Embed Size (px)
Citation preview

Carlos Bechara MD on behalf of the adhoc committeeAssociate Professor, Program DirectorHouston Methodist hospitalAPDVS 2017
AD HOC COMMITTEE ON CORE SURGERY TRAINING & DEFINED MINIMUMS FOR CASE LOGS REPORT
• We have nothing to disclose in relation to this talk
• Whether we should add other categories like dialysis and venous minimum cases*
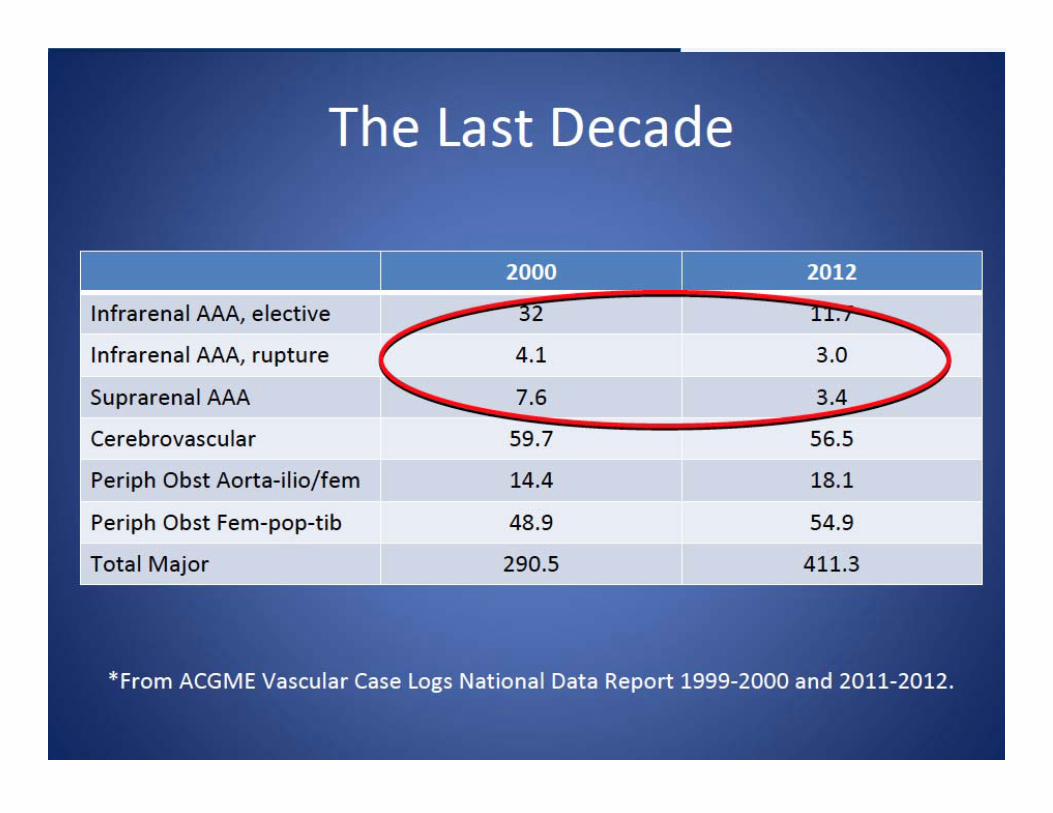
• Decline in open operative experience*– ?Role of courses and simulation
• There is variability in core rotations• Experience varies among different institutions • Can some of these be taught by vascular surgeons
– Other subspecialties reduced months on general surgery
WERE WE LEFT OFF LAST YEAR REGARDING CASE MINIMUMS AND CORE SURGERY ROTATIONS:
*affects fellowship and integrated programs
TOTAL CASE VOLUME REQUIRMENTS
• Residents in an integrated program should perform a minimum of 500 operations, to include 250 major vascular reconstructive procedures. (Core)– IV.A.6.c).(1) Operative experience in excess of 1500 total cases
must be justified by the program director. (Core)
• Residents in an independent program should perform a minimum of 250 major vascular reconstructive procedures. (Core) – Operative experience in excess of 900 total cases must be
justified by the program director. (Core)
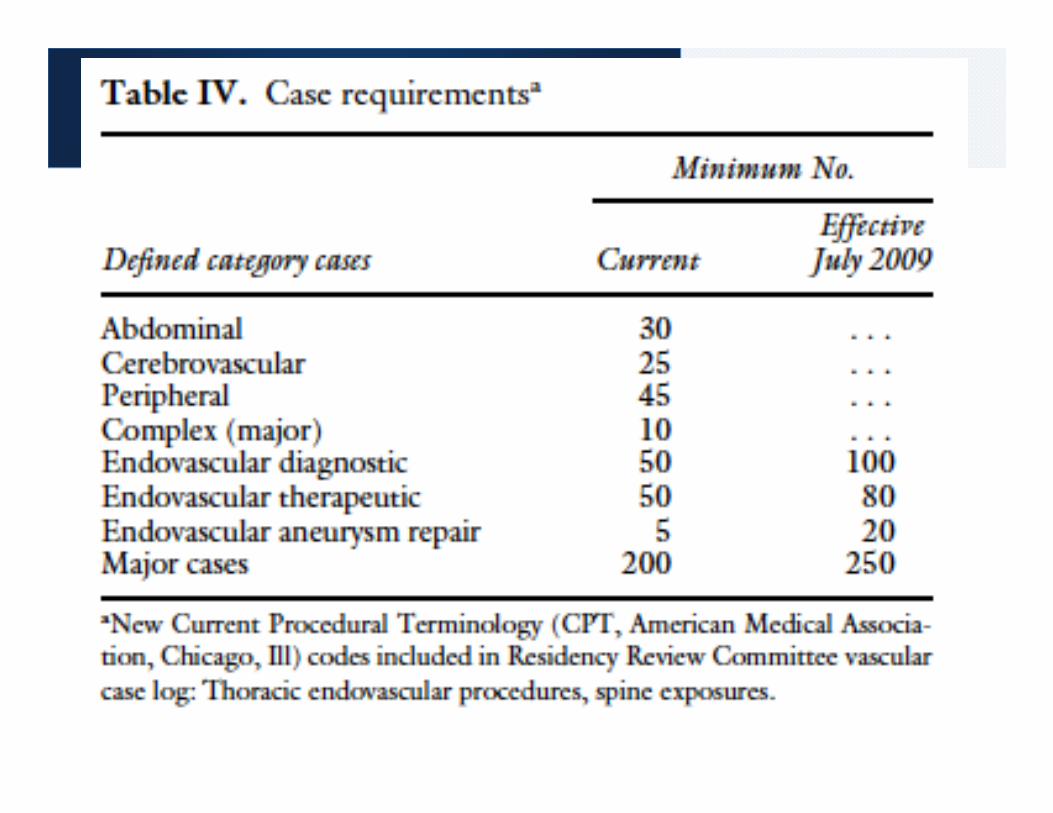

