Embed Size (px)
Citation preview

HABITUAL PHYSICAL ACTIVITY AND THE ASSOCIATION
WITH DISEASE SEVERI'N AND EXERCISE CAPACITY IN
CYSTIC FIBROSIS: A PILOT STUDY
by
Susan L. Pollock
A thesis submittcd in confonnity with the requhments for the degrce of Master of Science
Graduate Department of Community Health University of Toronto
The aushor has granted a non- exchisive licence allowing the National L h u y of Canada to npioduce, loan, distnite or sel1 copies of this thesis in microform, p a p or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the
may be printed or othawise teproduceci without the author's permission.
L'autnn a accordé me licence non exchisive permettant A la BibIiotMque nationale du Canada de np.oduke, p*, dimiiuer ou vendre des copies de cette thbe sous la fonne de microficbeI/nhn, de reproduction sur papier ou sin format 61ectronique.
L'auteur conserve la propnCtC du droit d ' a m qui protège cette thèse. Ni la thèse ni &s exbraits substantiels de celie4 ne doivent être imprimés ou auûement reproduits sans son autorisation.

Master of Science - 2000
Swan L Pollock
Graduate Department of Community Health
University of Toronto, Canada
Objectives: To detennine rccnlltment and compliance rates for the collection of habitual physicd
activity data, to profile trends in habitual physical activity patterns, and to detennine if a positive
relationship exists bctween lung function, habituai physical activity, nutritional status and
exercise capacity in cystic fibrosis (CF) patients.
Methods: For this cross-sectional pilot study, 40 CF patients were recdted from the CF clinic
at the Hospital for Sick Children over a three month period. Patients providecl a self-report of
their habitual physical activity patterns using two suwey instruments: the Habitua1 Activity
Estimation Scale (HAES), and the 7-Day Activity Diary. Rilmonary function and nutritional
status data were coliected from clinic records. Data on exercise capacity were available for a
subset of patients who completed their annual exercise test on or near to 4 3 months) the study
recrui tment date.
Resulis: High necmitment (89%) and compliance ( M E S , 100%; Acrivify Diary. 82%) rates
indicateâ the feasibility of collecting habinial physicai activity data in this study population.
Positive and sipficant correlation coefficients were demonstraîed bctween habituai physical
activity (HAES), lung hinction, nuiritional status and e x d s e capacity. Patients reportcd
significantly higher Total Activity scores (mild to vigorous physicai activity) for a typical
weekend day (HAES, 8.0 f 3.0 hodday; Activity Diaty, 4.8 f 2.3) than weekàay (HAES, 5 7 k
2.8; Actiwity Diary, 339 f 1.2). The Total Activt'iy score for a typicd weekday, deriveci fiom the
HAES, was demonstcated to be a sigeificant predïctor of fmed expiratory volume in one second
(Fm), the most important vaiabk in desctibhg lmg discase.
Co11cIiwio119: These pilot study rcsults will sme as the prceursor for a longitudùial follow-up
study that will begin to aâ&ess the direction of the causal ralaîiortship beniveen habitual physical
activity and FEVI in CF.

ACKNOWLEDGEMENTS
To Mary Corey, my supervisor, who provideci me with both opporiunity and inspiration. T h a h
for always reminding me of the "big pictm" and for allowing me to find my own way.
To Jane Schneiderman-Walker, my fnend and committce member who shand my vision and
who taught me about the importance of "pruning." Thanks for naduig and n-reading my thesis
and for never king shy to voice your opinions!
To Jacek Kopec and Joe Reisman, members of my cornmittee who provided me with helpfd and
invaluable feedback throughout the various phases of my thesis.
To the CF patients and their families who generously àonated their time to this study. Thanks for
compkting your Activity Diaries with such enthusiasm!
To the staff of the CF clinic who offereâ their assistance to me whenever called upon. Thank-you
for a i i of your invaluable help.
To Petet Katzmarzyk, Susan Jagial and Mary Chipman for nading and conûibuting to my thesis.
To Janey, whose emails and conversation entertained me at the worst and best of times, and
whose honesty and friendahip contnbuted to the successfur completion of this project.
To Lenny, for her tales of Ted and Ca~per, and for her contribution of dog pictures to the office
wds. Thanks for rnaking sure thaî I wasn't foqetting to eat, and for aii your advice.
To the nst of th team in Rwm 5406-thanks f a your support.
To aîi my fncnds who never gave up on m. Thenks for un&rstanding my absence durlng the
last few months.

To my Epidemiology coileagues, especiaIly Ali. Sue, Micheiie and Laurie, it's been fun! I
couldn't have asked for better classrnates.
To mom, dad, Heather, Marc, Ali, Trev, Grandpa, Maddie and Natasha, for believing in me.
Thank-you for instilling in me a love of learning and for teaching me the value of perseverance.
To Darren, for his love, support, and sense of humor, and for providing me with welcome
diversions fmm my work. n i a t h for helping me to open my eyes and see Life beyond my thesii.

CONTENTS
2 BACKGROUND mea.ea-..-....a ..ma..nama.ma..anna.nwM*a*w a . 4
2.1 CYSTIC FIBROSIS ........... .+ ... .. ......... ......... ...... * ........ *.* .............. ............................... O ................... 4
2 3 PHYSICAL A C ï M T Y IN CHILDREN AND YOUTH .................................................................. 8
.................................................................................................................... 2.2.1 HEALTH BENEFWS 8
........................................................................ 2 3 3 PATTERNS IN CHROMCAUY IW, PATIENTS 9
............................................................... 2.23 EXERUSE CONSIDERATIONS IN CF PATIENTS 9
................................................................................. 2 3 EXERQSE TRAINING PRûûRAMS IN CF 12
23.1 CHARACERiSTICS OF EXERUSE PRûGRAMS .................................................................. 12
.................................................... ............... 23.2 SUPERVISED PROGRAMS ....................*................ 13
2A3 UNSUPERVISED PROGRAMS ................................................................................................... 16
23.4 CHALLENGES OF TRAINING PRûGRAMS .. ............................ .............................................. 17
2.4 RELATIONSHIP BETWEEN HABïïüAL PHYSICAL ACMWTY. LUNG FUNCTION.
NUTRPfIONAL STATUS. AND EXERCISE CAPACITY IN CF ....................................................... 18
2 3 . OF PHYSICAL ACTMTY ................. ........ .................................................... 20
25.1 DOUBLY LABELED WATER .................................................................................................... 20
2.5.2 OBSERVATION ........................O ..................................... .............................................. 21
2.53 MOVEMENT ASSESSMENT DEVICES .... ........C..tt.....t-..t... .... .....,,. 21
......................... 23.4 HEART RATE MOmORING........ ..*e*.*+.o.*+.**.C...*.*...***.*H.**t*... ..... 22

3 M O W - ..m...mm.m~.m*.*o.*no~~omeom~.em~~~~mm.m~.m.muH~em...mm.a.~o.*~ ......m...... 32
3.1 OVERVIEW OF THE STUDY DESIGN o.................. ....................... ...........................O............... 32
3.2 PRACITCAL PLANNING AND IMPLEMENTATIOEJ .......................................................... 32
... .................................................................................... 33 SUBJECT SELECTION....... ......r.....r+....r.. 34
33.1 ELlGlBILSrY CRï ïERk ............................................................................................................ 34
33.2 SUBECT RECRUITMENT ...................................................................................................... 34
3.4 DATA COLLECïION ..................................................................................................................... 35
3.4.1 SUBJECT DATA .................... ............*......., .................................................................... 3 5
3.42 PULMONARY FUNCTION ......................................................................................................... 36
3.43 MEASUREMENT OF HA8lTUAL PHYSICAL A C T M T Y ..................................................... 37
3.43.1 THE HABlTüAL ACTMTY ESTIMATION SCALE (HAES) .................................... . . . . 37
3.432 THE 7-DAY ACI'NITY D M ................................................. t,........ ..................... 38
3.4.4 ADMINISTRATION OF THE HAES AND THE A C T M W DIARY ............................O................ 38
3.43 NUTRIMONAL STATUS .. .................*..*..m.........-.. ............................................................... 39
....... 3.4.6 EXERCISE CAPAQTY ..r..........r.i..r~.~ttt~..~..~..*~~~*~.......~~....*~......*-*......*-..**..~....***... 40
3.4.7 COMPLIANCE WïïH PHYSIOTHERAPY r ~ ~ ~ ~ ~ . H ~ . ~ ~ ~ ~ ~ ~ ~ . ~ ~ o ~ o H ~ o ~ ~ ~ t . ~ o o C ~ .... ..H.*o..w.oH*.**-.*-*. 42

3.43 POTENTIAL CORR5ATES OF PHYSICAL ACTMTY PARTIQPATION** ...c.**..t,Ce**.. 42
................................................................................................................................. 3.5 S m SIZE 44
3.6 DATA ANALYSIS ........... ...... ................* ....*..*...........*.*..................*...........-.. .......*...*............. 44
306.1 DATA SCORING .......................................................................................................................... 44
3.6.1.1 THE HAES ................................................................................... ....................... O.... 4 5
3.6.l.2 THE ACMWTY DïARY ................... , ..................................................................................... 45
3.6.13 ACïiVïîYTYPE ......................*............................................................................................... 46
3.6.2 DATA QUALiTY CONTROL ...*.......................... ,., ......*............................................................. -46
3.63 DESCRPTNE STATISTICS ..........*......... ....., ............................................................................. 48
... 3.6.4 PEARSONS CORRELAïïON ..................*...*............* ..,. 48
3.6.5 REGRESSION ANALYSES .............................................................. .................................... 4 9
3.6.5.1 MULTIPLE CORRELATION ................ .....,..*..*..*.....*....... ..................................................... 49
3.6.5.2 MODEIJNG FEVI AS OUTCOME VARIABLE ...................*......................................... 50
4.1.1 PATIENT CHARACi'ENSTICS ..........................~............................................................... 5 1
4Al.l Si'üDY PNUiciPANïS .*...*+....*....*...*..o......... W.* .....l..t..**...t.........* ..C...*.t....l..*..*l.*.*..H..*. .*..*...O 51
4.1.1.2 CF POPULATION VALUES ........... .................................................... ......... 5 1
..... .... ...... 4.1.13 STüDY REFüSALS ...... ...................... ..... ».. .......................................................... 52
4.l.2 MEASUREMENT OF HABiTüALPKYSICAL ACTIVITY .......*...... .........U....*................ 53
............................... 4.l.2.l THE HAES .....................*..*... ............ ..... ............. ................ 53
................................. 4.l.2.2 THE 7-DAY ACTIVfTY DfARY ... .....HH.......H...........C......e.H..C.....).. 55

4.133 A COMPARISON OF DATA FROM TEE HAES AND THE ACTfVITY DIARY .........-.... 58
4.13 PULMONARY FüNCTION .......................... ....... ...............O........... 58
4.1.4 ANNUAL EXERCISE TESTIN0 ................................................................................................. 59
................................................................................ 4.1A.i A SUB4 AMPLE OF STUDY PATIENTS 59
4.1.43 ASSESSMENT OF EXERCISE CAPACITY ....................................................................... 5 9
4.1.S COWUANCE W ï ï H PHYSlOTHERAfY ................................................................................ 6û
4.1.6 PARENT QUESMONNAIRE ....................................................................................................... 6û
............................................................................................ 4.1.7 A C T N ï ï Y CLASSiFiCATION 6 2
4.1.73 PERSONAL CARE ................................................... ... .......... .. ............................................... 63
4.1.73 DOMESTIC WORK .+................................................................................................................. 63
4.1.73 SCHOOL.RELATED. ............................................................................................................... 6 3
4.l.7.4 EMPLOYMENT .......... r.c ............................................................................................... 6 3
4.1.73 UNSTRUCX'URED PLAY ..................... .. ............................................................................. ...... 64
4.1.7.6 WALKING .......... .........,.+..*.+.... .................................................................................................. 64
4.1.7.7 SPORT ........................................................................................................................................ 65
4.1.7.8 UND- ................................................. ... ......................................................................... 65
4 3 CORRELATION ANALYSES .......................................O..... t., ........................................................ 72
4.2.1 THE HAES AND THE ACrrVPrY DiARY ...........* ....... .... .......... ... 72

43.6 A SUMMARY OF ReSULTS FROM CORRELATION ANALYSES .......................* ................ 80
4 3 REGRESSION ANALYSES ...... ................... .................................................................................. 81
43.1 MUTLIPLE CORRELATION ...........*o.H.... .... te ... .............. 82
4A1.1 SüMMARY OF MULTIPLE CORRELATION ....................................... ...... 84
4 3 2 MODELJNG FEVi AS THE OUTCOME VARIABLE ............................... ......... 93
4 . 1 A G ............................................................................................................................................ 94
432.2 PERCENT OF DEAL WEIGHT ............................................................................................... 94
43.23 HAES ACTMTY SCORES ...................................................................................................... 95
432.4 MULTIPLE VARIABLE M O D U .......................................................................................... 95
........................................... 43.25 SUMMARY OF FINAL MULTIPLE REGRESSION 97
S D I S ~ ~ I O N w m m m m ~ m m ~ m m m m m ~ w m ~ * m m w m m m n m - m m ~ m n ~ m m m m w w m m m ~ * m m ~ * ~ ~ m + n m ~ m ~ ~ * * m w * m w m m m ~ m m m m m w ~ m m w w w 99
5.1 INTERPRETATION OF RESULTS ............................... ............................................................... . 99
5.1.1 FEASIBILlW ............................................................................................................................... 99
5.13 HABïïüAL PHYSICAL ACMWTY ......................................................................................... Iûû
5.l.2.l TRENDS FOR THE HAES AND THE A C T M T Y DIARY .................................................. 1ûû
5.13.2 COMPARISON OF THE HAES AND THE A C î M T Y DIARY ........................... ...,... ..... 102
S.13 EXERCISE CAPACl'iY ........................... ..*.... ........................................................................... 103
5.1d C O M P W C E ~PHYSIOTHERAPY ......... ................ .. ........., ..................................... 104
5.l.S PARENT QUESTlONNAIRE.. ................................................................................................... 104
5.1.6 ACMViTY QIPLSStmCATION ................. .....r.*.r.+................ ...................................... ....... *.o.... 1M
5.1.7 SIMPLE CORRELATION OF ACI'MTY SCORE WlTH FEVt .. ..............n...-.....H.......t.. -- 106
SA8 REGRESSION ANALYSES ~ ~ ~ * ~ ~ ~ ~ n ~ ~ ~ ~ ~ ~ ~ b ~ o ~ ~ ~ o ~ ~ ~ ~ ~ * * ~ ~ ~ ~ ~ o ~ * * ~ ~ ~ o * ~ ~ ~ b ~ ~ ~ ~ ~ ~ * ~ ~ I ~ * ~ ~ ~ ~ ~ ~ - ~ ~ ~ ~ o ~ ~ C C ~ ~ ~ ~ ~ ~ m m ~ Io8

................................................................... .............................. 5.2 METIIODOLOGICAL ISSUES W.* 108
53.1 STUDY LIMPTATIONS .................... ......... .......................................................................... 108
.................... S.Zl.1 COMPLIANCE WITH, AND RETURN OF. THE 7-DAY ACTIWI'Y D m 109
52.1.2 RANDOM AND SYSTEMATIC ERROR IN SELF-REPORT OF A C T M T Y ..................... 109
........................................................................... 5.2.13 GENERALEABIlSrY OF THE RESUtTS 110
53.1.4 DIRECTION OF CAUSALSI"Y ......................................................................................... ..... . 111
5.23 SUGGESTED MODIFICATIONS OF THE CZTRRENT PROTOCOL. ................................... 111
5 3 FUTURE DIRECTIONS ......................................,........ ................................................................. 112
....................................................................... 53.1 PROPOS AL FOR A LONGITUDINAL STUDY 112
5.4 CONCLUSIONS ............................................................................................................................ 114
REFERENCE LIST ............................................................................................................................ 116

LIST OF TABLES
.......................... TABLE 3.1 SUMMARY OF THE SURVEY INSTRUMENTS ..,,,...................... 43
TABLE 3.2 ACTMTY SCORES COMPJLED FROM THE HAES AND TEIE ACTMTY
D M Y ...............-.........*........*.......*...*.......... .......................................................................................... 47
.........*................... .......*.......................** TABLE 4.1 STUDY PATIENT cf fCTERiST ICS ...... 5 2
TABLE 4.2 CF PATIENT CHARACTERISTICS FOR ALL ELIGlBLE PATIENTS ATTENDMG
...................................................................................... CLINIC FROM MARCH 9-JUNE 4. 1999 5 2
TABLE 4.3 A C T M T Y HOURS COMPILETl FROM THE HAES .................................................... 55
TABLE 4.4 ACTlVITY HOURS COMPiLED FROM THE ACTMTY DMRY ............................... 56
TABLE 4.5 PERCENT OF PREDICTED PWONARY FUNCTION .............................................. 58
TABLE 4.6 EXERCISE PARAMETERS.* ....... , ....................... ............................................. 6 0
TABLE 4.7 CORRELATES OF PHYSICAL ACTMTY PARTICIPATION .............. 62
TABLE 4.8 CORRELATION BETWEEN THE TOTAL AND HXGH A C T M T Y SCORES OF
THE KAES AND THE ACTMTY DIARY ......................................................................................... 72
TABLE 4 3 CORRELATION FOR WEEKDAY A C T M T Y SCORES OF THE HAES AND THE
A m DIARY ...... ............t.......t.....t..- 74
TABLE 4.10 CORRELATION FOR WEEKEND ACMVïW SCORES OF THE HAES AND THE
ACT'MTY DLARY ...m. ...*..****.+.****".*.*+.*...*.......+.*.*....*.*.*..**.....*..r.......~t...*.......~.....t*........*...~.*..**....**.. ...O 75
TABLE 4.11 CORRELATION FOR WEICiHTED A m SCORES OF THE HAES AND
THE ACTMTY DIARY .........................O................ ...o.............w.......w..........w...................~......*.t........ 76
... TABLE 4.12 CORRELATION BETWEEN WEEKDAY AND WEEKEND A~IVITY SCORES n
TABLE 413 CORRELATION ANALYSIS FOR FEVl .........,...,,,...........u.~e.~~..e..n..~.....CH . . 78

TABLE 4.14 CORRELATION BETWEEN ACTMTY SCORES AND POTENTIAt
CORRELATES OF PEZYSICAL ACTMTY PARTiCJPAmON ..................................................... .... 79
.................................... TABLE 4J5 MULTIPLe CORRELATION FOR THE ACTMTY SCORES 87
TABLE 4J6 MULTIPLE CORRELATION FOR FEV,. WITH DIFFERENT ACTMTY SCORES
INCLUDED AMONG THE CANDIDATE PREDICTORS ............................... ..,.. ..., ... 88
TABLE 4J7 MODEUNG FENc AS THE OUTCOME VARIABLE .................. .+ ............................. 98

LIST OF FIGURES
FIGURE 4.1 AVERAGE ACTMTY LJZvELS FOR THE HAES ........ -.. ...........~....C.....CI....... . 5 4
............. FIGURE 4 3 AVERAûE ACMVRY LEWU FOR THE ACTMTY DIARY .................. .. 57
........................................................ FIGURE 4.3 A C T I W N CLASSWICATION (CATEGORY O).. 66
FIGURE 4.4 ACXïVïR CLASSIFICATION (CATEGORY S).. ................... .......H...*.........*...**..... 67
.......................................................... FIGURE 4.5 A C T M T Y CLASSIFICATION (CATEûûRY 6) 68
FIGURE 4.6 A C T N R Y CLASSIFICATION (CATEGORY 7) ................. ...... ................................... 69
FIGURE 4.7 ACMWTY CLASSIFICATION (CATEGORY 8) ...................................... . 70
FIGURE 4.8 ACTNiTY CLASSIFICATION (CATEGORY 9) ................* ............. .........,... 71
FIGURE 4 9 PLOT OF FEVl BY AGE ................................................................................................ 89
FIGURE 4.10 PLOT OF FEVl BY PERCENT OF IDEAL WEIGHT ..................... ....... .......... ........... W
FIGURE 4.11 PLOT OF FEV, BY HAES WEEKDAY TOTAI, ACMVITY ..................................... 91
FIGURE 4.12 PLOT OF FEVl BY HAES WGHTED TOTAL ACTMTY .................................... 92

LIST OF APPENDICES
A ASUMMARY OFEXERCISE~VENTTONSTUDfES INCE5 ........................ .., ............. 124
B CONSEM: AND ASSENT FORMS ............... - ......... ..................................................................... 130
C GLOSSARY OF TERMS AND ~BREVIATIONS ............................................ 138
D THE HABïI'UAL, ACTMTY ESTIMATION SCGLE (HAES) ................ .. .................................. 140
E THE 7-DAY ACTNLTY DIARY .................................................................................................... 147
F PARENTQUESTIONNAiRE ....................... ..... ............................................................................ 153
G PûWER CALCULATION .............................................................................................................. 158
H SUMMARY OF ACTMTY TYPES .............................................................................................. 159

INTRODUCTION
1.1 Sinnificance
Cystic fibrosis (CF) is a chnic , inheriteà disorder chamcterized by progressive lung
disease in the majority of patients. Physiotherapy is preacn'bed as a conventioaal treabnent of
pulmonary impairment caused by lung infection and mucus obstruction. The goal of chest
physiotherapy is to improve or maintain lung function. Exercise may also ùenefit pulmonary
function, and has ken proposad as a supplementary therapy in CF.' An exercise training
program of an appropriate frequency, intensity, type and duration may psitively affect the
pulmonary status of CF patients through the facilitation of sputum expectoration,' and an
increase in respiratory muscle endurance? Patient cornpliance with a long-term urercise training
program, however, is difficult to maintain? Romoting healthy lifestyle changes in CF patients
may be a more practical means of incnasing physical activity levels. A longitudinal study is
needed to &termine whether the habituai physical activity level of CF patients is a significant
p d c t o r of the rate of change in pulmonary function.
Prior to the onset of a long-term investigation, an appropriate measunment of habitual
physicai activity is necessary for the CF population. The cumnt pilot study was conducted to
memm habitual physicd activity in a sample of CF patients at The Hospital for Sick Children
('SC). Two instMnents were used to capture this infinmation: the Habituai Activity Estimation
Scde @AES) and the 7-Day Activity Diary. Both insm~aeats provide data on the fkequcncy.
intensity and duration of activity. The Acîivity Diary, however, provides additional information
on the type of activity king paformod.

