Embed Size (px)
Citation preview

ResearchArticle
ConstipationprecedingParkinson’sdisease–asystematicreviewandmeta-analysis
KeralaL.Adams-Carr1,JonathanPBestwick2,SamuelShribman3,AndrewLees4,Anette
Schrag4,AlastairJNoyce4*
Affiliations:
1. CharingCrossHospital,London,UK
2. WolfsonInstituteofPreventiveMedicine,BartsandtheLondonSchoolofMedicine
andDentistry,London,UK
3. NationalHospitalforNeurologyandNeurosurgery,London,UK
4. InstituteofNeurology,UniversityCollegeLondon,London,UK
*CorrespondingAuthor
DrAlastairNoyce.DepartmentofMolecularNeuroscienceandRetaLilaWestonInstitute,
UCLInstituteofNeurology,1WakefieldStreet,LondonWC1N1PJ,UKTel:+44-207679
4246,Fax:+44-2072784993,Email:[email protected]
Keywords:Parkinson'sdisease,prodromalsymptoms,constipation,meta-analysis,
autonomicdysfunction
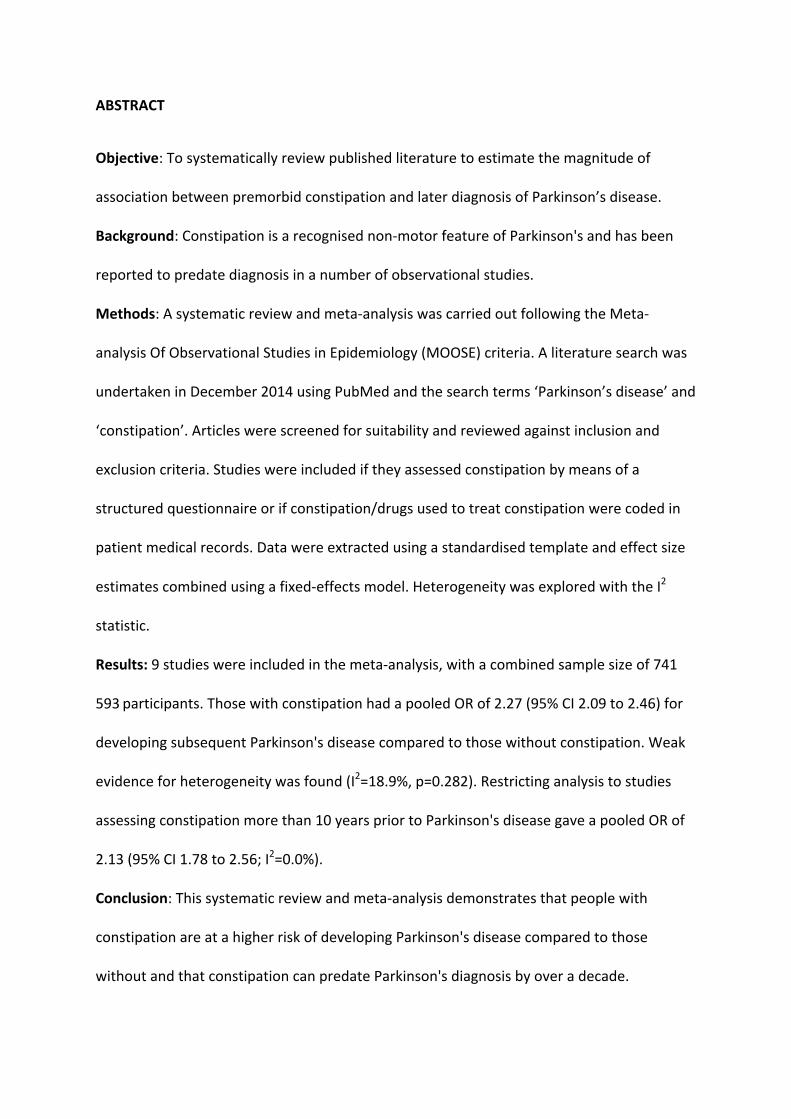
ABSTRACT
Objective:Tosystematicallyreviewpublishedliteraturetoestimatethemagnitudeof
associationbetweenpremorbidconstipationandlaterdiagnosisofParkinson’sdisease.
Background:Constipationisarecognisednon-motorfeatureofParkinson'sandhasbeen
reportedtopredatediagnosisinanumberofobservationalstudies.
Methods:Asystematicreviewandmeta-analysiswascarriedoutfollowingtheMeta-
analysisOfObservationalStudiesinEpidemiology(MOOSE)criteria.Aliteraturesearchwas
undertakeninDecember2014usingPubMedandthesearchterms‘Parkinson’sdisease’and
‘constipation’.Articleswerescreenedforsuitabilityandreviewedagainstinclusionand
exclusioncriteria.Studieswereincludediftheyassessedconstipationbymeansofa
structuredquestionnaireorifconstipation/drugsusedtotreatconstipationwerecodedin
patientmedicalrecords.Datawereextractedusingastandardisedtemplateandeffectsize
estimatescombinedusingafixed-effectsmodel.HeterogeneitywasexploredwiththeI2
statistic.
Results:9studieswereincludedinthemeta-analysis,withacombinedsamplesizeof741
593 participants.ThosewithconstipationhadapooledORof2.27(95%CI2.09to2.46)for
developingsubsequentParkinson'sdiseasecomparedtothosewithoutconstipation.Weak
evidenceforheterogeneitywasfound(I2=18.9%,p=0.282).Restrictinganalysistostudies
assessingconstipationmorethan10yearspriortoParkinson'sdiseasegaveapooledORof
2.13(95%CI1.78to2.56;I2=0.0%).
Conclusion:Thissystematicreviewandmeta-analysisdemonstratesthatpeoplewith
constipationareatahigherriskofdevelopingParkinson'sdiseasecomparedtothose
withoutandthatconstipationcanpredateParkinson'sdiagnosisbyoveradecade.

