Embed Size (px)
Citation preview
CHILDREN’S SERVICES
INCLUSION SERVICES GUIDANCE
Administering Medicines Policy (Model Policy for schools)
Responsible Officer Contact Details
Richard Marchant
(Specialist Teaching and Advice)
Tel: 01305 224063 e-mail: [email protected]
Date issued: 21 September 2012 Reviewed: December 2014
(No change to policy – attached Pages 8-11 Supporting students with Medical Conditions)
Blank Page
Administering medicines policy for Sturminster Newton High School This policy has been structured based upon the guidance provided by information from the Guidance and Code of Practice - First Aid at Work (Issue 2 April 2011) provided by Dorset County Council, guidance from local Health Services, professional teaching associations, Dorset County Council Health and Safety information and the most recent government advice to Schools and Early Years settings. Aims 1. To provide clear procedural guidance on the Administering of Medicines and record
keeping at Sturminster Newton High School 2. To ensure that the children and young people in our school are safe and are able to
attend school regularly. 3. To enable children and young people with medical conditions to be included in the
school curriculum and other activities. 4. To support children and young people with complex medical conditions and or long
term medical needs. Sturminster Newton High School will adhere to the advice contained in Managing Medicines in Schools and Early Years Settings – DfES 2005, Multi-Agency Guidance for the Management of Long Term Health Conditions for Children and Young People - DSCB 2011, and Supporting Pupils with Medical Needs – DfEE 1996. The school is mindful of the Dorset For You web document, Medical Advice for Schools and Early Years Settings (found on Schoolsnet). This policy should be read in conjunction with the school’s safeguarding policy and child protection procedures. Arrangements have been made for the following:
managing prescription medicines that may need to be taken during the day;
managing prescription medicines on trips and outings, including school transport;
the safe storage of medicines and accurate record keeping;
procedures for access to medicines during emergency situations;
adhering to risk management procedures involving medicines. More information is contained on the school website. Safeguarding of children is paramount. The Governing Body has a duty under Section 175 (or Section 157, for Academies) of the Education Act 2002 to safeguard and promote the welfare of children in this school. Sturminster Newton High School is responsible for adhering to Health Care Plans, maintaining and monitoring records and demonstrating that children are provided with appropriate medical support for which training has been given by qualified personnel. It should be noted that failure to adhere to Health Care Plans could affect insurance cover and increase liability. The school will follow First Aid principles and seek to act in the interest of preserving life when in the event of an emergency. The school will accept written notice from parents / carers that relate to particular medical or religious issues that might affect the manner in which emergency cases are managed.
Appropriate / standard forms will be used to support the management and administering of medicines (see ‘Managing Medicines in Schools and Early Years Settings’ DfES 2005
and Multi-Agency Guidance for the Management of Long Term Health Conditions for Children and Young People - DSCB 2011). We understand that the key information requested must not be changed as it would affect any potential insurance claims for medical malpractice. Responsibilities Parents It must be remembered that the prime responsibility for a child’s / young person’s health rests with the parents / carers. Where possible, prescribed or non-prescribed medicines should be administered by parents outside of the school day. If this is not possible, parents should talk to school staff and also make requests to administer medicines in writing to the Headteacher. Parents are asked to deliver medicines to school in the original container(s) and ensuring that the medicine is not out of date and that it has been stored correctly. All medicines must be marked with the following information clearly indicated:
the child’s name on the medicine;
when the medicine should be given;
the prescribed dose and pharmacist’s instruction, e.g., after meals. Parents must notify the school immediately (in writing) of any changes or alteration to a prescription requiring adjustment to be made to any previous arrangement about medicines for their child / young person. Headteacher The Headteacher will make appropriate arrangements for medicines to be stored safely in a locked cabinet. Medicines must be kept in the container supplied which must be clearly labelled with the name of the child and instruction for usage. The school will ensure that all medicines held are not out of date and that they are returned to parents routinely after use. Some medicines (insulin, liquid antibiotics) may need to be kept in a fridge but must not be frozen. These medicines must be placed in suitable additional sealed/airtight containers such as a Tupperware box and marked ‘medicines’. Medicine cabinets will be supervised closely and emptied at least once each term. The Headteacher will make suitable arrangements in partnership with parents that enable children / young people to maintain a prescribed course of treatment. They will liaise with staff / parents / nominated support so that recommended medical treatment can be sustained, and that those people are appropriately trained to administer medication. Staff will not be directed to administer medicines; however, they can choose to volunteer to do so if they so wish. All staff will be advised to refer to advice from their professional associations before volunteering to administer medicines. Together with school Governors, the Headteacher will review this policy at appropriate intervals, in line with local advice, so that the well-being of children and young people and their health is safeguarded. The Headteacher will ensure that all staff and parents/carers are aware of this policy and the procedures for dealing with medical needs at Sturminster Newton High School].

[School] will ensure the following: staff work in partnership with parents/carers to ensure the well-being of child and
young people; that interruption to school attendance for medical reasons will be kept to a minimum; staff who have agreed to administer medicines will receive the appropriate training; adherence to Health Care Plans; that records are maintained detailing an accurate history of the administration of
medicines for the school that information recorded when administering medicines includes: name of child /
young person, the name of the medicine to be administered, confirmation that the medicine is being given and that it is not out of date, that it is being administered to the correct person, the dosage given, and the name and signature of the person administering or supervising, the date, place and time that the medicine was administered;
that suitable back-up systems are in place to cover the administration of medicines staff duties in the event of staff absence;
if there are any doubts or confusion about arrangements for administering medication, staff must consult with the parents and Headteacher;
that no child or young person under 16 will be given medicines without their parents’ written consent;
all cultural and religious views, made known to the school in writing, will be respected; the principles and advice provided in Guidance for Administering Medicines in
Schools and Early Years Settings (DCC Nov 2011) will be used. The school is committed to assisting children with long-term or complex medical needs and working in partnership with their parents /carers to enable full access to schooling. Staff Training Most medicines to be administered will not require professional training; however the school will ensure that staff supervising the administering of medicines will understand that accurate records are to be kept and are completed at the time of being administered. Staff who maintain these records should be clear about what action to take, (such as referring to the Designated Senior Person for Child Protection) if they become concerned about the welfare of an individual pupil. If a Health Care Plan is applied to particular children / young people additional training must be given by a nominated Health professional, e.g., use of a nebuliser, using Epipens. Training received or cascaded from parents will not be accepted unless otherwise instructed by a health professional. Record of Training Forms must be completed by the Health Professional and copies held both with the child/young persons records and by the supervising member of staff (or the Headteacher). (See Multi-Agency Guidance for the Management of Long Term Health Conditions for Children and Young People – DSCB 2011; section 3.3 and 3.4 including Chart E.) Reasonable adjustments The school understands it’s duties under the Equality Act 2010 to make reasonable adjustments and enable children and young people to have equitable access to education. Children and young people with complex or significant medical needs will be included in activities for as much as their health permits. Child or young person refuses, or not well enough to take medicines If a child refuses to take medicine as prescribed, the records must state this clearly and the parents/carer must be informed immediately. Children / young people will not be forced to receive medicine if they do not wish to do so. ( E.g., see ‘Managing Medicines
in Schools and Early Years Settings’, Form 6 – enter REFUSED in the ‘dose given’ column.) If a child or young person is ill / injured and therefore unable to receive the agreed prescribed medication, the person designated to supervise the taking of medicine will consult with parents / carers immediately and advise the Headteacher of their actions. If the child vomits or has diarrhoea soon after receiving medication, parents must be contacted so that they can seek further medical advice. Self medication In some cases it might be appropriate that children/ young people self administer medicines, e.g., inhalers, epipens. The school will encourage those with long term medical conditions to take responsibility for administering their own medication but continue to ask staff to supervise so that the appropriate records can been complete for safeguarding purposes. Storage of Medicines The school will adhere to the advice contained in Guidance and Code of Practice - First Aid at Work (Issue 2 April 2011), and Guidance for Administering Medicines in Schools and Early Years Settings (DCC Nov 2011). Emergency arrangements Care is taken to ensure that all children and young people are safe. The school has [insert number] ‘First Aid at Work’ qualified first aiders, [insert number] ‘Emergency First Aid at Work’ qualified first aiders, [insert number] ‘Paediatric First Aid’ qualified first aiders (if applicable) and [insert number] Emergency First-Aid trained staff. [See DCC Guidance and Code of Practice – First Aid at Work (Issue 2 April 2011) for further information.] Children and young people with life threatening medical conditions or that require close monitoring / supervision may have Health Care Plans issued by Health professionals that provide contact details for emergency situations, e.g., anaphylaxis, diabetes, or epilepsy. Asthma can also be life threatening. All cases deemed ‘complex’ or ‘serious’ medical conditions have emergency contact details held in the school office.
Children and young people who are at risk due to their medical condition hold a Grab Pack (collated information to pass to a doctor or ambulance crew in an emergency) that must accompany them at all times. The purpose of the pack is to provide emergency services with up to date information such as: diagnosis of principle conditions, key personnel and medical contacts, medication taken, up to date records of medicines that have been administered together with other relevant medical information and an agreement with parents/carers about what to do in an emergency. Off-site activities / school trips All arrangements for medicines, including the storage of medicines, Health Care Plans, and Risk Management programmes will apply for any off-site activities or school trips. A member of staff will be appointed to ensure there are suitable arrangements for storage, and recording of the medicines when assessing any risks associated for the trip, particularly for those children and young people with long term or complex health conditions. All off-site activities will be evaluated in terms of proximity and accessibility to emergency services and any implications for those with short or long term medical conditions before receiving approval to go ahead from the Headteacher / Governors.
Equality Statement [SCHOOL] is mindful of its Equality Duties; respecting religious belief and ensuring that support is provided for those with disability needs that might be affected by this policy. Where there are language or communication issues, and to avoid any misunderstanding, the parents / carers and Headteacher will agree an appropriate course of action. The Headteacher will engage interpreters or signers when required to ensure that full understanding of a child’s / young person’s medicine needs are determined accurately. http://webarchive.nationalarchives.gov.uk/20110218194057/http://www.teachernet.gov.uk/docbank/index.cfm?id=8340 ] The member of staff overseeing medical arrangements is: The school has one medicine cabinet located: 1.School Front office
Adopted date: March 2012
Headteacher: Approved
Governing body: Approved
Reviewed date: Sept 2014
Next Review: Sept 2016

