Embed Size (px)
Citation preview

Adrenergic Receptors Within the Cardiovascular SystemBy NEIL C. MORAN, M.D.
THE CONCEPT that drugs react withspecific receptors in living tissues to pro-
duce pharmacologic effects is believed to haveoriginated with Langley in 19051 althoughEhrlich and others had certainly conceivedof specific drug-cellular interactions. Todayreceptors have achieved such status amnongpharmacologists to be almost commonplace inspite of the fact that their identity has notbeen established. In undertaking a discussionof adrenergic receptors in the cardiovascularsystem consideration should be given to whatis meant by " receptor."The definitions which follow are intended
to be operational and heuristic: operationalin the sense of providing a conceptual frame-work on which both the experimentalist andthe physician can establish a common basisfor understanding and classifying sympatho-mimetic drugs; heuristic in the sense thatthis framework may provide a basis forfurther investigation into mechanisms of ac-tion of drugs and to the design of morenearly "perfect" drugs. Until more refinedtechnics lead to precise description of themolecular dynamics of drug-receptor inter-actions, the definition of receptors must re-main general.
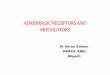
Let us first consider a schematic repre-sentation of a sympathetic nerve ending andthe adjacent effector cell (fig. 1). The chemi-cal transmitter-here labeled "sympathin"(probably norepinephrine*) -is synthesizedand bound in the nerve cell. In response toimpulses it is released to diffuse to the effectorcell and react with a receptor. The trans-
From the Department of Pharmacology, Divisionof Basic Health Sciences, Emory University, Atlanta,Georgia.
Publication No. 603 of the Division of BasicHealth Sciences, Emory University.
Supported by grant (H-2953) from the NationalHeart Institute, U. S. Public Health Service.
mitter-receptor combination (or combinationbetween sympathomimetic drug and receptor)can be considered as the triggering of amulti-step sequential reaction leading to thecellular response. For example, norepineph-rine, either released from the endings of thecardiac sympathetic nerves or of exogenousorigin, reacts with receptors in the heart in-itiating reactions leading to cardiac accelera-tion and increased contractility. That is, theadrenergic receptor is part of the effector cell.It is not a binding site in either the nerve orthe effector cell in which the transmitter ordrug is held inactive. In addition to the spe-cific adrenergic receptor there are other typesof receptors, depicted in figure 1 as II andIII, which react with other drugs.The structure of the adrenergic receptors
is not known, either biochemically or morpho-logically. What then is the basis for definingthe "adrenergic receptor" as distinct fromother receptors, as well as for distinguishingat least two types of adrenergic receptors?To elaborate on this question, gross physio-logic response of the effector cell may notallow distinction between two types of recep-tors, e.g., activation of either of the hypo-thetical receptors I and II in figure 1 leadsto augmented muscle contraction. Some dis-tinction between receptors may be made bycomparing characteristics of responses suchas magnitude, time course, etc., as well as bycontrasting the chemical families of drugsproducing similar responses, e.g., sympatho-mimetic amines versus cardiac glycosides.These distinctions, however, are vague and
*Although norepinephrine has the strongest claimto the title of "adrenergic neurohumoral transmit-ter," the possibility of related compounds acting astransmitters at some sites cannot be dismissed. Con-sequently, the designation "sympathin" seems mostappropriate and least committal for the sympathetictransmitter.
Circulation, Volume XXVIII, November 1963 987
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

MORAN
EFFECTOR CELL(e.g., smooth or cardiac muscle)
'TOR I
B
C^ MUSCLE/C > CONTRACTION
>7 B
Otherdrugs
Figure 1
Schematic representation of sympathetic neuro-effector junction.