INTRODUCTION
Parkinson’sdisease(PD)isthesecondmostcommonneurodegenerativedisorderwitha
prevalenceofapproximately0.4%-afigurewhichisexpectedtodoubleby2040.[1]PDis
diagnosedwhenmotorfeaturessuchastremor,bradykinesiaandrigiditybecomeovert,by
whichtimeapproximately50%ofneuronswithinthesubstantianigraremain.[2]Overthe
pasttwodecades,avarietyofprodromeshavebeenrecognisedandmaycomprisea
numberofearlynon-motorsymptomsincludingthoseattributabletoautonomic
dysfunction,moodandcognitivedisturbance,sleepdisordersandsensorydisruption.[3]
Greaterunderstandingoftheseearlyfeaturesmayhelptheidentificationofindividualsat
higherriskofbeingdiagnosedwithPD,someofwhommaybecandidatesfor
neuroprotectivedrugtrials.
Constipation,aconsequenceofautonomicdysfunction,isoneofthemoststudiedofthe
prodromalsymptomsofPD.Arecentstudyoftheprevalenceofselectednon-motor
symptomsbeforeandafterdiagnosisofPDfoundthatconstipationwasthesecondmost
commonnon-motorsymptomofPDafteranosmia,withaprevalenceof50%inestablished
PD,andoccurringpriortodiagnosisinapproximately20%ofpatientsoverall.[4]Todate
onlyonemeta-analysishasexaminedthemagnitudeofriskassociatedwithconstipation
andthelaterdevelopmentofPD,aspartofawiderinvestigationofriskandprotective
factorsforPD.[5]Inthis,datawerepooledfromtwostudiesgivinganeffectsize(ES)
estimateof2.34forthedevelopmentofPDinpeoplewithconstipationascomparedto
thosewithout.Howevertheconfidenceintervals(CI)wererelativelywide,withthetrue
populationestimatepotentiallybetween1.6and3.5timeshigher.Sincethisinitialmeta-
analysispublishedin2012,severallargecohortandcase-controlstudieshavebeen

published,[6–10]contributingafurther10,697PDcases,wheretherewerepreviouslyonly
545.WehaverefinedtheESestimateoftheriskoffuturePDinthosethatareconstipated,
aswellasundertakinganalysisrestrictedtostudiesprovidingriskestimatesforconstipation
withonset≥10yearspriortoPDdiagnosis.
METHODS
SearchStrategy
TheMeta-analysisOfObservationalStudiesinEpidemiology(MOOSE)guidelinesfor
systematicreviewandmeta-analysisofobservationalstudiesinepidemiologywereadhered
tothroughoutthisstudy.Tworesearchers(KLA-C&AJN)independentlyundertooka
literaturesearchonthe7December2014usingPubMedandthesearchterms
“constipation”and“Parkinson’sdisease”.ThesearchwasrestrictedtoEnglisharticles,and
titlesandabstractswerescreenedfortheirsuitability.Articleswhoseabstractsdidnot
reportonconstipationandPD,orsolelyreportedprevalenceormanagementof
constipationinestablishedPDwereexcluded.Fullarticleswerethenobtainedandreviewed
todeterminesuitabilityforinclusionorexclusion.Differencesofopinionwereresolved
throughdiscussion.Thereferencelistsofallfullarticlesincluded,aswellasthereferences
fromreviewsandmeta-analysesidentifiedintheoriginalsearch,werehand-searchedfor
additionalrelevanttitleswhichwerethensubjectedtothesamefilteringprocessdescribed
above.
Inclusioncriteria

Publishedstudiesthatmetthefollowingcriteriawereincluded:(1)observationalstudies
withacohortorcase-controldesign;(2)caseswerepatientsdiagnosedwithPDaccordingto
standardclinicalcriteria,suchasQueenSquareBrainBankCriteria;[11](3)controlswere
healthyorhadnohistoryofneurologicaldisease;(4)controlsweredrawnfromthesame
populationascases;(5)constipationincontrolswasassessedoverthesametimeperiodas
forpatients;(6)constipationwasassessedbymeansofastructuredquestionnaire,orcoded
inpatientmedicalrecordsasconstipationormedicationusedtotreatconstipationand(7)
originaldatawerereported.
Figure1-Flowchartdepictingliteraturesearch.(PD=Parkinson'sdisease).

Exclusioncriteria
Abstracts,editorials,reviewarticles,conferenceproceedings,casereportsandlettersthat
didnotreportnewdatawereexcluded.Wealsoexcludedstudiesthat(1)reportedon
constipationonlyafterthediagnosisofPD;(2)reportedonbowelfunctionotherthan
constipation;(3)reportedonthemanagementofconstipationinPD;(4)didnotprovide
adequatedetailsofthecontrolgroup,orusedinappropriatecontrols(chronicallyillor
neurologicaldisease);(5)didnotreportsufficientdatatocalculateriskestimates;(6)
recordedinformationdifferentlyforcasesandcontrols;or(7)studiedoutcomesotherthan
PD.
Datahandling
Studycharacteristicsandriskestimateswereextractedfromallstudieseligibleforinclusion
andtabulatedinstandardtemplatetables.Whereriskestimates(relativerisk(RR)/hazard
ratio(HR)/oddsratio(OR))werenotavailable,datawerereviewedandanORcalculated
wherepossible(oddsintheexposeddividedbyoddsintheunexposed).Whererisk
estimatesforconstipationwereprovidedatmultipletimepointslessthan10yearspriorto
PDdiagnosis,themediantimepointwaschosen.Asecondriskestimatestablewas
compiledtotabulatedatafromthosestudiesthathadanaveragetimebetween
constipationonsetandPDdiagnosis≥10years.Whereriskestimateswereseparatedinto
multipletimepoints≥10yearspre-PDdiagnosis(i.e.7-12,13-18,and19-24years[6])and
poolingofthesedatawasnotpossible,theseestimateswereexcluded.
Weusedadefinitionofconstipationof<3bowelmovements(BMs)perweek,acriterion
withintheRomeIIIdefinitionforFunctionalConstipation.[12]Wherethisdefinitionof