CF patients at HSC are ftbsuently overwhelmed by requests for their participation in
research studies. One important goal of this pilot study was therefore to calculate the recniitment
and compliance rates for the collection of habitual physical activity data in order to predict the
likeiihood of success in patient recnlltment and compliance for a long-term study. Tmds in the
relationship of pulmonary func tion with habitual ph ysical activity level, nutri tional status, and
exercir capacity were also examined These results were intendecl to encourage integration of
the regular collection of habitual physicai data into clinic management, generate further
hypotheses, and guide the design of hitue clinical trials of exercise as therap y.
For this pilot project, we hypothesized that a positbe relationship would be &monstrated
between pulmonary jiuacîion (forced expiratory volme in one second, Fm/), habitual physical
activity (Activiîy score), num'tional statu (percent of ideal weight) and excrcise capacity
(nrcu~*ml work capaciiiy or onygen consumption). We pmposed that CF patients with high values
for FEVl would have high activity scons, in addition to high percent of idcal weight and
maximai work capacity or oxygen consumption values. Although it is plausible that a causal
relationship ktween lung function and habitual physical activity could work in either direction.
the issue of causality could not be addresseci in this cross-sectional pilot study.
1.2 Obiectives
The objectives of the cumnt study were:
Rimsry
I . To detennine recruifment and conipliimce rates for the coilection of habituai physical
OCtMity dotajbm the CFpopulation,
2. To qvm~lfy tkfie~uetlcy, intensity, type Mddtumfa of hubitual pIrysical activity in CF
chiIriren.

3. To compare the datofrom two &ffermt rneasumnents Qhabincat physicd llctivity: the
7-Day Activity Dimy and the Habirual Activity Estimation Scde (HAES).
4 To detennine if a positive relationship exists between pulmnary fkncrion. habitua1
physical activity, nutnional stm and exercise capacity.
-adUr
5. To examine potential correlates of physical activiîy partz*cpati*on in CF children.

BACKGROUND
2.1 Cvstic Fibrosis
Cystic fibrosis is a chronic disease which is usually manifested in early childhood, and is
characterized by an abnormal transport of chloride ions across the epitheiial üning of multiple
surfaces inclwüng the nasal cavities, lower aimays, exocrine pancreatic ducts, and sweat ducts?
Clinical manifestations of CF include chronic obstructive pulmonary disease. pancreatic
insufficiency, and elevated sweat electrolyte levels? Although CF is the rnost common life-
shortening, autosomal recessive genetic disease in Caucasian populations~ this incurable disease
is much less common in Afncan and Oriental races? 1n Caucasian populations, the carrier rate is
appmximately 1 in 20. and the incidence is estitnated at 1 in 2500 live bas.'
CF was fmt recognized as a disease in the 1930's, at which time many patients âied in
their fmt year of life? Subsequent developments in CF research and treatment have dramatically
improved the iife expectancy of these patients h m 11 yem in 1960 to 3 1 years in 19977
hproved prognosis can be attributed to extensive international research efforts. At HSC in
Toronto. the gene nsponsible for CF was located in 1989.8 This discovery has enabled scientists
to consider gene therapy as an eventual tnatment for CF. Rennements in therapy, the aâvent of
anti-bacterial antibiotics, and more muent recognition of mild cases have also contributed to
improvements in pgnosis? Despite this progress, some patients stiiî do not survive put
childhood Resemh has demonstratecl that factors associated with good prognosis include care
in a CF chic, mak gcn&rp good nutrition, normal intesthai fat absorption! and hi&
~ a r d i o ~ c i l m o ~ ~ ~ fimess.'O

Lung fiuiction declïne is a primary featun of CF patients. An estimaîed 7596 of patients
suffet h m recumnt pulmonary infections: and 90% of ail deaths fiam CF cm be attniuted to
irnversible lung damage." Rilmonary dysfiuiction usually begins in inf'cy with an abnormally
fiequent cough, and eventually inhibits the cfiild's ability to clear smalI aimay secmions.
Bacterial infections arise when mucus becornes trapped in the aimays. As the cilia are unable to
clear inhaled bactena b m the lungs. chroNc irritation and inflammation of the aimays nsuit.
The bacterial agents most likely to cause infection are Pseudomonas aeruginosa, Staphyiococcus
aureus, and Burkholderia c e p ~ i a . ' ~ Virai agents also cause infection in CF patients. Originating
in the upper respiratory tract, these infections can descend to cause bronchitis. In CF, complete
obstruction of the bronchus by mucus will lead to a collapse of portions of the lung. As air
cannot move into and out of the lungs properly, less oxygen will mach the bloodstmam. Duriag
late childhood and early adulthcmd, many CF patients show a subsequent increased sensitivity of
the bronchi to a variety of challenges, ranging h m exercise to inhaled proteins?
Pancreatic insufficiency, an inability of the pancreas to secrete enough enzymes for food
digestion, is another common clinical feature of CF. Appmxiniately 85% of patients are unable
to absorb adequate amounts of nutrients h m their diets, and consequently quire enzyme
supplementation to help prevent growth delays and weight loss. Chest infections, in addition to
panmatic insufficiency, may also lead to weight loss through a reâuction in appetite or
inmascd energy expendit~n!~
Many factoni influence the p w t h pattern of CF patients, includhg lung disease
severity, respiratory infiection frequency, the extent of nutrient mdabsorption, and the &grec to
which tceatment affects these conditions. The mean birth weight of CF infants is appximately
5% lower than that of healthy babies." hi spite of delays in pubaty and skeletai mturity, C F

children usuaüy experieace steady incrases in height and weight during the first 10 years of Mee
These increases, however, arc below the averages for n o d chiidren. Final height and weight
values d l k much greater for CF childm who do not have sigmficant pulmonary involvement
than for children with severe lung impairment?
Beginning with their diagnosis, CF patients at HSC integrate regular clinic visits iuto
their lives. Approximetely once every ihrre months, patients and their families consult with a
s pecializeâ team of heal th professionals, which includes doctors, nwses, ph ysiotherapists,
dieticians, and social workers. Measurements of height, weight, and temperature are taken in
clinic, and sputum samples are collected. In chiIdren older than six years, partial puimonary
function testing (spirometry) is performed at every clinic visit. Exercise testing accompanies full
puhonary function testing once per year. Chest x-rays and blood tests are conducted on a
biannual basis. Xmys show changes within the lungs, helping the doctor to assess the patient's
clinical status. Blood tests demonstrate b e r functioning. nutritional status, hemoglobin levels,
the presence or absence of infection, and the degree to which the patient can fight infcctioneL2
Another component in the management of CF is in-hospital treatment. Penods of
hospitalization usually range fkom 7-10 Qys, and are necessary if an acute chest infection d œ s
not respond to at-home treatment This intensive trcabnent is compriseci of intravenous
antibiotics, physiotherapy, and adquate r e d 2 T ~ t m e n t ngimens routinely conducted at home
can resume once hospitaîization is complete.
The aim of CF matment is to aileviate symptoms and correct organ dysfunction. Patient
contentment and cornpliance with trratm#it an important considerations in deciding on the best
regimen to pscribe, and becom evm more important to consider in adolescent patients.

Panmatic enzyme replacement, the pmcription of antibiotics, and the clearance of lower airway
semtions comprise the plimpsr f o m of treatment.
To combat weight loss, the clinic dietician prescribes a high-energy meal plan and caldc
supplementation. CF patients need an energy intnLc of appximately 120-150% of n o d
requirements. Enzyme and vitamin supplements are ncommended for panmatic insuftcient
individuals. l2 Treatments for pulmonary impairment include bronchodilator therapy, antibiotics,
and chest physiotherapy. These therspeutic regimens have becn very successful in modifying the
natural history of lung disease to the extent that serious lung damage can now be delayeù, in
some patients, for many years.
Inhaled bronchodilator medications relax the branchial tubes in the lungs. The subsequent
increases in both the size of the air passages and in expiratory flow rates make it easier for
patients to breathe. Bronchodilators are useful in combating occasionai bouts of wheezing.
shortness of breath. and persistent coughing. Antibiotic therapy is prescribed for chest
exacerbations and for regular disease management. The patient's response to antibiotic therapy
may include a decrease in the fkquency of chest exacerbations, improvements in lung fimction, a
&mase in the bacterial density of sputum, and enhanced well-kingbL2
Chest physiotherapy mobilizes sputum from smallet to larger ainvays so that it can be
removed by cough. In addition to increasing sputum expectoration. physiotherapy may also
minimize lung tissue damage. Two common physiotherapy techniques nquire the assistance of a
caregiver. manuai percussion of the chat and postural drainage. Two independent techniques are
forceci expiration by the patient, and expiration against a positive pressure r n ~ k ! ~ Physiotherapy
should be ieguiarly administered so that infcctiou cm bs âelayed or prcvtntcd by the nduction

in obstructive mucus. Patients are recommended to perfonn two to thne sessions of
physiotherapy pet day, with cach session lasting 20 to 30 minutes?
Effective chest physiotherapy may requin special equipment and a caregiver to assist in
administration. and adequate compliance with treatment is essential. Compliance with
physiotherapy is often ciifficuit to encourage. however, especiaily if the physiotherapy sessions
interfere with dail y activities or set CF childmi apart h m theu peers. A supplemental treatment
for CF patients is ngular physical activity, which encoumges patients to cou&, and may leaâ to
inmased sputum expectoration4 and maintenance of pulmonary function?
2.2 Phvsical Activitv in Children and Youth
2.2.1 Heaith Benefits
The health effects of physical activity participation in chilâren and adolescents have not
been well documenteci. Based on the available research, the potential health benefïts of regular
physical activity likely incluâe: improved peak bone mass, immune status, catdiorespiratory
fitness, and psychologicai weii-king, teduced adiposity, and a decreased risk of musculoskeletd
injury. As a result of these reported benefits. physicai activity guidelines for adolescents have
been developed. Experts recommend that hdthy adolescents participate in a minimum of 3
weekly moderate to vigorous activity sessions, with each session lasting at least 20 to 30
minute^.'^
The health benefits of physicai activity in children and youth are difficult to determine.
Activity patterns in chiIbn and adolescents Vary as a function of gender, age, and season. Males
are g e n d y more active than fernales, and overaii participation in physical activity tends to
dccrease with age. Time spent in vigorous activity, however, may actuaily i n m u e with age.

Children appear to be more active when outdoors, and seasonal variation in activity patterns has
been rep~rted."*'~
2.23 Patterns in Cbronidy 11l Patients
in light of evidence supporting physical activity participation in healthy populations,
nsearchers surmise that regular physical activity may also be beneficial for individuals with
chronic disordem. Encouraging physical activity participation in childhood wiii help to establish
lifestyle habits that may modify the course of some diseases, and research suggests that physical
activity shouid becorne a regular component of CF management.''
Studies indicate that chronically ill children are more sedentary than their healthy
counterparts. Reduced physical activity in children with c h n i c disorciers may be amibutcd to
parental fear of h m , school worries about injury, physician concems about disease exacerbation
due to physical stress, timeconsuming matment ngimens, or fewer oppominities to exercise.
Exercise-related studies of children with asthma, Dom's syndrome, cerebral palsy, juvenile
rheumatoid arthritis, and CF suggest that exercise training programs are not deûimental. On the
contrary, these pmgrams may result in improved selfconcept, enhanced medical trcatment
benefits, and increases in physical fitness." In CF patients, extensive nsearch has been
conducted to determine the effects of exercise training on general weU-king, lung function and
exercise capacity.
2.2.3 Exerck Consiàerations in CF Patients
The htaith beaefits of lecnational exercirre for CF patients were fint recognized in 1969.
Enmise hbas since km proposcd as an adjunct to chest physiotherepy,'9 and is now widely
accepteci as a therapeutic intervention in CF? Studits have indicatcd that exacise training can
inmatje spuhim expectoration i u g h heightened coughing. impmvt respiratory muscle

endurance, and contribute to the maintenance of puimonary fuaction status.' In addition, exercise
may impmve clinical statu, fostcr the child's participation in nomial activities of childhmd, and
improve theù morale." As a supplementmy -ment, exercise is appeaiing because children cm
perform theu therapy independently or with their pers in activities of their own choosing. While
there is no evidence to suggest whether reguIar participation in physicai activity cm improve
prognosis in CF patients or be as effective as chest physiotherapy, CF patients who do not
exercise may experience nductions in muscle tone, strength, endurance, and aerobic ~apacity.'~
Although exercise in CF patients is considered to be generally safe, there may be
additionai risks for some individuals. Possible problems inch& a reduction in blood oxygen
resulting in tissue death. dehydration, the inducement of violent coughing, and weight loss.' As a
nsult of these potential risks, extra precautions may be necessary. If oxygen &saturation occurs
during exercise, it can k deviated with oxygen supplemmtation. Training at a target hem rate
of 10 beats per minute klow the point where desaturation occurs should also be prescritmi. A
gradua1 increase in activity levels should precede the onset of any training program if the patient
exhi bits ph ysical decondi tioning. ' Exercise testing is a usehl tooi in the assessrnent of disease pmgression." CF patients
suffer prognssively impairecl exetcise capacity as theû lung disease wor~ens.~' Although heart
rate and blood pressure responses to exerçisc arc normal, exercise testing demonstrates that
maximal values for work capacity, oxygen consumption and h e m rate are Iess than expccted
when compareâ to the hcaithy population. In CF, exen5se is limitcd by lung mechuiics, whereas
in heaithy individuals, exerciae i i Iimited by the cardiovascdar system. ExCrcise training
pro- of sufficient intcnsity in CF may nsuit in bcnefits to excrcise capacity, including

imptonments in maximai work capacity, maximal onygen consumption, maximal minute
ventilation, respiratory muscle endurance, and anaerobic ~ireshold.'~
Guidelines have been suggested for extrcise recommendations in CF patients. The
activity choice will depend partially on the patient's access to appropriate equipment and
f d t i e s . Aerobic activities that will pmmote sputum expectoration, such as swimming, running.
skating and dancing, should be encouraged h m an early age." Participation should entail th=
to five sessions per week at an intensity of 70 to 85% of the maximal heart rate. CF patients are
generally not able to attain an age-prcdicted maximal heart nite due to ventilatory limitations.
Therefore, maximum heart rate should be individually detemiined. Patients should be ailowed
significant input into the choice of activities in order to ensm gooâ compiiance with the
pmgram.'g
Cornpliance with exexcise programs cm be diKcult to foster in CF patients due to the
existence of time consuming matment regimes, forgedùlness, or a negative attitude towaràs
exercise. Although many CF centers do not offer organized exercise programs, such programs
may encourage cornpliance. Summer camps, in-patient hospital programs. and home-based
program are several possibilities. While summer camps offer brief periods of intense activity in
a positive social setting, in-patient hospitai programs cm teach patients how to incorporate
regular exercise into their Lives. At-home exercise participation requires patients to pprtelue
independentiy in unstnictured programs. In North America, however, summer camp and gmup
exercise programs arc no longer tt~ommcndcd due to the risk of cross-inféction of Burkholdaia
cepria." niercfore. home-bascd exercise progcams am the most viable option for CP patients.
As cornpliana with long-term uracise training pgrams is di&cult to maintain, a more
fa ib le alternative for CF patients may be a change in habituai physical activity psttcms.

Whereas exercise is characterizcd by an imposed and ngimented training program. habitual
physical activity refm to the level of activity one has incorporated into their daily Me. Changes
in habitual physical activity would represent a liftstyle modification. and may promote long-term
hedth benefits more easily than exercise programs. Until now, the quantification of and foliow-
up of habituai physical activity in CF patients have not been adequately addnssed. Research hm,
however, been conducted to examine the d e of exercise training programs in positively
affecting the health of CF patients. These studies an important to examine because they provide
evidence of the benefits of physical activity in CF.
2.3 Exercise Training Ronrams in CF
2.3.1 Characterisüa of Exercise Rognm~
Exercise-related studies in the CF population have been conducted to cietennine the
effects of exercise training programs on pulmonary function, exercise capacity, sputum
production, respiratory muscle endurance and psychological well-being. The various studies
have implemented training prognuns of differing types. duration, fnsuency, and intensity.
The degree of supervision is an important consideration in exercise presaiption.
Supe~sed pmgx'ams require regular inmention and program monitoring by an exercise
specialist such that the safety of the individual can be @odicPlly checked and individual
tailoring of exeiçise programs cm occur. These factors likely foster high patient compiiance with
the training program. On the contrary, the success of unsuperviscd training pmgrams depends on
the participmt's sociai support and seKmotivation. Aithough cornpliance with the program may
k less than optimal. unsupmised programs rsquire mlliimal monitoring. and thus have the

The desireci duration of the exercise program should be decideci on @or to the onset of
training. Whereas long- training pmgmms have been shown to benefit lung fuaction in
the effects of short-term exercise pgrams are still equivocal. Although positive results fiom
shortened training pend have ken demonsttgted, these effects are often short lived. 233
Training program of varying intensitiea en also pnsented in the CF literanire. High intensity,
exhaustive pmgrams have demonstrateci positive m~ults,~ but these pgrams may be difficult to
incorporate into daily life. Exercise pmgrams of lesser intensity have been considered as a more
feasible dternative.' Specific study examples of the various training program are presented
below.
2.3.2 Supervid Pmgrams
Supe~sed training progcams can occur in a formalized hospital setting, as demonstrated
by utc ch^ and AmericanL6 based studies. The conflicting results h m these investigations
demonstrated either benefit to pulmonary function,= or no harm to patients with training." In the
Amencan s t ~ d ~ : ~ there was no reported difference in pulmonary f'unction for subjects
mdornized to two groups: either two sessions of exercise plus one session of physiothmpy
(n=9), or three sessions of physiotherspy (n=8). Patients (mean age=ISA years) stayed on the
program for an average of 13 days. and perfonned exercise on a cycle ergorneter. Over this short
study pend the investigatom ensured hi@ cornpliance with trcatment, and concluded that
substiaiting exerdee sessions for regular physiotherapy was not harmful to patients.
The dutation of hospitalization paiods for CF patients are generally short. and are
brefore not conducive to the irnplernentation of an extended, superviseci training program.
Rccreational settings arc m a e suited to long-tenn pgrams. Eight supervised programs have
ban conducteci in recrcationai settings under the supe~sion of a traincd profcssional. The

activity types included swimming. n ~ i n i n ~ , ~ trampoline ex t rc i s~ ,~~ intensive and muiti-
activity training in a camp ~ e t t i n ~ , ~ ~ and aembic txercise directed by an instmctor. 3132
Two studies have evaluated the effets of a 12-week? d a seven wœk swim pm8f8m24
on the heplth of CF patients n$pectivcly. Research bas suggested the vaiue of swimming as a
training mode in CF because the welî-moisturizcd environment may inmase sputum
expectoration. Submersion-induced subtk changes in volume and presswe within the respiratory
system may also contribute to knefits in CF patients with smmming programs.u The seven
week s w i m program was coupled with repeated evaluation of lung function and sputum
production in 1 1 patients (median ag-10 years).u Children maintained their usual schedules of
therapy ihroughout the study. Sputum volumes were found to be significantly higher on
swimming days than on non-swimming days. In addition to enhanced mucus clearance. results
also demonstrated significant improvements in pulmonary function following the training
program. Although these patients w m recommended to remain physicaiiy active after
completion of the swim training, pulmonary huiction values eventuaily renimed to baseline
velues. The positive changes in pulmonary huiction may have resuîted fiam the sswimming itself,
or h m the supmised nahm of the program. Results h m the 12-week swimming program,n
on the other hand, demonstrateci no benefit to pulmonary function.
Trampoline jumping has been suggested as an appealing alternative to more typical and
arduous forms of exercise, and may mimic the actions of chest physiotherapy. Eigbt children
(mean agesll.5 years) participateci in an eight-week exmise program on a trampoline. for a
niaxinium of 109 minutts l~eck.~~ The @en& participatcd in a program that included rocking,
jogging, and jumping on a mini-trampoline. This program nsuiteâ in significant impvement in
faccd vitai capacity and maximal oxygcn coiuumpion.

