Embed Size (px)
Citation preview
128
For correspondence or reprints contact: Pr Pascal Chavanet,Service des Maladies Infectieuses, Hôpital du Bocage, 2 Boule-vard Maréchal Delattre de Tassigny, Dijon, 21034 France. Email:[email protected].
Purpose: Adherence to antiretroviral medications is critically important for thesuccess of therapy in patients treated for HIV infection. Patient self-report is asimple method to measure and explore adherence. Even though a variety of surveyshave been developed to monitor self-reported adherence, there is no standardizedinstrument that may be used in routine clinical practice. The usefulness of thePatient Medication Adherence Questionnaire (PMAQ) was evaluated in HIV-infectedpatients on protease inhibitor (PI)-containing regimens. Method: Data from 149patients were collected. Study participants completed the PMAQ and providedblood samples to measure plasma HIV-1 RNA concentrations and trough plasmalevels of PI. Patients were considered adherent if they had a virologic response and/or had an adequate trough plasma level of PI. Results: A close relationship wasfound between patient reports of adherence during the previous 4 days andobjective measures such as HIV RNA level and plasma levels of PI. Motivation withregard to antiretroviral treatment, confidence in personal skills, and an optimisticattitude to life were identified as important determinants of adherence. On the otherhand, sociodemographic background, social support, alcohol and illicit drug use,bothersome symptoms, and depression were not associated with a lowermedication adherence. Conclusion: Patient’s psychological and behavioral factorsare central in the acceptance and adherence to antiretroviral therapy. To improvethe feasibility and the reproducibility of the PMAQ, we propose a revised form of thePMAQ, focusing on the variables identified as strong predictors of adherence. Keywords: self-reported adherence, antiretroviral therapy, Patient MedicationAdherence Questionnaire
HIV Clinical Trials 2001;2(2):128–135© 2001 Thomas Land Publishers, Inc.
A ntiretroviral (ARV) therapy with potentcombinations of drugs has remarkablyimproved the prognosis of HIV infection.
ARV regimens that include HIV-1 proteaseinhibitors (PIs) have been shown to reduce plasmaHIV-1 RNA and to increase concomitantly CD4 cellcount. The extensive use of such treatments hasresulted in a substantial decrease in AIDS-relatedmorbidity and mortality. However, the efficacy ofARV therapies may be limited by poor adherenceresulting in a lack of clinical or viral response, theselection of drug-resistant variants, and secondarydrug failure.1–3 Additionally, suboptimal adherencecan lead to a misinterpretation of clinical efficacyand to inappropriate changes in treatment. Becauseadherence to ARV medications is critically
Evaluation of the Patient Medication AdherenceQuestionnaire As a Tool for Self-Reported
Adherence Assessment in HIV-Infected Patientson Antiretroviral Regimens
Michel Duong, MD,1 Lionel Piroth, MD,1 Michèle Grappin, MD,1 Fabien Forte, MD,1 GillesPeytavin, PhD,2 Marielle Buisson, MD,1 Pascal Chavanet, MD,1 and Henri Portier, MD1
1Division of Infectious Diseases, University Hospital, Dijon, France; 2Department of Clinical Pharmacokinetic,Bichat Hospital, Paris, France
important for the success of therapy in patientstreated for HIV infection, it is particularlywarranted for clinicians to have a convenient toolto monitor it. Several methods such as clinicianreports, returned pill counts, surrogate laboratorymarkers, drug levels, and computer-assistedelectronic monitoring devices have been proposedto evaluate adherence.4,5 However, all of these

PREDICTORS OF ADHERENCE TO ANTIRETROVIRAL THERAPY • DUONG ET AL. 129
methods have limitations, which is why, at themoment, no reference method can be recom-mended.