constipationwasnotusedbystudies,riskestimatescorrespondingtotheclosestavailable
definitionwereextracted.Fortheonestudywhereconstipationwasdefinedbylaxative-use
asaproxyforseverity,thecategorylikelytogivethemostconservativeriskestimate('mild'
laxativeuse)waschosen.Whereconstipationwascodedinmedicalrecordsasabinary
term,itwasnotpossibletoascertainthediagnosticcriteriausedbutdatawerestillincluded
withinthemeta-analysis.
Wherefigureswereavailablethatexcludedpatientsenrolledlessthan2yearspriortoPD
diagnosis,thesefigureswerepreferredinordertoavoidconfoundingbyprevalentdisease.
Wherefiguresadjustedforlaxativeuse,theunadjustedfigureswereselected.
Wheretheaboveconditionsweremetandtherestillremainedachoicebetweenrisk
estimates,theriskestimatesmatchedoradjustedforageandgender,thatreflectedthefull
rangeofparticipantsanddidnothavedatamissing,wereused.Finally,studieswere
assessedforqualityusingtheNewcastleOttawaScale(NOS).[13]
StatisticalAnalysis
Measuresofeffectwerecombinedusingstandardmeta-analysismethods.ORswereused
asanestimateofRRs/HRswherenecessary(givenrarediseaseassumption)alongwith
95%CIs.ApooledESestimatewascalculatedusingafixed-effectsmodelintheabsenceof
clearheterogeneity.StatisticalheterogeneitywasexploredusingtheI2statisticbasedona
χ2testofobservedESineachstudyagainstthe(expected)pooledestimate.Thepre-
specifiedsignificancelevelforheterogeneitywassetat5%.Publicationbiaswasassessed
usingtheEggertestandafunnelplot.[14]StatisticalanalysiswasundertakeninStataV.13.

RESULTS
Theliteraturesearchyielded366results(seefigure1).Ofthese,47wereexcludedasthey
werenotwritteninEnglish,andafurther240wereexcludedonthebasisoftheirtitleand
abstract.Reviewoftheremaining79fullarticlesledto72exclusionsbasedoncriteria
describedabove.Handsearchingofreferencesofincludedstudiesandallreviewsledtothe
inclusionofoneadditionalstudy,whichbroughtthetotalnumberofincludedstudiesto
eight.Oneoftheincludedstudies[6]describedtwoseparatecohorts-onemale(Health
ProfessionalsFollow-upStudy)andonefemale(Nurses’HealthStudy),andthesewere
includedastwodistinctstudiesforthepurposesofanalysis,bringingthetotalnumberof
studiesincludedintheanalysistonine.Ofthese,fourwereprospectivecohortstudies,
[6,8,15]andtheremainingfivehadacase-controldesign.[7,9,10,16,17]Fourofthefive
case-controlstudiesutilisedinformationfromformalpatientmedicalrecords.The
combinedsamplesizeoftheninestudieswas741593.
Summarycharacteristicsandriskestimatesforallincludedstudiesareprovidedintables1-3
andonlinesupplementarytableS1.StudieswereassessedforqualityusingtheNOSandthe
resultsofthiscanbeviewedinonlinesupplementarytableS2.WithNOSqualitycriteria,all
studiesscored≥6/9andfouroftheincludedstudiesscored8/9.
Meta-analysistopooldatafromallninestudiesrevealedapositiveassociationbetween
constipationandsubsequentdiagnosisofPD(figure2).TheESestimateforthosewith
constipationandtheassociationwithPDwas2.27(95%CI2.09to2.46)comparedtothose
withoutconstipation.Weakevidenceforheterogeneitywasfound(I2=18.1%,p=0.282)and
therewasnoevidenceforpublicationbias(p-value=0.757;seeonlinesupplementaryfigure
S4).

