Embed Size (px)
Citation preview
Acupuncture treatment of chronic tension headache -- a controlled cross-overtrial
Per Evald Hansen, John Hersted Hansen
CEPHALALGIA Hansen PE, Hensen JH. Acupuncture treatment of chronic tension headache-a controlledcross-over trial. Cephalalgia 1985;5:137-42. Oslo. ISSN 0333-1024
In a controlled trial the effect of traditional Chinese acupuncture v. placebo acupuncture wasevaluated in 18 patients with chronic tension headache (mean disease duration 15 years). Allpatients suffered from daily or frequently recurring headache, the intensity of which was recorded bythe patient over a period of 15 weeks. Each patient was treated by traditional Chinese acupunctureas well as by placebo acupuncture in a cross-over design following randomization. Each period oftreatment comprised six treatments. Traditional Chinese acupuncture was found to be significantlymore pain-relieving than placebo acupuncture, according to the pain registration of the patientsthemselves. The pain reduction was 31%. Acupuncture is therefore found to be a reasonabletreatment for chronic tension headache. ž Placebo acupuncture, tension headache, traditionalChinese acupuncture
Per Evald Hansen, John Hersted Hansen, University Department of Neurology, AarhusKommunehospital, DK-8000, Aarhus C, Denmark; Correspondence to Per Evald Hansen,Department of Neurology, Sønderborg sygehus, DK6400 Sønderborg, Denmark; Accepted 198505 22
Tension headache includes sensations of tightness, pressure, or constriction, widely varied in intensity, frequencyand duration, sometimes chronic, and commonly suboccipital (1). It is associated with sustained contraction ofskeletal muscles and without permanent structural change. As a chronic or frequently recurring condition, it hasmajor medical and socioeconomic importance (2). The medical treatment and physiotherapy often have onlytemporary effect (3, 4), while electromyographic feedback training seems to be effective (5).