provide little understanding of basic meeha-nisms.The most compelling evidence for formu-
lating an answer to our question comes fromthe use of specific antagonists. The schema infigure 2 exemplifies this approach from atheoretical basis. Activation of receptor Ileads to a type of response, depicted here as
a muscle contraction, and is antagonized byonly one type of blocking drug, e.g., blockingdrug I. Activation of receptor II produces aresponse similar in type to that elicited by Ibut distinguished from the latter by blockadeby still another drug, e.g., blocking drug II.Finally, activatioln of receptor III producesa response of qualitatively different type,which is blocked by a third type of antagonist.Thus, the distinction of receptor types be-comes more discrete by the use of specific an-
tagonists.From this hypothetical framework it fol-
lows that classification and description of re-
ceptors in these terms can be a logical andfruitful enterprise for a scientist without hisever seeing" a receptor. An analogous opera-
tion is the classifieation of antibodies on thebasis of antigen-antibody response, which maybe performed without isolation of the anti-bodies.The curreintly popular classification of
RECEPTOR RESPONSE
I .
BLOCKING DRUGSI LI m
rigure 2Schematic representation of concept of specificreceptors.
adrenergie receptors is that of Ahlquist,2, 3
which names two types-alpha and beta. Ae-cording to this classification, blood vessel con-striction in response to adrenergic stimuli issubserved by alpha receptors in vascularsmooth muscle and adrenergic vasodilatationby beta receptors. Cardiac responses are sub-served only by beta receptors. An importantstep in the development and confirmation ofthis classification camne in 1957 with the dis-covery by Powell and Slater4 that a chlo-rinated derivative of isoproterenol, dichloro-isoproterenol (DCI), antagonized certain"iinhibitory"' actions of sympathomimeticamines actions not blocked by conveintionaladrenergic blocking drugs.5 DCI has sincebeen employed extensively in analyses ofactions of sympathomimetic amines.
Dichloroisoproterenol selectively atagonizesadrenergically induced vasodilatation.4i Thatis, it inhibits the vasodepression induced byepinephrine and isoproterenol but not thevasoconstriction elicited by sympathomimeticamines. Nor does it antagonize the vasodila-tation evoked by histamine or acetyleholine.Thus, this evideniee supports the classificationof Ahlquist that svmpathetic vasodilatationand vasoconstriction are subserved by sepa-
rate receptors.Moran and Perkins6 demonstrated the abil-
ity of DCI selectively to antagonize the aug-
mentation of cardiac contractile force and theacceleration of heart rate produced by adren-ergic stimuli. Blockade of the positive ino-
Circulation, Volume XXVIII, November 1963
SYMPATHETIC NEURO-NERVE EFFECTORENDING JUNCTION
/ RECEF
!)8
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

SYMPOSIUM-ADRENERGIC CARDIOVASCULAR CONTROL9
A0,:
7777~~~~I
rtt:ffff:f$;sDCI {0000:^fw-7mg/
It"0sS";A0"
I IfgA IA smnnmncL.4
awn.:jow:cV
uon~~mz~~nwz IT±/k~:q A L.,wS__:4047S 37 ::I, ;SC t: i ^a ISO :IflENL 0 .: 5 ±/k
Figure 3Blockade of the positive inotropic effect of adrenergic stimuli by dichloroisop,roterenol(DCI). Cardiac contractile force recorded via a Walton-Brody strain-gage arch suturedto the right ventricle of an anesthetized, open-chest dog. Upper panels show responsesto left cardiac sympathetic nerve stimulation, and intravenous injections of norepinephrineand isoproterenol before administration of DCI. Lower panels demonstrate blockade by7 mg./Kg. of DCI.
Table 1Specificity of Cardiac Adrenergic Blockade by Dichloroisoprotereuol (DCI)
Drug
Digoxin0.15 mg./Kg.
Calcium chloride20 mg./Kg.
Theophylline10 mg./Kg.
Change in contractile forceWithout DCI After DCI
Gm.
Change in heart rateWithout DCI After DCI
beats/min.