Another approach may be patient self-report,which is simple, relatively inexpensive, and easyto implement in the patient’s follow-up. Self-re-ported nonadherence has been demonstrated to beassociated with worse virologic outcomes.4,6 How-ever this method has been shown to overestimateadherence, both in the HIV setting and non-HIVsetting, and nonconsistent results were foundwhen it was compared to more objective mea-sures.1,7 Nevertheless, another potential interest ofpatient self-report is that it can provide informa-tion about the reasons why a patient did or did nottake the medication properly. In fact, a patient’sclinical, social, psychological, and behavioral vari-ables are among the most important factors thatinfluence adherence; to date, few studies have as-sessed the impact of such factors.8–10
Even though a variety of surveys have been de-veloped to monitor self-reported adherence, thereis no standardized instrument that may be used inroutine clinical practice. In the present study, weevaluated the usefulness of the Patient MedicationAdherence Questionnaire (PMAQ) as a self-reportinstrument to measure and explore adherence inpatients on ARV regimens.
METHOD
Study Design and Patients
This study was approved by our Human Sub-jects Protect Care Committee. It was a prospective,cross-sectional study of HIV-infected patients whowere followed at the Dijon Hospital AIDS day-careunit. Patients with documented HIV infection,whether symptomatic or not, were eligible for en-try into the study if they had followed an ARVregimen represented by two nucleoside analoguesand one or a combination of marketed PIs, eitherindinavir (IDV), saquinavir (SQV), nelfinavir(NFV), or ritonavir (RTV). Patients were not awareof the study before attending their consultationand therefore did not know that they were havingblood drawn to measure PI plasma levels. The eli-gible patients were asked by the nurse if theywanted to participate in the study. Study partici-pants were asked to complete the PMAQ version1.0. Full blood count, CD4 cell count, routine bio-
chemistry analysis, HIV RNA level, and troughplasma PI level were performed the same day.
Measure of Adherence to ARV Therapy
Adherence was assessed by the means of twobiological markers: plasma PI levels and plasmaHIV concentrations.11,12 Adherence was consideredadequate when: (i) HIV RNA was undetectable(with a limit of detection of 20 copies/mL) or HIVRNA level was at least 2 log10 below the pretreat-ment level for patients who had taken PI for thefirst time and at least 1 log10 below the pretreatmentlevel for patients who had been treated at least onceby another PI regimen, or (ii) trough plasma PIlevels were above reference values. Conversely, ad-herence was considered inadequate when condi-tions (i) and (ii) were not met.
Plasma HIV RNA levels were assessed using theHIV-1 Amplicor Monitor assay (Roche DiagnosticSystems, Brachburg, NJ, USA) with a limit of detec-tion of 20 copies/mL and were transformed to log10values. The determinations of masked plasma PIlevels were performed using chromatographicmethods coupled with an ultraviolet detection forIDV, RTV, NFV, and SQV. The assays were found tobe linear over the concentration range and the lowerlimits of quantification were 5 ng/mL, 0.03 mg/L,0.03 mg/L, and 9 ng/mL for IDV, RTV, NFV, andSQV, respectively. The interday percent coefficientof variation for these assays was lower than 10%. Athreshold value for trough plasma concentrationwas determined for each PI by taking into accountthe value of the in vitro IC90 of the PI for HIV-1, thepharmacokinetic properties of the drug, and thelevel of protein binding. These reference values werethe following: IDV = 0.07 mg/L, NFV = 1 mg/L,RTV = 2.1 mg/L, and SQV = 0.1 mg/L. The interpre-tation of each plasma PI level was performed in ablind analysis that took into account the time inter-val between PI ingestion and blood sampling.
Self-Report Adherence
The PMAQ was filled in by the patient. A trainedresearch assistant was present to give explanationsto patients who had difficulty understanding someitems of the PMAQ. This questionnaire contained61 items that were designed to evaluate a patient’streatment adherence behavior and its determinantsby providing a quantitative measure of adherence

130 HIV CLINICAL TRIALS • 2/2 • MAR-APR 2001
and information on why a patient is or is not adher-ent. It is divided into two sections. Section 1 con-tains six items pertaining to medication-taking be-haviors and asks patients to rank on an ordinalscale how often they missed individual doses ordays of medication. Section 2 contains 55 itemspertaining to barriers and motivators to takingmedications. Each item is rated on a Likert scalefrom 0 to 3 or 0 to 5. The concepts assessed aresummarized in Table 1.
Statistical Analysis
Patient sociodemographics and measures ob-tained from the 61 items of the PMAQ were enteredinto the STATVIEW Statistics program (AbacusConcepts, Berkley, CA, USA). The chi-square testwas used to compare categorical variables. Con-tinuous variables (social support, trust in ARVtherapy, psychological functioning, etc.) were as-sessed by the Mann-Whitney test. A p value < .05was considered significant.
