Embed Size (px)
Citation preview

Adrenal carcinoma and pheochromocytoma
Salvatore Grisanti, Alfredo Berruti
Department of Medical Oncology
University of Brescia - Spedali Civili di Brescia
Milan, 02 March 2018 - Post ASCO-GU 2018

I am perfectly aware of the risk of being a speaker after lunch

Adrenocortical carcinoma (ACC)
Pheochromocytoma (PCC) & paraganglioma
Milan, 02 March 2018 - Post ASCO-GU 2018
Adrenal gland: physiology

The clinical management of ACC and PCC is complex because the clinician have to face two problems at the same time in most patients
• The neoplastic mass & metastases
• The endocrinological-associated disease (Cushing, etc …)
Two diseases in one
Milan, 02 March 2018 - Post ASCO-GU 2018

Milan, 02 February 2018 - Post ASCO-GU 2018
Endocrinology
Med. Treatment
Surg. Treatment
Radiol. Diagnosis

Adrenocortical Carcinoma:<br />Finding the Wolf in Sheep’s Clothing
Presented By William Mayo-Smith at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

What is the Concern with an Adrenal Incidentaloma?
Presented By William Mayo-Smith at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

7 Imaging Phenotypes to differentiate benign & pathologic adrenal
Presented By William Mayo-Smith at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

7 Imaging features to differentiate benign from pathologic adrenal
Presented By William Mayo-Smith at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Enhancement Patterns
Presented By William Mayo-Smith at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Adrenocortical Carcinoma: Putting it Together
Presented By William Mayo-Smith at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Milan, 02 February 2018 - Post ASCO-GU 2018
• Chi si deve trattare?
• Quale chirurgia?

Adrenal Tumors
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Adrenal Incidentalomas<br />Indications for Surgery
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Incidence of Adrenal Ca<br />According to Tumor Size<br />Review of 20 reported series and meta-analysis
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Stage disposition in localized ACC
Curable (39%)
2%
19%
18%
61%
%
Milan, 02 March 2018 - Post ASCO-GU 2018

Role of surgery in ACC
Surgery is the mainstay of therapy and represents the only chance of cure
Milan, 02 February 2018 - Post ASCO-GU 2018

Survival according to completeness of resection<br /> MSKCC experience
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Adrenocortical Carcinoma:<br />Consensus in Treatment
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Slide 17
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Slide 18
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Milan, 02 February 2018 - Post ASCO-GU 2018
Gronchi et al. JCO 2009

Adrenocortical Carcinoma<br />5-Year Survival Rates (%) from Reported Series
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Which surgery?
• Two different approaches are possible for adrenalectomy:
• Open surgery adrenalectomy (OA)
• Laparoscopic adrenalectomy (LA)
• No prospective trials are available to determine which is the best strategy
Milan, 02 March 2018 - Post ASCO-GU 2018

Laparoscopic Adrenalectomy in ACC – Spillage and Recurrence Risks
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Survival Analysis
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Open surgery vs laparoscopic adrenalectomy?
Porpiglia et al. Eur Urol 2010
• Comparable recurrence-free survival in OA and LA groups
• Type of surgical treatment is not a prognostic factor
Milan, 02 February 2018 - Post ASCO-GU 2018

Peritoneal Dissemination<br />A Complication of Laparoscopic Surgery
Presented By Antonio Fojo at 2017 ASCO Annual Meeting

Slide 6
Presented By Antonio Fojo at 2017 ASCO Annual Meeting

Laparoscopic vs Open: Meta-Analysis
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

OA vs LA: ESMO guidelines
• Open surgery with transperitoneal access is the standard treatment of all patients with localized (stage I–II) and local advanced stage (stage III) ACCs when complete resection can be achieved.
• Laparoscopic adrenalectomy is a safe and effective procedure for a selected group of patients with small ACCs (<8 cm) without preoperative evidence for invasiveness and adrenal masses (e.g. incidentalomas) that are judged as only potentially malignant.
ESMO guidelines. Ann Oncol 2012
Milan, 02 March 2018 - Post ASCO-GU 2018
Domanda ECM !

