Embed Size (px)
Citation preview

Adolescents´ sleep in a 24/7 society

to my family
Örebro Studies in Psychology 37
SERENA BAUDUCCO
Adolescents´ sleep in a 24/7 society Epidemiology and prevention

© Serena Bauducco, 2017
Title: Adolescents´ sleep in a 24/7 society. Epidemiology and prevention.
Publisher: Örebro University 2017 www.oru.se/publikationer-avhandlingar
Print: Örebro University, Repro 08/2017
ISSN 1651-1328 ISBN 978-91-7529-202-1
Cover photo: Gabriel Berg

Abstract
Serena Bauducco (2017): Adolescents´ sleep in a 24/7 society. Epidemiology and prevention. Örebro Studies in Psychology 37.
Sleep undergoes important changes during adolescence and many teenagers experience problems sleeping. These in turn affect adolescents´ academic, physical and psychosocial functioning. Moreover, there are some indica-tions that sleep problems in this age group may be increasing, possibly as a consequence of societal changes, e.g., internet availability. Research on ad-olescents´ sleep is growing, but more epidemiological studies are needed to clarify the prevalence of poor sleep, long and short-term outcomes associ-ated with it, and potential risk and protective factors to target in preventive interventions. The aim of this dissertation was to contribute to each of these goals; Study I investigated the longitudinal association between sleep prob-lems, defined as symptoms of insomnia, and school absenteeism; Study II explored the prevalence of poor sleep, defined as sleep deficit, in an adoles-cent population and psychosocial and contextual factors associated with it, including emotional and behavioral problems, stress, sleep hygiene and technology use; finally, Study III evaluated the short-term effects of a novel universal school-based intervention to improve adolescents´ sleep health.
The findings show that poor sleep was strongly related to adolescents´ functioning, including emotional and behavioral problems and school at-tendance, and that sleep deficit was prevalent in adolescents. This supports the need for prevention. Moreover, sleep deficit was associated with stress, technology use and arousal at bedtime, which may represent important bar-riers to sleep. A preventive intervention targeting these barriers to promote adolescents´ sleep health was successful with the individuals most at risk. However, it remains to be seen whether these changes will be maintained after the intervention and whether incidence of sleep problems will be lower relative to a control group. Implications for theory and practice are dis-cussed.
Keywords: Sleep problems, adolescents, sleep deficit, insomnia, sleep duration, technology, stress, prevention, epidemiology.
Serena Bauducco, School of Law, Psychology and Social Work Örebro University, SE-701 82 Örebro, Sweden, [email protected]


Acknowledgements First, I would like to thank my supervisors, Seven J. Linton and Ida Flink. Thank you for your support, your feedback, questions and encouragement. Steven, thank you for sharing your immense knowledge and experience and thank you for reminding me of the real world sometimes. Ida, thank you for your pragmatic approach, it has helped me forward when I felt stuck.
I would also like to thank Maria Tillfors. As a PhD student, you really need someone to check up on you, whether it is about your PhD journey or real life…and someone you can talk to about fluffy cats. So, thank you Ma-ria, you have been a great emotional support!
Another person I would like to thank is Katja Boersma. I think I should say this more often: Thank you! We would not have this amazing project without your hard work and I am very grateful that you have put your heart and soul into making it work.
Thank you Lauree Tilton-Weaver for your hard work with the data. I really enjoyed your courses, talking about statistics and animals with you and of course, the pumpkin cake!
Thank you Markus Jansson-Fröjmark for the collaboration on Study II and for interesting and stimulating discussions.
Talking about the project that has made this dissertation possible, I want to thank Jimmy, Roda, Jessica, Nikie, Sara N., and Minnia and all the stu-dents that have helped out throughout the years. Especially Kimberley, Mar-tina, Nadine, Elin, Sanna and Helena who helped me out with the sleep intervention, together with Jessica and Sara.
I also want to thank all the participants and their parents, I hope that the results from all the hard work will benefit you and all sleepy teens out there.
I also want to thank all the colleagues who make my workdays more interesting and fun; thank you Hisyar, David, John, Jan, Maria H., Reza, Sevgi, Metin, Håkan, Delia, Martien. Thank you Metin and Håkan for be-lieving in me very early on, I wouldn´t have started this journey without your encouragement. Delia, thank you for our long chats like real Italian “portinaie”. John, thank you for the language help, the discussions about life, and the nights out! Martien, thank you for the precious feedback at my half time seminar, you are a great researcher and a fun person to be around, how does that go together??
Selma and Sofia, from fellow doctoral students to bosses. You are cool and a source of inspiration! Thank you for your support.
This journey can be quite lonely at times and I am happy to have shared it with my fellow (some ex-) PhD-students, Elin, Linnea, Farzaneh, Ni-loufar, Tatiana, Nanette, Annika, Darun, Johan, Mika, Sara, Matilda, Ma-lin and Kelly (although close to being senior, we have accepted you in our club!). Thank you for our refreshing lunches, occasional frustration-spit-outs, and reality-checks.
Matilda, you deserve a special thank you, your door has always been open for me and I love discussing weird - and maybe unrealistic - but cer-tainly fun future plans with you!
Malin, I would not even have a dissertation if it wasn´t for you. My whole life would probably not be functioning without you! And I agree that this acknowledgements section should have been 2/3 about you, but I am trying to be politically correct here. Thank you for being there for me! I am so grateful to have shared this journey – the hard work, the doubts, the trips, the moments of joy – with you, from the very beginning. You are a beautiful friend and you will not get rid of me!
I also want to thank two amazing people I have met during my studies. Maria L., thank you for your support and friendship, you are a great prob-lem solver and a wonderful person. Mika, thank you for being you, for lis-tening to me and baking the best Key lime pie.
Finally, I want to thank those on “the other side”, who remind me that there is more fun to life than work.
Peplis, Felicia and the Nordkvist family, thank you for the best “mind-fulness sessions”. I don´t know any better way to recharge my batteries.
Thank you, family, old and new members, for always believing in me. Thank you friends, you might not always know exactly what I am doing, but you are always there for me!
Last but not least I want to thank Gabriel, this dissertation would have been an impossible task without your support. You have been patient and taken care of me when I needed to work just a bit harder. You have listened to me when I doubted myself, baked cakes, made dinner and distracted me from work when I needed it. You are my home, and I look forward to our next adventure.

List of studies The dissertation is based on the following studies, which hereafter will be referred to in the text by their Roman numerals:
I. Bauducco, S. V., Tillfors, M., Özdemir, M., Flink, I. K., & Linton, S. J. (2015). Too tired for school? The effects of insomnia on ab-senteeism in adolescence. Sleep Health, 1(3), 205-210.
II. Bauducco, S. V., Flink, I. K., Jansson-Fröjmark, M., & Linton, S. J. (2016) Sleep duration and patterns in adolescents: Correlates and the role of daily stressors. Sleep Health, 2(3), 211-218.
III. Bauducco, S. V., Flink, I. K., & Linton, S. J. Making room for sleep: The evaluation of a preventive school-based program to im-prove adolescents´ sleep. Manuscript submitted for publication.
Studies I and II were reprinted with kind permission of Elsevier.

List of abbreviations ASHS Adolescent Sleep Hygiene Scale ASQ Adolescent Stress Questionnaire BNSQ Basic Nordic Sleep Questionnaire BT Bedtime CES-DC Center for Epidemiologic Studies-Depression Child DST Delayed Sleep Timing DSWPD Delayed Sleep-Wake Phase Disorder FoMO Fear of Missing Out I-Change Model Integrated Model for motivation and behavioral change ICT Information and Communication Technology MI Motivational Interviewing NSF National Sleep Foundation OASIS Overall Anxiety Severity and Impairment Scale PSS Perceived Stress Scale SCN Suprachiasmatic nucleus SOL Sleep Onset Latency SPSQ-C Social Phobia Screening Questionnaire – Children SSHS School Sleep Habits Survey TIB Time in Bed TST Total Sleep Time WASO Wake After Sleep Onset WT Wake Time

Table of Contents
INTRODUCTION .................................................................................. 13 Normal sleep development in adolescence ............................................... 14
Biological changes ............................................................................... 15 Psychosocial and contextual changes .................................................. 16
Sleep Disturbances in Adolescence .......................................................... 17 Why is it important? Sleep and adolescents´ functioning ......................... 19
Emotional and behavioral problems.................................................... 19 School performance and attendance .................................................... 20
State of the art: Summary and implications ............................................. 21 What can we do about it? Preventing sleep deficit in adolescents ............ 22
Risk and protective factors .................................................................. 23 Sleep Hygiene ...................................................................................... 23 Information and communication technology (ICT) ............................ 23 Parents and peer influence .................................................................. 25 Academic demands, extracurricular activities and stress ..................... 26 Previous school-based interventions .................................................... 27 Sleep education ................................................................................... 28 Sleep education + Skills training .......................................................... 28 Sleep education + Skills training + Motivation to change .................... 29 Theoretical approach to behavioral change ......................................... 29 The Integrated Model for motivation and behavioral change (I-Change) ............................................................................................... 30
Motivational Interviewing (MI) to promote behavioral change ...... 32 Next step: Improving existing programs ............................................. 32
Summary and aims .................................................................................. 33 Specific aims ........................................................................................ 34
SHORT DESCRIPTION OF THE STUDIES .......................................... 35
STUDY I ................................................................................................. 35 Introduction ........................................................................................ 35 Aim ..................................................................................................... 35 Overview of the design ........................................................................ 35 Participants ......................................................................................... 35 Measures ............................................................................................. 35 Analyses .............................................................................................. 36
Results ................................................................................................. 36 Table 1 ................................................................................................ 37 Conclusions ......................................................................................... 36
STUDY II ................................................................................................ 38 Introduction ........................................................................................ 38 Aim ..................................................................................................... 38 Overview of the design ........................................................................ 38 Participants ......................................................................................... 39 Measures ............................................................................................. 39 Analyses .............................................................................................. 39 Results ................................................................................................. 40 Table 2 ................................................................................................ 42 Conclusions ......................................................................................... 41
STUDY III ............................................................................................... 43 Introduction ........................................................................................ 43 Aim ..................................................................................................... 43 Overview of the design ........................................................................ 43 Participants ......................................................................................... 44 Intervention ......................................................................................... 44 Measures ............................................................................................. 45 Weekly measures ................................................................................. 45 Pre- post-measures. ............................................................................. 45 Analyses .............................................................................................. 45 Results ................................................................................................. 45 Conclusions ......................................................................................... 46
GENERAL DISCUSSION ....................................................................... 48 Answer to the research questions............................................................. 48 Findings in relation to the theoretical framework .................................... 53 Implications ............................................................................................. 56 Future research ........................................................................................ 58 Methodological strengths and weaknesses ............................................... 60 Summary and concluding remarks........................................................... 61 Conclusions ............................................................................................. 62
REFERENCES ........................................................................................ 64

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
13
Introduction Developing individuals – humans and animals alike – show a greater sleep need compared to fully mature individuals (Dahl & Lewin, 2002). How-ever, many adolescents do not sleep enough, and this has serious conse-quences on academic, psychosocial, and physical functioning. While interest in adolescents´ sleep is growing, we still need to know more about preva-lence, long-term consequences, and potential risk and protective factors to be targeted to improve adolescents´ sleep health.
From a developmental perspective, changes in sleep patterns during ado-lescence (roughly between 10 years old and early 20s) are quite normal and most adolescents will experience difficulties falling asleep and daytime sleepiness at some time point. Sleep alterations in adolescence are due to both biological and psychosocial changes typical of this developmental pe-riod. Once adolescents reach maturation around early adulthood (i.e., in their 20s), sleep duration generally increases again before declining once more later on, during the 30s (Maslowsky & Ozer, 2014). Nevertheless, even though sleep problems may be temporary and normal, both short and long-term consequences of poor sleep are worrisome. Adolescents who sleep poorly in terms of both quality and quantity, are more depressed and anx-ious, more irritable, have worse school achievement, worse physical health, and engage more in risky behaviors (Gregory & Sadeh, 2012).
In addition to developmental trends in adolescence, there are indications of a general decline in sleep duration and quality over the last decades (Keyes, Maslowsky, Hamilton, & Schulenberg, 2015; Kronholm et al., 2015; Matricciani, Olds, & Petkov, 2012). These changes have been hy-pothesized as a byproduct of the modern lifestyle, including the unlimited possibilities offered by electronic media, such as smartphones, computers, television, music players, tablets, and video game consoles (Hale & Guan, 2015). About 97% of adolescents in the US as well as Sweden have access to at least one device in their bedroom and thus have the possibility to be connected and busy round-the-clock (Hale & Guan, 2015; Medieråd, 2015). Therefore, there is a need to identify risk factors that exacerbate re-duced sleep duration, to investigate the consequences of sleep deficit, and thereafter find a way to counteract this sleep decline.
The aim of this dissertation is to contribute to each of these goals, from epidemiology to prevention. Study I investigates sleep absenteeism as a long-term functional consequence of poor sleep (defined as symptoms of insom-nia). Study II explores the prevalence and distribution of insufficient sleep

14
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
duration among early adolescents, and psychosocial and contextual factors associated with sleep deficit, including emotional and behavioral problems, stress, technology and cognitive-emotional arousal at bedtime. Finally, Study III evaluates the short-term effects of a novel school-based sleep in-tervention.
Normal sleep development in adolescence
Fig. 1. The biopsychosocial model of sleep. Reproduced from Becker et al., 2015 with permission.
Sleep need does not decrease significantly from childhood to adolescence and the recommended sleep duration for adolescents (13-17 years), is be-tween eight and ten hours of sleep per night (Hirshkowitz et al., 2015). Ac-cordingly, experimental studies show that, if left undisturbed, adolescents consistently sleep about nine hours per night (Giannotti, Cortesi, & Carskadon, 2002). However, as described in the biopsychosocial model of sleep (Becker, Langberg, & Byars, 2015) biological, contextual and psycho-social changes contribute to adolescents´ preference for later bedtimes. This delay in bedtimes, combined with early school start times, leads to a weekly sleep deficit that adolescents often try to compensate for during weekends

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
15
and holidays. In turn, this shift in sleep timing between weekdays and week-ends can be problematic, as it might lead to disorganized sleep patterns and maintenance of the sleep debt.
Developmental trajectories of sleep duration show a decrease from child-hood to adolescence, and then an increase in later adolescence (from age 19) – likely due to maturation and contextual changes, such as more flexible school start times (Maslowsky & Ozer, 2014).
Biological changes The two regulatory processes of sleep – the circadian and the homeostatic processes (Borbély, 1982) – work independently, but their interaction is re-sponsible for our daily sleep regulation (Carskadon, 2011). The circadian rhythm is an internal mechanism regulating sleep-wake behaviors during the 24-h period. This is controlled by the suprachiasmatic nucleus (SCN) in the hypothalamus, which is sensitive to environmental cues such as daylight. The SCN also affects the release of the melatonin hormone, as well as body temperature, which are also both important for sleep regulation (Dahl & Lewin, 2002). The homeostatic process is responsible for the “sleep pres-sure” that accumulates when we are awake and reduces when we sleep (Crowley, Acebo, & Carskadon, 2007). At the onset of puberty, a prefer-ence for a later circadian phase emerges and adolescents feel more awake and active during the evening (‘eveningness’ as opposed to ‘morningness’). Similarly, homeostatic sleep pressure accumulates more gradually in teen-agers compared to children, resulting in teenagers feeling alert until later hours (Carskadon, Acebo, & Jenni, 2004). So, taken together, these changes in the homeostatic and circadian systems lead to a so-called ‘delayed sleep timing’ (DST) – a delay in both sleep and wake times (Carskadon et al., 2004). This would not be a problem if adolescents did not need to attend early morning school schedules, but, because late mornings are not possible, delayed bedtimes in combination with school obligations lead to shortened sleep duration (Carskadon, 2011). Furthermore, there is no evidence that adolescents need less sleep (e.g., as compared to before puberty). On the contrary, daytime sleepiness increases during adolescence (Dahl & Lewin, 2002).
As a consequence, many adolescents tend to enjoy late bedtimes and long sleep mornings when they have a chance; during holidays and weekends. This, however, creates a disorganized sleep pattern similar to jetlag and therefore commonly referred to as “social jetlag” (Wittmann, Dinich, Mer-row, & Roenneberg, 2006). During the school week, waking up early in the

16
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
morning and falling asleep at night might become a struggle, because the body is not ready to wake up at low temperature and high melatonin levels (Dahl & Lewin, 2002).
As the term social jetlag suggests, in addition to the biological changes pushing bedtimes to later hours, adolescents have many reasons to stay up later in the evenings, including socializing with peers, modern society´s un-limited entertainment possibilities, and school and family obligations.
Psychosocial and contextual changes Teenagers go through important changes in their social lives, including re-negotiating their relationship with parents, experimenting with new social interactions (including friendships and romantic relationships), and balanc-ing their free time with increasing academic demands. No wonder many define adolescence as a stressful period (Casey et al., 2010).
As part of the parent-child autonomy negotiation, adolescents might gain the ability to decide upon their bedtimes, which, not surprisingly, is associ-ated with later bedtimes (Short et al., 2011).
In addition, the access to electronic media provides unlimited opportuni-ties for social interaction and entertainment around-the-clock (Przybylski et al., 2013). In fact, adolescents often report a desire to sleep more but a lack of time to do so; they often prioritize other activities, including obligations and more rewarding activities, over sleep (Cassoff, Knäuper, Michaelsen, & Gruber, 2013).
Moreover, it might not only be the lack of time that gets in the way of teenagers’ sleep but also the emotional turmoil that they often experience. Brain maturation, together with the increase in stressors (Byrne, Davenport, & Mazanov, 2007), contribute to heightened emotional reactivity during adolescence (Casey et al., 2010) and this state of arousal is antithetical to the feelings of tranquility necessary to fall asleep (Dahl & Lewin, 2002).
While some of these changes are part of normal development (e.g., au-tonomy negotiation, social turmoil), others might be exacerbated by societal changes towards a 24/7 society such as pervasive use of technology, higher academic demands and an increase in stress (Keyes et al., 2015), which might explain the secular trends towards a general reduction in sleep dura-tion (Keyes et al., 2015; Kronholm et al., 2015; Matricciani et al., 2012). However, we do not know enough about these risk factors and their con-tribution to sleep problems in adolescence, over and above biological changes. Some of the psychosocial and contextual factors more central to