Patients (age rpngc=IO-30 yeare) vol~~~ttered for a three-month d n g pmgram in
another supervised s t ~ d ~ . ~ Twenty-one CF patients wen ailocated to the exercise group. whüe
the remaining 10 patients formed the control gmup. The exercise group participated in an aerobic
program three times per week that included wm-up, jogging, and cool-down components. The
control group was askeâ not to change dieV usuai activity. The exercise group demonstrateci
significant improvements in exercise capacity and in respiratory muscle endurance, but no
change in pulmonary function. In the control p u p , fomd exphtory volume in one second
showed significant decline.
Superviseci pmgrams have also been implemented in a pediatric rehabilitation centna
and at a s m e r ~ a r n ~ . ~ ~ h e s e types of settings provide optimal conditions for children to
participate in physical activity for brief time periods. Seven CF patients (mem age13.4 years)
participated in four weeks of summer camp, unâergoing 1.5 daily hours of intensive swimming
and canoeing aimed at upper body endurance? Respiratory muscle endurance, which has been
comlated with fatigue nsistance, impmved by 56.7% in these patients. No conclusions could be
drawn from this study, however. about the potential benefits of lower body endurance exercise.
At a pediaüic rchabilitation centre? patients partjcipated in a 17-day intensive training period,
replacing usual physiotherapy with physical activity. Although pulmonary function did show
signifiant improvement, less intensive emrcise may not have demonstratecl benefit to patients.
Results h m th- studies iUustraie diffmntial eff- of supmised training on lung
hmction, ex&r capacity, and respiratory muscle endurance in CF. A multitude of foctors mut
be considered @or to the onset of diis type of program, incltuhg the type, duration, and setting
of the program. A summary of the superviscd pfograms are depicteci in AppendiXA as Table A.I.

Seven unsupeivised training pmgrams have been implemented in the CF population. 333-38
h s u p e ~ s e d propus are usually canieâ out in the home setting, and an generally longer in
duration than supervised program due to minimal monitoring requirements.
The two longest studies to date have been 30 months3' and three years3 in duration. The
effects of physical training on work capacity, lung fhction and clinical condition were examined
in seven patients (mean age=10.4 yeam) participating in daily exercise over 30-months?' The
exercise program was compriscd of skipping, jumping, jogging end swimming. Chest
physiotherapy was withdnwn aftu the initial 12 months. As puhonary function parameters
were unchanged over the course of the study, the investigators concludeci that physical training
could replace conventional chest physiotherapy except where strenuous exercise was not
feasible.
In a three-year exercise inmention study in 65 CF patients (age range=7-19 years), the
effects of long-term training on lung hmction were evaluated? Subjects were randomized to
eitha an exercise or a control group. The exetcise group was instmcted to exercise a minimum
of t k times per week for 20-minute sessions, while the conml group was asked to maintain
their usual activity. Patients h m both groups continued their usual schedules of chest
physiotherapy. Subjects participaieci in aerobic activities of their own choosing, with a guideline
target hem rate pvidcd by the exercise physiologist. Results indicated a pater annual mean
rate of decline in forced vital capacity for the contml gmup cornparrd with the exercise p u p .
No Merences in exercise capacity were demonstrated.
An Australian studf invcstigatcd the effits of a 12-week home exercise program,
comprised of sprints and jogging, on 41 txerche and 45 conbol patients (age mp8-14 years).

The exercise group demonstrateci significant impmvements in exercise capacity, but no change
in puimonary function. The investigators noted declining compli~nce in the latter half of the
program which may have contributed to these non-significant muits.
The literature indicates a neeâ for m e r nsearch in the area of unsupe~sed programs.
Whereas one study suggested that exercise could have equivalent benefit to patients as
conventional physiotherapy~s another study nported no benefit to pulnionary function with
unsupervised training?' The unsupervised program am presented in Appendix A as Table A.2.
Another possibility for exercise training is to combine supervisecl and unsupervised
components into one exercise program. A study in the Netherlands showed improved pulmonary
function (forced expiratory volume in one second) following a short period of hospitalization,
and an increase in exercise capacity after one-year of at-home training? This type of program is
useful if patients begin exercise training during a hospital stay. and want to maintain a similar
level of physical activity once they rem home. This study is presented in Appendk A as Table
A.3.
23.4 Chaifenge~~ of Trsiiiing Program
The effects of e x d s e craining on CF patients are difficult to interpret due to small
sample &es and potential confounding variables. hvestigatom find it difficult to remit enough
patients for their studies because an extensive tims cornmitment is requifed, and some
individuals are not intmstcd in pmuing excrcise training. Las to follow-up is aiso a problem in
CF patient studies, m e r emphasizing the n d for a large sample sim. Chest exacerbations, for
example. may intafkre with the training protocol. Codounding variables mut be adequately
controIIed for. Potcntial confounders to consider inch&: the hetcrogcneity of the disease and its
dive= naturai course, unprsdictabk occumnas of infection, complexity of the thaipeutic

approsch, and variable degrees of cornpliance with inatment.40 These fwtors must al1 be
accounted for if conclusions are to be made on the relationship between exercise training and
health in CF,
Compüance issues and the individuai needs of the patient must also be given cmfui
consideration. Rogrtms that are too long or too intense* may deter patients h m paiticipating.
Individual tailoring of training pmgrams, such that each prograrn meets the training needs and
interests of the patient, is essential if heaith effects are to be demonstrated. Finaily, the benefits
in lung function and exercise capacity seen with training may not last beyond the training
program itself? Given the challenges involved in implemnting successful exercise training
programs in CF, M e r evaluation of habitual physicai activity and its relationship to important
health outcomes is necessary.
2.4 Relationshi~ between Habitual Ph~sical Activity. Lune Function. Nutritional
Status. and Exercise Ca~acitv in CF
Several studies have begun to explore the relationship between habitual physical activity
and lung function in CF. In one investigation, the physicd activity levels of 30 CF patients and
3 1 control subjects (ages 7-18 years) wen ~ o r n p a n d ~ ~ The investigators aiso evaluated whether
habituai physical activity was nlated to exercise performance and pulmonary function in these
CF patients. Kriska's Modinable Activity Questionnaire was used to assess habituai physical
activity. Total hours of physicai activity per wœk did not differ ktween the C F (7.3 hodweek)
and the control(7.1 hounlwcek) groups. The total hom engaged in vigorws activity, however,
were significantly lower in the C F patients (1.3 hourslwak) comparecl with the healthy controls
(3.2 hourdwœk). The rcsults indicated that activïty levd was unrelateci b both txercise
toleranct and lung hmction.

A Quebcc study ueed the Habituai Activity Estimation Scale w) as an estimate of
habitua1 physical activity in enamining the nlationship between activity levels, lung fuaction and
nutritional statu in 36 CF patients (aga 6-16 years)!2 Consistent with pnvious usage of the
HAES, patients classified theu actinty into 4 differcnt categories, and their activity level was
represented by the total percentage of time speat in the somewhat active (i.e., waücing) and
active (i .e., biking) categories. Boys and girls speni 8.1 and 7.5 hours respectively being at lest
somewhat active. In children with significant lung disease, activity level was positively
associated with nutritionai status, but unrelated to lung function. h m these nsults, the study
investigators concluded that activity levels may be rsstncted by nutritional status in more
severel y affected patients.
Disease progression in CF is characterized by malnutrition and lung hinction decline. As the
disease advances, exercise capacity is also limited? Researchers have h ypothesized that
pulmonary function may affect exercise capacity by limiting ventilatory capacity, or through
skeletal muscle deconditioning. Nutritional status may be influentid through reâuctions in
muscle mass or changes to muscle quality? The inter-relationship of nutritionai status,
pulmonary function and exercise capacity has ban p~viously investigated. a,r3,rs
In 50 CF patients, exercise testing was performed to determine limiting factors of
exercise cap~acity?~ in this sample of patients, exercise capocity was demonstrated to be
correlateci with both lung function and nutriti011al status. Another study was conducted in 22 CF
patients with advanced lung disease to evduate the effects of nutntional status on exercise
capacitya Results indicated that exercise capacity w u relatcd to the degree of respiratory
impairment. and independently infiuend by nutritionai status. In an investigation of 14 CF
patients, lung diseare sewrity and paipheral muscle hmction were both dctermined to be

lunithg factors of exercisc ~ a ~ a c i t ~ . ~ At HSC, long-term folîow-up of CF patients demonstrated
that the institution of a high fat diet resulted in improved nutritional status, and a subsequent
increase in survival! These saidies have demonstrated an association between nutritionai status.
exercise capacity and lung function in the CF population. The potentiel contribution of habituai
physical activity to this nlationship needs Mer investigation, as does the quantification of
habitua1 physical activity in CF.
2.5 Measwement of Phvsical Activit~
Pediaüic chronic disease nsearch has advocated the importance of incorporating a
quantifiable rneasure of physicai activity into reguiar disease management." A consensus has not
ken reacheâ, however, on the best mcthod of measuriag physical activity. The difficulty lies in
the many possible choices for physical activity quantification. ranging h m isotope consumption
to heart retc monitoring and self-report. Racticalîty, cost and measurement accuracy are
important considerations in chwsiag the most appropriate method.
2.5.1 Doubly LaMd Watet
Doubly-labeled water @LW) is a relatively new technique that is being considered as the
gold standard of energy expenditure estimation. Although the expense of this procedure deems it
impractical in largescale epidemiological snidies, the accuracy of DLW malw it an appealing
choice for field and laôoratory studies!' One limitation of this procedure, however, is that it
canot be ueed to &termine the proportion of energy expenditure associatecl specifically with
physical activity?
For this proceâun, patients ingest a quantity of water with a known concentration of
hydrogen and oxygen isotopes. ûnce the isotopes have distriibuted themselves m equilibrium
with body water, labeled hydrogcn exits the body as water, and labelcd oxygen leaves the body
as water and carbon dioxide. By knowing the difference in the elimination rates of the 2 isotopes,
the pduction of carbon dioxide cm be calcula& Total energy expenditure is calculateci from
standard respiratory gas exchange tquations?
2.52 O b ~ e ~ t t i o n
In contrast to DLW, the observation method is a niatively simple means of assessing
physical activity. Observation is usefd in studying pnschool and school-aged children. where
alternate methode may be neither feasible nor appropriate. An observer monitors the activities of
a subject for a predetermined amount of time, and records data on the type. fkequency, duration
and intensity of each activity. To calculate total energy enpaiditure, the estimated energy cost of
each activity is multiplied by the time spent in that activity?'
The observation method haî not been previously validateci, although it has been used as a
standard by which other techniques are compareci. Due to restrictions on time and cost, this
method is best suited for small studies. The= are severai other disadvantages to this technique.
Observations can only be made over short tirne periods, and are not refiective of habitua1
physical activity. Additionaîly, subjects may alter their usud activity if they know that they are
being observed!'
23.3 Movement Asmsmetlt Devices
Movement assessrnent devices arc wom on the tNnk or extremities, and are designed to
k t l y monitor movemcnt and store this data for subsequent analysis. Two examples of thcse
motion xnsors are the palorneter and the accelcrometer. Although the pedometer depends on
accelemtion and deceleration. it is not an a~celemrneter!~ An accelemmetcr mcasures
a c e l d o n of the body.

nie pedometer counts the nurnber of steps taken or estimates the distance waIked. It is
usehil in estimating physicai activity associateci with walking or m g , pmviding a quick
assessrnent of activity Ievels. ïndividuals tend to walk with a pa te r impact on one fwt than the
other, and pedometer readings will Vary depending on which side of the body the pedometu is
wom!' The pedometer wil l also underestimate activity Ievels for sports such as cycling, skating,
and rowing, where activity is not baseci on vertical displacement.
The most cornman single-plane acceleromeer is the Caltrac. This device clips close to
the body at the non-dominant hip to ensure an accurate estimation of acceleration and
deceleration. The Caltrac is designed to provide an activity score that nflects the intensity and
quantity of the movement, and allows for an estimation of energy expendiw for activities
within the vertical plane? Three-cümensional accelerometers reflect movement outside the
vertical plane, and can estimate energy expenditure for many different types of activities. These
triaxial accelemmeters measun motion in the vertical, horizontal and diagonal planes. There are,
however, disadvantages to use of the accelerometer. Energy expended as a result of lifting heavy
objects cannot be nflected in the data For water sports such as swimming, waterpmfing of the
accelerometer is necessary. For cycling, the &vice muet be wom on the leg instead of the
trunkt4'
2.5.4 Heart Raîe Monitoring
A demonstrated positive relationship behvem heart rate monitoring and cnergy
expenditure has led to the use of h m rate monitoring to estimate energy expendiiun. This
technique is appealing in populations where it is difficuit to assess physical activity kvels by
other means, such as in young children. Relatively inexpensive heart rate monitors are available
to assess daüy activity, complete wîth M-day storage capacity for minute by minute data

collection of h m rate? To obtain an individual's heart rate p d e , a minimum of four to five
recording days is nccessary in order to account for the variability seen in heart rate
measurements. Many factors e t heart rate and could infiuence the nlationship between heart
rate and energy expenditure, including the active muscle group, anxiety, training, ambient
temperatureT and the type of muscle contraction?' Using the hem rate monitor in conjunction
with a self-report instrument could better reflect physical activity than if the monitor is used
alone.
25.5 Seif-Report Instniments
In epidemiological saidies. activity diaries and questionnaires are the most common
techniques used for assessing habitua1 physical activity. These instruments can either be self-
administered or completed with the help of an interviewer. Parents or teachers may serve as
proxy respondents in estimstng the physical activity levels of young children. Habitual physical
activity patterns or physicd activity levels in the recent past may be of most interest to a
researcher. Activity type, intensity, duration and fkequency are the most common variables that
are meesund, and in some cases. an estimation of energy expenditure can be computod. 47.48
Advantages of using disries and questionnaires to mess physical activity include low
cost, quick administration tirne, the abiüty to gatha information over an extended time period,
and minimal staff* However, the vaüdity and nliability of these instnunents must be continually
evaluateâ. Disadvmtagts include potentiai recd bias, and subjective respoases to the questions.
In addition. studies indicate that self-report instruments an not useful in children unâer 10 years
01d?~*" Roxy response is, however, an acceptable alternative for completion of these
instruments.

253.1 The Aetnlty D m
Activity diaries requin subjects to &tail their daüy activity at intervals ranghg h m 1
minute to 4 hours. Individuais may bmadly classiry UicK activities, or express their activity
pattems in more specific temu, using prepared forms. Although this type of extensive reporthg
may be tedious, subjects can employ shorthand methods to efficiently report their activity levels,
and rnay discover patterns in their weekly activity, making recording easier.
A 3-day activity diary was developed by Bouchard et al to estimate the amount and
pattern of daily energy exPenditudg Every 15 minutes over a 3day period, 150 adults and
chilâren (ages 10-50 years) categorized their activities on an energy cost sale h m 1 to 9. Mean
energy expenditurc was positively comlated with physical working capacity and negatively
comlated with body fat. Reliability testing indicated high repducibility for this measurement.
This 3-day diary was modified as a 7-day activity diary in a Swedish investigation?' In
two groups of randomly selected adolescents (aged 15 years) h m two regions of Sweden
(n=374), activity pattmis were recordecl over a 7 day period. Each subject was provided with a
detailed explanation and demonstnition of the diary. Total energy expenditure and physical
activity level w m computed from the diary entries. Resuits dernonstrsted high and concordant
physical activity levels and energy expenditure in the two subject groups.
Validation of this activity diary was p g f o d in a sub-sample (n=SO) of these Swedish
adolescents? The 7&y activity diary was cornparcd to the doubly labeled water methoci, and
was found to pproviâe close es- of physicai activity level and total e n q expenditure.
These results suggestcd the suitability of the diaq for estimating energy txpnditurt in groups of
adolescents.
Although not previously used in a CF population. a Mar version of this activity diary
has been used in children with chioaic A sample of 23 cMdren (ages 5-1 1 yem) with
juvenile rheumatoid arthntis (JRA) were compared to an equd sample of healthy childnn on
àaily physical activity levels using a 3-day activity record. The investigators hypothesized that
childm with JRA would be las active than their healthy counteqsits. The 3day activity record
was completed by parents. and pmvided data on the type and intensity of the activities at 15-
minute intervals. Mean physical activity values w m significantiy lower in JRA patients than for
controls.
In a study of Quebec chilâren and youthy the 3-&y activity diary was used to examine
the relationship between puimonary function and habitua1 physical activity in 424 boys and 366
girls (ages 9-18 yem). Estimates of daily energy expenditure and time spent in moderate to
vigorous physical activity were computed h m the diary. R d t s demonstrateci that habitua1
physical activity was not associated with puhonary function in this sample of childmi and
adolescents. The investigators speculated that this lack of association could have been due to
inadquate stimulus, age, growth status, and type of activity.
The diary offers several advantages. Data cm be collected for many subjects
simultaneously, and the type, dmtion and hrquency of the activities can be recorded. This
technique incm a low cost to the investigator, and an estimation of energy expendihin is
possible. Due to a possible reduction in sccuracy over long periods of data collection$' however,
phone cals and careful description of the instniment rnay be necessary to encourage accuracy
and complcteness.