Pheochromocytoma<br />Principles of Surgery
Presented By Jonathan Coleman at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Milan, 02 February 2018 - Post ASCO-GU 2018
• Quali sindromi endocrine?
• Quale work-up?
• Quale trattamento? • Test genetici

Slide 9
Presented By Tobias Else at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Hormone excess in ACC
Hirsutism, deepening of the voice, breast atrophy, male pattern baldness, clitoral hypertrophy, oligomenorrhea, altered libido
Gynecomastia, breast tenderness, decreased libido, testicular atrophy
Severe hypertension, hypokaliemia
Lafemina et al. J Surg Oncol 2012
Milan, 02 February 2018 - Post ASCO-GU 2018

Cushing’s syndrome in ACC
• Secondary to corticosteroid (cortisol) excess
• Metabolic abnormalities:
• Glucose intolerance/Diabetes
• Osteoporosis/Fractures
• Hypertension
• Immunedeficiency (lymphocytotoxic effect of glucocorticoids)
• Psychiatric disorders
Milan, 02 February 2018 - Post ASCO-GU 2018

Adrenal Glands
Prognostic Roleof Overt Hypercortisolism in Completely Operated
Patients with Adrenocortical Cancer
Alfredo Berruti a,*, Martin Fassnacht b,g, Harm Haak c, Tobias Elsed, Eric Baudine,
Paola Speronef, Matthias Kroissg, Thomas Kerkhofsc, Andrew R. Williamsd, Arianna Arditoh,
Sophie Leboulleuxe, Marco Volantei, Timo Deutschbein g, Richards Feeldersj, Cristina Ronchi g,
Salvatore Grisanti a, Hans Gelderblomk, Francesco Porpiglia l, Mauro Papotti i,
Gary D. Hammer d, Bruno Alloliog, Massimo Terzoloh
aDepartment of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, Spedali Civili Hospital, Brescia, Italy;bDepartment of Internal Medicine IV, University Clinic, Munich, Germany; cInternal Medicine, Maxima Medical Centre, Eindhoven, The Netherlands;dMetabolism, Endocrinology and Diabetes, Department of Internal Medicine, University of Michigan Health System, Ann Arbor, MI, USA; eEndocrine
Oncology and Nuclear Medicine, GustaveRoussy Institute, Villejuif, France; f Department of Oncology, University of Turin, Medical Oncology Unit, San Luigi
Gonzaga Hospital, Orbassano, Italy; gDepartment of Medicine I, Endocrine Unit, University Hospital of Wurzburg, Germany; hDepartment of Clinical and
Biological Sciences, University of Turin, Internal Medicine I, S. Luigi Gonzaga Hospital, Orbassano, Italy; i Department of Oncology, University of Turin,
Pathology Unit, S. Luigi Gonzaga Hospital, Orbassano, Italy; j ErasmusMC, Rotterdam, TheNetherlands; k Department of Clinical Oncology, Leiden University
Medical Center, Leiden, The Netherlands; l Department of Oncology, University of Turin, Urology Unit, S. Luigi Gonzaga Hospital, Orbassano, Italy
EUROPEAN UROLOGY 65 ( 2014) 832–838
avai lable at www.sciencedi rect .com
journal homepage: www.europeanurology.com
Article info
Article history:
Accepted November 4, 2013
Published online ahead of
pr int on November 13, 2013
Keywords:
Adrenocortical cancer
Adjuvant therapy
Cushing syndrome
Mitotane
Abstract
Background: Although prognosticparametersareimportant toguideadjuvant treatment,very
few havebeen identified in patientswith completely resected adrenocortical carcinoma(ACC).
Objective: To assess the prognostic role of clinical symptoms of hypercortisolism in a large
series of patients with completely resected ACC.
Design,setting,andparticipants: Atotal of 524patients followed at referral centersfor ACCin
