Embed Size (px)
Citation preview

FACTORS AFFECTING THE POST-DIALYSIS LEVELS
OF VANCOMYCIN AND GENTAMICIN IN HAEMODIALYSIS PATIENTS.
Acute-Haemodialysis Team
St. Helier’s Hospital
Presenter: Albert Acheamfour Acute Haemodialysis Manger
St. Helier’s Hospital UK MSc. Advancing Healthcare Practice
BSc. (Hons) Healthcare Practice Undergraduate Diploma(critical care)
U.K (V300) N.M.C Independent and Supplementary Nurse Prescriber
Vancomycin and Gentamicin Audit
Renal Unit St Helier Hospital

INTRODUCTION
• Infections are not an uncommon occurrence in patients undergoing dialysis and is partly attributed to the usage of the HD CVC’s.
• Increased morbidity and mortality in dialysis patients.
• Targeted antibiotic after culture is the gold standard of care,
• Treatment in most cases often starts prior to the results of microbiological cultures taken.
• Vancomycin and Gentamicin commonly used by most units

OLDER STRATGIES OBSERVED
• The administration of higher doses of vancomycin (30
mg/kg) in the last two hours of haemodialysis achieved mean pre-haemodialysis plasma vancomycin concentrations of 11.7 ± 1.5 μg/mL in anuric patients on day 8
• Fix therapeutic dose of 20mg/kg after a loading leads substantially to sub therapeutic levels
• Drawbacks to this approach:
– unnecessarily high peak plasma drug concentrations – High risk of patients receiving sub-therapeutic dose,
especially patients with residual renal function
BACKGROUND
Vancomycin
• Glycopeptide antibiotic
• Gram-positive bacterial infections (MRSA)
Gentamicin
• Aminoglycoside antibiotic
• Gram-negative bacteria infections
Both are
• Renally excreted
• Narrow therapeutic window
• Can cause Nephrotoxic /ototoxic
• Effective in pathogens associated with vascular-access related infections

BACKGROUND
• Principles of monitoring: • Reduces risk of damage
• auditory and renal
• Ensures therapeutic levels of the drug are circulating • aids recovery
• Daily levels • further doses if required to correct sub-therapeutic serum levels

RETROSPECTIVE AUDIT IN 2014
Six main key audited:
1. daily monitoring
2. dosage omission
3. dosage administration
4. dose administration without drug serum levels?
5. micro approval (?within 48-72hrs)
6. Prescription of correct dose of Vancomycin and Gentamicin

METHODOLOGY
• Data collection:
– Retrospective
– Cohort of 55
• 6 excluded due to lack of information available
– Inclusion criteria: All inpatients on renal unit prescribed Vancomycin and/or Gentamicin between July and November 2014.
– Data collected by analysing case notes, drug charts and discharge summaries
– All data anonymised to maintain confidentiality

Results
Sex of patient 64% male
Average age of patient 62.7 years
Patients on RRT 93%
Positive blood cultures 38%
Immunosuppressed 18%
Co-prescription of both antibiotics
78%
DATA ANALYSIS

50
24
88 95
17 10
0
20
40
60
80
100
Micro approval (pre)
Micro approval (post)
Stat dose given of correct dose
(pre)
Stat dose given of correct dose
(post)
Daily levels performed(pre)
Daily levels performed (post)
Graph to show adequacy of antibiotic monitoring and prescribing
RESULT

13
29 29 33
29 29
0
20
40
60
80
100
Dosing without level (pre)
Dosing without level (post)
Dosed with high levels (pre)
Dosed with high levels (post)
Missed dosing (pre)
Missed dosing (post)
Graph to show adequacy of antibiotic monitoring and prescribing
RESULT
Results show poor performance in prescribing and monitoring of Vancomycin and Gentamicin in our Renal Unit:
• 27%patients missed antibiotic doses
• risk of ineffective treatment
• A significant proportion (29%) of patients had doses of antibiotic prescribed when their levels were high or without a level
• increases the risk of the patient suffering nephrotoxicity/ototoxicity
DISCUSSION

• Only 13% of patients had daily levels
• Of all vancomycin levels taken 16% were subtherapeutic (i.e. <15)
• Of all gentamycin levels taken 31% were subtherapeutic (i.e. <1)
DISCUSSION

Look critically and implement measures to ensure adequate dosing of Vancomycin and Gentamicin. • We needed to know 1) What the Pre levels are 2) The percentage reduction on HDF treatment • Decision was made to take Pre and post levels of all patients
on Vancomycin and Gentamicin • To investigate whether there were any parameters which
could help predict the percentage reduction of the drugs levels on HDF treatment.
• Information on Vancomycin and Gentamicin prescription added to patient list. Possibly adding an alert regarding the level in previous 24 hours if this
RECOMMENDATION

SECOND AUDIT
METHOD:
• Inpatients on RRT for AKI or CKD who required antibiotic therapy for various indications were included in this study.
• All the patients were on (HDF) using Fresenius 5008 machines and FX60 high-flux dialysers.
• Anticoagulation was varied depending on the dialysis duration and co-morbid conditions, with some patients receiving no anticoagulation and others receiving unfractionated heparin.
• Data on weight, dialysis access type, blood pump speed, duration of dialysis, litres processed per session and ultrafiltration volume.