2.5.5.2 QUestionnPirwP
Many questionnaires have been designed to quantify physical activity for various periods,
including: the previous 24 hours, one week, three months, and one year. Attempts have dso been
made to quanti0 Metime and occupational physicai activity, and to estimate usual or habitml
physicai activity. These questionnains are either self-administereâ, or administercd ui-puson or
over the phone by an interviewer?' Several of the more commonl y cited questionnaires are
described below . The Revious Day Physical Activity Recall (PDPAR) requires subjects to recall after-
school activities h m the prwious day. Activity is recordai in 30-minute intervals with a rating
of relative intensity provided by the subject. A listing of common youth activities is intendeci to
aid in subject recall. One studJ4 concludeci that PDPAR provided an acceptable estimate of
relative energy expenditure over an 8-hour recording period and accurately identified bouts of
moderate to vigorous physical activity. Although this instrument provides a summq of type,
fnsuency, intensity, and dmtion of the activities, then are iimitations. Results depend on the
accuracy of a one-day mail over an 8hour period, which may not be representative of usual
physicai activity participation. A validity study was perfonned in ol&r children only, and the
appropriateness of PDPAR for younger children is ~nascertained?~
The Physical Activity Questionnaire for Older Children (PAQC) is a self-atiministered
7day mal1 measun designcd to evduate moderate to vigorous habitual physicai activity during
a specific season. Physical activîty is describecl as sports or games that make you bnathe or
sweat hard, or maice your legs tirrd An activity score is calculateci h m a compilation of 9
questions. Although the PAQC was show to ôe a cost-efficient methocl of assessing children's
physicai activity during the s c h d it c m o t bs used to esbcmstt caloac expenditurc, is not

designed to UUKSS summer or holiday levets of physicd activity, and Qes not discriminate
between moderate and vigorws physical activity levels.
The Godin-Shephard Physical Activity Survey is a simple, quantitative physical activity
self-report masure in which subjects report the number of times in an average week that they
spent more than 15 minutes in activities classifieci as mild, modemte or strenuous. Examples of
activities in each of the thne categories is pmvided to subjects? This instrument was found to
be diable and positively comlated with PAR in one study, and investigators concluded that it
could be a usefiil self-report measure in young childrai? However, this insrniment may be
subject to recall bias as individuals must ncail theû participation in physical activity over seven
days.
The Habitua1 Activity Estimation Scale (HAES) is a self-report instrument âesigned to
estimate habitua1 physical activity. Completion of the HAES entails estimating the proportion of
time spent at each of four different activity categories for a typical day?* The HAES hm ôeen
used in both hedthy and ctuonically ill pediatric populations. In 36 childnn with acute
lymphoblastic leukemia, bone mass, minerai metabolism and physical activity were assessed.
The HAEs was completed for the most recent weckday and weekend day at 6-month intavals
over the course of the hempy? In a group of 156 grade nine students in Southem Ontario, the
relationship between babitual physicd activity, as estimateci thtough the HAES, and self-
perceptions of physical activity among Native and non-Native adolescents was e ~ a l u w d ~ ~ In an
investigation whkh examined normative values for lumbar spine bone mass in childnn in
relation to age, gender, dietary intake. and physical activity, the KAES was also employed to
assess physical activityPL Although îhis instrument hm wt ban used to estimate cnergy

expenditure, these stuciies have &monstrated successful use of the HAES as a seEreport
instrument in different populations
Investigators have attempted to determine the accuracy of the HAES in the following
thne studies. The sensitivity of the HAES to &tect change in activity patterns was evaluated in
24 hypoactive children (ages 5-16 years) with chronic conditions. Parents completed the HAES
for their childnn prior to and following an 8-week outpatient program &signecl to incrase
physical activity. Significant increases in physical activity were demonstrated in comparing the
two parental reports of activity.'* In a study of 52 girls (6-12 years), the relationship between
percent body fat, body mass index, and inactivity was evaluated. Parents reporteci the activity
levels of their children using the HAES for a typical weekday and typical weekend day.
Significant, positive correlations were demonstrated for inac tivity with both percent body fat and
body mass index?' In a sample of 17 schwl children, a positive and significant conelation was
found between activity rneasured by a Caltrac accelerometer and the active category of the
HAESPZ Although finther vaüdation of the HAES is desirable, results from these investigations
demonstrate bat the HAES is a practical and convenient tool that provides an acceptable level of
accuracy in measuring habitua1 physical activityPO
2.553 Summ~ry of Sell-Report Instruments
Questionnahs and diaries are practical and inexpensive tools used to quantify physical
activity in epi&miological studies. Research is stiii necded. however, to determine the validity
and nliability of these measms. Validation is challenging due to inadequate criteria by which to
judge these self-report masures. An instniment such as the HAES gives subjects a bill range of
activity options, h m inactivity to high activity. lessenhg the likelihood of b i d estimations
which might occur if only high activity Ievels w m npoireds8 nie bcst techniques will captuse

ail types of physical activity, including occupational, leisure, and household In addition, the
instrument should be able to quantiry the type, duration, frequency and intensity of the activity. It
may be necessary to integrate the use of two different activity measures into one study in order to
capture al l dimensions of activity.
25.6 Summary of Physicai Activity Measurememt
Many methods are avdable to measurc habitual physical activity. The quantification and
pmfiling of habituai physical activity is necessary in order to follow these pattems over the, and
to examine the association of physical activity with other important variables, such as lung
function in cystic fibrosis. An additional importance of the quantification of physical activity is
to explore potential cornlates of physical activity participation. This knowledge could M e r
explain differences in activity pattans betweea groups. and promote the adoption and
maintenance of regular physical activity participation.
2.6 Potential Correlates of Phvsical Activitv Partichation
As the health benefits of reguiar physical activity are well estabüshed in adults, the
habitual physical activity patterns of children and youth are also kginning to be investigated
more closely. Studies have suggested that an active childhood may pndispose individuals to
similar activity patterns in adultho0dp3 and may subsequently d u c e the risk of c h n i c
diseaseeU The quantification of habituai physical activity in childhood is an important,
preliminary step in understanding this association,
There is also a necd to study the potential comlatea of exercise behavior in childhood
and adolescence. These fxtors may help to explain the differences in self-motivation between
active and inactive individuais, and dlow for the establishment of guidelines to promote regular
participation in physical activity* Agc and gcada have alrieady kai recogaized as important

cietednants of exercï8e behavior, but modifiable fiwtors such as psychosocial and
environmental variables are of spccial interest, and rcquire hir<her studYew
The potential comlates of physicai activity behavior cm be summarized into three
categories. Persod chot~~teristics include age, seif-motivation, weight, and personal attitudes.
Envirolunental ckructerisrks cornpise access to facilities, family or peer influence, and
climate. Activity chamcteristics encompass activity intensity and type." In the CF population,
understanding the potential detemiinants of physical actinty couid have invaluable implications
for health c m professionais who maice recommendations on exercise participation to patients.
Studies in the healthy population have aiready proposeà potential comlates of physical activity
participation.
Modifying physical activity patterns through changes in the environment appears to k
more practical than implementing expensive public intervention pmgrams. A study was
conducted in 110 college students to examine variabks that may influence physical activity
behavior. The physical environment was the pximary variable of interest. In this investigation,
self-report items were uscd to assas environmental variables at home, in the neighborhood, and
on fnquently traveled routes. Home exercice equipment and accessibility of exercise facilities
were significant comlates of physical activity participation. After adjustrnent for neighbohood
sociocconomic status. however, home exercise equipment was the only significant cornlate."
In a p u p of 528 chiloiren (mdian age=ll yem), demographic, psychosocid, and
environmeneal dctcnninants of physicai activity were assesseci. Age, gender, television watching,
and la& of exercisa quipment in the home w a e found to be significant comlates of low
activity status aftaebination of non-8igDiticant variables. Rcsdts suggestcd that p m t s can

produce a home nivitonnient conducive to physical activity involvement by monitoring the time
that their childnn spend watchiag television, aud by providing wess to exercise equipmentP6
Robinson et al sought to evaluate the relationship between hours of television viewing,
adiposity, and physical activity in 671 f e d e adolescents (mean ag-124 years). Wours of after-
school television viewing, physical activity level, and stage of sexual maturation were assessed
with self-report instruments. In this sample, resuls suggested a weak association of television
viewing time with adiposity, physicai activity, or change in either over tirne? More nsemh is
needed to further assess the relationship between physical activity and television viewing.
For 30 Young children (ages 5-9 yem) and their parents, investigators sought to
determine the relationship between parent and child activity levels. The children exhibited
physical activity pattems that were similar to theu parents. These results suggesteâ that
children's physical activity participation may be incnased through the promotion of ngular
physical activity in their
Physical activity patterns are cletennineci by the complex interaction of biological,
psychological. social, cultural and environmental factors. No single variable can account for the
variance in childrni's physical activity participation. Further studies in both healthy and diseased
populations are needed to stimulate hypotheses and provide information for designing and testing
longitudind intervention prograrn~.~ Wective activity promotion interventions hold promise for
improving the hdth of both childm and adults h u g h the encouragement of exercise
involvement .@

METHODS
3.1 Overview of the St& Des@
This was a cross-sectional pilot study. The first component of the study was descriptive:
subject characteristics, nutritionai statu, pulmonary function measuranents, and habitual
physical activity levels of CF patients were dedbed. The second component was analyticai: the
relationship of pulmonary fùnction with habinial physicai activity, nutritional status, and exercise
capacity was explored.
3.2 Practical Planning and Irn~lementation
The study coordinator (graduate stuclent) conceptualized this pmject in September of
1998. The six-month planning period that foiiowed was necessary for the development of an
appropriate study pmtocol, and for securing project and ethics approval from HSC.
A thomugh literature search, conducted by the study coordinator, confirmed that nsearch
in the pmposed area was insufficient. This search entailed exploration of the PUBMED database
using the following key words: qsftcfibrosis, Mitml ppltycal activiîy, ppulmu~~~ryfunction~
and exetcise cqacity. While the quantification and evaiuation of habituai physical activity in CF
patients had not k e n adequately addrcssed, numemus studies had previously examined the
relationship between exerciee training programs and lung huiction. Thenfore, the study
coordinator concluded that the association ktwcen habitual physical activity and pulmonary
function needed m e r investigation in CF.
A second litcrature scarch was conducteci to assess the femiility and appmpriatcness of
diBertnt techniques useci to quantify phpical activity. Of particth intmst w a e ~ t ~ r c p o r t

instniments that could be s e E a d m i n i i e ~ by CF patients. Two instruments, which together
provideci a comprehensive profile of habituai physical activity, were chosen for this stuày.
Patients in the CF cliaic at HSC expenence frequent requests to participate in both
invasive and time-consuming tescarch snidies. A study coordinator must therefore infonn the CF
clhic staff of a new pmject, and gain thek approval prior to patient contact. For the cunait
pmject, support h m clinic staff was also intendeci to encourage maximal participation from
patients. In December of 1998, the study coordinator presented her thesis proposal at a weekiy
meeting attended by the CF c l i ~ c team, which included: one social worker, physiotherapist,
dietician, exercise ph ysiologist, biostatistician, five ph y sicians, two nurses. and three study
coordinators. The study coordinator invited the ch ic team to critique the proposal, offer
feedback and ask questions. The pmject received unconditional support, and the CF ch ic team
acknowledged its clinical relevana.
The study coordinator also arrangeci to meet individually with members of the cliaic
team. The physiotherapist offered a summary of her exercise recommendations for patients, and
discussed common problems in encouraging compiiance with therapy regimens. The exercise
physiologist contributed her observations on the wi& specrnim of physical fitness levels in CF
patients. Infonnai discussions with the pulmonary hction laboratory technicians proved to be
invaluable during subject rrcnlltment. The technicians helpeâ the snidy coordinator to identify
both potentiaî participants and those patients who were ineiigible due to chest exacerbations.
At HSC, all newly pfoposeâ nsc~rch pjects must undergo a comprehensive review
process wîth the Research Ethics Boani of the Rescatch Institute. The sndy coordinator prcpared
the pmject proposai pccording to established guidelines, which includcd designing the
appropriate consent and assent fomis. The 10-pagc proposai and appendices w a e submitted for

intanai review to cIinicians mthin the Division of Respiratory Medicine. Two intemai rtviewers
careflllly scn~tinized the project, and provided written and oral suggestions for improvemnt. The
study coordinator discussed the necessity for revisions with the reviewers and h a superviaor
prior to milMg changes. The revised proposal was nsubmitted to the R e m h Ethics Board,
and due to the non-invasive natm of this project, it nceived expedited appmval. The study
coordinator initiated subject m i t m e n t and data collection procedures in March of 1999.
3.3 Subiect Selection
33.1 EUgibility Criteii
Study participants were selected from patients (7-18 years) under the regular c m of the
CF chic at HSC (n=188). The number of eligible patients was determineci by extncting data
h m the Toronto CF database to determine how many patients had visiteû the HSC clinic over a
one-year penod (January of 1998 to January of 1999). Patients younger than seven years cannot
accurately perform the pulmonary function and exercise tests necessary for inclusion in this
study, and were therefore not approached to participate. Al1 other patients within the specified
age range who attendcd their three-month routine clinic visit within the designated study period
(March 4-June 6,1999) were deemed eiigible for participation (n=138). Patients w m excluded
if they presented a their c h i c visit with a chest exacerbation or were hospitaiîzed at this tirne.
Under these circumstances, the study coordinator decideci that their selfieport of habinial
physical activity would not k fepresentative of their usual physicai activity pattms.
3.3.2 Subject Recruitment
In oidct to f d t a t c efficient subject rtctuitmcnt, the study coo~nator nviewed cIinic
lists of acheduid patients prior to u c h of t b weekîy CF clinics. EIigible patients were
idencified bascd on tbeit age. Communication with chic staff allowed the study COOfdinator to

detenaine the most appropriate tim to a p p a c h patients. The thme other CF chic study
coordinators were consultai to ensure no overlap in subject recniitment.
Eligible patients were identified and approsçhed by the shidy coordinator while they
waited in clinic. These patients and their families were provideci with both a written and an orai
description of the study protoc01. and were given an oppommity to ask questions and to assess
the time requirements of their involvement. Benefits and rislrs of the study were outüned
Patients gave their informeci consait in W n g upon their agreement to participate. For children
younger than 16 yem, a parent provideci informed consent, and the child gave their o m
informed assent. The consent and assent forms are show in &pend& B.
During each Uuee-hour chic, the study coordinator made contact with as many patients
as possible. In an average clinic, a maximum of two patients could k successfully recniited
Generally, there was not enough time to recnait more than two patients. Depending prtidy on
the patient's understanding of the study nquirernents, the study coordinator spent between 20
minutes and one hour with patients. In addition, patients were often calleci away for routine
testing and consultation with clinic staff. In these cases, data collection was delayed. The study
coordinator had to wait for the patient to ntum to the waiting m m , pnventing the remitment
of other patients.
3.4 Data Collection
3.4.1 SubJect Data
For each patient rrcmitcd, the study coordinator miewed updated chic records to
obtain necessary subject d.ia The patient's age was calcuiateù h m th& d t m e n t and birth
dates. The clinic nurse mutinely collectô measurrs for height and weight and documents them in

the patient's fiie. These values were morded by the study coordinator, and uscd to compute a
masure of nurritionnl statu, percent of ideal weight.
Patients who refused to participate in the study wem documented In order to compare
these non-participants to the study sarnple, relevant data was dso coiiected h m their clinic
records. Subsequently, a cornparison of these hvo groups could be made.
3.4.2 Puimo~~~vy Fundion
Puimonary function tests are routinely conducted in CF patients in the pulmonary
function laboratory at HSC. These tests are designeci to identify and quantify the degree of lung
impairment." For the cumnt investigation, al1 study patients Wonaed pulmonary fuaction
tests either through full pulmonary function testing or spinwetry.
Spirometry is the procedure used to measure the rate at which the lung changes volume
during forced breathing maneuvers. The most commonly performed test procediin uses the
forced expiratory vital capacity maneuver. This procedure, in which the subject inhales
maximalîy and then exhales as rapidly and completely as possible, pmvided the pulmonary
function measuns necded for the culTent studY?O
At HSC, spirometry data is collecteci on the Vmax system (Sensor Medics Corp. Yoba
Linda, Califomia) according to accepted standards?' Pulmonary function variables are expressed
as percent of pmdicted value for height and sex? The four most common measmments are:
forced vital capsCity WC), forced expiratory volume in one second ml), peak expiratory
flow 0, and average forced expiratory flow over the middle 50% of WC
Complete data was available for all study patients on these four measUrCs. These tems are
further defined in 4pendUr C.

PEVi is the most reptoducible70 and sensitive indicator of disease severity? It has
previously been estabiished as the best pndictot of sW7nvai in fl For these nasons. FEVi
was the variable used to r e p e n t pulmonary function for ail data analyses.
3.4.3 Measurement of H;iibituai Pbysicai Activity
Two instruments were used in the cumnt study to quantifj~ habitual physical activity: the
Habitual Activity Estimation Scak and the 7Day Activity Diary. These instruments w e n chosen
because together they pmvided a comprehensive profile of habitual physical activity (frrquency,
intensity, type and duration), and could be seif-administered by the study patients. These
instruments are summarized in Table 3.1.
3.4.3.1 The Habituai Activity Estimation Serk (BAES)
The HAEs was initially designed as a ciinically feasible tool to assess habitual physical
activity levels in children with chmnic disorciers? In the HAES, as outlined in Appendix D, a
typical waking day is delineated by five periods: wake-up time, the thne main me&, and
bedtime. Activity intensity is partitioned into four categones: inactive fie., sleeping). somewhat
idve (i. e. , siîting), somewhcrt actiw (i. e.. waiking) and active (i.e., running). The HAES
captures data on the intensity, fkequency and duration of activity. The somewk active and
&ve categories were used to compiie the Acrivity scores* Patients were asked to recall one
d weekday and one ~ G M I Q I weekend day h m the past two weeks. They were then able to
complete the HAES. by estimating the proportion of timc spent in each of the four activity
categories for the specioed weekday and wetkcnd day nspectively. Data wcre coiiected for a
weekday and weekend day separatcIy to acwunt for any difft~tllccs in habituai activity patterns
for these two periods.

3.4.33 Tba 7 - h y Adlvitg Msrg
In addition to the intensity, hquency and duration of activity measured with the HAES.
the 7Day Activity ~ i a r y : ~ ~ as illustnted in Apperufa E, also captures data on the rype of
activity being perfonned For sevea consecutive days, study paîients useà the Activity Diery to
classify the intensity and type of their activity in 15-minute increments acconling to aine
pTedete&ed categories. Study patients listed the entin m g e of their activities, ngatdess of
intensity level. Category 1 repnsented inactivity (sleeping), Categories 2 and 3 npresented
sitting and standing respectively, Categories 4 and 5 represmted walking, Categories 6,7, and 8
represented physical activities of mil& moderate and hard intensity respectively, and Category 9
repnsented compctitive sport.
The Acriviry Diary Activity scores were compiled from cotcgories 4-9. For each diruy
entry, the patients were also asked to record specific details on the types of activitia they were
involved in. These entries allowed the study coordinator to constnict a profile of physical
activity, and smed as confirmation that the appropriate intensity level had beni documented. As
categories 1-3 represented varying leveh of inactivity, they were not incorporated into the
Activity score. These categories were important, however, as they encouraged patients to report
on the entire range of activity, decrrasing the chances for ovet-estimation of physical activity.
3.4.4 Administration of the LIAES rad the Activity Diary
The HAEs was self4dminisMed by ai l snidy patients in the clinic waiting area.
CompIetion of the two scaks (weekday and weekmd) typically nquind l a s than 15 minutes,
although a few patients nquir#l as long as 25 minutes to cornpletc it. Even though wrïtten
instructions and a sample entry wczc providtd to cach patient, the study coordinator offered
additional instruction and assistance as needed The completcd HAES waa ceninieci to the study

coordinator in clinic, who immediately examined it for completeness and accurscy. Missing
values or apparent m m were âiscwsed with the patient and comcted if necasary.
In clinic, patients were also introduced to the Activity Diary and given extensive
instruction on its p p e r completion. The study coordinator showed patients excerpts h m a
sample diary and reviewed the diffaent ceiegory definitions with them. Patients were sent home
with the diaries, and asked to prospectively record their activity for the following seven days.
During the completion period, the study coordinator telephoned each patient at leapt once to
encourage cornpliance and respond to any concems. The completed diaries were mailed to the
study cwrdinator for scoring and analysis.
The literature suggests that younger children are unable to provide an accurate
description of their own physical activity." Therefon, parents of children younger than 13 years
in the cumnt study were carefully bnefed on completion of the HAES and the Activity Diary,
and asked to serve as proxy nspondents. The study coordinator recommendcd that parents probe
their chilâren about their schwkelated activities, and where necessary, consult with teachers
and schwl staff. The childnn pmvided their parents with valuable input on their activities,
enabling them to cornpletc thcse measures.
3.4s Nutritionai Status
Measuns of height and weight wen used to calculate both height and weight percentiles
and percent of ideal weight, accordiag to standards of Tanner et al?* Although these standards
were publishd in 1965, the methods of meastument are considered superior, and oie mutinely
used h clinical rcscarch at HSC. nie hdght and weight pacentües illustraied whetha the study
patients d i f f ' fnrm the^ heahy pars in the sam agc-sex g r ~ u ~ ? ~ Percent of ided weight
was calculatcd as an hdicatot of nutritional statu.