Supporting Students with Medical Conditions Definition Pupils’ medical needs may be broadly summarised as being of two types: (a) Short-term, affecting their participation in school activities when they are on a course of medication. (b) Long-term, potentially limiting their access to education and requiring extra care and support School Ethos Schools have a responsibility for the health and safety of students in their care. The Health and Safety at Work Act 1974 makes employers responsible for the health and safety of employees and anyone else on the premises. In the case of students with special medical needs, the responsibility of the employer is to make sure that safety measures cover the needs of all students at the school. This may mean making special arrangements for particular students so that they can access their full and equal entitlement to all aspects of the curriculum. In this case, individual procedures may be required. Sturminster Newton High School is responsible for making sure that relevant staff know about and are, if necessary, trained to provide any additional support that students with medical conditions (long or short term) may need. The Children and Families Act 2014 places a duty on schools to make arrangements for children with medical conditions. Pupils with medical conditions have the same right of admission to school as other children and cannot be refused admission or excluded from school on medical grounds alone. However, teachers and other school staff in charge of students have a common law duty to act ‘in loco parentis’ and must ensure the safety of all students in their care. To this end, we reserve the right to refuse admittance to a child with an infectious disease, where there may be a risk posed to others or to the health of the child involved. This duty also extends to teachers leading activities taking place off the school site. The prime responsibility for a child's health lies with the parent, who is responsible for the child's medication and must supply the school with all relevant information needed in order for proficient care to be given to the child. The school takes advice and guidance from a range of sources, including the School Nurse, Health professionals and the child’s GP in addition to the information provided by parents in the first instance. This enables us to ensure we assess and manage risk and minimise disruption to the learning of the child and others who may be affected (for example, class mates). Our Aims
- To support students with medical conditions, so that they have full access to education, including physical education and educational visits
- To ensure that school staff involved in the care of children with medical needs are fully informed and adequately trained by a professional in order to administer support or prescribed medication
- To comply fully with the Equality Act 2010 for students who may have disabilities or special educational needs.
- To liaise where necessary with healthcare professionals, where a student has an Individual Healthcare Plan
- To respond sensitively, discreetly and quickly to situations where a child with a medical condition requires support
- To keep, monitor and review appropriate records

Unacceptable Practice While school staff will use their professional discretion in supporting individual students, it is unacceptable to:
Prevent children from accessing their medication
Assume every child with the same condition requires the same treatment
Ignore the views of the child or their parents / carers; ignore medical advice
Prevent children with medical conditions accessing the full curriculum, unless specified in their
a medical condition
Prevent children from eating, drinking or taking toilet breaks where this is part of effective management of their condition
Require parents to administer medicine where this interrupts their working day
Require parents to accompany their child with a medical condition on a school trip as a condition of that child taking part Entitlement Sturminster Newton High School provides full access to the curriculum for every child wherever possible. We believe that students with medical needs have equal entitlement and must receive necessary care and support so that they can take advantage of this. However, we also recognise that employees have rights in relation to supporting students with medical needs, as follows: Employees may:
- Choose whether or not they wish to be involved
- Receive appropriate training
- Work to clear guidelines
- Bring to the attention of Senior Leadership any concern or matter relating to the support of students with medical conditions Expectations It is expected that:
- Parents will inform school of any medical condition which affects their child.
- Parents will supply school with appropriately prescribed medication, where the dosage information and regime is clearly printed by a pharmacy on the container, and complete forms 3A and form 5
- Parents will ensure that medicines to be given in school are in date and clearly labelled
- Parents will co-operate in training their children to self-administer medicine if this is appropriate, and that staff members will only be involved if this is not possible
- Medical professionals involved in the care of children with medical needs will fully inform staff beforehand of the child’s condition, its management and implications for the school life of that individual
- Sturminster Newton High School will ensure that, where appropriate, children are involved in discussing the management and administration of their medicines and are able to access and administer their medicine if this is part of their Individual Healthcare plan (for example, an inhaler)
- School staff will liaise as necessary with Healthcare professionals and services in order to access the most up-to-date advice about a pupil’s medical needs and will seek support and training in the interests of the pupil
- Transitional arrangements between schools will be completed in such a way that Sturminster Newton High School will ensure full disclosure of relevant medical information, Healthcare plans and support needed in good time for the child’s receiving school to adequately prepare

- Individual Healthcare plans will be written, monitored and reviewed regularly and will include the views and wishes of the child and parent in addition to the advice of relevant medical professionals Procedure The Governing Body of Sturminster Newton High School ensures that an appropriate level of insurance is in place and reflects the level of risk presented by children with medical conditions. See QBE Insurance (Europe) Limited policy number Y096684QBE0114A. (Policy held by School Business Manager, Mr D James) Information Children with serious medical conditions will have their photo and brief description of condition, along with any other necessary information, in the staffroom. Children with medical conditions which may require emergency attention, e.g. epilepsy, diabetes, will have their names and an Individual Healthcare Plan clearly accessible on SiMs/PARs and all adults dealing with the child will have their attention drawn to this information. In an emergency In a medical emergency, teachers have been appropriately trained to administer emergency first aid if necessary. If possible, the school’s First Aiders, Mrs Moore and Mrs Reeves (front office) or in their absence Mrs Bruton, will be asked to attend. If an ambulance needs to be called, staff will:
Outline the full condition and how it occurred
Give details regarding the child’s date of birth, address, parents’ names and any known medical conditions. (taken from SiMs)
And then contact the child’s parent/carer If an ambulance has been called a member of SLT will need to be informed after the incident
When transferring children to hospital Staff cars should not be used. Parents must always be called in a medical emergency, but do not necessarily need to be present for a child to be taken to hospital. Administration of medicines Only essential medicines will be administered during the school day. Parents must complete written permission forms before any medicine is administered. Medicines to be given during the school day must be in their original container. Controlled drugs can also be administered, subject to all other conditions as described in the Policy. Essential medicines will be administered on Educational Visits, subject to the conditions above. A risk assessment may be needed before the visit takes place. Staff supervising the visit will be responsible for safe storage and administration of the medicine during the visit. Named staff members will give medicines (see end of Policy). Before administering any medicine, staff must check that the medicine belongs to the child, must check that the dosage they are giving is correct, and that written permission has been given. Any child refusing to take medicine in school will not be made to do so, and parents will be informed about the dose being missed. All doses administered will be recorded on the appropriate forms (located in the school reception office). All medicines will be stored safely. Medicines needing refrigeration will be stored in the fridge in the front office. Some medicines (inhalers, etc) will be kept in the child’s classroom and carried

