Embed Size (px)
Citation preview
CASE REPORT
Acute short radiolunate ligament rupture in a rock climber
Eric Y. Chang & Karen C. Chen & Matthew J. Meunier &
Christine B. Chung
Received: 18 July 2013 /Revised: 8 August 2013 /Accepted: 11 August 2013 /Published online: 5 September 2013# ISS (outside the USA) 2013
Abstract We report the occurrence of a short radiolunateligament rupture in a rock climber. To our knowledge, anisolated traumatic rupture of this ligament has not been de-scribed in the literature, and awareness of this entity allowsinitiation of therapy. The magnetic resonance imaging andultrasound appearances are reviewed and the mechanism ofinjury is discussed.
Keywords Extrinsic wrist ligaments . Short radiolunateligament tear . Rock climbing
Introduction
Rock climbing is an increasingly popular sport. Injuries thatare seen in rock climbers typically involve the hand and wrist
[1]. In particular, pulley injuries are well known, most com-monly due to overloading in the “closed crimp” grip position,where the proximal interphalangeal joint is flexed to 90° ormore with extension or hyperextension of the distalinterphalangeal joint [2]. Other common rock climbing grippositions include the open crimp, open grip, and pinch grippositions [3]. Another common hold that is less well known tothe non-climbing community is the “sloper” hold. Sloperholds vary in diameter, but common to all sloper holds is thereliance on friction over a large surface area in an open-handposition to maintain grip. The hand position on a sloper hold issimilar to “palming” a basketball (Fig. 1). To our knowledge,we report the first case of an acute short radiolunate ligament(SRL) tear in a rock climber and review the mechanism ofinjury.
Case report
A 34-year-old experienced rock climber was actively grippingwith both hands on a large “sloper” hold when his feet lostcontact with the rock-climbing wall. He noted a suddenpulling sensation within his right wrist and felt as if his,“forearm and wrist slightly separated.” After a week of rest,he resumed activities, but felt persistent instability with tensileforce across the wrist. Notably, the subjective instability im-proved with a full clenched grip position. The patient soughtmedical attention and physical exam demonstrated a positivemidcarpal shift test with a catch-up clunk [4]. The anteriordrawer test also demonstrated a notable clunk. Scapholunateand lunotriquetral instability tests were negative.
Magnetic resonance imaging (MRI) was performed in threeorthogonal planes, which included T2-weighted sequences(repetition time 3,000 ms, echo time 65 ms, 2.5-mm slicethickness, 2-mm inter-slice gap, matrix 384×308). This dem-onstrated an acutely torn SRL characterized by indistinct
E. Y. Chang :K. C. Chen :C. B. ChungDepartment of Radiology, VA San Diego Healthcare System, 3350La Jolla Village Drive, San Diego, CA 92161, USA
K. C. Chene-mail: [email protected]
C. B. Chunge-mail: [email protected]
E. Y. Chang :K. C. Chen :C. B. ChungDepartment of Radiology, University of California, San DiegoMedical Center, 200 West Arbor Drive, San Diego, CA 92103, USA
M. J. MeunierDepartment of Orthopedic Surgery, University of California,San Diego Medical Center, 200 West Arbor Drive,San Diego, CA 92103, USAe-mail: [email protected]
E. Y. Chang (*)3350 La Jolla Village Drive, MC 114, San Diego, CA 92161, USAe-mail: [email protected]
Skeletal Radiol (2014) 43:235–238DOI 10.1007/s00256-013-1717-1

margins of the ligament, increased intrasubstance signal in-tensity, discontinuous edges of ligament, and surroundingedema (Fig. 2a, b and c). The other palmar extrinsic ligamentswere normally intact, including the radioscaphocapitate(RSC) and long radiolunate (LRL) ligaments. The dorsalextrinsic and intrinsic ligaments, including the scapholunateand lunotriquetral interosseous ligaments, were intact. The tri-angular fibrocartilage complex, including the ulnolunate andulnotriquetral ligaments, was intact. Due to the unusual natureof this injury, the contralateral, asymptomatic wrist was alsoimaged utilizing the same imaging parameters, which demon-strated an intact SRL, but with mildly increased intrasubstance