CASE LOG MINIMUMSVASCULAR SURGERY DEFINED CATEGORY MAPPINGS

ACGME PROGRAM REQUIREMENTS FOR GME IN VS
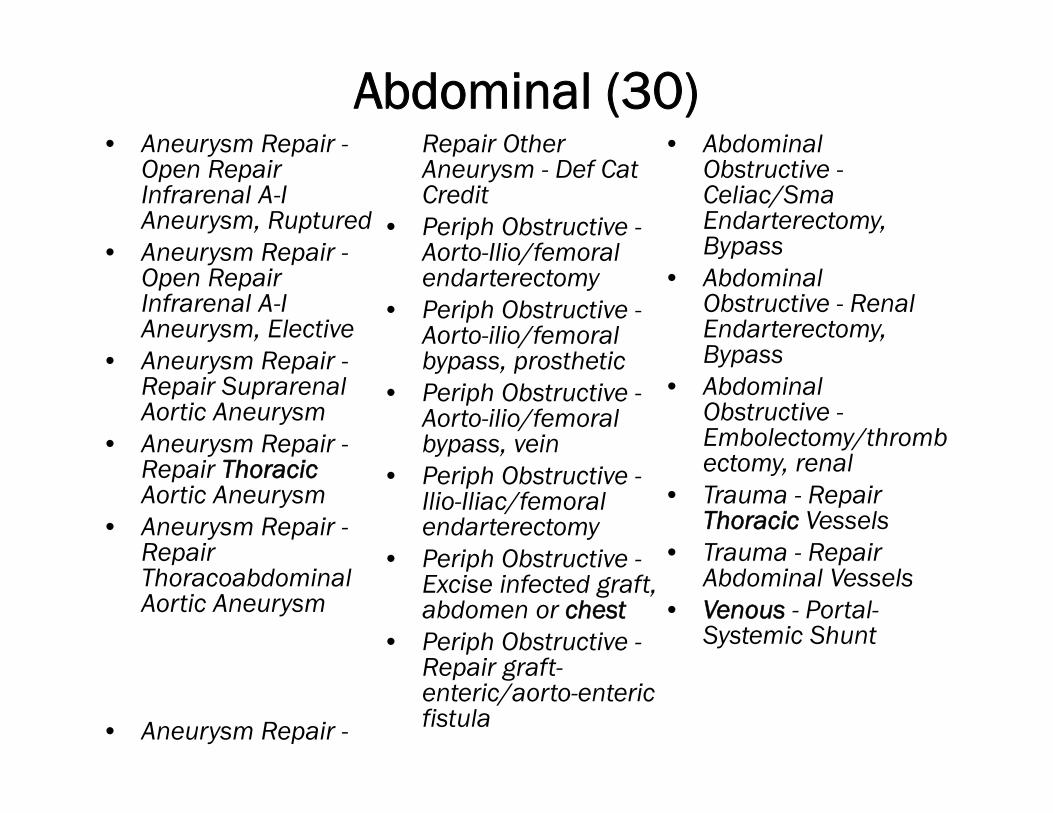
Abdominal (30) • Aneurysm Repair -
Open Repair Infrarenal A-I Aneurysm, Ruptured
• Aneurysm Repair -Open Repair Infrarenal A-I Aneurysm, Elective
• Aneurysm Repair -Repair Suprarenal Aortic Aneurysm
• Aneurysm Repair -Repair ThoracicAortic Aneurysm
• Aneurysm Repair -Repair ThoracoabdominalAortic Aneurysm
• Aneurysm Repair -
Repair Other Aneurysm - Def Cat Credit
• Periph Obstructive -Aorto-Ilio/femoral endarterectomy
• Periph Obstructive -Aorto-ilio/femoral bypass, prosthetic
• Periph Obstructive -Aorto-ilio/femoral bypass, vein
• Periph Obstructive -Ilio-Iliac/femoral endarterectomy
• Periph Obstructive -Excise infected graft, abdomen or chest
• Periph Obstructive -Repair graft-enteric/aorto-enteric fistula
• Abdominal Obstructive -Celiac/SmaEndarterectomy, Bypass
• Abdominal Obstructive - Renal Endarterectomy, Bypass
• Abdominal Obstructive -Embolectomy/thrombectomy, renal
• Trauma - Repair Thoracic Vessels
• Trauma - Repair Abdominal Vessels
• Venous - Portal-Systemic Shunt
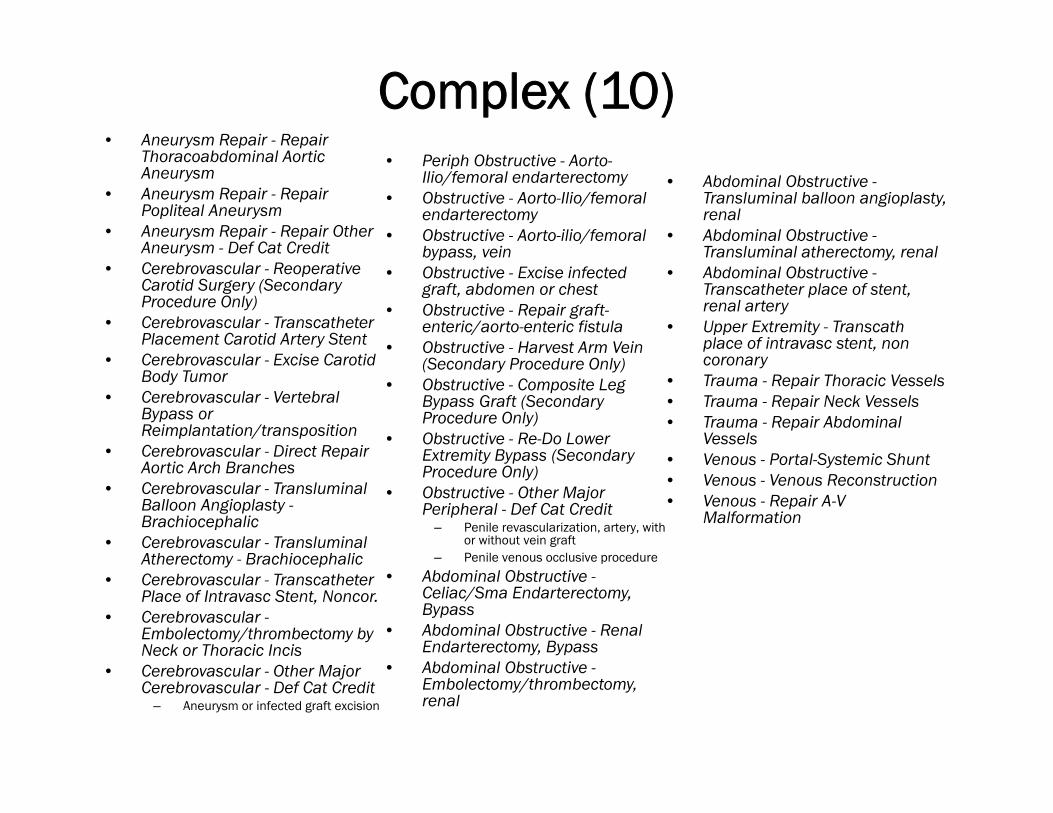
Complex (10) • Aneurysm Repair - Repair
Thoracoabdominal Aortic Aneurysm
• Aneurysm Repair - Repair Popliteal Aneurysm
• Aneurysm Repair - Repair Other Aneurysm - Def Cat Credit
• Cerebrovascular - ReoperativeCarotid Surgery (Secondary Procedure Only)
• Cerebrovascular - TranscatheterPlacement Carotid Artery Stent
• Cerebrovascular - Excise Carotid Body Tumor
• Cerebrovascular - Vertebral Bypass or Reimplantation/transposition
• Cerebrovascular - Direct Repair Aortic Arch Branches
• Cerebrovascular - TransluminalBalloon Angioplasty -Brachiocephalic
• Cerebrovascular - TransluminalAtherectomy - Brachiocephalic
• Cerebrovascular - TranscatheterPlace of Intravasc Stent, Noncor.
• Cerebrovascular -Embolectomy/thrombectomy by Neck or Thoracic Incis
• Cerebrovascular - Other Major Cerebrovascular - Def Cat Credit
– Aneurysm or infected graft excision
• Periph Obstructive - Aorto-Ilio/femoral endarterectomy
• Obstructive - Aorto-Ilio/femoral endarterectomy
• Obstructive - Aorto-ilio/femoral bypass, vein
• Obstructive - Excise infected graft, abdomen or chest
• Obstructive - Repair graft-enteric/aorto-enteric fistula
• Obstructive - Harvest Arm Vein (Secondary Procedure Only)
• Obstructive - Composite Leg Bypass Graft (Secondary Procedure Only)
• Obstructive - Re-Do Lower Extremity Bypass (Secondary Procedure Only)
• Obstructive - Other Major Peripheral - Def Cat Credit
– Penile revascularization, artery, with or without vein graft
– Penile venous occlusive procedure
• Abdominal Obstructive -Celiac/Sma Endarterectomy, Bypass
• Abdominal Obstructive - Renal Endarterectomy, Bypass
• Abdominal Obstructive -Embolectomy/thrombectomy, renal
• Abdominal Obstructive -Transluminal balloon angioplasty, renal
• Abdominal Obstructive -Transluminal atherectomy, renal
• Abdominal Obstructive -Transcatheter place of stent, renal artery
• Upper Extremity - Transcathplace of intravasc stent, non coronary
• Trauma - Repair Thoracic Vessels • Trauma - Repair Neck Vessels • Trauma - Repair Abdominal
Vessels • Venous - Portal-Systemic Shunt • Venous - Venous Reconstruction • Venous - Repair A-V
Malformation

