: 308-312.
13. Koch J, Pedersen HD, Jensen AL, et al. Activation of the renin-angiotensinsystem in dogs with asymptomatic and symptomatic dilatedcardiomyopathy. Res Vet Sci 1995; 59: 172-175.
14. Pedersen HD, Koch J, Poulsen K, et al. Activation of the renin-angiotensinsystem in dogs with asymptomatic and mildly symptomatic mitralvalvular insufficiency. J Vet Intern Med 1995; 9: 328-331.
15. Webester KT, Brilla CG. Pathological hypertrophy and cardiac interstitium.Firbrosis and renin-angiotensin system. Circulation 1991; 83:1849-1865.
16. Tan LB, Jalil JE, Pick R, et al. Cardiac myocycte necrosis induced byangiotension II. Circ Res 1991; 69: 1185-1195.
17. Pedersen HD, Koch J, Jensen AL, et al. Effects of a low sodium diet with ahigh potassium content on plasma endothelin-1, atrial natriuretic peptideand arginine vasopressin in normal dogs. J Vet Med 1994; 41: 713-716.
18. Pedersen HD, Koch J, Jensen AL, et al. Some effects of a low sodium diethigh in potassium on the renin-angiotensin system and plasma electrolyteconcentrations in normal dogs. Acta Vet Scand 1994; 35: 133-140.
19. Kock J, Pedersen HD, Jensen AL, et al. Short term effects of acute inhibitionof the angiotensin-converting enzyme on the renin-angiotension systemand plasma atrial natriuretic peptide in healthy dogs fed a low-sodium dietversus a normal-sodium diet. J Vet Med 1994; 41: 121-127.
20. Pensinger RR. Nutritional management of heart disease In: R. W. Kirk, ed.Current veterinary therapy III. Philadelphia: W. B. Saunders, 1968; 229-232.
21. Freeman LM, Rush JE, Kehayias JJ, et al. Nutritional alterations and theeffect of fish oil supplementation in dogs with heart failure. J Vet Intern Med1998; 12: 440-448.
22. Smith CE, Freeman LM, Rush JE, Cunningham SM, Biourge V. Omega-3fatty acids in Boxer dogs with arrhythmogenic right ventricularcardiomyopathy. J Vet Intern Med 2007; 21: 265-273.
23. Freeman LM, Brown DJ, Rush JE. Assessment of degree of oxidative stressand antioxidant concentrations in dogs with idiopathic dilatedcardiomyopathy. J Am Vet Med Assoc 1999; 215: 644-646.
24. McMichael MA, Freeman LM, Selhub J, et al. Plasma homocysteine, Bvitamins, and amino acid concentrations in cats with cardiomyopathyand arterial thromboembolism. J Vet Intern Med 2000; 14: 507-512.
25. O'Keefe D, Sisson DD. Serum electrolytes in dogs with congestive heartfailure. J Vet Intern Med 1993; 7: 118.
26. Cobb M, Michell AR. Plasma electrolyte concentrations in dogs receivingdiuretic therapy for cardiac failure. J Small Anim Pract 1991; 33: 526-529.
27. Pedersen H, Mow T. Hypomagnesemia and mitral valve prolapse in CavalierKing Charles Spaniels. Zentralbl Veterinarmed 1998; 45: 607-614.
28. Roudebush P, Allen TA, Kuehn NF, et al. The effect of combined therapywith captopril, furosemide, and a sodium-restricted diet on serum electrolyteconcentrations and renal function in normal dogs and dogs with congestiveheart failure. J Vet Intern Med 1994; 8: 337-342.
29. Freeman LM. Nutritional Modulation of cardiac disease. WALTHAM FocusSpecial Edition Advances in Clinical Nutrition, 2000; 36-42.
REFERENCES
Vitamin E concentrations have been negativelycorrelated with the severity of the disease (23).Vitamin B deficiencies have been reported in catswith cardiomyopathy (24). Hypomagnesemia maypotentiate cardiac arrhythmias, decrease myocardialcontractility and contribute to muscle weakness(25,26). This is often observed in the CavalierKing Charles Spaniel (27). Potassium, traditionallyhyper-supplemented in historic cardiac dietformulations to compensate for the urine wastingsecondary to diuretic therapy, is no longer necessary.With the advent of ACE inhibitor therapy thatincreases the renal absorption of potassium,modern cardiac diets should contain normallevels of potassium (28).
In summary, we must first identify early stagecardiac disease in our patients. Then we need toeducate pet owner’s that early cardiac disease leftuntreated may have drastic life long complications.Many of these consequences stem from a sub-clinical disease process not necessarily manifestingitself as outward clinical signs. As clinicians, wenow have the opportunity to offer our clients earlydietary therapeutic intervention in conjunctionwith close monitoring of their pet’s disease state.Together we can give owners and their belovedpets, the nutritional tools necessary to aid in themanagement of heart disease and to improve thechance of living longer, healthier lives.
NUTRITIONAL MANAGEMENT OF EARLY CARDIAC DISEASE: ACT WITH SPEED
Published in IVIS with the permission of the editor Close window to return to IVIS

36 / / Veterinary Focus / / Vol 18 No 3 / / 2008
HOW I APPROACH...
IntroductionThe brain, as the controlling organ for many of thebody's functions, has first priority for blood supply.Compared to other organ systems, which sufferearly loss of function, the brain receives adequateblood supply with an average arterial pressure of60-70 mmHg. A drop in blood pressure to approxi-mately 40 mmHg brings about a reduction inbrain oxygen uptake, CO2 production and glucoseutilization. Below this pressure, brain functiongradually comes to a standstill.
As a result of regional or global brain malperfusionattacks of dizziness can occur, as can spontaneous,
reversible, brief loss of consciousness, whichis medically defined as syncope (fainting). Aninterruption in the brain's blood supply of 8-10 seconds or more leads to loss of consciousnessand in serious cases even to the patient's death.