RESULTS
Population
One hundred and forty-nine (149) HIV-infectedpatients were enrolled in the study between July
and November 1998. The mean age was 40 years(range, 21–79 years). One hundred and four pa-tients (104; 70%) were men. The HIV infection riskfactors were the following: heterosexual (40%), ho-mosexual/bisexual (33%), intravenous drug use(24%), and blood products (3%). According to theCenters of Disease Control and Prevention (CDC)1993 criteria, 60 patients were on stage A, 49 onstage B, and 40 on stage C. At the time of study,mean CD4 cell count was 485 x 106 cells/L (range,2–1,126 x 106 cells/L) and HIV RNA was mean 4.6log10
copies/mL (range, 0–6.51 log10 copies/mL). Attime of inclusion into the study, 14 patients (9%)were on their first ARV regimen. Concerning PIuse, 93 patients (63%) were at least on their secondPI-containing regimen.
Adherence Assessment
Eleven percent (11%) of the 149 patients (16)were nonadherent according to the criteria out-lined in the Method section (virologic responseand/or adequate PI blood concentration). All pa-tients completed the PMAQ. Among the six itemsdesigned to assess adherence, three items were sig-nificantly associated with drug adherence: “ I havenot missed any doses of my ARV medications overthe last four days” (89%, p = .03); “ I have notmissed taking all my pills at least one day over thelast four days” (82%, p = .01); and “ I have followedthe special instructions associated with my ARVmedications over the last four days” (80%, p =.0005). Conversely, the following three items didnot predict adherence: “I did not miss taking myARV medications last weekend-last Saturday orSunday”; “I have closely followed the specificschedule associated with my ARV medicationsover the last four days”; and “I have never missedany doses of my medications over the last threemonths.”
Determinants of Adherence
Age, sex, education, risk behavior, stage of HIVinfection, employment, and having children athome did not correlate with adherence (see Table2). Neither the use of alcohol or illicit drugs norbothersome symptoms was significantly associ-ated with less adherence. Associations betweenpsychosocial variables and adherence to ARV
Table 1. Assessment measures
No.Concept assessed of items
Medication adherence 06Bothersome symptoms 12Social support 02Psychological status
Depression 05Stress 08Confidence in personal skills 02Optimism 02
Knowledge/attitudes/beliefsHIV medication self-efficacy 01Attitudes and beliefs about HIV 02
treatmentReasons for missing doses 12Alcohol and illicit drug use 05Sociodemographic background 04
xx

PREDICTORS OF ADHERENCE TO ANTIRETROVIRAL THERAPY • DUONG ET AL. 131
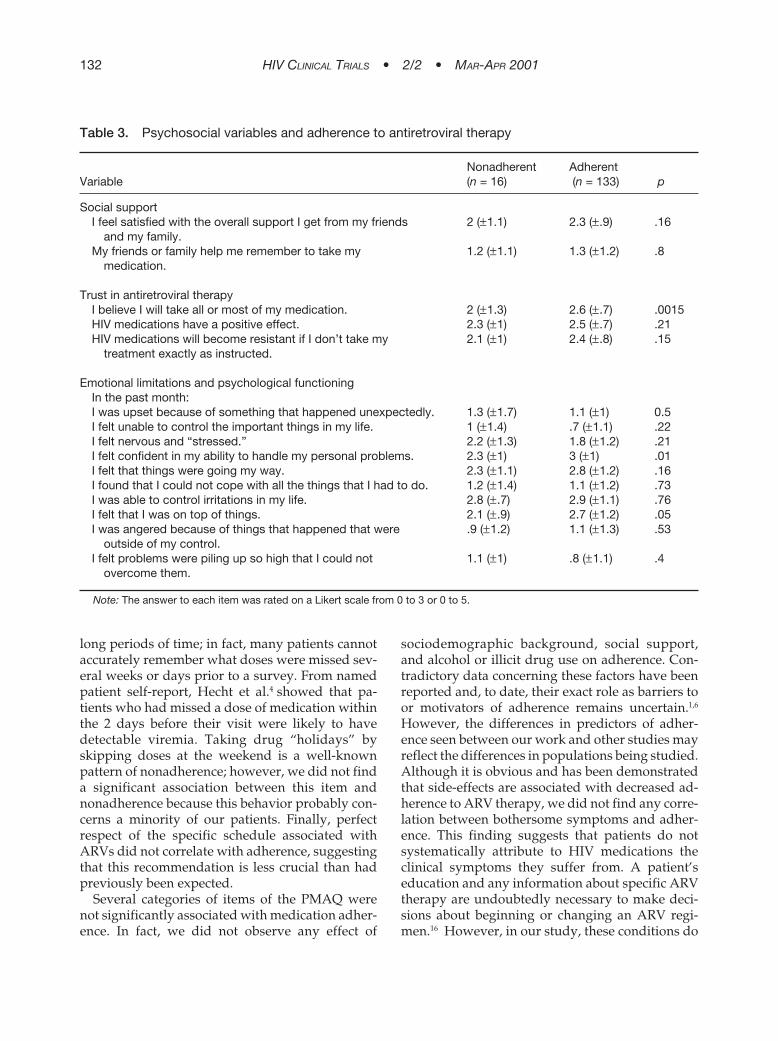