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
17
this dissertation will be discussed further in the section Risk and protective factors.
To conclude, sleep problems lie on a continuum between normal and pathological, that is, some adolescents are able to cope with the normal changes in sleep patterns, but some develop chronic problems. When does sleep become problematic in adolescence?
Sleep Disturbances in Adolescence The most common sleep disturbances during adolescence are sleep depriva-tion, insomnia, and Delayed Sleep-Wake Phase. Delayed Sleep-Wake Phase Disorder (DSWPD) is defined as a chronic inability to fall asleep and wake up at desired times, which causes significant impairment and distress (Amer-ican Psychiatric Association, 2013). In adolescents suffering from DSWPD, sleep timing is not synchronized with social obligations (e.g., school start times) and thus impairs academic and social functioning (Auger & Crowley, 2013). An important characteristic of DSWPD is that, when allowed to de-lay the sleep timing (bedtimes and wake times), individuals with DSWPD show adequate sleep duration and quality (Crowley et al., 2007). Only a small portion of adolescents fulfill the criteria for DSWPD (American Psy-chiatric Association, 2013). Estimates range between 0,13-7% (Auger & Crowley, 2013) but there is a high risk of overestimation due to imprecise measurements that only take into consideration one criterion, which is de-layed sleep timing (DST) (see Lovato, 2013). Therefore, showing a social jetlag pattern during weekends might be an indication of DSWPD, but is not enough to establish a diagnosis (e.g., in the absence of daytime impair-ment). In order to ensure a diagnosis, it is necessary to verify the stability of the delayed sleep pattern (>2 hours discrepancy between weekday and weekend wake times) by registering sleep patterns continuously for at least one week (including the weekend), to rule out any alternative explanations (e.g., insomnia) (Auger & Crowley, 2013).
Symptoms of insomnia are prominent in individuals with DSWPD, espe-cially sleep-onset insomnia (Gradisar, Gardner, & Dohnt, 2011). However, it is possible to distinguish between DSWPD and insomnia because sleep-onset insomnia symptoms are not schedule-specific (Auger & Crowley, 2013). That is, adolescents with insomnia would have difficulties falling asleep even if they self-selected their bedtime, whereas DSWPD adolescents would be able to fall asleep at their preferred bedtime. Insomnia is defined as difficulties falling asleep, maintaining sleep, and waking up too early at

18
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
least 3 nights per week for at least 3 months, which causes severe impair-ment during the day (e.g., in school) (American Psychiatric Association, 2013). Between 7-24% of adolescents fulfill this diagnosis (Dohnt, Gradisar, & Short, 2012; Hysing, Pallesen, Stormark, Lundervold, & Sivertsen, 2013; Johnson, Roth, Schultz, & Breslau, 2006). Moreover, prev-alence increases in girls as compared to boys following menarche (Johnson et al., 2006) and this difference is maintained through adulthood. Study I focuses on the symptoms of insomnia.
Finally, sleep deprivation in adolescents is a consequence of delayed sleep timing (DST) and the impossibility of delaying wake times due to social obligations. However, there is no clear agreement on how much sleep is considered optimal and what defines sleep deprivation in adolescents. Pre-vious studies have used the National Sleep Foundation´s (NSF) guidelines (2006) defining < 8 h as insufficient. These recommendations have recently been updated; for example, for adolescents (13-17 years), a sleep duration of 8 to 10 h is recommended, while 7 to 11 h may be appropriate, and less than 7 or more than 11 h is not recommended (Hirshkowitz et al., 2015). These new guidelines differ from the previous ones in that they include ex-cessive sleep duration as a risk, they are age-specific, and they are less re-strictive due to the addition of an intermediate level (“may be appropriate for some”). Sleeping less than 7 h is strikingly common among teenagers, with a prevalence of 24 to 73% (Do, Shin, Bautista, & Foo, 2013; Garaulet et al., 2011; Hysing et al., 2013; Mak, Lee, Ho, Lo, & Lam, 2012; Meldrum & Restivo, 2014). However, as previously mentioned, evidence points to a great sleep need in adolescent animals and humans, likely due to brain mat-uration (Dahl & Lewin, 2002). Studies II and III focus on sleep duration.
To summarize, sleep problems lie on a continuum between normal and pathological – and this is often a fine line. Some sleep problems can be as-sessed with a clear diagnosis (i.e., DSWPD and insomnia) whereas others (sleep deprivation) are harder to define. More research is needed in order to clarify how much sleep is considered a risk for adolescents´ functioning, be-cause many adolescents may suffer from sleep problems and their conse-quences, even though they do not fulfill a diagnosis. In fact, the risk brought by sleep deficit may be defined by individual differences and contextual fac-tors (Blunden & Galland, 2014). That is, in a particularly sensitive devel-opmental period such as adolescence, where the individual needs to perform on many fronts (e.g., socially and academically), sleep might play an even more crucial role.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
19
Why is it important? Sleep and adolescents´ functioning Sleep problems have been found to negatively impact a number of areas important for adolescents´ development and adjustment, including physical health, learning and school performance, and emotion regulation (Shochat et al., 2014). Research on the impact of sleep problems on adolescents´ func-tioning is quite recent and the picture that emerges is complex.
Emotional and behavioral problems Numerous studies point to the detrimental effect of poor sleep quality and quantity on adolescents´ emotional and behavioral problems (Gregory & Sadeh, 2012). In particular, sleep has been associated with mood deficits including depressive symptoms, anxiety, aggression and risk behaviors (e.g., substance use, unprotected sex, and suicidal ideation) (Shochat, Cohen-Zion, & Tzischinsky, 2014).
During adolescence, a normative peak in risk-taking behaviors and more negative mood and mood variability occurs (Maciejewski, van Lier, Branje, Meeus, & Koot, 2017; Spear, 2000); a widely accepted explanation for these changes is the faster maturation of the socioemotional system in con-trast to the later maturation of the cognitive control system (Casey et al., 2010; Casey, Jones, & Somerville, 2011). The socioemotional system can be seen as the acceleration system, pushing adolescents towards sensation-seeking, while the cognitive control system represents the brake system, con-trolling reward processing (Casey, Jones, & Somerville, 2011). On top of this, poor sleep appears to affect the cognitive control system situated in the prefrontal cortex and thus exacerbates this naturally occurring tendency to-ward sensation-seeking (Peach & Gaultney, 2013) and less positive affect (Dagys et al., 2012), and impairs emotion regulation (Baum et al., 2014). An experimental study with adults showed that, after sleep deprivation, amygdala activity increased in response to negative stimuli and connectivity between the medial prefrontal cortex and amygdala decreased; in other terms, the individuals in the study showed a lack of prefrontal control and thus difficulties in regulating emotional responses (Yoo, Gujar, Hu, Jolesz, & Walker, 2007). To further support this link, sleep interventions show positive effects on mood, including on depressive symptoms and aggression (Bonnar et al., 2015; Haynes et al., 2006).
On the other hand, research shows that poor emotion regulation itself disrupts sleep (Kahn, Sheppes, & Sadeh, 2013). For example, rumination following a psychosocial stressor was found to be predictive of longer sleep onset latency (SOL) in adults (Zoccola, Dickerson, & Lam, 2009). So, the

20
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
association between sleep and emotions seems to be bidirectional (Kahn et al., 2013). Similarly, sleep and adolescents´ substance use, including alco-hol, marijuana, and cigarettes, has shown a bidirectional relationship (Pasch, Latimer, Cance, Moe, & Lytle, 2012); that is, adolescents might use stimulants to counteract sleepiness (Lund, Reider, Whiting, & Prichard, 2010), which in turn disrupts sleep and maintains a vicious cycle of poor sleep and substance use. A few longitudinal studies suggest that sleep might precede substance use initiation (e.g., Miller, Janssen, & Jackson, 2016).
Interestingly, one study found that short sleep duration and later bed-times predicted delinquency, but the effects dissipated in adulthood, sup-posedly when the control system reaches maturation (Peach & Gaultney, 2006). This would suggest that adolescence is in fact a particularly sensitive period and that sleep plays an important role in the development of emo-tional and behavioral problems in this age group (Lemola, Schwarz, & Sif-fert, 2012). So, even though the evidence is not conclusive, sleep seems to be strictly intertwined with emotional and behavioral problems in a bidirec-tional manner, over and above the natural turmoil that characterizes the adolescent period. Therefore, investing in interventions to counteract a so-cietal decrease in sleep might be a cost-effective effort, especially in early adolescence, before emotional and behavioral problems bloom.
School performance and attendance School takes up a significant proportion of adolescents´ lives and school performance has important implications for their future adjustment, includ-ing employment opportunities. Sleepy teens, however, may have a hard time getting to school in the morning and performing well (Dewald, Meijer, Oort, Kerkhof, & Bögels, 2010).
Sleep has an important restorative and memory-consolidation function, and is critical for learning (Curcio, Ferrara, & De Gennaro, 2006). In an experimental study, adolescents who slept six-and-a-half hours, as opposed to ten hours, for five consecutive nights showed worse attention and learn-ing performance, and lower arousal in a laboratory classroom (Beebe, Rose, & Amin, 2010). Another experimental study applied a rigorous seven-day sleep restriction protocol with students from top-ranked schools (age 15-19) and found that cognitive performance, especially attention, decreased following sleep deprivation. Moreover, they found that two recovery nights were not enough to completely restore baseline performance (Lo, Ong, Leong, Gooley, & Chee, 2016). Therefore, it is not surprising that students sleeping poorly are at a higher risk of worse school achievement (Dewald et

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
21
al., 2010), lower grades (Saxvig, Pallesen, Wilhelmsen-Langeland, Molde, & Bjorvatn, 2012), and more school absenteeism (Hysing, Haugland, Stor-mark, Bøe, & Sivertsen, 2014; Rajaratnam, Licamele, & Birznieks, 2015).
However, studies on the association between sleep and school perfor-mance (including attendance) in adolescents have mostly been cross-sec-tional, which precludes any causal interpretation (Shochat et al., 2014). So, a question that remains to be answered is whether sleep problems predict future school performance, or whether these co-occur so that adolescents who are often absent and perform poorly in school also suffer from sleep problems. It could be that adolescents who have poorer grades stay up late to catch up with schoolwork. In fact, a few studies have found an associa-tion between school stress and sleep deficit in early adolescence (Fuligni & Hardway, 2006) and in college students (Blunden & Galland, 2014).
Nevertheless, the growing experimental evidence shows that sleep depri-vation does affect performance, even in good students (Lo et al., 2016), and it is therefore reasonable to think that better sleep would be beneficial for academic achievement.
State of the art: summary and implications To summarize, growing evidence shows that both biological and psychoso-cial changes during adolescence make poor sleep a common phenomenon, which creates a negative cycle with poor sleep negatively affecting daytime functioning and vice versa. Even though sleep changes are a normal part of adolescents´ development, poor sleep can have serious consequences. In ad-dition, a small portion of adolescents will develop chronic sleep problems. More epidemiological studies are needed to clarify the long and short-term outcomes associated with poor sleep and the extension of the problem.
Yet, based on the research currently available, sleep seems to be closely intertwined with daily functioning, and although little is known about the mechanisms and directionality, we can hypothesize that many of these rela-tionships are reciprocal. Thus, improving sleep should have positive conse-quences on adolescents´ functioning, which would supposedly benefit sleep in turn; this is particularly relevant in adolescence, as young people are de-veloping and performing in many important areas (e.g., social competence, academic functioning). In addition, sleep problems in this population ap-pear to be on the rise. Thus, sleep interventions might be necessary to im-prove sleep health in adolescents.
However, because there is no easy way of early identification and that many adolescents experience some degree of sleep problem (e.g., irregular

22
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
sleep, sleep deficit), universal preventive interventions might be a cost-effec-tive way to improve sleep health in this population, before poor sleep habits are established (Cassoff et al., 2013). The next section reviews what we know about preventing sleep problems in adolescents and the future chal-lenges we face.
What can we do about it? Preventing sleep deficit in adolescents Universal prevention entails programs aimed at improving health in the whole population, independent of their current risk of developing sleep problems (O'Connell, Boat, Warner, & Council, 2009). In the case of ado-lescents´ sleep, the aim of such programs would be to gradually shift the trajectories of adolescents sleeping less than the recommended eight hours, and to maintain the trajectories of those sleeping within the recommended eight-to-ten hours (Hirshkowitz et al., 2015). In fact, according to the “pre-vention paradox” (Rose, 2001), the majority of new cases will come from the larger group of “good” sleepers. This paradox advocates for a universal (i.e., targeting the whole population) rather than a selective (i.e., targeting a subgroup with a higher risk of developing sleep problems) or indicated approach (i.e., targeting individuals showing early signs of sleep problems) because there is no easy way to identify who will develop chronic sleep problems.
Moreover, adolescents are not likely to seek health care (Barker, 2007) and primary health care practitioners rarely screen for sleep problems (Blunden et al., 2004). Most adolescents spend a great deal of their time in school, which is usually mandatory in early-to-middle adolescence (up to 16-17 years old) (Christner, Forrest, Morley, & Weinstein, 2007); this makes the school a natural arena for interventions. Another advantage of a universal approach in schools is that, by including the whole population, peer norms and support can be used as a tool to boost change. In fact, in-terventions in schools naturally include the peer group and facilitate contact with parents. Parent and peer influences play an important role in adoles-cents´ health behaviors (Durlak, 1997). So, school-based interventions can be an effective way to deliver universal sleep interventions in this age group.
However, school-based sleep interventions are at an early stage and much needs to be done in order to develop effective programs. First, it is important to identify malleable risk and protective factors to target. Secondly, we need to review existing programs and learn from their successes and mistakes. Finally, we need to integrate behavioral change theories and knowledge from other health areas to improve their effectiveness.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
23
Risk and protective factors Risk factors are defined as variables or conditions that heighten the risk of developing a problem (e.g., sleep deficit), whereas protective factors in-crease the chance of positive outcomes (e.g., obtaining adequate sleep) and reduce the risk of negative outcomes (O'Connell et al., 2009). The aim of preventive interventions is to strengthen protective factors and reduce or counteract the effects of risk factors. The following sections will focus on psychosocial and contextual risk and protective factors for adolescents´ sleep health that can be targeted in prevention.
Sleep Hygiene ‘Sleep hygiene’ encompasses different factors that affect sleep quality and quantity, including behavioral arousal (e.g., playing videogames at bed-time), cognitive-emotional arousal (e.g., worrying about the next day at bedtime), sleep environment (e.g., room temperature), physiological arousal (e.g., caffeine intake), consistent sleep patterns (weekday-weekend), and napping (Storfer‐Isser, Lebourgeois, Harsh, Tompsett, & Redline, 2013). Sleep hygiene is a strong protective factor and has shown positive associa-tions with shorter SOL, earlier bedtimes and longer sleep duration (Bartel et al., 2016; Storfer‐Isser et al., 2013).
The use of information and communication technology (ICT) at bedtime is related to sleep hygiene, but it deserves particular attention as it represents one of the central interests of this dissertation.
Information and communication technology (ICT) The use of technology during the day and close to bedtime has been found to be consistently related to later bedtimes and shorter sleep duration (Hale & Guan, 2015). There are three possible mechanisms behind this associa-tion: 1) bright light may suppress melatonin and thus elicit alertness at bed-time, 2) ICT may provoke cognitive and emotional arousal that contributes to adolescents´ difficulties falling asleep, and 3) technological devices may simply distract adolescents from going to sleep (Cain & Gradisar, 2010).
The evidence of the effects of bright light on sleep is not compelling. Ex-perimental studies comparing sleep and alertness in adolescents exposed to bright light (e.g., from a tablet) with adolescents using a filtered screen be-fore bedtime have shown no differences in sleep duration or SOL between the two groups (Heath et al., 2014; van der Lely et al., 2015). Only one of the studies found that adolescents using the filtered screen were less alert and had higher levels of melatonin before bedtime (van der Lely et al.,
24
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
2015); these results are in line with similar studies on adults (Chang, Aes-chbach, Duffy, & Czeisler, 2015; Grønli et al., 2016; Rångtell et al., 2016). So, bright light from technological devices seems to have a minimal impact on sleep, at least sleep duration and onset. However, the majority of these studies were conducted in laboratories and limited to one night, which di-verges from most adolescents´ reality, where technological devices are part of their daily routine (Bartel & Gradisar, 2017).
Watching a TV show, actively playing a videogame, or socially interact-ing with others can all be arousing activities. Several experimental studies investigating the arousal hypothesis have shown that playing videogames increased alertness but not physiological arousal (e.g., heart rate), and led to longer SOL (< 5 min) (King et al., 2013; Weaver, Gradisar, Dohnt, Lov-ato, & Douglas, 2010). One study compared the effect of violent vs. nonvi-olent videogames and found that heightened physiological arousal and worse sleep only occurred in less-habitual players (playing < 1 h daily) (Gentile, Bender, & Anderson, 2016; Ivarsson, Anderson, Åkerstedt, & Lindblad, 2013). So, arousal might depend on the content of ICT and there is some indication of a habituation effect.
Furthermore, ICT can help fulfill the need for social interaction through messaging, social media, video calls, etc. As peer acceptance and inclusion are central concerns in adolescence, social ICT activities (i.e., involving so-cial interactions with others) can become emotionally charged and thus cre-ate arousal. However, studies on the effects of social ICT activities on arousal at bedtime are sparse. Some adolescents display anxiety and depend-ency feelings in relation to technological devices (Terry, Mishra, & Roseth, 2016), and these adolescents might be the ones sleeping poorly (Rosen, Car-rier, Miller, Rokkum, & Ruiz, 2016; Woods & Scott, 2016). The concept of ‘fear of missing out’ (FoMO), defined as a strong need to be online, up-dated and connected to others, and not to miss potentially important/fun experiences (Przybylski, Murayama, DeHaan, & Gladwell, 2013), describes accurately the emotional valence of ICT and might be a key factor in ex-plaining the link between technology and sleep.
In support of the displacement hypothesis, ICT – including chatting with friends, playing videogames, and watching TV – is a potential distraction from sleep but also from other less stimulating daytime activities (e.g., homework) (Levine, Waite, & Bowman, 2007). In fact, ICT use was found to impair executive functioning abilities, including maintaining focus and finishing a task, which in turn was related to poor sleep (Rosen et al., 2016). Moreover, the possibility to socialize around-the-clock can be problematic
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
25
(Beyens, Frison, & Eggermont, 2016). One study found that about 62% of adolescents (mean age 13) used ICT after bedtime, about 57% sent mes-sages, and 21% reported night awakenings due to incoming notifications (Polos et al., 2015). Daytime messaging, night awakenings and a compul-sion to check their phone were all related to worse sleep outcomes in both adolescents and emerging adults (Fobian, Avis, & Schwebel, 2016; Mur-dock, Horissian, & Crichlow-Ball, 2016). So, independent of timing, time allocated to ICT is subtracted from potential sleep time by, for instance, postponing schoolwork until the evening. This idea has been corroborated by interviews with first-year college students (Adams et al., 2016). How-ever, time spent on ICT, and being displaced from sleep, might be moder-ated by individual and contextual factors. For example, one study found that time spent on a videogame depended upon the adolescent´s perception of the consequences of risk-taking behaviors (Reynolds et al., 2015), and several studies found that parents´ rules about ICT were a protective factor against sleep loss (Pieters et al., 2014; Smith, Gradisar, King, & Short, 2017; Sormunen, Turunen, & Tossavainen, 2016). The 24/7 society we live in is defined by the unlimited access to information, social contact and entertain-ment made possible by the internet, and it might therefore be important to help adolescents set limits to their usage of ICT to promote sleep.
To conclude, even though evidence of the relationship between ICT and sleep is growing, there is a lack of studies on mechanisms explaining this relationship and whether it is a causal one. It may be that ICT is actually sometimes used as a sleep aid by those adolescents who have difficulties falling asleep (Eggermont & Van den Bulck, 2006). However, even if that is the case, using ICT as a sleep aid might delay bedtimes even further, given that there is some support for the impact of technology on sleep. Thus, help-ing adolescents to set limits on their ICT usage, perhaps with the help of parents and peers, might enhance their wellbeing. However, no intervention has yet targeted ICT specifically. One way to do so may be to help adoles-cents plan ICT use so that it does not interfere with sleep or other activities (e.g., homework), or agree with parents and peers on rules about ICT use, for example by limiting nighttime texting only to very urgent matters.
Parents and peer influence During adolescence, a transition occurs so that children gradually move to-wards autonomy from their parents, while peers gain a more central role. During this transition, peers and family norms are both influential in ado-lescents´ decision-making (Durlak, 1997).