Syncope is not a disease, but a symptom that canoccur in many conditions and diseases (Table 1).Cardiac-related syncope is caused by arrhythmiaor obstruction of the ventricular outflow tracts,congenital defects with cyanosis, as well as by heartdiseases, which lead to a decrease in cardiac outputwith global or regional malperfusion. Since loss ofconsciousness is accompanied by decreased skeletal
Marianne Skrodzki, DVMBerlin, Germany
Dr. Skrodzki studied law and veterinary medicine inBerlin and was awarded the “habilitation” and privatelectureship with venia docendi for her research work onsmall animal diseases. She has run her own SmallAnimal Cardiology practice in Berlin since 2002.Marianne Skrodzki has been a guest lecturer at theUniversity of Riga, St. Petersburg, Moscow and Tirana,with study visits to the University of Philadelphia,Utrecht and Edinburgh. Her main interests are thediagnosis and therapy of hereditary and acquiredcardiac diseases in small animals. Marianne Skrodzkiis internationally active, e.g. in the WSAVA and the Canine Heart Failure International Expert Forum(CHIEF).
Eberhard Trautvetter, DVMBerlin, Germany
Dr. Trautvetter has worked in the field of Small AnimalCardiology since 1967. Following a research trip toPennsylvania University in 1972, he was appointed
University Professor at the Freien Universität in Berlin.In 1984 he took over as Head of the Small Animal Clinic.
Since his retirement in 2000, Eberhard Trautvetter hasworked in a practice in Berlin and supervised graduate
students studying for a doctorate in Germany andabroad. His main scientific interest is in pedigree
analysis and genetic cardiac diseases in pedigree dogsand cats; he received worldwide distinctions for his
research successes, such as the Centennial Award ofMerit of the University of Pennsylvania and the Honorary
Medal of the CNVSPA (French Association of VeterinarySpecialists in Small Animals).
Syncope in dogs- a syndrome,not a disease
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 37
muscle tone, patients will fall over or collapse.Finally, cerebral hypoperfusion can also lead toseizures in the recovery position. Consequently,spasms, spontaneous sound utterances, as well asuncontrolled excretion and urination may beobserved. Various types of seizure can merge oroccur at the same time.
Extracardiac causes, which lead to sudden changesin body posture and movement, but which donot strictly fulfill the definition of syncope, mainlyinclude hypoglycemia, hypocalcemia, porto-systemic shunt, diseases of the central nervoussystem and breathing insufficiencies with severehypoxia (Table 1), aside from epilepsy primarilyof central origin.
Case historyIn many cases, it is difficult to explain a seizureevent by differential diagnosis. Nevertheless, givena specific case history, the cause of syncope can beidentified in many patients. Therefore, the nextquestion to ask is whether it is indeed a case ofsyncope, and not just a dizzy turn, or epilepsy. It isof considerable importance to know whether thepatient has a proven heart condition, or whether acardiac murmur is known to exist, without anyfurther diagnoses or therapy having been hithertoundertaken.
Faced with a seizure event for which theyare unprepared, dog owners, for the mostpart lay-persons, will be frightened to theextent that an objective description of theevent is scarcely to be expected, if at all.Details are especially unclear regarding theduration of the fit. Also, if asked whetherthe animal had fallen unconscious, mostowners will answer in the negative, saying:“My dog looked at me” and often misinter-pret the situation. One should not, there-fore, accept the details of the seizure eventas gospel, instead they should be criticallychallenged. A suggestive line of questioningis, however, to be strictly avoided.
Of particular interest is the time at which theseizure event occurs. Generally speaking,epileptic fits occur spontaneously, or duringrest or sleep. However, cardiac syncope isoften caused by characteristic triggers, suchas mental or physical exertion. “Cough
syncope” is exclusively observed during or immedi-ately after coughing, whereas most other seizuresof extracardiac origin are not dependent upon thesituation.
Characteristic of epilepsy are continuous tonic-clonic movements lasting more than 20 seconds,as well as a longer-lasting post ictal twilight state,the latter in contrast to syncope accompaniedby cramp. The onset of cramp likewise points toepilepsy. After a syncopal episode, patients regaintheir bearings within seconds. After longer-lastingseizures of one or two minutes, most animals alsoremain dazed or confused for only a few seconds.Longer-lasting disorientation is more indicative ofan epileptic fit. Exhaustion and fatigue also occurafter syncope, but are more frequent and morepronounced after epileptic fits. A less decisivefactor is whether, during the loss of consciousness,“spasms” are noted. Spontaneous movementsnot only occur in cases of convulsive seizure, butcan also occur in syncope. Uncontrolled excretionand/or urination are more or less equallyfrequent in generalized tonic-clonic and syncopalseizures.
The color of the mucous membranes or tongue,as well as type and rate of breathing during aseizure, provide important information for
Table 1. Breakdown of seizures based on cause
Cardiac origin
Arrhythmogenic AsystoleBradycardiaTachycardia
Organic heart disease Obstruction of ventricular outflow tract
- Aortic, pulmonary stenosis - Hypertrophic obstructive cardiomyopathy
- Heartworm disease
Tetralogy of Fallot (cyanosis)
Drop in cardiac output- Valvular insufficiency- Dilated cardiomyopathy
Cardiac tamponadeMyxoma
Drug-induced
Extracardiac origin
PulmonaryPulmonary hypertensionCough syncopeDiseases causing hypoxemia
Neurological/neurovascular Epilepsy Ischemia Central bleedingCerebral vasoconstriction Encephalitis (e.g. distemper)Portosystemic shunt
Metabolic/EndocrineHypoglycemiaHypocalcemiaHypoadrenocorticism
Drug-induced
OtherAnemiaTumors
Published in IVIS with the permission of the editor Close window to return to IVIS

38 / / Veterinary Focus / / Vol 18 No 3 / / 2008
HOW I APPROACH...
diagnostic discrimination, for example anemiafrom pulmonary disease.
Family case history is helpful for an evaluationof the genetic risk of seizure causes. It is worthknowing whether any animals related to thepatient died from sudden cardiac death, orwhether congenital heart disease or epilepsyare known to occur commonly.
