-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
1/10
Acute Compartment Syndrome ofthe Upper Extremity
Abstract
Acute compartment syndrome occurs when pressure within a
fibro-
osseous space increases to a level that results in a
decreased
perfusion gradient across tissue capillary beds. Compartment
syndromes of the hand, forearm, and upper arm can result in
tissue necrosis, which can lead to devastating loss of function.
The
etiology of acute compartment syndrome in the upper extremity
is
diverse, and a high index of suspicion must be maintained.
Pain
out of proportion to injury is the most reliable early symptom
of
impending compartment syndrome. Diagnosis is particularly
difficult
in obtunded patients and in young children. Early recognition
andexpeditious surgical treatment are essential to obtain a
good
clinical outcome and prevent permanent disability.
Compartment syndrome was firstdescribed in 1881 by Richardvon
Volkmann.1 The etiology, patho-
physiology, and management of
compartment syndrome and the as-
sociated complications have been ex-
tensively described. Acute compart-
ment syndrome (ACS) occurs with
elevation of interstitial pressure in a
closed fascial compartment, resulting
in microvascular compromise. This
causes the perfusion gradient to fall
below a critical value, leading to is-
chemia of the tissues within this con-
fined space. In the upper extremity,
the dorsal and volar compartments
of the forearm are the most com-
monly affected. Upper extremity
ACS can lead to devastating loss of
function, including Volkmann ische-
mic contracture, neurologic deficit,
infection, amputation, and death.
A wide range of causes of ACS in
the upper extremity has been re-
ported, and a high index of suspicion
must be maintained. Distal radius
fracture in adults and supracondylar
humerus fracture in children are the
most frequent causes of compart-
ment syndrome in the upper extrem-
ity.1,2 Compartment syndrome is a
clinical diagnosis, and it can be diffi-
cult to make in certain patient popu-
lations, such as persons who are ob-
tunded and children.2-5 Emergent
surgical treatment is required; themost important determinant of
out-
come is early recognition and expedi-
tious surgical intervention.3,5-9 Re-
constructive procedures can be
performed to improve the function
of the affected upper extremity in the
patient with Volkmann contracture;
however, return of normal function
should not be expected.10-16
Anatomy
The upper extremity contains 15
compartments. The upper arm con-
sists of a flexor (ie, volar) compart-
ment and an extensor (ie, dorsal)
compartment. The forearm is divided
into three compartments: volar, dor-
sal, and lateral (ie, mobile wad) (Fig-
ure 1). The hand has 10 compart-
Mark L. Prasarn, MD
Elizabeth A. Ouellette, MD
From the Department of
Orthopaedics, University of
Rochester, Rochester, NY
(Dr. Prasarn), and Physicians for
The Hand, Miami, FL (Dr. Ouellette).
Dr. Ouellette or an immediate family
member serves as a paid consultant
to or is an employee of Stryker.
Neither Dr. Prasarn nor any
immediate family member hasreceived anything of value from
or
owns stock in a commercial
company or institution related
directly or indirectly to the subject of
this article.
J Am Acad Orthop Surg2011;19:
49-58
Copyright 2011 by the American
Academy of Orthopaedic Surgeons.
Review Article
January 2011, Vol 19, No 1 49
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
2/10
ments: hypothenar, thenar, and
adductor pollicis as well as four dor-
sal interosseous and three volar in-
terosseous17 (Figure 2). The volar
forearm is the most commonly af-
fected compartment in the upper ex-
tremity. Compartment syndrome in
this area typically occurs following
fracture of the distal radius, supra-
condylar humerus, or diaphysis of
the radius or ulna.2,17,18 Any compart-
ment can be affected, however. Digi-
tal fasciotomy is necessary in some
cases19 (Figure 3).
In the upper arm, the medial and
the lateral intermuscular septa sepa-
rate the flexor compartment from
the extensor compartment. The bra-
chial fascia is a dense fibrous sheath
that surrounds the muscles in each of
the two compartments. In the fore-
arm, the stiff interosseous membrane
bridges the distance between the ra-
dius and the ulna. Just anterior to
this membrane lie the flexor digito-
rum profundus, flexor pollicis lon-
gus, and pronator quadratus mus-
cles. Some consider the pronator
quadratus to lie within an additional
compartment of the distal volar fore-
arm, separate from the flexor ten-dons at this level.20 These
deep volar
muscles are the most commonly
damaged muscles in forearm com-
partment syndrome. The remaining,
more superficial flexor muscles are
less prone to ischemia than their
deeper counterparts. The finger and
wrist extensors lie on the posterior
aspect of the forearm. Isolated
exercise-induced compartment syn-
dromes of the extensor carpi ulnaris
muscle have been noted in case re-
ports.21,22 The mobile wad, which
consists of the brachioradialis, flexor
carpi radialis longus, and flexor
carpi radialis brevis tendons, is rarely
involved.12 The antebrachial fascia,
which is a continuation of the bra-
chial fascia, envelops the compart-
ments and muscles in the forearm.