It has been reported that acupuncture treatment of tension headache is effective (6, 7, 8), and thatelectromyography can provide objective evidence of the effect of acupuncture (8). Furthermore, it has beenreported that insertion of a needle with or without injection into a trigger point may produce immediate as well asprolonged analgesia (9, 10).
We have carried out a controlled study of the effect of traditional Chinese acupuncture v. placebo acupunctureon chronic tension headache.
Material and methods
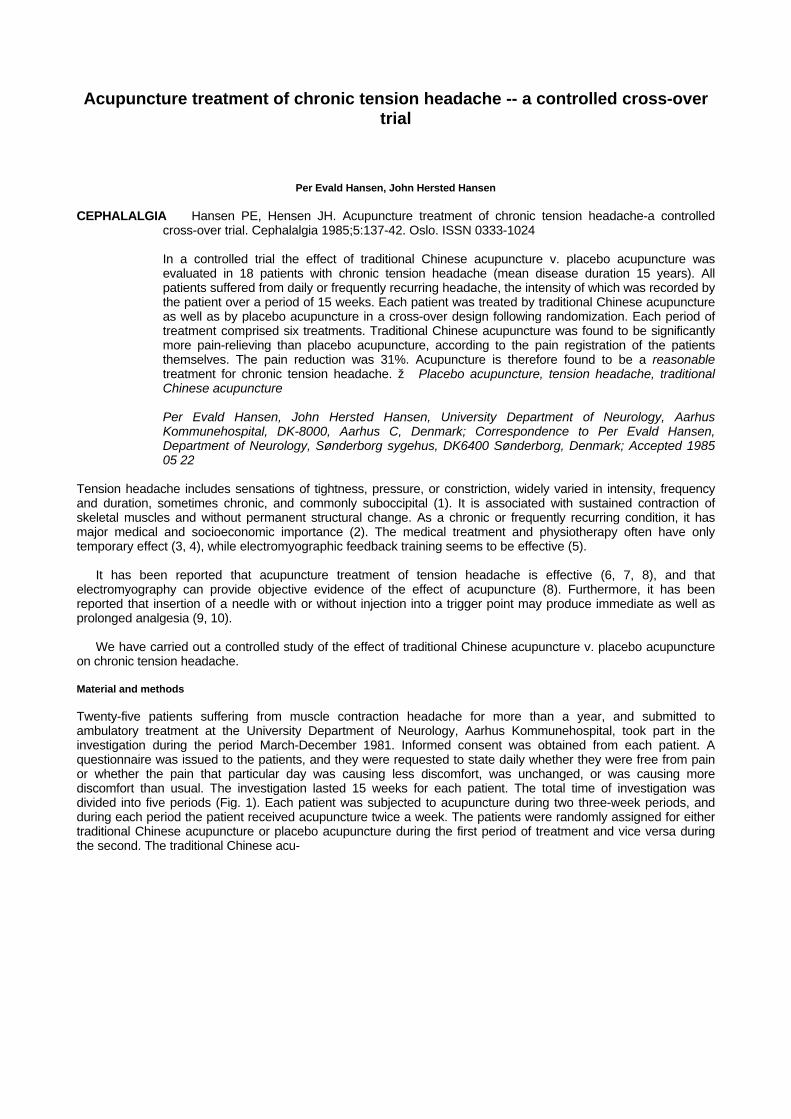
Twenty-five patients suffering from muscle contraction headache for more than a year, and submitted toambulatory treatment at the University Department of Neurology, Aarhus Kommunehospital, took part in theinvestigation during the period March-December 1981. Informed consent was obtained from each patient. Aquestionnaire was issued to the patients, and they were requested to state daily whether they were free from painor whether the pain that particular day was causing less discomfort, was unchanged, or was causing morediscomfort than usual. The investigation lasted 15 weeks for each patient. The total time of investigation wasdivided into five periods (Fig. 1). Each patient was subjected to acupuncture during two three-week periods, andduring each period the patient received acupuncture twice a week. The patients were randomly assigned for eithertraditional Chinese acupuncture or placebo acupuncture during the first period of treatment and vice versa duringthe second. The traditional Chinese acu-
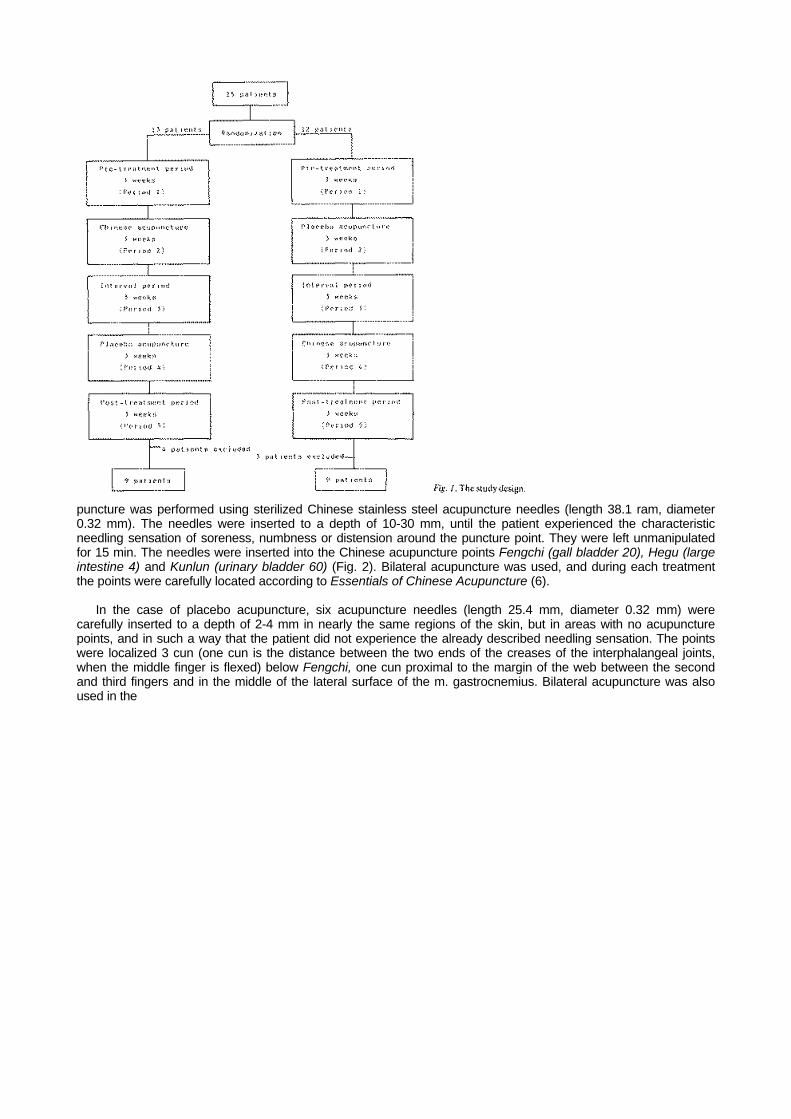
puncture was performed using sterilized Chinese stainless steel acupuncture needles (length 38.1 ram, diameter0.32 mm). The needles were inserted to a depth of 10-30 mm, until the patient experienced the characteristicneedling sensation of soreness, numbness or distension around the puncture point. They were left unmanipulatedfor 15 min. The needles were inserted into the Chinese acupuncture points Fengchi (gall bladder 20), Hegu (largeintestine 4) and Kunlun (urinary bladder 60) (Fig. 2). Bilateral acupuncture was used, and during each treatmentthe points were carefully located according to Essentials of Chinese Acupuncture (6).
