Embed Size (px)
Citation preview

Adaptive Processing of Bioelectric Abdominal Signals To Improve
the Reliability of Fetal Home Telemonitoring
TOMASZ KUPKA, JANUSZ JEZEWSKI, ADAM MATONIA, DAWID ROJ, KRZYSZTOF HOROBA
Department of Biomedical Signal Processing
Institute of Medical Technology and Equipment
Roosevelta 118, 41-800 Zabrze,
POLAND
Abstract: - Centralized system for fetal home telemonitoring with wireless data transmission based on GSM service
and internet is presented in this paper. Cardiotocographic signals are provided by mobile instrumentation which
consists of bioelectrical signal recorder and Tablet PC. It enables to support a classical interpretation of
cardiotocographic trace by information on fetal electrocardiogram morphology. The system enables analysis, dynamic
presentation and archiving of acquired signals and medical data. Novelty of proposed approach relies on modification
of the procedures to process the abdominal signals in mobile instrumentation and adaptive controlling of the
monitoring session in surveillance center. These adaptations are performed automatically through advanced algorithms
based on continuous analyzing of the quality and quantitative parameters of the acquired signals. In that way the
amount and content of data transmitted through remote channels to surveillance center can be controlled to ensure the
most reliable assessment of fetal well-being.
Key-Words: - home monitoring, telemedicine, high-risk pregnancy, fetal surveillance, FECG, signal processing
1 Introduction Cardiotocography (CTG) is commonly used method of
fetal monitoring, which enables evaluation of the fetal
wellbeing during pregnancy and in labour. The method
relies on the analysis of characteristic fetal heart rate
(FHR) patterns in relation to the uterine contractions
(UC) and fetal movements. The normal heart activity
indicates the adequacy of fetal oxygenation and correct
functioning of central nervous system. Usually the FHR
signal acquisition is based on the Doppler ultrasound
technique which records the mechanical activity of the
fetal heart. Determination of instantaneous FHR relies
on the detection of heart beats based on the analysis of
ultrasound beam reflected from the moving valves or
walls. The main advantage of the Doppler ultrasound
technique is simplicity of application and non-
invasiveness, although the accuracy is rather low for the
automated signal analysis comprising evaluation of FHR
variability at a level of single heart beats. The
mechanical method as an indirect measuring technique
records the effects of electric excitation i.e. fetal heart
movement. Considerably higher accuracy and reliability
can be obtained using the primary bioelectric signal –
fetal electrocardiogram (FECG). Consecutive cardiac
cycles can be determined more accurately through
detection of QRS complexes in fetal electrocardiogram
then by analyzing the reflected ultrasound beam of a
complex shape. Authors developed measurement
instrumentation for acquisition and analysis of the fetal
electrocardiogram and uterine contraction activity on a
basis of bioelectrical signals recorded from maternal
abdominal wall. This Mobile Instrumentation (MI)
provides the telemedical system being under
development with both the FHR and UC signals.
The signal processing procedures running in Mobile
Instrumentation are preliminary adapted to measurement
conditions being changed. The proposed strategy is
based on the estimated quality of the biosignals recorded
from abdominal wall of the pregnant women.
Additionally, in the Surveillance Center a detailed
analysis of the FHR signal loss is carried out to control
an adaptive modification of the biosignal interpretation
algorithms in the MI. The fetal state is assessed by
means so called non-stress test (NST), whose result
decides about further diagnostic procedures.
In medical centers, a need for simultaneous
monitoring of many patients leads to wide use of
centralized fetal surveillance systems [1]. Recorded
signals from all fetal monitors along with analysis results
are simultaneously presented on the monitoring station
in a form of graphical and numerical data. Database
contains the archive of traces, analysis results and
medical history of patients. The limitation of currently
used systems is a lack of possibility to monitor the
patient outside the hospital. So far continuous medical
care requires a hospitalization of pregnant woman even
if there is no direct risk for patient’s health. It results in
high cost of longer hospital stay and discomfort for a
patient. The optimal solution seems to be a remote fetal
LATEST TRENDS on COMPUTERS (Volume I)
ISSN: 1792-4251 196 ISBN: 978-960-474-201-1
monitoring at patient’s home. Patients with high-risk
pregnancy as well as with post-term pregnancy are
particularly predisposed to cyclic home monitoring
sessions for follow-up of the fetal development process
[2].
