Embed Size (px)
Citation preview

Addressing Disparities Through Organizational Quality Improvement Efforts
David R. Nerenz, Ph.D.Center for Health Services
ResearchHenry Ford Health System
October 21, 2005

Overview
• Health Care Disparities• Reasons for Disparities• Hospitals, Health Plans, and Quality
Improvement• Three Challenges:
– Identifying Significant Disparities– Measuring Effects of QI Initiatives– Setting Priorities


“Disparities in the health care delivered to racial and ethnic minorities are real and are associated with worse outcomes in many cases, which is unacceptable.”
- Alan Nelson, retired physician, former president of the American Medical Association and chair of the committee that wrote the Institute of Medicine report, Unequal Treatment: Confronting Racial and Disparities in Health Care
IOM Report, 2002: Assessing the Quality of Minority Health Care

0.0
1.0
2.0
3.0
0-14 15-24 25-44 45-64 65+
Ratio of Minority-White Death Rates, 1994-1996
Ratios are based on deaths per 100,000 resident populationSOURCE: DHHS Health, Unites States, 1998
Age Groups
Death rates of minority Americans comparedto those of white Americans at various ages
African American
American Indian/Alaska Native
Latino
Asian/Pacific Islander
White,non-Latino

Screening: Percent with Early Stage Cancer* Among Women with Breast
Cancer, 1978-1987 (Detroit)
20%
24%
29%
15%16%
19%
0%
10%
20%
30%
1978-1981 1982-1984 1985-1987
WhiteBlack
*Tumors <2cm and no auxiliary lymph involvement at diagnosisSOURCE: Swanson, M et al., 1990

Indicators of Children’s Access to Care, 1987
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Adjusted Odds RatiosMinority Children vs. White Children
Ratios > 1.0 indicate minority
more likely than white
children
0.56
2.44
1.77
1.45
2.12
1.54
Has a usual Source of
Care
Does not see a
specific physician
No After-hours
Emergency Care
Travel time of 30 min.
+
Wait time of 60 min. +
Physician Not Seen for
Selected Symptoms
DATA: 1987 NMESSOURCE: Newacheck et at, 1996

Heart Procedure Rates for Blacks and Whites, 1980 vs.1993
0.0
1.0
1980 1993
Ratios <1.0
indicates Blacks
less likely than
Whites to undergo procedur
e1980 1993 1980 1993
Equal procedure rate
(Ratio of Black/White procedure rates) *
•Rates were age-adjusted•SOURCE: Gillum R.F., et al., 1997
Cardiac Catheterizati
on
Angioplasty Bypass Surgery

Coronary Artery Surgery Rates by Race and Disease Severity, 1984-1992
35%
45%
25%31%
0%
20%
40%
60%
80%
Source: Peterson, et al., 1997.
Perc
en
t R
eceiv
ing
Byp
ass
Su
rgery
Mild Disease Severe Disease
Whites
African Americans

Disparities in Cardiac Revascularization
5,000 Medicare beneficiaries in 5 states – 1991 and 1992
RAND appropriateness criteria
Some gender disparities noted as well
Epstein et al, Medical Care, 2003
0
20
40
60
80
100
CABG orPTCA
ClinicallyAppropriate
ClinicallyInappropriate
BlackWhite

Evidence of racial/ethnic differences in cardiac care
1984-2001
68 studies find a racial/ethnicdifference in care(84%)
11 studies find no racial/ethnic difference in care(14%)
2 studies find racial/ethnic minority group more likely than whites to receive appropriatecare (2%)
Total= 81 studiesSource: Kaiser Family Foundation

Minorities are Less Satisfied with The
Quality of Care They Receive
3136
29
3834
41*
24*
36*
0
20
40
60
Better Care With Different Health Plan Rate Care from Doctor as Excellent
Total White Black Hispanic
*Significantly different from whites at p<.05 or lessSource: The Commonwealth Fund Biennial Health Insurance Survey (2003)
Percent adults 19-64 privately insured
THE COMMONWEALTH
FUND

Isn’t It All About Poverty and Lack of Insurance?