Europe and the United States entered the study. Inclusion criteria were 18 yr of age, a
histologic diagnosis of ACC, and complete surgery (R0). Exclusion criteria were a history of
other malignancies and adjuvant systemic therapies other than mitotane.
Intervention: All ACCpatientswerecompletely resected, and adjuvant mitotane therapy was
prescribed at the discretion of the investigators.
Outcomemeasurementsand statistical analysis: The primary end point was overall survival
(OS). The secondary end points were recurrence-free survival (RFS) and the efficacy of
adjuvant mitotane therapy according to cortisol secretion.
Resultsand limitations: Overt hypercortisolism wasobserved in197patients(37.6%).Patients
with cortisol excesswereyounger (p=0.002); no differenceaccording to sex and tumor stage
was observed. The median follow-up of the series was 50 mo. After adjustment for sex, age,
tumor stage,and mitotanetreatment, theprognosticsignificanceof cortisol excesswashighly
significant for both RFS (hazard ratio [HR]: 1.30; 95%confidence interval [CI], 1.04–2.62;
p=0.02) and OS(HR: 1.55; 95%CI, 1.15–2.09; p=0.004). Mitotaneadministration wasassoci-
ated with a reduction of diseaseprogression (adjusted HR: 0.65; 95%CI, 0.49–0.86; p=0.003)
that did not differ according to the patient’s secretory status. A major limitation is that only
symptomaticpatientswereconsidered ashavinghypercortisolism,thusexcludinginformation
on the prognostic role of elevated cortisol levels in the absence of a clinical syndrome.
Conclusions: Clinically relevant hypercortisolism is a new prognostic factor in patients with
completely resected ACC.Theefficacy of adjuvant mitotanedoesnot seem tobe influenced by
overt hypercortisolism.
# 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. OncologiaMedica, AziendaOspedalieraSpedali Civili,PiazzaleSpedali Civili
1, 20123 Brescia, Italy. Tel. +39 030 3995410; Fax: +39 030 3700017.
E-mail address: [email protected] (A. Berruti).
0302-2838/$ – see back matter # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.eururo.2013.11.006
Adrenal Glands
Prognostic Roleof Overt Hypercortisolism in Completely Operated
Patients with Adrenocortical Cancer
Alfredo Berruti a,*, Martin Fassnacht b,g, Harm Haak c, Tobias Elsed, Eric Baudine,
Paola Speronef, Matthias Kroissg, Thomas Kerkhofsc, Andrew R. Williamsd, Arianna Arditoh,
Sophie Leboulleuxe, Marco Volantei, Timo Deutschbein g, Richards Feeldersj, Cristina Ronchi g,
Salvatore Grisanti a, Hans Gelderblomk, Francesco Porpiglia l, Mauro Papotti i,
Gary D. Hammer d, Bruno Alloliog, Massimo Terzoloh
aDepartment of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, Spedali Civili Hospital, Brescia, Italy;bDepartment of Internal Medicine IV, University Clinic, Munich, Germany; cInternal Medicine, Maxima Medical Centre, Eindhoven, The Netherlands;dMetabolism, Endocrinology and Diabetes, Department of Internal Medicine, University of Michigan Health System, Ann Arbor, MI, USA; eEndocrine
Oncology and Nuclear Medicine, Gustave Roussy Institute, Villejuif, France; f Department of Oncology, University of Turin, Medical Oncology Unit, San Luigi
Gonzaga Hospital, Orbassano, Italy; gDepartment of Medicine I, Endocrine Unit, University Hospital of Wurzburg, Germany; hDepartment of Clinical and
Biological Sciences, University of Turin, Internal Medicine I, S. Luigi Gonzaga Hospital, Orbassano, Italy; i Department of Oncology, University of Turin,