The compartments of the hand are
divided by the carpal bones, metacar-
pals, and individual investing fascial
layers. Pressures within the carpal tun-
nel may become elevated in cases of
hand or volar forearm compartment
syndrome. Release of the transverse
carpal ligament is often necessary in
addition to release of the other in-
volved compartments. The digital fas-
cial compartments are bound by the
Cleland ligament and the Grayson lig-
ament, and elevated pressure may oc-
cur in individual digits (Figure 3).
Compartment syndrome of the hand
typically necessitates carpal tunnel re-
lease and dorsal interosseous compart-
ment releases; however, any compart-
ment may be involved and may require
release. The decision regarding the
number and location of incisions
should be based on the clinical findings
and on intraoperative pressure mea-
surements.3
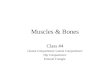
Cross section at the junction of the proximal and middle thirds
of the forearmdemonstrating the compartments and the important
neurovascular structures.The volar compartment contains the flexor
muscles of the wrist and digits,including the flexor digitorum
superficialis (FDS), flexor carpi radialis (FCR),flexor pollicis
longus (FPL), flexor digitorum profundus (FDP), and flexor
carpiulnaris (FCU), as well as the ulnar nerve (UN), ulnar artery
(UA), mediannerve (MN), median artery (MA), radial artery (RA),
superficial branch of theradial nerve (RN), anterior interosseous
artery (AIA), and anteriorinterosseous nerve (AIN). The dorsal and
volar compartments are separatedby the interosseous membrane. The
dorsal compartment contains the fingerand thumb extensors and the
long thumb abductor as well as the posteriorinterosseous artery
(PIA), posterior interosseous nerve (PIN), extensor carpiulnaris
(ECU), extensor pollicis longus (EPL), and extensor
digitorumcommunis (EDC). The mobile wad, which is often considered
to be a thirdcompartment, is composed of the extensor carpi
radialis brevis and longusmuscles (ECR) and the brachioradialis
(BR). (Reproduced with permissionfrom Ouellette EA: Compartment
syndromes in obtunded patients. Hand Clin1998;14[3]:431-450.)
Figure 1
Acute Compartment Syndrome of the Upper Extremity
50 Journal of the American Academy of Orthopaedic Surgeons
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
3/10
Etiology
ACS of the upper extremity is caused
by a myriad of factors, including
fracture, bleeding disorders, constric-
tive dressing and casting, arterial in-
jury, extravasation of intravenous or
intraosseous infusion, and regional
anesthesia3-5,23-35 (Table 1). Anything
that causes increased volume within
the confined fascial space (eg, bleed-
ing, edema, purulent material, extra-
neous fluids) or restricts the com-
partment from expanding (eg, burn,
casting, dressing, tourniquet) can
cause ACS.
It is difficult to estimate the true
incidence of compartment syndromeof the upper extremity, but
most
cases occur in the setting of fracture.
McQueen et al17 analyzed 164 pa-
tients with traumatic ACS. In 69%
of cases, compartment syndrome was
associated with fracture. The most
frequent fracture types observed
were of the tibial diaphysis (36%),
the distal radius (9.8%), and the di-
aphysis of the forearm bones (7.9%).
Only 2.5% occurred following hand
fracture, and the incidence was 0.6%each for elbow
fracture-dislocation
and humeral fracture. Soft-tissue in-
jury without fracture was the second
most common cause of injury
(23.2%). Incidence in the forearm
and hand was 5.5% and 0.6%, re-
spectively. Within this subgroup,
10.3% occurred in patients with
bleeding disorders or who were tak-
ing anticoagulants.
Grottkau et al2 reviewed a national
trauma database and found the inci-
dence of pediatric forearm compart-
ment syndrome to be 1%. Ouellette
and Kelly3 reported on 19 patients
with compartment syndrome of the
hand. Most cases were iatrogenic, re-
sulting from complications related to
intravenous or intra-arterial adminis-
tration of drugs. The incidence of
compartment syndrome in unstable
fractures of the distal end of the ra-
dius is substantially higher with con-
comitant ipsilateral elbow injury
than with distal radial fracture
alone.36
Pathophysiology
Compartment syndrome is caused by
an elevation of pressure within a
fibro-osseous space resulting in de-
creased tissue perfusion. The initial
rise in intracompartmental pressure
causes increased extravascular ve-
nous pressure. Because of lack of
musculature in the wall media, this
relatively small rise in pressure
causes the venule walls to collapse.