with the children, for ease of access during outside activities. All medicines must be clearly labelled. Controlled drugs or prescribed medicines will be kept in the locked cabinet in the front office. Access to these medicines is restricted to the named persons. Epipens are kept in a clearly labelled and easily accessible box in the reception office. Each individual’s Epipen is stored in a box with that has the student’s photo on the front of it. Inhalers that need to be stored in the office are marked with the child’s name. All children with an inhaler must take them on educational visits, however short in duration. Epipen – Any member of staff can administer an Epipen in an emergency. Epipen training is conducted in school on a yearly basis. Ambulances must be called for a child who may require an Epipen. An ambulance must be called immediately. Parents should be contacted after this call has been made. Complaints Should parents be unhappy with any aspect of their child’s care at Sturminster Newton High School, they must discuss their concerns with the school. This will be with the child’s form tutor in the first instance, with whom any issues should be managed. If this does not resolve the problem or allay concern, the problem should be brought to the attention of the Head of Year. If the problem is still not resolved then the complaint should be brought to a member of the leadership team who will, where necessary, bring concerns to the attention of the Headteacher. In the unlikely event of this not resolving the issue, the parents must make a formal complaint using the Sturminster Newton High School Complaints Procedure. Trained Staff School First Aiders (full certificate) are: Mrs K Moore – Admin Officer (training updated October 2014) Mrs V Reeves – Admin Assistant (training updated June 2014) Emergency First Aid: Mrs K Moore Office First Aid at Work Nov. 2014 ex. Dorset Ambulance Service Mrs V Reeves Office First Aid at Work June 2017 ex. Dorset Ambulance Service Mrs E Miles EM’s Emergency Aid in School June 2017 ex. St John’s Mrs R Weeks PE Emergency Aid in School June 2017 ex. St John’s Mr O Jones PE Emergency Aid in School June 2017 ex. St John’s Mrs J Quickfal lPE Emergency Aid in School June 2017 ex. St John’s Mr A Henley PE Emergency Aid in School June 2017 ex. St John’s Mrs J Bruton Office Emergency Aid in School June 2015 ex. Mrs S Matthews First Response Rota Named people for administering medicines: Mrs K Moore Admin Officer Mrs V Reeves Admin Assistant Mrs J Bruton Head’s PA/Admin Manager Mrs J Barron Headteacher Mr D Harris Deputy Head
Guidance and Code of Practice FIRST AID at WORK
ISSUE 2 April 2011 Health and Safety Team Human Resources
FIRST AID
2
Section 1 Contents
Contents Page Subject Section 1 Issue record and contents pages Page 1 Cover page, authorisation and issue details Page 2 Contents Section 2 Introduction Page 3 2.1 Purpose Page 3 2.2 References Page 4 2.3 Terms used in this document Page 4 2.4 Revisions to this document Page 4 2.5 Summary of changes in this issue Page 5 2.6 Contact details Section 3 Responsibilities / Training / Provision / Procedures
Page 5 3.1 Responsibilities Page 5 3.1.1 Heads of Service / Directors Page 5 3.1.2 Line Managers Page 6 3.1.3 Premises Managers / Headteachers Page 6 3.1.4 First aiders FAW / EFAW Page 6 3.1.5 Emergency First Aid (DCC ELS) trained personnel Page 7 3.1.6 Health & Safety Team Page 7 3.2 Risk Assessment of first aid requirements Page 8 3.3 Guidance for specific establishments Page 8 3.3.1 Social care premises Page 9 3.3.1(a) DCC social care minimum provision Page 9 3.3.1(b) Resuscitation in social care premises Page 10 3.3.2 Schools Page 10 3.3.2(a) Minimum recommended number of first aiders in schools Page 10 3.3.2(b) Further guidance for schools Page 10 3.3.2(c) Treatment of minor injuries Page 11 3.3.2(d) Identifying illnesses / injuries to children Page 11 3.3.2(e) Head injuries Page 11 3.3.2(f) Calling an ambulance / transportation / moving pupils Page 12 3.3.2(g) First aid requirements for schools with swimming pools Page 12 3.3.2(h) Off-site visits Page 13 3.4 Shared or multi-occupied sites Page 13 3.5 Provision of information to employees detailing first aid arrangements Page 14 3.6 First aid training Page 14 3.6.1 Training for first aiders Page 14 3.6.2 Basic skills refresher training Page 15 3.6.3 Selection of first aiders Page 15 3.6.4 Emergency First aid at work - EFAW (one-day course) contents Page 15 3.6.5 First aid at Work - FAW (three-day course) contents Page 16 3.6.6 Early Years – requirement for paediatric first aid training Page 17 3.6.7 Defibrillator training Page 17 3.7 Infection control / waste disposal Page 17 3.7.1 Universal precautions

3
Section 2 Introduction
Page 17 3.7.2 Blood/body fluid spills Page 18 3.7.3 Disposal of waste Page 18 3.7.4 Hazard disposal packs Page 18 3.8 Legal indemnity for first aiders Page 18 3.9 Guidance for first aiders on reporting accidents Page 19 3.10 First aid equipment, boxes, supplies and facilities Page 19 3.10.1 First aid boxes and content Page 20 3.10.2 First aid rooms Page 20 3.10.3 First aid supplies Page 20 3.10.4 Use of “Burnshield”(gel) dressings Page 21 3.11 Administering of medicines Page 21 3.12 Managing medicines in schools and early years settings Appendices
Appendix A Basic skill refresher training resource (annual refresher training) Appendix B First aid provision flowchart for schools with a swimming pool
2.1 Purpose Dorset County Council (DCC) undertakes, in so far as in reasonably practicable, to comply with the Health and Safety (First Aid) Regulations 1981 and it’s Approved Code of Practice. First aid provision is part of the wider management of health and safety within the County Council. The requirements within a Directorate or section will be determined by the hazards associated with the work or activities undertaken. The risk assessment process will determine the type, quantity and location of first aid facilities and numbers of personnel that will best meet the risks associated with the nature of the work. First aid can save lives and prevent minor injuries becoming major ones. DCC has a duty to ensure that there are adequate arrangements and appropriate equipment and facilities for providing first aid in the workplace. The purpose of this document is to provide a policy statement and guidance on good practice to help County Council Directorates and establishments assess their first aid arrangements. There is also specific advice for schools and managers of care facilities. Although the legislation only applies to the provision of first aid for employees, a general duty of care is owed to non-employees (e.g. pupils and service users), and they also need to be considered in any assessment of first aid provision. This guidance is relevant to all Dorset County Council premises, facilities, employees and contractors.
2.2 References Health and Safety (First Aid) Regulations 1981 Management of Health and Safety at Work Regulations 1999 Health and Safety (First Aid) Regulations 1981 - Approved Code of Practice and Guidance (1997) L74 Health and Safety Executive (HSE) First aid at work, your questions answered http://www.hse.gov.uk/pubns/indg214.pdf Dorset County Council: Insite/Staffnet or www.dorsetforyou.com
4
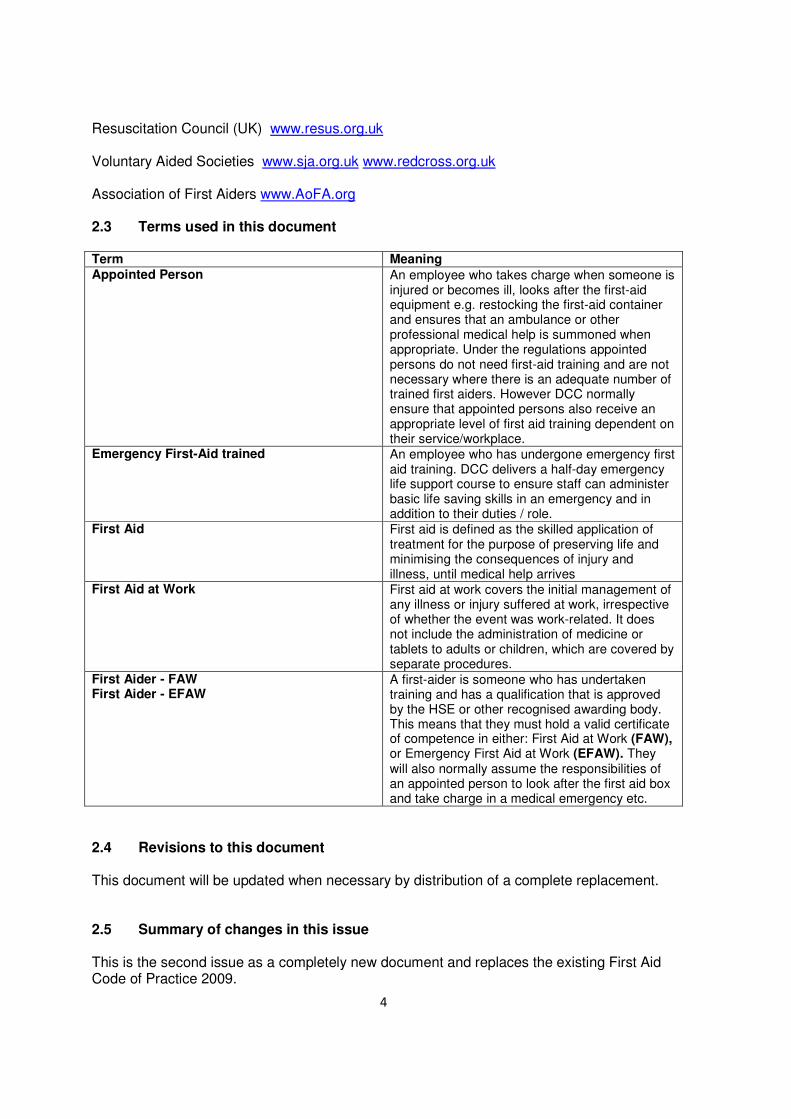
Resuscitation Council (UK) www.resus.org.uk Voluntary Aided Societies www.sja.org.uk www.redcross.org.uk Association of First Aiders www.AoFA.org 2.3 Terms used in this document Term Meaning
Appointed Person An employee who takes charge when someone is injured or becomes ill, looks after the first-aid equipment e.g. restocking the first-aid container and ensures that an ambulance or other professional medical help is summoned when appropriate. Under the regulations appointed persons do not need first-aid training and are not necessary where there is an adequate number of trained first aiders. However DCC normally ensure that appointed persons also receive an appropriate level of first aid training dependent on their service/workplace.
Emergency First-Aid trained An employee who has undergone emergency first aid training. DCC delivers a half-day emergency life support course to ensure staff can administer basic life saving skills in an emergency and in addition to their duties / role.
First Aid First aid is defined as the skilled application of treatment for the purpose of preserving life and minimising the consequences of injury and illness, until medical help arrives
First Aid at Work First aid at work covers the initial management of any illness or injury suffered at work, irrespective of whether the event was work-related. It does not include the administration of medicine or tablets to adults or children, which are covered by separate procedures.
First Aider - FAW First Aider - EFAW
A first-aider is someone who has undertaken training and has a qualification that is approved by the HSE or other recognised awarding body. This means that they must hold a valid certificate of competence in either: First Aid at Work (FAW), or Emergency First Aid at Work (EFAW). They will also normally assume the responsibilities of an appointed person to look after the first aid box and take charge in a medical emergency etc.
2.4 Revisions to this document This document will be updated when necessary by distribution of a complete replacement. 2.5 Summary of changes in this issue This is the second issue as a completely new document and replaces the existing First Aid Code of Practice 2009.