Pathology Unit, S. Luigi Gonzaga Hospital, Orbassano, Italy; j ErasmusMC, Rotterdam, TheNetherlands; k Department of Clinical Oncology, Leiden University
Medical Center, Leiden, The Netherlands; l Department of Oncology, University of Turin, Urology Unit, S. Luigi Gonzaga Hospital, Orbassano, Italy
EUROPEAN UROLOGY 65 ( 2014) 832–838
avai lable at www.sciencedi rect .com
journal homepage: www.europeanurology.com
Article info
Article history:
Accepted November 4, 2013
Published online ahead of
pr int on November 13, 2013
Keywords:
Adrenocortical cancer
Adjuvant therapy
Cushing syndrome
Mitotane
Abstract
Background: Althoughprognosticparametersareimportant toguideadjuvant treatment,very
few havebeen identified in patientswith completely resected adrenocortical carcinoma(ACC).
Objective: To assess the prognostic role of clinical symptoms of hypercortisolism in a large
series of patients with completely resected ACC.
Design,setting,andparticipants: Atotal of 524 patients followed at referral centersfor ACCin
Europe and the United States entered the study. Inclusion criteria were 18 yr of age, a
histologic diagnosis of ACC, and complete surgery (R0). Exclusion criteria were a history of
other malignancies and adjuvant systemic therapies other than mitotane.
Intervention: All ACCpatients werecompletely resected, and adjuvant mitotane therapy was
prescribed at the discretion of the investigators.
Outcomemeasurements and statistical analysis: The primary end point wasoverall survival
(OS). The secondary end points were recurrence-free survival (RFS) and the efficacy of
adjuvant mitotane therapy according to cortisol secretion.
Resultsand limitations: Overt hypercortisolism wasobserved in 197patients(37.6%).Patients
with cortisol excesswereyounger (p=0.002); no differenceaccording to sex and tumor stage
was observed. The median follow-up of the series was 50 mo. After adjustment for sex, age,
tumor stage, and mitotanetreatment, theprognostic significanceof cortisol excesswashighly
significant for both RFS (hazard ratio [HR]: 1.30; 95%confidence interval [CI], 1.04–2.62;
p=0.02) and OS(HR: 1.55; 95%CI, 1.15–2.09; p=0.004). Mitotaneadministration wasassoci-
ated with a reduction of disease progression (adjusted HR: 0.65; 95%CI, 0.49–0.86; p=0.003)
that did not differ according to the patient’s secretory status. A major limitation is that only
symptomaticpatientswereconsidered ashavinghypercortisolism,thusexcludinginformation
on the prognostic role of elevated cortisol levels in the absence of a clinical syndrome.
Conclusions: Clinically relevant hypercort isolism is a new prognostic factor in patients with
completely resected ACC.Theefficacy of adjuvant mitotanedoesnot seem tobe influenced by
overt hypercortisolism.
# 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. OncologiaMedica,AziendaOspedalieraSpedali Civili,PiazzaleSpedali Civili
1, 20123 Brescia, Italy. Tel. +39 030 3995410; Fax: +39 030 3700017.
E-mail address: [email protected] (A. Berruti).
0302-2838/$ – see back matter # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.eururo.2013.11.006
Berruti et al. Eur Urol 2014, 65:832-838
Domanda ECM !
Milan, 02 February 2018 - Post ASCO-GU 2018
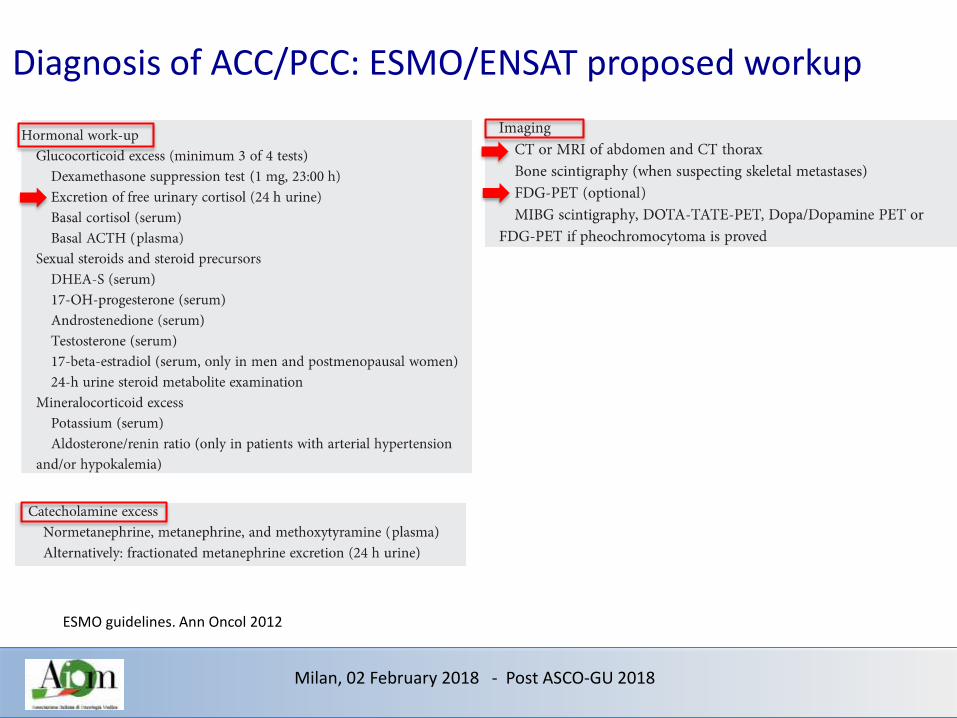
Diagnosis of ACC/PCC: ESMO/ENSAT proposed workup
ESMO guidelines. Ann Oncol 2012
Milan, 02 February 2018 - Post ASCO-GU 2018