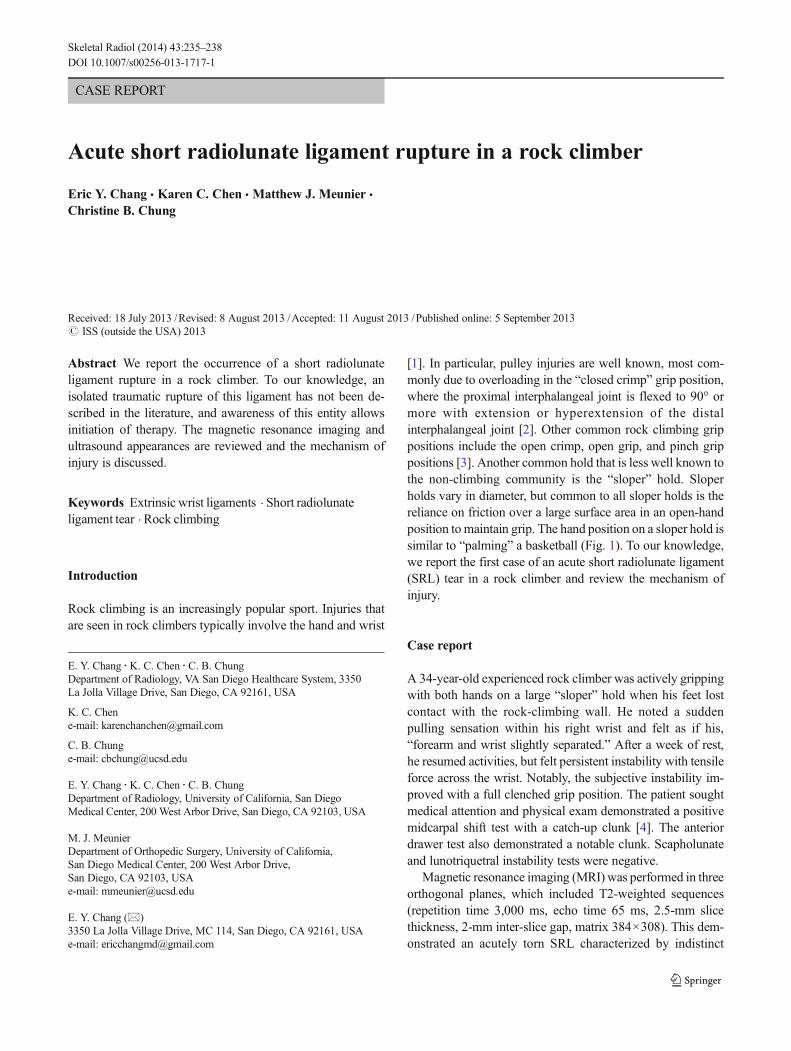
signal and trace surrounding edema suggesting previous injury(Fig. 2d, e and f). With an 18-MHz linear transducer and thewrists in slight extension, targeted ultrasound was alsoperformed, demonstrating the same findings as the MRI(Fig. 3). Conservative management was recommended,consisting of 4weeks of splinting, followed by physical therapy.
Discussion
The short radiolunate ligament (SRL) is an intracapsular,extrasynovial extrinsic ligament of the wrist, which was onlyfirst described in the orthopedic literature in 1990 [5]. Itoriginates just palmar to the lunate facet of the distal radialarticular surface and inserts into the proximal margin of thepalmar surface of the lunate [5]. There is a paucity of literaturedescribing traumatic abnormalities of this ligament [6, 7].Most typically, injury to the SRL occurs in association withsignificant surrounding ligamentous injury such as in aperilunate or lunate dislocation after a fall onto an outstretchedhand. In patients with inflammatory arthritis, extensivedamage to the volar radiocarpal ligaments causes ulnartranslocation of the carpus. To our knowledge, we presentthe first case of an acute SRL rupture in the literature.
Rock climbers place high demands on their wrists, hands,and fingers, which create unique injuries. In particular, indoorrock climbing allows for repetition of difficult climbs in quick
Fig. 1 Diagram of typical “sloper” hold (a) and picture of the open-handposition required to “palm” the rock climbing hold (b). Courtesy of MarkMatuszewski
Fig. 2 MR images of the symptomatic right wrist (a , b , c) and asymp-tomatic left wrist (d , e , f). Sagittal (a), coronal (b), and axial (c) T2-weighted MR images (TR 3,000 ms/TE 65 ms) show an indistinct shortradiolunate ligament with discontinuous, torn edges (short thin arrows)as well as fluid and edema tracking proximally (dashed arrows). Sagittal(d), coronal (e), and axial (f) T2-weighted MR images (TR 3,000 ms/TE65 ms) of the asymptomatic left wrist show an intact short radiolunateligament (block arrow), but with increased signal intensity compared
with the triquetrohamocapitate ligament (arrowhead) and trace surround-ing edema. Other extrinsic and intrinsic ligaments were carefully con-firmed through all imaging planes to be intact. Radioscaphocapitate(RSC) and long radiolunate (LRL) ligaments were intact, but volumeaveraging caused increased signal intensity on coronal images (b and e).Triquetrohamocapitate (THC), scaphocapitate (SC), and palmarscaphotriquetral (PST) ligaments were intact and well visualized on allimaging planes. Multiple tiny ganglion cysts were incidentally noted
236 Skeletal Radiol (2014) 43:235–238
succession. This approach causes strain and fatigue on mus-culoskeletal structures such as ligaments and tendons. Themechanism of injury in this case involved a tensile forceacross the wrist, which was dynamically loaded when theclimber lost his footing. With most other rock climbing grips,the flexor and extensor tendons across the wrist are moreengaged, acting to supplement and protect the passive wristligaments. However, unique to this case was the use of the“sloper” hold, which engages the dynamic stabilizers to amuch lesser degree. Rather, climbers rely mainly on frictionover a large surface area to grip a “sloper” hold, which can be
sufficient to hold forces greater than bodyweight. In thiscase, as the climber was falling, the tensile force exceededthe capability of the SRL, causing a tear. Fortunately, theforce was insufficient to tear the other extrinsic radiocarpalligaments.