therapy are summarized in Table 3. Satisfactionwith social support was not a significant predictor ofadherence, because neither being satisfied withfriend and family’s support nor having somebody toremind the patient to take the medications was asso-ciated with drug taking. The firm belief of being ableto take all or most of the HIV medications wasstrongly associated with adherence. In contrast, in-sufficient knowledge about the efficacy of HIVmedication and the risks of a suboptimal drug ad-herence was not predictive of nonadherence.Among psychological variables, positive feelingsabout personal life and trust in personal skills weresignificantly associated with better adherence. Nei-ther stress nor depression was significantly associ-ated with poorer ARV adherence.
Among the different reasons for missing ARVdoses, being away from home was the only vari-able significantly associated with nonadherence
(see Table 4). “Having problems taking pills atspecified times” was more frequently reported bynonadherent patients.
DISCUSSION
Patient self-report is now commonly collectedfor assessing adherence in HIV-infected patients.Among the different instruments that measureself-reported adherence, the PMAQ is one of themost frequently used questionnaires, especially inclinical trials.13,14 However, few studies had shownits utility and, to date, there is no clear validation ofthis self-administered questionnaire.15 A close rela-tionship was found between patient reports of ad-herence during the previous 4 days and objectivemeasures such as HIV RNA level and plasma lev-els of ARVs. This finding confirms the relevance ofan adherence evaluation over short rather than
Table 2. Sociodemographic variables and adherence of HIV-infected patients to antiretroviral therapy
Nonadherent Adherent Variable (n = 16) (n = 133) p
Age 39.9 40.7 .76Sex .15
Female 07 35Male 09 98
Education .55Grade school 02 11High school 05 23Technical school 04 64College 05 35
Risk behavior .45Men who have sex with men 06 43Heterosexual 07 52IV drug use 03 33Blood products 00 5
Employed .89Yes 07 73No 09 59
Working outside the home .60Yes 07 73No 06 36
Having any children .45Yes 09 53No 07 78
Note: IV = intravenous.
132 HIV CLINICAL TRIALS • 2/2 • MAR-APR 2001
long periods of time; in fact, many patients cannotaccurately remember what doses were missed sev-eral weeks or days prior to a survey. From namedpatient self-report, Hecht et al.4 showed that pa-tients who had missed a dose of medication withinthe 2 days before their visit were likely to havedetectable viremia. Taking drug “holidays” byskipping doses at the weekend is a well-knownpattern of nonadherence; however, we did not finda significant association between this item andnonadherence because this behavior probably con-cerns a minority of our patients. Finally, perfectrespect of the specific schedule associated withARVs did not correlate with adherence, suggestingthat this recommendation is less crucial than hadpreviously been expected.