Slide 14
Presented By Tobias Else at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Slide 15
Presented By Tobias Else at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Metirapone

Metyrapone is the fastest drug in controlling Cushing’s disease
Claps et al. Endocrine 2017
Milan, 02 February 2018 - Post ASCO-GU 2018

Abiraterone on biosynthesis of steroidal hormones
Veytsman et al. J Clin Oncol 2009
Milan, 02 February 2018 - Post ASCO-GU 2018

Abiraterone in Cushing’s syndrome: the Abacus trial
Milan, 02 February 2018 - Post ASCO-GU 2018

Genetic considerations
Presented By Tobias Else at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Slide 17
Presented By Tobias Else at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Slide 18
Presented By Tobias Else at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Milan, 02 February 2018 - Post ASCO-GU 2018
Strategies of treatment of PCC Adjuvant treatment of ACC Treatment of M+ ACC Neoadjuvant treatment of ACC

Malignant Phaeochromocytoma (and Paraganglioma) 2#
Presented By David Quinn at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

What is the prognosis of ACC?
Most of papers on ACC start with … “poor”
Oncotarget43016www.impactjournals.com/oncotarget
w w w .im pact journals.com / oncotarget / Oncotarget , Vol. 6 , No. 4 0
I nhibit ion of the Tcf/ beta- catenin com plex increases apoptosis
and im pairs adrenocort ical tum or cell proliferat ion and adrenal
steroidogenesis
Let ícia F. Leal1 , Ana Carolina Bueno1 , Débora C. Gom es1 ,2 , Rafael Abduch 1,
Margaret de Castro3, Sonir R. Antonini1
1Department of Pediatrics, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto, Sao Paulo, Brazil
2Department of Pediatrics, School of Medicine, Federal University of Uberlandia, Uberlândia, Minas Gerais, Brazil
3Department of Internal Medicine, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto, Sao Paulo, Brazil
Correspondence to:
Sonir R. Antonini, e- m ail: [email protected]
Keywords: adrenoc ortic a l c anc er, beta -c a tenin, steroidogenesis, apop tosis, ta rgeted therapy
Received: April 13, 2015 Accepted: September 05, 2015 Published: Oc tober 16, 2015
ABSTRACT
Background: To date, there is no effect ive therapy for pat ients w ith advanced/
metastatic adrenocortical cancer (ACC). The activation of the Wnt/ beta-catenin
signaling is frequent in ACC and this pathw ay is a prom ising therapeut ic target .
Aim: To investigate the effects of the inhibition of the Wnt/ beta-catenin in ACC cells.
Methods: Adrenal (NCI -H295 and Y1) and non-adrenal (HeLa) cell lines were
t reated w ith PNU- 7 4 6 5 4 ( 5–2 0 0 μM) for 2 4–9 6 h to assess cell viability ( MTS-based
assay) , apoptosis (Annexin V) , expression/ localization of beta-catenin (qPCR,
immunofluo rescence, immunocytochemistry and western blot) , expression of
beta-catenin target genes (qPCR and western blot) , and adrenal steroidogenesis
( radioim m unoassay, qPCR and w estern blot ) .
Results: I n NCI - H2 9 5 cells,PNU- 7 4 6 5 4 significa nt l y decreased cell proliferat ion
96 h after treatment, increased early and late apoptosis, decreased nuclear beta-
catenin accumulation, impaired CTNNB1/ beta-catenin expression and increased beta-
catenin target genes 48 h after treatment. No effects were observed on HeLa cells.
I n NCI -H295 cells, PNU-74654 decreased cortisol, testosterone and androstenedione
secretion 24 and 48 h after treatment. Additionally, in NCI -H295 cells, PNU-74654
decreased SF1 and CYP2 1 A2 m RNA expression as w ell as the protein levels of STAR
and aldosterone synthase 48 h after treatment. I n Y1 cells, PNU-74654 impaired
cort icosterone secret ion 2 4 h after t reatm ent but did not decrease cell viability.
Conclusions: Blocking the Tcf/ beta-catenin complex inhibits the Wnt/ beta-catenin
signaling in adrenocortical tumor cells triggering increased apoptosis, decreased
cell viability and impairment of adrenal steroidogenesis. These promising find i ngs
pave the way for further experiments inhibiting the Wnt/ beta-catenin pathway in
pre-clinical models of ACC. The inhibition of this pathway may become a promising
adjuvant therapy for pat ients w ith ACC.
INTRODUCTION
The management of patients with adrenocortical
carcinomas (ACCs) remains a challenge and patients
with invasive, metastatic or recurrent disease have a poor
prognosis [1, 2]. Although significa nt progress has been
achieved in recent years both in basic and clinical research,
adjuvant therapeutic options for patients with ACC remain
very limited [3]. Mitotane (M), the firs t line adjuvant
treatment, is highly toxic and its combination with
etoposide, doxorubicin, and cisplatin (EDP) is generally
ineffective and almost all patients will experience disease
Milan, 02 February 2018 - Post ASCO-GU 2018