ANALYSIS
• 88 samples were collected from 21 patients, 62% of whom were male.
• The mean age was 70.2 years (range 37-91).
• The average duration of dialysis was 3.3 hours (198 minutes)
• The median blood pump speed was 275mls/minute
• Ultrafiltration volumes per session ranged between 0 to 2.6L per session

Percentage reduction of pre-dialysis antibiotic level (y) against ultrafiltration volume in litres (x)
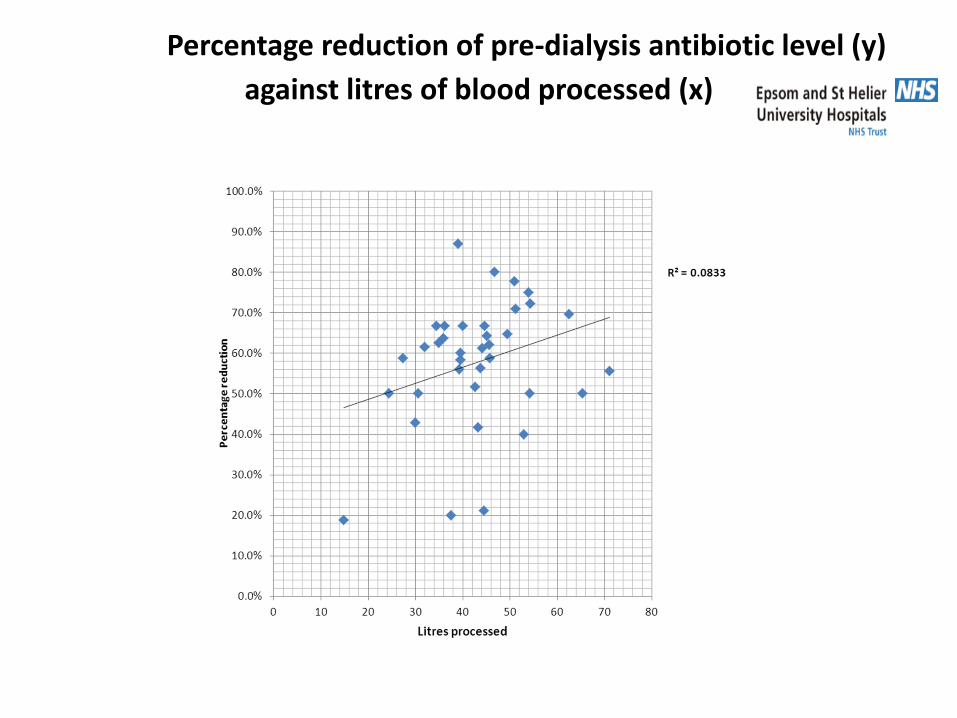
Percentage reduction of pre-dialysis antibiotic level (y)
against litres of blood processed (x)

Percentage reduction of pre-dialysis antibiotic level (y) against litres of blood processed per kilogram body weight (x)

RESULTS:
• There was no correlation between blood pump speed, duration of dialysis, litres processed per session, ultrafiltration volume and time on dialysis with the percentage reduction of the pre-dialysis drug level following dialysis.
• When the litres processed per session was adjusted for body weight pre-dialysis however, we found a close correlation (R2 = 0.23).

Predicting percentage reduction in 40 kg and 90kg with the same Litres process (80)using results from Pre HDF
serum levels

LIMITATIONS TO CONSIDER IN THE NEW AUDIT
• Glomerular Filtration rate of the patient
• Blood Albumen levels of the patients

MODEL SCALE OF EXPECTED REDUCTION
80 Blood
Litres
Processed
Weight of
90kg
22.5%
Reduction

CONCLUTION
• From the evidence above it is possible to come up with a ‘nomogram’, based on a few of these parameters (litres processed per body weight) to guide antibiotic dosing.
• it would be of great benefit, especially in the management of patients on these antibiotics in the outpatient setting, where it may not always be possible to get the results of drug levels in a timely fashion.

ACKNOWLEDGEMENT
Dabu-Tungu, E, Dorin G, Nsubuga M, Lutwama H, Padojino S, Seko P, Oumarou G, Bodneck C,
Miranda G, Hoyte J, Steele M, Mallinder S, Hurley A, Giannopoulous M, Sood B,
Makanjuola D
of the
Renal Unit, St. Helier Hospital, Carshalton, Surrey. U.K
REFERENCES
Vandecasteele, S.J., De Bacquer, D., De Vriesse, A.S,.2011. Implementation of a dose calculator for vancomycin to achieve target trough levels of 15-20 micro/ml in persons undergoing haemodialysis. clinical infectious disease, 53(2), p.124
Gomes, D.M., Smotherman, C., Birch, A, et al. 2014. Comparison of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or cefepime. Pharmacotherapy, (34), p 662
Brown, M,. Polisettv, R., Gracely, E.J., et al. 2011. Weight-based loading of vancomycin in patients on haemodialysis. clinical infection disease (53), p 164
Bray, B.D., Boyd, J., Daly, C et al. 2012. Vascular access type and risk of mortality in a national prospective cohort of haemodialysis patients. Q.J Medical . (105), p 1099
Rayner, H.C., Pisoni, R.L., 2010. The increasing use of haemodialysis catheter: evidence from DOPPS on its significance and ways to reverse it. Semin Dialysis. (23) p 6



![Cardiac stunning during haemodialysis: the therapeutic ...of gastrointestinal, cerebral and myocardial tissues [1, 9, 15]. Acute sub-clinical myocardial ischaemia during HD, or ‘car-diac](https://img.dokumen.tips/doc/110x75/5eca4597ce74ca60fc41deb7/cardiac-stunning-during-haemodialysis-the-therapeutic-of-gastrointestinal.jpg)