Rates of Hospitalization for Coronary Artery Bypass Surgery Among Medicare
Beneficiaries, 1993
0
2
4
6
White
Black
Coronary Artery Bypass Surgery Procedures per 1000 beneficiaries per year*
<$13,001 $13,001- $16,300
$16,301- $20,500
*Rates were adjusted for age and sex to the total Medicare population.SOURCE: Gomick, ME et al., 1996
>$20,500
Annual Income
4.8
1.8
4.8
2.2
4.9
2.1
4.6
2.2

Infant Mortality Rates: Mothers 20+ Years by Education and
Race/Ethnicity, 1995
7.6
4.7
17.3
14.8
12
6.0
5.9
5.0
6.4
LatinoAfrican American
White
Infant deaths per 1,000 live births
DATA: CDC National Center for Health StatisticsSOURCE: DHHS. Health, United States, 1998
College +
High SchoolLess than High School

16
THE COMMONWEALTH
FUND
Across Income Groups, African Americans Are Most Likely to Go without Needed Care Because
of Cost
37
24
36
23
31 29
36*
52*
0
20
40
60
Inc ome below 200% FP L Inc ome 200% or above FP L
Total White Afric an Americ an H ispanic
^Did not fill prescription, did not get specialist care, or skipped recommended test because of cost.*Significantly different from whites at p<.05 or betterSource: The Commonwealth Fund Biennial Health Insurance Survey (2003)
Percent adults 19-64 privately insured going without needed care

Across Income Groups – Hispanics Are Most At Risk for Forgoing Preventive
Care
849087 9086
95
74*84*
0
50
100
Income below 200% FPL Income 200% or above FPL
Total White African American Hispanic
*Significantly different from whites at p<.05 or betterSource: The Commonwealth Fund Biennial Health Insurance Survey (2003)
Percent adults 19-64 privately insured with blood pressure check in past year
THE COMMONWEALTH
FUND

Evidence on Disparities
“Racial and ethnic minorities tend to receive a lower quality of health care than non-minorities, even when access-related factors, such as patient’s insurance status and income, are controlled. ” (my emphasis)
IOM Report, Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care, 2002

Some of these studies are pretty old – haven’t things
changed since people started studying this?

Reperfusion Therapy in Medicare Beneficiaries with
Acute MI
Group % Eligible
receiving reperfusion
White men 59%
White women 56%
Black men 50%
Black women 44%
Canto JG, Allison JJ, Kiefe CI, Fincher CI, Farmer R, Sekar P,Person S, Weissman NW.Relation of race and sex to the use of reperfusion therapy in Medicare beneficiaries with acute myocardial infarction. N Engl J Med 2000 Apr 13;342(15):1094-100

Disparities in Management of AMI – Changes Over Time (1994-2002)
• Data Source – NRMI
• 600,000 Patients• Significant
disparities in several measures; no change over time
• Some disparities became not significant in adjusted analyses
• Vaccarino et al, NEJM, August 18, 2005

Receipt of Major Surgical Procedures – Medicare Data
1992-2001• Focus on 9 surgical
procedures• Analysis by hospital
referral regions for three procedures
• No evidence of change in disparity over 10-year period
• Disparity reduction in 22/158 regions, but no elimination of disparity in any region
• Jha et al, NEJM, August 18, 2005

Disparities in Medicare Managed Care (HEDIS)
Measures Over Time• Standard, widely-
used quality measures
• Trends from 1997 or 1999 to present
• Improvements in quality overall, reduction in disparities in some HEDIS measures, but not all
• Trivedi et al, NEJM, August 18, 2005

Disparities in Medicare Managed Care (HEDIS)
Measures Over Time (Cont.)• Additional
HEDIS measures
• Change in disparity from first to most recent year
• Trivedi et al, NEJM, August 18, 2005

All of these studies involve large national samples – what about disparities within single
health care organizations?

Comprehensive Diabetes Care:
Foot Exam Performed
0
20
40
60
80
100
White African American Hispanic Asian Overall
White vs. African American (p<0.001), White vs. Hispanic (p<0.001) and White vs. Asian (p<0.001).
Rate

Asthma: Outpatient Follow-up
After Acute Episodes• Core concept:
Outpatient follow-up after either ER visit or admission
• Children 5-17 years old
• Standard based on national expert panel guidelines
0
10
20
30
40
50
60
70
Follow-up Rate
Caucasian
African-American

Comparison of non-Hispanic/Hispanic Breast Cancer Screening by Commercial, Medicare
Risk, and Medicaid Products in a Single Health Plan, 2000
0
20
40
60
80
100
Commercial Medicare Risk Medicaid
non-Hispanic Hispanic
Rate
P=.001 non-Hispanic population