Case-controlandcohortstudieswereanalysedseparatelytoexamineheterogeneity
betweenestimates.ThesummaryESofcase-controlstudieswas2.24(95%CI2.05to2.46),
whilethatofcohortstudieswas2.36(95%CI2.00to2.80).Therewasnoevidencefor
heterogeneitybetweenthesesub-groups(p=0.592).
TheaveragetimebetweenexposureassessmentanddiagnosisofPDvariedgreatlyamongst
thesestudies,rangingfrom<2yearsto>20years.Whenanalysiswasrestrictedtothoserisk
estimatescorrespondingtoconstipationwithanonset≥10yearspriortoPDdiagnosis
(figure3),asimilarlystrongpositiveassociationwasagainfound,withanESof2.13(95%CI
1.78to2.56;I2=0.0%,p=0.758).
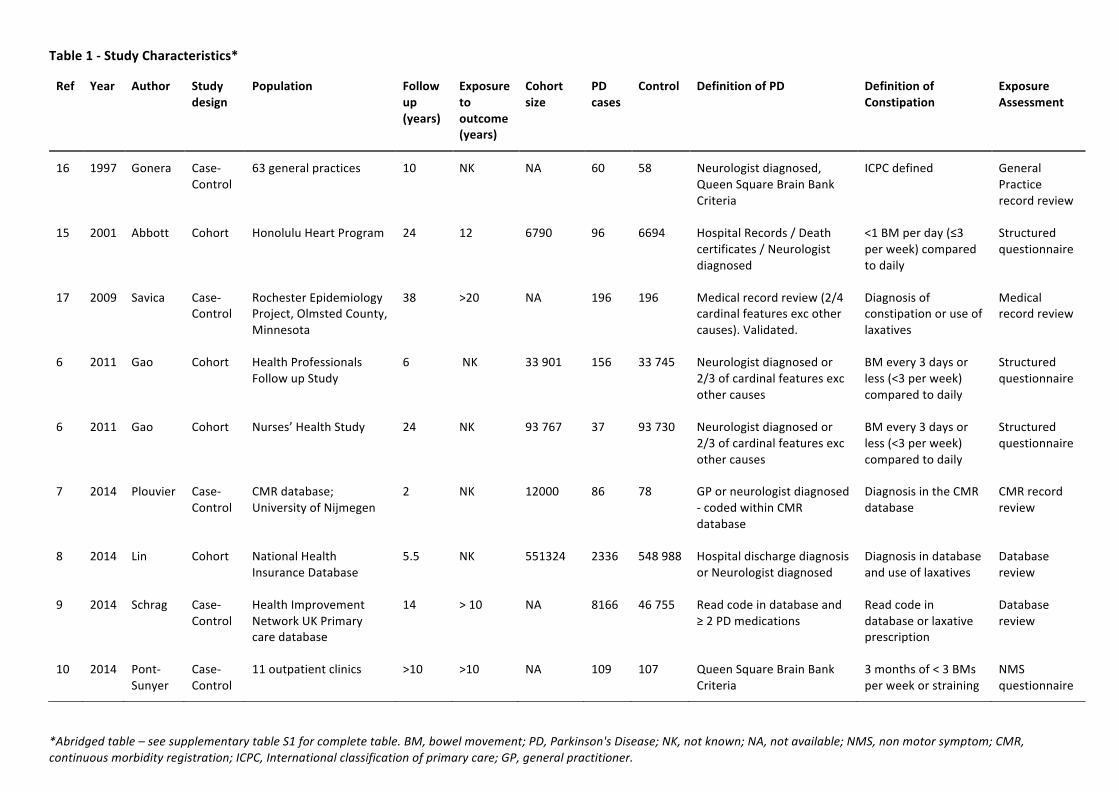
Table1-StudyCharacteristics*
*Abridgedtable–seesupplementarytableS1forcompletetable.BM,bowelmovement;PD,Parkinson'sDisease;NK,notknown;NA,notavailable;NMS,nonmotorsymptom;CMR,continuousmorbidityregistration;ICPC,Internationalclassificationofprimarycare;GP,generalpractitioner.
Ref Year Author Studydesign
Population Followup(years)
Exposuretooutcome(years)
Cohortsize
PDcases
Control DefinitionofPD DefinitionofConstipation
ExposureAssessment
16 1997 Gonera Case-Control
63generalpractices 10 NK NA 60 58 Neurologistdiagnosed,QueenSquareBrainBankCriteria
ICPCdefined GeneralPracticerecordreview
15 2001 Abbott Cohort HonoluluHeartProgram 24 12 6790 96 6694 HospitalRecords/Deathcertificates/Neurologistdiagnosed
<1BMperday(≤3perweek)comparedtodaily
Structuredquestionnaire
17 2009 Savica Case-Control
RochesterEpidemiologyProject,OlmstedCounty,Minnesota
38 >20 NA 196 196 Medicalrecordreview(2/4cardinalfeaturesexcothercauses).Validated.
Diagnosisofconstipationoruseoflaxatives
Medicalrecordreview
6 2011 Gao Cohort HealthProfessionalsFollowupStudy
6 NK 33901 156 33745 Neurologistdiagnosedor2/3ofcardinalfeaturesexcothercauses
BMevery3daysorless(<3perweek)comparedtodaily
Structuredquestionnaire
6 2011 Gao Cohort Nurses’HealthStudy 24 NK 93767 37 93730 Neurologistdiagnosedor2/3ofcardinalfeaturesexcothercauses
BMevery3daysorless(<3perweek)comparedtodaily
Structuredquestionnaire
7 2014 Plouvier Case-Control
CMRdatabase;UniversityofNijmegen
2 NK 12000 86 78 GPorneurologistdiagnosed-codedwithinCMRdatabase
DiagnosisintheCMRdatabase
CMRrecordreview
8 2014 Lin Cohort NationalHealthInsuranceDatabase
5.5 NK 551324 2336 548988 HospitaldischargediagnosisorNeurologistdiagnosed
Diagnosisindatabaseanduseoflaxatives
Databasereview
9 2014 Schrag Case-Control
HealthImprovementNetworkUKPrimarycaredatabase
14 >10 NA 8166 46755 Readcodeindatabaseand≥2PDmedications
Readcodeindatabaseorlaxativeprescription
Databasereview
10 2014 Pont-Sunyer
Case-Control
11outpatientclinics >10 >10 NA 109 107 QueenSquareBrainBankCriteria
3monthsof<3BMsperweekorstraining
NMSquestionnaire