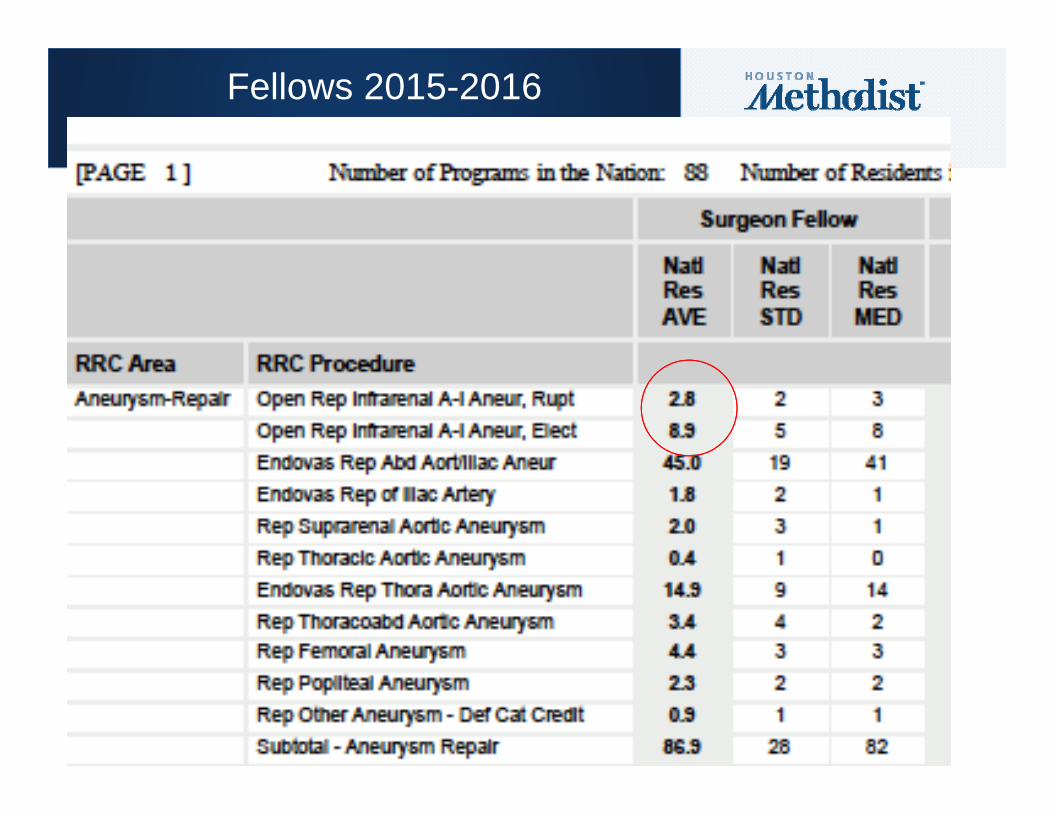
Fellows 2015-2016
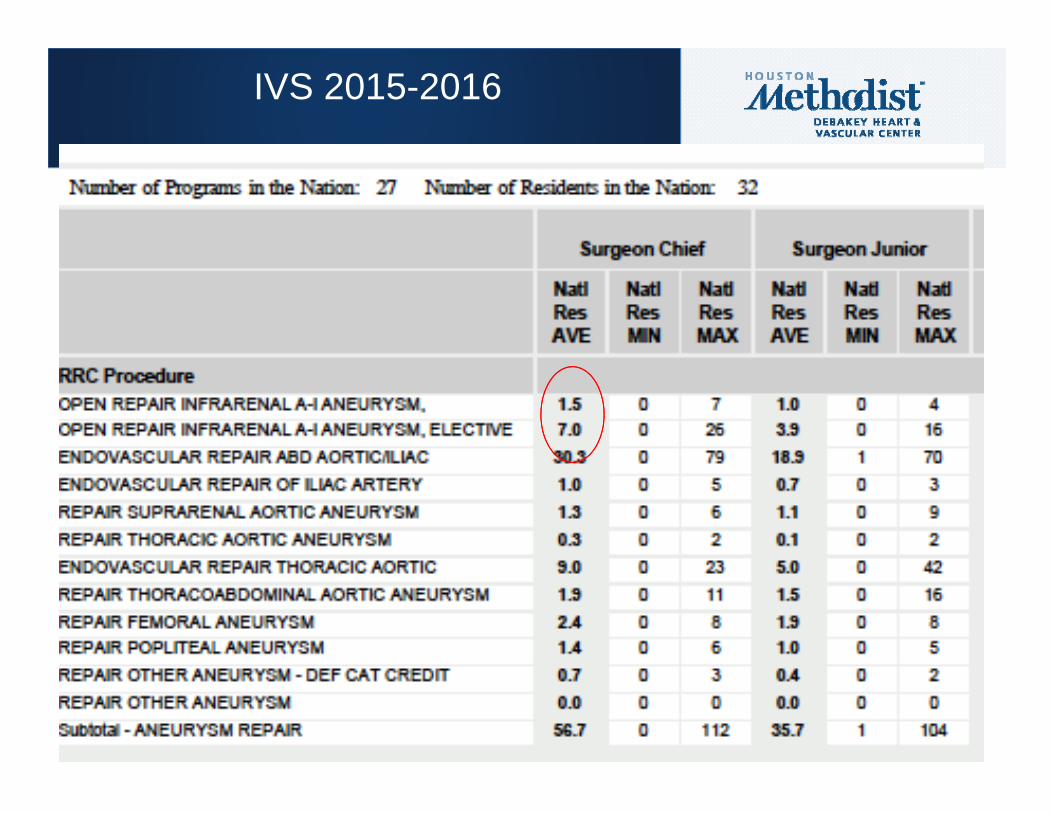
IVS 2015-2016
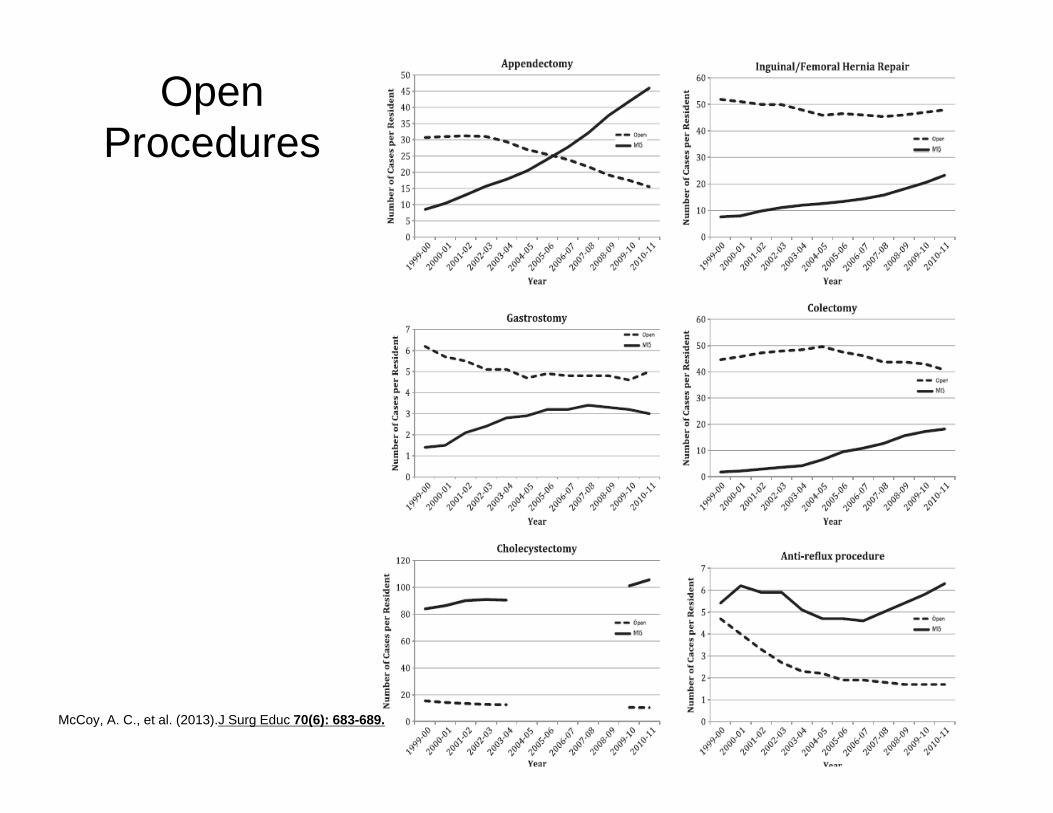
Open Procedures
McCoy, A. C., et al. (2013).J Surg Educ 70(6): 683-689.
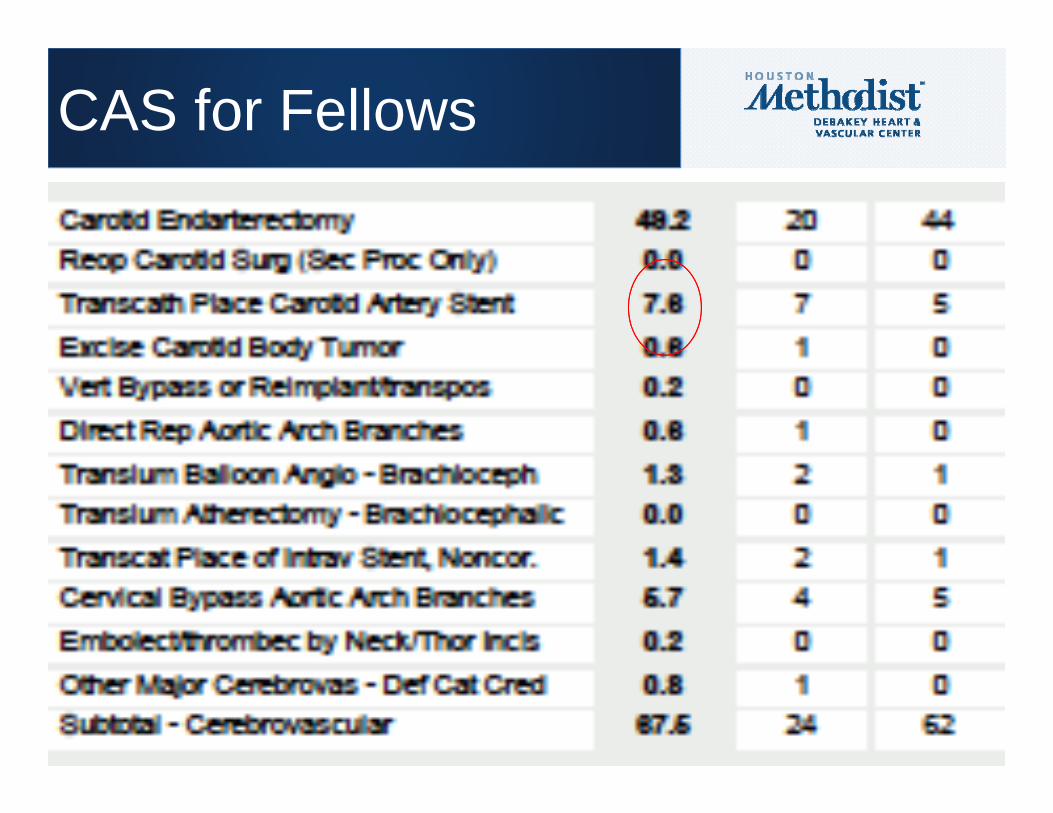
CAS for Fellows
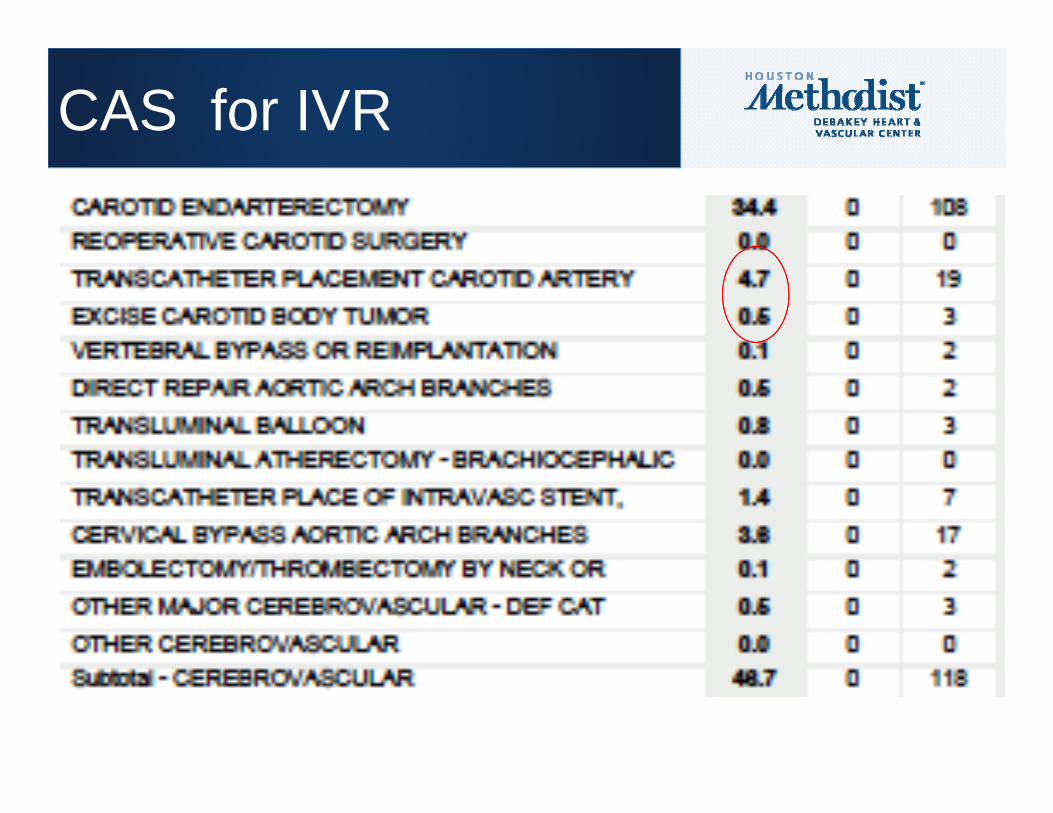
CAS for IVR