Target therapy in ACC: at best stable disease
Fassnacht et al. J Clin Endocrinol Metab 2013
• Wrong disease?
• Wrong patient setting/marker?
• Wrong drugs?
Milan, 02 February 2018 - Post ASCO-GU 2018

Immunotherapy
Fay et al. J Immunother Cancer 2015
Milan, 02 February 2018 - Post ASCO-GU 2018

Failure of immunotherapy
Tissier et al. Cancer Res 2005
Spranger et al. Nature 2015
Milan, 02 February 2018 - Post ASCO-GU 2018

• Up to 80% of radically operated patients relapse within 2 years
• Risk factors for relapse • Stage: I-II vs III • Radicality: R0 vs R1 • Ki67: <10% vs >10%
• This observation represents the rationale for adjuvant treatments
Risk of relapse in R0-R1 operated ACC
Berruti et al. J Clin Oncol 2012
Milan, 02 February 2018 - Post ASCO-GU 2018

ESMO algorythm for adjuvant strategies
• First, consider resection status (R0 vs R1-R2)
• Second, consider stage (I-II vs III) and Ki67 (<10% vs >10%)
Berruti et al. Ann Oncol 2012
Milan, 02 February 2018 - Post ASCO-GU 2018

Milan, 02 February 2018 - Post ASCO-GU 2018

ESMO algorythm for adjuvant strategies
Berruti et al. Ann Oncol 2012
• “patients with potential residual disease (R1 or Rx resection) and/or Ki67 more than 10% should be offered adjuvant mitotane”
• Caveat: No randomized trials in this setting!
Milan, 02 February 2018 - Post ASCO-GU 2018

Adjuvant Mitotane for operated ACC
• Retrospective analysis of two cohorts
• Median RFS 42 vs 10/25 months, p <0.001
• Median OS 110 vs 52 (p 0.01) and 67 (p 0.10) months
Terzolo et al. NEJM 2007
47 Italian pts
75 German pts
55 Italian pts
Milan, 02 February 2018 - Post ASCO-GU 2018

Adjuvant Mitotane for operated ACC: update 2017
Berruti et al. J Clin Endocrinol Metab 2017
Milan, 02 February 2018 - Post ASCO-GU 2018

What is Mitotane?
D-D-D
D-D-T
Milan, 02 February 2018 - Post ASCO-GU 2018

Toxicity of Mitotane
Allolio et al. J Clin Endocrinol Metab 2006
Milan, 02 February 2018 - Post ASCO-GU 2018

• The so called “therapeutic range” (14-20 mg/ml) is attained within 2-3 months
• Question: Is Mitotane adequate for an ACC with high proliferative activity (Ki67)?
Major drawback of adjuvant mitotane
Milan, 02 February 2018 - Post ASCO-GU 2018

Adjuvant chemotherapy for adrenocortical carcinoma: a multicenter randomized open label phase III trial: the ACACIA trial
Italian Agency of Medicine 2016 call
Funded !!!
Adiuvant Chemotherapy for Adrenocortical CarcInomA
Milan, 02 February 2018 - Post ASCO-GU 2018