Table2-Riskestimatesacrossallstudiesincludedinprimaryanalysis
RR,relativerisk;HR,hazardratio;OR,oddsratio;CI,confidenceinterval
Table3-Riskestimatescorrespondingtoconstipation≥10yearspre-PD
RR,relativerisk;HR,hazardratio;OR,oddsratio;CI,confidenceinterval,PD,Parkinson’sdisease
Ref Year Author StudyDesign pvalue RR HR OR CIlower CIupper
16 1997 Gonera Case-control 0.209 - - 0.45 0.13 1.57
15 2001 Abbott Cohort 0.013 2.30 - - 1.2 4.5
17 2009 Savica Case-control 0.0005 - - 2.48 1.49 4.11
6 2011 Gao–HPFS Cohort <0.0001 4.35 - - 1.80 10.5
6 2011 Gao–NHS Cohort 0.03 2.98 - - 1.09 8.14
7 2014 Plouvier Case-control 0.039 - - 3.32 1.1 10.4
8 2014 Lin Cohort <0.0001 - 2.29 - 1.91 2.74
9 2014 Schrag Case-control - 2.24 - - 2.04 2.46
10 2014 Pont-Sunyer Case-control <0.05 - - 2.7 1.4 5.2
Ref Year Author StudyDesign
Exposuretooutcome(years)
pvalue RR HR OR CIlower CIupper
15 2001 Abbott Cohort 12 0.013 2.30 - - 1.2 4.5
17 2009 Savica Case-control
>20 0.0005 - - 2.48 1.49 4.11
9 2014 Schrag Case-control
>10 - 2.01 - - 1.62 2.49
10 2014 Pont-Sunyer Case-control
>10 <0.05 - - 2.7 1.4 5.2

Figure2-ForestplotdemonstratingincreasedPDriskinthosewithpremorbidconstipation
ascomparedtothosewithout.(PD,Parkinson’sdisease;RR,relativerisk;HR,hazardratio;
OR,oddsratio;CI,confidenceinterval).
Figure3-ForestplotdemonstratingincreasedriskofdevelopingPDinthosewith
constipationofduration≥10yearsascomparedtothosewithoutconstipation.(PD,
Parkinson’sdisease;RR,relativerisk;OR,oddsratio;CI,confidenceinterval).

DISCUSSION
Thissystematicreviewandmeta-analysisoffersconfirmationforthepreviouslyreported
associationbetweenpremorbidconstipationandsubsequentdiagnosisofPD.The
consistencyoftheassociationarguesagainstthepossibilitythatthiscouldbeachance
findinganditsplausibilityishighgivensimilarfindingsindifferentstudydesigns;both
prospectiveandretrospective,withdifferentbiases,inherentassumptionsandmethodsof
exposureascertainment.TheCIfortheESistightsuggestingthetruepopulationrisk
estimateisintherangeof2.0-2.5-fold.Theobservationholdsforpooledanalysisofstudies
assessingtheperiodmorethan10yearsbeforediagnosis.
Quantifyingthemagnitudeofassociationbetweenearlynon-motorfeaturesand
subsequentPDmayunderpineffortstoidentifyhigherriskparticipantsforentryto
interventionalstudieswithneuroprotectiveaims.[18]Althoughthesizeofelevatedrisk
conveyedbyconstipationmightbemodestoverall,thisislikelyaconsequenceof
constipationbeingacommonsymptomencounteredinolderage,andthatmanywhosuffer
willnotgoontobediagnosedwithPD.However,thestrengthofassociationissimilarmore
thanadecadebeforediagnosiswithPD,suggestingalongwindowofopportunityfor
intervention,werecertaintyoffuturePDtobeimprovedthroughcombinationwithother
markers(clinical,imaging,laboratory)oftheprodrome.Ofnote,oneoftheincludedcase-
controlstudiesfoundsignificantassociationswithconstipationpredatingPDdiagnosisby20
years,buttheCisfortheassociationwerewide.[17]
ThreemainpossibleunderlyingreasonsfortheassociationofconstipationwithPDare:(1)
constipationisamanifestationofearlyPDwithinthebowelandthereforepartofthe