26
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Negative parenting styles (e.g., inconsistent rules) were found to be asso-ciated with worse sleep outcomes in adolescents (Brand, Hatzinger, Beck, & Holsboer-Trachsler, 2009), whereas monitoring and good relationship quality were associated with better sleep outcomes (Meijer, Reitz, & Dekoviċ, 2016). Surprisingly, parents´ negative attitudes towards sleep were not related to adolescents´ sleep in one study (Biggs et al., 2010), but ado-lescents whose parents set their bedtimes have shown longer sleep duration compared to peers whose parents did not set bedtime rules (Bartel et al., 2014). In addition to setting bedtimes, parents who regulate and monitor their children´s ICT use have also shown earlier bedtimes (Pieters et al., 2014; Smith et al., 2017; Sormunen et al., 2016). Thus, parents´ limit-setting seems to act as a protective factor for adolescents´ sleep, and can be encour-aged by interventions, at least in early adolescence. Later on, it might be more difficult to renegotiate bedtimes if adolescents have already earned bedtime autonomy (Wolfson, Harkins, Johnson, & Marco, 2015); this might explain why one study found no additional benefits of parental in-volvement in older adolescents (mean age 16) (Bonnar et al., 2015).
Peer influence, on the other hand, acquires a more important role. In other health-risk behaviors, such as smoking, teenage pregnancy, and alco-hol prevention, peer norms have been used to support changes in attitudes and behaviors (Durlak, 1997). Peer attitudes towards health behaviors can today be easily transmitted through social media (Dolcini, 2014). Moreo-ver, one study found that friendship networks were likely to have a homo-geneous sleep duration (Mednick, Christakis, & Fowler, 2010), which indi-cates that sleep and other health behaviors are influenced by peer norms. However, peer influence on sleep behaviors has not been targeted explicitly in school-based interventions. To conclude, both parent and peer influences might support good sleep routines and should be included in future inter-ventions.
Academic demands, extracurricular activities and stress Adolescence is a busy time and adolescents might prioritize other important activities, including socializing, schoolwork, and entertainment over sleep. Therefore, we might need to take a look at what adolescents are doing that might be taking time from their sleep, in order to understand how to help them make room for it.
Increasing academic demands and extracurricular activities are often cited as central changes contributing to the decrease in adolescents´ sleep. However, time spent on extracurricular activities (including sport, part-time

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
27
jobs, homework, and volunteer work) have been found to have a small im-pact on sleep; each hour spent on extracurricular activities predicted only four minutes’ less sleep (Short et al., 2013). Similar results were found in other studies (Fuligni & Hardway, 2006; Noland, Price, Dake, & Telljo-hann, 2009). Therefore, extracurricular activities alone do not explain shorter sleep duration. However, they might contribute to later bedtimes in combination with other risk factors (e.g., self-selected bedtimes and ICT use).
Another hypothesis is that, if adolescents do not feel in control of their time, even pleasurable activities might be perceived as stressful, which in turn can interfere with sleep. However, no study has looked at common daily stressors (e.g., school stress) in relation to sleep, which would give important information about relevant targets for prevention. Only a few studies have investigated the relationship between perceived stress and sleep disturbances and found a significant association in adolescents (Chung & Cheung, 2008) and college students (Lund et al., 2010). Similarly, stress due to ICT-accessibility was also related to sleep problems in young adults (Tho-mée, Härenstam, & Hagberg, 2011). Therefore, giving adolescents tools to counteract daily stress might be an important goal for preventive interven-tions; for example, time management skills may help students to handle the balance between schoolwork and leisure time.
To summarize, in line with the biopsychosocial model of sleep, psycho-social and contextual factors are strictly intertwined with sleep. Moreover, as studies in other age groups (adults and college students) and qualitative evidence suggest, it seems relevant to further investigate the association be-tween both daytime (e.g., social stressors) and nighttime factors (e.g., arousal and ICT use at bedtime) that might interfere with sleep. These po-tential barriers to sleep should be taken into account when planning pre-ventive interventions.
Previous school-based interventions There is an increasing number of school-based sleep interventions. How-ever, as suggested by a recent review (Blunden & Rigney, 2015), these pro-grams are in their infancy and have had limited success. Previous attempts to change adolescents´ sleep habits have operated at different levels, includ-ing 1) sleep education only, 2) sleep education along with sleep-related skills training, and 3) sleep education, skills training with the addition of a moti-vational element.

28
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Sleep education Sleep education consists of information about how sleep works, sleep need in adolescence, good sleep habits before bed and during the daytime, and the importance of maintaining consistent sleep/wake cycles on weekdays and weekends. Sleep education has been found to effectively improve ado-lescents´ knowledge about sleep (Bakotić, Radošević-Vidaček, & Košćec, 2009; Cortesi, Giannotti, Sebastiani, Bruni, & Ottaviano, 2004; Díaz-Mo-rales, Prieto, Barreno, Mateo, & Randler, 2012), with a few exceptions (Ga-brielle et al., 2015; Kira, Maddison, Hull, Blunden, & Olds, 2014). How-ever, only a few studies have assessed whether sleep education also affects adolescents´ sleep behaviors and have found no effects (Blunden, Kira, Hull, & Maddison, 2012; Rigney et al., 2015); this finding is in line with the broader health education literature, suggesting that in order to translate knowledge into healthy choices and behaviors, programs need to include skills training to put this knowledge into practice (Nation et al., 2003).
Sleep education + Skills training Skills training in school-based sleep interventions have included, for exam-ple, goal setting, changing unhelpful thoughts, resisting social pressure, self-regulation, and behavioral experiments (e.g., maintaining regular weekday-weekend sleep schedules). Sleep education, together with skills training, have also led to increased sleep knowledge. More specifically, one study found significant improvements in social jetlag in a subgroup of adolescents with DSP, but these changes had not been maintained at follow-up (Moseley & Gradisar, 2009). Similarly, another study found that adolescents who improved their sleep knowledge also reported significant improvements in sleep onset difficulties, which indicates that sleep education is an important precursor of behavioral change (Wing et al., 2015). Nevertheless, both stud-ies found that adolescents were not motivated or confident to change their sleep behaviors. One program, however, managed to improve early adoles-cents´ confidence in changing sleep behaviors and showed improved sleep hygiene, longer time in bed (TIB), and earlier bedtimes relative to a control group (Wolfson et al., 2015). Again, these changes had not been maintained at follow-up. Moreover, TIB is a problematic measure for adolescents´ sleep as there is no guarantee that adolescents are actually sleeping rather than lying awake and engaging in other activities in bed (e.g., watching TV). Taken together, these studies highlight the renowned difficulties in motivat-ing adolescents towards long-term behavioral changes.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
29
Sleep education + Skills training + Motivation to change Engagement and motivation are crucial aspects to address in order to change sleep-related behaviors in adolescents. To address this issue, a num-ber of sleep interventions have incorporated a motivational component in their curriculum. One such program adopted a motivational framework in-spired by motivational interviewing (MI) (Miller & Rollnick, 2012), includ-ing, for example, raising ambivalence between current sleep-behaviors and personal goals. This program was successful in increasing adolescents´ sleep knowledge and motivation to maintain regular wake times, but not their motivation to increase sleep duration, and once again no actual change in behaviors occurred (Cain, Gradisar, & Moseley, 2011).
A subsequent trial compared this motivational sleep intervention with parental involvement and/or bright light and showed a significant increase in motivation to regularize wake times and to get bright light in the morn-ing, but not motivation to increase sleep duration. Yet, all three conditions showed improved sleep outcomes – including sleep duration – relative to a control group (Bonnar et al., 2015).
Overall, the majority of school-based sleep education programs have proven to be effective in improving adolescents´ knowledge about sleep but not powerful enough to boost and maintain behavioral changes. Therefore, we might need to integrate knowledge gained from previous interventions with behavioral change theories to improve the impact of school-based sleep interventions.
Theoretical approach to behavioral change Behavioral change is difficult to trigger and this is especially true for ado-lescents. A large body of research on the key ingredients of effective school-based prevention programs indicates that interventions should provide tools to overcome barriers to change in addition to providing knowledge, that they should target important risk and protective factors identified in the literature and based on theory, and that they should be timely and target multiple contexts to trigger behavioral change (Nation et al., 2003). Previ-ous programs have targeted these aspects separately (e.g., skills training, parental involvement, MI), but it might be helpful to integrate them into one program (Blunden & Rigney, 2015; Cassoff et al., 2013). Moreover, in reviewing the existing sleep school-based programs, Cassoff et al. (2013) identified the lack of focus on motivation as a theoretical shortcoming. To overcome this limitation, they suggested the Integrated Model for motiva-tional and behavioral change (I-Change) (de Vries, Mesters, Van de Steeg,

30
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
& Honing, 2005) as a useful framework for school-based sleep programs (see Fig. 2) and to use a more individually tailored approach, for example by making use of new technologies.
The integrated model for motivation and behavioral change (I-Change Model) The I-Change Model (de Vries et al., 2005) was originally developed to change adolescents´ smoking behaviors and has recently been adapted to sleep behaviors by Cassoff et al. (2014). According to the I-Change Model, attitudes, social influences and self-efficacy are the motivational elements that lead to intention to change and eventually to behavioral change. Inten-tion to change is measured as the different stages described by the Trans-theoretical Model: precontemplation (not considering change in the close future), contemplation (considering change), action (behavioral change), maintenance (of the new behavior), and relapse (Prochaska & Diclemente). The I-Change Model is in line with the Theory of Planned Behavior (Ajzen & Fishbein, 1975; Madden, 1986) but it also emphasizes the importance of social influence in accordance with the Social Learning Theory (Bandura, 2006). Social pressure and social modeling are the bases for numerous health behavior interventions in adolescence, given the growing importance of the peer group in this developmental period (Durlak, 1995). Further-more, in line with the Health Belief Model (Janz & Becker, 1984), the I-Change Model views awareness as an important precursor of intention to change. Awareness is, in turn, determined by knowledge (i.e., sleep knowledge), risk perception (i.e., risks associated with insufficient sleep du-ration), and cues to action (i.e., feeling tired, friends and family saying good-night).
More in detail, in the context of adolescents´ sleep, attitudes refer to the affective and cognitive evaluation of sleep, including the positive/negative valence of sleep and the costs and benefits of obtaining adequate sleep. As mentioned before, adolescents have busy lives and, therefore, much to lose when anticipating bedtimes. A few studies have tackled this issue by provid-ing decisional balance sheets (MI), and embedding sleep education in ado-lescents´ life goals (Social Learning) (Cain et al., 2011; Wolfson et al., 2015). Social influences refer to social norms, the perceived behaviors of others, and pressure/support from parents, peers and the broader community. As previously mentioned, parents have been involved in a few programs (e.g., Bonnar et al., 2015 and Wolfson et al., 2015); whereas, surprisingly, peers have not explicitly been targeted, even though both are known to affect

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
31
adolescents´ decision-making (Durlak, 1997). In addition, social influences include the larger context of adolescents´ sleep; that is, an ambitious 24/7 society that values accessibility around the clock at the expense of sleep (Blunden, Benveniste, & Thompson, 2016). Therefore, raising a discussion about the relevance of sleep in adolescence, involving parents and peers and exploring sleep norms and values, is of great relevance for preventive efforts. Finally, self-efficacy refers to the perceived ability to change sleep behaviors and refers to adolescents´ difficulties to prioritize sleep over other activities. Because adolescents often report a lack of time as a reason for not obtaining adequate sleep, it might be useful to teach them strategies to better organize daytime and nighttime activities so that they do not interfere with sleep.
Moreover, in line with the I-Change Model, MI (Miller & Rollnick, 2012) may be a useful technique for promoting change in adolescents, as it aims at enhancing self-efficacy, resolving ambivalence, and can be tailored to individual needs (Cassoff et al., 2013).
Figure 2. The I-Change Model. Reproduced from de Vries et al., 2005 with permis-sion.

32
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Motivational Interviewing (MI) to promote behavioral change Motivational Interviewing (Miller & Rollnick, 2012) is a useful framework when working with adolescents, given that it is non-confrontational in na-ture and respectful of the client´s autonomy, which are sensitive areas in this developmental period (Cassoff et al., 2013). MI is based on four important principles, including showing empathy to the client, raising ambivalence be-tween the current behavior and the client´s goals and values, rolling with resistance (i.e., non-confrontational attitude to resistance), and supporting autonomy. So, in line with the I-Change Model, MI aims at resolving am-bivalence created by, for example, the pros and cons of anticipating bed-times (Cain et al., 2011). In other words, to be able to change their behav-iors individuals need to feel “ready” (i.e., it has to be the right time for change and commitment), “able” (i.e., they have to feel confident) and “willing” (i.e., they have to appreciate that the change is important). An-other characteristic of MI is that it is client-oriented, which is difficult to address in a group-format but may be facilitated by the use of technology, for example, through computerized individualized feedback (Cassoff et al., 2013). A tailored component might be especially useful because adolescents may have different barriers to sleep (e.g., extracurricular schedules and so-cial obligations). MI has been integrated into sleep education before and has been successful in improving adolescents´ motivation (Bonnar et al., 2015; Cain et al., 2011).
Next step: Improving existing programs To summarize, the next step in school-based sleep programs might be to integrate sleep hygiene education with skills training to help adolescents overcome barriers to change. Time management skills, together with sleep education, might help adolescents make more room for sleep in addition to schoolwork, extracurricular activities, and entertainment. Moreover, par-ents and peers can be supportive of time management strategies and good sleep routines.
The timing of the intervention might be a crucial aspect of school-based sleep programs because parental involvement is likely to be more easily ac-cepted by early adolescents, whereas it might be seen as a bigger threat to autonomy by older adolescents. Another advantage of interventions with early adolescents is that poor sleep habits might not yet be rigidly estab-lished.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
33
In addition, the aid of new technology in delivering school-based sleep interventions would allow for an effective delivery of a personalized com-ponent, which is better suited to MI techniques (Cassoff et al., 2013). Be-cause adolescents have different schedules and activities that can interfere with sleep, it might be useful to address each individual with relevant infor-mation and strategies that apply to their unique situation. Moreover, rather than being a contradiction, using technology to deliver the intervention may show an open attitude towards ICT that views it as a useful resource and not one to ban; on the contrary, a negative attitude towards ICT might have a negative impact and provoke greater resistance.
Summary and aims The focus on adolescents´ sleep has increased drastically in the last decade, and the picture that emerges is complex; there are many more pieces to this puzzle that need to be explored. The overall aim of this dissertation is to extend the knowledge on adolescents´ sleep problems, including prevalence, risk and protective factors, and possible consequences on daytime function-ing, to guide the development of effective preventive interventions.
Studies on the causes and consequences of poor sleep are emerging. How-ever, we do not know enough about longitudinal associations between sleep and adolescents´ functioning. In adults, sleep problems, including insomnia, have a strong association with sick leave (Linton & Bryngelsson, 2000; Sivertsen, Øverland, Bjorvatn, Mæland, & Mykletun, 2009). However, we do not know whether this is true for adolescents as well, that is, whether adolescents sleeping poorly are more absent from school.
Moreover, there are some indications that adolescents´ sleep duration might be declining (Keyes et al., 2015; Kronholm et al., 2015; Matricciani et al., 2012). So, more studies are needed to describe the prevalence of in-sufficient sleep duration and irregular sleep patterns (i.e., social jetlag), and to investigate whether insufficient sleep is associated with emotional and behavioral problems.
Further, adolescents may be particularly vulnerable to sleep deficit as they find themselves in an important life transition (Blunden & Galland, 2014). A growing number of studies shows that poor sleep is strictly inter-twined with adolescents´ well-being. Therefore, implementing early inter-ventions to promote sleep health in this age group is crucial. Existing inter-ventions, however, have not been particularly effective in changing adoles-cents´ sleep behaviors (Cassoff et al., 2013) and there is a need to identify more powerful risk and protective factors to target. In fact, adolescents may

34
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
encounter many barriers to sleep, including daily stressors and ICT. More-over, in order to prompt behavioral change, school-based sleep programs would benefit from integrating knowledge from other health-behavior pro-grams and theories of behavioral change. In particular, interventions should provide adolescents with not only information but also concrete strategies to overcome barriers to sleep, promote social support from parents and peers, and include some degree of individual feedback.
Specific aims I. Study I is a longitudinal study, where adolescents were fol-
lowed over a one-year period. The aim was to investigate the association between sleep problems (defined as symptoms of insomnia) and adolescents´ school attendance one year later.
II. Study II is a cross-sectional study of a large cohort of adoles-cents. The aim was to describe the prevalence and patterns of sleep duration, and to assess whether sleep duration was re-lated to mental health (i.e., emotional and behavioral prob-lems) and to potential targets for sleep interventions (i.e., stress, technology and sleep hygiene).
III. Study III is a pre- and post-test evaluation of a new school-based sleep intervention informed by the I-Change Model. The program sought to improve early adolescents´ sleep through sleep education combined with time management strategies, peer and parent support, and individualized feedback via an app. The aim of the study was to evaluate the impact of the intervention on motivation to change, sleep hygiene, perceived stress, ICT and sleep.
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
35
Short description of the studies
Study I
Introduction Sleep has important consequences for a person's daytime functioning. Nu-merous studies have shown that insomnia predicts work absenteeism and work disability in adults (Linton & Bryngelsson, 2000; Sivertsen et al., 2009), but only a few studies have examined this association in adolescents. Given the rise in sleep problems during adolescence (Dahl & Lewin, 2002), it is important to investigate long-term associations between sleep and ado-lescents´ functioning.
Aim This study aimed to explore whether symptoms of insomnia in adolescents predicted school absenteeism one year later, over and above known psycho-logical risk factors for absenteeism.
Overview of the design The study used a longitudinal design with two measurement points over one year.
Participants Students in the 10th to 12th grades in a Swedish upper secondary school completed questionnaires during school hours at baseline and again at fol-low-up one year later (age, 16-20 years; N = 353; 48.1% girls).
Measures School absenteeism was assessed through a single item “Have you been away a whole day from school in the last three months?” Responses were dichotomized into ‘high’, 4-10 times or > 10, and ‘low’, 0-3 (Kearney, 2008) (Centrala Studiestödsnämnden, 2013).
Insomnia symptoms were assessed through four items from the Basic Nordic Sleep Questionnaire (BNSQ) (Partinen & Gislason, 1995) and the Uppsala Sleep Inventory (Liljenberg, Almqvist, Hetta, Roos, & Agren, 1987), including 1) subjective perception of sleep problem, 2) difficulties falling asleep, and 3) staying asleep (Owens & Mindell, 2011). Based on their responses, adolescents were divided into three groups: no symptoms of insomnia, moderate symptoms, and severe symptoms.