5
Section 3 Responsibilities/Training/Provision/Procedures
2.6 Contact details Dorset County Council: Dorset Direct 01305 221000 Health and Safety Team 01305 224296 [email protected] Occupational Health 01305 224094 Service Manager-Outdoor Education 01305 224517 www.dorsetforyou.com/outdoored Children’s Services - Special Educational Needs Team (SEN) 01305 224888
3.1 Responsibilities 3.1.1 Heads of Service / Directors Will ensure that arrangements are in place for:
• implementing this procedure;
• ensuring that suitable first aid arrangements are in place at all times whilst employees and other persons are engaged in County Council activities;
• carrying out risk assessments to determine that the level of first aid provision is commensurate with the risks associated with their operations;
• the periodic monitoring of first aid provision;
• coordinating and co-operating with other employers or organisations in the provision of first aid in establishments of shared occupation.
3.1.2 Line Managers
Will ensure that:
• this procedure is implemented and monitored within their area of responsibility and an assessment of appropriate first aid cover is carried out;
• sufficient suitable persons are nominated to provide first aid cover, in accordance with the requirements outlined in this document;
• risk assessments incorporate appropriate reference to first aid provision where necessary;
• first aiders and appointed persons receive appropriate training to carry out their duties;
• first aiders hold a current first aid at work certificate;
• where required that first aiders re-qualify before the expiry date of their certificate;
• bring to the attention of all staff, particularly at induction, the first aid arrangements e.g. names of first aiders and/or appointed persons and locations of first aid boxes;
• adequate communications are in place for contacting first aiders and/or appointed persons and emergency services; sufficient first aid boxes are provided and first aid notices displayed;
• accidents, injuries and dangerous occurrences are reported when work-related.

6
3.1.3 Premises Managers / Headteachers Will (in addition to the key responsibilities of line managers listed in 3.1.2.) ensure that:
• there are adequate first aid notices indicating the names, location and telephone numbers of first aiders and first aid boxes, around the premises, including meeting and training rooms;
• agree and document joint first aid arrangements where a workplace is shared with other employers, agencies or departments. This should extend to the whole of the premises.
• contractors, visitors, service users and pupils and others working temporarily on the premises are made familiar with the first aid arrangements;
• any arrangements for letting the facility incorporate consideration of first aid arrangements
3.1.4 First Aiders (FAW/EFAW) First aiders will be required to:
• take control of a medical emergency situation and give appropriate first aid in line with their training and where necessary delegate members of staff to ring emergency services, wait for ambulance, and direct paramedics to scene of incident in line with local procedures;
• in a serious emergency clear the area of anyone not involved in the incident;
• be responsible for checking the contents of first aid boxes, ensuring there is an adequate supply of materials and items have not passed any expiry date.
• ensure that all used first aid material/soiled dressings etc are disposed of appropriately. Note that infectious items are to be treated as hazardous waste and placed in appropriate containers (e.g. yellow bags) and disposed of in accordance with local arrangements;
• ensure necessary records are kept of all first aid administered, in line with the DCC Accident Reporting Policy and Procedure and that managers are made aware;
• be aware that the County Council’s Employers Liability and Public Liability insurance arrangements extend to the provisions of first aid at work;
• annually refresh first aid knowledge and skills. 3.1.5 Emergency First Aid (DCC Emergency Life Support ELS) trained personnel
Will:
• take control of a situation when a first aider is either not appointed or not available and give appropriate first-aid assistance in line with their training and where necessary delegate members of staff to undertake the following tasks:
• phone emergency services, • wait for ambulance, • direct paramedics to scene of incident
• provide first aid provision for low risk activities/visits when a first aider is not deemed necessary by a specific risk assessment;
• be responsible for first aid equipment where a first aider is not appointed to do so i.e. be responsible for checking the contents of first aid boxes, ensuring there is an adequate supply of materials and items have not passed any expiry date.