• 12 Questions FOCUSED ON– MINIMUN CASE LOGS– Core general surgery rotations
THE COMMITTEE CAME UP WITH
SURVEY SENT TO 180 PD’S45 RESPONDED (25%)

• We are not going to solve all these problems
• Have an understanding from other PD’s about their struggles
• Are some of the issues faced by all programs or few?– Case volume– General surgery experience
PURPOSE

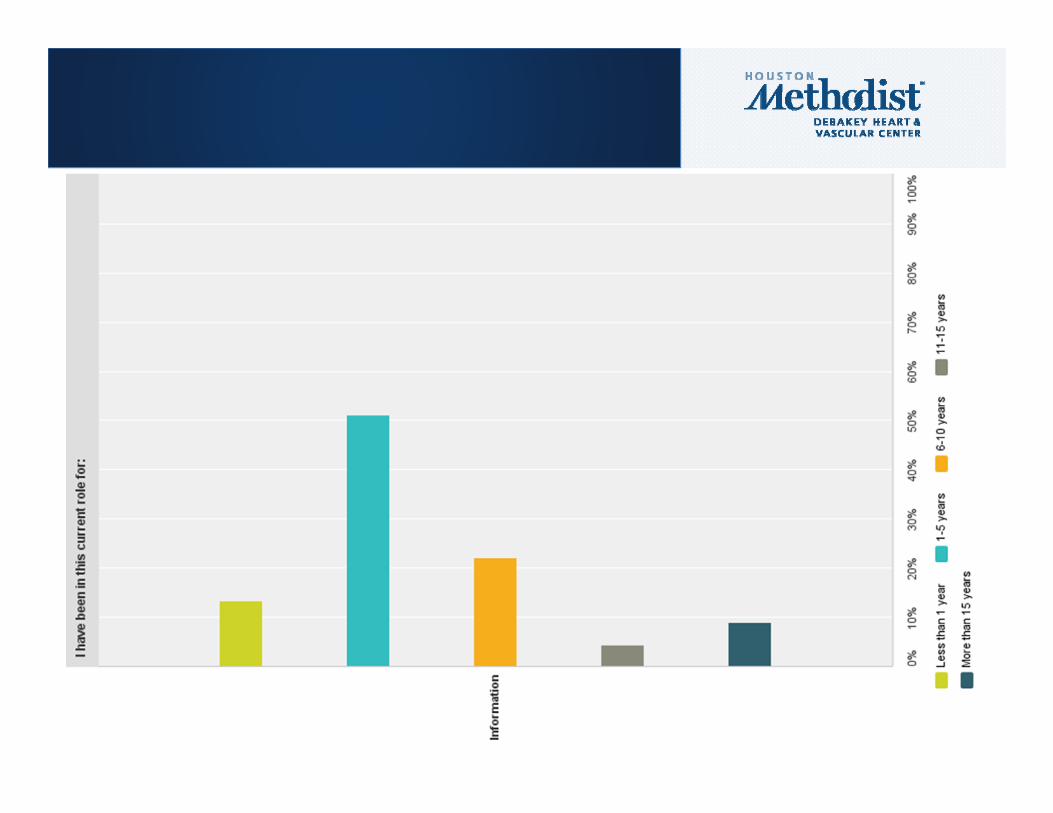
Q1 SPECIFY YOUR CURRENT DETAILS BELOW.ANSWERED: 45 SKIPPED: 0
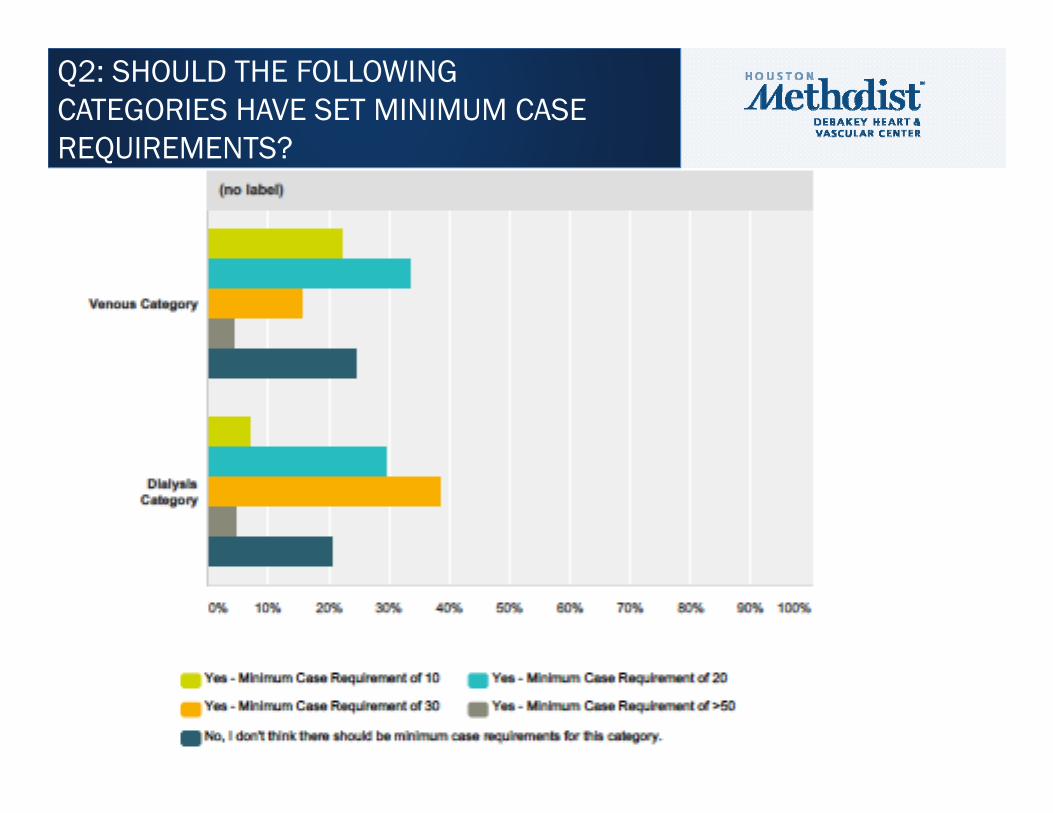
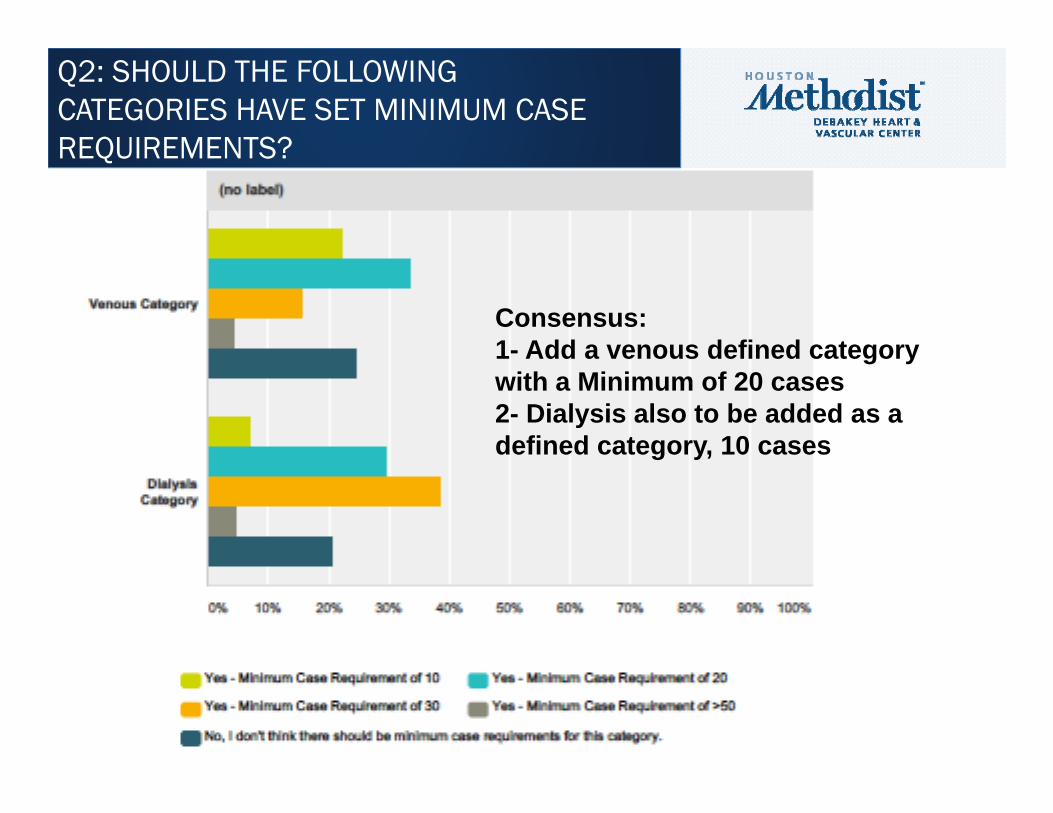
Q2: SHOULD THE FOLLOWING CATEGORIES HAVE SET MINIMUM CASE REQUIREMENTS?
Q2: SHOULD THE FOLLOWING CATEGORIES HAVE SET MINIMUM CASE REQUIREMENTS?
Consensus:1- Add a venous defined category with a Minimum of 20 cases 2- Dialysis also to be added as a defined category, 10 cases
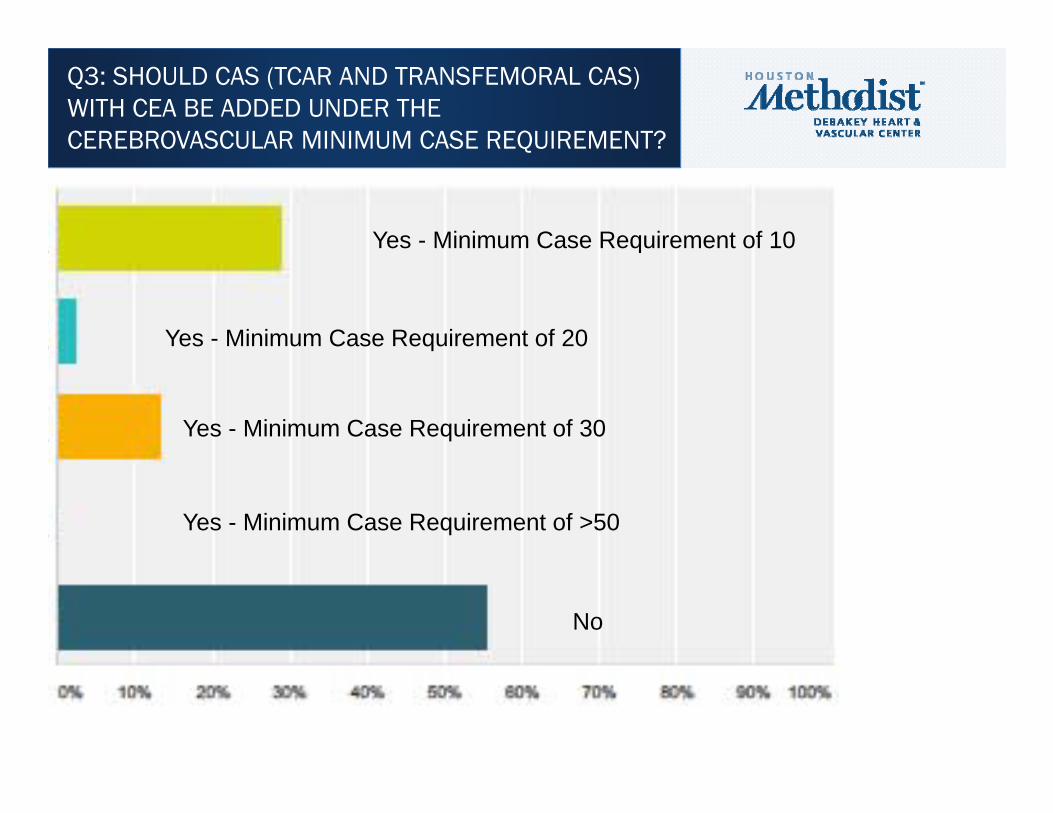
Q3: SHOULD CAS (TCAR AND TRANSFEMORAL CAS) WITH CEA BE ADDED UNDER THE CEREBROVASCULAR MINIMUM CASE REQUIREMENT?
Yes - Minimum Case Requirement of 10
Yes - Minimum Case Requirement of 20
Yes - Minimum Case Requirement of 30
Yes - Minimum Case Requirement of >50
No