17.9 ± 2.1 28.3 ± 7.2
60.3 + 3.7 54.0 ± 7.3
37.8 ± 7.7 35.2 ± 10.3 36.2 ± 3.7 28.2 + 2.1
Isoproterenol0.5 pug./Kg. 127.2 ± 28.6 9.5 ± 3.1 50.2 ± 6.8 0.4 + 0.2
Cardiac contractile force was measured in anesthetized, vagotomized dogs by means ofa Walton-Brody strain gage arch sutured to the right ventricle. All drugs were injectedintravenously. Seven mg./Kg. or more of DCI was administered. Values are means ±standard errors. Modified from table 4, reference 6, with permission of Williams & Wilkins Co.
tropic action has been confirmed by Drese]7aind by Furchgott.5 Figure 3 shows the nearly(oinplete blockade by DCI of the effects ofcardiac sympathetic nerve stimulation, nor-
Circulation, Volume XXVIII, November 1963
epinephrine, anid isoproterenol oni cardiaccontractile force in an anesthetized dog. Table1 illustrates the specificity of this blockadefor adrenergic type stimuli.
.1.i47.. .:::. ...
989
:. . ... X
-00AtR;0 :00A0:|--ff CTee i..y tr-- Tf .00 Cl-: tE ..-000
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

990
CUMULATIVE DOSES- mgkgPHENOXYBENZAMINE
200 , , .-m_m-I I
Ep6. I.O^/kg Noi. LO,o/q isp0.5a A~ ~~SA
150-.. \
IO -- I t -
50;
100 ,,, l
50~~~ -8
0 O I's71 3 7T 15, 0' 3, 7T 6fCUMULATIVE DOSES - mgJ/kDICHLOSORIROTERENOL
Figure 4Comparison of adrenergic blocking properties of phenoxybenzamine and dichloroiso-proterenol (DCI). Upper graphs depict right ventricular conttractile force and lowergraphs diastolic blood pressure in anesthetiz ed open-chest dogs. Closed circles are"{control" measurements immediately before i.v. injection of epinephrine (Epi), nor-epinephrine (Norepi), or isoproterenol (Isopro). Open circles are maximum responses,the arrows showing the direction and magnitude of change. Left hand part: dogs weregiven phenoxybenzamine in geometrically progressing doses, the responses to arminesbeing tested after each dose. Right hand part: effect of progressive increase of dose ofDCI. (Reproduced with permission of WTilliams & TWilkins Co. from J. Pharmacol. KExper. Therap. 133: 194, 1962).
The cardiac adrenergic blocking effect ofDCI gave support to the view proposed byAhlquist that the cardiac adrenergic receptorsare of a different type from those which sub-serve vasoconstriction and are similar to thosemediating vasodilatation, e.g., beta receptors.
Further supporting evidence comes fromthe studies of Nickerson and Chan9 and ofMoran and Perkins,10 showing that conven-tional adrenergic blocking agents such asphenoxybenzamine (Dibenzyline) do not havespecific cardiac blocking actions. Figure 4demonstrates a comparison of phenoxybenz-amine and DCI. Phenoxybenzamine, given inprogressively larger doses to dogs, producesprogressive blockade of the vasoconstrictoractions of epinephrine and norepinephrine,leading to a reversal of the vasopressor actionl
of epinephrine and abolition of that of nor-epinephrine. Even at the highest dose ofphenoxybenzamine, however, there is no an-tagonism of the positive inotropic effect ofthe two amines, the maximum contractileforce produced by epinephrine and norepi-nephrine after phenoxybeuzamine equalingor exceeding that before. In contrast, DCIdoes not block the vasopressor effect of eitherepinephrine or norepinephrine but antago-nizes both the vasodilator action of isopro-terenol and the positive inotropic action ofthe three amines. Thus, phenoxybenzamineblocks the responses subserved by alpha re-ceptors, e.g., vasoconstriction, but not thosesubserved by beta receptors. DCI, by com-parison, is a beta receptor-blocking compound.DCI itself has sympathomimetic activity.
Circulation, Volume XXVIII, November 1963
MORAN
I
U-§1
lf
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

SYMPOSIUM-ADRENERGIC CARDIOVASCULAR CONTROLI
Table 2Ca rdiac Adrenergic Block,ade byl 1.C.01. 38,171
Mean increase in cardiac contractile force in grams ± S.E.Cardiac sympathetic Epinephrine Calcium chloridenerve stimulation 1 ,tg./Kg. i.v. 20 mg./Kg. i.v.
