Embed Size (px)
Citation preview

Heart Attacks“Mended Hearts” Presentation, January, 2017
Quinn Capers, IV, MDAssociate Professor of Medicine (Cardiovascular Medicine)
Director, Transradial Coronary Interventions
Division of Cardiovascular Medicine


Acute Coronary Syndromes
Definition• Life-threatening episodes of abrupt decrease in coronary blood flow
in the patient with coronary atherosclerotic heart disease
• Continuum (clinical): from unstable angina to ST segment elevation
myocardial infarction (STEMI)
• Clinical continuum correlates with degree of coronary artery
obstruction, from partial to complete.

Stable angina
Unstable angina/
NSTEMI
STEMI
Coronary Atherosclerosis:
Vascular Biology

Acute Coronary SyndromesBiological/Clinical Correlation
• Stable plaque:• Chronic, stable exertional angina pectoris
• Low inflammatory state
• “Chronic coronary syndromes”
• Unstable or “vulnerable” plaque:• Unstable angina, acute MI
• High systemic inflammatory state (CRP, ESR, IL1)
• “Acute coronary syndromes”

1: Excess circulating LDL cholesterol gets sub-
endothelial and becomes oxidized, stimulating an inflammatory
response.

2: Circulating inflammatory cells are attracted to the
subendothelial compartment to participate in the inflammation

3: Once in the subendothelial compartment, the macrophages
ingest the lipid, becoming “foam cells”

4: Accumulation of foam
cells make up the early atherosclerotic
lesion: the “fatty streak”

5: Plaque progression.
Over 20 to 40 years, the plaque continues
To grow, until …

Coronary Artery Plaque/Rupture

12
Lessons Learned from Intravascular Imaging

13
Coronary Angiogram:
Provides a great silhouette of the lumen
But the action is in the
vascular wall

14
Coronary ImagingIntravascular Ultrasound (IVUS)

Unstable/Vulnerable Plaque vs Stable Plaque
Thickness
of fibrous
cap
covering
plaque
Lipids,
WBC’s and
enzymes
within
plaque
Connective
tissue
within
plaque
Risk of
rupture
Associated
clinical
sydromes
Stable
plaque
Thick Small amt Large amt Low Stable
exertional
angina
Unstable/
vulnerable
plaque
Thin Large amt Small amt High Acute
coronary
syndromes,
sudden
death

16
Unstable vs Stable Plaque

Acute Coronary SyndromesBiological/Clinical Correlation
Changing the vulnerable plaque to a quiescent, stable plaque is major focus of treatment of CAD patients
Statins (lipid lowering drugs)
BP control
Inhibition of renin angiotensin system
Tobacco avoidance
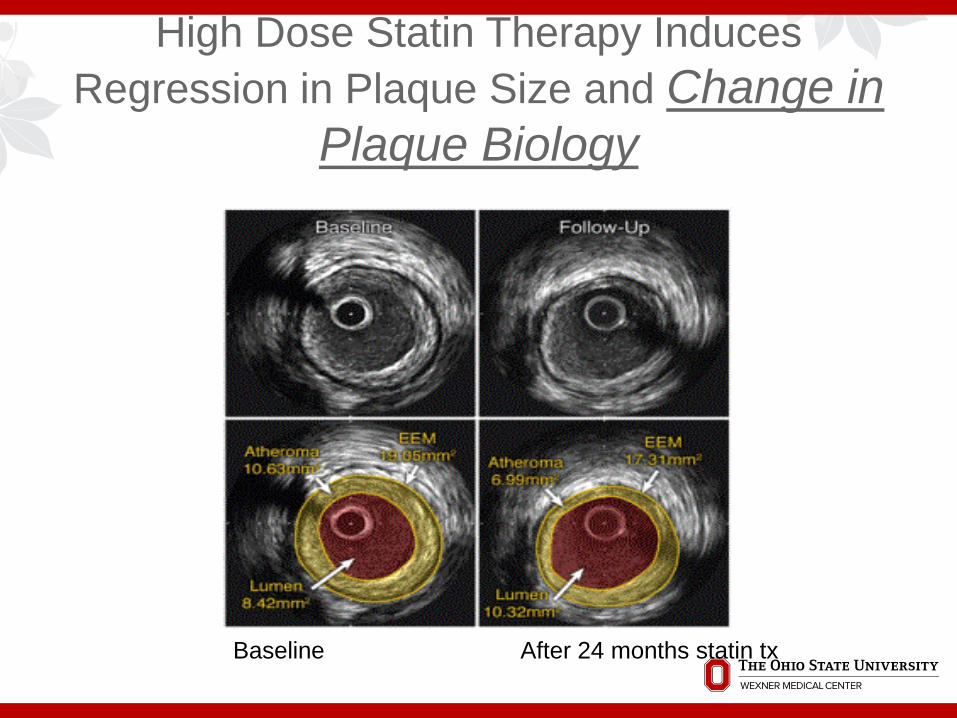
High Dose Statin Therapy Induces
Regression in Plaque Size and Change in
Plaque Biology
Baseline After 24 months statin tx