In the case of placebo acupuncture, six acupuncture needles (length 25.4 mm, diameter 0.32 mm) werecarefully inserted to a depth of 2-4 mm in nearly the same regions of the skin, but in areas with no acupuncturepoints, and in such a way that the patient did not experience the already described needling sensation. The pointswere localized 3 cun (one cun is the distance between the two ends of the creases of the interphalangeal joints,when the middle finger is flexed) below Fengchi, one cun proximal to the margin of the web between the secondand third fingers and in the middle of the lateral surface of the m. gastrocnemius. Bilateral acupuncture was alsoused in the
placebo procedure, and the needles retained for 15 min unmanipulated.
Before inclusion in the trial the patients were informed both verbally and in writing that the purpose of the investigation was tocompare the effect of two different techniques of acupuncture widely used in China and Europe. They were not allowed to discussthe effects of the treatments with the acupuncturist (PEH), nor were they allowed to discuss anything about the actual procedureswith the other investigator (JHH), who was the only one to receive the patients' registration forms. Both investigators aimed at auniform neutral contact with the patients during the various periods, and during the acupuncture treatments themselves theacupuncturist did not speak with the patients. The acupuncture records and the clinical records were kept apart, and the code wasnot broken until after the end of the investigation.
Seven of the patients were excluded (three were unable to fill out the patient calendar regularly, three suffered frompsychogenic headache, defined as headache, which is considered as a delusional or a conversion reaction and a peripheral painmechanism is nonexistent (1), and one was so hypersensitive that she experienced a pronounced needling sensation even duringplacebo acupuncture) (Fig. 1). All seven patients were excluded before the code was broken. So the material ultimately consistsof 18 patients (12 females, 6 males, aged 16-69, mean 36.1 years).
The duration of the disease was 1.5-60 years (mean 15 years). All patients had tried prolonged and varied medical treatmentsand physiotherapy without satisfactory results.
By means of the daily headache registration of the patients a period index (PI) has been calculated using the formula: PI = 0 ×A + 1 × B + 2 × C + 3 × D, A being the number of headache-free days in the period, B the number of days in the period with lessheadache than usual, C the number of days in the period with usual headache, and D the number of days in the period with moreheadache than usual. As the PI has been calculated on the basis of the headache registration in the three non-treatment periods,the duration of each being 21 days (A + B + C + D = 21), the range of the PI = 0-63.
Results
The PIs of the group (9 patients) who received acupuncture as the first treatment are shown in Table 1, and those of the group (9patients) who received placebo as the first treatment in Table 2.
Comparing the PI-means of periods 1, 3, and 5 in the two groups separately, a reduction is seen in periods 3 and 5 (Table 3).In both patient groups, statistically significant differences appear (Friedman two-way analysis of variance by ranks, p = 0.025, 2µ £0.05). Within the groups the differences are only statistically significant between period 1 and the post-acupuncture period (Odeh'snon-parametric test for the distribution of the maximum sum of ranks, p = 0.048, 2µ £ 0.05) (11).