To compute percent of ideal weight, the patient's height is f h t plotted on a growth cbsit
and the height centile is detelipuled. The ideai weight for height is detennined by finding the
weight on the same centile as that for height. age and sex. Percent of ideal weight is a moasure of
actual weight diviàed by ideal weight for height, multiplied by 1007 Pezcent of ideal weight
was previously found to be a diable indicator of nutritional statw in both healthy subjects, and
in childnn and aduits with CF?
3.4.6 Exedse Caprity
Exercise testing was pesfomed in those study patients who were scheduled for their
annuai exercise test on or near to their study rrcniitment date. The annual scheduling of the
exercise test and the three-month recruitment period meant that only a sample of the total study
patients underwent exercise testing on the same &y as study ncniitment. Exercise data was
accepted hwn the previous or subsequent chic visit (& 3 months) if the patient's ciinical status
had not changeci significantly beiwcm visits. based on the stability of their pulmonary function
test results ktween clinic visits. It has ban previously established that a change of less than
12% predicted in FEVI is within the normal range of ~ariabilit~?~
Patients perforrned a maximal, inmmentd cycling t d 9 0 n an electrically braked cycle
ergorneter (Rodby Electronik AB, Enhoma, Sweden). Similar to previous HSC
investigations?&" incnments were chosen b& on the patient's sex and height, so that the
patient typically terminateci the test in 8 to 10 minutes due to exha~stion?~ The last completed
minute of the exercise test was docmc~~ted as Uu patient's maximai workioad. niroughout the
test, patients b t h e d tluough a mouthpicce connected to a two-way Y-valve of low resistance
and dead space. Aeut rate (Lead II, ECG), oxygen saturation (Ohmeda, Biox 3700 pulse
oximetcr, Louisnlle, KY). inspirrd minute ventilation ~atiQnson-Cowan dry gas meter,

Manchester, England), mixed expired oxygen (Applied Eîectrochernistry oxygen aaalyzer,
Sumyvale CA), carbon dioxiâe (C02-44A rapid nsponse carbon dioxide analyzer, Fitness
Instrument Technologies Corp., Quogue, NY) and respiratory rate (themister) were monitored
continuously on an eight-channel recorder. Ox ygen consumption, carbon dioxide production,
tidal volume and respiratory exchange ratio were measund continuously on-iine through an
automated exercise testing pmgmm dtveloped in the exemise lab at HSC. Wood pnssun was
measured at rest and immediately after peak exercise by a mercury sphygmommometer.
The exercise test was conducted by an experienced exercise physiologist who evaluated
the validity of the data. In several study patients, a maximal effort was not achieved on the cycle
ergorneter due to maturity level and uncontroiIable coughing, and these data were not used The
exercise test provided data on the following mairimal exercise panuneters: heart rate, minute
ventilation, oxygen saniration, oxygen consumption, work capacity, and ventüatory resewe.
These terrns are defined in Appendù C. Values for percent body fat and lean body mass were
caiculated by the exercise physiologist prior to the exercise test. Percent body fat was computed
h m the sum of four skinfolds @iceps. triceps, subscapularis. and suprailliac)?' Lean body m a s
was calculated by subtracting the patient's fat mass (calculateâ h m percent body fat) h m their
total weight.
For the ppurposes of the current study, maximai oxygen consumption and d m d work
capacity were the two most relevant exercise parameters. In tht CF population, maximal oxygen
consumption has k e n suggested as a prcdictor of ~urvival,'~ while maximal work capacity has
been documented as an indicator of overaiî clinicai striais."

3AS7 CampUuiee with Physbthempy
Cornpliance with physiotherapy was an important variable to evaiuate in the cumat
study. Most CF patients are prescribed daily chest physiotherapy to meintain or improve their
pulmonary hction, yet compliance is difficult to encourage. Some patients deliberately replace
their physiotherapy with reguiar physical activity under their own assumption that the benefits
will be quivalnit. Patients who do comply with physiotherapy, on the other hand, may have less
time for participation in regular physical activity. A measun of compliance with physiotherapy
was essential considering its potential to confound the relationship between habitual physical
activity and puimonary function.
Patients were asked to rank their compliance with physiothmpy h m three possible
nsponses. This scoring system was pnviously developed for use in the CF population." The
choices, zero, one and ~ Y O represented poor, pamhl andfil1 cornplimice nspectively. The clinic
physiotherapist was able to verify or dispute the patient's response, if necessary.
3.4.8 Potential Corniates of Wysicai Activity Participation
Potential comlates of physicai activity participation were evaluated through a series of
questions answered by parents. The Pamt Questionnaire (PQ), as shown in Appendix F, was
intendeâ to provide data on environmental f ~ r s that could be nlated to the study patient's
participation in physical activity. The factors of interest included: parental activity level. the # of
organizcû activities that the child was involved in, pfoximity of the household to sporting
facilities, safety of the f d y ' s neighborhood, and the number of exercise-related items in the
home. The shidy coordinator compilcd the PQ fiom relevant questions pubiished in other
A description of the PQ is prmidcd in Table 3.1. surveys.

Table 3.1: Sumrnary of the survey instruments
s w e y nt Rvpasc Type of Approxûnate Recordhg Variables Administration Time to Period Asses&
Adniiaister
Habitual Activity Estimation Scaie wA=)
7-Day Activity Diary
To assess Seif- 15-25 Usual #of hm spent habituai physical administered in minutes week&zy at each of 4 activity levels by chic, patient and uctiviïy levets patient ncall and parentt weekend
day activity
To prospectively Self- 15-20 1-week # of hrs spent assess habituai administered at minutes / day at each of 9 physical activity home, patient activity levels, levels and parentt type of activity
P m t Questionnaire To examine Self- 10-15 Once @QI potential administered in minutes
correlates of chic, parent physical activity participation
parent's activity level, # of organized activities, pronimity to facilities, safety of neighborbod, home exercise equipment

3.5 S m l e Size
As determineci h m the CF database, 188 patients (7-18 years) made at least one mutine
visit to the CF c h i c between January of 1998 and January of 1999. This estimated numkr of
patients saved as the sampling h e for the c m n t pilot study. For the purpose of sample size
estimation, the study coordinator approximated that 50% of the eligible number of patients
would be schedulcd to visit the CF chic during the thnc-month rtcniitmenî period From these
94 potentiai participants, a sample size of 40-50 patients was p d c t e d The final sample size for
this study was 40 patients.
Logistics and estimates of feasibility were used to generate the estimated sarnple size
pnor to the onset of subject recruitment. Time constraints of CF patients in clinic, personnel
limitations, and refusals were the main limitations of sample size for this pilot study.
In order to conduct a longitudinal study based on the demonstrated trends of this pilot
study, a power calculation wül be needed. This power calculation is depicted in AppendLr G, and
will be the basis for a longitudinal study examining the relationship of FEVl with habitua1
physical activity , nutritional status and exercise capacity.
3.6 Data Andysis
The Statisticai Analysis S ystem (SAS), version 6.12, was the sofhvm package used for
statistical analysis. A permanent SAS dataset was c ~ t e d for storage of the snidy data.
3 1 Datasforhg
To compare the habituai physical activity data capnued by the HAES and the Activity
Diary, comparable activity scons werc needed B a d on the activity category definitions for the
HAES and the Activiiy Diary, cotegories 4-5 of the Activiîy Diary repmmted the somewhat
uctnte category of the HAES, and categoriw 6-9 rcprcscntcd the OCtiVe category of the HAES.

3.6.1.1 The HAES
The complete HAES âaîa was entercd into a Microsoft Exce1497 program tha it was
previously developeâ to compile activity data hwn die HAES. The program computed the totai
proportion of tirne (96) that the subject spent in each of the four activity categories (inactive,
somewhat inactive, sornewhat active. and active) for the reported weekday and w e e h d day
nspectively. These percentage values w e n subsequentîy converteci into hours/&y using a SAS
PwP='*
The final HAES Activiry scores, as depicted in Table 3.2, were compiled from the two
categories cepresenting the highest levels of physical activity: somewhat actiw and acrive. Based
on a pnvious study, habituai physical activity can be represented by a combination of the
sornewhat active and active categories (Total Activity), or by the active category (High Activity)
oniy?
For the curnnt study, separate scores were calculated for the HAES data to reflect
diffmnces between both weekday and weekend day activity, and total and high activity levels.
A Weighted Actbity score was ais0 compiled for each of the Total and Hi@ Activity levels to
npresent a combination of weekday and weekend day activity. The Weighted Aaivify score was
created by assigning a weight of five to the weekday activity and a weight of two to the weekend
activity, and then divided by seven.
3.613 T& Activity Dhry
The stuây coordinator developed score sheets for this study to compile activity data h m
the Activity Diary. As the subjects nported theh activity in Srninute increments, each 15-
minute t h e pcriod was &signateci as one unit. For each of the nine activity categories (1-9). a
summry n u m k was computed basai on the totai amber of uni& in that category. The total

number of hours spent in each category was subsequently calculated (total number of units 1 4).
The Activity Diary Active scores. as depicteci in Table 3.2, were based on activity
categories 4-9. In a previous study, a compilation of cutegories 6-9 repsented moderate to
vigorous physical a ~ t i v i t ~ . ~ ~ which was tenned High Activity for this investigation. Subsequently,
a summation of nitegories 4-9 repnsented mild to vigoroue physical activity. which was tenned
Total Actiwity. Similar to scoring for the HAES, separate Activity Diary Actr'vity scores were alao
cornputeci to represent weekday and weekend activity, and Weighred Activity scores were
calculated to combine weekday and weekend day activity.
3.6.13 Activity Type
The activities listed in the Activity Diary were classified individually by their Vpe. A
listing of the different types of activities (categories 4-9 on1 y) was first compilecî from all the
Activity Diaries. The activity types and the time spent perfonning each type were then dlocated
to an activity classification within their spedic activity category. For each activity category
(categones 4-9). the eight possible activity classifications were: porsonol care, domestic wo&
school-related, employment, unstructund play, wwalng, p o r t and tmd$ned. Histogramo were
matcd to compare the amount of time spent in each activity classification.
3.6.2 Data Qwuty Contn,l
The raw dita was enterai into the SAS dataset by the study coordinator, and data checks
were conducted to ensun the accuracy of the data Maximal and minimal values for al1 variables
were examine& and any discnpant values were checkcd against the raw drta In addition, a
netarch assistant u n f d a r with the study entered the data a second time into a t e m m
dataset. A complnson program written in SAS connrmd the accuracy of the data entry.

Table 3.2: Activity scons compilecl h m the BAES and the Activity Diary
High ~criviiy'
Weighted Total Actbity
Weighted High Activity
Catenories: Carnories :
Somewhat 4+5+6+7+8+9 active* + active'
Cate~ories: Catenories :
Active only 6+7+8+9
[(S * Weekday [(Weekday Total Total Activity) Activity) + + (2 * Weekend (Weekend Total Total Activity)]/7 Actinty)]n
[(5 * Weekday [ ( ' k d a y High High Activity) Activity) + + (2 * Weekend (Wcchd High High Activity)]!7 ActiVity)]n
t scores for both weekday and wcekend &y rtspcctjvcly tt somewhat active: e.g., wallting
active: e.g, biking

3.63 Dcreelpîîve StatWct~
Univariate analysis was conducted to compute the range, fnquency. man and standard
deviation (SD) of each study variable. SAS m a m pmgrams were used to compute weight and
height percentiles, percent of i&ai weight. and m e n t pndicted values for pulmonary function.
The study dataset was merged with data files in the Toronto CF database to obtain additional
subject data, including biah date and gender. A dummy variable was created for gender, a
categorical variable.
PROC UNVARIATE was used to compare weekday and weekend Activity scores by
means of a p a i d t-test. PROC 'LTEST was used to evaluate whether any statistically significant
differences wne present ktween males and fernales.
3.6.4 Pearson y s Correlation
Pearson's comlation was used to assess the strength of the association between pairs of
variables through the creation of comlation d c e s . The significance of a comlation
coefficient is a function of both the magnitude of the conelation coefficient (R), and the sampie
size. Therefore, the importance and sangth of each celationship was assessed in addition to the
significance of the conelation coefficient R-square values were assesseci as an approximation of
the amount of variabiiity in one variable that was explained by association with anothet variable.
Scattet plots were also createâ for each of the pairs of interest to evaiuate whether outlying data
points w e n causing the correlation coefficient to be larger or smailer than the overail trend?
The comlations of the different HAES and Activity DÙwy Activity scores with FEVL w m
the primmy focus. As part of mode1 building, the comlation coefficients and pmbability vatues
(p-vaiues) were examined to determine which of the diffenat activity scores &monstrPted the
strongtst relatioaship with FE&. The HAES and Activity Diary ActMty scores that Qmionstratcd

both significant pvalues and the highest comlation coefficients when snaiyzed with FWl wcre
of most interest for regression andysîs.
The correlation coefficients for the association of the ActMry scores and FEVl with age.
gender, peEent of ideal weight, meXimal oxygen consumption. maximal work capacity, and
compiiance with physiotherapy were of secondary interest. The süength of these comlation
coefficients were imponant in esdmating which variables might be important in the relationship
between FEVi and the Activity scores, and thus practical for multiple regression analysis. In
addition, the comlation of the HAES Activiv scores with the Activity Diary ActrYity scores w m
examined to estimate the degree of consistency between these two measunments.
3.6.5 Regmaaion Anaîyics
In sepiuate multiple correlation analyses, either FEVi or one of the Activity scons was
considerad as the outcome variable as the direction of causation between lung h c t i o n and
habitua1 physicai activity could not be established h m this pilot study. The ActWity scores used
in the final ngnssion models were chosen based on the strength and significance of the
association dernonstrateci in multiple comlation.
The expianotory variables were:
i) FEVl or an Activity DiaryMMS Activity score (whichewr wa9 not the outcome), ii) percent
of ideal weight. iii) one of maximai oxygen comumption, or manimal work capacity, iv)
compiiance with physiotherapy, v) age, and vi) gender.
3.6.5.1 Multiple Condation
Muitipk comlations between variables were examined by means of the ail possible
regression mbsets technique. AU possible regession anaiysis rcquires the fitting of every
possible regnasion cquation thrt involves the outcorne variable plus the explanatory variables.

As m e r model building for the final multiple regnssion analysis, the technique of 1
possible regession analysis was used to find the best fitting model. It is pferable to stepwise
regnssion, where important nlationships among variables may be misscd. This technique was
well-suited for this study because the number of explanatory variables was rellveiy mail. The
adjusted R-square values and the Cp Mallow statistic were evaluated to detemine the best
models. PROC REG in SAS produces efficient output of these statistics.
The model that was most pSVSUIlonious (i.e., the fewest explanatory variables explaining
the most variability in the outcorne variable as determincd by the adjusted R-square values), and
for which the Cp Maiiow statistic most closely matched the number of parameters in the model
was considered the be the strongest candidate for final multiple regression analysis.
3.6.5.2 Modehg FEVl as the Outeome Variable
Multiple linear regression involves expnssing the continuously distributed outcome
variable as a linear function of a certain number of explanatory variables." PROC REG in SAS
was used to generate mon detailed results of the best multiple ngression models selected h m
the results of multiple comlation. The adjusted R-square values, parameter estimates and
standard errors were examined to evaluate changes in the amount of variability explained with
additional variables in the model. An interaction term was also included.
RESULTS
4.1 Descri~tive Statistics
The study variables are presented as mean f standard deviation (SD) for males. females.
and the total study population. It was important to look for any ciifferences between males and
femaîes in this sampie because of a nported poorer sumival in fernale CF patients compand io
males?8
4.1.1 Patient Characteristics
4.1.1.1 Study Participants
Twenty-three males (57.5%) and 17 females (42.5%) were recruited nom the CF c h i c at
HSC over a three-month period (March 9-June 4, 1999). Subject characteristics for these 40
study patients are detailed in Table 4.1. Mean height and weight values below the 5 0 ~ percentile
in this group of patients indicateâ subnormal gr0wth.l3 Percent of ideai weight, however, did not
reveal any &gne of maln~trition.'~
4.1.1.2 CF Population Values
Table 4.2 displays the characteristics for 77 males (55.8%) and 61 females (44.2%) who
met the study eligibility criterion (7-18 yem) and also attended the CF clinic during the three-
month study recruinnent peW. The study sample was similar to ali eligibk CF clinic patients.
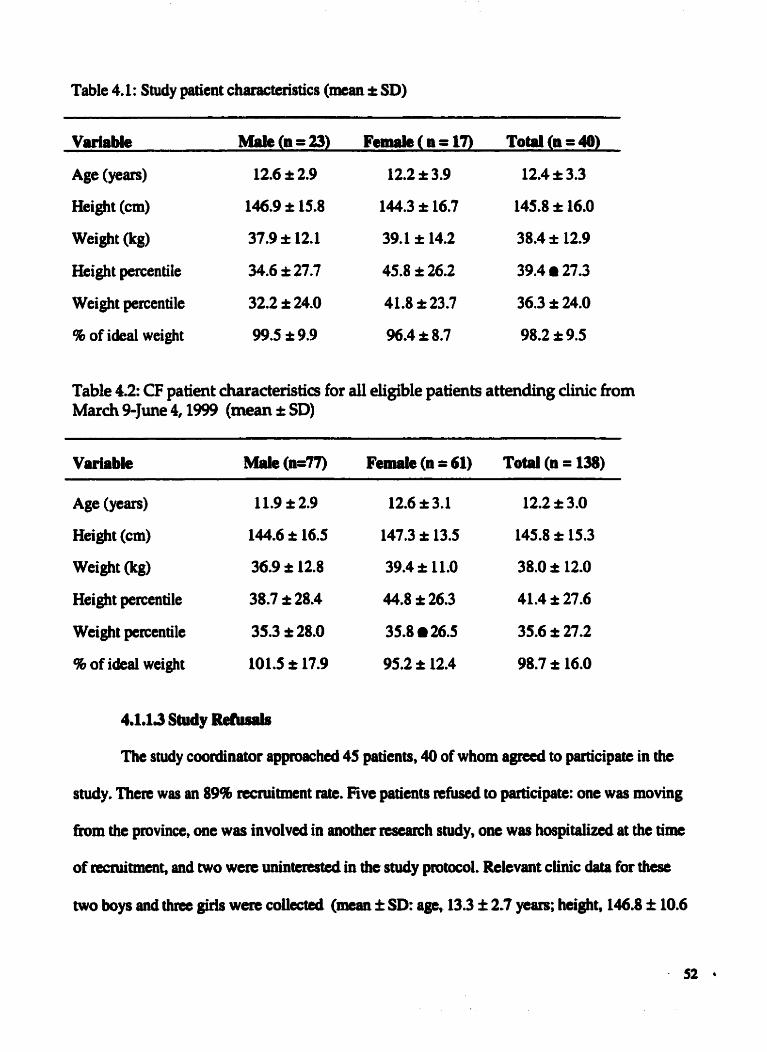
Table 4.1: Study patient characteristics (mean i SD)
Variable M'aie (a = 23) Feude ( n = 17) Total (a = 40)
Age (ye-) 12.6 * 2.9 12.2 + 3.9 12.4 4: 3.3
HeiQt (cm) 146.9 î 15.8 144.3 + 16.7 145.8 + 16.0 wei%t (irg) 37.9 î 12.1 39,l i 14,2 38.4 î 12.9
Height percentile 34.6 i 27.7 45.8 î 26.2 39.4 r 27.3
Weight paantile 32.2 I 24.0 41.8 î 23.7 36.3 î 24.0
% of ideal weight 99.5 I: 9.9 96.4 + 8.7 98.2 i 9.5
Table 4.2: CF patient diatacteristics for al1 eligible patients attending dinic fiom March 9-June 4,1999 (mean ,: SD)
Variable Male (n=77) Femik (n = 61) Total (n = 138)
Age (Y=@ 11.9 i 2.9 12.6 3.1 12.2 I: 3.0
Height (cm) 144.6 i 16.5 147.3 * 13.5 145.8 + 15.3 @g) 36.9 * 12.8 39.4 & 11.0 38.0 * 12.0
Height percentile 38.7 î 28.4 44.8 î 26.3 41.4 i 27.6
Weight percentile 35.3 î 28.0 35.8 26.5 35.6 î 27.2
8 of ideal weight 101,s î 17.9 95.2 & 12.4 98.7 i 16.0
4.1.13 Study R e k d s
The study coordinator apploachcd 45 patients, 40 of whom agned to participate in the
study. There was an 89% rccruitment rate. Five patients refused to participate: one wos moving
h m the province, one was invoIved in another rescarch sndy, one w u hospitaiizcd at the tim
of recruitment, and two wen UIUIItcrested in the study pmtocol. Relevant clinic daîa for these
two boys and thres girls w m coilected (man f SD: age, 13.3 f 2.7 ycrw; height, 146.8 f 10.6