Metastatic pattern of ACC
• Majority of ACC with tumor extending beyond the adrenal
• Lungs (45%)
• Liver (42%)
• Lymphnodes (24%)
• Bone, pancreas, spleen, diaphragm, peritoneum
Milan, 02 February 2018 - Post ASCO-GU 2018

Strategy for inoperable/metastatic ACC
• Backbone of treatment is mitotane or chemo + mitotane
+ local regional options
EDP-M for non secreting ACC
EDP-M-M for secreting ACC
Milan, 02 February 2018 - Post ASCO-GU 2018

EDP efficacy the FIRM-ACT trial: the first phase III trial in ACC
Fassnacht et al. NEJM 2012
Milan, 02 February 2018 - Post ASCO-GU 2018

The FIRM-ACT trial: >300 ACC patients randomized
Fassnacht et al. NEJM 2012
Crossover permitted at PD
Milan, 02 February 2018 - Post ASCO-GU 2018

The FIRM-ACT trial: results
Fassnacht et al. NEJM 366(23):2189-97; 2012
EDP-M median PFS: 5.0 months
Sz-M median PFS: 2.1 months
EDP-M median OS: 14.8 months
Sz-M median OS: 12.0 months
Milan, 02 February 2018 - Post ASCO-GU 2018

At 18 months pts without PD
EDP-M 16.5%
Sz-M 5.2%
Milan, 02 February 2018 - Post ASCO-GU 2018

What is the advantage of combining mitotane and chemo?
Chemo effect
Mitotane maintenance
Chemotherapy can obtain a disease control when mitotane levels is not in the therapeutic range
ACC highly-proliferative: chemotherapy activity predominant
ACC slowly-proliferative: mitotane activity predominant
Milan, 02 February 2018 - Post ASCO-GU 2018

Stesso approccio in neoadiuvante
Metabolic downstaging
Tumor volume downstaging
Ki67 60% Ki67 12%
Milan, 02 February 2018 - Post ASCO-GU 2018

Big successes in clinical oncology & survival @ 2 years a provocative slide
M+ cancer First author Drug/Schedule OS @ 2 yrs Journal/Year
Breast Her2+ Baselga D + Trast + Pert 80% NEJM 2012
Lung Alk+ Shaw Crizotinib 50% NEJM 2013
Adrenal Fassnacht EDP-M 30% NEJM 2012
Glioblastoma Stupp RT + TMZ 26% NEJM 2005
Melanoma Robert Ipilimumab 18% NEJM 2011
Gastric Van Cutsem DCF 18% JCO 2006
Pancreas Conroy Folfirinox 12% NEJM 2011
Milan, 02 February 2018 - Post ASCO-GU 2018