When monitoring is based on recording of
bioelectrical abdominal signals, very careful preparation
of patient’s skin is required to obtain the signal of good
quality. Additionally, in the first stage of monitoring,
when template maternal QRS complexes are created,
patient should not move. This is the reason that the home
monitoring procedure should be carried out by the
hospital patient’s care staff. The operator with a mobile
fetal monitoring instrumentation visits particular patients
appointed to be monitored according to a fixed schedule.
However, some logistic problems with visit scheduling,
especially for large medical centers incorporating
numerous patients, should be solved.
2 System structure Fetal centralized surveillance system can be defined as a
set of fetal monitoring bedside devices, which transmit
cardiotocographic data to the central computer. In case
of telemonitoring the remote channel is assumed to work
on-line, so the monitoring session will be carried out in
the real-time. If a continuous data transmission is
assured, the monitoring can run in the same way as if the
patient would be in hospital (Fig.1). Wireless
communication is based on the data transmission service
used in cellular phones system, and internet which is
used for data transfer between GSM network and the
Surveillance Centre [3]. SC includes TCP/IP interface
allowing communicating with Mobile Instrumentation
via Internet. The system software has to be extended to
assure continuous, error-free data transmission and to
enable communication with the patient.
Mobile Instrumentation comprises a bioelectrical
signal recorder and Tablet Personal Computer or the
Personal Digital Assistant (PDA) as a computer with
built–in GSM module assuring the wireless connection
through the internet [4]. The computer software enables
acquisition and processing the signals from recorder,
their dynamic presentation and on-line evaluation of
their quality. Additionally, all the data acquired from the
fetal recorder are converted into the format established in
the surveillance system.
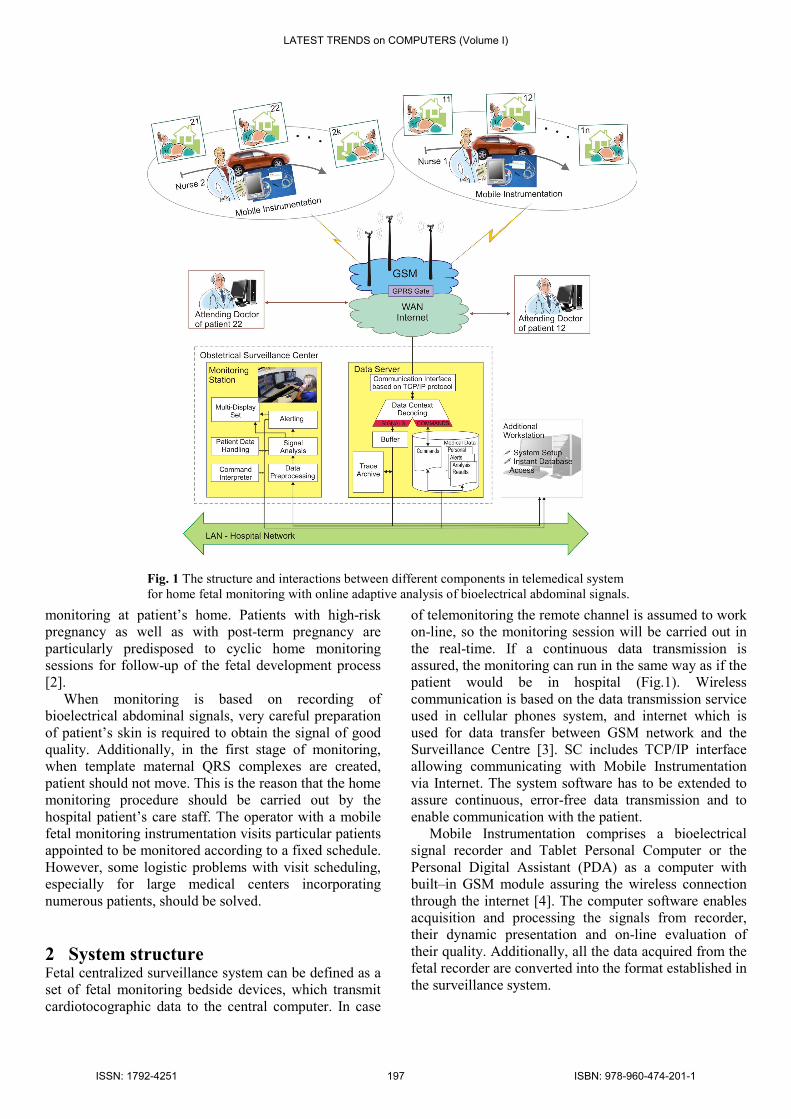
Fig. 1 The structure and interactions between different components in telemedical system
for home fetal monitoring with online adaptive analysis of bioelectrical abdominal signals.