In the case of repeat seizures, it is important toseek information concerning the frequency,pattern of seizure and duration of previousepisodes.
If the patient is known to suffer from heart diseaseand already undergoing therapy, the drug casehistory is of crucial importance. Drugs can causea syncopal seizure, either due to an undesirablevasodilatory effect, or bradycardiac or tachycardiaceffects. Aside from vasodilatory hypertensiveagents (ACE inhibitors, calcium antagonists anddihydralazine) cardiac glycosides and most anti-arrhythmic drugs and diuretics can be responsiblefor syncope.
Diagnostic evaluationPatients with syncope and primary cardiac diseaseshow a considerably higher mortality than dogswith extracardiac syncope and syncope of anunclear cause.
After an examination of the case history, thediagnosis focuses on a basic general examination,auscultation of heart and lungs, an electro-cardiogram, blood pressure monitoring and ageneral neurological examination. During thephysical examination, close attention will bepaid to not only determining capillary returnand the color of the mucous membranes, butalso, and more especially, pulse rate and qualityand symmetry of pulse waves in both rearextremities.
Particular attention during auscultation is to bepaid to the heart beat and also pathologicallyaltered heart sounds. For example, a loudersecond heart sound can be heard in casesof pulmonary hypertonia. A more extensiveauscultation will also reveal paroxysmal brady-cardia or arrhythmia. A pulse deficit noted
during a simultaneous assessment of pulseand heart rate can point to a clinically relevantarrhythmia.
A longer electrocardiogram recording at rest isvital for a basic diagnosis. During electrocardio-graphy, while awake and with the help of anassistant, the animal is held on its right side. Caremust be taken to be able to conclude heartdisease on the basis of characteristic indices. Anelectrocardiogram at rest may reveal nothing,even in patients with severe heart disease. Insome dogs signs of myocardial malperfusion ordisturbed heart rhythms are visible only duringphysical exertion, another ECG should thereforebe taken during, or shortly after, the patient'sexertion in doubtful cases or in cases of syncope ofunclear origin. Here it is simply a question ofrecognizing heart rhythm disturbances anddetermining heartbeat frequency. Accordingly, itdoes not matter how the dog is lying. However,an analysis of ECG amplitude should not beundertaken.
Generally speaking, a conventional ECG shouldtake a few minutes maximum and will moreor less represent a “snapshot”. Rare events,such as major heart rhythm disturbances ormerely sporadic arrhythmia can often onlybe determined following prolonged ECG. Inprolonged ECG or Holter ECG, the ECG recordingis taken continuously over 24 hours and the datastored. However, the recording of a “snapshot”after 24 hours can, in itself, still be too short.
In seizure diagnosis, laboratory analysis simplyprovides additional information. Nevertheless,a complete blood count (anemia), determinationof blood sugar (hypoglycemia) and electrolytes(hyperkalemia, hypocalcemia) should beconducted.
In all animals presenting with syncopal seizures,an echocardiographic examination is alsoadvisable for the identification or exclusion ofa heart defect. In suspected heart disease orrespiratory disease, the thoracic radiographis part of a standard examination. Special neuro-logical examinations can prove necessary fordifferential diagnostic purposes, supplemented,where applicable, by a CT or MRT scan.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 39
Cardiogenic syncopeCerebral perfusion is governed by systemic bloodpressure, in other words by cardiac output andperipheral vascular resistance. For this reason,a decrease in cardiac output due to various heartdiseases on its own or as a result of rhythmdisturbances and a drop in peripheral vascularresistance, for example through reflex-mediatedvasodilation, will promote syncope.
Adams-Stokes syndromeAll types of heart rhythm disturbance that lead tocentral hypoxia can trigger cardiac seizures. Suchattacks were described for the first time last centuryby two physicians from Dublin (Robert Adamsand William Stokes), hence the term Adams-Stokes seizure. These include asystole, pronouncedbradycardia and supraventricular and/orventricular tachycardia and ventricular fibrillation.Miscellaneous forms also occur (Table 2). Whileit is possible in dogs with a healthy heart tocompensate for a rhythm disturbance to a broadextent by adapting stroke volume, for most dogswith heart disease presenting with arrhythmia it isimpossible. Syncope consequently ensues. Typicalof syncope is the sudden onset irrespective ofposition. With the occurrence of rhythmogenicsyncope, patients mostly become pale and mayshow tonic-clonic convulsions. The only decisivefactors in the seizure pattern are the severity andduration of the heart rhythm disturbance orthe degree of impaired cerebral blood flow. Theclinical manifestations of seizure activity duringparoxysmal brady- or tachyarrhythmia can vary
with minimal cerebral blood flow. Momentarystaggering or gradual collapse in the animal occurparticularly in the presence of constant arrhythmia,such as atrial fibrillation or total AV block, butmostly just in the event of physical exertion orexcitement. Generally speaking, rhythmogenicsyncope should be viewed as an abortive form orprecursor of sudden cardiac death.
AsystoleAsystole is medically described as a complete lackof electrical and mechanical activity in the heart,which is recognized as a flatline on an ECG. Bloodpressure drops suddenly. Asystole of a few secondsgenerally only causes dizzy spells. However, theabrupt, complete interruption of cerebral bloodflow can also lead to the patient's sudden collapse.Cardiac arrest lasting ten seconds brings aboutcollapse, muscle spasms and paleness of themucous membranes. Dogs with longer-lastingasystole suffer seizure, are cyanotic and oftenexhibit uncontrolled excretion or urination due tosphincter weakness. The pulse can no longer befelt, although the absence of a detectable pulse initself is not a sure sign of asystole, since ventricularfibrillation (pulseless tachycardia) can also displaythe same symptom. Detectable heart sounds areabsent in asystole. In cases of asystole lastingmore than three minutes most patients die.