36
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Depressive symptoms were measured with six questions from the Center for Epidemiologic Studies’ Depression Child Scale (CES-DC) (Olsson & von Knotting, 1997). To measure social anxiety, we used the Social Phobia Screening Questionnaire for children (SPSQ-C) (Gren-Landell et al., 2009). In addition to social anxiety, we used a single diagnostic question on symp-toms of school-related social phobia from the SPSQ-C (Gren-Landell et al., 2009). One question assessed alcohol intoxication frequency (Koutakis, Stattin, & Kerr, 2008). Bully victimization was evaluated with a yes or no question. Finally, somatic symptoms (stomach ache, headache, and back pain) were assessed through three questions from the Modified Somatic Per-ception Questionnaire (MSPQ) (Main, 1983).
Analyses We used logistic regression analyses, controlling for previous absenteeism, alcohol intoxication, school-related social phobia, social anxiety, depressive symptoms, somatic symptoms, and bully victimization to predict problem-atic school absenteeism vs. low or no absenteeism.
Results Previous absenteeism, school-related social phobia, and alcohol intoxica-tion entailed a two-fold risk for future absenteeism. Over and above these factors, adolescents reporting severe symptoms of insomnia were almost three times more likely than adolescents reporting no or low symptoms to report problematic absenteeism one year later. We did not find any gender difference.
Conclusions Similar to studies on adults, symptoms of insomnia were associated with adolescents' daytime functioning as measured by school attendance. This is in line with the growing evidence showing that adolescents sleeping poorly have worse grades and attention difficulties in school (Beebe et al., 2010; Wolfson & Carskadon, 2003), which in turn has negative consequences on future employment and adjustment (Kearney, 2008). Therefore, improving sleep may be an important target to prevent future problems and might need to be targeted earlier on, before poor sleep habits are established. Even though more longitudinal studies and studies focusing on the mechanisms through which sleep affects functioning are needed, it is reasonable to as-sume that improving sleep health would benefit adolescents´ wellbeing, be-cause many of these relationships are bidirectional (Kahn et al., 2013). To

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
37
begin to address this issue, there is a need for studies to describe adolescents´ sleep patterns (i.e., sleep duration, bedtimes and wake times, and irregular school day and weekend sleep times), including age and gender differences, and factors associated with problematic sleep patterns. Study II is, therefore, an epidemiological study of sleep problems in an adolescent population, of emotional and behavioral correlates, and of potential targets for interven-tions.
Table 1
Binomial logistic regression estimates to predict absenteeism one year later. The table shows the contribution of insomnia symptoms over and above psychological risk factors and previous absenteeism. B(SE) Wald Sig. Exp(B) 95% C.I.for
EXP(B) Lower Upper
Absenteeism T1 0.95 (0.41) 5.39 .020 2.58 1.16 5.75 Alcohol intoxication 0.81 (0.34) 5.83 .016 2.25 1.16 4.35 Social phobia 0.76 (0.39) 3.87 .049 2.15 1.00 4.59 Bully victimization 0.05 (0.42) 0.08 .782 1.12 0.49 2.59 Depressive symptoms 0.05 (0.04) 1.14 .286 1.05 0.96 1.14 Social anxiety -0.09 (0.06) 1.92 .166 0.92 0.81 1.04 Somatic (stomach) -0.25 (0.21) 1.51 .220 0.78 0.51 1.16 Somatic (head) -0.09 (0.18) 0.22 .637 0.92 0.64 1.31 Somatic (back) -0.02 (0.18) 0.01 .916 0.98 0.69 1.39 Gender 0.06 (0.35) 0.40 .528 1.25 0.63 2.47 Insomnia s. (mild) -0.06 (0.40) 0.02 .873 0.94 0.43 2.05 Insomnia s. (severe) 1.07 (0.44) 5.94 .015 2.92 1.23 6.91 Note. Model fit: R2 = .085 (Cox & Snell)-.139 (Nagelkerke). Model χ2 (12) = 31.298. p = .002. Block χ2 (2) = 6.303. p = .043.

38
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Study II
Introduction Sleep deficit is a growing problem in adolescence and has negative conse-quences on physical and mental health, and academic achievement (Shochat et al., 2014). The National Sleep Foundation (NSF) has recently updated its sleep duration recommendations according to age group (Hirshkowitz et al., 2015). These recommendations are an important tool to describe the extent of the problem and to identify psychosocial and contextual factors related to insufficient sleep duration. However, no study has yet used these guidelines in an adolescent population. Moreover, epidemiological studies are the basis for the development of effective sleep interventions. Existing programs have shown limited effects, and this may be due to the fact that they do not take into account the many barriers to adolescents getting ade-quate sleep (Cassoff et al., 2013); that is, adolescents may prioritize school obligations, socializing with peers and use of information and communica-tion technology (ICT) over sleep (Carskadon, 2011). To begin to address this issue, it is important to investigate whether these factors are associated with insufficient sleep duration.
Aim The first aim of this study was to assess the prevalence of sleep deficit using the new NSF´s guidelines in a large sample of adolescents. In particular, we inspected the prevalence and patterns of sleep duration in the whole sample, in boys vs. girls, and in younger (12-13) vs. older adolescents (14-16). Sec-ondly, this study aimed to assess whether short sleep duration was associ-ated with emotional and behavioral problems including depression, anxiety, anger, and norm-breaking. Lastly, this study aimed to assess whether there was any association between sleep duration and potential protective/risk factors including daily stressors, sleep hygiene, ICT use.
Overview of the design This study used a cross-sectional survey.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
39
Participants Participants were high school students in the 7th and 8th grade (N = 2768; 48% girls, age range: 12-16 years) from 17 public schools in three commu-nities in middle Sweden. Students filled out questionnaires in school during the spring of 2014.
Measures Sleep measures from the School Sleep Habits Survey (SSHS) (Wolfson & Carskadon, 1998) included bedtime, wake up time, and sleep onset latency, for weekdays and weekends separately. Total sleep time (TST) was calcu-lated by subtracting students´ self-reported bedtime from their wake up time, minus SOL. Weekday sleep duration was then transformed into a cat-egorical variable according to the NSF guidelines (Hirshkowitz et al., 2015).
Depressive symptoms were measured through 20 items from the Center for Epidemiological Studies’ Depression Scale (CES-D) (Radloff, 1977). Anxiety was assessed through the Overall Anxiety Severity and Impairment Scale (OASIS) (Norman, Hami Cissell, Means‐Christensen, & Stein, 2006). Anger was assessed through an adapted version of the OASIS. Norm-break-ing behaviors were assessed through 13 questions about stealing, violence, contact with police and social services, and the use of illegal drugs (Kerr & Stattin, 2000).
Daily Stressors were measured using a short version (27 items) of the Adolescent Stress Questionnaire, ASQ (Byrne et al., 2007). Cognitive-emo-tional arousal was measured through one sub-dimension of the Adolescent Sleep Hygiene Scale, ASHS (Storfer‐Isser et al., 2013). ICT in bed including TV, computer, tablet or mobile was assessed through a single item.
Analyses Independent sample t-tests were used to test for age and gender differences, whereas paired t-tests were used to investigate differences between weekday and weekend sleep patterns. A multivariate analysis of variance was used to test for differences in emotional and behavioral outcomes (i.e., depression, anxiety, delinquency and anger) at the different levels of TST (i.e., optimal, borderline and poor). A multinomial logistic regression was used to deter-mine risk and protective factors, including use of technology after lights out, cognitive-emotional arousal at bedtime, and daily stressors.

40
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Results Of the younger adolescents (age 12-13), 58% reported optimal weekly TST, 30% reported borderline TST and 12% reported poor TST. In the older age group (age 14-16), 48% of students reported optimal sleep duration during the week, 33% reported borderline TST, and 19% reported poor TST. Girls and older students generally reported shorter sleep duration. Moreover, sleep timing and duration were significantly different during the school-week as compared to the weekend, with later bedtimes (ca. 2 hours) and later wake times (ca. 3-4 hours) for both younger and older adolescents.
Moreover, students sleeping in the poor TST range reported significantly higher levels of emotional and behavioral problems as compared to those sleeping in the borderline or optimal range (age 12-13, V = 0.12, F(8, 2210) = 17.4, p < .001, ηp ² =.06; age 14-16, V = 0.12, F (8, 2836) = 22., p < .001, ηp ² = .06). Girls generally reported higher rates of emotional problems (Fig. 3).
Fig. 3. Interaction between gender and emotional and behavioral problems for older adolescents (age 14-16, N = 1426) reporting optimal, borderline and poor sleep du-ration. Note. Score range for depression (0-80), anxiety (0-20), anger (0-20), and norm-breaking behaviors (0-52). TST = total sleep time

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
41
Finally, sleep duration was closely related to cognitive-emotional sleep hygiene and ICT use at bedtime, with adolescents sleeping poorly (com-pared to optimal TST) also reporting worse sleep hygiene and more frequent use of ICT at bedtime. In regard to daily stressors, school demands were relevant for older adolescents, whereas arguments at home were associated with poor sleep for younger adolescents (Table 2).
Conclusions A significant portion of adolescents reported insufficient sleep duration, but more so for older adolescents. This is in line with a number of studies (Maslowsky & Ozer, 2014) suggesting that rates of insufficient sleep dura-tion increase from puberty through late adolescence. So, in order to prevent sleep deprivation, interventions should be implemented in early adoles-cence, before poor sleep habits become deeply rooted. Furthermore, adoles-cents significantly delayed their sleep phase during weekends, which may lead to delayed bedtimes during the week and further sleep deprivation (Crowley et al., 2007).
The new NSF recommendations are informative, and we found a signifi-cant association with both emotional and behavioral problems and poten-tial targets for intervention. In particular, poor sleep hygiene, use of elec-tronic media and stress might represent barriers to sleep and future studies should investigate this further. Nevertheless, even though the direction of the association cannot be established in a cross-sectional design, we can hy-pothesize that these relationships are likely bidirectional and that targeting these factors may still be beneficial. For example, even if adolescents use ICT in bed because they cannot fall asleep, they may get caught in a reward-ing activity that is difficult to interrupt and thus delay bedtime even further. So, even though the mechanisms are important for further understanding adolescents´ sleep deficit, with the knowledge available, targeting these risk factors (e.g., ICT) in future interventions might be a good choice. Study III describes the development and preliminary results of a novel school-based sleep intervention, based on the results of Study II and informed by the I-Change model.

42
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Table 2
Multinomial Logistic Regression Exploring How Stressors, ICT in bed and Sleep Hygiene relate to Borderline and Poor TST for the two Age Groups. Age 12-13 (N = 1069) Age 14-16 (N = 1386)
Variable OR 95% CI OR 95% CI
Stress-School performance
Borderline 1.02 (0.85-1.24) 1.12 (0.95-1.31) Poor 1.16 (0.90-1.51) 1.26* (1.04-1.53) Stress-School/leisure Borderline 1.05 (0.88-1.26) 0.99 (0.85-1.16) Poor 1.03 (0.81-1.32) 1.10 (0.91-1.32) Stress-Home Borderline 1.12 (0.90-1.39) 1.14 (0.95-1.38) Poor 1.40* (1.06-1.84) 1.20 (0.96-1.50) Stress-Peers Borderline 1.60* (1.07-2.38) 0.88 (0.69-1.12) Poor 1.04 (0.57-1.90) 0.84 (0.64-1.10) Sleep Hygiene Borderline 0.80* (0.68-0.95) 0.75*** (0.65-0.87) Poor 0.64*** (0.52-0.80) 0.58** (0.49-0.69) ICT in bed Borderline 1.37*** (1.21-1.55) 1.30** (1.17-1.45) Poor 1.43*** (1.19-1.71) 1.61** (1.40-1.85) Gender (girl) Borderline 5.35*** (2.53-11.34) 1.51** (1.16-1.96) Poor 1.52 (0.53-4.41) 1.33 (0.96-1.86) Gender (girl)*Stress-Peers Borderline 0.47** (0.28-0.78) - - Poor 1.13 (0.58-2.23) - - Note. Model fit (age 12-13) R2 = .149 (Cox & Snell), .176 (Nagelkerke) and model fit (age 14-16) R2 = .157 (Cox & Snell), .181 (Nagelkerke). *p < .05 **p < .01, ***p < .001 ICT = information and communication technology; TST = total sleep time

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
43
Study III
Introduction School-based sleep education programs have proven effective in increasing adolescents´ sleep knowledge, but they have generally been less successful at translating knowledge into behavioral change (Cassoff et al., 2013).
In order to produce behavioral change, interventions need to incorporate skills training to overcome barriers to change. In addition to providing knowledge, they should target important risk and protective factors, they should be timely, target multiple contexts, and involve some level of indi-vidualized feedback (Nation et al., 2003).
Because adolescents often report a lack of time as a primary reason for not obtaining adequate sleep, we added time management to a regular sleep education curriculum to help adolescents plan time for sleep. Moreover, we discussed ICT (including Fear of Missing Out [FoMO]) as a potential bar-rier to both daytime activities (e.g., homework) and sleep, and encouraged parents and peers to support rules about ICT usage and time management. In addition, in order to give individually tailored feedback and enhance ad-olescents´ motivation, the program was delivered with the support of a web and mobile app.
We hypothesized that, at the end of the intervention, adolescents would show better sleep knowledge and sleep hygiene, higher motivation to change sleep behaviors and reduced perceived stress, reduced ICT use and FoMO, and reduced social jetlag (i.e., discrepancy between weekend and weekday wake times). Moreover, because the majority of early adolescents sleep be-tween 8-10 hours, which is considered optimal, we hypothesized that short-term changes in sleep duration would occur only for at-risk adolescents (i.e., those sleeping less than 8 hours per night).
Aim The aim of this study was to investigate the preliminary effects (pre-post within group) of a new school-based intervention on adolescents´ motiva-tion to change perceived stress, ICT use, and sleep behavior.
Overview of the design The study used a within-subject (repeated measures) design (see Fig. 4), where students filled out questionnaires on two baseline occasions (B1-2)

44
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
and then at the beginning of each session, S1-5 (post-test measurements re-fer to the 5th and final sessions).
Fig 4. Overview of design and measurement points.
Participants Participants were 286 high school students in 7th and 8th grades from two public schools in Sweden. Data were collected from 222 eligible students (60% girls, mean age = 13.9).
Intervention After conducting focus groups with high school adolescents, important bar-riers to sleep emerged, including school stress and the strong desire for lei-sure time, use of technology, and FoMO. Also, adolescents reported mixed attitudes about parent-set bedtimes and this led to us choosing younger ad-olescents as our target group. On the other hand, adolescents confirmed the important influence of peers on bedtimes but also expressed the need for autonomy and individualized help according to one´s own schedule and needs. This led to the development of a web and mobile app to facilitate individual contact with the participants.
The final curriculum included sleep education, time management training (e.g., planning homework without distractions, planning pleasurable activ-ities, quiet time before bed), parental information, and peer involvement in the classroom (e.g., rules about evening interactions via ICT).
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
45
The intervention consisted of five sessions of 50-60 min in length, once a week for six or seven weeks. Sessions were held by psychology students in the last year of their program, plus one psychologist and one teacher.
Measures
Weekly measures Weekly measures included a sleep diary from the School Sleep Habits Survey (SSHS) (Wolfson & Carskadon, 1998), including BT, WT, SOL, WASO, that allowed the calculation of sleep duration during weekdays and week-ends and social jetlag (i.e., the difference between weekend and weekday bedtimes). Subgroups according to the NSF´s guidelines (Hirshkowitz et al., 2015) were created based on baseline sleep duration. Information & com-munication technology (ICT) after bedtime and Fear of Missing Out (FoMO) were assessed through single items assessing the frequency of the behavior. Motivation to change was assessed through a three-item screen-ing, including importance, ability and commitment (Miller & Johnson, 2008).
Pre- and post-measures. Perceived stress was assessed through the Perceived Stress Scale (PSS-14) (Cohen, Kamarck, & Mermelstein, 1983). Sleep hygiene was measured through the Adolescents Sleep Hygiene Scale (ASHS) (Storfer‐Isser et al., 2013), including the cognitive/emotional factor and the behavioral arousal factor. Finally, sleep knowledge was measured through a multiple-choice quiz that covered topics discussed during the intervention.
Analyses We explored changes in sleep knowledge, sleep hygiene, perceived stress (pre and post), motivation, social jetlag and sleep duration (weekly) using repeated measures ANOVA. Chi-square analysis was used to determine changes in ICT use and FoMO. The results are displayed both for the whole group and separately for sleep duration subgroups (i.e., optimal, borderline, and poor sleep duration).
Results Sleep knowledge improved for the whole group, independent of baseline sleep duration – F(1, 178) 133.04, p < .001, ηp
2 = .428. Sleep hygiene (be-havioral) improved significantly for the risk group only – F(1, 50) 9.77, p =