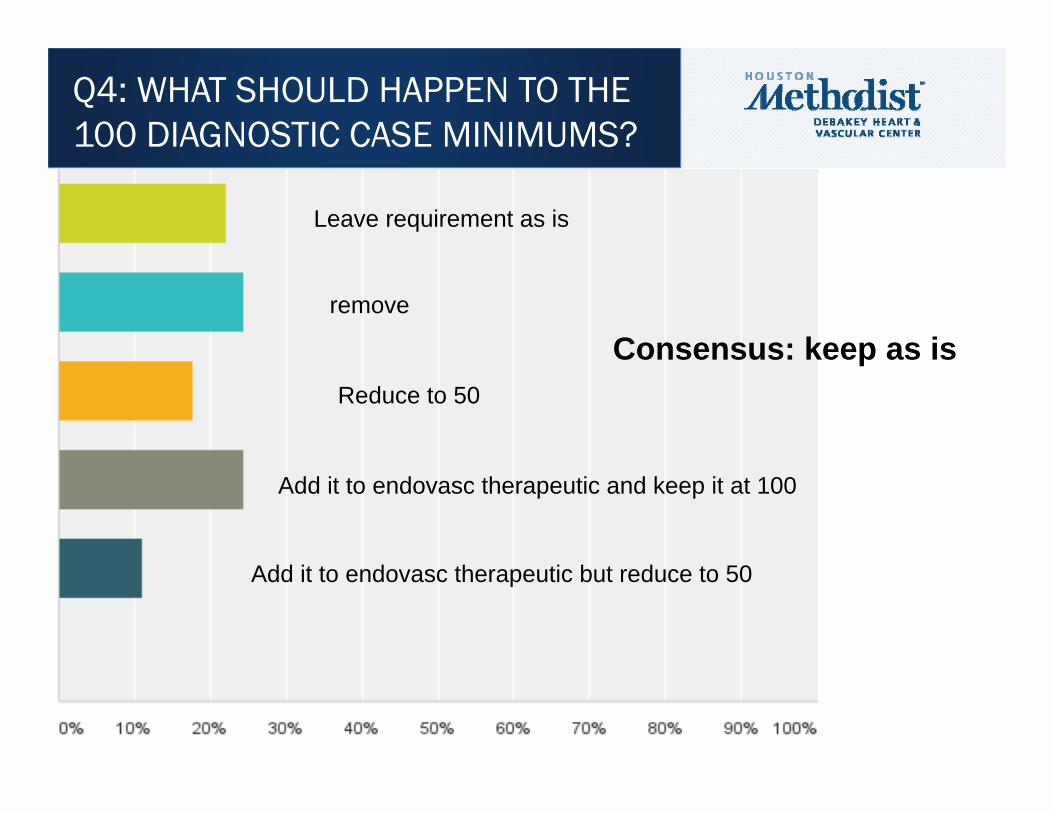
Q4: WHAT SHOULD HAPPEN TO THE 100 DIAGNOSTIC CASE MINIMUMS?
Leave requirement as is
remove
Reduce to 50
Add it to endovasc therapeutic and keep it at 100
Add it to endovasc therapeutic but reduce to 50
Q4: WHAT SHOULD HAPPEN TO THE 100 DIAGNOSTIC CASE MINIMUMS?
Leave requirement as is
remove
Reduce to 50
Add it to endovasc therapeutic and keep it at 100
Add it to endovasc therapeutic but reduce to 50
Consensus: keep as is
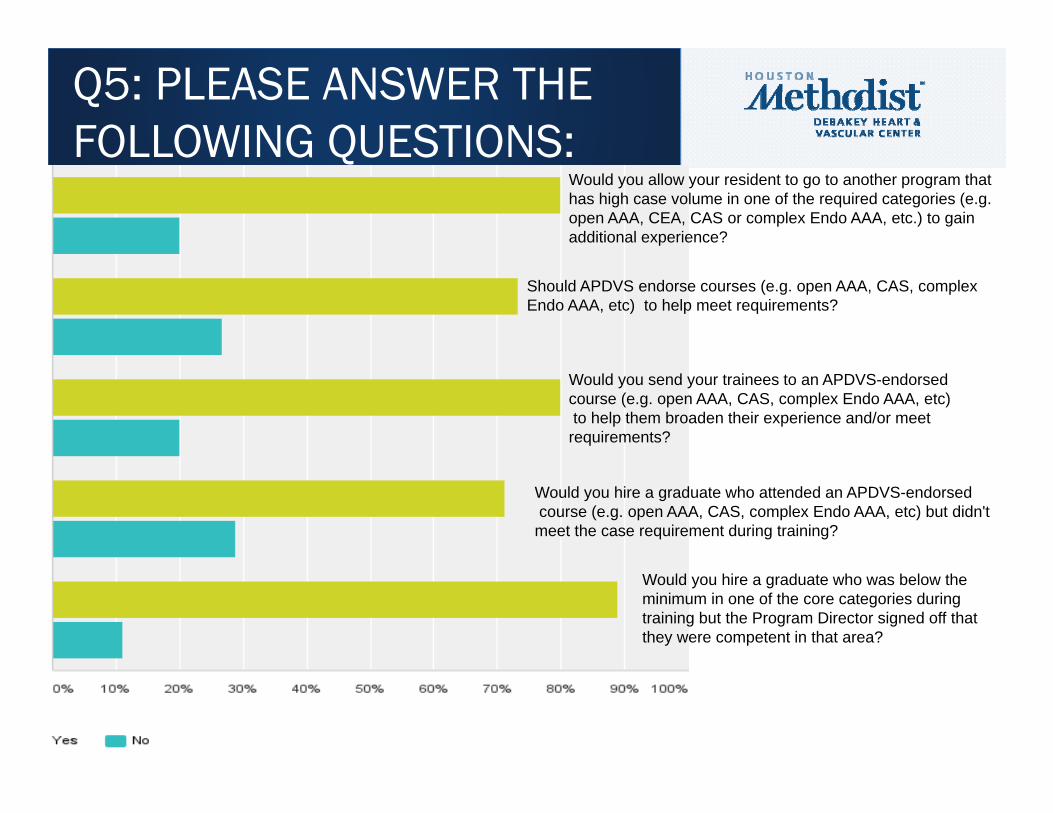
Q5: PLEASE ANSWER THE FOLLOWING QUESTIONS:
Would you allow your resident to go to another program that has high case volume in one of the required categories (e.g. open AAA, CEA, CAS or complex Endo AAA, etc.) to gain additional experience?
Should APDVS endorse courses (e.g. open AAA, CAS, complex Endo AAA, etc) to help meet requirements?
Would you send your trainees to an APDVS-endorsed course (e.g. open AAA, CAS, complex Endo AAA, etc)to help them broaden their experience and/or meet
requirements?
Would you hire a graduate who attended an APDVS-endorsedcourse (e.g. open AAA, CAS, complex Endo AAA, etc) but didn't
meet the case requirement during training?
Would you hire a graduate who was below the minimum in one of the core categories during training but the Program Director signed off that they were competent in that area?