The resulting decrease in hydrostatic
gradient causes reduced local perfu-
sion and increased interstitial pres-
sure. This increased interstitial pres-
sure in turn causes increased edema
within the compartment, and this
cascade of events repeats itself per-
petually.12 Vasospasm and shock lead
to decreased arteriolar pressure and
possibly closure of end arterioles,
leading to a further decrease in tissue
perfusion4 (Figure 4).
Ischemia occurs when a critical
threshold is reached in the local arte-
riovenous gradient and when circula-
tion is compromised to the point that
blood flow is insufficient to meet the
metabolic demands of the tissue.4
This critical variable is represented
by the absolute difference between
compartment pressure and blood
pressure.37 Heppenstall and col-
leagues38,39 prefer to compare intra-
compartmental pressure with mean
arterial pressure, but diastolic blood
pressure is easier to obtain and cal-
culate. Experimental data in a canine
model have shown that terminal ar-
terial pressure is equal to diastolic
blood pressure;40 thus, we use dia-
stolic blood pressure to determine
the critical threshold.
In a canine study, muscle necrosis
occurred when the intracompart-
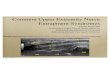
Cross section at the level of the metacarpal shafts
demonstrating the 10compartments of the hand: hypothenar, thenar,
and adductor pollicis as wellas four dorsal interosseous and three
volar interosseous. (Reproduced withpermission from Ouellette EA:
Compartment syndromes in obtundedpatients.Hand
Clin1998;14[3]:431-450.)
Figure 2
Mark L. Prasarn, MD, and Elizabeth A. Ouellette, MD
January 2011, Vol 19, No 1 51
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
4/10
mental pressure rose to a level 20
mm Hg below diastolic blood pres-
sure.40 Heckman et al41 demonstrated
that irreversible changes to the pe-
ripheral nerves and skeletal muscle
occur following 8 hours of complete
ischemia. Following onset of cellular
anoxia, affected cells begin anaero-
bic metabolism and may die. Devas-
tating loss of function may occur fol-
lowing substantial loss of muscle and
neural tissue in the upper extremity.
Muscle ischemia can lead to release
of myoglobin, which can cause myo-
globinuria, metabolic acidosis, and
hyperkalemia. Renal failure, cardiac
arrhythmia, cardiac failure, and
shock may then ensue. The magni-
tude of these systemic effects is de-
pendent on the duration of ischemia
and the size of the muscle compart-
ments involved.4
Clinical Evaluation
Historically, the five Ps (pain, pallor,
pulselessness, paralysis, paresthesia)were taught as the
symptoms that
herald compartment syndrome.
Pulselessness is rare, occurring only
after arterial injury. Most of these
symptoms present only after a sub-
stantial amount of time has elapsed
following the onset of compartment
syndrome, and outcomes typically
are poor even with expedient fasciot-
omy. Pain out of proportion to in-
jury and pain with passive stretching
of muscles in the involved compart-ment are the earliest
indicators of
compartment syndrome.23 Compart-
ment syndrome also should be sus-
pected with tense, swollen compart-
ments. In a series of patients with
compartment syndrome of the hand,
Ouellette and Kelly3 demonstrated
that the most consistent clinical find-
ing was a tense, swollen hand in an
intrinsic minus position (ie, exten-
sion of the metacarpophalangeal
joints and flexion of the intercarpal
joints) (Figure 5).
ACS is typically diagnosed clini-
cally. However, it may be necessary
to measure compartment pressure
(Figure 6). Animal studies demon-
strate that compartment syndrome is
indicated in the presence of a differ-
ence between diastolic blood pres-
sure and the compartment measuring
Table 1
Causes of CompartmentSyndrome of the UpperExtremity3-5,23-35
Fracture
Crush injury
Injection injury
Ring avulsion
Suction injury
Penetrating trauma
Constrictive dressings
Casts
Burns
Infection
Bleeding disorders
Spider bite
Snakebite
Arterial injury
Reperfusion
In utero compression
Extravasation of infusions
Injection of illicit drugs
Regional anesthesia
Prolonged compression
Finger decompression. A, Illustration demonstrating a midaxial
incision madeon the index finger. This incision is made on the
ulnar side of digits 2 through4 and on the radial side of digits 1
and 5. The neurovascular bundles areidentified and retracted
volarward, and the fascia between them is cut alongwith the flexor
sheath. B and C, Clinical photographs following fasciotomiesof the
hand and digits. (Reproduced with permission from Ouellette EA:
Compartment syndromes in obtunded patients. Hand
Clin1998;14[3]:431-450.)