46
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
.003, ηp2 = .163. Use of ICT after bedtime and motivation to change did not
change significantly for any of the groups, but adolescents in the optimal TST group reported less FoMO by the end of the intervention (χ2(1)=4.76, p = .049). Poor and borderline sleepers reported more perceived stress at the beginning of the intervention, as compared to optimal sleepers (p < .001). Perceived stress decreased significantly for both groups by the end of the intervention (borderline; F(1, 47) 6.97, p = .011, ηp
2 = .129, and poor sleepers; F(1, 48) 4.47, p = .04, ηp
2 = .085) (Fig. 5). Only the risk group showed an increase in weekly sleep duration (F(6, 186) 5.18, p < .001, ηp
2 = .143), and a reduced discrepancy between weekend and weekday wake times (F(3.59, 75.50) 2.78, p = .04, ηp
2 = .117). However, neither were sig-nificantly different from baseline by the end of the intervention. Optimal sleepers showed a significant decrease in sleep duration (F(4.75, 213.62) 7.32, p < .001, ηp
2 = .140), whereas borderline sleepers´ TST did not change (Fig. 6). Adolescents´ feedback about the program was positive and the app was rated positively. However, 22% did not find the program helpful.
Conclusions The addition of time management, individualized feedback, and the focus on ICT use and FoMO did not boost adolescents’ motivation to change as expected. Moreover, even though adolescents appreciated the app, 22% of the participants did not find the program helpful, which indicates that there is room for improvement.
The poor TST group´s behavioral sleep hygiene, stress, social jetlag and sleep duration improved significantly during the intervention, but TST and social jetlag worsened again post-test. Thus, longer sleep duration might not be maintained after the intervention. Optimal sleepers reported shorter sleep duration by the end of the intervention, although still within the opti-mal range (i.e., >8 h). A shorter sleep duration in this group might be due to the drastic increase in bright light hours during the spring (Figueiro & Rea, 2010) but a control group and follow-up data are necessary to clarify this. On the positive end, both poor and borderline sleepers showed signif-icant improvements in stress, but TST improved for poor sleepers only. So, it remains to be seen whether the intervention will show a preventive effect by, 1) maintaining the gains in the poor TST group, 2) preventing the bor-derline group from worsening, and 3) preventing optimal sleepers from de-veloping sleep problems in the future, relative to a control group. Neverthe-less, the lack of change in the hypothesized mechanisms (motivation and technology) are disappointing and might undermine future gains.
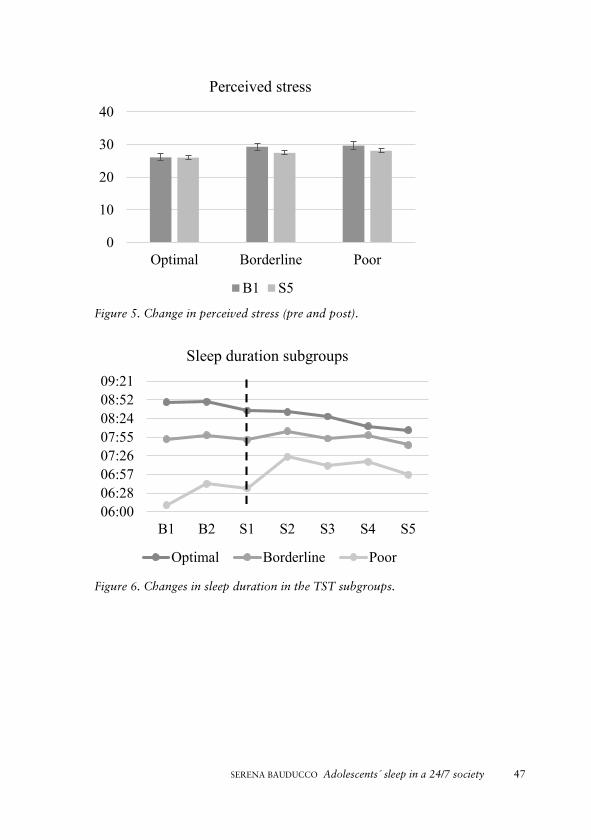
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
47
Figure 5. Change in perceived stress (pre and post).
Figure 6. Changes in sleep duration in the TST subgroups.
0
10
20
30
40
Optimal Borderline Poor
Perceived stress
B1 S5
06:0006:2806:5707:2607:5508:2408:5209:21
B1 B2 S1 S2 S3 S4 S5
Sleep duration subgroups
Optimal Borderline Poor

48
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
General discussion
Answer to the research questions The overall aim of this dissertation is to expand the current knowledge about sleep patterns and correlates in adolescents to inform a preventive intervention. Study I demonstrated that poor sleep can be problematic for adolescents´ future functioning in the form of school absenteeism. Moreo-ver, Study II showed that insufficient sleep duration affected a significant portion of early adolescents and was associated with behavioral and emo-tional problems. Social stressors, ICT use and arousal at bedtime were as-sociated with insufficient sleep duration, as hypothesized by the biopsycho-social model of sleep. In Study III, targeting these potential barriers to sleep through time management, with the support of parents and peers and indi-vidualized feedback via an app, resulted in small but positive changes for sleep-deprived adolescents, but the future preventive effect for adolescents currently not at risk is yet to be determined.
More specifically, sleep problems, defined as symptoms of insomnia in Study I, were associated with a threefold risk of future school absenteeism. This is in line with studies on adults (Kessler et al., 2011; Lallukka, Haar-amo, Lahelma, & Rahkonen, 2011; Sivertsen et al., 2009) but also a few other studies showing a cross-sectional and longitudinal association be-tween symptoms of insomnia and absenteeism in adolescents (Egger, Cos-tello, & Angold, 2003; Hysing et al., 2014). This study adds to previous studies by controlling for other psychological risk factors for school absen-teeism (e.g., anxiety, drinking) and thus identifying sleep problems as an important factor for adolescents´ adjustment. These results prompt new questions on whether sleep should be targeted in interventions in order to promote adolescents´ wellbeing and future adjustment, also given the wide-spread reduction in sleep duration in this population.
Study II investigated the prevalence and patterns of sleep duration in a large population of early adolescents. The first aim was to describe the ex-tent of problematic sleep patterns; insufficient sleep duration affected be-tween 12 and 19% of early adolescents, in grades 7 and 8 respectively. This prevalence is lower than in other studies (Do et al., 2013; Garaulet et al., 2011; Hysing et al., 2013; Mak et al., 2012; Meldrum & Restivo, 2014) but this might be explained by the fact that our population was younger (M = 13.6 y) as compared to the majority of studies. Irregular sleep-wake pat-terns on schooldays vs. weekends was extremely common and, on average,

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
49
adolescents went to bed 2 h 15 m later and woke up over 3 h 30 m later on weekends as compared to schooldays. This shift between weekday and weekend sleep times is common worldwide (Gradisar et al., 2011), although wake times were extremely delayed in our sample (1h more than previous studies). This extreme shift is alarming because it is a risk for DSWPD and further sleep deficit (Crowley et al., 2007).
The second aim of Study II was to investigate whether sleep duration was associated with emotional and behavioral problems in a dose-response fash-ion; that is, whether the National Sleep Foundation´ s guidelines for insuf-ficient, borderline and optimal sleep duration (Hirshkowitz et al., 2015) were informative and showed meaningful associations with daytime func-tioning. Results showed that there was a dose-response relationship, inde-pendent of age and gender – although, as expected, girls reported higher levels of emotional problems. These findings demonstrate that emotional and behavioral problems go hand in hand with sleep duration and that sleep duration below the recommended 8-10 hours is in fact related to worse functioning, in line with a growing body of research (Shochat et al., 2014). Experimental evidence has shown that this close relationship between emo-tional-behavioral problems and sleep may be explained by the detrimental effect of lack of sleep on impulse control and emotion regulation, and that sleep and emotions likely affect each other in a bidirectional way (Kahn et al., 2013). So, improving sleep health in adolescents would likely have ben-eficial effects on their daytime functioning as well, which leads to the final aim of Study II.
The third and final aim was to explore potential targets for prevention. According to the biopsychosocial model of sleep (Becker et al., 2015), psy-chosocial and contextual factors (including technology, stress and worry), in conjunction with biological changes, contribute to sleep problems in ad-olescents. Higher cognitive-emotional arousal at bedtime, including think-ing about things to do the next day or replaying the day in one´s mind, were consistently related to worse sleep, independent of age. These results are in line with a comprehensive review of risk and protective factors (Bartel et al., 2014) and suggest that cognitive and emotional arousal at bedtime may be an important target for sleep interventions.
Moreover, almost 50% of the adolescents reported “often” or “almost always” using ICT after bedtime, and this was in turn significantly associ-ated with shorter sleep duration. A recent review (Hale & Guan, 2015) found that ICT was associated with worse sleep outcomes in 90% of the studies, including later bedtimes and shorter sleep duration. ICT use may

50
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
impact sleep by displacing time from sleep, by creating arousal or by delay-ing melatonin release (Cain & Gradisar, 2010). However, given the cross-sectional design in Study II and the majority of studies reviewed (Hale & Guan, 2015), it cannot be excluded that adolescents who have difficulties falling asleep use ICT as a sleep aid. This possibility was supported by a study investigating bidirectional associations between sleep and technology over time. In this study, young adults´ sleep difficulties predicted ICT use but not vice versa (Tavernier & Willoughby, 2014). On the other hand, another study on children (ages 4, 6 and 8) showed reciprocal associations between sleep and technology (Magee, Lee, & Vella, 2014). Furthermore, parents´ rules about ICT have a positive effect on adolescents´ sleep, which supports a causal association between ICT and sleep (Pieters et al., 2014; Smith et al., 2017; Sormunen et al., 2016). So, it is reasonable to assume that sleep and technology may trigger a negative cycle, which is in line with qualitative evidence as well (Adams et al., 2016). Therefore, limiting ICT use at bedtime may promote better sleep.
Furthermore, social stressors, including stress of family life (e.g., conflicts with parents) and school stress (e.g., homework) were associated with poor sleep duration for, younger and older adolescents respectively. In line with these results, a meta-analysis found that a negative family environment was associated with worse sleep in adolescents (Bartel et al., 2014). Moreover, time spent on homework per se was not associated with shorter sleep dura-tion or later bedtimes (Bartel et al., 2014), but this effect might depend on how stressful the activity is perceived to be (Fuligni & Hardway, 2006). So, including stress management strategies and problem-solving in sleep inter-ventions may be a useful strategy to promote sleep.
The results from Study II support the hypothesis that adolescents may be faced with numerous barriers when trying to change their sleep behaviors. Therefore, sleep education programs should include strategies to help ado-lescents overcome these hurdles, such as stress, in order to promote behav-ioral change. This idea was corroborated by focus groups with adolescents (Study III), which confirmed that school stress, combined with the strong need for leisure time, use of technology, and FoMO were perceived as crit-ical barriers to sleep.
Therefore, Study III hypothesized that sleep education, together with time management training, might help adolescents make room for sleep. In ad-dition, the program involved parents and peers and was delivered with the
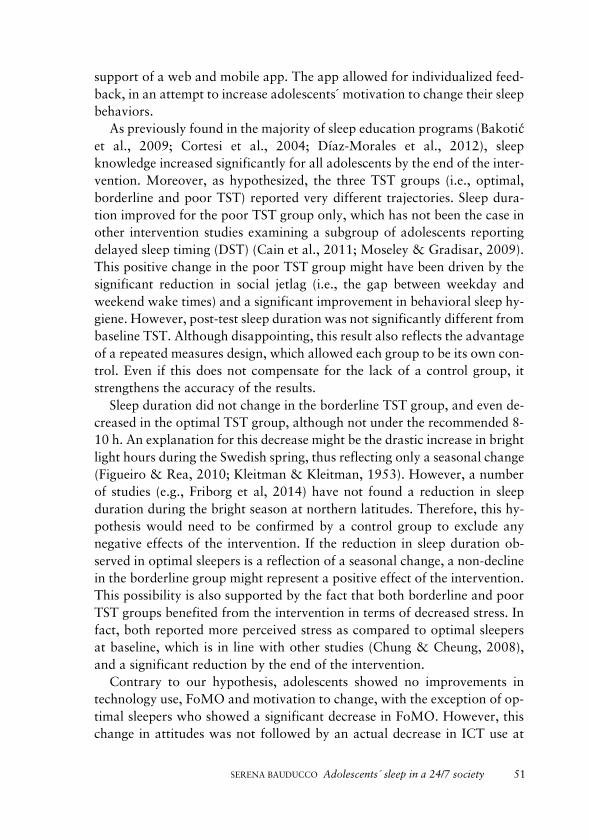
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
51
support of a web and mobile app. The app allowed for individualized feed-back, in an attempt to increase adolescents´ motivation to change their sleep behaviors.
As previously found in the majority of sleep education programs (Bakotić et al., 2009; Cortesi et al., 2004; Díaz-Morales et al., 2012), sleep knowledge increased significantly for all adolescents by the end of the inter-vention. Moreover, as hypothesized, the three TST groups (i.e., optimal, borderline and poor TST) reported very different trajectories. Sleep dura-tion improved for the poor TST group only, which has not been the case in other intervention studies examining a subgroup of adolescents reporting delayed sleep timing (DST) (Cain et al., 2011; Moseley & Gradisar, 2009). This positive change in the poor TST group might have been driven by the significant reduction in social jetlag (i.e., the gap between weekday and weekend wake times) and a significant improvement in behavioral sleep hy-giene. However, post-test sleep duration was not significantly different from baseline TST. Although disappointing, this result also reflects the advantage of a repeated measures design, which allowed each group to be its own con-trol. Even if this does not compensate for the lack of a control group, it strengthens the accuracy of the results.
Sleep duration did not change in the borderline TST group, and even de-creased in the optimal TST group, although not under the recommended 8-10 h. An explanation for this decrease might be the drastic increase in bright light hours during the Swedish spring, thus reflecting only a seasonal change (Figueiro & Rea, 2010; Kleitman & Kleitman, 1953). However, a number of studies (e.g., Friborg et al, 2014) have not found a reduction in sleep duration during the bright season at northern latitudes. Therefore, this hy-pothesis would need to be confirmed by a control group to exclude any negative effects of the intervention. If the reduction in sleep duration ob-served in optimal sleepers is a reflection of a seasonal change, a non-decline in the borderline group might represent a positive effect of the intervention. This possibility is also supported by the fact that both borderline and poor TST groups benefited from the intervention in terms of decreased stress. In fact, both reported more perceived stress as compared to optimal sleepers at baseline, which is in line with other studies (Chung & Cheung, 2008), and a significant reduction by the end of the intervention.
Contrary to our hypothesis, adolescents showed no improvements in technology use, FoMO and motivation to change, with the exception of op-timal sleepers who showed a significant decrease in FoMO. However, this change in attitudes was not followed by an actual decrease in ICT use at

52
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
bedtime. The fact that changes in attitude do not always translate into be-havioral change is a well-known fact (Ajzen & Fishbein, 1975), but another possibility is that there was limited room for improvement as optimal sleep-ers also reported the lowest ICT use at bedtime. Hopefully, this early change in attitudes will benefit optimal sleepers in the future.
Regarding motivation to change, the importance of increasing sleep du-ration decreased in the optimal and borderline TST groups, whereas it did not change for the poor TST group. These results are disappointing given the effort to improve motivation through MI, individualized feedback, and peer and parent support. However, the measure used focused exclusively on motivation to improve sleep duration (by anticipating bedtimes), which has been found difficult to improve in similar interventions (Cain et al., 2011), even when sleep duration actually improved (Bonnar et al., 2015). Also, it might not be surprising that optimal sleepers´ motivation to change (im-portance and commitment) decreased, given that the change in sleep dura-tion may be perceived as less relevant by this group. However, it is worri-some that borderline sleepers considered improving sleep duration as less important by the end of the program. Interestingly, behavioral changes oc-curred in the poor TST group with no apparent improvement in motivation to change (importance, ability, or commitment). This might mean that ad-olescents in this group were already motivated enough (contemplation stage) but it might also indicate that the measure used did not fully capture their motivation to change.
Finally, students´ feedback was generally positive and the app was rated as ‘helpful’, but a significant portion of adolescents did not find the program helpful (22%). Similar studies have found only a small group of adolescents reporting that the program was not relevant, as they did not have a sleep problem (Moseley & Gradisar, 2009). In general, one downside of universal interventions is that they might not be perceived as relevant for all. So, it is crucial to establish whether universal interventions are in fact the best op-tion by evaluating the preventive effect of such interventions (Cassoff et al., 2013). That is, whether the prevalence and incidence of insufficient sleep duration in the population receiving the intervention are lower relative to a control group.
Taken together, these studies show that sleep is strictly related to adoles-cents´ functioning, both longitudinally and cross-sectionally, which suggests that sleep is important for adolescents´ adjustment, which is in line with a growing number of studies. Therefore, further research is needed to improve interventions aimed at promoting sleep health in adolescents. If preventive