Cardiac asystole can occur, for example, fromcardiomyopathies, heart tumors or myocarditis. It isnot uncommon for asystole to be preceded byventricular fibrillation, which, for its part, can betriggered by any cardiovascular disease. Non-cardiacorigins include, among other things, metabolicchanges, such as severe acidosis in diabetes mellitus,hyper- or hypokalemia, and drug intoxication.
Atrioventricular blockDeceleration, intermittent interruptions or long-lasting block of conduction between the atria andventricles are referred to as atrioventricular block(AV block). While grade I or grade II type I AV blocksremain free of symptoms and are merely indicativeof the risk of a higher-grade block, grade II type IIAV block, as a result of bradycardia with regular orirregular dropping of ventricular complexes, canlead to a presyncopal attack, and more rarely toseizure. It is also possible for grade III AV blockto develop.
Table 2. Rhythm disturbances with manifestation ofsyncope
Bradycardia
Sinusbradycardia
High-grade AV block
Sick Sinus syndrome
Tachycardia
Atrial fibrillation
Supraventricular tachycardia
Ventricular tachycardia
Ventricular flutter Ventricular fibrillation
Wolf-Parkinson-Whitesyndrome
Asystole
SYNCOPE IN DOGS - A SYNDROME, NOT A DISEASE
Published in IVIS with the permission of the editor Close window to return to IVIS

40 / / Veterinary Focus / / Vol 18 No 3 / / 2008
HOW I APPROACH...
In the case of grade III AV block, which is alsoreferred to as complete or total AV block, due to thetotal block of conduction between the atria andventricles, the result is a complete dissociationof atrial and ventricular excitation (Figure 1).The atria and the ventricles beat separately andindependently and the atrial rate is very muchhigher than the ventricular rate. The rate of theventricular escape rhythm generally measures lessthan 40 beats/min. Accordingly, it is importantto immediately consider the possibility of totalAV block where the pulse rate is under 40/min.The clinical picture ranges from asymptomaticbradycardia with a sufficiently fast escape rhythm(very rare!) through dizziness to collapse. A verylow ventricular rate of, say, 25 beats/min is nolonger sufficient to attain a normal minutevolume, which often clinically manifests itselfas an Adams Stokes seizure. The frequency ofseizures varies greatly and can range from theoccasional syncopal event to several seizures aday. Since there is always the danger of theabsence of ventricular automatism as well, thepatients in question are in constant danger oflosing their lives, regardless of the frequency ofthe seizure.
Heart muscle diseases and congenital or acquiredheart valve disease and other diseases involvingthe electrical conduction system (ventricularseptal defect, myocarditis, degenerative diseases)come into consideration as causes of high-grade AV block. Breed-specific changes, as thatoccurring in the bundle of His in Dobermans,occur rarely. Furthermore, various conduction-inhibiting drugs (e.g. beta-receptor blockers,digitalis, calcium antagonists), and also theinfluence of the autonomous nerve system andhyperkalemia are causally responsible for totalAV block.
Sick Sinus syndromeSick Sinus syndrome, also known as "Sinus nodedysfunction", is the generic term for variousbradycardiac heart rhythm disturbances, and alsofor the pathological transition from bradycardia totachycardia. The essential causes are symptomsof fatigue, or sinus node dysfunction followingstrain on the left atrium, or degenerative changesin the atrial conduction pathways. The isolatedor combined occurrence of sinus bradycardia,sinus arrest, SA block, atrial or AV nodal escaperhythm, extrasystoles with tachycardiac episodes,paroxysmal atrial fibrillation, atrial flutter, as wellas tachy-bradycardiac syndrome with changingatrial rhythm lead to ataxia or syncope as a resultof a decrease in cerebral blood supply. Typicalsigns are absence of, or insufficient heart rateincrease during exertion.
Atrial fibrillationIn atrial fibrillation, the sinus node ceases to beeffective as a normal pacemaker (Figure 2). Theelectrical impulses to start a heart contractionoriginate in various areas of the atria. On anECG, no regular atrial activity is discernible.Fibrillation waves may be distinguished by their
Figure 1.
Total AV block in a dog presenting with AV insufficiency as a result of chronic degenerative mitral valve disease; note the regular presenceof atrial contractions, total block of conduction, atria and ventricles contract separately and independently, escape rhythm with broad,bizarre QRS complexes, atrial rate 120/min; Paper feed: 25 mm/s, calibration 0.5 cm = 1 mV.
Figure 2.
Dog presenting with dilated cardiomyopathy; atrial fibrillationwith irregular atrial fibrillation waves (F waves) and irregularRR intervals; heart rate 240/min: Paper feed 25 mm/s,calibration 1 cm = 1 mV.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 41
shape, amplitude and direction. Conduction to theventricle is irregular. Hemodynamically speaking,atrial fibrillation means atrial stand still, sincethe pump function of the atrium fails. In a rapidsequence of strokes, the diastolic duration issometimes so short that ventricular filling isinadequate and the stroke volume is unable totrigger a pulse wave, which is clinically discernibleas a pulse deficit.
Atrial fibrillation in itself is not life-threatening,but can lead to insufficiency even in a primarilyhealthy myocardium. In patients with myocardialdamage or cardiac insufficiency, tachycardiac atrialfibrillation can speed up the advancing diseaseprocess within a very short time. The faster theheart activity, the stronger the hemodynamic, andtherefore also clinical, effects, since the share of theblood volume propelled by the atrial contraction isnot contributing to the ventricular stroke volume.If the heart's performance, already underminedby the basic disease, is further reduced due totachycardiac atrial fibrillation, syncope can occuras a result of peripheral or cerebral hypoxia.
Mostly of secondary occurrence, atrial fibrillationappears in dogs with dilated cardiomyopathy, mitralvalvular disease or persistent Ductus arteriosus,as a result of pronounced atrial dilation. Idiopathicatrial fibrillation is relatively rare.