7
3.1.6 Health & Safety Team
Will:
• provide additional advice and guidance, on request, to assist with the implementation of this policy, and ensure it is kept up to date in accordance with any changes in legislation and to reflect current best practice;
• ensure monitoring of first aid provision and arrangements through health and safety audits of DCC premises;
• provide advice on the suitability of training/training courses for first aiders;
• ensure that first aid training courses are accredited or approved by the HSE or appropriate awarding body;
• provide advice and information to employees; 3.2 Risk assessment of first aid requirements The level of first aid provision and number of first aiders should be determined by managers on the basis of an assessment of the likelihood of injury arising in a workplace or as a result of a work activity. It is the policy of the County Council to ensure there are sufficient suitable persons trained either as first aiders or emergency first aid trained persons, as appropriate, to meet the needs of employees in all directorates and establishments. Some directorates or sections will only need to make the minimum first aid provision. However, there are factors which will make greater provision necessary. There is also a need to take into account the provision for non-employees e.g. pupils, service users, non paid events such as school/PTA events etc. and to ensure first aid cover is available at all times allowing for holidays and sickness absence. Any risk assessment of first aid needs will therefore have to consider the following factors when determining the adequacy of first aid cover:
• proximity and accessibility to emergency services;
• premises spread over a large area;
• inexperienced workers;
• members of the public on site;
• staffing levels and type of establishment, school, care establishment, office etc;
• risk levels and workplace hazards e.g. tools, machinery, hazardous substances, kitchens and workshops;
• previous incidents and cases of ill health that required first aid treatment;
• the needs of peripatetic staff e.g. lone workers, and employees, service users or pupils with special needs and disabilities;
• annual leave, shift patterns and other foreseeable absences of first aiders and appointed persons;
• the risks associated with other employers or organisations sharing the workplace. How many first aiders are required depends on the nature and risks inherent in each workplace. There is no prescribed fixed level for numbers of first aiders but as a guide the following ratios are deemed suitable for most workplaces:
8
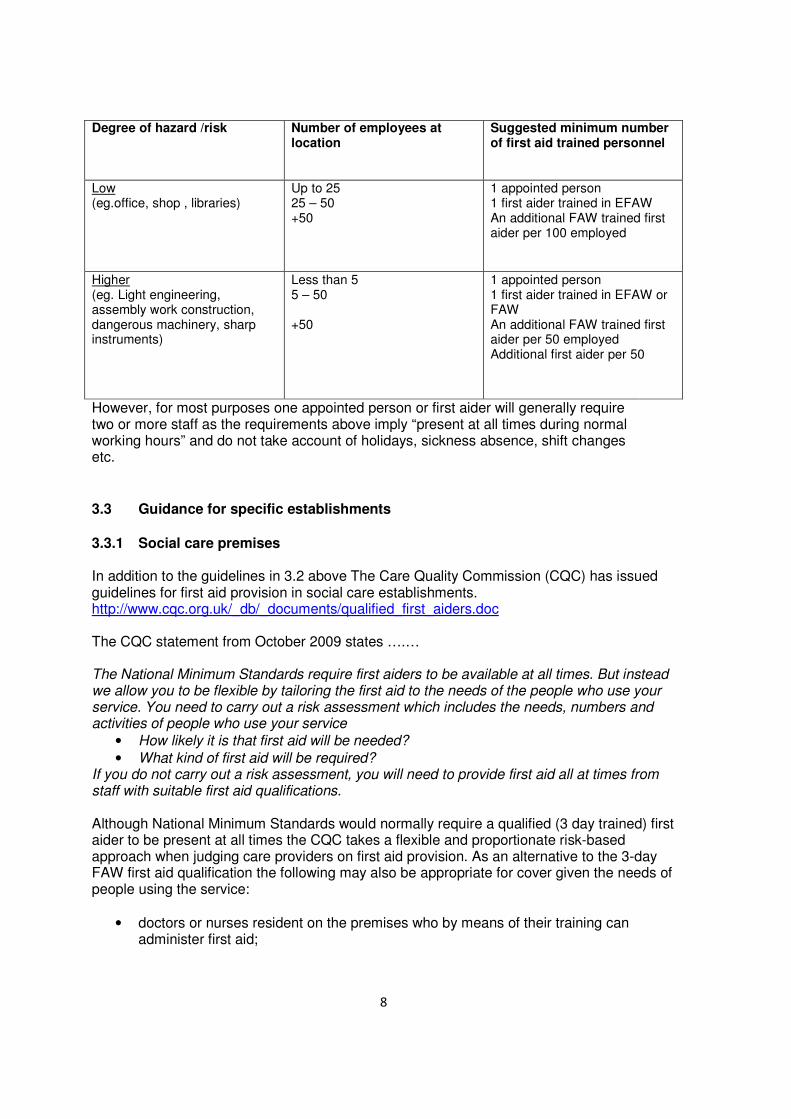
Degree of hazard /risk Number of employees at location
Suggested minimum number of first aid trained personnel
Low (eg.office, shop , libraries)
Up to 25 25 – 50 +50
1 appointed person 1 first aider trained in EFAW An additional FAW trained first aider per 100 employed
Higher (eg. Light engineering, assembly work construction, dangerous machinery, sharp instruments)
Less than 5 5 – 50 +50
1 appointed person 1 first aider trained in EFAW or FAW An additional FAW trained first aider per 50 employed Additional first aider per 50
However, for most purposes one appointed person or first aider will generally require two or more staff as the requirements above imply “present at all times during normal working hours” and do not take account of holidays, sickness absence, shift changes etc.
3.3 Guidance for specific establishments
3.3.1 Social care premises In addition to the guidelines in 3.2 above The Care Quality Commission (CQC) has issued guidelines for first aid provision in social care establishments. http://www.cqc.org.uk/_db/_documents/qualified_first_aiders.doc The CQC statement from October 2009 states ….… The National Minimum Standards require first aiders to be available at all times. But instead we allow you to be flexible by tailoring the first aid to the needs of the people who use your service. You need to carry out a risk assessment which includes the needs, numbers and activities of people who use your service
• How likely it is that first aid will be needed?
• What kind of first aid will be required? If you do not carry out a risk assessment, you will need to provide first aid all at times from staff with suitable first aid qualifications. Although National Minimum Standards would normally require a qualified (3 day trained) first aider to be present at all times the CQC takes a flexible and proportionate risk-based approach when judging care providers on first aid provision. As an alternative to the 3-day FAW first aid qualification the following may also be appropriate for cover given the needs of people using the service:
• doctors or nurses resident on the premises who by means of their training can administer first aid;
9
• Emergency first aid trained personnel who have been trained to provide basic emergency first aid. (all employees receiving care induction training undertake a half-day emergency first aid course)
• Emergency First Aid at Work- EFAW (one-day) trained first aider. Social care residential and day care providers must ensure senior staff all hold this qualification as a minimum. (see 3.3.1.(a))
In addition to the factors listed in 3.2 the following must be considered in any risk assessment of first aid provision:
• do service users have any health conditions or illnesses requiring sudden, urgent or specialist attention (e.g. heart conditions or epilepsy) ? Is challenging behaviour or self-harm a feature?
• are accidents and injuries prevalent amongst people using the service? What injuries are most likely to be expected, e.g. slips/falls, cuts and bruises, burns?
• what kinds of activity are people using the service involved in? Are these higher risk activities that could lead to injury or accidents?
• the layout of the premises. A large establishment with people accommodated on more than one floor, or in more than one building, may require more first aid cover then a smaller, single storey building;
• differing demand for first aid during day/night periods e.g. there may only need to be minimal cover at night, and increased cover during the day when most potential accidents and injuries take place;
• the raised expectations of society in general, people using services, their relatives, and friends and family, that basic first aid will be provided, including resuscitation if appropriate.
3.3.1(a) Dorset County Council social care minimum first aid provision;
Each social care premises should have at least one 3-day FAW trained first aider. Social care senior staff in residential homes and day care should be trained to EFAW 1-day first aider level (if not designated as the FAW First Aider). 3.3.1(b) Resuscitation in social care premises
There may be occasions when there may be doubt as to whether resuscitation should be instigated or continued if already started;
1. If collapse is witnessed then CPR should be commenced and maintained until paramedics arrive.
2. If it is absolutely clear and there is no doubt that the casualty has been deceased for a prolonged period of time then the manager/duty officer could instruct the first aider/rescuer not to commence CPR or to cease resuscitation. If in doubt, CPR should be continued until professional medical help arrives.
3. If a formal decision has been agreed by an individual, relevant family members and health professionals in accordance with the County Council’s “Resuscitation, Allow a
Natural Death (DNAR) Policy “, then CPR should not be attempted. If any rescuer has not been made aware of this information then they should instigate CPR until help arrives.