Plaque STABILIZATION (Not Regression/Shrinkage) is
the major benefit of aggressive lipid lowering
Lower levels of circulating LDL cholesterol
Less oxidized LDL infiltrating the arterial wall
Fewer macrophages infiltrating the arterial wall
Fewer enzymes to degrade the cap of the plaque
Plaque less likely to rupture
Lower risk of myocardial infarction
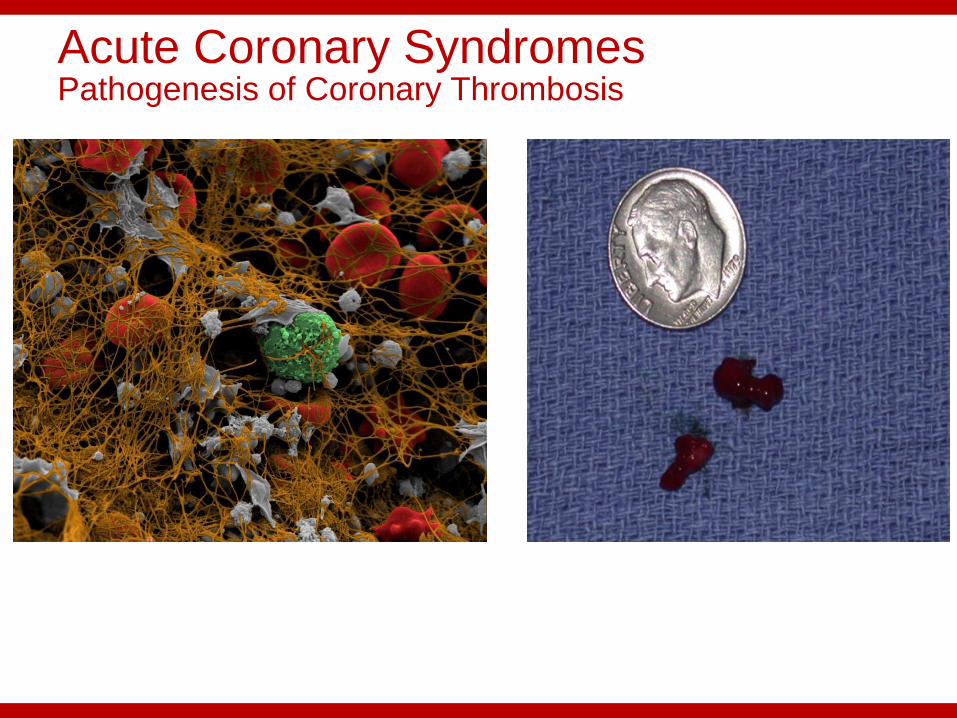
Acute Coronary SyndromesPathogenesis of Coronary Thrombosis
Fibrin strands
Platelets
RBC’s
WBC’s

Coronary Thrombosis:Clot begets Clot
Thrombin stimulates
platelet activation
Activated platelets
accelerate thrombin formation
Ruptured plaquepromotes thrombin
formation and recruits platelets
to site

Coronary Thrombosis:
Clot begets Clot
Thrombin stimulates
platelet activation
Activated platelets
accelerate thrombin formation
Ruptured plaquepromotes thrombin
formation and recruits platelets
to site
Antiplatelet drugs
Antithrombin drugs
Antiplatelet drugs
Antithrombin drugs
Antiplatelet drugs
Antithrombin drugs