Ventricular tachycardiaVentricular tachycardia originates in the right or leftTawara branches of the conduction system, or in themyocardium and always has a serious cardiac
or extracardiac cause (Table 3). In GermanShepherds, ventricular tachycardia is geneticallyfound in the form of a primary arrhythmia. Highlyfrequent ventricular tachycardia leads very quickly,especially in primary cardiac disease, to failure ofthe pump function with Adams-Stokes seizures,cardiogenic shock and possibly also suddencardiac death. Breeds especially at risk are Boxersand Doberman Pinchers. In both breeds, suddencardiac death can occur as a result of ventriculartachycardia as the first and only “symptom”of dilated cardiomyopathy.
On an ECG, ventricular tachycardia is recordedas at least three rapidly successive abnormalities,in other words deformed ventricular complexes(Figure 3). Ventricular tachycardia generally arisesthrough a re-entry mechanism. In normal heartactivity, an action potential is generated in the sinusnode, directed through the atria and AV nodes intothe ventricular myocardium and subsides in theheart's apex area, because the surrounding myo-cardium is not yet in an excitable state (refractoryphase). Atrial excitation can be retrograde andtherefore independent of ventricular action.Interspersed P waves of normal shape and directionare occasionally visible in the ventricular rhythm.
Ventricular flutter and ventricular fibrillationare life-threatening rhythm disturbances. While inventricular flutter at rest, the cardiac output volumeis sufficient for a limited time, the increase involume during the patient's exertion can lead toan Adams-Stokes seizure, as a momentary event.Without therapeutic treatment it is not uncommonfor ventricular flutter to develop into ventricularfibrillation.
With ventricular fibrillation the heart's activityremains hemodynamically ineffective. Cardiacoutput drops so quickly that it can result inirreversible brain and heart damage in only a fewminutes. While ventricular flutter is depicted in anECG as wave-shaped QRS complexes of more or lesssimilar shape, size and frequency, in ventricularfibrillation QRS complexes are seen to vary greatly.
Wolff-Parkinson-Whitesyndrome (WPW syndrome)In a healthy heart, excitation can only spreadfrom the atria to the ventricles through the
Table 3. Common causes of arrhythmia
Cardiac
CardiomyopathyNeoplasiaAcquired valve diseasesCongenital diseasesGenetic (German Shepherd)Myocarditis
Extracardiac
Stomach torsion, volvulus
Neoplasia (e.g. mammarytumor, pheochromocytoma)SepticemiaFeverTrauma, painPulmonary diseasesHypoxiaAnemiaUremiaAcidosisElectrolyte imbalancesDrugs
SYNCOPE IN DOGS - A SYNDROME, NOT A DISEASE
Published in IVIS with the permission of the editor Close window to return to IVIS

42 / / Veterinary Focus / / Vol 18 No 3 / / 2008
HOW I APPROACH...
AV node. Wolff-Parkinson-White syndrome involvesarrhythmia in which there is usually a second andsometimes, although rarely, several electricalconduction pathways between the atria andthe ventricles. A part of the ventricle is activatedprematurely by means of circulating electricalexcitation through accessory conduction pathwaysbetween the atria and the ventricles, e.g. theso-called bundle of Kent. Therefore the sinus nodeimpulse is not transmitted to the ventricles throughthe AV node and the bundle of His. On an ECG, anelevation is often visible just before the R wave seensuperimposed on the Q wave. This is referred toas the delta wave. Paroxysmal tachycardia, withnormal or wide and bizarre QRS complexes,occurs due to the circulating excitation (re-entrymechanism). The P waves are inconspicuousand often not even recognizable. The PQ durationis shortened. ST changes are possible. WPWsyndrome occurs congenitally in isolated form, butis also to be observed in AV valve dysplasia, mitralinsufficiency as a result of chronic degenerativevalve disease and in hypertrophic cardiomyopathy.
Treatment of arrhythmic syncopeIn the first instance, it is always important inthe treatment of arrhythmic syncope to considerand recognize the cause of the heart rhythmdisturbances, since a causal treatment alwaysconstitutes the best therapy. It is not uncommonfor the therapeutic treatment of the underlyingdisease to make the additional administration of anantiarrhythmic drug unnecessary. This goes forall patients with arrhythmic seizures, regardlessof whether the origin is cardiac or extra-cardiac.If the animal is already being given an anti-arrhythmic drug or a cardiac glycoside, possibleside-effects of the drug are to be causally clarified(Table 4) and the on-going therapy may need to bechanged immediately, before further therapeuticmeasures are taken.
Owing to their pro-arrhythmic and negativeinotropic characteristics and other far-reachingside effects, antiarrhythmic drugs are not withoutdanger. They should therefore be prescribed withcaution and only after totally eliminating existingcongestive heart failure.
Bradycardiac heart rhythm disturbances withsyncopal episodes can be altered with drugs,
temporarily at best. Intravenous atropine injectionshould only be considered for acute treatment(Table 4). In symptomatic patients with brady-cardiac arrhythmia or, for example, in Sick Sinussyndrome, causal therapy is not possible, thereforethe implantation of a pacemaker is the method ofchoice for continually raising the pacing rate.
If syncopal seizures occur in patients withventricular stand still or total AV block as a resultof pronounced hyperkalemia, the serum potassiumin the blood must be lowered as quickly as possible.In such cases, for example, the intravenousadministration of a 10% solution of calciumgluconate (0.1-0.3 ml/kg by slow i.v. injection) isrecommended. The treatment of the underlyingdisease, e.g. acute kidney failure, chronic kidneydisease, or hypoadrenocorticism must follow.
Should syncope occur as a result of asystole, animmediate resuscitation with artificial respirationand cardiac massage would be required. Asystolecan, however, not be treated through defibrillation,since an irregular heart activity must still be presentfor it to work.
Figure 3.
Dog presenting with gastric dilation volvulus: rhythm control.Line 1: tachycardiac rhythm, heart rate 220/min with normal QRScomplexes, P waves present but partly obscured by precedingT waves. Line 2: supraventricular tachycardia with 2 prematureventricular extrasystoles; Line 3: ventricular tachycardia withdeformed QRS complexes, heart rate 300/min, P waves notdiscernible: Paper feed 25 mm/s, calibration 0.5 cm=1 mV.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 43
SYNCOPE IN DOGS - A SYNDROME, NOT A DISEASE
Figure 1.