diseaseitself,(2)constipationisariskfactorforPDandithasacausalassociationwith
subsequentdisease,or(3)constipationandPDarebothoutcomesofacommonexposure.
Immunohistochemicalstudieshavedemonstratedtheexistenceofabnormaldepositsofα-
synucleinwithinthesubmucosalandmyentericplexusesoftheentericnervous
system.[19,20]Whilstthepathophysiologicalbasisforcolonicdysmotilityandpelvicfloor
dysfunctionthatcausesconstipationinPDremainsunclear,[21]thepresenceofthese
depositsraisesthepossibilityofmakingatissuediagnosisofPDduringlife.Severalstudies
havereportedpositivefindingsfrombiopsiestakenduringroutinecolonoscopyinpatients
withPDcomparedwithcontrols.[22,23]Theinvestigationofgutbiopsyinarchivaltissue
obtainedpriortoPDdiagnosisinsmallnumbersofparticipantswaspromptedbythe
observationthatconstipationwasanearlynon-motorfeatureofPD.[24]Subsequently,α-
synucleinaccumulationhasbeendetectedincolonicbiopsiestakenupto7yearsbeforethe
onsetofmotorsymptoms.[25]
EndoscopicgastrointestinalbiopsyremainsanactiveareaofPDbiomarkerresearch,but
thereisnowalsogrowinginterestinthegutmicrobiome.Inarecentpilotstudy,the
abundanceofPrevotellaceaeinfaeceswassignificantlylowerinPDpatientscomparedto
controlsandpositiveassociationswerefoundbetweenabundanceofEnterobacteriaceae
andmotorsymptomsofPD.[26]Whetherchangesingutfloraarereplicablemustnowbe
elucidatedthroughfurtherstudy,andifso,thematterofwhethertheyareacauseor
consequenceofdiseasemustbedeterminedsincebothcouldconfoundtheassociation
betweenconstipationandPD.Additionalchallengeslieinunderstandingtheimpactof
laxativeuseanddietaryhabits,andthesemustbemetbeforethemicrobiomecouldbe
consideredapotentialbiomarkerofdiseasestate.
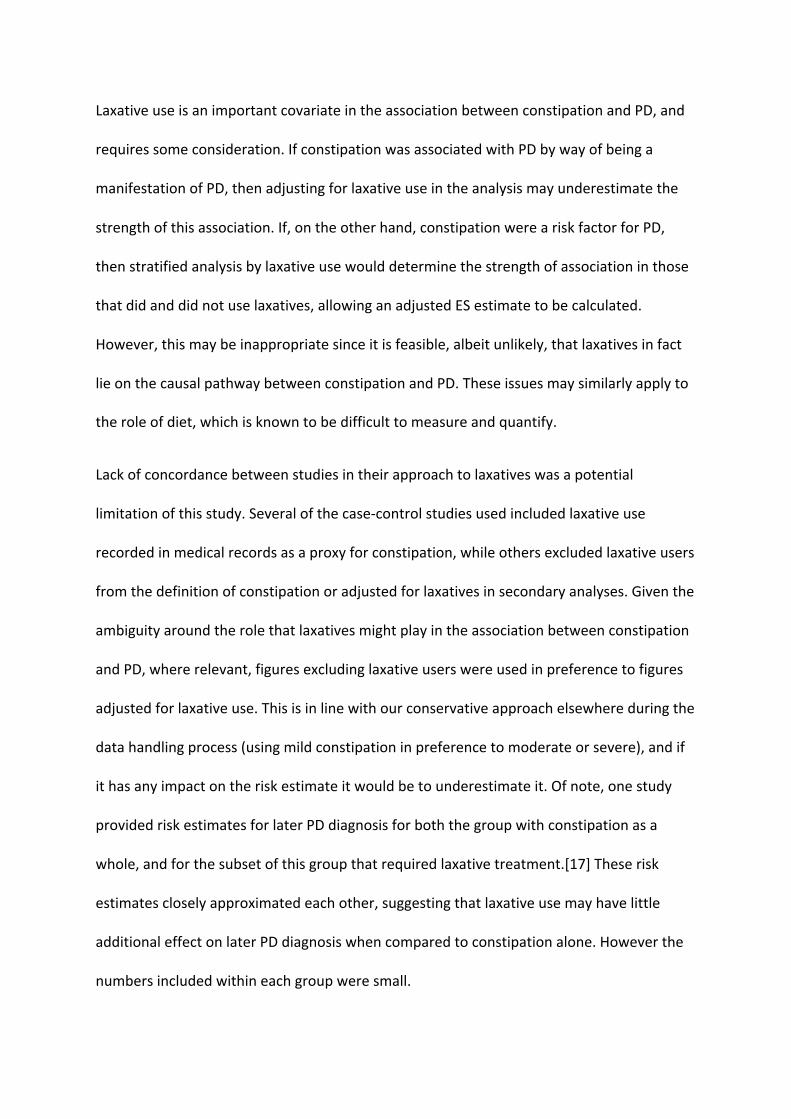
LaxativeuseisanimportantcovariateintheassociationbetweenconstipationandPD,and
requiressomeconsideration.IfconstipationwasassociatedwithPDbywayofbeinga
manifestationofPD,thenadjustingforlaxativeuseintheanalysismayunderestimatethe
strengthofthisassociation.If,ontheotherhand,constipationwereariskfactorforPD,
thenstratifiedanalysisbylaxativeusewoulddeterminethestrengthofassociationinthose
thatdidanddidnotuselaxatives,allowinganadjustedESestimatetobecalculated.
However,thismaybeinappropriatesinceitisfeasible,albeitunlikely,thatlaxativesinfact
lieonthecausalpathwaybetweenconstipationandPD.Theseissuesmaysimilarlyapplyto
theroleofdiet,whichisknowntobedifficulttomeasureandquantify.
Lackofconcordancebetweenstudiesintheirapproachtolaxativeswasapotential
limitationofthisstudy.Severalofthecase-controlstudiesusedincludedlaxativeuse
recordedinmedicalrecordsasaproxyforconstipation,whileothersexcludedlaxativeusers
fromthedefinitionofconstipationoradjustedforlaxativesinsecondaryanalyses.Giventhe
ambiguityaroundtherolethatlaxativesmightplayintheassociationbetweenconstipation
andPD,whererelevant,figuresexcludinglaxativeuserswereusedinpreferencetofigures
adjustedforlaxativeuse.Thisisinlinewithourconservativeapproachelsewhereduringthe
datahandlingprocess(usingmildconstipationinpreferencetomoderateorsevere),andif
ithasanyimpactontheriskestimateitwouldbetounderestimateit.Ofnote,onestudy
providedriskestimatesforlaterPDdiagnosisforboththegroupwithconstipationasa
whole,andforthesubsetofthisgroupthatrequiredlaxativetreatment.[17]Theserisk
estimatescloselyapproximatedeachother,suggestingthatlaxativeusemayhavelittle
additionaleffectonlaterPDdiagnosiswhencomparedtoconstipationalone.Howeverthe
numbersincludedwithineachgroupweresmall.