10
4. On discovering a collapsed non-responsive casualty, all staff should call or send for help (first aider and duty officer). The first aider or any employee who has undertaken current first aid training will carry out Basic Life Support (primary survey) and commence Cardio Pulmonary Resuscitation on an unconscious casualty who is not breathing normally, having first established that an ambulance has been called. CPR should continue until professional medical help arrives
3.3.2 Schools 3.3.2(a) First aiders in schools (minimum recommendation)
No of Pupils FAW trained (3 day) first aider
EFAW trained (1 day) first aider
less than 100 1 1 100 – 250 1 2 250 – 500 2 2 500 - 1000 2 3 greater than 1000 3 3 First aid provision must be available at all times while staff and pupils are on school premises, and also off the premises whilst on school visits (see para 3.3.2(h) below for more details). When assessing first aid requirements schools will need to determine how many first aiders (FAW, EFAW or emergency first aid trained personnel) to provide taking into account the numbers of staff and pupils and the factors listed in section 3.2. More specifically when selecting first aiders, schools should consider those staff involved in high risk activities, such as physical education teachers and those leading out-of-school activities, as particularly appropriate and, conversely, consider those who cannot leave their classes unattended in an emergency as probably unsuitable. It is recommended therefore that non-teaching staff are also considered. 3.3.2(b) Further guidance for schools: Guidance on first aid in schools - Department for Education http://publications.teachernet.gov.uk/eOrderingDownload/GFAS98.pdf Department for Education - Managing Medicines in Schools and Early Years Settings http://publications.teachernet.gov.uk/eOrderingDownload/1448-2005DCL-ENv3final.pdf Guidance on Infection Control in Schools and other Child Care Settings. April 2010 - Health Protection Agency http://www.hpa.org.uk/web/HPAwebFile/HPAweb_C/1194947358374 3.3.2(c) Treatment of minor injuries in schools
There is often conflicting information regarding what can and cannot be done for minor injuries. Hopefully this recommended guidance will help to the positions:
11
Scissors; It is generally good practice to keep a pair of scissors (preferably tuff cut type with a moulded end to prevent damage to skin) in a first aid kit. These can be used to cut dressings or remove clothing in an emergency to expose a severe or life threatening wound. Tweezers; It would be good practice to keep disposable plastic tweezers in your first aid kits. These could be used for removing grit and dirt from minor wounds. They can also be used for removing minor splinters from hands/skin. Small splinters; Aim to remove the splinter and minimise risk of infection. If the splinter is small and not embedded and can easily be removed, pull out along the track of entry then gently squeeze the area which will help to flush out dirt. Clean the area and pat dry then apply a plaster. If it is not possible remove the small splinter then clean the area, pat dry and apply a plaster. The parent/carer should be informed who can then deal with this when the child returns home. Large embedded splinters must not be removed and referred to a medical professional. Alcohol free moist cleansing wipes; These can be used to clean minor wounds in the absence of soap and water or on completion of washing prior to applying a plaster or non-adherent dressing (always read and follow manufacturer’s advice given on the label). Plasters; Cover a minor wound (after cleaning) with a plaster providing the plaster is large enough to cover the area. If the child has an known allergy to plasters (which you should already know) then a low-allergenic plaster or non adherent dressing may be applied to prevent spread of infection.
3.3.2(d) Identifying illnesses / injuries to children
Young children may not give a full description of symptoms so additional care is necessary so that injuries or illnesses are not overlooked. If you have doubts or concerns, then other first aiders, key teaching staff and senior management should be consulted. If remaining at school the child should be kept under observation for the rest of the school day and all relevant supervising staff and a parent/guardian informed. Further advice can be sought from the parent, the child’s care plan if available or by telephoning NHS Direct on 0845 4647. 3.3.2(e) Head injuries
Any head injury is potentially a very serious condition. A head injury to a pupil however minor must be assessed by a first aider (FAW/EFAW) and treated in accordance with current first aid guidance. If a pupil has fully recovered but there has been evidence of impaired consciousness the child must be seen by a doctor. If the injury is assessed as minor and does not require the child to be referred to a doctor, then the pupil must be kept under observation for the rest of the school day for signs of deterioration and the parent/guardian informed of the nature of the injury. Some schools find it useful to issue an advice sheet to parents. 3.3.2(f) Calling an ambulance / transporting to hospital / moving injured children Where there is any uncertainty about a child’s condition or extent of injury then medical assistance should be sought, and where it is required urgently, this should be by ambulance. If the situation warrants calling an ambulance then this should take

12
priority over informing the parent/guardian. The parents can be contacted after calling the ambulance. If parents cannot arrive at the school before the anticipated arrival of the ambulance then they should arrange to meet their child at the hospital. Consideration should also be given to the extent of discomfort and pain which can be inflicted when self-transporting a child without appropriate immobilisation and pain relief and medical expertise afforded by paramedics/ambulance. School staff must also exercise caution before moving a pupil into or to another part of the school for further examination and treatment. If a more serious injury is evident or likely then a first aider should make a more thorough assessment of the child before deciding if it is appropriate to move a pupil. Consideration must be given to manual handling risks before first aiders attempt to move children who are injured or ill. It may be advisable to wait for paramedic staff who are trained to move casualties and carry equipment to assist when doing so.
• Paramedic staff are able to give emergency treatment immediately using equipment carried on the ambulance
• Emergency vehicles travel faster through traffic congestion to hospital, and can alert A&E to any special requirements prior to their arrival.
• Paramedic crews are trained, and are equipped to move casualties without worsening any injury.
When a child is taken to hospital, the school having responsibility for that child must ensure that they are accompanied by an adult from the school, and that they remain accompanied until a parent/guardian arrives. 3.3.2(g) Swimming pools on school premises Advice and guidance for supervision, emergency procedures and first aid provision at swimming pools on school premises can be found in the Dorset County Council Swimming Pool Health and Safety Manual; Volume 4, School Use Swimming Pools – Arrangements for Safety During Swimming. Appendix B of this document details qualifications, training and supervision requirements for pool use dependent on size, depth and type of use. 3.3.2(h) Off site visits First aid provision must be considered and provided on all off school/site visits. The level of provision is decided by teachers or leaders on the basis of a risk assessment; the likelihood of injury or illness arising at a particular location or as a result of any planned activity. Visit leaders must ensure availability of first aid cover for all visits where there is no immediate external first aid cover provided. In these situations, an appropriate first aid kit should be carried and one of the leaders should hold a first aid qualification appropriate to the environment and activity. The risk assessment may indicate that a higher level qualification is appropriate in circumstances where the risk of injury is higher or when the arrival at the scene by the emergency services may be delayed. An example could be an adventurous activity in a remote area. In this case, qualifications such as a current first aid at work certificate may be required. When planning a visit, school management, offsite visits coordinator or leaders must make a judgment as to the level of first aid required for a particular visit. The decision could be influenced by a number of factors such as:
13
Dorset for You, Offsite Events and Adventurous Activities. http://www.dorsetforyou.com/index.jsp?articleid=341365 3.4 Shared or multi-occupied sites
On a shared or multi-occupied site, DCC will co-operate and coordinate with other employers or organisations to ensure there is adequate first aid cover available for all employees, non-employees and visitors throughout the whole of the premises. In these cases, a full exchange of information about the hazards and risks associated with all of the different organisation’s operations should help ensure that the shared provision is adequate. All employers should agree the arrangements and ensure employees are kept informed. A written agreement between employers which outlines responsibilities for first aid provision and training is strongly recommended to avoid any misunderstandings. 3.5 Provision of information to employees detailing first aid arrangements
All local methods of conveying information to staff should be used to ensure staff are made fully aware, understand and accept the first aid systems. The procedures should also identify who will provide this information to new staff. Strategically placed notices, stating the name, contact place and telephone extension of the nearest first aider or appointed
• location - population, terrain, response and accessibility for emergency services
• duration of visit
• weather, exposure to elements
• type of activity/supervision
• line of communication between group / emergency services
• numbers of pupils
• numbers of support staff
• age, challenging behaviour from pupils
• special needs, illnesses, medical conditions of pupils / staff
• medical / first aid provision already provided at location
• first aid kit / equipment and it's accessibility
• associated risks at location
• history of previous visits to location
• first aid provision remaining at school to cover school curriculum activities The Dorset Off Site Visit 24 hour emergency phone number is 07623 544346. This is for use in serious emergencies only where additional support is required from the County Council. Further advice on first aid provision / planning for off-site visit emergencies – see links below: Children’s Services Policy of Safety and Guidance for Offsite Events and Adventurous Activities. Adherence to the content of this policy is a requirement for all who are working with children and young people where the local authority is the employer. http://www.dorsetforyou.com/media.jsp?mediaid=142609&filetype=pdf