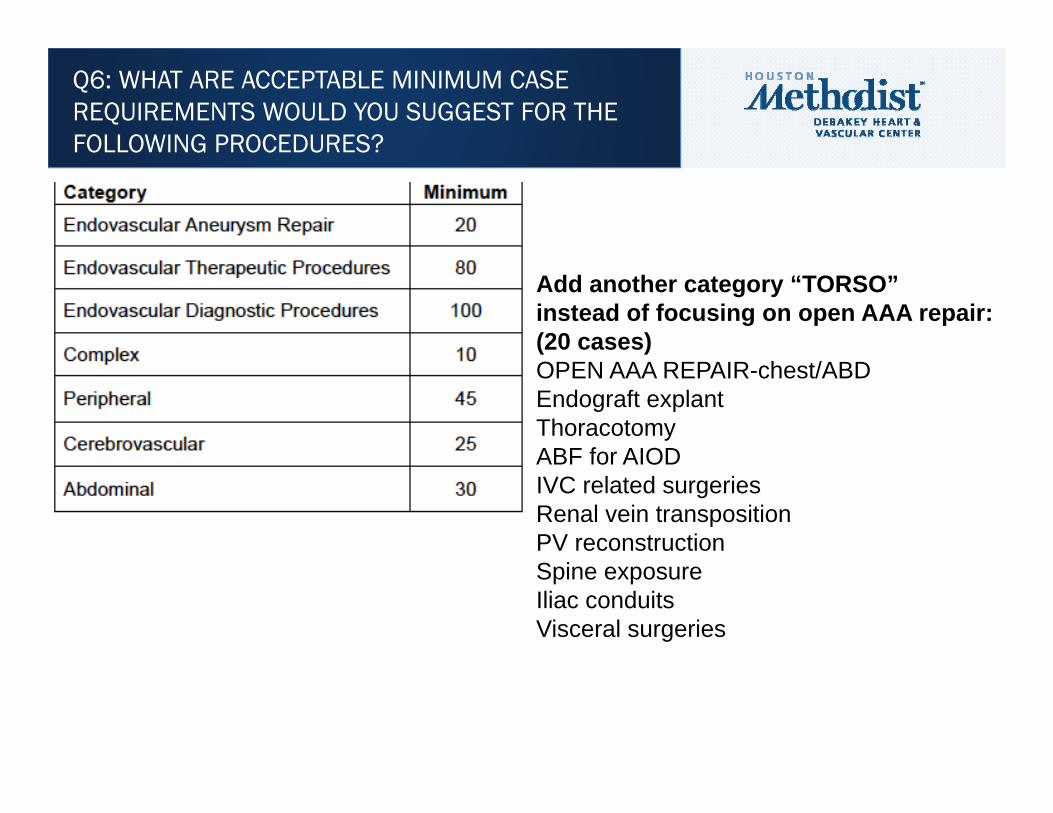
Q6: WHAT ARE ACCEPTABLE MINIMUM CASE REQUIREMENTS WOULD YOU SUGGEST FOR THE FOLLOWING PROCEDURES?
18
28
59
31
10
25
14
13
16

Q6: WHAT ARE ACCEPTABLE MINIMUM CASE REQUIREMENTS WOULD YOU SUGGEST FOR THE FOLLOWING PROCEDURES?
18
28
59
31
10
25
14
13
16
Q6: WHAT ARE ACCEPTABLE MINIMUM CASE REQUIREMENTS WOULD YOU SUGGEST FOR THE FOLLOWING PROCEDURES?
Add another category “TORSO” instead of focusing on open AAA repair:(20 cases)OPEN AAA REPAIR-chest/ABDEndograft explantThoracotomyABF for AIODIVC related surgeriesRenal vein transpositionPV reconstructionSpine exposureIliac conduitsVisceral surgeries

Q6: WHAT ARE ACCEPTABLE MINIMUM CASE REQUIREMENTS WOULD YOU SUGGEST FOR THE FOLLOWING PROCEDURES?
Add another category “TORSO” instead of focusing on open AAA repair:(20 cases)OPEN AAA REPAIR-chest/ABDEndograft explantThoracotomyABF for AIODIVC related surgeriesRenal vein transpositionPV reconstructionSpine exposureIliac conduitsVisceral surgeries
Might as well add another category for complex endo AAA repair, 10 cases
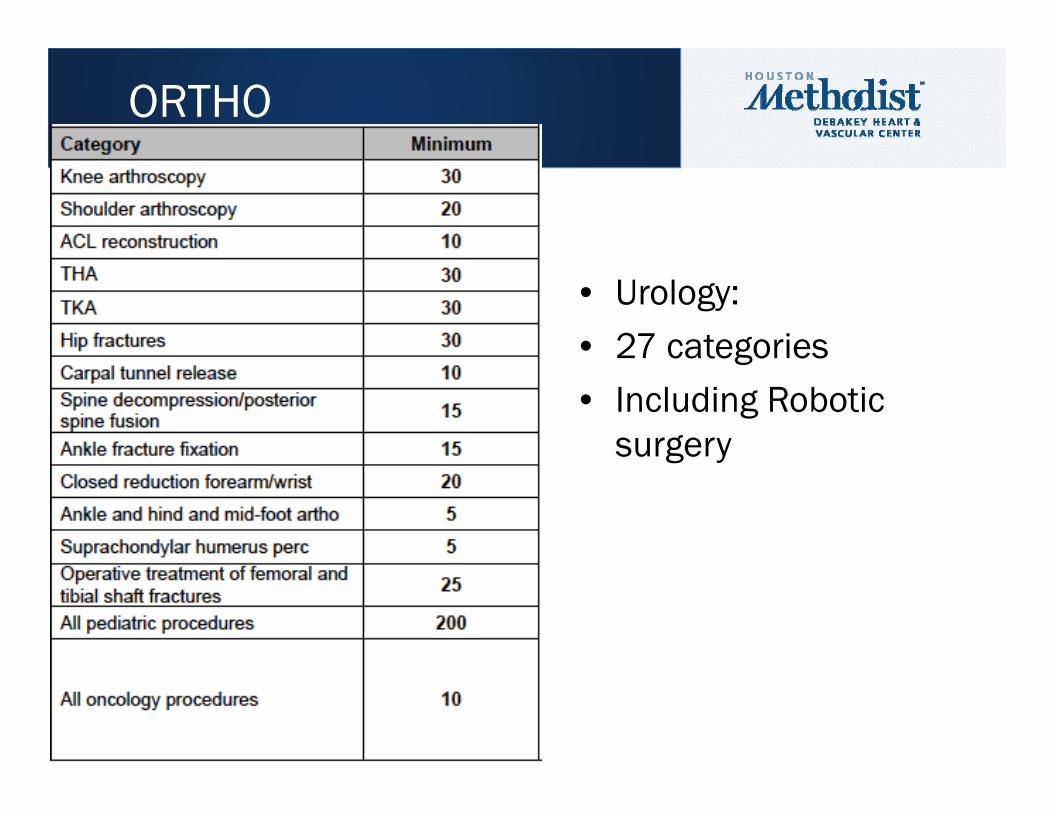
• Urology: • 27 categories• Including Robotic
surgery
ORTHO