Figure 3
Acute Compartment Syndrome of the Upper Extremity
52 Journal of the American Academy of Orthopaedic Surgeons
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
5/10
20 mm Hg40 or a difference be-
tween mean arterial pressure and the
compartment measuring 30 mm
Hg.41 Fasciotomy is often performed
in patients with absolute pressure
measuring >30 mm Hg.6,42 We con-
sider a differential between diastolic
pressure and the compartment of
20 mm Hg to be an absolute indica-
tion for emergent fasciotomy. In the
patient with swollen compartments
and nearly normal pressures (20
mm Hg. Compartment pressure
should be measured when suspected
in a patient who is uncooperative,
who has an altered mental status, or
whose young age renders the clinical
examination inadequate.3-6,8,23 In pe-
diatric patients, Bae et al6 demon-
strated that an increased need for an-algesics was most
predictive of
compartment syndrome.
Compartment PressureMeasurement
We typically measure compartment
pressures in patients with equivocal
Algorithm demonstrating the cascade of events in the
pathophysiology of compartment syndrome.
Figure 4
A and B, Photographs demonstrating a tense, swollen hand and
forearm.The hand is held in the intrinsic minus position.
(Reproduced with permissionfrom Prasarn ML, Ouellette EA,
Livingstone A, Giuffrida AY: Acute pediatricupper extremity
compartment syndrome in the absence of fracture. J
PediatrOrthop2009;29[3]:263-268.)
Figure 5
Mark L. Prasarn, MD, and Elizabeth A. Ouellette, MD
January 2011, Vol 19, No 1 53
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
6/10
examination and in those who can-
not be examined fully. An equivocal
examination is one in which com-
partment syndrome is suspected anduncertainty exists regarding
the clini-
cal examination. Measurements are
also often taken in the operating the-
ater to verify which compartment or
compartments are affected and to en-
sure that they are fully decompressed
following fasciotomy. Compartments
that clinically appear to be involved
are tested, and measurements are
taken when the compartment ap-
pears to be the most tense and swol-
len. In the case of associated frac-
ture, the catheter is inserted close to
the fracture site. Otherwise, mea-
surements are taken at the location
that is most accessible to the com-
partment. Typically, a single mea-
surement is taken for each suspected
compartment. When in doubt re-
garding the resulting pressure value,
repeat measurements should be ob-
tained at other sites.
The two most common measure-
ment techniques involve the use of a
slit catheter or a side port needle.Straight needles have been
shown to
provide less accurate results.43 The
catheter may be left in situ for repeat
or continuous pressure measure-
ments. In the past, we used an arte-
rial line and a pressure transducer
similar to the continuous-infusion
technique described by Matsen,8 but
we did not use the infusion pump.
More recently we have begun using
the Stryker Intra-Compartmental
Pressure Monitor System (Stryker,
Kalamazoo, MI), which is more con-
venient and requires no setup. Boody
and Wongworawat43 evaluated three
commonly used modalities for com-
partment pressure measurement and
found an arterial manometer to be
the most accurate method, followed
by the Intra-Compartmental Pressure
Monitor System. They concluded
that the Whitesides manometer lacks
the precision required for clinical
use.
Fasciotomy
The main goals in the management
of ACS of the upper extremity are
expedient release of all fascial and
epimysial envelopes and decompres-
sion of all affected compartments
and nerves. Compartments that are
clearly affected clinically are re-
leased, and those that cannot be ex-
amined adequately are measured
with the Intra-Compartmental Pres-
sure Monitor System or an arterial
manometer. Pressure in the carpaltunnel is measured when
involve-
ment of that area is suspected. Pres-
sure measurement 20 mm Hg with
decreased sensation and/or dimin-
ished strength in the thenar muscles
is an indication for open carpal tun-
nel release.
Ronel et al20 described a technique
that allows decompression of the su-
perficial muscles and the deep mus-
cles of the volar forearm as well as
release of the median nerve at possi-
ble sites of compression. We use this
approach because it causes the least
amount of iatrogenic injury to the
superficial muscles, arteries, and
nerves compared with other de-
scribed approaches to the volar fore-
arm. A longitudinal skin incision is
made beginning just radial to the
flexor carpi ulnaris at the wrist. The
incision is extended proximally to
the medial epicondyle, then curved
radially over the antecubital fossa
(Figure 7). Distally, the incision may
be extended to the midline to incor-
porate open carpal tunnel release.
The lacertus fibrosus and fascia over
the flexor carpi ulnaris are opened.
The flexor carpi ulnaris is retracted
ulnarly, and the flexor digitorum su-
perficialis is retracted radially to al-
low visualization and opening of the
Algorithm for evaluating and managing suspected compartment
syndrome.
Figure 6
Acute Compartment Syndrome of the Upper Extremity
54 Journal of the American Academy of Orthopaedic Surgeons
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
7/10
fascia over the deep muscles of the
forearm.