What is the prognosis of ACC?
Most of papers on ACC start with … “poor”
Oncotarget43016www.impactjournals.com/oncotarget
w w w .im pact journals.com / oncotarget / Oncotarget , Vol. 6 , No. 4 0
I nhibit ion of the Tcf/ beta- catenin com plex increases apoptosis
and im pairs adrenocort ical tum or cell proliferat ion and adrenal
steroidogenesis
Let ícia F. Leal1 , Ana Carolina Bueno1 , Débora C. Gom es1 ,2 , Rafael Abduch 1,
Margaret de Castro3, Sonir R. Antonini1
1Department of Pediatrics, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto, Sao Paulo, Brazil
2Department of Pediatrics, School of Medicine, Federal University of Uberlandia, Uberlândia, Minas Gerais, Brazil
3Department of Internal Medicine, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto, Sao Paulo, Brazil
Correspondence to:
Sonir R. Antonini, e- m ail: [email protected]
Keywords: adrenoc ortic a l c anc er, beta -c a tenin, steroidogenesis, apop tosis, ta rgeted therapy
Received: April 13, 2015 Accepted: September 05, 2015 Published: Oc tober 16, 2015
ABSTRACT
Background: To date, there is no effect ive therapy for pat ients w ith advanced/
metastatic adrenocortical cancer (ACC). The activation of the Wnt/ beta-catenin
signaling is frequent in ACC and this pathw ay is a prom ising therapeut ic target .
Aim: To investigate the effects of the inhibition of the Wnt/ beta-catenin in ACC cells.
Methods: Adrenal (NCI -H295 and Y1) and non-adrenal (HeLa) cell lines were
t reated w ith PNU- 7 4 6 5 4 ( 5–2 0 0 μM) for 2 4–9 6 h to assess cell viability ( MTS-based
assay) , apoptosis (Annexin V) , expression/ localization of beta-catenin (qPCR,
immunofluo rescence, immunocytochemistry and western blot) , expression of
beta-catenin target genes (qPCR and western blot) , and adrenal steroidogenesis
( radioim m unoassay, qPCR and w estern blot ) .
Results: I n NCI - H2 9 5 cells,PNU- 7 4 6 5 4 significa nt l y decreased cell proliferat ion
96 h after treatment, increased early and late apoptosis, decreased nuclear beta-
catenin accumulation, impaired CTNNB1/ beta-catenin expression and increased beta-
catenin target genes 48 h after treatment. No effects were observed on HeLa cells.
I n NCI -H295 cells, PNU-74654 decreased cortisol, testosterone and androstenedione
secretion 24 and 48 h after treatment. Additionally, in NCI -H295 cells, PNU-74654
decreased SF1 and CYP2 1 A2 m RNA expression as w ell as the protein levels of STAR
and aldosterone synthase 48 h after treatment. I n Y1 cells, PNU-74654 impaired
cort icosterone secret ion 2 4 h after t reatm ent but did not decrease cell viability.
Conclusions: Blocking the Tcf/ beta-catenin complex inhibits the Wnt/ beta-catenin
signaling in adrenocortical tumor cells triggering increased apoptosis, decreased
cell viability and impairment of adrenal steroidogenesis. These promising find i ngs
pave the way for further experiments inhibiting the Wnt/ beta-catenin pathway in
pre-clinical models of ACC. The inhibition of this pathway may become a promising
adjuvant therapy for pat ients w ith ACC.
INTRODUCTION
The management of patients with adrenocortical
carcinomas (ACCs) remains a challenge and patients
with invasive, metastatic or recurrent disease have a poor
prognosis [1, 2]. Although significa nt progress has been
achieved in recent years both in basic and clinical research,
adjuvant therapeutic options for patients with ACC remain
very limited [3]. Mitotane (M), the firs t line adjuvant
treatment, is highly toxic and its combination with
etoposide, doxorubicin, and cisplatin (EDP) is generally
ineffective and almost all patients will experience disease
Milan, 02 February 2018 - Post ASCO-GU 2018

Conclusioni
• La prognosi ATTUALE dei pazienti con ACC è severa perché:
• Intrinsecamente malattia aggressiva • È rara • È trattata in modo inadeguato dagli endocrinologi • È trattata in modo inadeguato dagli oncologi • La chirurgia deve essere dedicata
• La chirurgia R0 rimane l’elemento terapeutico decisivo
• Considerare CT neoadiuvante
• Considerare sempre l’associazione di terapia endocrina + oncologica
• Importanza dei centri di riferimento e della collaborazione internazionale
Milan, 02 February 2018 - Post ASCO-GU 2018

ACC epidemiology: very, very, very rare disease
• Annual incidence: (adult) 0.5-2.0 case per million people per year
(children) 0.2-0.3 case per million people per year
• Ratio Male/Female: 1 : 1.5
• Bimodal age distribution: First peak < 10 years
Second peak 4°-5° decade (mean age 45)
Milan, 02 February 2018 - Post ASCO-GU 2018

UNIBS
Milan, 02 February 2018 - Post ASCO-GU 2018

Thanks! ACC Fans Brescia Medical Oncology Alfredo Berruti Sara Cerri Deborah Cosentini Melanié Claps Andrea Crema Laura Ferrari Vittorio Ferrari Barbara Lazzari Experimental Pharmacology Silvia Beretta Sandra Sigala Internal Medicine & Endocrinology Maurizio Castellano Surgery Department Guido M. A. Tiberio Pathology Department Simona Fisogni Luigi P Poliani Fabio Facchetti













![adrenal cbc.ppt [Somente leitura] - cbcsp.org.br · 0 - 2: Comportamento benigno 3 ou +: Comportamento maligno ... Cisto de Adrenal / mielolipoma 4. Sd . Cushing 5. Incidentaloma](https://img.dokumen.tips/doc/110x75/5be3b64609d3f219598bb6dc/adrenal-cbcppt-somente-leitura-cbcsporgbr-0-2-comportamento-benigno.jpg)