LATEST TRENDS on COMPUTERS (Volume I)
ISSN: 1792-4251 197 ISBN: 978-960-474-201-1

The recorder is equipped with four differential
channels for measurement of abdominal signals. Typical
configuration comprises four electrodes placed around
the navel and the reference electrode placed above the
pubic symphysis. Additionally, the common mode
reference electrode is placed on the left leg. The
necessity of using four abdominal leads results from the
fact that very often the FECG signal of good quality is
present only in one lead. Considering abdominal FECG,
the basic merit of the presented recording unit is a very
low level of its own noise which does not exceed 1 µV
(peak-to-peak) measured with reference to the inputs,
and a high value of CMRR coefficient (120 dB). These
parameters have been obtained thanks to novel recorder
electronic circuits structure including complete
separation of analog part from the digital one [5]. Each
channel is equipped with an amplifier with gain control
that allows the amplification of recorded signals from
the tens of microvolts up to the level of several volts.
The band-pass filter removes low frequency components
and thus prevents the reaching of saturation state by
amplifiers in case of strong isoline drift.
The surveillance system located in hospital has a
capability of simultaneous monitoring of up to 24
patients, both remotely and within hospital. The main
system tasks are: the analysis of incoming data, dynamic
presentation of traces along with analysis results as well
as storing and printing the data. The quantitative
parameters describing acquired signals are used to detect
alerting situations.
Fig. 2 Computer screen of a surveillance centre presenting an
enlarged cardiotocographic trace from one of the patients
(scale 1 cm/min). The upper signal is the fetal heart rate, the
lower one is the uterine activity and markers between them
represent detected fetal movements. The horizontal bars
directly above the waveforms identify the characteristic trace
patterns. On the right side there is a window presenting last
three averaged fetal P-QRS-T complexes and corresponding
values of T/QRS coefficient.
The form of information displayed by the system
should not affect the interpretation of CTG trace. Since
in classic cardiotocography the acquired signals are
visualized as waveforms printed on thermosensitive
paper, the display provides the same graphic forms with
regard to quality, aspect ratio and waveforms flowing
(Fig.2). For records which are provided by bioelectrical
recorder an additional window can be displayed,
containing last three averaged fetal P-QRS-T complexes
and corresponding values of T/QRS coefficient. In
addition, any time-amplitude relationships can be
measured and stored in the database with appropriate
comment.
Optional workstation, connected through the local
network, provides an instant access to patients data and
acquired signals. Workstation can be used to set up the
system, to create paper documentation as well as to
process the signals recorded in the off-line mode (e.g. in
case of total breaking of the communication link). It is
possible to access the information stored in the archive
from outside the hospital via internet. This feature allows
the obstetrician to view the monitoring records at any
time he needs. However, due to the personal data
protection, the access is permitted only for attending
doctor for a given patient.
2.1 Signal analysis in Mobile Instrumentation The signal analysis is aimed at determination of fetal and
maternal heart rate signals (FHR and MHR), uterine
contractile activity (UC) from electrical activity of
uterine muscle - electrohysterogram (EHG), as well as
averaged P-QRS-T complex from fetal
electrocardiogram (Fig. 3).