Release of the volar compartment
often results in decompression of the
dorsal compartment and the mobile
wad, as well. Should the pressures
remain elevated in the dorsal com-partment or the mobile wad, a
sec-
ond fasciotomy is performed. We use
a dorsal longitudinal incision extend-
ing from 2 cm distal to the lateral
epicondyle of the humerus toward
the midline of the wrist. Deep dissec-
tion is made through the interval be-
tween the extensor digitorum com-
munis and the extensor carpi radialis
brevis. This allows decompression of
the musculature in the dorsal com-
partment and the mobile wad.Release of the volar and dorsal
in-
terosseous compartments and the ad-
ductor compartment to the thumb is
begun by making two longitudinal
incisions dorsally over the 2nd and
4th metacarpals (Figure 2 and Figure
8). The fascia over the dorsal in-
terosseous muscles is incised. To de-
compress the first volar interosseous
and adductor pollicis muscles, blunt
dissection is performed along the ul-
nar side of the 2nd metacarpalthrough the more radial
incision.
The second and third volar interosse-
ous compartments are released by
dissecting along the radial aspect of
the 4th and 5th metacarpals through
the more ulnar incision. To release
the thenar and hypothenar compart-
ments, longitudinal incisions are
made at the junctions of the glabrous
and nonglabrous skin over the radial
side of the 1st metacarpal and the ul-
nar side of the 5th metacarpal.
Compartment syndrome of the up-
per arm is rare. The anterior and the
posterior compartments can be de-
compressed through a single medial
or lateral incision. Maginn and El-
liot44 suggested that the creation of
two separate midline incisions di-
rectly over the anterior and posterior
compartments causes less disruption
Surgical approaches to the volar compartment of the forearm. A,
Illustrationdemonstrating the skin incision for the ulnar approach.
B, The intervalbetween the flexor carpi ulnaris muscle and the
flexor digitorum superficialismuscle is entered. C, After the ulnar
nerve and artery are identified andprotected, the fascia over the
deep compartment is opened completely.D,Incision for the Henry
approach, which is performed through the intervalbetween the flexor
carpi radialis and the brachioradialis muscles.(Reproduced with
permission from Ouellette EA: Compartment syndromes inobtunded
patients. Hand Clin1998;14[3]:431-450.)
Figure 7
Mark L. Prasarn, MD, and Elizabeth A. Ouellette, MD
January 2011, Vol 19, No 1 55
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
8/10
to the perforating septal vessels, re-
sulting in decreased iatrogenic ische-
mia to the muscles and flaps com-
pared with a single medial incision.
In our experience, compartment syn-
drome in the upper extremity is usu-
ally associated with humeral frac-
ture, which requires open reduction
and internal fixation. This cannot be
done through a medial approach. It
is rare that both compartments are
involved. Thus, we make a longitudi-
nal incision over the affected com-
partment to first perform thorough
decompression. We use the same in-
cision for open reduction and inter-
nal fixation of the fractured hu-
merus. If the other compartment is
also involved, a second fasciotomy is
made over it.
Wound Closure
Wounds are typically left open and
initially are covered with sterile wet-
to-dry dressings. The skin should not
be closed acutely following fasciot-
omy. We do not routinely use reten-tion sutures or rubber
catheters to
prevent wound edge retraction. In
wounds with exposed tendon, bone,
or neurovascular structures, a bovine
collagen matrix wound dressing (In-
tegra artificial dermis; Integra Life-
Sciences, Plainsboro, NJ) is applied
to prevent desiccation. This can be
grafted over later. The patient is re-
turned to the operating suite after 48
to 72 hours for irrigation and d-
bridement. Delayed primary woundclosure may be done at this
time, as
well. In the patient with muscle ne-
crosis, all nonviable muscle is
sharply dbrided. When muscle via-
bility is a concern, repeat dbride-
ment is done every 48 hours. Under-
mining the skin flaps often assists
with tension-free closure. For
wounds that cannot be closed, a
vacuum-assisted wound closure sys-
tem (VAC Therapy System; KCI, San
Antonio, TX) is placed, and split-thickness skin grafting is
performed
at a later date. Potential advantages
of a vacuum-assisted closure system
include shorter hospital stays, re-
duced need for skin grafting, and a
lower rate of nosocomial infec-
tion.45,46
Outcomes andComplications
Outcomes following compartment
syndrome are dependent on injury
severity, duration of ischemia, and
preinjury status and comorbidities.
The amount of infarction varies con-
siderably, as do outcomes. Time
from diagnosis to fasciotomy is the
most important predictor of out-
come. The critical delay from diag-
nosis to treatment is reported to be 6
to 24 hours.3-6,8,9,23,37,47 Irreversible
damage has been shown to occur af-
ter 8 hours in a canine model.40 Full
recovery with minimal residual dys-
function can be expected with
prompt diagnosis and intervention ofcompartment syndrome of the
upper
extremity.3-6,12,13,25,48 Delay beyond 6
to 24 hours may result in Volkmann
ischemic contracture, neurologic def-
icit, infection, amputation, or death.
