Embed Size (px)
Citation preview

Advanced Management of HIV-related Opportunistic Infections
Christopher Mathews, M.D.
UCSD Owen Clinic
HRSA Global AIDS Program

Case 1: Cavitary Infiltrate
By: Emily J. Erbelding, M.D., M.P.H. Johns Hopkins AIDS Service

A 41 year old woman with AIDS presented to the emergency department with fevers, and night sweats. HIV infection had been diagnosed 4 years prior, with a CD4 cell count of 11/mm3 at an outpatient visit 3 months previously. Her symptoms began approximately 4 weeks prior to admission when she began to experience fever and a cough productive of brown sputum. Her symptoms progressed, and she noted right-sided pleuritic chest pain and night sweats, along with a 12 pound weight loss.
History of Present Illness

Past Medical History
Asthma. Bacterial pneumonia 10 months prior. P. carinii pneumonia 6 months prior. Uterine cancer status post total abdominal hysterectomy/bilateral oophorectomy 4 years prior. Depression. Heroin addiction treated with methadone maintenance.
She reported an allergy to trimethoprim-sulfamethoxazole. Medications prescribed included dapsone 100 mg daily; trazodone; methadone; and inhaled albuterol.

Physical Examination
Physical exam revealed a thin woman who appeared chronically ill. Temperature was 39oC, heart rate 104/minute, respiratory rate 24/minute, and blood pressure 120/80. The oral cavity showed thrush and poor dentition. The neck was supple. Exam of the chest was notable for crackles in the right anterior lung fields. The cardiac exam revealed only tachycardia, but no murmurs or gallops. The abdomen was soft and nontender; there was no organomegaly noted. Extremities were without lesions, and neurological exam was normal.

Laboratory Studies
The hematocrit was 24% with a normal mean corpuscular volume. The white blood cell count was 6,400/mm3 with a differential of 90% segmented forms, 1% bands, 2% lymphocytes, and 7% monocytes.
ABG: Room Air, pH 7.52, pO2 70, pCO2 29
Creatinine 0.7, Na 131, K 3.4, Cl 98, CO2 21


Management Questions
• What is your differential diagnosis?
• What diagnostic tests do you want?
• What therapeutic interventions, if any, do you prescribe the night of admission?

Discussant’s DDx
• Mycobacterium tuberculosis. • Mycobacterium kansasii. • Cavitary Pneumocystis carinii pneumonia. • Necrotizing gram negative pneumonia.• Rhodococcus equi pneumonia • Nocardiosis• Tricuspid-valve endocarditis due to Staphylococcus
aureus. • Cryptococcus neoformans pneumonia. • Lymphoma• Cytomegalovirus pneumonia. • Histoplasma capsulatum or Coccidioidomycosis (with
proper epidemiologic exposures).

Hospital Course
Sputum induction was performed using nebulized hypertonic saline.
Bronchoscopy was scheduled for the next day, but this procedure proved unnecessary when the sputum studies were reviewed in the microbiology lab.



Clinical Course
• Upon careful review, the history of "sulfa allergy" could not be substantiated. She was started on trimethoprim-sulfamethoxazole, which she tolerated well, but her fever persisted. Minocycline was added with good clinical response. She was discharged home on minocycline and continued to improve.

Comment• Nocardia species have long been recognized as opportunistic
pathogens in immunocompromised patients, particularly those with specific defects in cell-mediated immunity.
• Compared to many other opportunistic pathogens, it is a relatively rare cause of disease in HIV infection. In a review of 30 patients with AIDS and nocardiosis, the disease was confined to the lungs in 70%. The median CD4 lymphocyte count at presentation was 109/mm3. Radiographic appearances described included alveolar infiltrates (67%), mixed reticulonodular/alveolar pattern (29%), cavitary disease (19%), with pleural effusions appearing in 14%. Effective agents include sulfisoxazole, trimethoprim-sulfamethoxazole, sulfadiazine, ceftriaxone, amikacin, and minocycline. Twenty-two of 27 patients described in this series responded to therapy, though for 14 of these, there was rapid recurrence with discontinuation of treatment. Prophylaxis with trimethoprim-sulfamethoxazole for PCP may provide effective prophylaxis against nocardiosis as well.

Case 2: Papular Eruption
Contributed by:Anisa Mosam, M.D. Department of Dermatology, Nelson R Mandela School of Medicine, University of Natal, Durban, South Africa

History & Physical
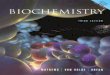
• A man in his twenties presented with a 3-week history of fevers and papules on his face and body.
• The patient was heterosexual and incarcerated in South Africa at the time of his presentation. He denied a history of exposure to animals, and had never traveled outside of the country.
• Physical ExaminationThe patient looked ill. His temperature was 38.5°C (101.3°F). Papules were present diffusely, involving the face, limbs , and trunk.