3-year-old male Boxer presenting with subvalvular aortic stenosis.ECG tracing I, II, III, left first third of image left-ventricularextrasystole, middle of image sinus rhythm with three ventricularcomplexes of nomotropic origin followed by right-ventricularextrasystole, beginning with a supraventricular extrasystole: Paperfeed 25 mm/s, calibration 0.5 cm= 1 mV.
Figure 2.
ECG of the same Boxer as in Figure 1; ventricular tachycardia(210 beats/min) after brief exertion with collapse/syncope in thegradual rest phase; sinus rhythm established after a further2 minutes.
CASE REPORT
A three-year-old Boxer (weighing 25 kg) was brought into the practice after one hour's intensive play withother dogs. At the start of the seizure the dog appeared dazed and his hindquarters gradually slumped.He eventually fell on his side. His extremities were limp and respiration was slow. After approximately30 seconds to one minute, breathing became frequent again. The dog got up, became responsive againand walked slowly over to his owner.
In the otherwise hitherto symptomless dog, stamina and physical resistance in the previous three monthshad been somewhat limited, which his owner had put down to the high temperatures outside. Previously,on two different days, while giving his owner an enthusiastic welcome at the front door, both of the dog'srear extremities briefly gave way. It was only after in-depth reflection that the owner realized thesignificance of these episodes. Until then he had not set any great store by the event, since he felt that thedog had just moved awkwardly. Although the dog originated from Poland and had no known family casehistory, a heart noise was known to exist. However, further examinations had not yet been conducted.He was not receiving any medication.
The general clinical examination concluded no particular findings, merely that the arterial pulse in bothrear extremities was symmetrical and only irregular at times (pulsus irregularis) with a small pulsepressure amplitude (pulsus parvus).
Thoracic auscultation identified a grade IV/VI ejection systolic murmur in the region of the aorta with thePmax in the 4th intercostal space left side with transmission into the carotid arteries. The murmur wasalso audible cranially in the right half of the thorax. The dominant sinus rhythm was punctuatedparoxysmally by short series of extrasystoles. During the paroxysm, a pulse deficit was partly palpable.Respiratory auscultation was within normal limits. On the ECG, with the heart rate at 180 beats/min,short and longer bursts of ventricular extrasystoles were recorded (Figure 1).
During this first ECG recording, the animal was observant and showed undisturbed behavior.Subsequently, the dog was forced to climb the stairs. In doing so, he very soon had difficulty in breathingand suddenly collapsed on his side. According to the owner, this seizure pattern resembled the onepreviously experienced in the woods. The ECG conducted within a few seconds with the dog in seizureindictated the presence of a ventricular tachycardia as illustrated in Figure 2.
The echocardiography showed the concentric left ventricular hypertrophy with normal systolic functionand a dilated left atrium. The Doppler sonography examination measured a maximum speed of trans-valvular blood flow of 4.8 m/sec, which corresponds to severe aortic stenosis with a maximum gradient of
Published in IVIS with the permission of the editor Close window to return to IVIS

44 / / Veterinary Focus / / Vol 18 No 3 / / 2008
HOW I APPROACH...
An indication for immediate intravenousadministration of an antiarrhythmic drug issymptomatic tachyarrhythmia in patients whoare acutely threatened by sudden cardiac death.In dogs with ventricular tachyarrhythmia Lidocaneis primarily used intravenously via bolus orcontinuous intravenous drip. The administrationof Mexiletin is also possible, wherein it isimperative that the pronounced negative inotropiceffect of this substance be taken into consideration.
As a possible parenteral treatment of patients withsyncope resulting from tachycardiac arrhythmia,targeted use of an antiarrhythmic drug, afterhaving excluded or eliminated congestive heartfailure, can considerably improve quality of lifeand prognosis and reduce the risk of a recurrentseizure (Table 4). Cardiac glycosides are mainlyused in cases of supraventricular tachycardia oratrial fibrillation or flutter to decrease the heartrate and must, where necessary, be supplementedby potassium and magnesium substitution.
In dogs presenting with WPW syndrome, catheterablation by means of radiotherapy is necessary toensure the long-term elimination of accessorybundles.
Syncope as a result of organicheart diseaseIn dogs with structural changes in the heart or thelarge blood vessels in direct proximity to the heart(Table 1), and therefore with organic heartdiseases, syncope predominantly occurs underphysical or mental strain and is nearly alwaysaccompanied by a heart sound. Clinical symptomsof cardiac insufficiency, or signs of the underlyingdisease can be observed to varying degrees justbefore the seizure.
The most common causes for syncope areaortic (AS) and pulmonary (PS) stenoses withobstruction of the ventricular outflow tracts, aswell as dilated cardiomyopathies and severe mitralinsufficiency resulting from reduced minutevolume.
In Germany, cardiac seizures resulting fromheartworm disease with right ventricular outflowtract obstruction are rare. Similarly, hypertrophicobstructive cardiomyopathy (HCM, HOCM) indogs is hardly ever diagnosed. Causes of isolatedsyncope can be baroreflex afferent mismatchin a more pronounced obstruction of the leftventricular outflow tract induced by exertion, and
around 92 mmHg. Thickening of the mitral valve was evident together with middle-grade mitralinsufficiency detected by Doppler sonography. The right half of the heart, as well as the tricuspidal andpulmonary valves were, however, macroscopic and not visible by Doppler sonography.
Radiographs showed the enlarged silhouette of the heart. Compared to the arteries the V. lobaris in the areaof the upper lobes of the lung appeared somewhat widened. Pulmonary edema was not discernible.
The results of the blood test (hemogram, electrolytes, blood glucose, liver enzyme, creatinine and urea)were within normal biological variations.
In order to reduce the load on the myocardium and regulate the rhythm, the 25 kg dog was prescribedPropranolol at a dosage of 0.8 mg/kg 3 times a day, and 40 mg Furosemide twice daily, to eliminatevenous congestion.