How late is too late to perform
surgical decompression? In most
cases the exact time of onset of com-
partment syndrome cannot be deter-
mined; thus, it is impossible to deter-
mine its duration. In such instances,
the clinical examination is relied onheavily. Voluntary muscle
contrac-
tion in the setting of compression is
indicative of the existence of viable
muscle, and emergent fasciotomy
should be performed. In the patient
with no demonstrable muscle func-
tion, the best treatment may involve
supportive care for myoglobinuria
and aggressive splinting to maintain
the arm and hand in a functional po-
sition.37
Ouellette and Kelly
3
noted poor re-sults in 4 of 19 patients with hand
compartment syndrome. All four pa-
tients were obtunded at the time of
onset, and two required amputation.
A high index of suspicion for com-
partment syndrome must be main-
tained in persons who are who are
difficult to examine and who cannot
communicate effectively. Gelberman
et al49 reported the results of surgical
decompression of compartment syn-
drome of the forearm in 10 patients.
No patient developed Volkmann
contracture, but only two patients
had normal postoperative results. Six
patients who underwent volar fas-
ciotomy required supplemental skin
grafting. The worst results were ob-
served in patients with severe crush
injuries and in another with arterial
injury.
Illustration demonstrating twolongitudinal incisions made
overthe 2nd and 4th metacarpals torelease the dorsal and
volarinterosseous compartments andthe adductor compartment of
thethumb. (Reproduced withpermission from Ouellette EA:Compartment
syndromes inobtunded patients. Hand Clin1998;14[3]:431-450.)
Figure 8
Acute Compartment Syndrome of the Upper Extremity
56 Journal of the American Academy of Orthopaedic Surgeons
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
9/10
Volkmann Contracture
Irreversible tissue ischemia results in
muscle necrosis within the affected
compartment, which leads to con-
tracture. In the forearm, the typical
posture that develops includes elbow
flexion, forearm pronation, wrist
flexion, and thumb adduction with
the metacarpophalangeal joints in
extension and the interphalangeal
joints in flexion. The median nerve is
often affected to a greater degree
than the ulnar nerve because the me-
dian nerve lies in the deeper zone
that is more severely compromised
by ischemia.
Tsuge
15
classified contracture asmild, moderate, and severe. The
mild
type involves mild ischemic contrac-
ture primarily of the flexor digito-
rum profundus and no neurologic
deficit. In the moderate type, the
flexor digitorum profundus, flexor
pollicis longus, and pronator teres
are affected, and the flexor digito-
rum superficialis and flexor carpi ul-
naris are affected to a lesser degree.
Intrinsic muscle paralysis and sen-
sory neuropathy of the median and
ulnar nerves are also present. The se-
vere type involves ischemic damage
to all of the flexors in the fore-
arm, variable involvement of the ex-
tensors, and severe neurologic
injury.12,14-16
The main goal in the management
of Volkmann contracture is to re-
store function; however, normal
function of the upper extremity
should not be expected.10-16 Affected
muscles are exposed, and fibrotic or
necrotic tissue is dbrided. Thorough
neurolysis of the median and ulnar
nerves should be performed as well
as tenolysis of scarred tendons. Iso-
lated tendon lengthening is not rec-
ommended because it typically re-
sults in recurrent contracture and
loss of grip strength.12,16 In persons
with mild contracture, the flexor/
pronator slide may be performed to
improve hand position as well as
function of the forearm flexors. Ten-
don transfer may be performed to
improve specific dysfunction in per-
sons with moderate contracture.
Usually this involves use of an exten-sor tendon transfer;
however, flexor
tendons can be transferred in the
case of dorsal contracture. Free mus-
cle transfer, typically using the graci-
lis muscle, is necessary to improve
function in persons with severe con-
tracture.12,15,16
Summary
ACS of the upper extremity is a poten-
tially devastating condition that can
lead to substantial loss of function.
Compartment syndrome has many
causes, and a high index of suspicion
must be maintained. The final common
pathway is a vicious cycle of increased
tissue pressure with resulting cellular is-
chemia. All affected compartments in
the upper extremity must be recog-
nized, and thorough decompression
must be performed in an expedient
manner. Compartment syndrome is dif-
ficult to diagnose in some cases, partic-
ularly in obtunded patients and young
children. Prompt diagnosis and emer-
gent surgical decompression are essen-
tial to obtain a good clinical outcome
and preventing a catastrophic result.
References
Evidence-based Medicine: Levels of
evidence are described in the table of
contents. In this article, references2-6, 9, 10, 14-20, 28, 31,
42, 46,
and 47 are level IV studies. Refer-
ences 11-13, 23, 37, 44, and 45 are
level V expert opinion.