Q9: HOW LONG DO YOU FEEL GENERAL SURGERY CORE ROTATION REQUIREMENTS SHOULD BE FOR VASCULAR SURGERY INTEGRATED RESIDENTS?
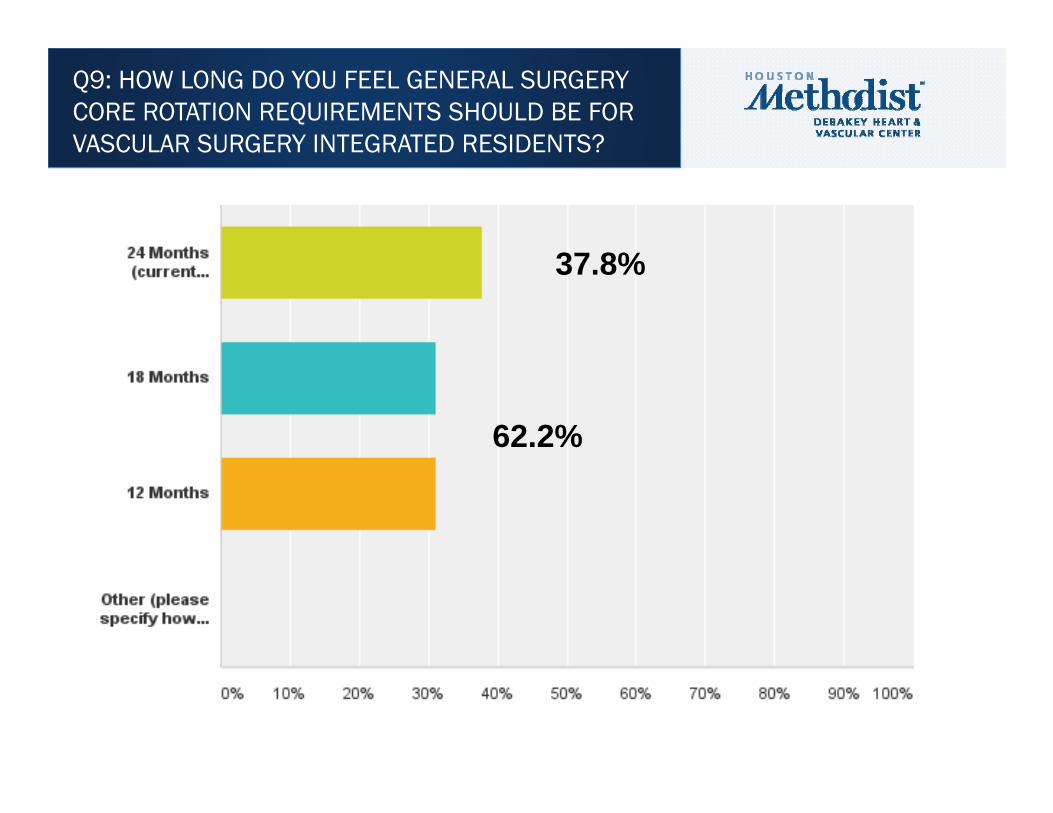
Q9: HOW LONG DO YOU FEEL GENERAL SURGERY CORE ROTATION REQUIREMENTS SHOULD BE FOR VASCULAR SURGERY INTEGRATED RESIDENTS?
37.8%
62.2%
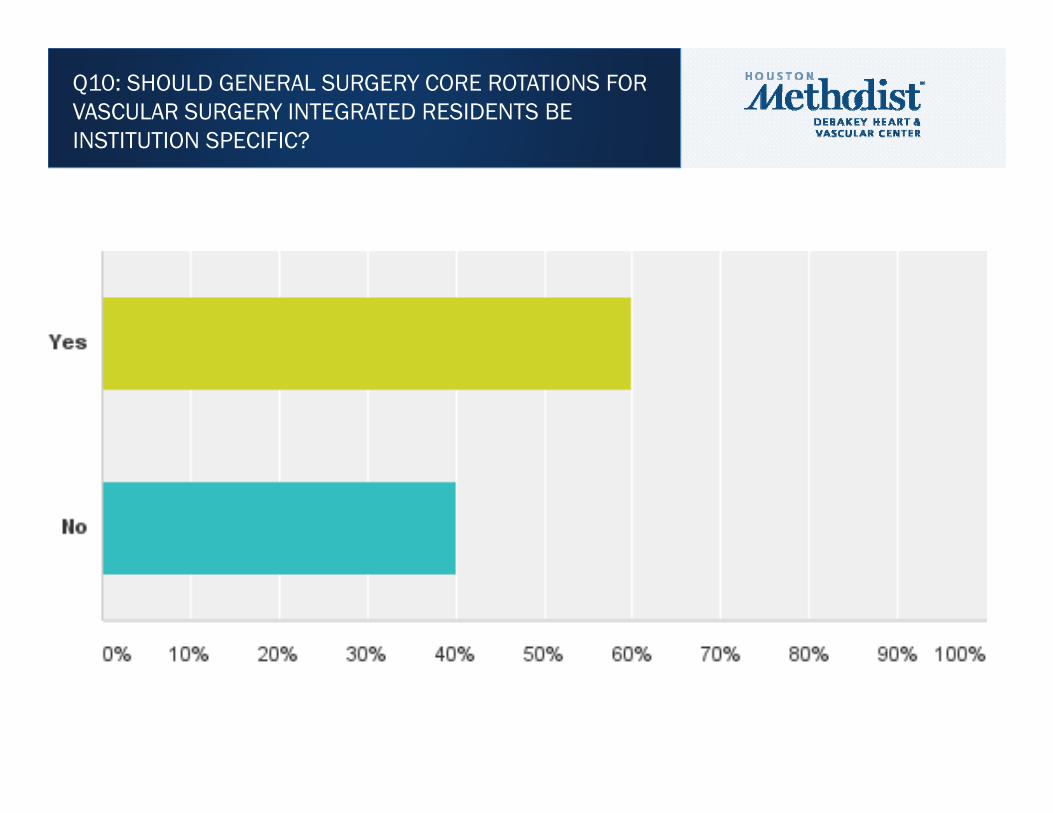
Q10: SHOULD GENERAL SURGERY CORE ROTATIONS FOR VASCULAR SURGERY INTEGRATED RESIDENTS BE INSTITUTION SPECIFIC?
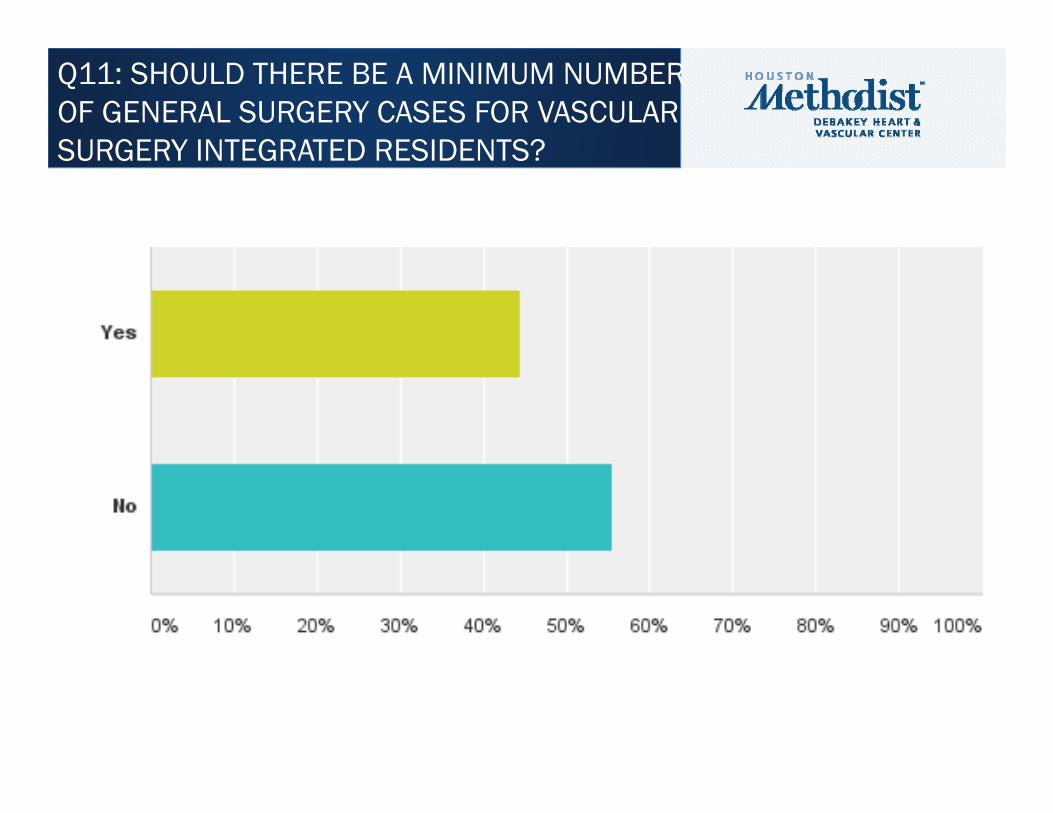
Q11: SHOULD THERE BE A MINIMUM NUMBER OF GENERAL SURGERY CASES FOR VASCULAR SURGERY INTEGRATED RESIDENTS?
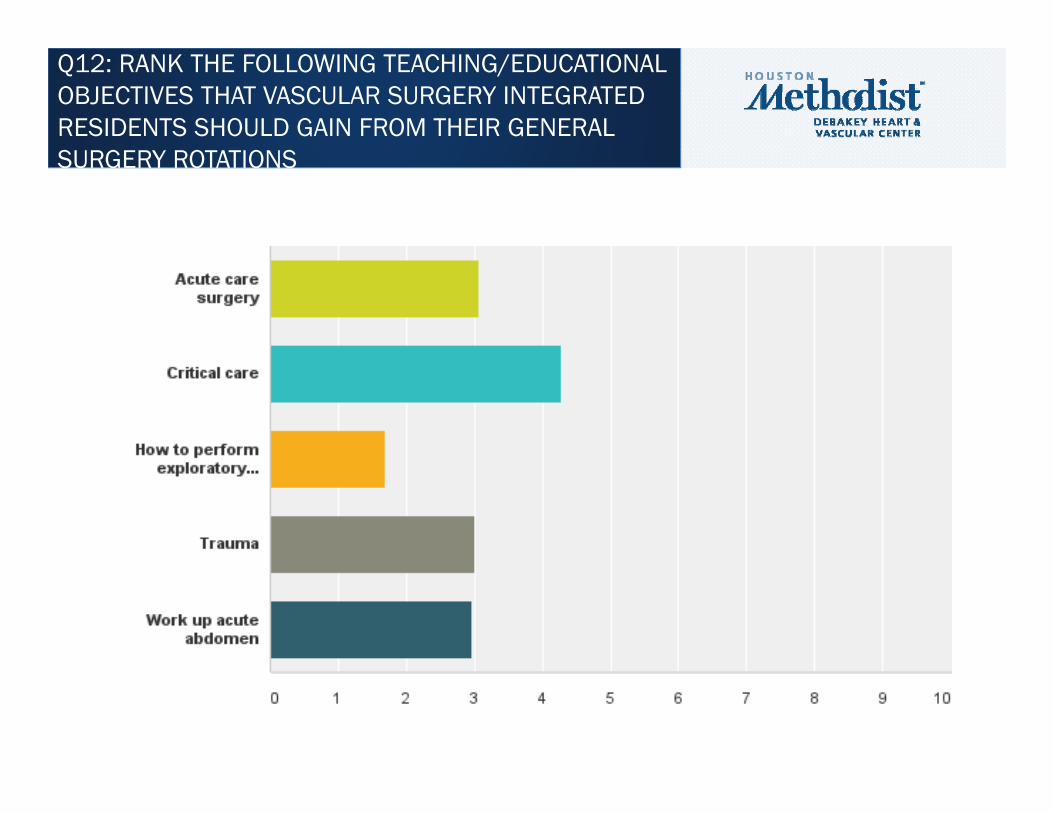
Q12: RANK THE FOLLOWING TEACHING/EDUCATIONAL OBJECTIVES THAT VASCULAR SURGERY INTEGRATED RESIDENTS SHOULD GAIN FROM THEIR GENERAL SURGERY ROTATIONS
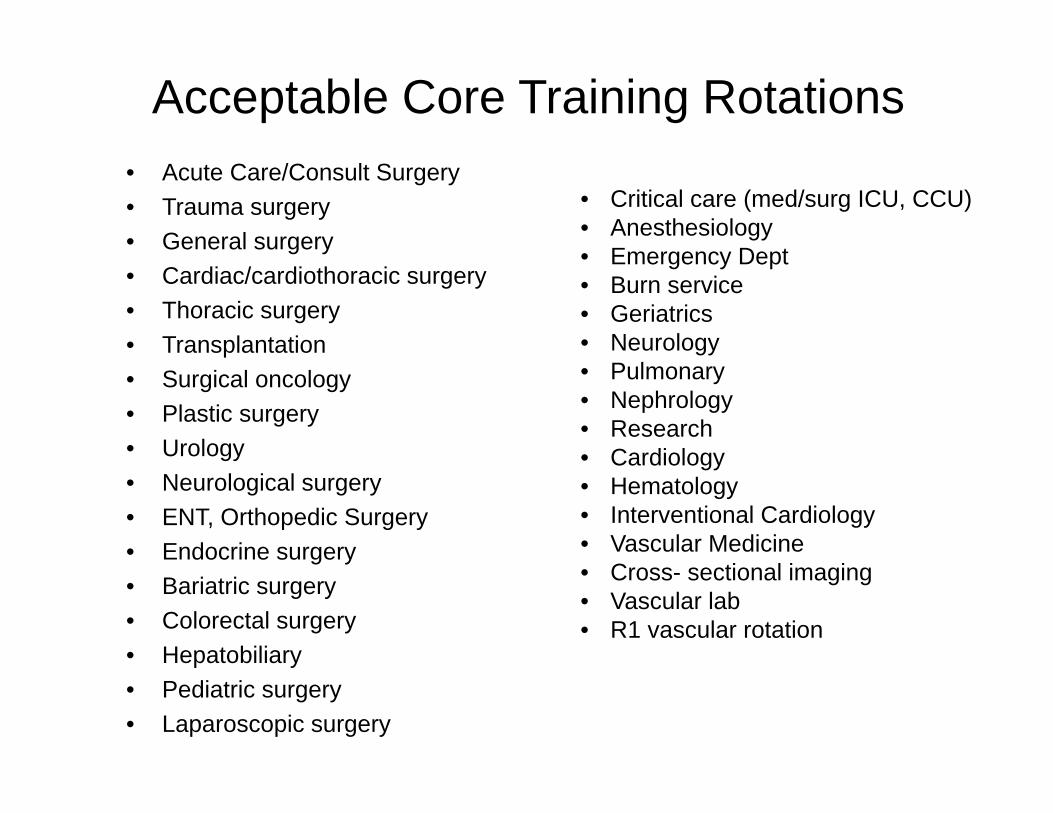
Acceptable Core Training Rotations• Acute Care/Consult Surgery• Trauma surgery• General surgery• Cardiac/cardiothoracic surgery• Thoracic surgery• Transplantation• Surgical oncology • Plastic surgery• Urology• Neurological surgery• ENT, Orthopedic Surgery• Endocrine surgery• Bariatric surgery• Colorectal surgery• Hepatobiliary• Pediatric surgery • Laparoscopic surgery
• Critical care (med/surg ICU, CCU)• Anesthesiology• Emergency Dept• Burn service• Geriatrics• Neurology• Pulmonary• Nephrology• Research• Cardiology• Hematology• Interventional Cardiology• Vascular Medicine• Cross- sectional imaging• Vascular lab• R1 vascular rotation