14
person should be available. This information should also be incorporated into School/workplace safety systems. 3.6 First aid training First aid training must be provided by accredited organisations and must conform to the criteria laid down in the approved code of practice and guidance (HSE) Dorset County Council Health and Safety Team is approved by the HSE to provide first aid at work training. A comprehensive corporate first aid training programme is available on the Learning Portal or directly from the Health and Safety Team. “In-house” first aid courses can also be provided. 3.6.1 Training for First Aiders First Aid at Work (FAW First aiders) must have fully attended and passed: An initial First Aid at Work Certificate course (3 days), valid for three years followed by; A First Aid at Work Refresher course (2 days), also valid for three years. Note: recertification must be completed during the period of three months before or twenty eight days after the expiry date of the certificate to maintain the qualification otherwise the first aider must repeat the full three day course. Emergency First Aid at Work (EFAW First aiders) must attend a one-day Emergency First Aid at Work Course which is valid for three years. 3.6.2 Basic Skills Refresher Training
Although not mandatory, the HSE strongly recommends first aiders (FAW and EFAW) undertake annual refresher training. First aiders attending an annual refresher course should demonstrate their competence to;
• assess the situation in an emergency;
• administer first aid to a casualty who is unconscious (including seizure);
• administer cardiopulmonary resuscitation;
• administer first aid to a casualty who is wounded and bleeding;
• administer first aid to a casualty who is suffering from shock. Managers should allow for a minimum of three hours per year to enable a FAW/EFAW first aider to update their skills and knowledge with annual “Basic Skills Training”. Establishments / schools can achieve this refresher training by either using a competent first aid trainer to deliver an in-house annual refresher course (approximately three hours duration) or alternatively, Appendix A of this document provides a resource which will enable establishments to conduct their own “self-teach” interim refresher training for their qualified first aiders (FAW and EFAW). This will enable those who do not require a first aid trainer led course to refresh their first aid skills, competency and confidence. This resource can obviously be used more frequently than annually if required to improve competence and confidence. Some establishments / directorates may have access to half day emergency first aid courses which could be used as an interim basic skills refresher for FAW/EFAW first aiders.
15
For example, some social care staff have to attend three-yearly care refresher training which incorporates a half day emergency first aid course or a school/establishment may hold a half day emergency responder course. These short courses would count as basic skills refresher training. 3.6.3 Selection of first aiders: The selection of first-aiders depends on a number of factors, including:
• Ability to act safely, promptly and effectively when an emergency situation occurs at work.
• Availability, reliability and communication skills
• Aptitude and ability to absorb new knowledge and learn new skills
• Ability to cope with stressful and physically demanding emergency procedures
• Normal duties. These should be such that they may be left to go immediately and rapidly to an emergency.
The purpose of training is to equip candidates to deal effectively with injuries or illness which may occur at work. The key objective is that, on completion of training, successful candidates will be able to apply the following competencies in practice: 3.6.4 HSE One-Day Emergency First Aid at Work (EFAW) Course:
• understand the role of the first aider including reference to the importance of preventing cross infection, the need for recording incidents and actions, use of available equipment
• assess the situation and circumstances in order to act safely, promptly and effectively in an emergency;
• administer first aid to a casualty who is unconscious (including seizure);
• administer cardiopulmonary resuscitation;
• administer first aid to a casualty who is choking;
• administer first aid to a casualty who is wounded and bleeding;
• administer first aid to a casualty who is suffering from shock;
• provide appropriate first aid for minor injuries (including small cuts, grazes and bruises, minor burns and scalds, small splinters).
3.6.5 HSE Three- Day First Aid at Work (FAW) Course:
• provide emergency first aid as above
• administer first aid to a casualty with: - injuries to bones, muscles and joints, including suspected spinal injuries; - chest injuries; - burns and scalds; - eye injuries; - sudden poisoning; - anaphylactic shock; - recognise the presence of major illness and provide appropriate first aid - (including heart attack, stroke, epilepsy, asthma, diabetes).
Where required, DCC (Health & Safety Team) EFAW courses will include child and baby CPR and allow time to discuss any other relevant workplace emergencies. School staff should refer to relevant DCSF documentation and procedures for managing medical conditions.
16
3.6.6 Early Years Foundation Stage – Requirement for Paediatric First Aid Training The DCSF Statutory Framework for the Early Years Foundation Stage have introduced first aid requirements for schools and other settings with young children (i.e. children from birth to the end of the academic year in which a child has their fifth birthday). From September 2008 schools and other registered providers must have at least one person present on site (and for off site visits) who is competent to provide paediatric first aid at all times when young children (as defined above) are present. Paediatric first aid training must meet the criteria set out in Practice Guidance for the Early Years Foundation Stage Appendix 1. http://nationalstrategies.standards.dcsf.gov.uk/node/84490 The main requirements for paediatric training and refresher training are a minimum of 12 hours tuition time and for it to be renewed every three years. The DCSF requirement for paediatric first aid training does not replace existing HSE first aid requirements for staff and children but is in addition to it. Ofsted inspections from September 2008 onwards have been checking on the provision that schools have made (or have planned) to meet these new DCSF requirements. With regard to the DCSF guidance, schools with reception year only (not pre-reception or nursery provision) will need to determine whether their existing first aid facilities and staff training takes into account issues relating to younger children (4-5 years) There are a number of ways this type of school could ensure it meets with the requirements:
a. the accredited first aid training provider for individual first aid staff has been able to focus on younger child issues as part of the qualification (one day EFAW, three day FAW or two day FAW refresher courses)
b. the school has opted to run an in-house emergency first aid course for some or all staff and have asked the accredited training provider to include younger child issues within the programme
c. the school can decide to fully comply with the DCSF guidance and nominate an appropriate number of staff for a paediatric first aid certificate to provide cover for school and off site activities.
For options (a) and (b), the training provider should ensure that they provide a written outline of the programme to ensure schools can evidence that younger child issues have been covered. All schools and settings should consider which option best suits its current training needs and take appropriate action towards fully complying with the DCSF guidance. Schools that have provision for children below reception year will need to ensure they are fully complying with the requirements of the DCSF. Dorset Surestart currently commissions an approved Early Years paediatric first aid training provider. Dorset County Council Health and Safety Team are planning to include paediatric first aid courses into their training programme from April 2011. 3.6.7 Defibrillator training
There has been a Department of Health campaign in recent years to provide defibrillators in public places such as railway stations and airports. The idea is that early intervention can make a positive difference to recovery. The training, maintenance costs and the unlikelihood

17
of a speedy response by an ambulance service would result in few DCC workplaces justifying the provision of defibrillators. However, where a decision is made to provide a defibrillator in a workplace, it is important that those who may use it are appropriately trained. The Health and Safety Executive (HSE) does not specify the content of this training and organisations providing it do not need HSE approval. However if this is required, training courses on Cardiopulmonary Resuscitation (CPR) and Automated External Defibrillation (AED) are available from the DCC Health and Safety Team, South Western Ambulance Service Trust and Voluntary Aided Societies. 3.7 Infection control / waste disposal 3.7.1 Universal Precautions
The following hygiene precautions are recommended as safe practice for all staff. They are common sense precautions that will protect against blood borne viruses and infections that may be transmitted via blood or body fluids.
• Always keep cuts or broken skin covered with waterproof dressings.
• Wear disposable gloves when contact with blood or body fluids is likely.
• Avoid direct skin contact with blood or body fluids.
• If blood is splashed onto the skin, it should be washed off immediately with soap and water.
• Splashes of blood into the eyes or mouth should be washed immediately with plenty of water.
• If a sharps injury is sustained or blood is splashed into the eyes or mouth, or on to broken skin (e.g., eczema) medical advice should be sought promptly.
• Always wash and dry hands after removing gloves.
• Always wash and dry your hands before and after giving first aid.
• Educate employees, service users and pupils in the need to avoid contact with other people’s blood and body fluids and to wash and dry their hands before meals and after using the toilet.
3.7.2 Blood and body fluid spills
Spillages of blood, vomit, urine and excreta should be cleaned up immediately. The following general actions must be taken by the person dealing with the spill.
• Clear the immediate area of people. Hazard signs and cordoning off may be necessary.
• Disposable personal protective equipment (PPE); disposable gloves and if necessary a disposable plastic apron should be worn.
Small spills or splashes on hard surfaces:-
• Clean with disinfectant detergent and hot water. Large spill:-
• Remove spillage as much as possible using absorbent paper towels.
• If possible (do not block the toilet) flush these down the toilet or dispose of carefully in waste bag.
• Cover remaining with paper towels soaked in diluted bleach solution (1:10 dilution with cold water) or local bleach alternative, soak, wipe clean and dispose

18
Alternatively use a Hazard Disposable Pack (see 3.7.4) – follow instructions and clean area with natural detergent and hot water. 3.7.3 Disposal of Waste
Generally used paper towels, together with gloves and aprons, should be put into a plastic waste sack/bag, top tied and placed in the outside waste collection bin. Vomit, urine and faeces should be flushed down the toilet. All first aid kits should contain hazard (yellow) disposable bags. These can be used when treating a blood injury within a first aid context and disposed of in accordance with local procedures, into a sanitary bin or other suitable clinical waste container. Establishments/workplaces that generate larger amounts of clinical waste will need to have a disposal contractual arrangement in place. 3.7.4 Hazard Disposal Packs A hazard disposal pack is a safe system for the disinfection and removal of blood, vomit or urine. Each pack contains granules, disinfectant spray, scoop and scraper, pair of vinyl gloves, biohazard disposable bag and bag closure. Instructions are:-
1. Wear disposable gloves. 2. Sprinkle the contents of the sachets over the spill. This will solidify a liquid spill in 2
minutes. 3. Using the scoop and scraper provided remove the now solidified spillage and place
in the biohazard bag. 4. Use the disinfectant spray to disinfect the area of the spill. 5. Place the scoop and scraper into the bag and tie securely. 6. Dispose of the bag in the outside waste collection bin
3.8 Legal indemnity for first aiders Administering first aid in the workplace is considered to be an act of taking reasonable care. Dorset County Council (or governing bodies where applicable) will fully indemnify all first aiders, emergency first aid trained and appointed persons staff against claims for alleged negligence in relation to first aid treatment providing they are acting within the remit of their employment and training. 3.9 Guidance for first aiders on reporting of accidents DCC establishments and schools should all have a copy of the Accident Reporting Policy and Procedure 2007. First aiders must ensure that accidents and incidents that they have provided support to are accurately recorded and any actions highlighted. For full details of the requirements of the policy, follow this link: http://staffnet/index.jsp?articleid=207411