Otherlimitationsofthisstudyincludethelimitsoftheliteraturesearch:restrictedto
PubMed,toarticleswritteninEnglish,andtothesearchterms'constipation'and
'Parkinson'sdisease',whichmayconceivablyhaveledtosomemissingstudies.However,
thereferencesofallfullarticlespickedupintheinitialsearchwerehandsearchedfor
additionalrelevantstudies,andonlyoneadditionalpaperwasidentifiedviathisstrategy.A
broadrangeofstudydesignswasincluded,withavarietyofmethodsemployedto
determineanddefine'constipation'.Welimitedvariabilitywherepossiblebyselectingthe
definitionsmostinkeepingwithoneanother,andadefinitioninlinewiththeRomeIII
criteriaforfunctionalconstipation.[12]Whereconstipationorlaxativeusewascodedin
medicalrecords,theexactdefinitionofconstipationineachcasecouldnotbedetermined.
However,despitetheimpactthiscouldhavehadonvariabilitybetweenstudyresults,our
analysisshowedlittleevidenceforheterogeneitybetweenstudies,andbetweencase-
controlandcohortsub-groupsasawhole,suggestingthattheeffectthatdifferent
definitionsofconstipationandstudydesignshadonriskestimatesdidnotdiffergreatly.
Recallbiasisaconcernwhenincludingresultsfromsomecase-controlstudies,however
onlyoneofthenineincludedstudiesadoptedaretrospectivedesign,wherebyparticipants
wereaskedtorecallthedateofonsetofanumberofnon-motorsymptoms.The
introductionofrecallbiasinthisparticularstudywasminimisedbyrecruitingpatientsonly
recentlydiagnosedwithPD,withamediantimebetweenPDdiagnosisandstudyevaluation
of1month.[10]
ThequalityofthestudieswasassessedviameansoftheNOS.[13]Allstudiesincludedinthe
mainanalysishadscores≥6/9,andallstudiesinthesecondaryanalysis(studiesthat
examinedconstipationoveradecadebeforePDdiagnosis)hadascoreof8/9(seeonline

supplementarytableS2).Therefore,theriskestimatethatresultedfromthisanalysismay
alsobeviewedasafairly'stringent'estimate,aresultofthepoolingofdatafromonly
highestqualitystudies.Afurtherbenefitofthesecondaryanalysisisthatanysubjectswith
undiagnosedprevalentPDwouldlikelynothavebeenincluded,andsoitavoidspotential
biasthatwouldariseinthisscenario.
Itshouldbenotedthattheriskestimatesprovidedherearemorelikelytounderestimate
thetruemagnitudeofassociationbetweenconstipationandlaterdevelopmentofPDthan
overestimateit.Thisisbecausemoreconservativedefinitionsofconstipationwereselected
whereachoicewasavailable.Infuturestudies,werecommend:(1)thatauniversal
definitionofconstipationisusedwherepossible,suchas<3BMsperweekinthepresence
ofotherfeatures(e.g.strainingorhardstools),inlinewithRomeIIIcriteria;and(2)that
measuresofeffectaredeterminedforbothconstipationandlaxativeuseandunadjusted
andstratum-specificmeasuresofeffectarereportedtobetterdeterminetheassociation
witheach.
Inconclusion,wepooldatafrom741593 peopleacrossninestudiestoprovidea
consolidatedriskestimaterelatingpremorbidconstipationtoalaterdiagnosisofPD.Our
riskestimatesuggeststhat,comparedwithsomeonewithout,anindividualwith
constipationisata2.27-foldincreasedriskofdevelopingPD,andthisincreaseinrisk
persistsoveradecadepriortodiagnosis.Thisupdatespreviousriskestimates(with
associatedwideCIs)andprovidesinformationthatwillhelpascertainthoseatincreasedrisk
ofPDandperhapsbetterunderstandtheearlystagesofdisease.

CONTRIBUTORS:KLA-Ccollecteddata,performedstatisticalanalysisanddraftedthe
manuscript.JPBconceivedtheproject,performedstatisticalanalysisandprovidedcritical
revisionofthemanuscript.SSprovidedcriticalrevisionofthemanuscript.ALandAS
conceivedtheprojectandprovidedcriticalrevisionofthemanuscript.AJNconceivedthestudy,collecteddata,performedstatisticalanalysisanddraftedthemanuscript.
FUNDING:AJNisfundedbyParkinson’sUK(grantreferenceF-1201).ALhasreceived
honorariafromNovartis,Teva,Meda,BoehringerIngelheim,GSK,Ipsen,Lundbeck,Allergan
andOrion.AShasreceivedgrantmoneyfromGEHealthcareandhonorariafromUCB.AJNhasreceivedgrantsfromÉlan/ProthenaPharmaceuticalsandfromGEHealthcare.
COMPETINGINTERESTS:Nonedeclared.
PROVENANCEANDPEERREVIEW:Notcommissioned;externallypeerreviewed.
DATASHARINGSTATEMENT:Alldatawithinthestudyareavailableinpublishedform.
REFERENCES
1 KowalSL,DallTM,ChakrabartiR,etal.ThecurrentandprojectedeconomicburdenofParkinson’sdiseaseintheUnitedStates.MovDisord2013;28:311–8.doi:10.1002/mds.25292
2 FearnleyJM,LeesAJ.AgeingandParkinson’sdisease:substantianigraregionalselectivity.Brain1991;114:2283–301.
3 PostumaRB,AarslandD,BaroneP,etal.IdentifyingprodromalParkinson’sdisease:pre-motordisordersinParkinson’sdisease.MovDisordOffJMovDisordSoc2012;27:617–26.doi:10.1002/mds.24996
4 ChenH,ZhaoEJ,ZhangW,etal.Meta-analysesonprevalenceofselectedParkinson’snonmotorsymptomsbeforeandafterdiagnosis.TranslNeurodegener2015;4:1.doi:10.1186/2047-9158-4-1
5 NoyceAJ,BestwickJP,Silveira-MoriyamaL,etal.Meta-analysisofearlynonmotorfeaturesandriskfactorsforParkinsondisease.AnnNeurol2012;72:893–901.doi:10.1002/ana.23687
6 GaoX,ChenH,SchwarzschildMA,etal.AprospectivestudyofbowelmovementfrequencyandriskofParkinson’sdisease.AmJEpidemiol2011;174:546–51.doi:10.1093/aje/kwr119
7 PlouvierAOA,HameleersRJMG,vandenHeuvelEAJ,etal.ProdromalsymptomsandearlydetectionofParkinson’sdiseaseingeneralpractice:anestedcase-controlstudy.FamPract2014;31:373–8.doi:10.1093/fampra/cmu025