The Primacy of the Platelet in Acute Coronary Syndromes
Inferior STEMI
100% native RCA
Acute thrombosis
of LAD stent

Keys to breaking the “Vicious Cycle” of Coronary Thrombosis
Antiplatelet drugs Aspirin
Clopidogrel
Prasugrel
IIb/IIIa glycoprotein receptor antagonists
Antithrombin drugs Unfractionated Heparin
Low molecular weight heparins
Bivalirudin
Argatroban

Acute Coronary Syndromes (USA/NSTEMI/STEMI):Treatment Principles
Restore normal coronary blood flow as soon as possible
Address coronary thrombosis, interrupt cycle
Optimize myocardial oxygen demand-supply ratio (Decrease HR, BP, wall tension)
Interrupt sympathetic nervous system/catecholamine stimulation of heart
In STEMI patients and high risk, unstable USA/NSTEMI patients, immediate cardiac cath/reperfusion

Acute Coronary SyndromesTreatment:USA/NSTEMI/STEMI
Statins Reduce inflammation inside culprit plaques and other plaques
throughout the body.
Beta blocker Decrease HR, BP, myocardial oxygen demand
Nitrates Decreases myocardial oxygen demand by decreasing preload, wall
tension
Improves coronary perfusion directly by dilating coronary arteries

Acute Coronary SyndromesTreatment:USA/NSTEMI/STEMI
Clopidogrel/Prasugrel/Ticlopidine/Ticagrelor Inhibits ADP-induced platelet activation
Aspirin Inhibits thromboxane A2-mediated platelet activation
IIb/IIIa platelet receptor antagonists Inhibits final common pathway of platelet aggregation
Reduces composite of death and MI in ACS pts
Unfractionated Heparin or Low molecular weight Heparin Inhibits thrombin

Acute Coronary Syndromes Treatment: USA/NSTEMI/STEMI
When or whether to perform cardiac catheterization with coronary angiography?
In STEMIs---emergently, unless there is a major contraindication
If pain persists despite maximal medical treatment, urgent cardiac cath with revascularization (coronary stent placement or CABG) is indicated
If pain resolves with medical treatment, but patient with high risk markers, cardiac cath and revascularization before hospital discharge (High TIMI Risk Score)
Very low risk patients without recurrent symptoms can be managed conservatively, with cardiac catheterization performed only for recurrent symptoms

Cardiac Catheterization/Coronary Angiography

Acute Coronary Syndromes:
Treatment:STEMI
Lumen
Thrombus
Complex plaque

Acute Coronary Syndromes:Treatment:STEMI
Immediate reperfusion therapy(coronary balloon angioplasty/stent placement or fibrinolytic drug therapy )
Restore normal coronary blood flow ASAP (“Time is muscle”)
Beta blockers, nitrates, antiplatelets, anti-thrombins, and statin drugs are initiated immediately

Acute Coronary SyndromesSTEMI
Fibrinolytic therapy Plasmin: enzyme that digests fibrin strands of a clot, effectively
“lysing” the clot
Plasminogen: Pro-enzyme of plasmin. Needs to be cleaved to plasmin
Plasminogen activators: enzymes that cleave plasminogen to plasmin:
Streptokinase (rarely used in US)
Tissue type plasminogen activator (tPA)
Tnk-tPA (modified tPA with longer half-life)
rPA (modified tPA with longer half-life)
Others (urokinase, APSAC, vampire bat saliva, etc.)

Fibrinolytic therapy: (Plasminogen activators that cleave plasminogen to plasmin)
Plasmin: digests fibrin strands, rendering clot unstable
Antiplatelet agents: prevent further platelet aggregation
Antithrombin agents: prevent production of more fibrin strands
Clot

STEMI: Percutaneous Coronary Intervention (PCI)
Catheter introduced into femoral, Brachial, or radial artery, advanced up to heart
X ray dye injected into coronary arteries to identify blocked artery
Blocked artery opened with tiny balloon and stent