Possible Explanations for Disparities
• Environmental Factors– Income/Poverty– Insurance coverage– Geographic access– Poor-quality facilities
and providers in minority neighborhoods
– Cultural competence of providers and systems
– Language barriers– “Institutional racism”
• Individual Factors– Cultural beliefs and
preferences– Trust in providers and
organizations (lack of)– Literacy– Biased clinical decision-
making– Some possible
biological differences

Conceptual Model of Health Care Disparities
Patient Factors
Health CareSystem Factors
Treatments Outcomes
Environmental Factors
Provider Factors

Conceptual Model of The Operation of a Car
Engine Factors
Chassis and Body Factors
Movement ofCar
Arrival atDestination
Environmental Factors
Driver Factors

Treatment Treatment or or
Service PtService PtReceivedReceived
ProviderDecision-making
(Diagnosis,Treatment)
ProviderInterpretation of
SymptomsProvider Provider cognition and affect cognition and affect
regarding patientregarding patient
Provider Provider CharacteristicsCharacteristics
Setting
Pt
Rac
e/et
hn
icit
yP
t R
ace/
eth
nic
ity
Cla
ss
Culture
Pt Cognitive & Affective Factors(e.g., acceptance of advice, attitude, self-efficacy, intention, feelings of
competence, attitude toward med care, trust)
Pt Behavior in Encounter
(e.g., question-asking self-disclosure, assertiveness)
Pt Satisfaction
Pt BehaviorPt Behavior (e.g. self management,
information-seeking, utilization)
Encounter characteristics
Provider Behavior in Encounter
(e.g., participatory style, warmth, content, information giving,
question-asking)
Understanding the Provider Contribution to Disparities
(Michelle VanRyn)

CHRONOLOGY BIRTH DIAGNOSIS TREATMENT
INN
AT
EE
XP
OS
UR
ES
/ A
CQ
UIR
ED
FA
CT
OR
SD
IAG
NO
ST
IC
IN
TE
NS
ITY
CA
NC
ER
-R
EL
AT
ED
Age
Sex / Gender
Race / ethnicity (B vs. W)
Socioeconomic status
Comorbidities (adverse)
Unstaged cancer
Stage (higher / advanced)
Symptoms (adverse)
No surgery, localized NSCLC
SU
RV
IVA
L
Marital status (spouseless)
Smoking status (current)
Illicit drug (use vs. not)
No chemotherapy, SCLC / advanced NSCLC
No Rx, any
Histology NOS


Conceptual Model for Contribution of Race/Ethnicity and SES to
Treatment and Outcome Disparities
SES
Race/Ethnicity
Education
Income
Job Class
Language
Culture
Biological Differences Bias/Discrimination in
Medical Settings
Dis
parit
ies
in T
reat
men
t
Historical Bias/Discrimination
Dis
parit
ies
in O
utco
mes
FinancialAccess
Benefits,ScheduleFlexibility
Tumor Histology,Comorbidities
Health Beliefs,Trust in Providers
Comprehension,Trust
Literacy

Disparities in Cardiac Surgery –
Steps in a Process• Notice and interpret symptoms• Get primary care doctor appointment• Get tests• Deal with insurance and payment
issues• Get referral to Cardiology• Get Cardiology appointment• Get additional tests• Discuss treatment options and ask
questions• Get referral to Cardiac Surgeon• Get appointment with surgeon• Get additional tests• Discuss treatment options and ask
questions• Get surgery scheduled• Arrange time off work and family
support• Deal with comorbid conditions• Get surgery

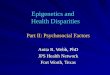
Disparities in Breast Cancer Treatments and Outcomes
Mammography
Histology
Stage at DiagnosisTreatment by
StageSurvival
Comorbidities,Obesity
Yood et al, OthersTammemagi et al, Griggs et al
Hershman et al,DignamStark et al
Grann et al
Bibb, Mandelblatt,Others
Bynum et alLipscombe et al
Chlebowski et al

Understanding Underlying Factors – Role of
Comorbidities
• Comorbidities as mediators of treatment choices, or of treatment effectiveness
• Comorbidities as predictors of survival or other health outcomes, independent of treatment for primary condition being studied
• Higher prevalence of comorbidities (e.g., hypertension, diabetes) among minority patients.