193 + 48 (5) 187 + 19 (11) 118 ± 12 (3)
38,174 2.4 2.4 (5) 10.9 3.9 (11) 103 + 3.3 (3)P < 0.001 < 0.001 > 0.1
Experiments were performed on anesthetized, open-chest dogs; right ventricular con-
tractile force measured with strain gage arch. I.C.I. 38,174 was given in divided dosesto cumulative dose of 7 or 15 mg./Kg. Results of two dose levels are pooled. I.C.I. 38,174was supplied by Dr. J. W. Black of Iniperial Chemical Industries Limited. P values are forsignificance of differences by paired t test.animals used.
Initial injections in dogs produce a fall inblood pressure and increased cardiac contrac-tile force and rate. This "intrinsic?" activityis a disadvantage, both in terms of experi-mental and possible clinical use of the com-
pound. Another beta adrenergic blocking drughas recently been described by Black andStephenson.'1 It is a naphthyl isopropyl-aminoethanol (I.C.I. 38,174; nethalide). Table2 illustrates the selective cardiac adrenergicblockade produced by this agent.
It has been stated that alpha adrenergicblocking drugs are able to antagonize cardiacarrhythmias induced by sympathomimeticamilies although unable to block the positiveinotropic and chronotropic effects.12 Mooreand Swain,'3 Luechesi and Hardman,14 andMoran et al.15 have recently shown that DCIantagonizes several types of ventricular ar-
rhythmias produced by catecholamines. It isnot definitely established, however, that thisantagonism is entirely explained on the basisof specific blockade; that is, DCI may havean antiarrhythmic action distinct from itsadrenergic blocking action.14 The antagonismof catecholamine-induced arrhythmias byalpha adrenergic blocking agents is probablynonspecific and related to the antagonism ofthe vasopressor effect of amines by theseblocking drugs.1'5 16
Another effect of adrenergic stimuli whichis antagonized by DCI and not by phenoxy-benzamine is the activation of glycogen phos-phorylase in the dog heart.'7 The relatively
Circulation, Volume XXVIII, November 1963
Numbers in parentheses are number of
specific activation of this enzyme system,which catalyzes the first step of glycogenoly-sis, by adrenergic stimuli and the selectiveblockade of this effect by DCI suggests thata beta type receptor subserves this adrenergicaction.The adrenergic receptors in blood vessels,
as indicated above, are either alpha or beta.It is presumed that adrenergic vasoconstric-tion in the systemic circulation is alpha, inthat isoproterenol has negligible arteriolarconstrieting action and DCI does not blockthe vasoconstriction induced by potent amines.Adrenergic vasodilatation in the systemic cir-culation, mostly in skeletal muscle, is sub-served by beta receptors since isoproterenolis the most potent amine and DCI blocksthe effect.5 6 Mohlme-L-undholm and L-und-holmls 19 have postulated that adrenergicvasodilatation in skeletal muscle is secondaryto the lactic acid released in response to theglycogenolytic effect of adrenergic stimuli. Ifthis hypothesis is correct, one need not assume
a beta receptor specific to adrenergic aminesin the vascular smooth muscle. Furchgott,8however, has presented evidence that adren-ergically induced relaxation of smooth musclecan occur without increase in tissue lacticacid.
The available evidence suggests the exist-ence of both alpha and beta receptors in thepulmonary circulation, that is, vasoconstric-tion mediated by alpha and vasodilatationmediated by beta receptors.20 21
ControlAfter I.C.I.