cm; weight. 36.7 i 7.5 kg; height perccntile, 29.2 i 20.5; weight percentile, 26.3 f 239; percent
ofi&d weight, 97.9 i 17.8). This p u p of study nfusals, who also had subnonnal growth and
nomel nutritional statue, did not differ h m the study patiente.
4.1.2 Measmement of Eabitual Phpicai Activity
4.1.2.1 The HAES
AU study patients completed the HAES either in clinic, 97.5% (39/40) or at home, 2.5%
(1/40). Results from the HAES indicated sigdficantly higher scons for the Total and High
Activity categoties of a weekend day than a weekday, suggestiag that the study patients were
mon physicaüy active on a weekend day than a weekday (sec Table 3.2 for clarification of the
Activity scores). Figure 4.1 depicts the average activity levels for each category of the HAES.
The reported time spent in the Total Activity category for males and females was slightly lower
than that reported in another CF population?2
Although not statistically significant, maies consistently nported more time than females
in the High Activity category, while females reported more tim than males in the Total Activity
category. These results are shown in Table 4.3.
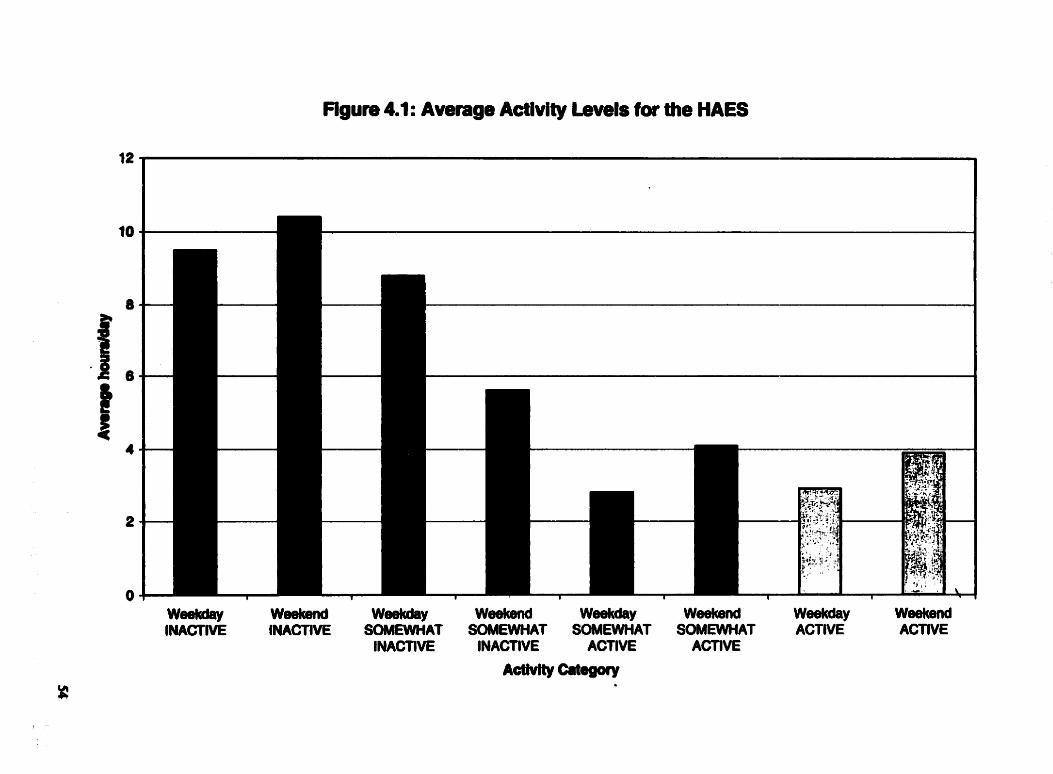
Figuie 4.1 : Average Activity Levels for the HAES
w-Y w- we-Y weekend W-kday wee(cend Weeûday Weekend lCYACTlVE lNACTlVE SOMEWHAT SOMEWHAT SOMEWHAT SOMEWHAT ACTIVE ACTIVE
INACTIVE INACTIVE ACTIVE ACTIVE

Tabk 4.3: Activity hours (hodday) compiled b r n the HAES (mean t SD)
Maies (n = 23) Femaies (a = 1'7) Totai (n = 40) Activity Category
Weekday Score
Total Activityt 5.5 + 2.8 6.0 î 2 3 5.7 î 2.8
High ~ctivity'l 3.1 r 1.7 2.6 1.3 2.9 î 1.5
Weekend Day Score
Total ActivitYt 7 3 + 3.5 8.2 I 2.4
High Activitye 4,s I 3.3 3.1 2.5
Weighted Score
Total ~c t iv i t~ ' 6.2 f 2.7 6.6 f 2.5
High ~c t i v i t~* 3.5 + 2.0 2.7 f 1.3
t somtwhat active + active tt active
4.1.2.2 The 7-Day Activity D h y
Thirty-nine patients (97.5%) a m to complete the 7day Activity Diary at home. One
patient did not agree because he was moving residences, and did not thînk that the diary wouid
be representative of his usual activity. From the 39 patients who were sent home with the
Activity Diary, 33 (84.6%) retumed th& diaries by mail or at a subsequent clinic visit to the
stucly coordinator. Thirty-two of the 33 retumed dimies (97%) were filled out according to
instructions. One àiary was too iacomplete for any score to be estirnated. The study patients who
completed the Activity Diary did not differ frnn those who did not complete it.
The Activity scores reportai in Table 4.4 were based on an average of the 5 nported
weekdays or 2 reported weekend days such that a cornparison with the HAES could be made (see
Tabk 3 2 for clarification of the Activity scores). Average activity levels are iiiustrated in
Figure 4.2. The Activity scons showed similarands to those of the HAES. Aithough not

statisticaily significant, d e s consistently spent mon time in the High Acti~ty category, while
females spent more time in the Total Activity category. Significantl y more tirne was reporteci for
the High and Total Activity categories of a weekend &y than a weekday.
Table 4.4: Activity hours (hodday) compiled from the 7-Day Activity Diary (mean + SD)
Activity Category Male8 (a = 17) Femaies (n = 15) T o u (n = 32)
Weekday Score
Total ~ctivit~' 3.5 * 1.1 4.3 * 1.2 3.9 I 1.2
High ~ c t i v i t ~ ~ 2.3 î 1.0 1.9 * 1.2 2.1 * 1.1 Weekend Day Score
Total Activityt 4.7 î 1.9 5.1 î 2.8 4.8 * 2.3 High ~ c t i v i t ~ ~ 3.1 i= 1.7 2.2 & 2.0 2.7 î 1.9
Weighted Score
Total ActivitYt 3.8 I 1.3 4.5 + 1.4 4.1 f 1.4
High ~ctivity't 2.5 I 1.1 2.0 I 1.3 2.3 f 1.2
t catcgory 4+5+6+7+8+9 tt catcgory 6+7+8+9

Figura 4.2: Average Activity Levels for the Activity Diary

4.1.2.3 A Compuiion of Data h m the HAES and the Activity DtPry
In comparing self-report of activity h m the HAES and the Activity Diary for patients
who completed both instruments, significantly more thne was reported in both the Total and
High Activity categories (weekday and wakend) as reported with the HAES. This suggests that
the HAES and the Diary may have been capniring different dimensions of activity.
4.1.3 Rilmonary Funclion
Pulmonary function data, illuscrated in Table 4.5, were coUected for al1 patients.
Depending on the statu of their lung disease ml), patients were classifiecl as sevcrely (do%
predicted), moderately (50-8046 pndicted) or rnildly (> 80% predicted) impaireci, Twenty-six
patients (65%) had mild pulmonary impallment, 1 1 patients (27.5 9) haâ moderate impairment,
and thne patients (7.5%) had severe impairment, demonstrating that this sample was comprised
rnainly of patients with mild pulmonary disease. This high prevalence of mild lung impairment
has been previously documenteci for pre-adolescent and adolescent CF patients?
Table 4.5: Percent of precücted pulmonary function (mean i SD)
Variable mes (a = 23) Fe- (n = 17) ToW (a = 40)
ml 86.7 + 18.4 84.2 I 24.5 85.7 i 21.0
FVC 89.8 i 16.0 90.9 A 18.0 90.3 I: 16.7
FEF25-75 74.8 î 28.8 66.8 +31.6 71.4 * 29.9
PEF 83.5 î 15.2 80.8 î 21.8 82.3 r 18.1
Definition of abbreviations, sec Appendix C

4.1A.l A sub-sample of study patients
Only patients scheduled for their annual exercise test on or near to C+ 3 months) their
nmiitment date had data on exercise capacity Although exercise data was available fm 26
patients (65.0%), the exercise tests fiam 2 patients (1 M, 1 F) were considend invaiid by the
exercise physiologist. The female patient was too immature to perform the test, and was
uncooperative with the testing protocol. The male patient was unable to complete the test due to
uncontrollable coughing. These results were not included in the final analysis. Twenty-two of the
26 patients (85%) completed their exercise test on the same day as their study ncruitment date.
The remaining 4 patients (15%) completed their exercise test prior to, or foilowing their
rrcniitment date & 3 months). As a nsult of the two invalid exercise tests, final exercise
capacity data was avaüable for 24 patients.
4.1.4.2 Amessrnent of exercise capacity
Values for exercise parameters are docurnented in Table 4.6. Study patients (n=24) had
mean maximal values for workîoad and oxygen consumption slightly lower than those ceported
in a similarly aged group of hdthy ~hildren,~ suggesting that these CF patients had reàuced
enmise capacity compared to normal, school age ~ h i l d r e n ? ~ ~ Fernales had a statisticaily
significant higher percent body fat than males. These values are consistent with trends presented
elsewhere." reflecting mual clifferences between heaithy boys and girls?'

Table 4.6: Exercise parameters (mean t SD)
Variable Mlaiea n Fernales n Total n
(beatslmin) 179.0 k6.1 14 175.3 + 14.4 10 177.5 * 10.3 24
V-(~min) 70.6 f 24.1 14 60.6 I 19.9 10 66.5 i 22.5 24
Sa02 at max (96) 9S.Oî1.4 12 93.6k3.6 9 94.4î2.6 21
Vo2,max min) ~.s*o.s 14 1.2î0.4 10 1,4*0.5 24
v 02max (ml.kg%nin-L) 39,7 i 5.8 14 34.5 î 7.9 10 37.5 i7.1 24
Wmax (46 predicted) 82.2 i 9 .8 14 86.6 a 19.1 10 84.0 î 142 24
MVV 72.2 î 26.1 15 64.4 t26.9 12 68.7 f 26.3 27
Q M W 97.0 I: 18.1 14 103.4 I 35.4 10 99.7 î 26.2 24
% body fat 12.5 î 2.9 15 22.3 *3.2 11 16.7 î 5.8 26
Lean body mass (kg) 32.3 * 11.2 15 27.6 * 9.6 11 30.3 î 10.6 26
Max, parameter at maximal woriûoad; Definition of abbreviations, sec Appeadix C
4.1.5 Cornpliance with Pbgsiothecapy
Patients were asked to rank their compiiance with physiotherapy h m choices of O, 1 or
2. The mean compliance value was 1.6 î 0.6 (males, 1.7 t 0.6; fernales, 1.5 t O.7), which
indicated a hi& reporteci mean level of cornpliance with physiotherapy.
Parent questionnaires, comprised of six questions, were successfully completed by 97.5%
of parents. One parent took the questiomsire home to complete because of the constmints in
chic, but did not retum it to the study coordinator. The data are presented in Table 4.7
In Question 1, parents ranked their own kvel of physical activity participation, based on a
scak of 1-5 (1, inactive; 5, vigomus physical activity). In Question 2. patents reportcd the
number and type of organized physical activities in which their childrcn were i~ivoIved. The most

commonly listed organizations were a sport's team or league (33.3%). and public park or
m a t i o n department activities (28.2%). In Question 3, the child's accessibüity to exercise
related facilities in their community was assessed. The most commonly cited facilitics were a
public park (949%). playing field (82.1%). skating rink (74.4%). and public recteation center
(71.8%). In Question 4, parent's evaluated the safety of theK neighôorimd (1. very unsafe; 5.
very safe). For Question 5, parents chose from a list of chmcte~9tics that b a t describeci their
own neighbohood. This question was intended to estimate the number of neighborhood-nlated
features that were either conducive or non-conducive to exercise. The most commonly cited
feanues were a high fresuency of people walliing or exercising (84.6%). enjoyable scenery
(82.1%). sidewaiks (79.5%). and street Lights (69.2%). Findly, in Question 6. parents estimateci
the number of exercise-nlated items in their home. The most commonly cited items were
running shoes (100%). bicycle (97.4%), sports equipment (Le., b a h and racquets) (97.496). and
skates (89.7%).

Table 4.7: Potential cornlates of physical activity pdcipsiion (man t SD)
Variable Males (n = 22) Femaim (n = 17) Totai (n = 39)
Parent's activity level (range: 1 to 5)
Numbu of organizeâ physical activities (range: O to 8) 1.5 * 1.4 1.2 I 1,O 1.3 I 1.3
Accessibility of facilities (range: O to 18) 9.3 * 3.8 10.4 * 4.4 9.8 k4.1
Neighborhood spfety (range: 1 to 5)
Neighborhood feaaires conducive to exercise 2.4 * 1.3 2.3 I 1,3 2.4 î 1.3 (range: -4 to +4)
Exercise-rdated items in the home (range: O to15) 7.0 î 1.7 6.8 I 1.9 6.9 I 1.8
4.1.7 Activity Classification
The activity types reported by patients for Categories 4 to 9 of the Activity Diary
represented activities of mild to vigorous intensity. The study coordinator compiled a list of
approximately 200 terms used by patients to describe their activity. This list is found in Appendix
H. Many activity types were listai wider mon than one category of intensity. Soccer, for
example, was listed by the same individual in both Categories 8 and 9. The 2 0 t e m were
subsequently aüocated to one of 8 classifications: personal cure, domestii work, schwl-related,
entploynient, unstmcturedplay. walkhg, sport, and undefine& These classifications were chosen
to encompass and describe al1 the diffcrent activity types in the most specific manner possible.
The iesults of this activity classification are prcsentcd in Figures 4 3 to 4.8 for each of the six

categories (4 to 9). The results are presented in average ddly minutes. The following section
outlines the trends in the data according to activity classification.
4.1.7.1 Pemnal Care
Personut cure encompassed activities such as getting ready for school or bed, and CF
seIf-treatment. These types of activities were only reported for the two lowest intensity
categones, categories 4 and 5. In Category 4, an average of 53 daily minutes was reporteci, with
this number decreasing to 0.4 daily minutes in Category S.
4.1.7.2 Domestic Work
Domestic work (household and outside chores) incluàeû cleaning, cooking, dusting,
mowing the lawn, shopping, watering the plants, taking out the garbage. and raking. Activities
included in this classification were nported in Categories 4,s. and 6. The average time spent in
this classification deciined with increasing intensity of the category. In Category 4, 13.0 average
daily minutes were reported, with this number decreasing to 4.0 and 2.3 minutes for Categories 5
and 6 respective1 y.
4.1.73 School-Related
Childm also reported their participation in specific school-reluted ach'w'ties such as
classmom activity, homework, acting, helping the teacher, and school field trips. Schwlielated
activities were reported for Categories 4,s and 6 on1 y, indicating that these activities were not of
a high intensity. The highest report for these activities is 2.0 daily minutes for Category 4,
followed by 0.9 minutes for Category 5 and 0.13 minutes for Category 6.
4mle7m4 Empbyment
As this study sample was compriscd of chilârcn as old as 18 years. an employment
classincation was inclpded Employment included Ifter-school and weekend job, in addition to

delivering papem. These Pctivitie~ were Listed in Categories 4 to 7, indicating the range of
intensity requhements in these jobs. For Category 4.62 average daüy minutes were spent in
employment, with this number dtcreasing dramaticaiîy to 0.13 minutes in Category 5. h m
Category 5 to Category 6 there was a large inmase to 7.4 minutes, foilowed by a demase to 0.8
miriutes in Category 7.
4.1.73 Unstmchucd Play
Both childm and adolescents engage in fkee play. Although this type of activity does not
meet the structured definition of sport, it cm nevertheless be quite ckmanâing, and yet erratic in
nature. Uhstmctured play was reported for al1 six categonui, Categones 4 to 9. The activities
that were labtled in this classification included group games (hide and seek, hopscotch), recess,
playground activity. swinging, and bail playing. In Category 4,4.6 average daüy minutes were
nported. A predominance of unstruchind play was documenteci for Categories 5 (12.4 daily
minutes) and 6 (13.1 daily minutes). Values for Categories 7 (4.6 minutes), 8 (0.8 minutes) and 9
(0.07 minutes), however, demonstrated that less time was spent in utlstructured p l q at these
higher intensities.
4.1.7.6. Wallring
The definition used to describe the inteusity levels of Categories 4 and 5 were walking
indoors and waîking outdoors respcctively. Correspondingly, study patients reportcd the majonty
of walking time in these catcgories. Activities in this classification includcd going to lunch,
sociaiizing with fnenâs, wslking the h g , Wring work breaks, and walking 'harâ'. A total of 20.2
daiiy minutes were reportcd for Category 4 and 37.2 minutes for Category 5. Values for
categories 6 (0*6 minutes) and 7 (0.7 minutes) indicated that cMdren spmt minimal time
participating in high intetlgity waiking.

4.1.7.7 Sport
Sport is a structmd, definable activity that cm be p e r f o d at many different intensity
levels. For this study sample, sports were npoited in a l l six categories and there were a wide
range of activity types: mnning, b h g , track and field, trampoline jumping, dancing, fis-
bowiing, fighting, swimming, and lacrosse. For Categories 4 and 5, only 0.27 and 0.87 average
daily minutes were reported, demonsûating that childnn did not rank their sporting activities in a
low intensity category. Categories 6.7, and 8 on the other han& wcre comprised of 27.5,35.9
and 18.4 daily minutes of activity nspectively. By cornparison, the total hours spent in sporiing
activities of higher intensity, category 9 (4.2 minutes) were relatively small. This suggested that
this group of CF chifdren were spending relatively little time in competitive sports compared
with sporiing activities of lower intensity.
4.1.7.8 Undeîined
Some study patients did not complete the Activity Diary according to instructions, and
subsequently, recorded the category intensity of the activity without listing the activity type. So
as not to exclude this data fiom the activity profiles, the total number of hours at the specific
intensity was classifieci in a separate classification, undejlned.