Several categories of items of the PMAQ werenot significantly associated with medication adher-ence. In fact, we did not observe any effect of
sociodemographic background, social support,and alcohol or illicit drug use on adherence. Con-tradictory data concerning these factors have beenreported and, to date, their exact role as barriers toor motivators of adherence remains uncertain.1,6
However, the differences in predictors of adher-ence seen between our work and other studies mayreflect the differences in populations being studied.Although it is obvious and has been demonstratedthat side-effects are associated with decreased ad-herence to ARV therapy, we did not find any corre-lation between bothersome symptoms and adher-ence. This finding suggests that patients do notsystematically attribute to HIV medications theclinical symptoms they suffer from. A patient’seducation and any information about specific ARVtherapy are undoubtedly necessary to make deci-sions about beginning or changing an ARV regi-men.16 However, in our study, these conditions do
Table 3. Psychosocial variables and adherence to antiretroviral therapy
Nonadherent AdherentVariable (n = 16) (n = 133) p
Social supportI feel satisfied with the overall support I get from my friends 2 (±1.1) 2.3 (±.9) .16
and my family.My friends or family help me remember to take my 1.2 (±1.1) 1.3 (±1.2) .8
medication.
Trust in antiretroviral therapyI believe I will take all or most of my medication. 2 (±1.3) 2.6 (±.7) .0015HIV medications have a positive effect. 2.3 (±1) 2.5 (±.7) .21HIV medications will become resistant if I don’t take my 2.1 (±1) 2.4 (±.8) .15
treatment exactly as instructed.
Emotional limitations and psychological functioningIn the past month:I was upset because of something that happened unexpectedly. 1.3 (±1.7) 1.1 (±1) 0.5I felt unable to control the important things in my life. 1 (±1.4) .7 (±1.1) .22I felt nervous and “stressed.” 2.2 (±1.3) 1.8 (±1.2) .21I felt confident in my ability to handle my personal problems. 2.3 (±1) 3 (±1) .01I felt that things were going my way. 2.3 (±1.1) 2.8 (±1.2) .16I found that I could not cope with all the things that I had to do. 1.2 (±1.4) 1.1 (±1.2) .73I was able to control irritations in my life. 2.8 (±.7) 2.9 (±1.1) .76I felt that I was on top of things. 2.1 (±.9) 2.7 (±1.2) .05I was angered because of things that happened that were .9 (±1.2) 1.1 (±1.3) .53
outside of my control.I felt problems were piling up so high that I could not 1.1 (±1) .8 (±1.1) .4
overcome them.
Note: The answer to each item was rated on a Likert scale from 0 to 3 or 0 to 5.

PREDICTORS OF ADHERENCE TO ANTIRETROVIRAL THERAPY • DUONG ET AL. 133
not seem to be sufficient to ensure adherence. Inassessing ARV use among HIV-infected femaleprisoners, Monstashari et al.17 also found that trustin safety and efficacy of ARV therapy was not asso-ciated with a statistically significant increase indrug taking. Previous studies had demonstratedthat stress and depression were more frequent innonadherent patients.18,19 We are unable to confirmthese results. The discrepancy between our studyand the others may be related to the fact that thePMAQ is not an appropriate tool to evaluate de-pression precisely. Using the Beck HopelessnessScale, which consists of 20 true–false statementsdesigned to assess hopelessness, Singh et al.10
found that depression was a significant factor.Through the PMAQ, we have identified some
psychosocial behavior factors that are critical de-terminants of ARV consumption; in particular, mo-tivation with regard to ARV treatment, confidencein personal skill, and an optimistic attitude to life.The conviction of being able to take the treatmenthas been identified in several studies as a centralfactor.8 This belief refers to a patient’s own decisionabout being treated. Involvement of the patient intreatment (in particular, acceptance of ARVtherapy) is also associated with the patient’s ac-knowledgment of the seriousness of the diseaseand the understanding of its potential complica-tions. Thus, patients’ feelings about illness andtheir mental capacities to handle a regimen are
Table 4. Relation between possible reasons for missing an HIV medication dose andadherence
Nonadherent AdherentVariable (n = 16) (n = 133) p
I was away from home. 1.6 (±1.3) .9 (±1.3) .05I was busy with other things. .9 (±1.3) .6 (±1.2) .24I simply forgot. .8 (±1.2) .5 (±.9) .27I had too many pills to take. .3 (±.8) .2 (±.7) .73I wanted to avoid side effects. .4 (±1) .3 (±.8) .68I did not want others to notice me taking medication. .6 (±1.1) .4 (±.8) .2I had a change in daily routine. .8 (±1.2) .4 (±.9) .2I thought the drug was toxic/harmful. 0 .1 (±.3) .46I felt sleepy/slept through dose time. .3 (±.8) .3 (±.7) .66I felt sick or ill. .3 (±.8) .25 (±.7) .76I felt depressed/overwhelmed. .6 (±1.1) .2 (±.7) .09I found difficult to take pills at specified times. 1 (±1.3) .5 (±.9) .08
Note: The answer to each item was rated on a Likert scale from 0 to 3 or 0 to 5.