19
3.10 First aid boxes, equipment, supplies and facilities 3.10.1 First aid boxes and contents The minimum requirement is one suitably stocked first aid box which must be available in all establishments. However additional boxes and equipment may be required. There is no mandatory list of items to put in a first aid box, it depends what you assess your needs to be. The HSE recommended minimum contents where work involves low hazards/risk would include;
• A leaflet/booklet giving general guidance; http://www.hse.gov.uk/pubns/indg347.pdf
• 20 individually wrapped assorted plasters
• 2 eye pads
• 4 triangular bandages (preferably sterile)
• 6 safety pins
• 2 large wound dressings (non medicated)
• 6 medium wound dressings (non medicated)
• Disposable gloves Other factors to consider when deciding on the provision of first aid kits, their location and content would include the number of employees, service users, pupils, visitors, hazards, activities, geographical location, vulnerable people, specific hazards, other requirements/requirements such as CLEAPSS (Science and Technology in Schools Advisory Service), COSHH (Control of Substances Hazardous to Health Regulations) and previous history of accidents. As a result of an assessment of need, the following additional first aid items may be added, particularly in schools, for treating minor injuries: Scissors, bio-hazard clean up kit, clinical waste bags, disposable aprons, moist wipes, microporus tape, eye wash phials, finger dressings, blankets, foil blankets, conforming bandages, gauze swabs, non adherent dressing, tweezers. However, first aid kits should not contain any tablets, medicines or lotions. Boxes or kits are the responsibility of the first aider or appointed person who should ensure they are fully stocked, that expiry dates are not exceeded, and the contents are in good condition. Contents should be replenished as quickly as possible after use. In addition first aid materials must be disposed of after their expiry date. First aid boxes should be clearly marked and easily identified with a green /white cross/background. They should be clearly visible to employees in the vicinity, portable and not be locked away, however they can be secured with a tamper seal if necessary to prevent unauthorised use. Traveling first aid kits should be made available for employees required to work away from the normal workplace, where access to facilities may be restricted such as:
• Working with dangerous equipment / activities
• Traveling in vehicles on a regular basis
• In contact with vulnerable people
• Remote / isolated locations
20
3.10.2 First Aid Rooms There is no explicit requirement to have a dedicated first aid room, although there are advantages in having a room set aside for first aid treatment or recovery for persons who are ill. A suitable room should be nominated for the provision of first aid where the assessment of first aid identifies this as necessary. It does not have to be specifically used for first aid. The room should contain essential first aid facilities and equipment. Typical examples of these are:
• a sink with running water
• drinking water and disposable cups
• soap and paper towels
• a store for first aid materials
• foot-operated refuse containers, lined with disposable yellow clinical waste bags or a container for the safe disposal of clinical waste
• a couch with waterproof protection, clean pillows and blankets
• a chair
• a telephone or other communication equipment
• accident report forms for recording incidents where first aid has been given It should be clean, easily accessible to emergency services and be sited within reasonable distance from a toilet and be clearly signposted and identified. 3.10.3 First Aid Supplies First aid supplies should be purchased from the current procurement contracted supplier via DES. 3.10.4 Use of Burnshield dressings The use of specialised dressings, sprays and gels to cool burns is not normally recommended. However the following guidance applies if they are used; Sometimes insufficient water is available to effectively cool the burn such as remote workers/activities and in this situation it is good practice to use a water cooling gel dressing. Water cooling gels come in sealed packs. Each pack contains a water based soluble gel that is designed to draw heat out of the burn. The gel is primarily composed of de-ionised water thickened to help it stay in place and a small amount of tea tree oil. The non-adherent sterile polyester carrier traps the gel and holds it in place over the burn site Burnshield Dressings can be purchased if required following an individual assessment of needs. A Burnshield hydro shield dressing can be used in different situations:
• To cool a burn when water is unavailable • To keep a burn cool after water has been used first to cool the burn (place on top of
dressing).
21
3.11 Administration of medicines Whilst the Health and Safety Executive has no objection to medicines such as paracetamol or aspirin being made available to employees, first aid at work does not generally cover the administration of tablets or medication to treat illness. Paracetamol is an effective pain killer if used correctly to treat mild to moderate pain and/or raised body temperature. However the giving of paracetamol is not a life saving first aid issue and first aiders should not be required to administer paracetamol in the workplace. An exception to this is where a casualty with a suspected heart attack can self administer their own prescribed aspirin in accordance with currently accepted first aid protocols if safe to do so. Tablets, medicines and lotions must not be kept in the first aid container and not be kept where they can be accessed by vulnerable persons. Some first aiders, as a result of their job role and training (e.g. in schools) may administer life saving medicines for which they have been trained in emergency situations such as an Epipen / Auto injector to treat anaphylactic shock for which the casualty has been prescribed. A first aider may also assist a casualty to self administer their own life saving medication providing the casualty takes the decision to use it and requires assistance. 3.12 Managing Medicines in Schools and Early Years Settings Safeguarding of children is paramount. It is strongly recommended that Schools and Early Years settings have a statement of policy on the managing of medicines and medication. Schools/settings are responsible for adhering to Health Care Plans, maintaining and monitoring records and demonstrating that children are provided with appropriate medical support for which training has been given by qualified personnel. It should be noted that failure to adhere to health care plans could affect insurance cover and increase liability. In order to safely manage a child’s special medical/medication needs, procedures and protocols laid down in the policy statement must be adhered to. The following sources will assist in developing policies and implementing procedures (including individual health care plans) to ensure that children with complex health needs can access education and childcare; ‘Managing Medicines in Schools and Early Years Settings’ Department for Education and Skills http://www.education.gov.uk/publications/standard/publicationdetail/page1/DFES-1448-2005 ‘The Administration of Medicines’ National Association of Headteachers NAHT - PM006 www.naht.org.uk/medicines ‘Including Me’ Managing Complex Health Needs in Schools and Early Years Settings – Department for Education and Skills / Council for Disabled Children. http://www.education.gov.uk/publications/standard/publicationdetail/page1/DFES-1448-2005 ‘Dorset Policy for Children with Complex Health Needs in School, Social Settings and on Transport’ www.dorsetforyou.com ‘Management of Long Term Health Conditions’ - Dorset Paediatric Safeguarding Board. www.dorsetforyou.com
22
‘Administration of Medicines’ UNISON - Guide for Health and Safety Representatives http://www.unison.org.uk/acrobat/13797.pdf A policy will contain information on:
• Safeguarding children;
• the roles and responsibilities of staff with regard to supporting children with complex health needs;
• what the school or early years setting expects from the parents in terms of being kept informed and updated about their child’s health needs;
• the training which staff can expect to receive when managing children with long term health conditions;
• indemnity and additional insurance arrangements for staff working with specific children with complex medical needs;
• risk management, detailed record keeping and procedures to be followed;
• responses to emergency situations
• any additional arrangements which need to be in place for activities which take place away from the usual school / setting.
Schools/settings should keep prescribed medicines only where it would be detrimental to a child’s health if the medication was not administered during the school/working day. Health services will provide advice and training for staff when the health care plan identifies this. Schools/ settings should arrange for competent staff to administer medication. Alternatively voluntary staff or parents could be asked to do this. An individual’s suitability must be assessed in every case, taking into account the complexity of the tasks to be undertaken and training required (see assessment tool for training staff in the Dorset Policy for Children with Complex Health Needs in School, Social Settings and on Transport or the Management of Long Term Health Conditions - Dorset Paediatric Safeguarding Board). Department for Education and Skills Managing Medicines in Schools and Early Years Settings (see 3.11) gives detailed advice and guidance on managing medical conditions and medication including relevant documentation;
Form 2 Health care plan Form 3 A Parental agreement for a school/setting (self administered) Form 3B Parental agreement for a school/setting to administer medicine Form 4 Head Teacher/ Head of setting agreement to administer medication Form 5 Record of medicine administered to an individual child Form 6 Record of medicine administered to all children Form 7 Request for a child to carry their own medicine Form 8 Staff training record – administration of medicines Form 9 Authorisation for the administration of rectal diazepam End.