Figure 4.3: Activity Classification (category 4)

Figum 4.4: Activity Classification (categoy 5)

Figure 4.5: Activity Classffication (category 6)


Figun, 4.2 Activity Classification (category 8)


4.2 Comlation Analyses
4.2.1 The BAES and the Adivity DLuy
Pearson's comlation coefficients were calcdated to evaluate the relationship between the
Activity scores of the HAES and the Activity Diary. A separate comlation was conducted
between each Activity score of the HAES and the comparable Activity score of the Activity
Diary. Table 4.8 illustrates the correlation between the Weekday, Weekend, and Weighted Total
and High Activity scores of the HAES and the Activity Diary respectively.
Positive associations were confirmed for each pair of activity scores. A significant
comlation was demonstrated for the Weekday High Activity scons of the HAES and the Diary,
and for the Weekend Total Activity scores. For the Weighted Activity score, significant
comlations were demonstrated between both the Total and High Activity scores of the two
instruments. Although the strength of the comlation coefficients are similar to those reported
between other pairs of self-report instnrment~,~ the relatively moderate values (R < 0.5) imply
that the HAES and the Activity Diary were only captwing some of the same dimensions of
habitua1 physical activity, or suggest the presence of different reporting biases for the two
instruments.
Table 4.8: Comlation between the Total and High Activity scons of the HAES and the Activity Diary (n = 32)
Weekday Weekend Weightcd
R P R Q R P
Total Activity .33 .O7 A4 .O1 37 .O4
High Activity Al .O2 -31 .O9 .O9 ,005
4.23 Habituai Paysicaî Activïty
Comlation analyses were conducted for both the HAeS and the Activity Diary to
evaluate the association of each of the Total and High Activity scores (weekday, weekend and
weighted) with M l , 96 of ideal weight, age, gender, cornpliance with physiotherapy, Wmax a
and V%mx. Table 4.9 &tails Weekday Activity, Table 4.10 illustrates Weekend Activity, and
Table 4.1 1 depicts the Weighted Activity score, a combination of weekday and weekend activity.
Table 4.9 demonstrates several important nlationships. Positive, significant cornlation
coefficients were demonstrated for the associations of the Total and High Activity scons of the
HAES with FEVi, 96 of ideal weight, and Wmax. Pattems for the Activity Diary were very
different. A negative, significant relationship was demonstrated between the High Activity score
and age, and a rnarginally significant positive cornlation was seen between Total Activity and
gender, suggesting higher Total Activity for fernales.
As Qcumented in Table 4.10 for weekmd activity, then was less overall correlation of
Activity scores with candidate comlates. A positive, significant relationship was dcmonsmted
between the HAES Total Activity score and FEVI, and between the HAES High Activity score t
and V02max. For the Activity Diary. a negative, significant relationship was demonstrated fot
the Total Activity score with age, suggesting a decnase in Total Activity with age.
The comlation andysis for the Weighted Activity Scores of the Activity Diary and the
HAES are shown in Table 4.1 1. No significant correlations were âemonstrated for the Activity
Diary. For the HAES, however, positive and significant nlationships were demonstrated for the
Total Activity category with FEVI, % of idepl weight, and Wmax. These results are similar to
those seen for the Wœkday Activity scons. Positive and significant nlationships were dm
d e r n o m for the High Activity categocy with FEV,, and %rum.
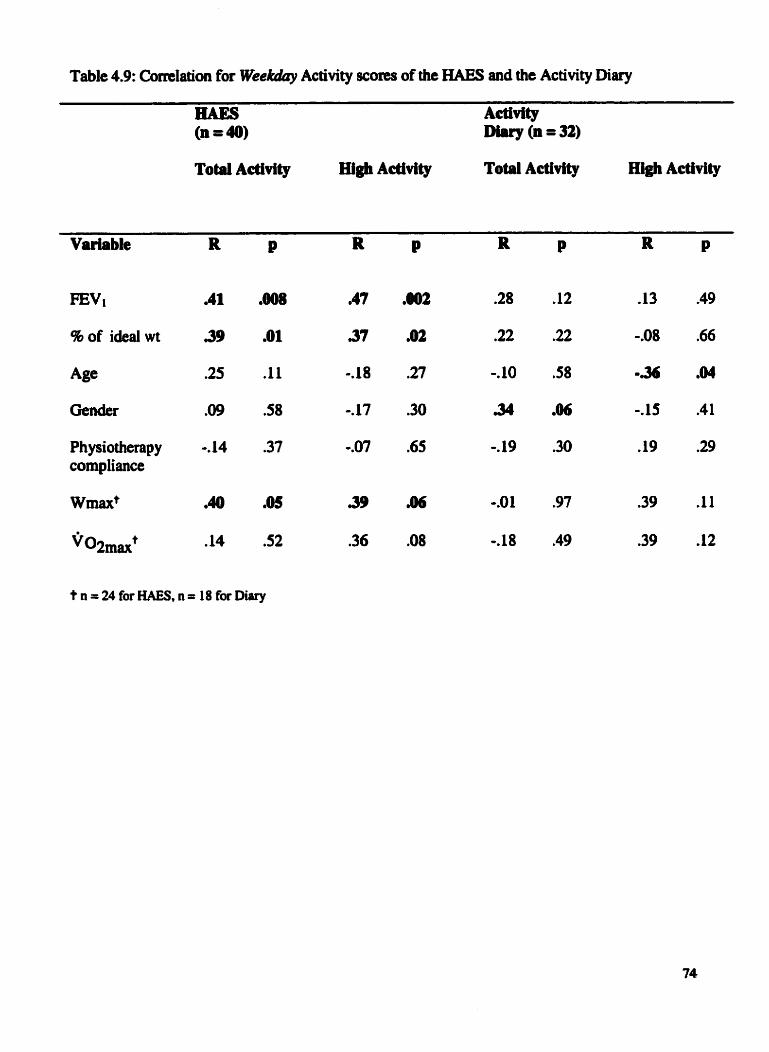
Table 4.9: Correlation for Wee* Activity scores of the HAES and the Activity Diary
Totai Activity High Activity Totai Activity High Activity
Variable R P R P R P R P
Physiotherap y -, 14 .37 -.O7 .65 -. 19 -30 .19 .29 cornpliance
t n = 24 for HAES, n = 18 for Diary

Table 4.10: Correlation for WeeRend Activiîy scores of the HAES and the Actinty Diary
Totai Activity High Aeüvity Totil Advity High Activity
Variable R P R P R P R P
Ph ysiotherap y -.22 .18 0.22 .18 .18 .32 .26 -16 cornpliance
t n = 24 for HAES, n = 18 for Diary

Table 4.1 1: Correlation for Weigkd Activity scores of the HAES and the Activity Diary
BAES Activity (n=40) . Diary (n = 32)
Totai Activity m@ ~ftivitg ToW Actîvity Hi* Activity
Variable R P
mv1 .44 .O05
% of ideal wt 38 .O2
Age -16 .32
Gerider .O9 -58
Ph y siotherap y -. 18 .26 cornpliance
Wmaxt .41 .O5
Y~2maxt .21 .32
t n = 24 for HAES, n = 18 for Diary

4.23 WcdrQy and Weekend Activlty
As presented in Table 4.12, cornlation anaiysis demonstrated positive and significant
comlations between Weekday and Wakend High and Total Activity scores for each of the
HAES and the Activity Diary. These results &monstrateci that children who reported king
physicaliy active during a typical weekday also reported hi@ levels of physical activity for a
typicai weekend day.
Table 4.12: Comlation behveen Weekday and Weekend Activity scons
Totai Activity High Activity
4.2.4 FE&
Table 4.13 demonstrates the comlation analyses for Fmt with 46 of ideal weight. age,
gender, cornpliance with physiotherapy, V b a x and ~ 0 ~ ~ . These analyses were impomt in
beginning to understand the relationships between FEVl and those variables which may be
important in the multiple regression models.
These data indicateâ a significant conelation for FEVi with % of ideal weight and
Wmax. Although there are no other significant comlation coefficients, the direction of the
cornlation coefficient for age is consistent with previous studies that have shown FEV1 to
decluie with age?*

Table 4.13: Comlation Aiialysis for FEVl (n 340)
4.2.5 Potentid Cornlates of Phpical Activity farticipation
The degree of association between each of the Activity Scons and the potential correlates
of physical activity participation was evaluated by means of a cornlation coefficient. The nsults
are demonstrated in Table 4.14. The HAES Activity Scores demonstrated the strongest, positive
relationships with two variables: parent's physical activity level and orgmized physicd uctivity
involvement. The Weekda y, Weekend, and Weighted Total Ac tivity scores demonstrated
significant relationships with parent's physical rtivity level. The Weekend Total, Weekend
High and Weighted High Activity scores demonstrated significant associations with organized
physical activity. The Weekday and Weighted Total Activity scons of the HAES also showed a
si gni ficant nlationshi p with accessibility &xercise-related facitities. For the Activi ty Diary, on
the other han& there was only one positive. significant comlation: the Weighted Total Activity
score with organized physical activity. The nsults suggested a positive nlationship of parent's
physical activity level, involvement in organizcd physical activity, and accessibility of exercist
relateci faciiities with habituai physical activity.

Table 4.14: Correlation bctwecn Activity sams and potentid correlates of physicai activity participation
WeekendT .43 ,007
H -10 .5s
Activity (n=32)
WeekendT .O2 -91
Wetkend H .O9 .61

4.2.6 A Siimmsrg of Resuîts h m Correlation Analyses
The correlation analyses were performed to probe the strength and direction of the
nlationships behveen the Activity scores of the Activity Diary and the HAES, and between the
Activity scons and the other study variables, most importantly FWI. The intent of this process
was to decide which Activity Scores were of most interest for further inclusion in multiple
regression analysis.
Positive and significant associations were demonstraad between the HAES Activity
scores and FEVi. The Weekday High Activity score demonstrated the strongest, significant
comlation with FEVl, followed by the Weighted Total Actinty score, the Weekday Total
Activity score, the Weighted High Activity score, and finali y, the Weekend Total Activity score.
Only the Weekend High Activity score was not strongl y correlated with FEVl. Scatter plots
demonstrated that these correlations were not artifactual; then were no outlying variables that
greatiy enhanced or obscured an o v e d pattern. Results h m comlation analysis between the
Activity Diary Activity scores and FEVI, b y cornparison, àemonsaatcd weak associations.
Although further analysis of the Activity Diary scores took place, mon emphasis was placed on
the inclusion of the HAES Activity scores in multiple regression models, specifically those
scores that àemonstrated the highest correlation coefficients with FEVi.
In determinhg which other study variables couid be of importance in multiple regession.
the comlation coefficients and pvaiues ftom Table 4.13 (Correlation Analysis for FEV1) were
assessed. Pacmt of i&al weight demonstrateci the shwigest correlation with FEVl, foilowed by
Wmax and y. Percent of ideai weight and age were expected to be important in m e r
modeling of Fm in this study. Duc to the small sample of patients with &a on exercise
ca@t~ (n = 24). Wmax w a e not condaed for incIusion in hrther anaiyses.

Their potnuial importance in a friture study of habituai physical activity with a larger sample,
however, shouid not discounteci. Signincant, positive correlations were also demonstrated for
these exercise parameters with the HAES Activity scores.
Two of the study variables that were included in Pearson's correlation analysis, gen&r
and compliance with physiotherapy, were not continuous. For gender, a binary variable. pvalues
for the test of no comlation between gender and masures of FEV, or activity reflected identicai
p-values for t-tests of no difference in mean values khueen males and females. The ordinal
compüance score was developed in an attempt to quanti@ an underlying continuous
measunment of physiotherapy compliance, and was therefore treated as a continuous variable
for this study. Whether or not this score does in fact represent an underlying linear variable will
be explond in hi- long-term study of a larger sample.
Although the Pearson's comlation coefficient may not be a valid estimate of the true
population comlation coefficient for non-normal variables, R is still appropriate for the test of
the nul1 hypothesis of no comlation, provided that one of the variables is normal? The literature
further suggests that a Pearson's comlation coefficient is appropriate for a categorical variable
that is assigneci meaningfd numericd values?
Although the conelation of FEVl with geader and compüance with physiotherapy was
c ' neither stmng nor statisticaily signifiant, both variables were ntained for regression analysis
due to an established rclationship betwœn age and FEV1. and because of the potential
importance of compliance with physiotherapy to both FEVl and habituai physical activity.
4.3 m s s i o n A n d m
Although complete a was avaiiabie for 18 of the 40 study patients, regression anaiyses
wen not conducted on this d sample of the total study population. Analyses werc conducted

on eitha the total numbcr of study patients (n = 40). or on the sample thaî completed the Activïty
Diaries (n = 32).
4.3.1 Multiple Correlation
Multiple comIation analysa w a e conducted by means of the al1 possible remsion
subsets technique. In separate analyses. eitha PEVl or one of the Activity scores was considmd
as the outcome variable. The other variable (FEVl or one of the Activity scores) was then
included as an explanatory variable in addition to age, gender, cornpliance with physiotherapy
and % of i&ai weight The two best models for each Activity score were chosen and have been
presented in Tables 4.15 and 4.16. Tk best models were chosen with consideration to both the
adjusted R-square value and the Cp Mallow statistic.
The R-square is the fraction of the variance in the dependent variable that the regmision
mode1 explains. It dways inmases as more variables are added to the ngnssion equation, even
if these new variables have very Little preâictive value. The adjusted R-square (R2adj), on the
other han& makes you pay a penalty for using additional degnes of fnedorn?' Thmfore, the
adjusted R-square allowed for a cornparison of models with difierent numbers of parameters in
this analysis. The best regression models were g e n e d y considend to be those with the largest
adjusted R - ~ q ~ a r r .
Although the sdjusted R-square was the primary criterion in chaosing the k s t models,
the Cp Mdow statistic was also used to screen for the best regrtssion models. The vdue for Cp
had to be within an acceptable range, near to p @ = the # of parameters = # of preâictor
variables + inteme~t)?~ Thacforc, a combination of fwtors was considercd in selccting the best
and m a t parsimonious models for nnal regrwsioa anrlysis.

Table 4.15 demonstrates the inter-relationships between the Activity scores and the
explanatory variables that best accounted for the variabïiity in these scores. For the HAES
Activity scores, the best individual predictors of these scores were FEVl, followed by percent of
ideal weight. For the Activity Diary Activity scons. on the other hand, either age or gender was
the best individual predictor variable, followed by compiiance with physiotherapy. The highest
adjusted R-squares were demonstrated for the HAES Activity scores. The explanatory variables
accounted for less variability in the Activity Diary Activity scores, suggesting that other
unknown variables were contributing to the variability seen for these scores. This effect was not
due to the reduced sample size (n=32) because when analysis was conducted for this smaller
subset, the R-square values were very similar. The stmngest relationships were demonstrated for
the HAES Weekâay Totai Activity score with age and FEVl (R2adj = 0.27) and for the HAES
Weighted Total Activity score with age and FEV ad adj = 0.23).
Table 4.16 contains the results for multiple comlation analyses where FEVi was the
outcome variable. The results are listed according to the Activity score that was included in the
list of potential predicton. With inclusion of a HAES Activity score as a potential explanatory
variable, percent of ideal weight was the ks t individual predictor of FEV,, followed by the
HAES Activity score. When an Activity Diary score was included as the activity variable,
percent of ideai weight was again the single ks t individual predictor of FEVl, foilowed by either
the Activity Diary scom or cornpliance with physiotherapy. The two best models containeci one
of two HAES Activity scores as a candidate pndictor: the Weekday Totai Activity score. or the
Weighted Totai Activity score. The multiple correlation of Weekday Total Activity, age, and
percent of ideal weight with FEVi pioduccd an adjustcd R-square of 0.41. The comlation of the
Weightad Total Activity score, age and percent of ideal weight with FEVi produccd an adjusted
R-square of 0.40. A separate analysis conducted in the subset of patients who completed the
Activity Diiuy (n =32) also iadicated that the inclusion of these two HAES Activity scores in
separate comlation analyses accounted for the most variability in ml. These analyses
demonstrateci that these two HAES Activity scores ahould be included as potentiai explanatory
variables in fiuther multiple repssion analyses on FEVI.
4.3.1.1 Summ~ry of Muiüple C o r d t b n
n i e primary intent of this multiple comlation malysis was to examine the potential
predictors of FEVi in this study sample. Specificaily, it was important to evaiuate which Activity
scores explained the most variability in mi, the most important variable in desmibing lung
disease in CF. FEVi has already been indicated as the best predictor of survival in CF
and is the primary outcome variable of interest in many CF clinical studies.
Multiple comlation anaiysea were conducted with either one of the Activity scores or
with FEVl as the outcome variable. The results h m these separate analyses confiied a sirnilar
pattern: a positive relationship was demonstrateci between FEVl and the Activity scons, and this
relationship was strongest for the HAES Activity scores. Specificaily. two HAES Activity scores
were demonstnrted to explain the most variability in W1. Candidate explanatory variables also
explained the most variability in these same two HAES Activity scons.
When FEVl was the outcorne variable, the adjusteci R-square values for the best multiple
variable models were higher than the adjusted R-square values for the k s t models whm the
Activity scores wem the outcome variable. #en the HAES Activity scores w a e the outcome
variable, the adjusted Rsquan values ranged h m 0.1 1 to 0.27, meaning that 11% to 27% of the
variabiiity in these HAES Activity scores were explained by the candiAatc explanatory variables.
Whm the Activity Diary scores w m entend as the outcome variable, 5% to 17% of the

variabüity in these scons was explained by the explanatory variables. Pinaliy, w h m FEVl was
entered as the outcome variable, 33% to 4196 of the variabiîity was explainai by the set of
explanatory variables that iacluded the HAES Activity scons, whereas 24% to 27% of the
variability was explained by the set of explanatory variables that included the Activity Diary
scores.
These ~ u l t s confirrned the importance of FEVi as the primary outcome variable for
M e r multiple ngression analysis, and clarified the significant role of the HAES Activity
scores, as compared with the Activity Diary scons, as the candidate explanatory variables to
represent habituai physical activity. In particular, two RAES Activity scores wen indicated for
inclusion as explanatory variables in the final ngression models (Weekday Total and Weighted
Total Activity). In addition to these two Activity scores, age and % of ideal weight were also
indicated as potential explanatory variables based on their consistent pnsence as expianatory
variables of FEVl in multiple comlation. Plots of FEVl by age, percent of ideal weight,
Weekday Total Activity and Weighted Total Activity have been included in Figures 4.9-4.12 to
illustrate the nlationships ktween these variables.
Gender is an important variable in pndicting prognosis of CF patients, and is therefore an
important variable to include in any suMval model. For this analysis, however, genàer did not
enter into any of the best models where FEVi was the outcome variable, even though it did
consistently tum up in the modcls where the Activity scons were the outcome variable. When
both the Activity score and gen&r wcre e n t d as cuididpte explanatory variables, the Activity
score was always selected as the more important explanatory variable. This suggcsted that both
veriabks were explainhg simüar variability in FEVt. Widiin the nauow age nnp of this study
sample, gender did not have any important pradictive vdue in the model. This may nflect the

gender effect being to some extent explaincd by the Activity scores. These nsults do not
undermine the importance of gender in predicting CF survival. Nonetheless, gender was not
includeâ as a candidate predictor variable in final ngnssion analysis, which focused on the
parameters for predicting FEVi.

Table 4.15: Multiple comIation for the Activity scons
Activity Seare ss Best Modeis the Outcorne
WDTHAES Age. ML 0.27 1.9 Age, Gender, FEVl 0 2 7 2.8
WDHHAES FINl, 96 ideal wt Age, FEV1, 96 ideai wt
WTHHAES Genâer, FEVl 0,15 2,4 Age, Genâer, mi, Compiiance 0.14 4.8
WDTAD Gender, FEVl Genâer, FEVl, 96 i&al wt
WETHAES mi
FEVI, Compliance
WDHAD Age Age, Gender
WTT AD Age, Gender Age, Genâer, 96 ideal wt
WEHHAES Age, Gender, Cornpliance 0.10 2.3 Age, Gender, ml, Compüance 0.08 4.0
WTHAD Age. Gender Age. Gender, Compüance
WEHAD FEVl, Cornpliance Gcnder, FEVl, Compiiance
AD, Activity Diary; cornplionce, complianee with physiotberrpy; wt, weight; WDH, Wdcday High; WDT,
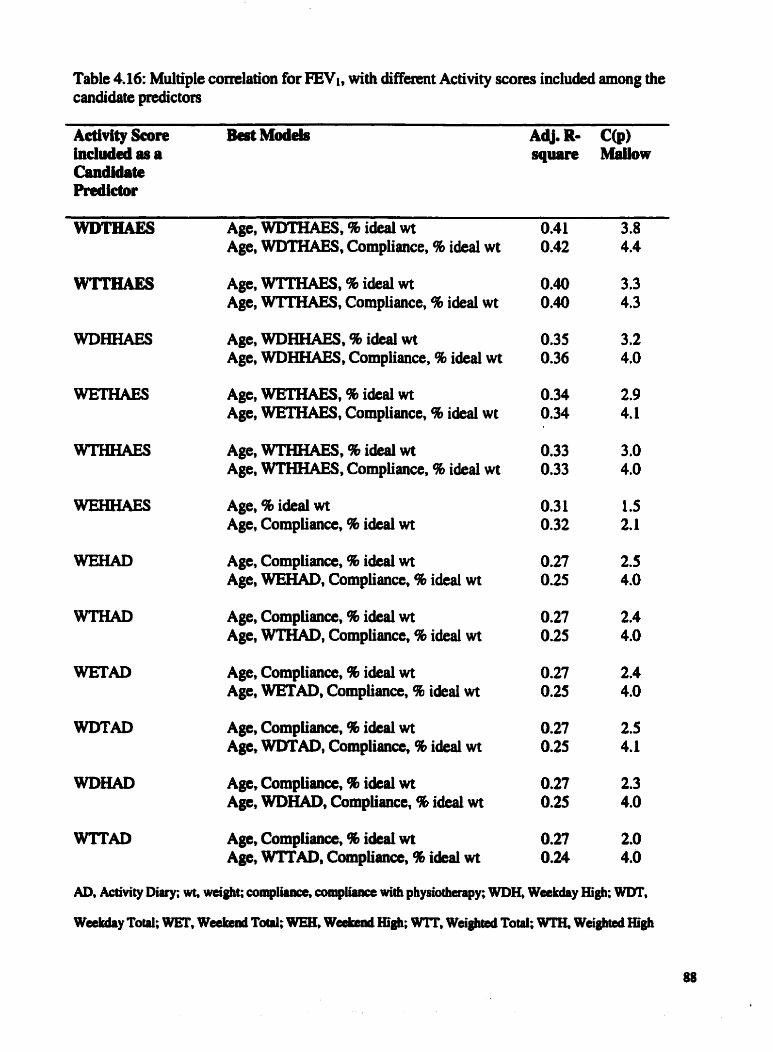
Table 4.16: Multiple comlation for ml, with diffemt Activity scores included among the candidate predictols
A~tivity Seor~ Bcet Md& AdJ. R- C@) included as a square Mlailow Candidate Predic tor
wDmAES Age, WDTHAES, 9b ideal wt 3.8 ~ g e , WDTHAES, Compliance, % ideal wt
Age, WTIKAES, % ideal wt Age, WTTHAES, Compliance, % ideal wt
Age, WDHHAES, % i&al wt Age, WDHHAES, Compliance, % ideai wt
Age, WETHAES, 9b ideai wt Age, W ' , Compüance, % ideal wt
Age, WTHHAES, % ideal wt Age, WTHHAES, Compliance, % i&d wt
Age, % ideal wt Age, Compliance, 96 ideal wt
Age, Compliance, % ideai wt Age, WEHAD, Compliance, 9b ideal wt
Age, Compüance, % ideai wt Age, WTHAD, Cornpliance, % ideal wt
Age, Cornpliance, 96 ideal wt Age, WETAD, Compliance, 46 ideai wt
Age, Cornpliance, % i&d wt Age, WDT'AD, Cornpliatm, % ideal wt
Age, Compüance, % idcai wt Age, WDHAD, Compii~na, 9b ideal wt
Age, Compi.îance, 9b ideai wt Age, WITAD, Compiianœ, 96 ideal wt
AD, Activity Diary; wt, weight; cornpliince, compiinnct with physiotherapy; WDIE, Weekday High; WDT,
Wakday Total; WET, Weekend T e WEK Wabend HÏgh; WTT, Weighted Totai; WTH, Weighted High

\
Figure 4.9: Pbt of FEVf by Age



\
Figure 4.12: Plot of FEVl by HAES Wdghbed Tiptel AdMLy

Multiple linear regression was pafonned to determine the nature of the individual and
combined effects of t h . explanatory variables on PEVi. The explanatory variables were: i) age.
ü) percent of ideal weight. and iii) either the HAES Weekday Total Activity score or the HAES
Weighted Total Activity score. As there were two Activity scons to consider, the same steps
were followed to include each of these scons into the different potential madels.
Aithough both FEVl and the Activity scores were outcome variables in the al l possible
regcession analysis, only FEVl was an outcome variable in the final multiple ngnssion because
the.primary nlationship of interest was the explanation of variability in FEVl by habitua1
physical activity. In addition. only the HAESActivity score was used as an explanatory variable
for activity in the final multiple regression andysis because the Activity Diary Activi~ scores
demonstrated lirnited association with FEVl in both Pearson's correlation and al1 possible
regression.
Every possible combination of variables was examined. For each model, the regression
coefficients and theu standard emrs were evaluated to detemine the relative influence of each
variable on The regression coefficient signifies the amount of change in the outcome
variable per one unit change in the explanatory variable, while controlling for al1 other variables
in the model. If the ngression coefficient was large relative to its standard emr, then that
variable was considend to be a sipificant pndictor of FE&. If the value of the regression
coefficient nmained stable with ctdditional vuiabies in the model, then the vaiable was b m e d
an independent prcdictor. If the tegression coefficient did not remain stable wiüi the addition of
more variables, then confounding of the varirrble's effit was indicatcd. The results an pnseated
in Table 4.17. .