Acceptable Core Training Rotations• Acute Care/Consult Surgery• Trauma surgery• General surgery• Cardiac/cardiothoracic surgery• Thoracic surgery• Transplantation• Surgical oncology • Plastic surgery• Urology• Neurological surgery• ENT, Orthopedic Surgery• Endocrine surgery• Bariatric surgery• Colorectal surgery• Hepatobiliary• Pediatric surgery • Laparoscopic surgery
• Critical care (med/surg ICU, CCU)• Anesthesiology• Emergency Dept• Burn service• Geriatrics• Neurology• Pulmonary• Nephrology• Research• Cardiology• Hematology• Interventional Cardiology• Vascular Medicine• Cross- sectional imaging• Vascular lab• R1 vascular rotation
No podiatry

• Make core rotations 18 months.• Keep Vascular rotations at least 36 months• Remaining 6 months up to the discretion of the PD
– Institution specific– Emphasis on critical care, trauma and acute care surgery– Can be vascular– Allow for electives
• No minimum case requirement for core rotations
CONSENSUS

UROLOGY
The ABU mandates a minimum of five clinical years of postgraduate medical training. The training must include:
48 months in an ACGME-approved urology programThree months of general surgery in an ACGME-approved surgical programThree months of core surgical training (e.g., intensive care unit, trauma, vascular surgery, cardiac surgery, etc.) in an ACGME-approved surgical programSix months of other rotations, not including dedicated research time, in an ACGME- or RCPS(C)-approved core surgery program
ORTHOPEDICS
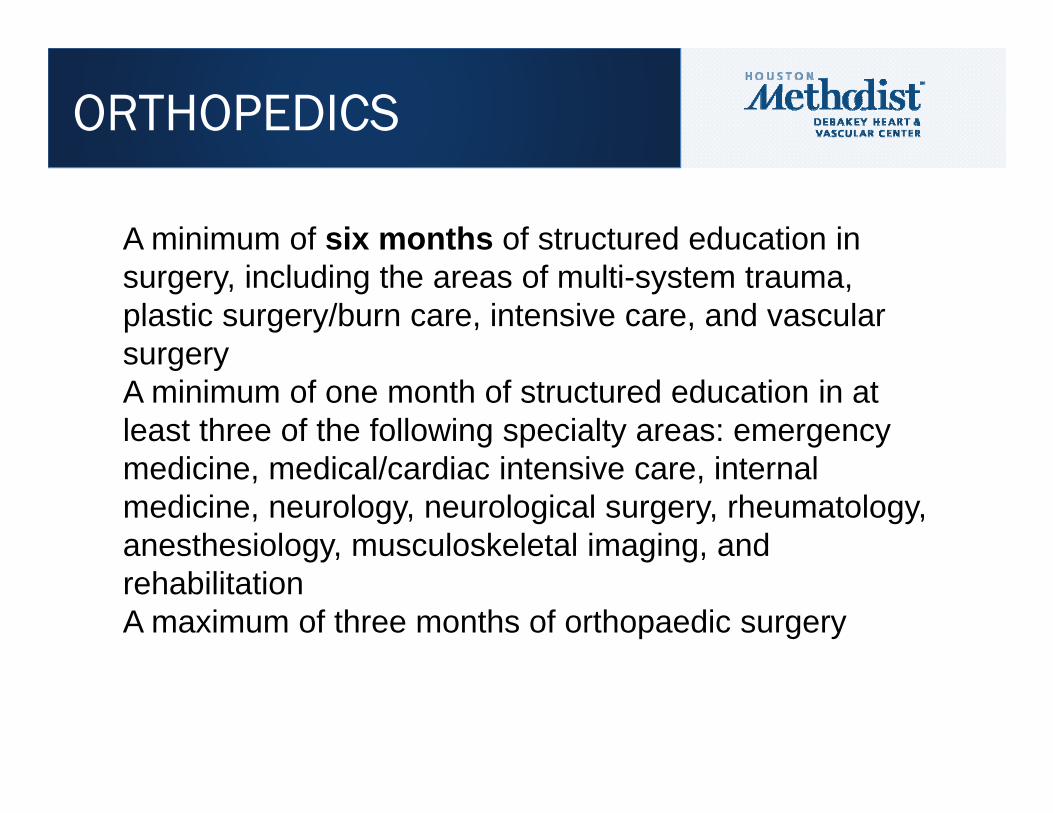
A minimum of six months of structured education in surgery, including the areas of multi-system trauma, plastic surgery/burn care, intensive care, and vascular surgeryA minimum of one month of structured education in at least three of the following specialty areas: emergency medicine, medical/cardiac intensive care, internal medicine, neurology, neurological surgery, rheumatology, anesthesiology, musculoskeletal imaging, and rehabilitationA maximum of three months of orthopaedic surgery
NEUROSURGERY
As of July 1, 2009, the training program in neurological surgery no longer requires a prerequisite year of general surgery.
The neurological surgery training program is at least 72 months in duration. Programs can be approved for up to 84 months of training: 72 months for clinical and didactic education and 12 months for research or subspecialty training.

THANK YOU



• We have a problem with open exposure– Abd exploration/LOA– Open AAA repair
• What is the solution?– Simulation– Courses– Electives at high volume centers– Outside the US
• Role of APDVS• Credentialing• Rollover cases from GS?
CONCLUSION