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
53
interventions show long-term effects, we might continue to implement uni-versal programs and try to sharpen their impact on motivation and behav-ioral change. One important direction may be to work on supporting an environment that promotes sleep, because asking adolescents to change their sleep behaviors on their own might be an unreasonable demand, given their relatively immature cognitive system (e.g., difficulties weighing long-term consequences vs. immediate rewards) (Steinberg, 2005). If long-term evaluations show that universal programs are not effective, we might need to reevaluate our approach to sleep interventions and turn to selective and indicated approaches. To do so, we need to become better at early identifi-cation. That is, we need to improve our understanding of who is at risk by studying the development of sleep disturbances over time. Psychosocial and contextual factors such as stress and technology are intertwined with sleep but only explain a small portion of variance. Thus, we need to ascertain causality and elucidate the mechanisms through which they might affect sleep – if they do – through experimental and longitudinal studies. Moreo-ver, we need to keep looking for powerful risk and protective factors.
Findings in relation to the theoretical framework The broader theoretical framework for this dissertation was the biopsycho-social model of sleep (Becker et al., 2015), whereas the more specific theo-retical framework used for the intervention (Study III) was based on theories of behavioral change as synthetized by the I-Change model (de Vries et al., 2005).
According to the biopsychosocial model of sleep (Becker et al., 2015), biological, contextual and psychosocial changes typical of adolescence sig-nificantly affect sleep in this developmental period. In Study II, we found a striking shift between weekday and weekend sleep timing, which indicates a large mismatch between adolescents´ circadian preference and societal de-mands (e.g., school start times). This shifting is likely affected by psychoso-cial and contextual variables as well (e.g., the availability of technological devices), but is mainly driven by the changes in the homeostatic and circa-dian systems (Dahl & Lewin, 2002). So, one important area for further re-search is to clarify the contribution of each of the areas involved in the bi-opsychosocial model (i.e., biological, psychosocial, and contextual factors) on sleep changes in adolescence. Studies looking at changes in adolescents´ sleep duration over the last few decades have found a possible global reduc-tion in sleep duration (Keyes et al., 2015; Kronholm et al., 2015; Matric-ciani et al., 2012). Given that biological influence is supposedly stable
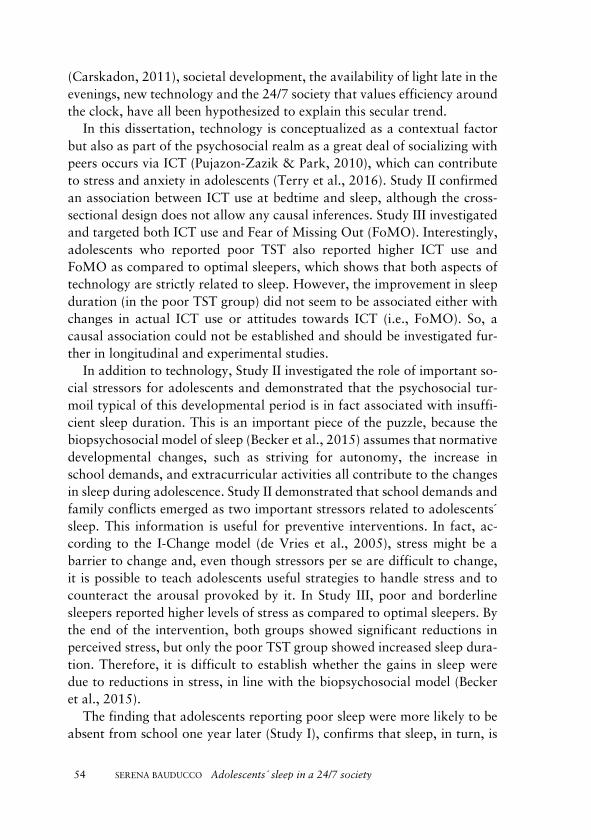
54
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
(Carskadon, 2011), societal development, the availability of light late in the evenings, new technology and the 24/7 society that values efficiency around the clock, have all been hypothesized to explain this secular trend.
In this dissertation, technology is conceptualized as a contextual factor but also as part of the psychosocial realm as a great deal of socializing with peers occurs via ICT (Pujazon-Zazik & Park, 2010), which can contribute to stress and anxiety in adolescents (Terry et al., 2016). Study II confirmed an association between ICT use at bedtime and sleep, although the cross-sectional design does not allow any causal inferences. Study III investigated and targeted both ICT use and Fear of Missing Out (FoMO). Interestingly, adolescents who reported poor TST also reported higher ICT use and FoMO as compared to optimal sleepers, which shows that both aspects of technology are strictly related to sleep. However, the improvement in sleep duration (in the poor TST group) did not seem to be associated either with changes in actual ICT use or attitudes towards ICT (i.e., FoMO). So, a causal association could not be established and should be investigated fur-ther in longitudinal and experimental studies.
In addition to technology, Study II investigated the role of important so-cial stressors for adolescents and demonstrated that the psychosocial tur-moil typical of this developmental period is in fact associated with insuffi-cient sleep duration. This is an important piece of the puzzle, because the biopsychosocial model of sleep (Becker et al., 2015) assumes that normative developmental changes, such as striving for autonomy, the increase in school demands, and extracurricular activities all contribute to the changes in sleep during adolescence. Study II demonstrated that school demands and family conflicts emerged as two important stressors related to adolescents´ sleep. This information is useful for preventive interventions. In fact, ac-cording to the I-Change model (de Vries et al., 2005), stress might be a barrier to change and, even though stressors per se are difficult to change, it is possible to teach adolescents useful strategies to handle stress and to counteract the arousal provoked by it. In Study III, poor and borderline sleepers reported higher levels of stress as compared to optimal sleepers. By the end of the intervention, both groups showed significant reductions in perceived stress, but only the poor TST group showed increased sleep dura-tion. Therefore, it is difficult to establish whether the gains in sleep were due to reductions in stress, in line with the biopsychosocial model (Becker et al., 2015).
The finding that adolescents reporting poor sleep were more likely to be absent from school one year later (Study I), confirms that sleep, in turn, is

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
55
associated with contextual factors such as academic functioning. This sup-ports the bidirectional relationship between sleep and psychosocial/contex-tual factors depicted in the biopsychosocial model of sleep (Becker et al., 2015).
According to the I-Change Model (de Vries et al., 2005), the intention to change is prompted by the individual´s attitudes towards the behavior (ben-efits of sleep), the perceived ability to change (self-efficacy), and social in-fluences (social norms). In line with this, MI argues that individuals need to feel “ready”, “able” and “willing” in order to change their behaviors (Mil-ler & Johnson, 2008). We hypothesized that time management would in-crease adolescents´ self-efficacy to change their sleep behaviors. Interestingly however, the changes in sleep behaviors (e.g., sleep hygiene and duration) observed in the poor TST group occurred with no apparent improvement in motivation to change (importance, ability or commitment). This might mean that adolescents in this group were already motivated and confident in their ability to change (contemplation or preparation stage) and benefited from the concrete action plan (e.g., when and how to implement a calm bedtime routine) offered by the intervention (Gollwitzer & Sheeran, 2006).
However, the positive changes in sleep duration and social jetlag ob-tained by this group were already declining by the end of the intervention, suggesting that adolescents might have not felt confident enough to main-tain these gains (de Vries, Backbier, Kok, & Dijkstra, 1995). Another rea-son for this relapse might be that adolescents were not convinced that the benefits of changing their sleep behaviors outweighed the costs, thus moving them back to the pre-contemplation stage (i.e., not considering change). This is not surprising given the numerous reasons adolescents have to stay up in the evenings. Moreover, early adolescents might have difficulties tak-ing into account long-term goals and consequences in their decision-making (Steinberg, 2005). Therefore, it is crucial to promote an environment that supports sleep. This includes removing possible contextual barriers to sleep, i.e., by moving sport practice earlier in the evenings, and encouraging posi-tive social influences such as parent-set bedtimes and conveying healthy sleep norms through the media. Although we did not measure social influ-ence in Study III (e.g., perceived peer norms and pressure, parent support), the involvement of parents and peers in the program was limited and should be intensified in future interventions. Future studies would also benefit from integrating theories of behavioral change and should measure social influ-ence, efficacy and attitudes more thoroughly, both to be able to better tailor programs to individual needs and to clarify the mechanisms of change.

56
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Regarding the use of a more individually tailored approach to improve adolescents´ motivation, an observation from Study III is that not all partic-ipants might have benefited from the individual feedback. That is, there is a risk that adolescents who were already more motivated were also more likely to read and respond to the feedback.
To conclude, in accordance with the biopsychosocial model of sleep, sleep in adolescence is a complex behavior and in order to prompt a change in this population it is necessary to undertake a comprehensive approach. Modifying contextual factors might be necessary in order to promote ado-lescents´ sleep because it might be too much to ask for adolescents to change their sleep habits on their own. Another important consideration is that the magnitude of effect that can be expected from sleep interventions might de-pend on the impact that psychosocial and contextual targets have on ado-lescents´ sleep, over and above biological influences.
Implications The findings from this dissertation have several implications for practice.
Study I showed that poor sleepers were three times more likely to report future school absenteeism and Study II showed that sleep problems seem to be strictly intertwined with emotional and behavioral problems. So, an ad-olescent who is not sleeping well might not be functioning well either. Of-ten, however, sleep problems are underreported by parents and under-iden-tified by practitioners (Blunden et al., 2004). Study II demonstrated that insufficient sleep duration was prevalent in early adolescents and more so in the older cohort (+ 1 year). So, it is important to raise awareness of prob-lematic sleep patterns in adolescents, their consequences, and the im-portance of sleep hygiene among teachers, parents, GPs, psychologists, and school nurses. Sleep problems might be less visible than behavioral problems and academic underachievement. However, sleep is intertwined with these problems and sleepiness and attention difficulties might be an important early sign to pay attention to. One of the most dramatic changes is the shift-ing between weekend and weekday bedtimes and wake times (Crowley et al., 2007). However, one study found that parents do not usually set week-end bedtimes, even when they do set weekday bedtimes (Short 2011). So, parents´ might need to be informed of the importance of regular sleep sched-ules early on to prevent DST disturbances. On the other hand, it is as im-portant to normalize sleep changes occurring during adolescence in order to avoid creating ‘sleep-anxiety’ among adolescents and parents.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
57
DST was extremely common (studies II and III) and weekend vs. weekday wake times differed by more than three hours. According to the DSM-V (American Psychiatric Association, 2013), a difference of more than two hours is a diagnostic feature of DSWPD. However, the diagnosis includes other criteria (e.g., daytime functioning) that help distinguish between a normal and problematic pattern and DST should not be used alone (Lovato, Gradisar, Short, Dohnt, & Micic, 2013). So, the majority of adolescents displaying a large shift in sleep timing do not fulfill the diagnosis for DSWPD (i.e., the prevalence of DSWPD is much lower), but this pattern might still be problematic because the effort to realign bedtimes and wake times to early school times is hard. That is, our body adapts more easily to delaying than to anticipating sleep (Dahl & Lewin, 2002). Moreover, a large shift between weekends and weekdays may maintain a pattern of insuffi-cient sleep duration during the school week. Nevertheless, not all adoles-cents report daytime consequences of social jetlag (Lovato et al., 2013; Saxvig et al., 2012) and a much lower portion of adolescents reported in-sufficient sleep duration in Study II. This might also depend on school start times. In Europe, school start times are usually later than in the US and may be more suited to adolescents´ preferred sleep schedules (Crowley et al., 2007). This would speak against the need to delay school start times in all countries. In addition, in Sweden, school schedules include a few later morn-ings, which might fit adolescents´ circadian timing better, but might also promote irregular sleep schedules. So, it is worth investigating this further to develop useful recommendations to parents, schools and practitioners.
Study II also aimed to identify important targets for prevention and Study III aimed to test a new intervention. Thus, there are several important im-plications for prevention. As expected, stress, technology, and cognitive and emotional arousal at bedtime were significantly associated with reduced sleep duration. Therefore, in order to promote sleep, it is important to help adolescents reduce arousal at bedtime by promoting good sleep hygiene and a healthy lifestyle (Bartel et al., 2016). Because sleep is a complex behavior (Cassoff, Gruber, & Knäuper, 2014), sleep programs should probably be longer in order to consolidate changes in sleep habits. As shown in other health preventive interventions (e.g., drug use), persistence rather than in-tensity might lead to better effects (Durlak, 1997). This would be possible if sleep programs were integrated into the school curriculum from early grades throughout adolescence. Moreover, it would be beneficial to inte-grate the sleep curriculum with other health areas as well, such as physical

58
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
activity and diet (Blunden et al., 2016). This would require some adjust-ments to the curriculum but would likely integrate well with existing efforts in schools.
Furthermore, given the limited success in motivating adolescents to sleep more and that they might be cognitively too immature to make long-term health plans (Steinberg, 2005), it might be helpful to create an environment that promotes sleep. This starts, as mentioned before, with raising aware-ness about the importance of sleep in this developmental period and in-volves parents, schools, sport organizations, health services, and media. For example, sport organizations should be asked not to schedule practice late in the evenings, and parents should be supported in their bedtime and ICT use rule-setting throughout adolescence (Bartel et al., 2014).
This approach is also compatible with a stepped care approach for sleep programs, where sleep education is the first step (universal), followed by some additional clinical guidance in case of more severe problems (selective and indicated), and finally more intensive clinical guidance in the case of a diagnosed sleep disorder (Blunden et al., 2016). A stepped care approach would therefore facilitate identification of more severe cases but certainly require additional resources and a joint effort of several actors (e.g., school nurses, teachers and health care services).
A stepped care approach might be facilitated by the use of new technol-ogies to more effectively deliver individually tailored sleep education, which is advancing in other health promotion areas (Portnoy, Scott-Sheldon, John-son, & Carey, 2008). However, in our experience, the addition of an app did not facilitate contact with the adolescents. In fact, the participants had difficulties in completing the homework assignments and readings without reminders from the teachers. An important difference between sleep and other health behaviors, such as drinking or smoking, is that it is difficult for adolescents to recognize the negative consequences of insufficient sleep du-ration (Cassoff et al., 2013). A prevailing positive attitude towards late bed-times and short sleep might lead to a lower engagement in sleep programs. This warrants further research on how (or whether) sleep behaviors differ from other health behaviors, and a thorough examination of successful online promotion programs.
Future research There is a clear need for longitudinal studies to investigate the development of sleep problems in adolescence, which would allow better identification of who will develop problems and how to improve intervention efforts.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
59
Individual-oriented analyses over time may help identify subgroups that run a higher risk of developing chronic sleep problems. This might make early identification possible and shift the focus of interventions from the whole population (universal) to subgroups at particular risk of developing sleep disturbances and their related consequences (selective or indicated). For example, poor sleepers showed higher levels of depression, anxiety, an-ger, norm-breaking behaviors and stress in studies II and III. So, more stud-ies are needed to disentangle how emotional and behavioral problems relate to the development of sleep disturbances and vice versa.
Another vital research agenda is to examine the effectiveness of preven-tive interventions. In fact, according to the prevention paradox (Rose, 2001), the majority of new cases will come from the larger group that is yet not showing a risk of developing the problem. Therefore, the knowledge and skills delivered through preventive interventions will come to hand only when the problem presents. However, no study has yet looked at the long-term preventive effects of sleep interventions. Moreover, it is necessary to compare school-based interventions with alternative interventions, such as postponing school start times, to determine the most cost-effective option.
Furthermore, in order to improve sleep education programs, a thorough examination of their mechanisms of change is needed. In the case of the I-Change model (de Vries et al., 2005), attitudes, social influences and self-efficacy need to be measured adequately to establish whether the program works through the hypothesized mechanisms. Social influences in particular deserve some special attention. There is a paucity of research on peer norms and influences in relation to sleep behaviors. Only one study to date has used peer network analysis to explore this issue (Mednick et al., 2010). Moreover, peer networks may be studied to further explore the relationship between sleep and technology, as ICT is often used in a social context. Peer norms can be used in interventions to normalize and promote a desired be-havior; for example, by showing that peers are not as likely to drink alcohol as expected or not as likely to have unprotected sex (Durlak, 1995). On the other hand, it might be that sleep norms agree upon an inadequate amount of sleep (e.g., “7 h of sleep is enough”); in that case, one aim of sleep inter-ventions would be to change the norm. So, social norms may be a very pow-erful tool for improving adolescents´ sleep.
Finally, it is vital to continue to investigate the causes and consequences of sleep deficit and disentangle the contribution of biological changes, and psychosocial and contextual influences. In particular, longitudinal studies are needed to identify risk and protective factors for the development of

60
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
sleep problems. For example, more studies are needed to clarify the rela-tionship between technology and sleep. One area that may be further ex-plored is how FoMO, or feelings of dependency on technology, affect sleep in adolescents. It might be that adolescents who experience FoMO are also more prone to displacing time for sleep by engaging in ICT activities. Fur-ther, daily diaries may give some insights into the time displacement hy-pothesis. What distracts adolescents from sleeping? Could it be that ICT, which involves socializing with others, provokes cognitive and emotional arousal (e.g., rumination) and thus disrupts sleep? These situations are dif-ficult to reproduce in laboratory experiments, but may be observed through daily diaries (Sally et al., 2015).
Methodological strengths and weaknesses A potential limitation was that all variables used in this dissertation were self-reported, which might have resulted in response bias and inaccuracy of responses and lead to spurious associations between variables (Fan et al., 2006). On the other hand, some countermeasures were taken to limit the potential pitfalls of self-reporting questionnaires. For example, teachers were asked to leave the room while adolescents filled out the questionnaires to ensure confidentiality, and questionnaires included reversed items and were inspected after data collection for unserious responses.
Moreover, sleep was not measured through objective measures and there is a risk for over or underestimation. For example, sleep onset latency (SOL) may be confused by adolescents with time spent doing calm activities in bed (e.g., ICT) and not actually trying to fall asleep. Adolescents’ self-reports, however, have been found to be accurate when validated with objective sleep measures (Short, Gradisar, Lack, Wright, & Carskadon, 2012; Wolfson & Carskadon, 2003). Moreover, a strength of our sleep duration measure was that it was a combination of multiple questions (i.e., bedtime, SOL, and wake time), which might be advantageous over a single item.
Furthermore, the cross-sectional design used in Study II has obvious lim-itations. No temporal relation can be established between sleep and emo-tional and behavioral problems, or between potential risk and protective factors. However, the cross-sectional design was valuable in that it allowed us to identify in a timely manner some potentially important factors for adolescents' sleep.
Another advantage of Study II was the large sample size. All public schools in the county were included, which likely included participants from a wide range of socioeconomic backgrounds, thus making the sample likely