Signal recorded from maternal abdomen includes the
maternal (MECG) and the fetal (FECG)
electrocardiograms, EHG as well as many unwanted
muscle and low frequency components. Suppression of
the dominating component in the abdominal signal –
maternal electrocardiogram – is the first, and at the same
time, the decisive step in abdominal fetal
electrocardiography [2, 6]. At first, the spatial filtering
based on the generalized singular value decomposition
(GSVD) is applied to extract pure dominating maternal
electrocardiogram from abdominal signal [7]. Having
such MECG the maternal QRS complexes can be
detected very precisely. Then, information on maternal
QRS complexes localization is used to determine the
maternal heart rate and to suppress the maternal ECG in
the abdominal signal which makes possible further
detection of the fetal QRS complexes. The basic
approach to MECG suppression is blanking, where
suitably long segment of the abdominal signal
comprising maternal complex is simply replaced by
isoline values. Unfortunately, in case of coincidence of
LATEST TRENDS on COMPUTERS (Volume I)
ISSN: 1792-4251 198 ISBN: 978-960-474-201-1

maternal and fetal complexes the latter one is rejected
causing partial FHR signal loss [6]. Nevertheless, this
disadvantage does not affect clinician’s interpretation
since for classical visual analysis the FHR signal is
averaged over 2.5-second periods. Additionally, low
computational complexity of the blanking approach
leads to significant reduction of power consumption in
Tablet or PDA computers.
Fig. 3 Adaptation of the biosignal analysis algorithms in the
MI controlled by the FECG quality index (SQI).
Blanking is applied to the abdominal signal in every
acquisition channel, with simultaneous controlling of the
quality of final FECG signal. The signal quality index
(SQI) takes values from 0 to 3, where 0 means very
weak signal, whereas 3 – its best quality. If the SQI
reaches the value of three in particular channel then the
fetal QRS complexes detection and consecutively
calculation of Trr intervals are carried out using the
signal acquired through this channel. The detection
function relies on matching filtering and application of a
set of decision rules [8]. Only these FHR values which
fulfill physiological criteria are finally accepted as
correct ones. If the SQI takes a value of two (satisfying
signal quality) in the best channel, then additional noise
suppression based on projective filtering [9] is applied
before QRS detection starts. If none of the channels
provides satisfying quality of the signal (2 or 3) this
means that the one-channel detection with blanking does
not ensure good results which causes significant FHR
loss. In that case more precise and advanced maternal
ECG suppression method has to be used, i.e. the method
based on subtraction of appropriately rescaled and
adaptively modified the reference maternal P-QRS-T
complex [2]. Suppression takes place in every abdominal
channel, and thus the fetal QRS detection is
multichannel. In this approach the additional noise
removal procedure is applied to improve FECG quality
before detection process starts. Any channel with SQI
equal to 0 is excluded from the fetal QRS detection.
Surveillance Center decides about a way of analysis
of the recorded signals to evaluate the fetal state.
Primary, an interpretation of CTG records is carried out.
If its result is unclear the additional morphology analysis
of fetal P-QRS-T complex is performed. Then, the
advanced suppression algorithm basing on subtraction of
reference maternal P-QRS-T complex is involved
automatically. Consecutive fetal P-QRS-T complexes
obtained in such way undergo the weighted averaging
[5]. For consecutive averaged complexes the relation of
the amplitude of T wave to the amplitude of QRS
complex is calculated (T/QRS ratio). Averaged
complexes together with relating T/QRS values are sent
to the Surveillance Center, where their further analysis is
carried out.
The contractile activity signal is determined basing
on electrical uterine muscle activity. For this task, the
abdominal signals are fed to low-pass filter with cut-off
frequency of 3.5 Hz, which corresponds to
electrohysterogram frequency band. The signals are then
downsampled from 500 Hz to 10 Hz. In the next stage
the resulting signal of the contractile activity is obtained
by composition of the signals from four leads. After that
the RMS values are calculated in the window of 60-s
width shifted with 3 seconds to obtain the consecutive
values of the UC signal [10].