Citation numbers printed in bold
type indicate references published
within the past 5 years.
1. von Volkmann R: Die ischmischen
Muskellhmungen und Kontracturen.
Centralblatt fr Chirurgie, Leipzig1881;
8:801-803.
2. Grottkau BE, Epps HR, Di Scala C:
Compartment syndrome in children and
adolescents.J Pediatr Surg2005;40(4):
678-682.
3. Ouellette EA, Kelly R: Compartmentsyndromes of the hand. J
Bone JointSurg Am1996;78(10):1515-1522.
4. Ouellette EA: Compartment syndromesin obtunded patients.Hand
Clin1998;14(3):431-450.
5. Prasarn ML, Ouellette EA, LivingstoneA, Giuffrida AY: Acute
pediatric upperextremity compartment syndrome in theabsence of
fracture.J Pediatr Orthop2009;29(3):263-268.
6. Bae DS, Kadiyala RK, Waters PM: Acutecompartment syndrome in
children:Contemporary diagnosis, treatment, andoutcome.J Pediatr
Orthop2001;21(5):
680-688.
7. Mabee JR, Bostwick TL: Patho-physiology and mechanisms
ofcompartment syndrome.Orthop Rev1993;22(2):175-181.
8. Matsen FA:Compartmental Syndromes.New York, NY, Grune and
Stratton,1980.
9. McQueen MM, Christie J, Court-BrownCM: Acute compartment
syndrome intibial diaphyseal fractures.J Bone JointSurg
Br1996;78(1):95-98.
10. Bunnell S, Doherty EW, Curtis RM:Ischemic contracture,
local, in the hand.Plast Reconstr Surg1948;3:424-433.
11. Dellaero DT, Levin LS: Compartmentsyndrome of the hand:
Etiology,diagnosis, and treatment.Am J Orthop(Belle Mead
NJ)1996;25(6):404-408.
12. Friedrich JB, Shin AY: Management offorearm compartment
syndrome. HandClin 2007;23(2):245-254, vii.
13. Gelberman RH, Garfin SR,Hergenroeder PT, Mubarak SJ, Menon
J:Compartment syndromes of the forearm:Diagnosis and treatment.Clin
OrthopRelat Res1981;(161):252-261.
14. Stevanovic M, Sharpe F: Management ofestablished Volkmanns
contracture of
the forearm in children.Hand Clin2006;22(1):99-111.
15. Tsuge K: Treatment of establishedVolkmanns contracture.J
Bone JointSurg Am1975;57(7):925-929.
16. Ultee J, Hovius SE: Functional resultsafter treatment of
Volkmanns ischemiccontracture: A long-term followup study.Clin
Orthop Relat Res2005;(431):42-49.
17. McQueen MM, Gaston P, Court-Brown
Mark L. Prasarn, MD, and Elizabeth A. Ouellette, MD
January 2011, Vol 19, No 1 57
-
8/10/2019 Acute Compartment Syndrome Upper Extremity JAAOS
REVIEW
10/10
CM: Acute compartment syndrome:
Who is at risk? J Bone Joint Surg Br
2000;82(2):200-203.
18. Elliott KG, Johnstone AJ: Diagnosing
acute compartment syndrome. J Bone
Joint Surg Br2003;85(5):625-632.
19. Schnall SB, Vu-Rose T, Holtom PD,
Doyle B, Stevanovic M: Tissue pressuresin pyogenic flexor
tenosynovitis of the
finger: Compartment syndrome and its
management.J Bone Joint Surg Br1996;
78(5):793-795.
20. Ronel DN, Mtui E, Nolan WB III:
Forearm compartment syndrome:
Anatomical analysis of surgical
approaches to the deep space.Plast
Reconstr Surg2004;114(3):697-705.
21. Tompkins DG: Exercise myopathy of the
extensor carpi ulnaris muscle: Report of
a case.J Bone Joint Surg Am 1977;59(3):
407-408.
22. Schmidt GL, Uroskie JA: Isolated
compartment syndrome of the extensor
carpi ulnaris: A case report. Am J
Orthop (Belle Mead NJ)2004;33(10):519-520.
23. Whitesides TE, Heckman MM: Acutecompartment syndrome: Update
ondiagnosis and treatment.J Am AcadOrthop
Surg1996;4(4):209-218.
24. Docker C, Titley OG: A case of forearmcompartment syndrome
following a ringavulsion injury.Injury2002;33(3):274-275.
25. Cosker T, Gupta S, Tayton K:Compartment syndrome caused
by
suction.Injury2004;35(11):1194-1195.26. Bacal D, Lampman RM,
Hogikyan JV,
Wolk SW: Compartment syndrome ofthe arm and disseminated
intravascularcoagulation.Am J Orthop (Belle
MeadNJ)2001;30(5):422-423.