Studies
• White blood cell (WBC) count 4,500/mm³ (lymphocytes 600/mm³), hemoglobin 9.9 g/dL, platelets 507,000/mm³.
• Urea and electrolytes were normal• Alkaline phosphatase 168u/L, gamma glutamyl-
transpeptidase (GGT) 236 u/L and alanine aminotransferase (ALT or glutamic pyruvate transaminase GPT) 65u/L.
• Chest x-ray (CXR) and ultrasonography of the abdomen were normal.

Questions
• What is your differential diagnosis?
• What is your management plan?

Differential Diagnosis
1. Bacillary angiomatosis
2. Cryptococcosis
3. Disseminated pyogenic granulomas
4. Kaposi's sarcoma
5. Verruga peruana

Diagnostic Studies & Treatment
• An HIV screening test and Elisa confirmation test were positive. The CD4 cell count was 10/mm3.
• Skin biopsy showed vascular proliferation with a neutrophilic infiltrate. Warthin starry stain revealed clumps of organisms consistent with Bartonella.
• Treatment / Follow up:– The patient improved after treatment with
erythromycin 500 mg every six hours for two weeks.


Discussion
• This patient with AIDS had bacillary angiomatosis (BA). This disease is caused by Bartonella quintana and Bartonella henselae.
• BA occurs in immunocompromised patients, such as individuals with AIDS and is characterized by proliferation of endothelial cells.
• BA generally involves the skin and lymph nodes, but may occasionally affect the liver or spleen (bacillary peliosis) or other internal organs.
• The cutaneous lesions of BA often have a vascular appearance and may bleed when incised.
• The appearance of the cutaneous lesions is similar to that of verruga peruana, but the latter is restricted to South America.

Case 3: Dyspnea and Cough
By Chloe L. Thio, M.D. andEmily J. Erbelding, M.D., M.P.H.

History
• A 37 year old man with HIV infection and a CD4 count of 5/mm3 presented with worsening cough and shortness of breath.
• His present illness began 2 weeks prior to admission when he developed a non-productive cough. The cough worsened with smoking and in the evening.
• His physician treated him symptomatically for an upper respiratory tract infection.
• The cough continued, and 2-3 days prior to admission he noticed shortness of breath which was worse with exertion.
• He denied fevers, chills, night sweats, and chest pain. • He reported anorexia and weakness along with a 5
pound weight loss over the preceding 4 months.

History
• He had a history of idiopathic thrombocytopenic purpura, for which he took prednisone; pulmonary Mycobacterium kansasii, diagnosed 16 months prior, which responded to therapy; and gonorrhea and chlamydia infections which were treated in the past.
• His medications on admission included zidovudine, lamivudine, trimethoprim-sulfamethoxazole, azithromycin, prednisone 10 mg daily, rifampin, isoniazid, ethambutol, and megace.
• He reported no difficulties with medication compliance except for missing a few days of his trimethoprim-sulfamethoxazole prophylaxis approximately 1 month previously

Physical Exam
• General: He was a well developed, well nourished male resting comfortably in bed, but with perioral cyanosis.
• Temperature 36.9 C, respiratory rate 28/min, heart rate 96/min, blood pressure 110/58, and oxygen saturation of 86% on room air.
• His skin exam showed no rashes or other lesions. Eyes, ears, nose, and oral cavity examination were unremarkable.
• The neck had a 2 cm non-tender, mobile submandibular lymph node that had been documented previously and was decreasing in size.
• The cardiac exam was normal. • The chest exam revealed crackles at the bases bilaterally. • The abdominal exam was unremarkable. • His extremities revealed cyanosis but no edema. • His neurological examination was normal.

Laboratory Studies
• Hematocrit 41%; WBC count 3,700/mm3, platelets of 55,000.
• Arterial blood gas (room air): pH 7.46, pCO2 32 mm Hg, pO2 52 mm Hg.
• Serum chemistry– Na (mmol/L)136, K (mmol/L)4.3, Cl
(mmol/L)102, HCO3 (mmol/L)23, BUN (mg/dl)10, CR (mg/dl)0.9
– Liver tests normal



Questions
• What is your differential diagnosis?
• What is your immediate management plan?

Discussant’s DDx
• Pneumocystis carinii pneumonia
• Tuberculosis
• Nontuberculous mycobacterial infection
• Lymphoma
• Pulmonary Kapsosi's sarcoma
• Pulmonary nocardiosis
• Cryptococcal neoformans pneumonia

Discussion
• Pneumocystis carinii pneumonia (PCP) is the commonest cause of an interstitial infiltrate in an HIV-infected patient with a CD4 count less than 200/mm3.
• The course of symptoms and the dry cough are characteristic of PCP.
• However, his presentation would be unusual for PCP because he is afebrile and has been adherent with his PCP prophylaxis.