8 LinC-H,LinJ-W,LiuY-C,etal.RiskofParkinson’sdiseasefollowingsevereconstipation:Anationwidepopulation-basedcohortstudy.ParkinsonismRelatDisord2014;20:1371–5.doi:10.1016/j.parkreldis.2014.09.026
9 SchragA,HorsfallL,WaltersK,etal.PrediagnosticpresentationsofParkinson’sdiseaseinprimarycare:acase-controlstudy.LancetNeurol2015;14:57–64.doi:10.1016/S1474-4422(14)70287-X
10 Pont-SunyerC,HotterA,GaigC,etal.TheonsetofnonmotorsymptomsinParkinson’sdisease(theONSETPDstudy).MovDisordOffJMovDisordSoc2015;30:229–37.doi:10.1002/mds.26077
11GibbWR,LeesAJ.TherelevanceoftheLewybodytothepathogenesisofidiopathicParkinson’sdisease.JNeurolNeurosurgPsychiatry1988;51:745–52.
12 RomeFoundation.Guidelines--RomeIIIDiagnosticCriteriaforFunctionalGastrointestinalDisorders.JGastrointestLiverDisJGLD2006;15:307–12.
13WellsGA,SheaB,O’connellD,etal.TheNewcastle-OttawaScale(NOS)forassessingthequalityofnonrandomisedstudiesinmeta-analyses.2000.
14 EggerM,SmithGD,SchneiderM,etal.Biasinmeta-analysisdetectedbyasimple,graphicaltest.BMJ1997;315:629–34.doi:10.1136/bmj.315.7109.629
15 AbbottRD,RossGW,PetrovitchH,etal.Bowelmovementfrequencyinlate-lifeandincidentalLewybodies.MovDisordOffJMovDisordSoc2007;22:1581–6.doi:10.1002/mds.21560
16GoneraEG,HofMV,BergerHJC,etal.Symptomsanddurationoftheprodromalphaseinparkinson’sdisease.MovDisord1997;12:871–6.doi:10.1002/mds.870120607
17 SavicaR,CarlinJM,GrossardtBR,etal.MedicalrecordsdocumentationofconstipationprecedingParkinsondisease:Acase-controlstudy.Neurology2009;73:1752–8.doi:10.1212/WNL.0b013e3181c34af5
18 BergD,MarekK,RossGW,etal.Definingat-riskpopulationsforParkinson’sdisease:lessonsfromongoingstudies.MovDisordOffJMovDisordSoc2012;27:656–65.doi:10.1002/mds.24985
19 BraakH,deVosRAI,BohlJ,etal.Gastricα-synucleinimmunoreactiveinclusionsinMeissner’sandAuerbach’splexusesincasesstagedforParkinson’sdisease-relatedbrainpathology.NeurosciLett2006;396:67–72.doi:10.1016/j.neulet.2005.11.012
20 BeachTG,AdlerCH,SueLI,etal.Multi-organdistributionofphosphorylatedalpha-synucleinhistopathologyinsubjectswithLewybodydisorders.ActaNeuropathol(Berl)2010;119:689–702.doi:10.1007/s00401-010-0664-3
21WangC-P,SungW-H,WangC-C,etal.EarlyrecognitionofpelvicfloordyssynergiaandcolorectalassessmentinParkinson’sdiseaseassociatedwithboweldysfunction.

ColorectalDisOffJAssocColoproctologyGBIrel2013;15:e130–7.doi:10.1111/codi.12105
22 PoucletH,LebouvierT,CoronE,etal.AcomparisonbetweencolonicsubmucosaandmucosatodetectLewypathologyinParkinson’sdisease.NeurogastroenterolMotilOffJEurGastrointestMotilSoc2012;24:e202–5.doi:10.1111/j.1365-2982.2012.01887.x
23 LebouvierT,NeunlistM,BruleydesVarannesS,etal.ColonicbiopsiestoassesstheneuropathologyofParkinson’sdiseaseanditsrelationshipwithsymptoms.PloSOne2010;5:e12728.doi:10.1371/journal.pone.0012728
24 ShannonKM,KeshavarzianA,DodiyaHB,etal.Isalpha-synucleininthecolonabiomarkerforpremotorParkinson’sDisease?Evidencefrom3cases.MovDisord2012;27:716–9.doi:10.1002/mds.25020
25HiltonD,StephensM,KirkL,etal.Accumulationofα-synucleininthebowelofpatientsinthepre-clinicalphaseofParkinson’sdisease.ActaNeuropathol(Berl)2014;127:235–41.doi:10.1007/s00401-013-1214-6
26 ScheperjansF,AhoV,PereiraPAB,etal.GutmicrobiotaarerelatedtoParkinson’sdiseaseandclinicalphenotype.MovDisordOffJMovDisordSoc2015;30:350–8.doi:10.1002/mds.26069