27. Kleshinski J, Bittar S, Wahlquist M,Ebraheim N, Duggan JM:
Review ofcompartment syndrome due to group Astreptococcal
infection.Am J Med Sci2008;336(3):265-269.
28. Ramos C, Whyte CM, Harris BH:Nontraumatic compartment
syndrome ofthe extremities in children.J Pediatr
Surg2006;41(12):e5-e7.
29. Cohen J, Bush S: Case report:Compartment syndrome after
asuspected black widow spider bite. AnnEmerg
Med2005;45(4):414-416.
30. Roberts RS, Csencsitz TA, Heard CW Jr:Upper extremity
compartmentsyndromes following pit viperenvenomation.Clin Orthop
Relat Res
1985;(193):184-188.31. Ragland R III, Moukoko D, Ezaki M,
Carter PR, Mills J: Forearmcompartment syndrome in the
newborn:Report of 24 cases.J Hand Surg Am2005;30(5):997-1003.
32. Benson LS, Sathy MJ, Port RB: Forearmcompartment syndrome
due toautomated injection of computedtomography contrast material.
J OrthopTrauma 1996;10(6):433-436.
33. Moen TC, Sarwark JF: Compartmentsyndrome following
intraosseousinfusion.Orthopedics2008;31(8):815.
34. Funk L, Grover D, de Silva H:Compartment syndrome of the
handfollowing intra-arterial injection ofheroin.J Hand Surg
Br1999;24(3):366-367.
35. Ananthanarayan C, Castro C, McKee N,Sakotic G: Compartment
syndromefollowing intravenous regionalanesthesia.Can J
Anaesth2000;47(11):1094-1098.
36. Hwang RW, de Witte PB, Ring D:Compartment syndrome
associated withdistal radial fracture and ipsilateralelbow injury.J
Bone Joint Surg Am2009;91(3):642-645.
37. Olson SA, Glasgow RR: Acutecompartment syndrome in
lowerextremity musculoskeletal trauma.J AmAcad Orthop
Surg2005;13(7):436-444.
38. Heppenstall RB, Scott R, Sapega A, ParkYS, Chance B: A
comparative study ofthe tolerance of skeletal muscle toischemia:
Tourniquet applicationcompared with acute compartmentsyndrome.J
Bone Joint Surg Am1986;68(6):820-828.
39. Heppenstall RB, Sapega AA, Scott R,et al: The compartment
syndrome: Anexperimental and clinical study ofmuscular energy
metabolism usingphosphorus nuclear magnetic resonance
spectroscopy. Clin Orthop Relat Res1988;(226):138-155.
40. Matava MJ, Whitesides TE Jr, Seiler JGIII, Hewan-Lowe K,
Hutton WC:Determination of the compartmentpressure threshold of
muscle ischemia ina canine model. J Trauma 1994;37(1):50-58.
41. Heckman MM, Whitesides TE Jr, GreweSR, Judd RL, Miller M,
Lawrence JH III:Histologic determination of the ischemicthreshold
of muscle in the caninecompartment syndrome model.J OrthopTrauma
1993;7(3):199-210.
42. Yuan PS, Pring ME, Gaynor TP,Mubarak SJ, Newton PO:
Compartmentsyndrome following intramedullaryfixation of pediatric
forearm fractures.
J Pediatr Orthop2004;24(4):370-375.
43. Boody AR, Wongworawat MD:Accuracy in the measurement
ofcompartment pressures: A comparison ofthree commonly used
devices. J Bone
Joint Surg Am2005;87(11):2415-2422.44. Maginn P, Elliot D: Upper
arm
fasciotomy: A new approach.J HandSurg [Br]1996;21:59-62.
45. Tarkin IS: The versatility of negativepressure wound therapy
with reticulatedopen cell foam for soft tissuemanagement after
severe musculoskeletaltrauma.J Orthop Trauma
2008;22(10suppl):S146-S151.
46. Yang CC, Chang DS, Webb LX:Vacuum-assisted closure for
fasciotomywounds following compartmentsyndrome of the leg. J Surg
Orthop Adv2006;15(1):19-23.
47. Hope MJ, McQueen MM: Acutecompartment syndrome in the
absence offracture.J Orthop Trauma 2004;18(4):220-224.
48. Vaienti L, Vourtsis S, Urzola V:Compartment syndrome of the
forearmfollowing an electromyographicassessment.J Hand Surg
Br2005;30(6):656-657.
49. Gelberman RH, Garfin SR,Hergenroeder PT, Mubarak SJ, Menon
J:Compartment syndromes of the forearm:Diagnosis and treatment.Clin
OrthopRelat Res1981;(161):252-261.
Acute Compartment Syndrome of the Upper Extremity
58 Journal of the American Academy of Orthopaedic Surgeons