Survival Disparities in Breast Cancer – Role of Comorbidities
• Comorbidity and Survival Disparities Among Black and White Patients With Breast Cancer
• C. Martin Tammemagi, PhD; David Nerenz, PhD; Christine Neslund-Dudas, MA; Carolyn Feldkamp, PhD; David Nathanson, MD
JAMA. 2005;294:1765-1772.
• Approximately 900 Black and White Women with Breast Cancer, 10-Year Follow-up

Comorbidities and Breast Cancer (Cont.)
• African American women more likely than White women to have comorbidities
• Comorbidities associated with survival
• Comorbidities explained most of the disparity in all-cause survival, but not in cancer-specific survival.

DisparitiesDisparities in Lung Cancer Outcomes in Lung Cancer OutcomesHR (Black vs. White) = 1.21 (95% CI 1.05, 1.38; p = 0.008)HR (Black vs. White) = 1.21 (95% CI 1.05, 1.38; p = 0.008)Median survival Blacks = 8.5 months; Whites = 11.2 monthsMedian survival Blacks = 8.5 months; Whites = 11.2 months
Kaplan-Meier survival estimates, by race
Surv
ival
pro
porti
on
Follow-up in years0 1 2 3 4 5
0.00
0.25
0.50
0.75
1.00
Black
White

Kaplan Meier survival plots for 1154 LCA patients, Kaplan Meier survival plots for 1154 LCA patients, stratified bystratified by
.S
urvi
val p
ropo
rtion
Follow-up in years0 1 2 3 4 5
0.00
0.25
0.50
0.75
1.00
No comorbidity
Comorbidity.
Sur
viva
l pro
porti
on
Follow-up in years0 1 2 3 4 5
0.00
0.25
0.50
0.75
1.00
Absent
Present
Adverse comorbidity Adverse symptoms

Predictors of LCA survivalPredictors of LCA survival – hazard ratios & distributions (OR) by race/ethnicity – hazard ratios & distributions (OR) by race/ethnicity
Prognostic Factors Univariate HR Multivariate HR Black White Odds RatioB vs. W
Innate
Age (per 10 year increase) 1.16 (p <0.001) 1.24 (p <0.001) 67.5 yr 67.1 yr
Race/ethnicity (Black vs. White) 1.21 (p = 0.008) - -
Acquired
SES * (BGMHI $10,000) 0.92 (p < 0.001) $19,913 $38,822 0.37 (p < 0.001)
Marital status (spouseless vs. not) 1.27 (p = 0.001) 50.3% 37.1% 1.72 (p < 0.001)
Smoking status (current smk vs. not) 1.29 (p < 0.001) 1.32 (p < 0.001) 53.4% 44.2% 1.45 (p = 0.003)
Illicit drug use (user vs. not) 2.17 (p < 0.001) 1.99 (p = 0.004) 4.3% 0.3% 15.67 (p < 0.001)
Adverse comorbidity (≥1 vs. 0) 1.45 (p < 0.001) 1.42 (p < 0.001) 65.7% 59.0% 1.33 (p = 0.02)
Diagnostic intensity
Unstaged (vs. stage I) 4.61 (p < 0.001) 2.71 (p < 0.001) 7.8% 4.8% 1.69 (p = 0.03)
Histology (unspecified vs. SqCCA) 1.80 (p < 0.001) 1.26 (p = 0.03) 28.0% 20.9% 1.47 (p = 0.006)
Cancer-related factors
Adverse symptoms (≥1 vs. 0) 2.20 (p < 0.001) 1.65 (p < 0.001) 80.7% 70.5% 1.75 (p < 0.001)
Stage IStage IIStage IIIStage IV *
referent group2.16 (p < 0.001)3.49 (p < 0.001)7.09 (p < 0.001)
referent group2.11 (p = 0.001)3.37 (p < 0.001)6.90 (p < 0.001)
20.2%6.6%
33.2%40.0%
26.8%5.1%33.5%34.5%
OR (adv vs. local) =1.33 (p = 0.03)
Treatment
Surgery in localized NSCLC * 0.23 (p < 0.001) 55.2% 70.1% 0.53 (p = 0.01)
Chemotherapy (SCLC, III/IV NSCLC) 0.43 (p < 0.001) 45.9% 53.5% 0.74 (p = 0.03)
Any treatment (treated vs. not) 0.34 (p < 0.001) 70.6% 80.8% 0.57 (p < 0.001)
Surgery 0.51 (p < 0.001) 19.9% 30.4%
Chemotherapy 0.48 (p < 0.001) 41.3% 45.5%
Radiation therapy 0.89 (p = 0.15) 42.2% 43.1%

