Embed Size (px)
Citation preview

Acute Chest PainAcute Chest Pain“Can I go back to sleep?”“Can I go back to sleep?”
Dr. Hussam Al-FalehDr. Hussam Al-Faleh
Residents CourseResidents Course

OutlineOutline
Clinical presentationsClinical presentations Causes of chest painCauses of chest pain Clinical aids to diagnose Ischemic Clinical aids to diagnose Ischemic
CPCP summerysummery

It’s so painful I can’t It’s so painful I can’t breath!breath!

25yr old male with CP for 3 days25yr old male with CP for 3 days Sharp, central, worse with inspiration, Sharp, central, worse with inspiration,
and lying down, better sitting up, No and lying down, better sitting up, No relation to exertionrelation to exertion
H/o URTI 7 days agoH/o URTI 7 days ago No RF No RF BP 110/70, HR 100 bpm, triphasic BP 110/70, HR 100 bpm, triphasic
pericardial rubpericardial rub Wide spread ST elevation, PR Wide spread ST elevation, PR
depressiondepression Diagnosis: PericarditisDiagnosis: Pericarditis

The Sky is fallingThe Sky is falling

40yr old female40yr old female CP for 3 monthsCP for 3 months Can not be described, all over the chest Can not be described, all over the chest
and both shoulders, radiates to her head, and both shoulders, radiates to her head, continuous, not continuous, not ↑ ↑ exertion, but exertion, but exacerbated with emotional distressexacerbated with emotional distress
Divorced and physically abused by Divorced and physically abused by daughterdaughter
No RFNo RF Normal PE and ECGNormal PE and ECG Diagnosis: Psychogenic chest painDiagnosis: Psychogenic chest pain

Nothing is wrong with Nothing is wrong with me!me!

63yr male63yr male CP for last monthCP for last month Central burning, non radiating Central burning, non radiating
occurring only on exertion , occurring only on exertion , relieved with rest.relieved with rest.
HTNHTN PE & ECG NormalPE & ECG Normal Diagnosis: Typical anginal painDiagnosis: Typical anginal pain

I am like no other!I am like no other!

45yr male45yr male Upper back pain for 2 weeksUpper back pain for 2 weeks Never occurs at rest or change in Never occurs at rest or change in
posture, and provoked by effort relived posture, and provoked by effort relived with restwith rest
H/o Premature atherosclerosisH/o Premature atherosclerosis Normal PE & ECGNormal PE & ECG Diagnosis: very suspicious for ischemic Diagnosis: very suspicious for ischemic
painpain

Causes of Chest painsCauses of Chest pains


Panjue et al JAMA 1998;280,14

Goals of CP Goals of CP assessmentassessment
1- Need to r/o serious causes of chest 1- Need to r/o serious causes of chest pain “ pain “ what is the chance that my what is the chance that my patient will die due his underlying patient will die due his underlying conditioncondition” ”
2- Need to refer for further testing i.e 2- Need to refer for further testing i.e EST, V/Q scan , Angiogram etc..EST, V/Q scan , Angiogram etc..
3- If cause of CP is not serious how can i 3- If cause of CP is not serious how can i help? eg. NSAIDS for MSL CP, PPI help? eg. NSAIDS for MSL CP, PPI trial/GI consult for Refluxtrial/GI consult for Reflux

Risk stratificationRisk stratification
1.1. High risk AMI, High risk UAHigh risk AMI, High risk UA Lyse or cathLyse or cath
2.2. NSTEMI, LBBB, High risk UANSTEMI, LBBB, High risk UA Admit to CCUAdmit to CCU
3.3. Low risk UA, Non ischemic Low risk UA, Non ischemic painpain admit to ward or see as admit to ward or see as outpatient outpatient

HistoryHistory

Chest Pain description:Chest Pain description:
Location and radiation Location and radiation Character Character Onset and durationOnset and duration Aggravators and relieversAggravators and relievers Severity Severity Associated symptomsAssociated symptoms
Vital signs/ECG

Panjue et al JAMA 1998;280,14

Panjue et al JAMA 1998;280,14


Typical/Atypical CPTypical/Atypical CP
Typical:Typical: 1. Substernal1. Substernal
2. Burning/heavy/squeezing2. Burning/heavy/squeezing
3. 3. ↑ by exertion ↓ rest or NTG↑ by exertion ↓ rest or NTG


If clinically angina , If clinically angina , classify:classify:

Risk factorsRisk factors
Age : males ≥45, females ≥55Age : males ≥45, females ≥55 Gender Gender DM DM DyslipidemiaDyslipidemia HTNHTN SmokingSmoking Family history of Premature CAD: Family history of Premature CAD:
males ≤55 females ≤65 males ≤55 females ≤65 Metabolic syndrome Metabolic syndrome

Physical examPhysical exam
Vitals, Vitals, VitalsVitals, Vitals, Vitals BP (measure both sides)BP (measure both sides) Pulses paradoxicusPulses paradoxicus Heart rate (tachy/bradycardia)Heart rate (tachy/bradycardia) Respiratory rate Respiratory rate FeverFever O2 SatO2 Sat

Physical examPhysical exam
CVS exam:CVS exam:- JVPJVP- Carotid bruitCarotid bruit- Palpation of chest wall (where is the Palpation of chest wall (where is the
pain?)pain?)- Extra Heart sounds (S3 or 4)Extra Heart sounds (S3 or 4)- Murmurs (eg, early diastolic, )Murmurs (eg, early diastolic, )- Pericardial rubPericardial rub

Physical examPhysical exam
Chest exam:Chest exam:- TracheaTrachea- Breath soundsBreath sounds
Abdomen:Abdomen:- - TendernessTenderness

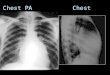
InvestigationsInvestigations
ECG:ECG:- NORMAL ECG DOES NOT ROLE OUT NORMAL ECG DOES NOT ROLE OUT
ISCHEMIAISCHEMIA- Serial ECG’sSerial ECG’s- Always compare to an old ECGAlways compare to an old ECG- ST ST ↑ (localized vs. Wide spread)↑ (localized vs. Wide spread)- ST ↓ST ↓- T wave inversion (location and symmetry) T wave inversion (location and symmetry)
or peakingor peaking

ECG (cont.)ECG (cont.)
- Q waves (new)Q waves (new)- New conduction defects (LBBB/RBBB)New conduction defects (LBBB/RBBB)- Voltage/electrical Voltage/electrical
alternans/Tachycardiaalternans/Tachycardia- PE patterns (Q1 S3 T3), RBBB,PE patterns (Q1 S3 T3), RBBB,

Other investigations Other investigations (PRN)(PRN)
Depending on Hx/PEDepending on Hx/PE CBCCBC D-dimersD-dimers ABG’sABG’s CXRCXR

Troponins I & TTroponins I & T
Most sensitive and specific cardiac Most sensitive and specific cardiac markersmarkers
Rise 3-12hr after onset of CPRise 3-12hr after onset of CP Peak I (24hr), T (12hr-2 days)Peak I (24hr), T (12hr-2 days) Return to normal 5-14 daysReturn to normal 5-14 days Has both diagnostic and Has both diagnostic and
prognostic valuesprognostic values Sample at baseline and after 6-8hr Sample at baseline and after 6-8hr

ConclusionConclusion
History and physical are corner History and physical are corner stones in diagnosis of Chest painstones in diagnosis of Chest pain
Ensure that patient is stable Ensure that patient is stable before taking a detailed historybefore taking a detailed history
Serial ECG’s and cardiac enzymes Serial ECG’s and cardiac enzymes for selected patientsfor selected patients