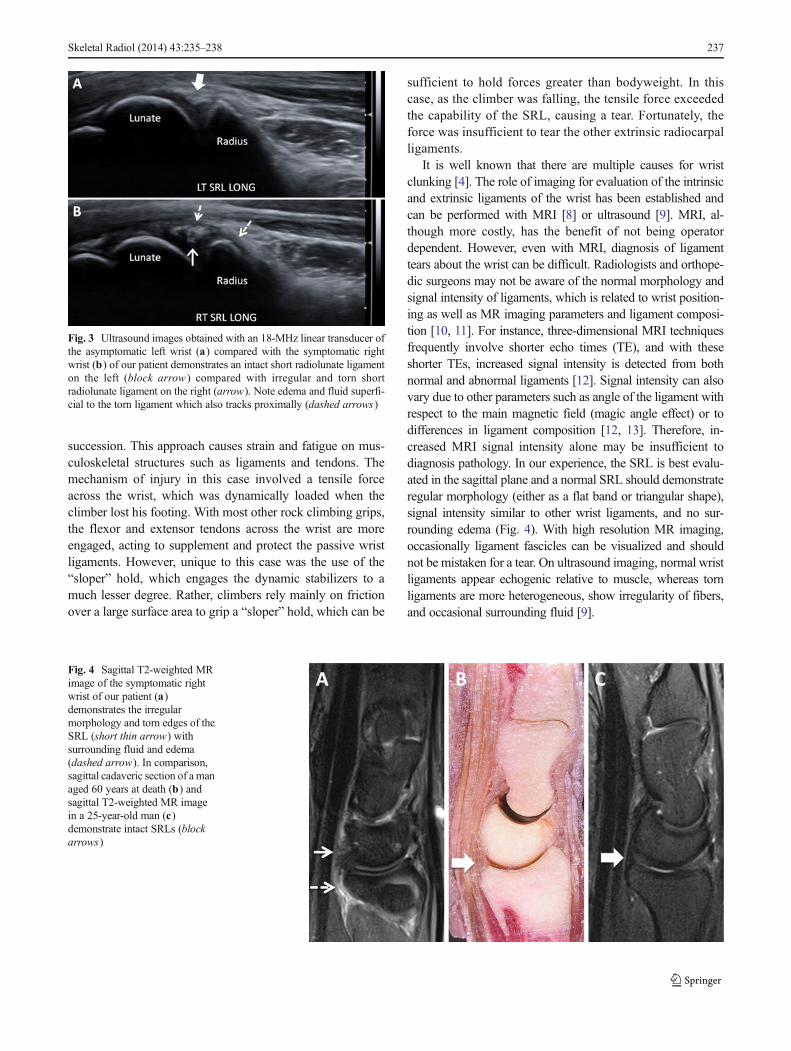
It is well known that there are multiple causes for wristclunking [4]. The role of imaging for evaluation of the intrinsicand extrinsic ligaments of the wrist has been established andcan be performed with MRI [8] or ultrasound [9]. MRI, al-though more costly, has the benefit of not being operatordependent. However, even with MRI, diagnosis of ligamenttears about the wrist can be difficult. Radiologists and orthope-dic surgeons may not be aware of the normal morphology andsignal intensity of ligaments, which is related to wrist position-ing as well as MR imaging parameters and ligament composi-tion [10, 11]. For instance, three-dimensional MRI techniquesfrequently involve shorter echo times (TE), and with theseshorter TEs, increased signal intensity is detected from bothnormal and abnormal ligaments [12]. Signal intensity can alsovary due to other parameters such as angle of the ligament withrespect to the main magnetic field (magic angle effect) or todifferences in ligament composition [12, 13]. Therefore, in-creased MRI signal intensity alone may be insufficient todiagnosis pathology. In our experience, the SRL is best evalu-ated in the sagittal plane and a normal SRL should demonstrateregular morphology (either as a flat band or triangular shape),signal intensity similar to other wrist ligaments, and no sur-rounding edema (Fig. 4). With high resolution MR imaging,occasionally ligament fascicles can be visualized and shouldnot be mistaken for a tear. On ultrasound imaging, normal wristligaments appear echogenic relative to muscle, whereas tornligaments are more heterogeneous, show irregularity of fibers,and occasional surrounding fluid [9].