Despite recommendations to avoid strenuous exercise, the owner allowed the dog to run along beside hisbike only two days after the initial examination and in outside temperatures of around 26° C. Shortlyafter the start of the bike ride, the dog collapsed and had another seizure as previously described. The dogdied on the street within a few minutes.
The postmortem examination confirmed the diagnosis of severe subvalvular aortic stenosis.
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 45
SYNCOPE IN DOGS - A SYNDROME, NOT A DISEASE
Table 4. Therapeutic treatment of heart rhythm disturbances in dogs
Indication
Bradycardia arrhythmia
Ventricular tachycardia
Ventricular tachycardia
AF, Supraventricular tachycardia
AF
AF
Supraventriculartachycardia
Ventricular tachycardia
AF, Ventricular arrythmia
AF, Ventricular arrythmia
Drug
Vagolytic drug
Atropine in emergencies0.02-0.4 mg/kg i.v., s.c.
Local anesthetic
Lidocaine in emergencies 2-4 (-6) mg/kg, i.v. CRI*: 50-80 µg/kg/min in the first 24 hrs, i.v.
Sodium channel blocker
Mexiletin in emergencies30 µg/kg/min in the first 24 hrs. i.v., thereafter CRI* 5 µg/kg/min, i.v. Long-term therapy: 3-5 (-10) mg/kg2-3x daily, oral
Digitalis
Digoxin0.01 mg/kg/d i.v., oral
Calcium channel blocker
Verapamil0.1 mg/kg 3x daily, i.v.1.0 mg/kg 3x daily, oral
Calcium channel blocker
Diltiazem0.5-1.5 (-2) mg/kg 3x daily, oral
ß receptor blocker
Propranolol0.2-1.0 mg/kg 3x daily, oral
ß receptor blocker
Atenolol0.25-1.0 mg/kg 2x daily, oral
ß receptor blocker (not selective)
Sotalol1-2 (-2.5) mg/kg 2 x daily, oral
Side effects
Ventricular fibrillation,CNS disturbances (syncope, coma)
Negative inotropic effects!
Cardiac insufficiency,bradycardiac arrhythmia,bundle branch block,polymorphous v tachyc.,gastrointestinal or CNSdisturbances
AV block, bundle branchblock, anorexia, vomiting,apathy
Bradycardia, asystole, AVblock, increased cardiacinsufficiency, drop in bloodpressure, loss of appetite,nausea, dizziness,constipation
as Verapamil
Cardiodepressive effect,cardiac insufficiency,hypotonia, bronchialobstruction, gastrointestinaldisturbances
as Propranolol
Brady- and tachyarrhythmia, CNS disturbances,bronchial obstruction
Contra-indications
Use only in life-threateningsituations, hence relativecontra-indications
AV block (2nd and 3rd°),bradycardia
Congestive heart insufficiency,increased QT time, SA-, AV- orintraventricular performancedisturbances
Sick Sinus syndrome,AV block (1st, 2nd and 3rd°),WPW syndrome,HCM, HOCM, AS
Congestive cardiac insufficiency,shock, bradycardia, sick sinussyndrome, SA block, AV block,WPW syndrome,Atrial fibrillation withhypotonia,Simultaneous administration ofß blockers,liver diseases
as Verapamil
Congestive cardiacinsufficiency,sick sinus syndrome, high-grade AV block obstructiverespiratory diseases
as Propranolol
Cardiogenic shock,bradycardia, AV block (2nd and 3rd°), obstructive bronchitis
CRI*: constant rate infustion; AF: atrial fibrillation.
Published in IVIS with the permission of the editor Close window to return to IVIS

46 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Hainsworth R. Syncope and fainting: classification andpathophysiological basis. In: Mathias CJ, Bannister R, Hrsg.:Autonomic failure. A textbook of clinical disorders of theautonomic nervous system, 4th edition Oxford: Oxford University Press1999, pp. 428-436.
Schaller B, Lyrer Ph. Synkopen bei neurologischenErkrankungen. Geriatrie Praxis 2001; 5: 36-41
Tobias R, M Skrodzki, M. Schneider. KleintierkardiologieKompakt; 1 Auflage: Schlütersche Verlagsgesellschaft, 2008.
FURTHER READING
also an arrhythmogenic trigger, which generallymanifests itself as ventricular tachycardia.
In patients presenting with Tetralogy of Fallot,hypoxic seizures can occur as an indication ofpronounced cyanosis.
Atrial myxoma is generally located in the leftatrium. Dependant upon the size and position ofthe mass, it can lead, owing to an intermittentdisplacement of the mitral valve opening area,to a sudden decrease in the left ventricular fillingvolume and therefore heart minute volume,together with syncopal episodes.
In cases of pericardial tamponade, certainsymptoms resulting from impaired right ventricularfilling predominate, including right-sided heartfailure with inefficiency and syncope. Asidefrom sinus tachycardia, atrial and ventriculartachycardia are also recorded.
In patients presenting with cardiac insufficiencyand reduced heart minute volume resulting fromdilated cardiomyopathy (DCM) or severe mitralvalve insufficiency, the most common cause ofsyncopal episodes are malignant heart rhythmdisturbances.
As a result of severe ventricular arrhythmia,syncope or collapse occur more frequently inDobermans and Boxers presenting with DCMthan in other breeds of dog. Cardiomyopathy inBoxers corresponds to a large degree to arrhythmo-genic right ventricular cardiomyopathy in humans.In this form of DCM, probably of autosomalheredity, the steady replacement of the rightventricular muscles by adipose tissue leads, amongother things, to loss of function and disturbances inelectrical conduction. While at first only isolatedventricular extrasystoles occur, the developmentof the disease can lead to severe ventriculartachycardia with syncope and left-sided heart
failure. In the final stages, ventricular fibrillationcan lead to sudden death.