important factors that must be taken into consider-ation when making decisions about beginning HIVtherapy. Initiation of ARV therapy at an inappro-priate time leads in most cases to poor adherencewhatever the accuracy of the treatment plan.Therefore, clinicians should always evaluate pa-tient readiness to begin therapy.20
“Fighting spirit” was identified as being a strongdeterminant; in this study, individuals who feltmore confident in their personal skills were morelikely to remain adherent to therapy. Active behav-ioral coping positively influences the desire andthe ability to organize the complicated drug regi-mens that HIV therapy may require; moreover,lack of fighting spirit and loss of motivation havebeen identified as characteristics of the patients atrisk for missing doses.9
We also found that faith in the future was astrong predictor of medication adherence. Ourfinding confirms those of other studies that re-ported that individuals who had an optimistic atti-tude toward their life were more likely to take theirmedications regularly.
Finally, our nonadherent participants signifi-cantly reported that they missed ARV doses be-cause they were away from home. Other authorshave reported that the most common reasons formissing medications included “simply forgot,” be-ing busy and being away from home, and justify-ing the need of a perfect fit between ARV medica-

134 HIV CLINICAL TRIALS • 2/2 • MAR-APR 2001
tion schedule and the patient’s daily routine.8,13 In-terestingly, Gifford et al.8 have shown that integrat-ing medication regimens with daily activities was acentral factor to achieve plasma HIV suppression.
The main limitation of our study lies in our goldstandard of adherence, which leads to a generousdefinition of adherence (a great majority [89%] ofthe patients was adherent) and a somewhat harshdefinition of nonadherence, resulting in a relativelylow number of poorly adherent patients. These cri-teria detected patients with very low levels of ad-herence but probably missed people with moder-ate level of nonadherence (i.e., 25%–50%). Thus,our study did not evaluate the factors associatedwith the more subtle cases of nonadherence.
Nevertheless, the present study confirms thecentral role of a patient’s psychological and behav-ioral factors in the acceptance and adherence toARV therapy and provides some evidence of theusefulness of the PMAQ. Even though each cat-egory of items is potentially interesting, our find-ings suggest that the PMAQ should focus on sev-eral key variables. From a practical point of view,limiting the number of items in this questionnairecould improve its feasibility and its reproducibilityin routine practice. We propose a revised form ofthe PMAQ that focuses on the variables that havebeen significantly correlated with adherence in thepresent study and have also been found to bestrong predictors of adherence in other studies.These variables are the following: self-reported ad-herence over the 4 days before the visit; confidencein medication-taking ability; psychological status,including an evaluation of depression and copingstyle; and convenience of the medication regimenas assessed by the reasons for missing doses. Ourrevised form of the PMAQ needs to be validated bystudies of different populations with a broaderspectrum of barriers to drug adherence. Thesestudies may ideally be conducted with other vali-dated measures of adherence such as electronicmonitoring or pill counts.
REFERENCES
1. Paterson D, Swindells S, Mohr J, et al. Adherence to pro-tease inhibitor therapy and outcomes in patients with HIVinfection. Ann Intern Med. 2000;133:21–30.
2. Rodriguez-Rosado R, Jimenez-Nacher I, Soriano V, AntonP, Gonzalez-Lahoz J. Virological failure and adherence to
antiretroviral therapy in HIV-infected patients. AIDS.1998;12:1112–1113.
3. Bangsberg D, Hecht F, Charlebois E, et al. Adherence toprotease inhibitors, HIV-1 viral load, and development ofdrug resistance in an indigent population. AIDS.2000;14:357–366.