Why Think About Disparities in Terms of Quality of Care?
• Relatively strong science base of published literature and evidence-based guidelines conceptual and moral clarity
• Build on existing staff, data collection infrastructure, and organizational relationships
• Build on existing QI concepts, models, and approaches

Disparities in Standard Hospital Measures of Quality
of Care
• JCAHO/CMS Standard Measure Set– CHF– AMI– Pneumonia
• Commonwealth Fund – HRET Project• RWJF Initiative – “Expecting Success”

CMS/JCAHO Measures for CHF and AMI
0
10
20
30
40
50
60
70
80
90
100
Disch Inst LVEF ACE @Disch
SmokingAdvice
Asprin -Arrival
Aspirin -Disch
ACEI forLVSD
SmokingAdvice
B-Block atDisch
B-Block @Arriv
Mortality
BlackWhite
*
*
Per
cent

Analysis of Disparities – Basic Requirements
• Well-defined, accepted measures of quality, access, satisfaction, clinical outcomes
• Data on race/ethnicity, SES, primary language

Methods of Data Collection – Direct from Members/Patients• Pros:
– Most Flexible– Generally Preferred
for Accuracy
• Cons:– Can be Expensive– Can Raise Concerns
about Health Plan’s Real Objectives

Methods of Data Collection – Geocoding
• Pros:– Relatively Easy,
Fast, and Inexpensive
– Requires only Information you Already Have
• Cons:– Won’t Work in
Residentially Integrated Areas
– Won’t Identify Small, Dispersed Groups

Methods of Data Collection – Surname Recognition
• Pros:– Relatively Easy, Fast,
and Inexpensive– Can be Combined
with Geocoding
• Cons:– Only Works for
Groups with Distinct Names
– May not Work in All Market Areas

Health Plans as Catalysts for Quality Improvement
As agents of purchasers, health plans:
• Organize Quality Improvement Projects and
Programs
• Define Important Quality Domains and Develop Measures
• Disseminate Practice Guidelines
• Identify High-Priority Target Populations
• Identify High-Priority Clinical Conditions
• Develop Incentive Systems
• Direct Communications to Members

Comparison of Caucasian and African American
HbA1c Testing in a Single Plan
0
20
40
60
80
100
1998 1999 2000
Caucasian African American
Rate

Multiple Disparities in HEDIS Measures
in Single Health Plan(Six-State Medicaid Project)
0
10
20
30
40
50
60
70
HbA1cTesting
GoodGlycemicControl
AppropriateAsthma
Meds
PrenatalCare
CaucasianAfrican American
Hispanic
Per
cent
Source: Single Health Plan analysis of HEDIS data – 2003, unpublished

Asthma Medication ManagementAsthma Medication ManagementReporting Year 2003Reporting Year 2003
African-AmericanAfrican-American CaucasianCaucasian
NumeratNumeratoror
DenominatDenominatoror
RateRate NumeratNumeratoror
DenominatDenominatoror
RateRate
All Co’sAll Co’s 411411 600600 69%69% 698698 921921 76%76%
AA 189189 272272 69%69% 174174 218218 80%80%
BB 153153 213213 72%72% 375375 499499 75%75%
CC 6969 115115 60%60% 149149 204204 73%73%

Breast Cancer Screening Breast Cancer Screening Reporting Year 2003Reporting Year 2003
African-AmericanAfrican-American CaucasianCaucasian
NumeratNumeratoror
DenominatDenominatoror
RateRate NumeratNumeratoror
DenominatDenominatoror
RateRate
All Co’sAll Co’s 11161116 14681468 76%76% 25812581 31683168 81%81%
AA 390390 519519 75%75% 536536 650650 82%82%
BB 435435 561561 78%78% 14151415 17191719 82%82%
CC 291291 388388 75%75% 630630 799799 79%79%

African-AmericanAfrican-American CaucasianCaucasian
NumeratNumeratoror
DenominatDenominatoror
RateRate NumeratNumeratoror
DenominatDenominatoror
RateRate
All Co’sAll Co’s 211211 304304 69%69% 689689 837837 82%82%
AA 9494 142142 66%66% 161161 204204 79%79%
BB 8585 116116 73%73% 349349 429429 81%81%
CC 3232 4646 70%70% 179179 204204 88%88%
Appropriate Testing for Children with Appropriate Testing for Children with Pharyngitis Pharyngitis Reporting Reporting Year 2003Year 2003

Quality Improvement Interventions
in Single Health Plans
• Patient Reminders• Provider Reminders• Culturally-Sensitive Member
Education Materials• Disease Management Programs• Partnerships with Community Groups
to Raise Awareness of Prevention