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
61
representative of the population. However, as demonstrated in Study I, ad-olescents who report sleep problems are also more likely to be absent from school. Therefore, some important individuals might be missing from the analyses because students who systematically missed school could have been missing at the time of data collection and were excluded.
The strength of Study I was its longitudinal design, which allowed us to establish a temporal relationship between sleep and school absenteeism.
Study III did not include a control group or a follow-up and the schools that participated were not randomized. Therefore, the results should be in-terpreted with caution. The lack of a control group limits the interpretation of the changes in sleep duration as being either due to the intervention, nat-ural development, or seasonal changes. Moreover, the lack of a long-term follow-up does not allow evaluation of the preventive effect of the interven-tion; however, follow-up data and the possibility of using a natural control group have been planned and are now underway, although are not available within the time frame for this dissertation.
Moreover, the lack of thorough measures of social influence, self-efficacy and attitudes does not allow us to investigate the hypothesized mechanisms of change. The choice of a short motivational screening was partly to limit the length of the questionnaire and leave more time for the actual lesson. On the other hand, one advantage of the weekly measures, although time-consuming, was that each group worked as its own control, thus facilitating the interpretation of the results. Another advantage of the intervention study was the sample size, which allowed for subgroup analyses and yielded different results worth investigating further.
Summary and concluding remarks Sleep seems to play an important role in adolescents´ functioning. In par-
ticular, there was a possible association between sleep problems and school attendance and a cross-sectional association between sleep deficit and emo-tional and behavioral problems. This is worrisome, given that sleep deficit was prevalent in 12-19% of early adolescents. Therefore, preventing sleep problems in adolescents is a pressing issue. However, previous efforts to improve sleep in this population have not been completely successful and this might be because they do not take into account the numerous barriers that adolescents´ sleep faces. Factors such as social stressors, ICT use and cognitive-emotional arousal at bedtime were associated with shorter sleep duration, as hypothesized by the biopsychosocial model. Therefore, we hy-pothesized that, by improving time management skills, adolescents might
62
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
be able to allocate more time for sleep. The intervention was universal (i.e., delivered to the whole population) so we did not expect that optimal sleep-ers would sleep more by the end of the intervention, but we hypothesized that all adolescents would show early improvements in sleep hygiene, moti-vation to change, ICT, and stress. As expected, the poor sleepers improved the most, showing better sleep hygiene, less perceived stress, longer sleep duration and more stable weekend-weekday sleep patterns. However, the gains in sleep duration were already declining by the end of the intervention. Furthermore, there were no early improvements in the other groups, except for a reduction in stress in the borderline group. Contrary to expectations, motivation to change and ICT use and FoMO did not improve for any of the groups, which might undermine the case for long-term benefits of the intervention. Future studies should investigate the long-term effects of pre-ventive interventions, to determine whether they are effective in: 1) reducing the prevalence of insufficient sleep (in the poor TST group), and 2) reducing the incidence of new cases (in borderline and optimal TST groups), relative to a control group. Further, we might need to consider alternative or addi-tional approaches to sharpen our efforts to improve adolescents´ sleep health. In particular, contextual changes might be necessary to support bet-ter sleep habits in adolescents (e.g., school start times, extracurricular sched-ules, parental support, peer norms) and stepped care approaches could de-liver tailored interventions to adolescents suffering from sleep problems, while also promoting sleep health in the general adolescent population.
Conclusions • Adolescents reporting poor sleep in the form of insomnia symp-
toms, were three times more likely to be absent from school at one-year follow-up. So, improving adolescents´ sleep may be beneficial for adolescents´ functioning.
• Sleep deficit, defined as weekly sleep duration below the recom-mended seven hours, was common and more prevalent in older ad-olescents, and was associated with emotional and behavioral prob-lems. So, preventing sleep deficit in this population is especially im-portant.
• Social stressors, cognitive and emotional arousal and technology use at bedtime were significantly associated with insufficient sleep duration. Mechanisms and causal associations should be further in-vestigated through longitudinal and experimental studies, but these preliminary results support the contribution of psychosocial and

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
63
contextual factors as depicted by the biopsychosocial model of sleep in adolescents.
• A preventive school-based sleep intervention that aimed to improve adolescents´ time management strategies was successful in improv-ing sleep duration and regularizing sleep patterns in adolescents at risk. However, these changes might not be maintained after the in-tervention. Future studies should investigate the long-term effects of universal interventions.
• Future sleep interventions should carefully study mechanisms of change (including changes in attitudes, ability and social support as suggested by the I-Change model), and might benefit from promot-ing environmental changes that support sleep health and relieve ad-olescents from the sole responsibility of changing their own sleep behaviors.
• Studying developmental trajectories of sleep problems is crucial to identifying risk and protective factors to inform future sleep inter-ventions, whether universal, selective, or indicated.

64
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
References
Adams, S. K., Williford, D. N., Vaccaro, A., Kisler, T. S., Francis, A., & Newman, B. (2016). The young and the restless: Socializing trumps sleep, fear of missing out, and technological distractions in first-year college students. International Journal of Adolescence and Youth, 1-12.
Ajzen, I., & Fishbein, M. (1975). Belief, attitude, intention and behavior: An introduction to theory and research: Reading, MA: Addison-Wesley.
American Psychiatric Association, A. (Ed.) (2013). The Diagnostic and Statistical Manual of Mental Disorders: DSM 5: bookpointUS.
Auger, R. R., & Crowley, S. J. (2013). Circadian Timing: Delayed Sleep Phase Disorder. The Oxford Handbook of Infant, Child, and Adolescent Sleep and Behavior, 327.
Bakotić, M., Radošević-Vidaček, B., & Košćec, A. (2009). Educating adolescents about healthy sleep: experimental study of effectiveness of educational leaflet. Croatian medical journal, 50(2), 174-181.
Bandura, A. (2006). Adolescent development from an agentic perspective. Self-efficacy beliefs of adolescents, 5(1-43).
Barker, G. (2007). Adolescents, social support and help-seeking behaviour. Geneva: World Health Organization, 10-11.
Bartel, K., & Gradisar, M. (2017). New Directions in the Link Between Technology Use and Sleep in Young People Sleep Disorders in Children (pp. 69-80): Springer.
Bartel, K., Williamson, P., van Maanen, A., Cassoff, J., Meijer, A. M., Oort, F., . . . Gradisar, M. (2016). Protective and risk factors associated with adolescent sleep: findings from Australia, Canada, and The Netherlands. Sleep Med, 26, 97-103. doi:10.1016/j.sleep.2016.07.007
Bartel, K. A., Gradisar, M., & Williamson, P. (2014). Protective and risk factors for adolescent sleep: A meta-analytic review. Sleep medicine reviews.
Baum, K. T., Desai, A., Field, J., Miller, L. E., Rausch, J., & Beebe, D. W. (2014). Sleep restriction worsens mood and emotion regulation in adolescents. Journal of child psychology and psychiatry, 55(2), 180-190.
Becker, S. P., Langberg, J. M., & Byars, K. C. (2015). Advancing a biopsychosocial and contextual model of sleep in adolescence: a review and introduction to the special issue. Journal of Youth and Adolescence, 44(2), 239-270.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
65
Beebe, D. W., Rose, D., & Amin, R. (2010). Attention, learning, and arousal of experimentally sleep-restricted adolescents in a simulated classroom. Journal of Adolescent Health, 47(5), 523-525.
Biggs, S. N., Pizzorno, V. A., van den Heuvel, C. J., Kennedy, J. D., Martin, A. J., & Lushington, K. (2010). Differences in parental attitudes towards sleep and associations with sleep–wake patterns in Caucasian and Southeast Asian school-aged children in Australia. Behavioral sleep medicine, 8(4), 207-218.
Blunden, S., Benveniste, T., & Thompson, K. (2016). Putting Children’s Sleep Problems to Bed: Using Behavior Change Theory to Increase the Success of Children’s Sleep Education Programs and Contribute to Healthy Development. Children, 3(3), 11.
Blunden, S., & Galland, B. (2014). The complexities of defining optimal sleep: Empirical and theoretical considerations with a special emphasis on children. Sleep medicine reviews, 18(5), 371-378.
Blunden, S., Kira, G., Hull, M., & Maddison, R. (2012). Does sleep education change sleep parameters? Comparing sleep education trials for middle school students in Australia and New Zealand. The Open Sleep Journal, 5(1), 12-18.
Blunden, S., Lushington, K., Lorenzen, B., Ooi, T., Fung, F., & Kennedy, D. (2004). Are sleep problems under-recognised in general practice? Archives of Disease in Childhood, 89(8), 708-712.
Blunden, S., & Rigney, G. (2015). Lessons learned from sleep education in schools: a review of dos and don'ts. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine, 11(6), 671.
Bonnar, D., Gradisar, M., Moseley, L., Coughlin, A.-M., Cain, N., & Short, M. A. (2015). Evaluation of novel school-based interventions for adolescent sleep problems: does parental involvement and bright light improve outcomes? Sleep Health, 1(1), 66-74.
Brand, S., Hatzinger, M., Beck, J., & Holsboer-Trachsler, E. (2009). Perceived parenting styles, personality traits and sleep patterns in adolescents. Journal of adolescence, 32(5), 1189-1207.
Byrne, D., Davenport, S., & Mazanov, J. (2007). Profiles of adolescent stress: The development of the adolescent stress questionnaire (ASQ). Journal of adolescence, 30(3), 393-416.
Cain, N., & Gradisar, M. (2010). Electronic media use and sleep in school-aged children and adolescents: A review. Sleep medicine, 11(8), 735-742.
Cain, N., Gradisar, M., & Moseley, L. (2011). A motivational school-based intervention for adolescent sleep problems. Sleep medicine, 12(3), 246-251.

66
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Carskadon, M. A. (2011). Sleep in adolescents: the perfect storm. Pediatric Clinics of North America, 58(3), 637-647.
Carskadon, M. A., Acebo, C., & Jenni, O. G. (2004). Regulation of adolescent sleep: implications for behavior. Annals of the New York Academy of Sciences, 1021(1), 276-291.
Casey, B., Jones, R. M., Levita, L., Libby, V., Pattwell, S. S., Ruberry, E. J., . . . Somerville, L. H. (2010). The storm and stress of adolescence: insights from human imaging and mouse genetics. Developmental psychobiology, 52(3), 225-235.
Casey, B., Jones, R. M., & Somerville, L. H. (2011). Braking and accelerating of the adolescent brain. Journal of Research on Adolescence, 21(1), 21-33.
Cassoff, J., Gruber, R., & Knäuper, B. (2014). Evaluating the effectiveness of the Motivating Teens To Sleep More program in advancing bedtime in adolescents: a randomized controlled trial. BMC Psychology, 2(1), 1.
Cassoff, J., Gruber, R., Sadikaj, G., & Knäuper, B. (2014). What Motivational and Awareness Variables are Associated with Adolescents’ Intentions to Go to Bed Earlier? Current Psychology, 33(2), 113-129.
Cassoff, J., Knäuper, B., Michaelsen, S., & Gruber, R. (2013). School-based sleep promotion programs: Effectiveness, feasibility and insights for future research. Sleep medicine reviews, 17(3), 207-214.
Centrala Studiestödsnämnden, C. (2013). Questions and answers about absenteeism.
Chang, A.-M., Aeschbach, D., Duffy, J. F., & Czeisler, C. A. (2015). Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proceedings of the National Academy of Sciences, 112(4), 1232-1237.
Christner, R. W., Forrest, E., Morley, J., & Weinstein, E. (2007). Taking cognitive-behavior therapy to school: A school-based mental health approach. Journal of Contemporary Psychotherapy, 37(3), 175-183.
Chung, K.-F., & Cheung, M.-M. (2008). Sleep-wake patterns and sleep disturbance among Hong Kong Chinese adolescents. Sleep, 31(2), 185.
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of health and social behavior, 385-396.
Cortesi, F., Giannotti, F., Sebastiani, T., Bruni, O., & Ottaviano, S. (2004). Knowledge of sleep in Italian high school students: pilot-test of a school-based sleep educational program. Journal of Adolescent Health, 34(4), 344-351.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
67
Crowley, S. J., Acebo, C., & Carskadon, M. A. (2007). Sleep, circadian rhythms, and delayed phase in adolescence. Sleep medicine, 8(6), 602-612.
Curcio, G., Ferrara, M., & De Gennaro, L. (2006). Sleep loss, learning capacity and academic performance. Sleep medicine reviews, 10(5), 323-337.
Dagys, N., McGlinchey, E. L., Talbot, L. S., Kaplan, K. A., Dahl, R. E., & Harvey, A. G. (2012). Double trouble? The effects of sleep deprivation and chronotype on adolescent affect. Journal of child psychology and psychiatry, 53(6), 660-667.
Dahl, R. E., & Lewin, D. S. (2002). Pathways to adolescent health sleep regulation and behavior. Journal of Adolescent Health, 31(6), 175-184.
de Vries, H., Backbier, E., Kok, G., & Dijkstra, M. (1995). The Impact of Social Influences in the Context of Attitude, Self‐Efficacy, Intention, and Previous Behavior as Predictors of Smoking Onset1. Journal of applied social psychology, 25(3), 237-257.
de Vries, H., Mesters, I., Van de Steeg, H., & Honing, C. (2005). The general public’s information needs and perceptions regarding hereditary cancer: an application of the Integrated Change Model. Patient education and counseling, 56(2), 154-165.
Dewald, J. F., Meijer, A. M., Oort, F. J., Kerkhof, G. A., & Bögels, S. M. (2010). The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: a meta-analytic review. Sleep medicine reviews, 14(3), 179-189.
Díaz-Morales, J. F., Prieto, P. D., Barreno, C. E., Mateo, M. J. C., & Randler, C. (2012). Sleep beliefs and chronotype among adolescents: The effect of a sleep education program. Biological Rhythm Research, 43(4), 397-412.
Do, Y. K., Shin, E., Bautista, M. A., & Foo, K. (2013). The associations between self-reported sleep duration and adolescent health outcomes: What is the role of time spent on Internet use? Sleep medicine, 14(2), 195-200.
Dohnt, H., Gradisar, M., & Short, M. A. (2012). Insomnia and its symptoms in adolescents: comparing DSM-IV and ICSD-II diagnostic criteria. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine, 8(3), 295.
Dolcini, M. M. (2014). A New Window Into Adolescents' Worlds: The Impact of Online Social Interaction on Risk Behavior. Journal of Adolescent Health, 54(5), 497-498. doi:http://dx.doi.org/10.1016/j.jadohealth.2014.02.013
Durlak, J. A. (1995). School-based prevention programs for children and adolescents (Vol. 34): Sage Publications.

68
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Durlak, J. A. (1997). Successful prevention programs for children and adolescents: Springer Science & Business Media.
Egger, H. L., Costello, J. E., & Angold, A. (2003). School refusal and psychiatric disorders: a community study. Journal of the American Academy of Child & Adolescent Psychiatry, 42(7), 797-807.
Eggermont, S., & Van den Bulck, J. (2006). Nodding off or switching off? The use of popular media as a sleep aid in secondary‐school children. Journal of paediatrics and child health, 42(7‐8), 428-433.
Fan, X., Miller, B. C., Park, K.-E., Winward, B. W., Christensen, M., Grotevant, H. D., & Tai, R. H. (2006). An exploratory study about inaccuracy and invalidity in adolescent self-report surveys. Field Methods, 18(3), 223-244.
Figueiro, M. G., & Rea, M. S. (2010). Evening daylight may cause adolescents to sleep less in spring than in winter. Chronobiology international, 27(6), 1242-1258.
Fobian, A. D., Avis, K., & Schwebel, D. C. (2016). The Impact of Media Use on Adolescent Sleep Efficiency. Journal of developmental and behavioral pediatrics: JDBP, 37(1), 9.
Friborg, O., BJORVATN, B., Amponsah, B., & PALLESEN, S. (2012). Associations between seasonal variations in day length (photoperiod), sleep timing, sleep quality and mood: a comparison between Ghana (5) and Norway (69). Journal of sleep research, 21(2), 176-184.
Fuligni, A. J., & Hardway, C. (2006). Daily Variation in Adolescents' Sleep, Activities, and Psychological Well‐Being. Journal of Research on Adolescence, 16(3), 353-378.
Gabrielle, R., Sarah, B., Carol, M., James, D., Somayeh, P., Lisa, M., & Timothy, O. (2015). Can a school-based sleep education program improve sleep knowledge, hygiene and behaviours using a randomised controlled trial. Sleep medicine.
Garaulet, M., Ortega, F., Ruiz, J., Rey-Lopez, J., Beghin, L., Manios, Y., . . . Kafatos, A. (2011). Short sleep duration is associated with increased obesity markers in European adolescents: effect of physical activity and dietary habits. The HELENA study. International journal of obesity, 35(10), 1308-1317.
Gentile, D. A., Bender, P. K., & Anderson, C. A. (2016). Violent video game effects on salivary cortisol, arousal, and aggressive thoughts in children. Computers in Human Behavior.
Giannotti, F., Cortesi, F., & Carskadon, M. (2002). Sleep patterns and daytime function in adolescence: an epidemiological survey of an Italian high school student sample. Adolescent sleep patterns: Biological, social, and psychological influences, 132-147.