991
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

MORANTable 3
Example of Classification of Sympathomimetic Amines in Terms of Actions on Alphaand Beta Receptors
Responses to amines
Beta
Iso Epi
Alpha
Norepi Methox
Blockade ofresponses by
DCI (,8) PBZ (a)
HeartChronotropicInotropieEctopic fociMetabolism
++±± +++ -f+++++++ +H++ +++[±+±±V'] ++1+ +±±++++ -[++ ++±
VesselsVasodilatation ++++ +++Vasoconstriction +++
Iso-isoproterenol Norepi norepinepiEpi-epinephrine Methox methoxam
a-Potential ability. Manifestations of thisnounced sinus taehyeardia produced by isoproteren
The concept of two types of adrenergicreceptors in the circulatory system is sum-
marized in table 3. Four sympathomimeticamines are considered: isoproterenol, whichhas predominantly beta action; epinephrine,which has both alpha and beta actions; nor-
epinephrine, which is primarily an alpha stim-ulant but possesses potent beta actions on theheart; and finally, methoxamine (Vasoxyl),which is predominantly an alpha receptor an-
tagonist. The spectrum of actions of thesefour amines indicates the overlapping effectsone encounters in symnpathomimetie drugs.The two adrenergic blocking drugs, DCI andphenoxybenzamine are shown selectively toblock beta and alpha receptors, respectively.The concept of two receptors in the circu-
latory system has obvious implications to theexperimental pharmacologist. Does it, how-ever, have value to the physician? I believeit does. One, a classification of the type pre-
sented in table 3 might enable the physicianto select more rationally a sympathomimeticamine for specific therapeutic effects. For ex-
ample, if one desires a vasoconstrictor aminedevoid of cardiac stimu]ant actions one wouldchoose a predominantly alpha agent. Drugswith varying degrees of dual action are avail-able and finally a "pure" beta stimulant isfound in isoproterenol with its profoundeardiae stimulant action. Two, the therapeutic
+4- + 0
o +
hrine DCI-dichloroisoproterenoline PBZ-phenoxybenzamineaetioni obscured in miost instainees by pro-
ol.
potential of beta type adrenergic blockingagents remains to be assessed. DCI, becauseof its marked intrinsic activity, producestachyeardia and, therefore, has little thera-peutic promise. I.C.I. 38,174, (nethalide)which has less intrinsic activity than doesDCI, would theoretically not have this sideeffect to as prominent a degree. In fact,Dornhorst and Robinson22 have reported thatI.C.I. 38,174 (nethalide) increases the exer-
cise tolerance and reduces exercise tachycar-dia in patients with angina pectoris. Therationale of therapy of angina pectoris withbeta adrenergic blocking compounds is basedupon their ability to antagonize the tachy-cardia, augmented contraction, and increasedmetabolic activity brought about throughsympathoadrenal discharge, thereby moderat-ing the myocardial hypoxia resulting fromstress. Whether beta adrenergic blockingdrugs are of importance in therapy of anginapectoris or of other circulatory conditions isnot established at present.
References1. LANGLEY, J. N.: On the reaction of cells and
of nerve-endings to certain poisons, chieflyas regards the reaction of striated muscle tonicotine and to curari. J. Physiol. 33: 374,1905.
2. AHLQUIST, R. P.: A study of the adrenotropicreceptors. Am. J. Physiol. 153: 586, 1948.
Circulation, Volume XXVIII, November 1963
992
-
H-4 +
00-4-
0
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

SYMPOSIUM-ADRENERGIC CARDIOVASCULAR CONTROL
3. AHLQUIST, R. P.: Adrenergic drugs. In Pharma-cology in Medicine. Ed. 2. Drill, V. A. ed.,New York, McGraw-Hill Book Company, Inc.,1958, Chap. 27.
4. POWELL, C. E., AND SLATER, I. H.: Blocking ofinhibitory adrenergic receptors by a dichloroanalog of isoproterenol. J. Pharmacol. &Exper. Therap. 122: 480, 1958.
5. NICKERSON, M.: The pharmacology of adrenergicblockade. Pharmacol. Rev. 1: 27, 1949.
6. MORAN, N. C., AND PERKINS, M. E.: Adrenergicblockade of the maimmalian heart by a dichloroanalogue of isoproterenol. J. Pharmacol. &Exper. Therap. 124: 223, 1958.