2.2 Signal analysis in Surveillance Center In the Surveillance Center the algorithms have been
implemented to analyze CTG signal being received. The
analysis performed is consistent with guidelines of the
FIGO Subcommittee on Standards in Perinatal Medicine
[11]. The CTG analysis is accomplished in a number of
stages. In the first stage the FHR signal is verified basing
on identification and elimination of artifacts. Then the
analysis of signal loss and averaging over 2.5-s period
with interpolation of the lost values are carried out. It is
LATEST TRENDS on COMPUTERS (Volume I)
ISSN: 1792-4251 199 ISBN: 978-960-474-201-1

crucial for estimation of the FHR baseline – a basis for
recognition of the acceleration and deceleration patterns
as well as tachycardia and bradycardia episodes. In
addition, a set of indices is determined to estimate an
long and short term instantaneous FHR variability [5].
These indices are calculated for each one-minute
segment basing on a heart beat marker obtained from
FECG. Analysis of the uterine contraction activity signal
is aimed at recognition of the contraction episodes in
relation to so called basal tone, and then determination
of parameters describing contractions. They are very
important for recognition and classification of the
deceleration patterns, whereas information on fetal
movement activity is crucial for acceleration patterns.
Fig. 4 Adaptation of the biosignal analysis algorithms in the
Surveillance Center.
The FHR signal loss evaluated in Surveillance Centre
is key element for adaptive control of the algorithms for
analysis of the biosignals recorded in Mobile
Instrumentation (Fig. 4). But, preliminary adaptation
takes place automatically in Mobile Instrumentation on a
basis of the FECG quality index. Depending on its value,
less or more advanced method is selected to process the
bioelectrical signals recorded from maternal abdomen. In
the Surveillance Center the loss level of the FHR signal
(evenly sampled at 4 Hz and averaged over 2.5-second
segments) is continuously evaluated and checked.
When FHR loss exceeds 10% for at least two
minutes, the message is sent to MI which informs the
operator to check contact between electrodes and skin,
current position of patient (left side is recommended
during CTG monitoring session) as well as measurement
conditions. If the FHR loss signal remains above 10%
for the next five minutes the message is sent
automatically to Mobile Instrumentation in order to
execute more advanced processing of recorded
biosignals. If despite this action the FHR loss level is not
lower than 10% for next five minutes then alerting
message is displayed in Surveillance Center. It should be
taken into account by clinician during assessment of
CTG record since significant FHR signal loss may affect
his interpretation. As long as the FHR loss is below 10%
the selection of appropriate signal processing algorithms
is controlled in Mobile Instrumentation by fetal ECG
quality index evaluated.
Apart from procedures to control algorithms of
biosignal processing, an adaptive controlling of the CTG
monitoring session has been implemented in SC (Fig. 5),
according to non-stress test. This name emphasizes the
fact that NST is fully noninvasive. When computer-
aided CTG monitoring system is used this test is based
on detailed analysis of CTG record and provides
qualitative evaluation of fetal state. Procedure of
automated non-stress test leads to determination of test
result (reactive, nonreactive or suspicious) by means of a
set of decision rules applied to parameters of quantitative
CTG analysis. Usually, the test is carried out for at least
30 minutes.
If NST is reactive the CTG monitoring is finished,
because fetal well-being has been confirmed. In case of
any other test result, the test can be prolonged by next 30
minutes, however it is a decision made by doctor on call.
This is justified because the fetal activity can be
significantly lower during fetal sleep phase.
Fig. 5 Adaptive controlling the CTG monitoring in the
Surveillance Center.
LATEST TRENDS on COMPUTERS (Volume I)
ISSN: 1792-4251 200 ISBN: 978-960-474-201-1

The other approach relies on providing averaged fetal
P-QRS-T complex and T/QRS ratio that are sent from
Mobile Instrumentation on a request from Surveillance
Center. The aim of this additional information is to help
a clinician in making appropriate decision concerning
further patient’s treatment and necessity of her
hospitalization.
3 Conclucions The proposed system of fetal monitoring will certainly
improve patient’s comfort and reduce the cost of medical
care. Additionally, instant access to database will make
the communication between the patient and her attending
doctor much easier.