Table 1. Period index (PI) among ninepatients receiving Chinese acupunctureas the first treatment.
Period no.Patient no. 1 3 5
1 46 43 514 31 28 215 41 4 149 43 35 4011 50 0 012 32 33 2115 45 37 4224 52 32 4025 40 26 42
Mean 42.2 26.4 30.1
Carry-over effect (i.e. interaction between treatment and time) is tested by adding for each patient the PI-valuesfor periods 3 and 5 and comparing the results for the two groups (Mann-Whitney rank sum test for independentsamples, value for the lesser sum
Table 2. Period index (PI) amongnine patients receiving placeboacupuncture as the first treatment.
Period no.Patient no. 1 3 5 2 42 42 42 3 34 33 23 7 38 29 30 8 41 21 32 10 47 47 39 16 49 26 21 18 17 27 14 20 54 45 43 22 44 47 34Mean 40.7 35.2 30.9
Table 3. The distribution of period index means.Period
1 3 5 PAcupuncture/placebo 42.2 26.4 30.1 0.025Placebo/acupuncture 40.7 35.2 30.9 0.025
Friedman two-way analysis of variance by ranks.
of ranks = 78.5, significance limits for 2µ £ 0.10: 66-100) (12). Thus, it can be concluded that no carry-over effect isdetectable. Period effect (i.e. time influence) is tested by subtracting for each patient the PI-values for period 3 andperiod 5 and comparing the results for the two groups as for carry-over effect (value for the lesser sum of ranks =68.5, significance limits for 2µ £ 0.05: 62-109) (12). It is concluded that no period effect is detectable. With noconfounding carry-over effect and period effect it is permissible to seek for a treatment effect (i.e. differencebetween the regimes). Thus, putting the two groups together (Table 4), the reduction of PI is significantly greater inthe post-acupuncture periods as compared with the post-placebo periods (Wilcoxon's test for pair differences, p <0.05, one-tailed test). Thus, a statistically significant treatment difference is detectable.
The PI-median values (or intervals) for all patients for period 1, post-placebo period, and post-acupunctureperiod (with distribution-free confidence limits, 2µ £ 0.05, in parentheses) are as follows: 42-43 (38-47), 33-40(21-42), 32 (23-37). So, there is a considerable overlap between the confidence limits for the post-placebo periodand the
Table 4. Period index (PI) means for both treatment groups.PI mean before treatment (a) 41.45PI mean after placebo acupuncture (b) 32.65PI mean after Chinese acupuncture (c) 28.65PI mean proportionate decrement followingplacebo acupuncture (in percentage) a-b/a × 100 21%PI mean proportionate decrement followingChinese acupuncture (in percentage) a-c/a × 100 31%
between the limits for period 1 and the post-acupuncture period.
The total PI-mean proportionate decrement following Chinese acupuncture amounts to 31% (Table 4)-roughlycorresponding with the decrement in PI-median values for the same periods.
Discussion
We have previously described the difficulties by adapting the traditional Chinese acupuncture to the method ofinvestigation of western medicine (13). In an uncontrolled trial, Mann & Halfhide discovered that Chineseacupuncture gave rise to considerable improvement of unspecified and intractable headache in 80% of theirpatients (14). In our patients with specified chronic and otherwise intractable tension headache, we noticed a totalPI-mean reduction of only 31%, probably because we reduced the effect of Chinese acupuncture by adapting it tothe settings of a clinically controlled trial.
We have also previously discussed the question whether the chosen placebo acupuncture, i.e. subcutaneousinsertion of needles in skin areas with no acupuncture points and causing no needling sensation, is a real placebotechnique (13). With such a technique, we noticed a placebo effect of 21%.
We did find a tendency towards a fall in PI throughout the whole investigation, but no carry-over effect or periodeffect was apparent.
It may be argued that this study is not a double-blind design because the acupuncturist knows the therapy he isoffering the patient, who may therefore be manipulated by the doctor's bias. In order to minimize any possibleinfluence, there was no verbal communication between the patient and the acupuncturist, except the patient sayingyes when the needling sensation was obtained.