In aortic stenosis there is a fixed obstruction ofthe left ventricular outflow tract, generally witha subvalvular, less commonly a valvular, andextremely rarely a supravalvular location.Depending upon the degree of severity of thechange, there can be increased pressure load on theleft ventricle. In order to maintain cardiac output,a concentric left hypertrophy develops, whichis often connected with a disturbed ventriculardiastolic function. A critical decrease in cardiacoutput is not only the result of the constantobstruction of the left ventricular outflow tract, itis also mainly caused by paradoxical baroreflexvasodilation. Invasive examinations could atleast be conducted in humans to demonstratethis. There is a special form of neurocardiogenicsyncope, which amounts to a discrepancy in thebaroreflex afferents of the ventricle (high pressure)and the vessels (low pressure) with vasodilatationin the non-working muscles. Increasing cardiacoutput during exertion in severe cases of aorticstenosis is generally not adequately possible. Thehigh pressure overload and the reduced coronaryflow lead to myocardial oxygen deficit with greaterleft ventricular insufficiency and induce severeventricular arrhythmia.
The increasingly weak contractility of themyocardium leads, on its own or together with anaortic valve and/or mitral valve insufficiency, tocongestive left-sided insufficiency. In some cases,heart rhythm disturbances occur only at thispoint, and arrhythmia already in existence becomemore pronounced.
Breed disposition is seen in Boxers, GoldenRetrievers, St. Bernard's, German Shepherds,Newfoundlands, Bull Terriers, German ShorthairedPointers, Great Danes and Rottweilers.
SYNCOPE IN DOGS - A SYNDROME, NOT A DISEASE
Published in IVIS with the permission of the editor Close window to return to IVIS

Vol 18 No 3 / / 2008 / / Veterinary Focus / / 47�
A n ECG recording is most commonly of2 types. A standard recording records arhythm over several minutes. A Holter
recording, requiring a strap on device, can providea recording over 1-7 days.
Single or multi-channel recordings may be used.The latter typically record 3 or 6 leads simultan-eously. The most useful paper speed settings are25 or 50 mm/second. Most useful sensitivitysettings are 1 cm/ mV (standard setting (Figure 1-10)) with 1/2 cm/ mV for large complexes and 2 cm/mV for very small complexes (often seen in cats).
Contra-indications toperforming an ECGIn general ECGs are probably performed morefrequently than necessary. They are not of benefitfor example in the diagnosis of the cause of amurmur in small animals. They are also unlikelyto be of benefit where the rate and rhythm appearnormal on auscultation. The ECG is not usually anaccurate guide to heart size. If cardiomegaly issuspected, other tests particularly radiology shouldbe considered. In cases of collapse where a cardiacorigin is suspected, a standard ECG is only likely to
provide information if an abnormality is clearlypresent on auscultation. More useful in suchcases would be a prolonged ECG such as a Holterrecording over one or more days.
Indications to performing an ECGIf there is marked bradycardia or tachycardiapresent on auscultation, an ECG can determinethe etiology. Chaotic rhythms usually representatrial fibrillation but all such rhythms should bedocumented with an ECG. Premature or missedbeats may also be characterized on ECG. If thearrhythmia is quite infrequent, it is unlikely to bedetected on a standard recording and a prolongedor Holter recording may be necessary.
Positioning for ECG recordingThe conventional recording is obtained in rightlateral recumbency. Recording in other positionsis quite acceptable. The standing position may bepreferred in nervous or large dogs for example.Varying the position will lead to some alteration inthe morphology of the complexes recorded. This isnot clinically important however and the rhythm,which is the most important aspect of the recording,will remain unaffected.
Electrocardiography in dogs
Michael Johnson, MRCVS, MVB, DVC, Veterinary Cardiorespiratory Centre, Kenilworth, UK
CUT-OUT AND KEEP GUIDE
Michael Johnson graduated from UCD Dublin. He spent the next 10 years in mixed, mainly large animal practice in Ireland, Wales, Australia and Canada. This was followed by 6 years in small animal practice in Manchester, UK. He obtained the certificate examinations in small animal medicine and veterinary cardiology during this time. For the past 7 years Mike Johnson has specialised in cardiorespiratory medicine at a referral practice in the UK,Martin Referrals, during which time he was awarded his Diploma in veterinary cardiology.
Published in IVIS with the permission of the editor Close window to return to IVIS

48 / / Veterinary Focus / / Vol 18 No 3 / / 2008
Figure 3.
St Bernard with atrial fibrillation due to DCM. Note the rapidrate at 180/minute, chaotic rhythm and absence of P waves.
Figure 5.
A 7-year-old Shetland Sheepdog presented for lethargy. Theoverall heart rate is low at 45/minute. P waves are unrelated toQRS complexes, representing third degree AV block.
Figure 2.
A West Highland White Terrier with marked depression andanorexia had a marked bradycardia on auscultation. Heart rateaverages 35/minute. No P waves are visible. This represents atrialstandstill. This occurred secondary to hyperkalemia caused byhypoadrenocorticism.
Figure 4.
Sometimes altered morphology of complexes provides usefulinformation. Note that the QRS complexes alternate markedlyin amplitude. This dog had a pericardial effusion, which oftenleads to electrical alternans as noted here.
Figure 7.
Persistent sinus tachycardia at 180/minute in a dog with heart failure.
Figure 6.
A single supraventricular premature beat in a dog with atrialenlargement. Such complexes resemble the normal QRS com-plexes but occur early.
Figure 10.
West Highland White Terrier presented with occasional collapse.Note the sinus arrest/ pauses which occur, in this case due tosick sinus syndrome. This is well recognized in older Westies.
Figure 9.
Normal dog showing wandering pacemaker. The P wave variesin amplitude and conformation from beat to beat. This is not anabnormality however.
Figure 8.
Dog with DCM showing initially 2 ventricular premature beats,VPCs, followed later by a run of rapid ventricular tachycardia.Note that VPCs appear quite different from the normal sinuscomplexes.
Figure 1.
This ECG shows normal sinus rhythm at 140 beats per minute.
ELECTROCARDIOGRAPHY IN DOGS
Published in IVIS with the permission of the editor Close window to return to IVIS