Automated and adaptive adjusting of the algorithms
applied to process recorded biosignals as well as
adaptive controlling the CTG monitoring session enable
considerable reduction of amount of data that have to be
sent to Surveillance Center from particular Mobile
Instrumentation. In most cases, the simplest algorithms
and regular duration (30 minutes) of CTG monitoring
session are sufficient. It is very important considering
many tasks that have to be accomplished by Surveillance
Centre simultaneously managing many patients. In
Mobile Instrumentation the proposed approach leads to
lengthening of the battery operating time and reducing
the cost of transmission through GSM/Internet.
Application of the bioelectrical signals recorder
enables information on fetal heart rhythm to be obtained
in a form of event series (heart beats). This enables more
precise calculation of the FHR instantaneous variability
indices, which is carried out in the Surveillance System.
Additionally, very important part of information is
provided by analysis of the averaged fetal P-QRS-T
complex, particularly with evaluation of the T/QRS
value changes. This information enables verification of
suspicious cardiotocographic traces.
Acknowledgement:
Scientific work financed from the State Committee for
Scientific Research resources in 2007-2011 years as a
research project No. N518 335935.
References:
[1] Jezewski J, Wrobel J, Horoba K, et al, Centralised
fetal monitoring system with hardware-based data
flow control, Proc III Conf MEDSIP, 2006,
pp. 51-54.
[2] Jezewski J, Matonia A, Kupka T, Gacek A, Horoba
K, Suppression of maternal ECG interference in
abdominal fetal electrocardiogram, IFMBE Proc of
the 12th Nordic Baltic Conference on Biomedical
Engineering and Medical Physics, Iceland, 2002,
pp.162-163.
[3] Salvador CH, Carrasco MP, et al. Airmed-Cardio, A
GSM and Internet Services-Based System for Out-of-
Hospital Follow-Up of Cardiac Patients, IEEE Trans
Inf Technol Biomed, 2005, Vol. 9, pp. 73-85.
[4] Hod M, Kerner R, Telemedicine for antenatal
surveillance of high-risk pregnancies with
ambulatory and home fetal rate monitoring: an
update, J Perinat Med, Vol. 31, 2003, pp. 195-200.
[5] Gacek A, Matonia A, Jezewski J, Kupka K,
Recognition of early symptoms of fetal distress with
on-line analysis of bioelectrical signals from
maternal abdomen, Biocybernetics and Biomedical
Engineering, 2007, Vol. 27(1), pp. 207-216.
[6] Kupka T, Jezewski J, Matonia A, Wrobel J, Horoba
K, Coincidence of maternal and fetal QRS complexes
in view of fetal heart rate determination, J Med
Inform Technology, Vol. 4, 2002, pp. 49-55.
[7] Callaerts D, DE Moor B, Vandewalle J, Sansen W,
Comparison of SVD method to extract the fetal
electrocardiogram from cutaneous electrode signals,
Med Biolog Eng Comput, 1990, Vol. 28,
pp. 217-224.
[8] Gibson NM, Woolfson MS, Crowe JA, Detection of
fetal electrocardiogram signals using matched filters
witch adaptive normalization, Med Biol Eng Comput,
1997, Vol. 35, pp. 216-222.
[9] Kotas M, Jezewski J, Matonia A, Kupka T, Spatio –
temporal filtering for fetal QRS enhancement,
IFMBE Proceedings of the World Congress on
Medical Physics and Biomedical Engineering,
Munich, IX 2009, Vol. 25, pp. 389-392.
[10] Radhakrishnan N, Wilson JD, Lowery C, et al., A
fast algorithm for detecting contractions in uterine
electromyography, IEEE Eng Med Biol, 2000,
pp. 89-94.
[11] Rooth G, Guidelines for the use of fetal monitoring,
Int J Gynaecol Obstet, 1987, 25, pp. 159-167.
LATEST TRENDS on COMPUTERS (Volume I)
ISSN: 1792-4251 201 ISBN: 978-960-474-201-1





























