Embed Size (px)
Citation preview
THERAPY 19
Administer ACE inhibitors early following acute MI
In the absence of contraindications, ACE inhibitor therapy should be commenced early in the treatment of acute myocardial infarction (MI), report researchers from the ACE Inhibitor Myocardial Infarction Collaborative Group. 1
They conducted a systematic overview of 4 randomised trials involving> 98 000 patients with acute MI who had either commenced ACE inhibitor therapy within 0-36 hours of symptom onset* or served as controls. Generally, the duration of therapy ranged from 4-6 weeks.
Reduced 30-day mortality The 30-day cumulative mortality was significantly
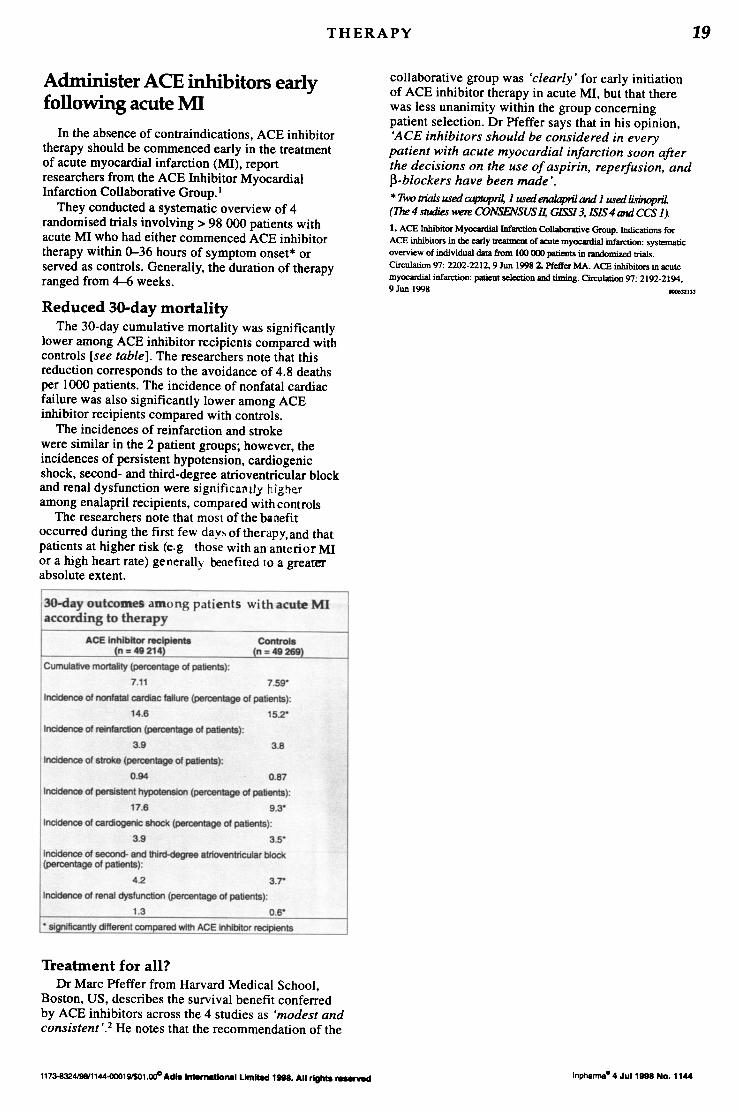
lower among ACE inhibitor recipients compared with controls [see table]. The researchers note that this reduction corresponds to the avoidance of 4.8 deaths per 1000 patients. The incidence of nonfatal cardiac failure was also significantly lower among ACE inhibitor recipients compared with controls.
The incidences of reinfarction and stroke were similar in the 2 patient groups; however, the incidences of persistent hypotension, cardiogenic shock, second- and third-degree atrioventricular block and renal dysfunction were significalllly highe.r among enalapril recipients, compared with controls
The researchers note that most of the banefit occurred during the first few days of therapy, and that patients at higher risk (e.g those with an anterior MI or a high heart rate) generally .benefited to a greater absolute extent.
3O-day outcomes among patients with acute MI according to therapy
ACE Inhibitor ntClplents Controls (n:: 49 214i (n ::49269)
Cumulative mortallty (percentage of patients);
7.11 7.59"
Incidence 01 nonfatal carciac failure (percentage 01 patients);
14.6 152'
Incidence of reinlarction (percentage of patients);
3.9 3.8
Incidence 01 stroke (percentage of patients);
0.94 0.87
Incidence of persistent hypotension (percentage of patients);
17.6 9.3"
Incidence 01 cardlogenlc shock (percentage of patients);
3.9 3S
Incidence of second- and third-degree atrioventtlcular block (percentage 01 patients) ;
42 3.r
Incidence 01 renal dysfunction (percentage of patients);
1.3 0.6"
• significantly different compared with ACE inhibitor recipients
Treatment for all? Dr Marc Pfeffer from Harvard Medical School,
Boston, US, describes the survival benefit conferred by ACE inhibitors across the 4 studies as 'modest and consistent'.2 He notes that the recommendation ofthe
1173-832419811144"()()()1WS01.000 Acl181rMrnetion111 L1mn.d 1"'. All rlghta ~
collaborative group was 'clearly' for early initiation of ACE inhibitor therapy in acute MI, but that there was less unanimity within the group concerning patient selection. Dr Pfeffer says that in his opinion, 'ACE inhibitors should be considered in every patient with acute myocardial infarction soon after the decisions on the use of aspirin, reperfusion, and P-blockers have been made' . * Two trWJs used coptopril, 1 used enoJapril and 1 used lisinopriL (The 4 studies were CONSENSUS II, GISSI3, ISIS 4 and CCS 1). 1. ACE Inhibitor Myocardial Infarction Collaborative Group. Indications for ACE inhibitors in the early treaIJDeI1t of acute myocardial infarction: systematic
overview of individual data from 100 000 patients in randomized trials.
Circulation 97: 2202·2212.9 Jun 19982. Pfeffer MA. ACE inhibitors in acute
myocardial infarction: patient selection and timing. Circulation 97: 2192-2194. 9 Jun 1998 1D06l2133
Inpharma- 4 Jul 11K18 No. 1144





![Impact of clinically tested NEP/ACE inhibitors on tumor ... · Impact of clinically tested NEP/ACE inhibitors on tumor uptake of [111In-DOTA]MG11—first estimates for clinical translation](https://img.dokumen.tips/doc/110x75/5b7a152f7f8b9ad77e8ed6da/impact-of-clinically-tested-nepace-inhibitors-on-tumor-impact-of-clinically.jpg)