Fibrinolytic drug tx
Improves survival in STEMI pts
Works within 90 min of initiation of tx
Initial success in 65-75% of pts
20-30% of pts reocclude artery
Intracranial bleed in approx 1%
Artery often left with moderate or severe residual stenosis
Available in all hospitals
Percutaneous intervention
Improves survival in STEMI pts
Works within <30 min of initiating cath
Initial success in >95% of pts
<1% of pts reocclude artery
Intracranial bleed risk <0.1%
Artery usually left with 0% residual stenosis
Available in <1/3 of hospitals
Immediate Reperfusion in STEMI: FibrinolyticTherapy vs PCI

STEMI Treatment: Fibrinolytic Therapy vs Percutaneous Coronary Intervention (PCI)
In multiple head-to-head studies, PCI (balloon angioplasty with stent placement) in STEMI pts proved superior to fibrinolytic drug therapy (better survival, better myocardial salvage, lower complication rates)
Most hospitals do not have an interventional cath lab
If pts present to hospitals without cath lab, they have better outcomes if they can be transported to a cath lab and have PCI within 90 minutes

Treatment of STEMI:Coronary Stenting vs Fibrinolytic therapy
Bottom line:
Stenting >>>fibrinolytic therapy>>>nothing

Acute Coronary Syndromes:Treatment:STEMI Whether treating the STEMI pt with fibrinolytic therapy or mechanical
revascularization, patients who receive the treatment early (2-3 hrs from pain onset) have ½ the mortality of people who receive the treatment late (>6 hrs after pain onset)
This is a major problem, with delays at several steps:
Patient delays seeking medical help (denial, poor access, social issues)
Delay in ER staff performing EKG
Delay in EKG being presented to MD for interpretation
Delay in drugs being mixed in pharmacy and administered to pt
Delay in transporting pt from ER to cath lab or from one hospital to another
Delay in cath lab staff coming in from home

Cases from The OSU Ross Heart Hospital

Inferior STEMI
EKG 1615 after ROSC







Sudden Cardiac Death While Exercising








Inferior STEMIArtery Reperfused With Lytic Therapy

Inferior STEMIArtery Reperfused With Lytic Therapy

Inferior STEMIArtery Reperfused With Lytic Therapy

Anterior-Lateral MI with Cardiogenic Shock

Anterior-Lateral MI with Cardiogenic Shock

Anterior-Lateral MI with Cardiogenic Shock

Anterior-Lateral MI with Cardiogenic Shock
Unstable Angina

Unstable Angina

Unstable Angina

Anterior STEMI

Anterior STEMI
Occluded prox-mid LAD

Anterior STEMI

Anterior STEMI

5 Minutes Later . . .

. . .

72
Discharge after STEMI: What Rx?

73

Acute Coronary SyndromesSTEMI: The Aftermath Therapies to start before hospital discharge:
ACE inhibitors (prevent post-MI cardiac enlargement or “remodeling”, and sudden death)
Statins (decrease lipids and change vulnerable, rupture-prone plaques to stable plaques)
Aldosterone receptor antagonists (improve survival in pts with severe LV dysfunction post-MI)
(These are all in addition to ASA, P2Y12 inhibitor, beta-blocker)

Acute Coronary Syndromes:
Summary• Acute coronary syndromes range from unstable angina without
infarction, to STEMI.
• Stable plaques are filled with connective tissue, are metabolically
inactive, and cause stable exertional angina
• Unstable or “vulnerable” plaques are lipid-filled, tense, metabolically
active, and prone to rupture, causing acute coronary syndromes
• A main focus of treating CAD pts is transforming vulnerable plaques
to stable plaques. Statins are the drugs with the most evidence
supporting this.

Acute Coronary Syndromes:
Summary
• Coronary thrombosis is a hallmark of acute coronary syndromes
• Much of the therapy for ACS is directed at interrupting the vicious cycle of thrombosis (e.g., ASA, clopidogrel, heparin, IIb/IIIa blockers)
• In STEMI, emergent reperfusion can be life-saving, the sooner the better
• In STEMI patients, PCI (coronary stenting) results in greater myocardial salvage and better survival than fibrinolytic therapy, but only if it can be performed expeditiously. If no cath lab is available, do not delay giving fibrinolytic therapy, which is also a life-saving therapy






