4. Hecht F, Colfax G, Swanson M, Chesney M. Adherenceand effectiveness of protease inhibitors in clinical practice.Presented at: Fifth Conference on Retrovirus and Opportu-nistic Infections; February 1998; Chicago. Abstract 151.
5. Miller L, Hays R. Measuring adherence to antiretroviralmedications in cl inical tr ials. HIV Clin Trials .2000;1(1):36–46.
6. Haubrich R, Little S, Currier J, et al. The value of patient-reported adherence to antiretroviral therapy in predictingvirologic and immunologic response. California Collabora-tive Treatment Group. AIDS. 1999;13:1099–1107.
7. Frick P, Gal P, Lane T, Sewell M. Antiretroviral medicationcompliance in patients with AIDS. Aids Patient CareSTDS.1998;12:463–470.
8. Gifford A, Bormann J, Shively M, Wright B, Richman D,Bozzette S. Predictors of self-reported adherence andplasma HIV concentrations in patients on multidrugantiretroviral regimens. J Acquir Immune Defic Syndr.2000;23:386–395.
9. Holzemer W, Corless I, Nokes K, et al. Predictors of self-reported adherence in persons living with HIV disease.Aids Patient Care STDS. 1999;13:185–197.
10. Singh N, Berman S, Swindells S, et al. Adherence of humanimmunodeficiency virus-infected patients to antiretroviraltherapy. Clin Infect Dis.1999;29:824–830.
11. Duong M, Piroth L, Forte F, Chavanet P, Portier H. Serumprotease inhibitor level as a marker of adherence toHAART; correlation with self-reported adherence and HIVRNA. Presented at: 36th Interscience Conference on Anti-microbial Agents and Chemotherapy; September 1999;San Francisco. Abstract 2069.
12. Murri R, Ammassari A, Gallicano K, et al. Patient-reportednonadherence to HAART is related to protease inhibitorlevels. J Acquir Immune Defic Syndr. 2000;24:123–128.
13. Chesney M, Ickovics J, Chambers D, et al. Self-reportedadherence to antiretroviral medications among partici-pants in HIV clinical trials: The AACTG adherence instru-ments. AIDS Care. 2000;12(3):255–266.
14. Eron J, Yetzer E, Ruane P, et al. Efficacy, safety, andadherence with a twice-daily combination lamivudine/zidovudine tablet formulation, plus a protease inhibitor, inHIV infection. AIDS. 2000;14:671–681.
15. Childress J, Jhingran P, Scott-Lennox J, Tolson J. Devel-opment and initial evaluation of the Patient MedicationAdherence Questionnaire. Presented at: Sixth EuropeanConference on Clinical Aspects and Treatment of HIV In-fection; October 1997; Hamburg, Germany.
16. Weiss L, French P, Finkelstein R, Waters M, Kluger M,Agins B. Knowledge, attitudes and adherence to HAART:Results of a multisite adherence evaluation project. Pre-sented at: 13th International AIDS Conference; July 2000;Durban, South Africa. Abstract ThPeB 5018.
17. Mostashari F, Riley E, Selwyn P, Altice F. Acceptance andadherence with antiretroviral therapy among HIV-infected

PREDICTORS OF ADHERENCE TO ANTIRETROVIRAL THERAPY • DUONG ET AL. 135
women in a correctional facility. J Acquir Immune DeficSyndr Hum Retrovirol. 1998;18:341–348.
18. Valente S, Saunders J, Ulman G. Self-care, psychologycaldistress and HIV disease. J Assoc Nurs AIDS Care. 1993;4:15–25.
19. Singh N, Squier C, Sivek C, Wagener M, Nguyen M, Yu V.Determinants of compliance with antiretroviral therapy in
patients with human immunodeficiency virus: Prospectiveassessment with implications for enhancing compliance.AIDS Care.1996;8:261–269.
20. Andrews L, Friedland G, Mannheimer S, et al. A method forassessing patient readiness to begin and adhere toHAART. Presented at: 13th International AIDS Conference;July 2000; Durban, South Africa. Abstract ThPeB 4987.





