Improvements in Quality of Care for African American Health Plan
Members with Diabetes
HbA1c Testing
0
20
40
60
80
100
African American Members
Percent2003
2004
LDL-C Testing
0
20
40
60
80
100
African American Members
Percent 2003
2004

Another Approach to Evaluating
QI Program Success• Asthma severity
definition involving ER visits and admissions
• Focus on African-American members with asthma
• Used shift in distribution of severity categories as measure of program success
• Statistically significant using Chi-square test
0
10
20
30
40
50
60
70
80
90
100
Mild Moderate Severe
Pre-InterventionPost-InterventionP
erc
en
t

Childhood Immunization – Combo I – (HEDIS 1999 Definition)
0
5
10
15
20
25
2002 2003 Rolling2003-2004
First Q2004
HispanicTotal
Perc
ent

Example of Quality of Care Disparities
Found in HEDIS Data(Six-State Medicaid Project)
0
10
20
30
40
50
60
70
HbA1cTesting
GoodGlycemicControl
AppropriateAsthma
Meds
PrenatalCare
CaucasianAfrican American
Hispanic
Per
cent
Source: Single Health Plan analysis of HEDIS data – 2003, unpublished

Which Disparity to Work On?
• Largest absolute difference?• Statistical significance of difference?• Size of denominator population?• Likelihood of making a difference?• Cost-effectiveness of intervention(s)?• Something else?
– Purchaser incentives/preferences– Community preferences

Commonwealth Fund Simulation Modeling Project -
Basic Premise
• Limited budgets and other resources to invest in disparity reduction initiatives
• A reasonable evidence base exists for modeling effects of disparity reductions on several measures of health– Mortality– Quality of life– Attendance at work or school

HEDIS Effectiveness of Care Measures - 2004
• Childhood Immunization Status• Adolescent Immunization
Status• Appropriate Treatment for
Children With Upper Respiratory Infection
• Appropriate Testing for Children With Pharyngitis
• Colorectal Cancer Screening• Breast Cancer Screening• Cervical Cancer Screening• Chlamydia Screening in Women• Osteoporosis Management in
Women Who Had a Fracture• Controlling High Blood
Pressure• Beta-Blocker Treatment After a
Heart Attack
• Cholesterol Management After Acute Cardiovascular Event
• Comprehensive Diabetes Care• Use of Appropriate Medications
for People With Asthma• Follow-Up After Hospitalization
for Mental Illness• Antidepressant Medication
Management• Medical Assistance With
Smoking Cessation• Flu Shots for Adults Age 50–64• Flu Shots for Older Adults• Pneumonia Vaccination Status
for Older Adults• Medicare Health Outcomes
Survey• Management of Urinary
Incontinence in Older Adults

Simulation Models – Basic Features
• Generally use existing published data, although it’s possible to collect and use primary data.
• Define key clinical/biological events and assign probabilities (and utility values) to those events.
• Create model structure that matches essential features of key clinical or biological processes.

Example of State TransitionsWhen Cancer Found (Stage III)

Sensitivity Analysis - Diabetes

QALY Gains for Alternative Disparity Reduction Initiatives
0
10
20
30
40
50
Diabete
s - All
Diabete
s - H
bA1c
Beta
Blocke
r - "B
ase"
Beta
Blocke
r - "O
ptim
istic"
Asthma
Mam
mog
raphy
- "B
ase"
Mam
mog
raphy
- "O
ptim
istic"
QA
LY
Gain
Per
1,0
00

Simulation Models - Conclusions / Next Steps
• Under basic sets of assumptions, health benefits related to eliminating disparities in four existing HEDIS measures are relatively modest.
• There is a significant range – approximately a hundred-fold variation - of potential benefits across all measures examined.
• Health benefits associated with other quality of care disparities in these clinical populations may be more significant (e.g., other dimensions of diabetes care, breast cancer treatment vs. breast cancer screening)
• We would like to expand the modeling effort to include attention to these other quality of care disparities.
• As available data allow, these methods can be applied to other HEDIS measures and other specific groups.

Overall Conclusions
• Plenty of documentation of disparities – need to know more now about underlying reasons and potential solutions.
• Policy changes are important, but clinical change happens at the local, single organization level.
• Quality improvement concepts and structures are a useful way to address disparities.
• We’ve made some progress in handling data collection and measurement challenges, but we have much yet to do.