Fig. 4 Sagittal T2-weighted MRimage of the symptomatic rightwrist of our patient (a)demonstrates the irregularmorphology and torn edges of theSRL (short thin arrow) withsurrounding fluid and edema(dashed arrow). In comparison,sagittal cadaveric section of a managed 60 years at death (b) andsagittal T2-weighted MR imagein a 25-year-old man (c)demonstrate intact SRLs (blockarrows)
Fig. 3 Ultrasound images obtained with an 18-MHz linear transducer ofthe asymptomatic left wrist (a) compared with the symptomatic rightwrist (b) of our patient demonstrates an intact short radiolunate ligamenton the left (block arrow ) compared with irregular and torn shortradiolunate ligament on the right (arrow). Note edema and fluid superfi-cial to the torn ligament which also tracks proximally (dashed arrows)
Skeletal Radiol (2014) 43:235–238 237

In conclusion, this case highlights a unique injury incurredwhile rock climbing, an increasingly popular sport. We feelthat knowledge of this injury is important for diagnosis, whichcan be readily made on MRI or a targeted ultrasound. Thisallows initiation of therapy to prevent further injury to theremaining palmar extrinsic ligaments.
Acknowledgement of funding Eric Y. Chang acknowledges salarysupport from the Veterans Affairs (Career Development Award:1IK2CX000749-01)
Conflict of interest None
References
1. Logan AJ, Makwana N, Mason G, Dias J. Acute hand and wristinjuries in experienced rock climbers. Br J Sports Med. 2004;38(5):545–8.
2. Schweizer A. Biomechanical properties of the crimp grip position inrock climbers. J Biomech. 2001;34(2):217–23.
3. Kubiak EN, Klugman JA, Bosco JA. Hand injuries in rock climbers.Bull NYU Hosp Jt Dis. 2006;64(3–4):172–7.
4. Feinstein WK, Lichtman DM, Noble PC, Alexander JW, Hipp JA.Quantitative assessment of the midcarpal shift test. J Hand Surg Am.1999;24(5):977–83.
5. Berger RA, Landsmeer JM. The palmar radiocarpal ligaments: astudy of adult and fetal human wrist joints. J Hand Surg Am.1990;15(6):847–54.
6. Apergis E, Darmanis S, Theodoratos G, Maris J. Beware of the ulno-palmar distal radial fragment. J Hand Surg Br. 2002;27(2):139–45.
7. Earp BE, Waters PM, Wyzykowski RJ. Arthroscopic treatment ofpartial scapholunate ligament tears in children with chronic wristpain. J Bone Joint Surg Am. 2006;88(11):2448–55.
8. Brown RR, Fliszar E, Cotten A, Trudell D, Resnick D. Extrinsic andintrinsic ligaments of the wrist: normal and pathologic anatomy atMR arthrography with three-compartment enhancement. Radio-graphics. 1998;18(3):667–74.
9. Taljanovic MS, Goldberg MR, Sheppard JE, Rogers LF. US of theintrinsic and extrinsic wrist ligaments and triangular fibrocartilagecomplex–normal anatomy and imaging technique. Radiographics.2011;31(1):e44.
10. Robson MD, Gatehouse PD, Bydder M, Bydder GM. Magneticresonance: an introduction to ultrashort TE (UTE) imaging. J ComputAssist Tomogr. 2003;27(6):825–46.
11. Seidel T, Hammer N, Garnov N, Schneider G, Steinke H. An algo-rithm for the calculation of three-dimensional collagen fiber orienta-tion in ligaments using angle-sensitive MRI. Magn Reson Med.2013;69(6):1595–602.
12. Totterman SM, Miller R, Wasserman B, Blebea JS, Rubens DJ.Intrinsic and extrinsic carpal ligaments: evaluation by three-dimensional fourier transform MR imaging. AJR Am J Roentgenol.1993;160(1):117–23.
13. Johnston RB, Seiler JG, Miller EJ, Drvaric DM. The intrinsic andextrinsic ligaments of the wrist. A correlation of collagen typing andhistologic appearance. J Hand Surg Br. 1995;20(6):750–4.
238 Skeletal Radiol (2014) 43:235–238





