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
69
Gollwitzer, P. M., & Sheeran, P. (2006). Implementation intentions and goal achievement: A meta‐analysis of effects and processes. Advances in experimental social psychology, 38, 69-119.
Gradisar, M., Gardner, G., & Dohnt, H. (2011). Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep medicine, 12(2), 110-118.
Gregory, A. M., & Sadeh, A. (2012). Sleep, emotional and behavioral difficulties in children and adolescents. Sleep medicine reviews, 16(2), 129-136.
Gren-Landell, M., Björklind, A., Tillfors, M., Furmark, T., Svedin, C. G., & Andersson, G. (2009). Child and Adolescent Psychiatry and Mental Health. Child and adolescent psychiatry and mental health, 3, 36.
Grønli, J., Byrkjedal, I. K., Bjorvatn, B., Nødtvedt, Ø., Hamre, B., & Pallesen, S. (2016). Reading from an iPad or from a book in bed: the impact on human sleep. a randomized controlled crossover trial. Sleep medicine, 21, 86-92.
Hale, L., & Guan, S. (2015). Screen time and sleep among school-aged children and adolescents: A systematic literature review. Sleep medicine reviews, 21, 50-58.
Haynes, P. L., Bootzin, R. R., Smith, L., Cousins, J., Cameron, M., & Stevens, S. (2006). Sleep and aggression in substance-abusing adolescents: results from an integrative behavioral sleep-treatment pilot program. SLEEP-NEW YORK THEN WESTCHESTER-, 29(4), 512.
Heath, M., Sutherland, C., Bartel, K., Gradisar, M., Williamson, P., Lovato, N., & Micic, G. (2014). Does one hour of bright or short-wavelength filtered tablet screenlight have a meaningful effect on adolescents’ pre-bedtime alertness, sleep, and daytime functioning? Chronobiology international, 31(4), 496-505.
Hirshkowitz, M., Whiton, K., Albert, S. M., Alessi, C., Bruni, O., DonCarlos, L., . . . Kheirandish-Gozal, L. (2015). National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health, 1(1), 40-43.
Hysing, M., Haugland, S., Stormark, K. M., Bøe, T., & Sivertsen, B. (2014). Sleep and school attendance in adolescence: Results from a large population-based study. Scandinavian journal of public health, 1403494814556647.
Hysing, M., Pallesen, S., Stormark, K. M., Lundervold, A. J., & Sivertsen, B. (2013). Sleep patterns and insomnia among adolescents: a population‐based study. Journal of sleep research, 22(5), 549-556.
Ivarsson, M., Anderson, M., Åkerstedt, T., & Lindblad, F. (2013). The effect of violent and nonviolent video games on heart rate
70
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
variability, sleep, and emotions in adolescents with different violent gaming habits. Psychosomatic medicine, 75(4), 390-396.
Janz, N. K., & Becker, M. H. (1984). The health belief model: A decade later. Health education quarterly, 11(1), 1-47.
Johnson, E. O., Roth, T., Schultz, L., & Breslau, N. (2006). Epidemiology of DSM-IV insomnia in adolescence: lifetime prevalence, chronicity, and an emergent gender difference. Pediatrics, 117(2), e247-e256.
Kahn, M., Sheppes, G., & Sadeh, A. (2013). Sleep and emotions: bidirectional links and underlying mechanisms. International Journal of Psychophysiology, 89(2), 218-228.
Kearney, C. A. (2008). School absenteeism and school refusal behavior in youth: A contemporary review. Clinical Psychology Review, 28(3), 451-471.
Kerr, M., & Stattin, H. (2000). What parents know, how they know it, and several forms of adolescent adjustment: further support for a reinterpretation of monitoring. Developmental psychology, 36(3), 366.
Kessler, R. C., Berglund, P. A., Coulouvrat, C., Hajak, G., Roth, T., Shahly, V., . . . Walsh, J. K. (2011). Insomnia and the performance of US workers: results from the America insomnia survey. Sleep, 34(9), 1161.
Keyes, K. M., Maslowsky, J., Hamilton, A., & Schulenberg, J. (2015). The Great Sleep Recession: Changes in Sleep Duration Among US Adolescents, 1991–2012. Pediatrics, 135(3), 460-468.
King, D. L., Gradisar, M., Drummond, A., Lovato, N., Wessel, J., Micic, G., . . . Delfabbro, P. (2013). The impact of prolonged violent video‐gaming on adolescent sleep: an experimental study. Journal of sleep research, 22(2), 137-143.
Kira, G., Maddison, R., Hull, M., Blunden, S., & Olds, T. (2014). Sleep education improves the sleep duration of adolescents: a randomized controlled pilot study. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine, 10(7), 787.
Kleitman, N., & Kleitman, H. (1953). The sleep-wakefulness pattern in the Arctic. The Scientific Monthly, 76, 349-356.
Koutakis, N., Stattin, H., & Kerr, M. (2008). Reducing youth alcohol drinking through a parent‐targeted intervention: the Örebro Prevention Program. Addiction, 103(10), 1629-1637.
Kronholm, E., Puusniekka, R., Jokela, J., Villberg, J., Urrila, A. S., Paunio, T., . . . Tynjälä, J. (2015). Trends in self‐reported sleep problems, tiredness and related school performance among Finnish

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
71
adolescents from 1984 to 2011. Journal of sleep research, 24(1), 3-10.
Lallukka, T., Haaramo, P., Lahelma, E., & Rahkonen, O. (2011). Sleep problems and disability retirement: a register-based follow-up study. American journal of epidemiology, 173(8), 871-881.
Lemola, S., Schwarz, B., & Siffert, A. (2012). Interparental conflict and early adolescents’ aggression: Is irregular sleep a vulnerability factor? Journal of adolescence, 35(1), 97-105.
Levine, L. E., Waite, B. M., & Bowman, L. L. (2007). Electronic media use, reading, and academic distractibility in college youth. CyberPsychology & Behavior, 10(4), 560-566.
Liljenberg, B., Almqvist, M., Hetta, J., Roos, B., & Agren, H. (1987). The prevalence of insomnia: the importance of operationally defined criteria. Annals of Clinical Research, 20(6), 393-398.
Linton, S. J., & Bryngelsson, L. (2000). Insomnia and its relationship to work and health in a working-age population. Journal of Occupational Rehabilitation, 10(2), 169-183.
Lo, J. C., Ong, J. L., Leong, R., Gooley, J. J., & Chee, M. (2016). Cognitive performance, sleepiness, and mood in partially sleep deprived adolescents: the need for sleep study. Sleep, 39(3), 687-698.
Lovato, N., Gradisar, M., Short, M., Dohnt, H., & Micic, G. (2013). Delayed sleep phase disorder in an Australian school-based sample of adolescents. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine, 9(9), 939.
Lund, H. G., Reider, B. D., Whiting, A. B., & Prichard, J. R. (2010). Sleep patterns and predictors of disturbed sleep in a large population of college students. Journal of Adolescent Health, 46(2), 124-132.
Maciejewski, D. F., van Lier, P. A., Branje, S. J., Meeus, W. H., & Koot, H. M. (2017). A daily diary study on adolescent emotional experiences: Measurement invariance and developmental trajectories. Psychological assessment, 29(1), 35.
Madden, T. J. (1986). Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology, 22(5), 453-474.
Magee, C. A., Lee, J. K., & Vella, S. A. (2014). Bidirectional relationships between sleep duration and screen time in early childhood. JAMA pediatrics, 168(5), 465-470.
Main, C. J. (1983). The modified somatic perception questionnaire (MSPQ). Journal of psychosomatic research, 27(6), 503-514.
Mak, K. K., Lee, S. L., Ho, S. Y., Lo, W. S., & Lam, T. H. (2012). Sleep and academic performance in Hong Kong adolescents. Journal of School Health, 82(11), 522-527.

72
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Maslowsky, J., & Ozer, E. J. (2014). Developmental trends in sleep duration in adolescence and young adulthood: evidence from a national United States sample. Journal of Adolescent Health, 54(6), 691-697.
Matricciani, L., Olds, T., & Petkov, J. (2012). In search of lost sleep: secular trends in the sleep time of school-aged children and adolescents. Sleep medicine reviews, 16(3), 203-211.
Medieråd, S. (2015). Ungar & medier 2015. Retrieved from Mednick, S. C., Christakis, N. A., & Fowler, J. H. (2010). The Spread of
Sleep Loss Influences Drug Use in Adolescent Social Networks. PloS one, 5(3), e9775. doi:10.1371/journal.pone.0009775
Meijer, A. M., Reitz, E., & Dekoviċ, M. (2016). Parenting matters: a longitudinal study into parenting and adolescent sleep. Journal of sleep research, 25(5), 556-564.
Meldrum, R. C., & Restivo, E. (2014). The behavioral and health consequences of sleep deprivation among US high school students: Relative deprivation matters. Preventive medicine, 63, 24-28.
Miller, M. B., Janssen, T., & Jackson, K. M. (2016). The prospective association between sleep and initiation of substance use in young adolescents. Journal of Adolescent Health.
Miller, W. R., & Johnson, W. R. (2008). A natural language screening measure for motivation to change. Addictive Behaviors, 33(9), 1177-1182.
Miller, W. R., & Rollnick, S. (2012). Motivational interviewing: Helping people change: Guilford press.
Moseley, L., & Gradisar, M. (2009). Evaluation of a school-based intervention for adolescent sleep problems. Sleep, 32(3), 334.
Murdock, K. K., Horissian, M., & Crichlow-Ball, C. (2016). Emerging Adults’ Text Message Use and Sleep Characteristics: A Multimethod, Naturalistic Study. Behavioral sleep medicine, 1-14.
Nation, M., Crusto, C., Wandersman, A., Kumpfer, K. L., Seybolt, D., Morrissey-Kane, E., & Davino, K. (2003). What works in prevention: Principles of effective prevention programs. American Psychologist, 58(6-7), 449.
National Sleep Foundation, N. (2006). 2006 Sleep in America Poll: Summary of Findings. Washington, DC: National Sleep Foundation.
Noland, H., Price, J. H., Dake, J., & Telljohann, S. K. (2009). Adolescents’ sleep behaviors and perceptions of sleep. Journal of School Health, 79(5), 224-230.
Norman, S. B., Hami Cissell, S., Means‐Christensen, A. J., & Stein, M. B. (2006). Development and validation of an overall anxiety severity

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
73
and impairment scale (OASIS). Depression and anxiety, 23(4), 245-249.
O'Connell, M. E., Boat, T., Warner, K. E., & Council, N. R. (2009). Using a developmental framework to guide prevention and promotion.
Olsson, G., & von Knotting, A.-L. (1997). Depression among Swedish adolescents measured by the self rating scale Center for Epidemiology Studies-Depression Child (CES-DC). European child & adolescent psychiatry, 6(2), 81-87.
Owens, J. A., & Mindell, J. A. (2011). Pediatric insomnia. Pediatric Clinics of North America, 58(3), 555-569.
Partinen, M., & Gislason, T. (1995). Basic Nordic Sleep Questionnaire (BNSQ): a quantitated measure of subjective sleep complaints. Journal of sleep research, 4(s1), 150-155.
Pasch, K. E., Latimer, L. A., Cance, J. D., Moe, S. G., & Lytle, L. A. (2012). Longitudinal bi-directional relationships between sleep and youth substance use. Journal of Youth and Adolescence, 41(9), 1184-1196.
Peach, H. D., & Gaultney, J. F. (2013). Sleep, impulse control, and sensation-seeking predict delinquent behavior in adolescents, emerging adults, and adults. Journal of Adolescent Health, 53(2), 293-299.
Pieters, D., De Valck, E., Vandekerckhove, M., Pirrera, S., Wuyts, J., Exadaktylos, V., . . . Cluydts, R. (2014). Effects of pre-sleep media use on sleep/wake patterns and daytime functioning among adolescents: the moderating role of parental control. Behavioral sleep medicine, 12(6), 427-443.
Polos, P. G., Bhat, S., Gupta, D., O'Malley, R. J., DeBari, V. A., Upadhyay, H., . . . Chokroverty, S. (2015). The impact of Sleep Time-Related Information and Communication Technology (STRICT) on sleep patterns and daytime functioning in American adolescents. Journal of adolescence, 44, 232-244.
Portnoy, D. B., Scott-Sheldon, L. A., Johnson, B. T., & Carey, M. P. (2008). Computer-delivered interventions for health promotion and behavioral risk reduction: a meta-analysis of 75 randomized controlled trials, 1988–2007. Preventive medicine, 47(1), 3-16.
Prochaska, J., & Diclemente, C. Stages and procesess of self-change of smoking: toward an integrative model of change. J Consult Clin Psichol. 1983; 51: 390-5.
Przybylski, A. K., Murayama, K., DeHaan, C. R., & Gladwell, V. (2013). Motivational, emotional, and behavioral correlates of fear of missing out. Computers in Human Behavior, 29(4), 1841-1848.
Pujazon-Zazik, M., & Park, M. J. (2010). To tweet, or not to tweet: gender differences and potential positive and negative health outcomes of

74
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
adolescents’ social internet use. American journal of men's health, 4(1), 77-85.
Rajaratnam, S. M., Licamele, L., & Birznieks, G. (2015). Delayed sleep phase disorder risk is associated with absenteeism and impaired functioning. Sleep Health, 1(2), 121-127.
Reynolds, C. M., Gradisar, M., Kar, K., Perry, A., Wolfe, J., & Short, M. A. (2015). Adolescents who perceive fewer consequences of risk‐taking choose to switch off games later at night. Acta paediatrica, 104(5), e222-e227.
Rigney, G., Blunden, S., Maher, C., Dollman, J., Parvazian, S., Matricciani, L., & Olds, T. (2015). Can a school-based sleep education programme improve sleep knowledge, hygiene and behaviours using a randomised controlled trial. Sleep medicine, 16(6), 736-745.
Rose, G. (2001). Sick individuals and sick populations. International journal of epidemiology, 30(3), 427-432.
Rosen, L., Carrier, L. M., Miller, A., Rokkum, J., & Ruiz, A. (2016). Sleeping with technology: cognitive, affective, and technology usage predictors of sleep problems among college students. Sleep Health, 2(1), 49-56.
Rångtell, F. H., Ekstrand, E., Rapp, L., Lagermalm, A., Liethof, L., Bucaro, M. O., . . . Benedict, C. (2016). Two hours of evening reading on a self-luminous tablet vs. reading a physical book does not alter sleep after daytime bright light exposure. Sleep medicine, 23, 111-118.
Sally, I., Kuo, C., Updegraff, K. A., Zeiders, K. H., McHale, S. M., Umaña-Taylor, A. J., & De Jesús, S. A. R. (2015). Mexican American adolescents’ sleep patterns: Contextual correlates and implications for health and adjustment in young adulthood. Journal of Youth and Adolescence, 44(2), 346-361.
Saxvig, I. W., Pallesen, S., Wilhelmsen-Langeland, A., Molde, H., & Bjorvatn, B. (2012). Prevalence and correlates of delayed sleep phase in high school students. Sleep medicine, 13(2), 193-199.
Shochat, T., Cohen-Zion, M., & Tzischinsky, O. (2014). Functional consequences of inadequate sleep in adolescents: A systematic review. Sleep medicine reviews, 18(1), 75-87.
Short, M. A., Gradisar, M., Lack, L. C., Wright, H., & Carskadon, M. A. (2012). The discrepancy between actigraphic and sleep diary measures of sleep in adolescents. Sleep medicine, 13(4), 378-384.
Short, M. A., Gradisar, M., Lack, L. C., Wright, H. R., Dewald, J. F., Wolfson, A. R., & Carskadon, M. A. (2013). A cross-cultural comparison of sleep duration between US and Australian adolescents the effect of school start time, parent-set bedtimes, and

SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
75
extracurricular load. Health Education & Behavior, 40(3), 323-330.
Short, M. A., Gradisar, M., Wright, H., Lack, L. C., Dohnt, H., & Carskadon, M. A. (2011). Time for bed: parent-set bedtimes associated with improved sleep and daytime functioning in adolescents. Sleep, 34(6), 797.
Sivertsen, B., Øverland, S., Bjorvatn, B., Mæland, J. G., & Mykletun, A. (2009). Does insomnia predict sick leave?: The Hordaland Health Study. Journal of psychosomatic research, 66(1), 67-74.
Smith, L. J., Gradisar, M., King, D. L., & Short, M. (2017). Intrinsic and extrinsic predictors of video-gaming behaviour and adolescent bedtimes: the relationship between flow states, self-perceived risk-taking, device accessibility, parental regulation of media and bedtime. Sleep medicine, 30, 64-70.
Sormunen, M., Turunen, H., & Tossavainen, K. (2016). Self-reported bedtimes, television-viewing habits and parental restrictions among Finnish schoolchildren (aged 10–11 years, and 2 years later aged 12–13 years): Perspectives for health. European Journal of Communication, 0267323116629877.
Spear, L. P. (2000). The adolescent brain and age-related behavioral manifestations. Neuroscience & Biobehavioral Reviews, 24(4), 417-463.
Steinberg, L. (2005). Cognitive and affective development in adolescence. Trends in cognitive sciences, 9(2), 69-74.
Storfer‐Isser, A., Lebourgeois, M. K., Harsh, J., Tompsett, C. J., & Redline, S. (2013). Psychometric properties of the adolescent sleep hygiene scale. Journal of sleep research, 22(6), 707-716.
Tavernier, R., & Willoughby, T. (2014). Sleep problems: predictor or outcome of media use among emerging adults at university? Journal of sleep research, 23(4), 389-396.
Terry, C. A., Mishra, P., & Roseth, C. J. (2016). Preference for multitasking, technological dependency, student metacognition, & pervasive technology use: An experimental intervention. Computers in Human Behavior, 65, 241-251.
Thomée, S., Härenstam, A., & Hagberg, M. (2011). Mobile phone use and stress, sleep disturbances, and symptoms of depression among young adults-a prospective cohort study. BMC public health, 11(1), 66.
van der Lely, S., Frey, S., Garbazza, C., Wirz-Justice, A., Jenni, O. G., Steiner, R., . . . Schmidt, C. (2015). Blue blocker glasses as a countermeasure for alerting effects of evening light-emitting diode screen exposure in male teenagers. Journal of Adolescent Health, 56(1), 113-119.

76
SERENA BAUDUCCO Adolescents´ sleep in a 24/7 society
Weaver, E., Gradisar, M., Dohnt, H., Lovato, N., & Douglas, P. (2010). The effect of presleep video-game playing on adolescent sleep. J Clin Sleep Med, 6(2), 184-189.
Wing, Y. K., Chan, N. Y., Yu, M. W. M., Lam, S. P., Zhang, J., Li, S. X., . . . Li, A. M. (2015). A school-based sleep education program for adolescents: a cluster randomized trial. Pediatrics, 135(3), e635-e643.
Wittmann, M., Dinich, J., Merrow, M., & Roenneberg, T. (2006). Social jetlag: misalignment of biological and social time. Chronobiology international, 23(1-2), 497-509.
Wolfson, A. R., & Carskadon, M. A. (1998). Sleep schedules and daytime functioning in adolescents. Child development, 875-887.
Wolfson, A. R., & Carskadon, M. A. (2003). Understanding adolescent's sleep patterns and school performance: a critical appraisal. Sleep medicine reviews, 7(6), 491-506.
Wolfson, A. R., Harkins, E., Johnson, M., & Marco, C. (2015). Effects of the Young Adolescent Sleep Smart Program on sleep hygiene practices, sleep health efficacy, and behavioral well-being. Sleep Health, 1(3), 197-204.
Woods, H. C., & Scott, H. (2016). # Sleepyteens: Social media use in adolescence is associated with poor sleep quality, anxiety, depression and low self-esteem. Journal of adolescence, 51, 41-49.
Yoo, S.-S., Gujar, N., Hu, P., Jolesz, F. A., & Walker, M. P. (2007). The human emotional brain without sleep—a prefrontal amygdala disconnect. Current Biology, 17(20), R877-R878.
Zoccola, P. M., Dickerson, S. S., & Lam, S. (2009). Rumination predicts longer sleep onset latency after an acute psychosocial stressor. Psychosomatic medicine, 71(7), 771-775.





