7. DRESEL, P. E.: Blockade of some cardiac actionsof adrenaline by dichloroisoproterenol. Canad.J. Biochem. Physiol. 38: 375, 1960.
8. FURCHGOTT, R. F.: The receptors for.epinephrineand norepinephrine (adrenergic receptors).Pharmacol. Rev. 11: 429, 1959.
9. NICKERSON, M., AND CHAN, G. C-M.: Blockadeof the responses of isolated myocardiumn toepinephrine. J. Pharmacol. & Exper. Therap.133: 186, 1961.
10. MORAN, N. C., AND PERKINS, M. E.: An evalua-tionl of adrenergic blockade of the mammalianheart. J. Pharnmacol. & Exper. Therap. 133:192, 1961.
11. BLACK, J. W., AND STEPHENSON, J. S.: Pharma-cology of a new adrenergic beta-receptor block-ing compound (nethalide). Lancet 2: 311, 1962.
12. NICKERSON, M., AND SMITH, S. M.: Protectionagainst cyclopropane-epinephrine arrhythmiasby dibenamine and other agents. Anesthesi-ology 10: 562, 1949.
13. MOORE, J. I., AND SWAIN, H. H.: Sensitizationto ventricular fibrillation. I. Sensitization bya substituted propiophenone, U-0882. J. Pharm-acol. & Exper. Therap. 128: 243, 1960.
14. LUcCHESI, B. R., AND HARDMAN, HI. F.: Theinfluence of dichloroisoproterenol and related*compounds upon ouabain and acetylstrophan-thidin induced cardiac arrhythmias. J. Pharma-col. & Exper. Therap. 132: 372, 1961.
15. MORAN, N. C., MOORE, J. I., HOLCOMrB, A. K.,AND MUSHET, G.: Antagoinism of adrenergic-ally-induced cardiac arrhythmias by dichloro-isoprotereniol. J. Pharmaeol. & Exper. Tlherap.136: 327, 1962.
16. MOE, G. K., MALTON, S. E., RENNICK, B. R., ANDFREYBURGER, W. A.: The role of arterial pres-sure in the induction of idioventricular rhythmsunder cyclopropane anesthesia. J. Pharmacol.& Exper. Therap. 94: 319, 1948.
17. MAYER, S. E., AND MORAN, N. C.: Relationbetween pharmacologic augmentation of cardiaccontraetile force and the activation of myo-cardial glycogen phosphorylase. J. Pharmacol.& Exper. Therap. 129: 271, 1960.
18. MOHME-LUNDHOLM, E.: Mechanism of the relax-ing effect of adrenaline on bovine coronaryvessels. Acta physiol. scandinav. 38: 255, 1957.
19. LUNDHOLM, L.: The mechanism of the vaso-dilator effect of adrenaline. I. Effect on skele-tal muscle vessels. Acta physiol. scandinav. 39:Suppl. 133, 1957.
20. AvIADo, D. M., JR., AND SCHMIDT, C. F.: Effectsof sympathomimetic drugs on pulmonary circu-lation: with special reference to a new pul-monary vasodilator. J. Pharinacol. & Exper.Therap; 120: 512, 1957.
21. CASTRO DE LA MATA, R., PENNA, M., AND AvIADO,D. M.: Reversal of sympathetic bronchodila-tion by dichloroisoproterenol. J. Pharmacol. &Exper. Therap. 135: 197. 1962.
22. DORNNORST, A. C., AND ROBINSON, B. F.: Clinicalpharmacology of a beta-adrenergic blockingagent (nethalide). Lancet 2: 314, 1962.
Kt2
Circulation, Volume XX VIII, November 1968
99:3
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from

NEIL C. MORANAdrenergic Receptors Within the Cardiovascular System
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1963 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.28.5.987
1963;28:987-993Circulation.
http://circ.ahajournals.org/content/28/5/987.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 24, 2018
http://circ.ahajournals.org/D
ownloaded from