Discussion
• This presentation could represent a relapse of Mycobacterium kansasii, especially if he were noncompliant with his medication.
• Other mycobacterial infections, including a drug-resistant strain of M. tuberculosis, could also have evolved had he been intermittently compliant with his antimycobacterial therapy.
• The radiographic appearance of tuberculosis is more likely to be atypical, as in this case, in those with advanced HIV infection.
• If he were taking his medication regularly, however, a mycobacterial infection would be very unlikely.

Discussion
• Malignancy is a strong consideration. A bothersome cough is a common feature of Kaposi's sarcoma, and the radiographic appearance would be consistent with this diagnosis.
• KS would be a stronger consideration if there were mucocutaneous evidence of the process.
• The radiograph shown would be an unusual radiographic presentation of lymphoma

Discussion
• Pulmonary cryptococcosis and nocardiosis can both present with an interstitial infiltrate.
• Pulmonary nocardiosis may also present with cavitary lesions on chest radiograph.
• The absence of fevers and other systemic symptoms would make these diagnoses less likely.

Diagnostic Procedures
• The patient was started on presumptive therapy for PCP with trimethoprim-sulfamethoxazole and prednisone.
• Sputum specimens induced by inhalation of hypertonic saline were negative for P. carinii and acid fast bacilli.
• Since his sputum studies were nondiagnostic, he underwent a bronchoalverolar lavage.
• All studies, including stains for P. carinii, acid fast bacilli, and bacteriologic culture, were negative.
• His clinical condition remained unchanged on the trimethoprim-sulfamethoxazole, so he underwent a bronchoscopy and transbronchial biopsy.
• There were no endobronchial lesions visualized, but the biopsy specimen was diagnostic.


Case Discussion
• Pulmonary KS without mucocutaneous involvement is relatively uncommon, but has been reported in up to 11% of all KS cases in some clinical series.
• The presentation of pulmonary KS is often insidious in onset, and includes progressive dyspnea, non-productive cough, and chest tightness.
• Fever is seen only 50% of the time. • The chest readiograph usually reveals mid- and lower
lung zone involvement. • Common radiographic patterns include nodules, tumor
masses, bronchovascular thickening, and pleural effusions.

Case 4: Meningitis followed by Hydrocephalus
• A 30 year old male is admitted to hospital with headache,fever, vomiting, and papular skin lesions
• There are no focal neurologic findings nor papilledema. There is thrush in the mouth. A CT scan could not be obtained for 48 hours. CXR is normal.
• His sensorium is clear, he is alert and oriented, and consents to a rapid HIV test which is +

Questions
• Would you perform a spinal tap now or wait?
• What is your differential diagnosis?
• What are your immediate treatment plans?

Follow-up
• You suspect cryptococcal meningitis with cryptococcal skin lesions
• You scrape one of the skin lesions and examine it by gram stain and india ink, both confirm your suspicion.
• Because there are no focal findings and no depression of sensorium, you believe it is safe to do a lumbar puncture
• Opening pressure is >300 mm H2O, WBC =15 (100% lymphs), glucose is normal and protein 150mg%. India ink stain is +

Questions
• How would you treat this patient for cryptococcal meningitis?
• What other medications would you prescribe?

Follow-up
• 48 hours later, he is complaining of severe headache with vomiting
• He is receiving 0.7 mg/k of amphotericin B
• CD4 comes back at 75, viral load 500,000
• WHAT SHOULD YOU DO?

More Follow-up
• You do a large volume lumbar puncture. The CSF shoots out the top on the manometer. You take off 25 cc of fluid. The patient tells you his headache is much relieved.
• You have to repeat the procedure daily for 5 days, but then his headache abaits.
• You complete 2 weeks of intravenous amphotericin and discharge him on fluconazole 400 mg/d

More Follow-up
• He sees you in clinic a month later, feeling well.
• You discuss antiretroviral therapy, assess his readiness and that of his family to support him. Disclosure and stigma issues have been dealt with.
• You recommend d4T + 3TC + EFV
• He is completely adherent to the regimen

More follow-up
• He calls 3 weeks later complaining of severe headache and vomiting again. He insists that he has been taking his fluconazole
• LP shows opening pressure 350 mm H20• CSF WBC 250 (90% lymphs 10% segs), glucose
is 30 mg%, protein 200 mg%• CT scan shows evidence of hydrocephalus• Gram stain and AFB smear are negative but
India Ink is +

Questions
• What is your assessment?
• What additional information do you want to obtain?
• What is your immediate treatment plan?

Assessment
• DDx– Relapse or treatment failure of cryptococcal
meningitis– Tuberculous meningitis– Immune reconstitution syndrome
• You want to know his current CD4 and VL• You put him back on Amphotericin B and start
antituberculous therapy• CSF pressure is managed with repeat lumbar
punctures

Lab follow-up
• Culture of the CSF is sterile for bacteria and fungi at 1 week.
• CD4 is 150 and viral load has dropped to 15,000 copies
• WHAT DO YOU NOW SUSPECT?
• HOW WOULD YOU ALTER MANAGEMENT?