A weak aspect of this trial is that seven out of 25 patients had to be excluded. The fact that three patients didnot fill in the patient schemes regularly may indicate that they experienced no effect of acupuncture. Inclusion ofthose three patients would have brought about a reduction in the treatment differences. However, we have notbeen able to calculate this reduction because the patient schemes were not filled in.
The three patients suffering from psychogenic headache should probably have been excluded before therandomization according to the trial protocol, but it was not until during the trial that the diagnosis became evident.Psychogenic pain will often be aggravated during acupuncture, whether traditional or placebo. Inclusion of the threepsychogenic headache patients might therefore increase the risk of a Type II error (i.e. the probability of a reallyexisting difference not being detected between the two regimes). We have not made an error excluding these threepatients, because they were excluded before the code was broken, and without knowing their pain registration.Later we experienced that their pain schemes were so irregularly filled out that We could not use them in thestatistical analysis. Exclusion of the seventh patient was necessary because the needling sensation is essential forobtaining a therapeutic effect (15), and because we have defined placebo acupuncture in this trial as superficialneedling without obtaining needling sensation. If we had included the patient the risk of a Type II error would haveincreased.
Bearing in mind the above-mentioned difficulties, our conclusion is that traditional Chinese acupuncture appearsmore pain relieving than placebo acupuncture, as evaluated by the daily headache registration of the patients.
The clinical level of significance (i.e. the minimal relevant difference between treatment and placebo effect) canonly be established arbitrarily (16). Although the difference demonstrated in this investigation from a clinical point ofview may be rather small, it is our opinion that it is reasonable to use acupuncture as a treatment for chronic andotherwise intractable tension headache if the PI-mean proportionate reduction is about 33%. Obviously, there is aneed for conducting an unpaired large scale trial contrasting acupuncture treatment and various more establishedtreatments of chronic tension headache.
References
1. Ad hoc committee on classification of headache. Classification of headache. JAMA 1962;179:717-18
2. Hollnagel H, Nørrelund N. Headache among 40-year-olds in Glostrup. Ugeskr Læger1980;142:3071-7
3. Dalessio DJ. Wolff's headache and other head pain. New York: Oxford University Press, 1972
4. Lance JW. Mechanism and management of headache. London: Butterworths, 1978
5. Bruhn P, Olesen J, Melgaard B. Controlled trial of EMG feedback in muscle contraction headache.Ann Neurol 1979;6:34-6
6. Essentials of Chinese acupuncture. Beijing: Foreign Languages Press, 1980
7. Bischko JJ. Acupuncture in headache. Res Clin Stud Headache 1978;5:72-85
8. Jensen LB, Tallgren A, Troest T, Jensen SB. Effect of acupuncture on myogenic headache. Scand JDent Res 1977;85:456-70
9. Frost FA, Jessen B, Siggaard-Andersen J. A controlled, double-blind comparison of Mepivacaineinjection versus saline injection for myofascial pain. Lancet 1980;1:499-501
10. Lewitt K. The needle effect in the relief of myofascial pain. Pain 1979;6:83-90
11. Sachs L. Statistische Methoden. Berlin-Heidelberg-New York: Springer-Verlag, 1976
12. Koch GG. The use of non-parametric methods in the statistical analysis of the two-period changeoverdesign. Biometrics 1972;28:577-84
13. Hansen PE, Hansen JH. Acupuncture treatment of chronic facial pain-a controlled cross-over trial.Headache 1983;23:66-9
14. Mann F, Halfhide A. Treatment of headache by acupuncture. Med World 1963;98:284-7
15. Chang HT. Acupuncture analgesia today. Clin Med J 1979;29:7-16
16. Feinstein AR. Quantitative significance and statistical indexes for a contrast of two groups. ClinPharmacol Ther 1980;27:567-78












![Lapkas Tension-type Headache [Autosaved]](https://img.dokumen.tips/doc/110x75/577c7e1a1a28abe054a08fb8/lapkas-tension-type-headache-autosaved.jpg)















![Tension-type headache [1]](https://img.dokumen.tips/doc/110x75/58763c381a28ab206f8b94e2/tension-type-headache-1.jpg)