43.2.1 Age
The negative association between age and FEVl bas been previously established,** and is
M e r confirmed by results h m simple comlation between these two variables (R= -0.26,
pcO. 11). Aithough not statistically sigdficant, the negative sign of the correlation coefficient
suggested that FEVi decreaseg with age. From multiple comlation, we see that age is the ihird
best individual predictor of the varhibility in FEVi, following behind percent of ideal weight and
the HAES Activity score. When age was entend into a model as the oaly predictor variable of
FE&, 4.0% of the variability in PEVl was explaineci, as indicated by the adjusteci R-square
value. The regression coefficient demonstrated that for a one-year increase in age, FEVl would
demase by 1.63% predicted. This npss ion coefficient, however, was not significant (p=0.11).
4.3.2.2 Percent of Ideai Weight
In addition to FWi, nutritional status is also an indicator of disease severity in CF. From
simple comlation, we see a comlation coefficient of 0.47 (p=û.O2) between FEVl and percent
of ideal weight. demonstrating a positive and significant nlationship between these variables.
From the nsults of multiple comlation. percent of ideal weight was consistently the single best
individual predictor of FEVI.
With percent of ideal weight entaed individuaiiy into a model of FINl, the adjwted R-
square was much higher than the value seai when age was mtered singly into a model. However,
this was expccteâ because a significant nlationship was demonstrated between FEVi and percent
of ideal weight in simple comlation, but not betwem FEVL and age. The adjutcd R-square
indicated that 20.0% of the variability in FEVi was explpiaed by percent of ideal weight for this
study population. The regrasion coefficient, for which the pvalue was sippincmt @ = 0.002).

indicated that for an increase of 1% in p e n t of ideai weight. there was en incnase of 1.05 %
predicted in FEVi.
43.2.3 HAES Activity Seores
Although a causal nlationship between FEVl and habitua1 physicd activity has not been
estabLished this snidy hypothesized that a positive nlationship would be demonstrateci between
these two variables. Results h m comlation analyses (simple and multiple) indicated that the
HAES Activity scores, as compareci with the Activity Diary Activity scores, had the strongest
comlation with FEVl and thus explaineci more variability in FEVl than the Activity Diary
scores. Fmm the six possible HAES Activity scores, two were selected from multiple comlation
analyses as the best potential preàictors of FEVl: Weekday Total Activity and Weighted Total
Activity. These scores were factored into separate regression models.
By itself, the Weighted Activity score explained more of the variability in FEVl (17.0%)
than did the Weekday Activity score (15.0%). The regmision coefficients for the Weekday and
Weighted Activity scores indicated that for a one-howlday increase in Total Activity, FEVl
would increase by 3.1% predicted (p = 0.008) and 3.5% predicted (pc0.05) respectively.
43.2.4 Multiple Variable Moàeis
A second and third variable wu, added to each of the models containing only one
explanatory variable, and the effects on the adjusted R-square. the regnssion coefficients and the
standard emrs were evaluated,
As a single prodictor of FEVi, age was not significant. Whm entaed into a mode1 with
the Activity score or with percent of iâed weight, however, age became a significant predictor of
FEVIS in this two vari-able modeI, the effcçts of both explmatory variables (age + % ideal
weight, or ags + Activity score) on wcrc augmentcd For exampIe, the effect of percent of

ideal weight on PEVl was enhancecl when age differences were explaineà. While the estimates
of standard emr remained relatively stable, the parameter estimates increased. Consequently, the
significance of these variables as predictors of FEVl incteased, and confounding was indicated
Confounding is an association between two variables that is caused by a third variable (the
confounâer), which is conrlated with the f h t two va~iables?~ This enhancement effect
demonstrated the need to consider controlling for age, for exarnple stratifjing by age group, in a
similar analysis of a larger sample size.
When percent of ideal weight and the Activity score were entered into the same two
variable model, the effects of both variables were reduced which also indicated confounding,
This was not surprising kcause then was a moderate, yet significant comlation of the Activity
score with percent of iàeai weight. Therefore, these two variables were explaining sorne of the
same variability in ml. While the standard error estimates remaimd stable, the parameter
estimates and the significance of these variables also decrraseâ.
The best model incluâed al1 thne explanatory variables, age, the HAES Activity score
(Weekday Total or Weighted Total), and percent of ideal weight. With the Weighted Activity
score in the three vanable model, the adjusted R-square indicateâ that 40.0 % of the variability in
FEVl was explained by the combined effects of age, percent of i&ai weight, and the Weighted
Activity score. This was an increase of 9.0% h m the best two variable model, which included
age and percent of ideal weight. nie three variable madel that included the Weekday Activity
score demonstrated an adjusted R-square of 41.046, which was an incnase of 10.0% over the
best two variable mode1 (age and pcrccnt of i&d weight).
While Table 4.17 iUustrPt#, the totai vuiability explaineci by the best multiple variable
model @ment of ided weight, agc, and Weekday Totai Activity scon), the contribution of cach
predictor variable to the total variability explained was examineci by means of partial comlation.
In this diree variable model, percent of ideal weight, age and Weekday Total Activity
respectively explained 20.096, 11.0% and 10.0% of the variability in FEVI.
Although gender did not contribute to any muitivariable models. the possibility of gender
intexaction was considmd Age and gendet were combined wïth each of the HAES Activity
scores to form interaction terms. These terms were entered into different rnodels with the other
explanatory variables. including gender. The interaction tem. however, were not statisticdy
significant, and did not effect change to the adjustecl R-square value. A larger sample size may
be necessary to detect a significant interaction between these variables.
4.3.2.5 S u a m t q of Finai Multiple Regmaion
The final mode1 was chosen b d on the principles of parsimony and common sense.
The thne variable mode1 explained enough additional variability in m l , as compared with the
best two variable model. to justify inclusion of a t h i d variable. the HAES Activity score. The
relationship between FEVI and each of the thne explanatory variables dso makes biologicai
sense, as h a ôeen previously discussed.
These results h m multiple regnssion indicated a negative relationship between age and
FEVl in this study s~mple, and a positive relationship for both percent of idcal weight and the
HAES Activity scores with FEVi. The choice of the HAES Activity score (Weekday Total or
Weighted Total) did not affect the amount of variability explained in FEVl by the three variable
model. The thrce explanatory variables wen statistically significant predictors of FEVt in the
final model. These muits indicated thaî eitha of these two HAES Acaivity scores should be
considaed for inclusion in a modcl to explain vaziabiiity in FEVi in CF patients.

Table 4.17: Modeling PEVl a, the outcome variable
Mode1 Au. hterœpt hameter Stsadud p-value R2 Estirnate Error
One Varidle:
AGE 0.04
96 IDEAL WT 0.20
wwmAEs O* 15
W'ITHAES 0-17
Two Variables,.
AGE + % IDEAL WT 0.3 1 Age % Ideal Wt
96 IDEAL WT + WDTaAES 0.24 96 Ideal Wt WDTHAES
%IDMLWT+WTTHAES 0.26 96 Ideal wt WTTHAES
AGE + WDTEiAES 0.27 Age WDTHAES
AGE + WTTHAES 0.27 Age WlTHAES
Three Variables:
AGE + 9b IDEAL WT + WDTEAES 0.41 Age % Ideal Wt WlYImEs
Am+% Ideal Wt+WTTBAES 0.40 Age % Ideal Wt wTmAEs
WDTHAES, HAES Wcekday Total Acîivity score; WTTHAES, HAES Weightcd Tocal Activity soore; wt, weight

CHAPTER 5
DISCUSSION
5.1 Interpretation of the Resuits
Results from this cross-sectional pilot study codirmed the hypothesis that a positive
relationship would be demonsrnited between FEVi. habitual physical activity scores. percent of
ideal weight, and exercise capacity. In addition, ngression analyses demonstrated that the two
best Activity scores in pndicting FEVl were the HAES Weekday Total and HAES Weighted
Total Activity scores. A combination of either of these scores with two other explanatory
variables, age and percent of ideal weight, explained approximately 40% of the variability in
FEVl, the most important variable in âescribing CF lung disease. These positive results, in
addition to the physiological and psychological benefits that CF childrni may &rive M m
ngular physical activity, confirm the need for continued nsearch to investigate the causal
nlationship between habitual physical activity and lung hction.
5.1.1 Feasibuity
A primary objective of this study was to determine the ncnritment and compliance rates
for the collection of habituai physicai activity data using the HAES and the 7-Day Activity
Diary. The non-invasive and relatively short nature of this study k l y contnbuted to the high
recruitxncnt rate (89%) demonstratecl for this CF cünic population. Separate compliance rates for
the HAES (100%) and the Activity Diary (82%) dtmonstrated that most patients were retuming
the instruments, and f011owing study protoc01 with rcgarûs to their accmte cornpkioa.
The compliance rate with the HAES was bigbct than with the Diary, WIsly as a n u i t of
the telitive case of adminisartioa for the HAES. The EUES was completcd in approximately 15
minutes by ma t patients in cünic, whaeas completion of the Diary requhd IS to 20 minutes

each day over a consecutive period of seven days. These ciifferences, demonstrateci in this pilot
sample, suggest that the Diary would best serve specifically as a study tool to colIect data on the
rypc of activity being performed, information that cannot be captureci b y the HAES. The HAES,
as has been pnviously s ~ ~ ~ e s t e d , ~ ~ c o u l d more easily be integcated into routine chic follow-up.
In addition. the HAES is sensitive to detect change in actinty patterns in populations?8 and
therefore is suited to longitudinal usage intended to chart activity pattems.
5.1.2 Habituai Physid Activity
5.1.2.1 Trends for the HAES and the AcLlvity Diary
A cornparison of Activity scores between this study sample, the healthy population and
other groups of CF patients is advantageow in evaluating whether the habitual physical activity
pattems of the study patients represented expected levels. Direct cornparisons of Activity scores
can be made between the cumnt study and those investigations that also utiiized the HAES and
the Activity Diary in their study population. For investigations that have uscd altemate self-
report methods to collect physical activity data, general trends in the data can k compared,
including male versus female and weekday vereus weekend activity patterns.
The Total Activity scores for the curent study were consistentiy lower than those
reported for other study populations. In a similady aged group of 36 CF children? patients uscd
the HAES to report their perceived average of wual weekday and weekend day activity. Males
reported 8.1 hours/day and females reportcd 7.5 houfflday. The cumnt study population ais0
fcported lower Total Activity scores thm those documenteci for a group of healthy children
(Maies, 9.1 î 0.4 hours; Fernales, 8.9 f 0.4 hours),1° implying that the CF patients of the currcnt
study may have bem Iess physically active than thcir healthy pe9s. Anotha study of habituai
physical activity in CF sccm to support this suggestion. CF patients npo~W fewer hours

engaged in vigorous physical activity c o m p ~ with a healthy control group?' The h o u
engaged in Total Activiîy, however, did not differ ktwcen groups.
The iiterature suggests that healthy maies participate more frrquently in vigonwls
activities than females.16 Although not statisticaüy significant, maies in the cumnt study
population consistently reported more t h e in High Activity than fernales, confirming the trend
suggested by the literature. In a study of heaithy youth,n moderate to vigorous activity (High
Activity) was assessed by means of the 3-day Activity Diary. Pattems in the data reveal that
males reported consistently higher values for High Activity cornparrd with femaies.
III contrast with High Activity scores, Total Activity scores wen consistently higher in
fernales compared with males for the current investigation. These results suggested that femaie
patients spent more time in mild to moderate ph ysical activities. Two other studies involving CF
patients42 and healthy individu al^^^ nspcctively repurted the opposite trend: higher Total
Activity for males versus femaies. This indicates the need for further investigation of trends in
physical activity participation for males and femaies in a larger sample of CF patients.
The pilot study nsults confimed the importance ofcollecting weekday and weekend day
activity separately. For ail Activity scores. the reports of weekend day activity were significantly
larger than reports for weekday activity. In general, the evidence is equivocai as to whether
children an typicaily more active on a weekday or a weekend The literanue does,
however. agne that diffemces l k l y eexist. Che study suggested chat children may be more
active on the weekend due to the seâentary nature of school. Use of the 3day Activity Diary in
heaithy stuây p ~ ~ u l a t i o n s ~ ~ ~ ~ has e n s d coUcction of habituai physical activity data for both
weekday and weekaid days, confîtming the need to mapure thcse activity intervals sepoiratcly.

Positive, significant correlation coefficients were dernonstrattd between weekday and
weekend Total and High Activity scores for the HAES and the Diary. These results suggested
that children exhibit consistent pattems of physical ectivity participation throughout the week
These trends may nsult h m infîuences in the home environment, such as parental
encouragement of physical activity, or may be related to extemal environmental cues, such as
accessibility of exercise-related facilities.
This study supportcd some of the trends in physical activity participation previously
documented in the literature. Recautions must be taken, however, in àrawing conclusions From a
small sample of patients. Differences in Activity scores between males and females. for example.
were not statistically signifcant. and a larger sample is needed to assess the tnic effects of
gender on habituai physical activity participation. The higher values for Total Activity in females
versus males have not been nported elsewhere. and may reflect a nonnpresentative sample of
study patients. Altematively, these differences could be attributed to unique activity behaviors in
this CF population. Research is still needed to m e r understand and profile the activity patterns
of male and female CF patients in a larger sample.
5.132 Cornparison of the HAES and the Activity Diary
A correlation coefficient was cdculated between the HAES and the Activity Diary in this
pilot study to evaluate the constnict validity of the instniments. Constnict validity can be
confirmeci if a hypothesizcü association ktween the survey measure and a measun of the same
concept actualiy exists? The stmigth of the positive correlation between the HAES and the
Diary was only moderate. In Ilddition. mdy patients nported signifîcantfy more t h e for the
High and Total Activity scores as reportcd with the HAES comparai with the Diary. This
suggested some Merences ktwccn the two instruments.

Other snidies have investigateâ the association between M i n t seKreport measuns of
activity. A comparison study of four habituai physical activity in fernales
âemonstrated agreement between these instruments ranging h m r = 0.17 to d . 4 0 . A second
study demonstrated comlation coefficients behvan survey instruments ranging h m d . 2 2 to
d.39. These comlations are similar to the range of moderate conelation coefficients
documentecl for the comparison of the HAES and the Diary (range h m r = 031 for Weekend
High Activity to r = 0.49 for Weighted High Activity).
The results h m correlation analysis between the Activity Diary and the HAES are
similar to those of other studies. However, the moderate smngth of the correlations suggests that
there may have been na1 differences between the report of sctivity using the Activity Diary and
the mal1 of activity for HAES completion. Recall limitations, ramiom error, or ümitations due to
proxy nsponse may have affected the vaiidity and reliability of the results? Further
investigation in a larger sample is warranted to determine whether real differences exist between
the Activity Diary and the HAES.
5.1.3 Exerciae Capacity
A positive. significant comlation was dmionstrated for the HAES Activity scores with
maximal work capacity and maillmel oxygen consumption. Two other studies have demonstrated
similar resuits in healthy ~hildrcn.%~ although the HAES was not used to quantify habitua1
physical activity. The rclationship betwem physical actinty Ievel and e x d s e capacity is still
equivocal. In a 3-year exercise intervention trial in CF patients? a minimum of thne weekly
m b i c sessions was enough to e f f i t change in pulmonary hction. however, insuffident to
effect any change in wercise capacity. A training efféct may not have been demonstrateci
because of the patients rclatively high fitncss levels at baseline. Establishing thresholds of

physical activity participation for a training effect ha9 many challenges in CF: the start and stop
nature of young children's physical activity patterns. the demanding daily treatment routines of a
CF family, and the potential apathy toward exercising in the adolescent group. These factors
must be considered if fiinirt activity intewtntion studies are to be conducteci.
In m e r investigating the association between physical activity and exercise capacity,
several factors muet be considemi, including the methods useà to evaluate habituai physical
activity patterns and exercise capacity status, and the contribution of gemtic endowment to both
physical activity and physical fitness. In CF, the longitudinal follow-up of exercise capacity and
habitua1 physical activity in a large number of patients will allow for a heightened understanding
of this nlationship.
5.1.4 Cornpliance with Physiotherspr
The compliance with physiotherapy scores did not contribute as pndictors of FEVl in the
current study. Although compliance with physiotherapy was the third best individual predictor of
the Activity Diary scons. it did not contribute to the explanation of variability in multiple
correlation for FEVl. In the CF population, the accuracy of compliance with physiotherapy
scores, and their actuai condation with lung hction status are challenging issues. Patients who
comply with physiotherapy are iikely heaithier than those who do not. Ch the other han& some
patients who fa1 healthy do not comply with their ptescribed physiotherapy because they
personally dam it to k unncccssary. This extreme variaôility in rtual compüance with
physiouiaapy may have rended it unimpomt in this cro~s~sectionai regression analysis.
5.1s Psrwt Q u e s t i o ~
Analysis of data h m the parent questionnaire nvealed sevaal potcntiaily important
relatiowhips for physicat activity participation with acccssibüity of facilitics, partllt's physicai

activity level and organized phyaical activity involvement. The mean score for neighborhood
safety suggested that the majority of parents felt they lived in extmnely spfe neighborhoods. As
then was minimal variability in the scores. thae wen ais0 no important comlatioas with the
Activity scores. In a larger study sample, there may have ken more variability in ihis score. and
therefore a larger effect.
These results suggested associations common to other studies. Childnn of active and less
active parents exhibited similar physical activity patterns as their parents in one such study?' An
examination of the relationship between a mile walwrun test of physical fitness and cornlates of
activity participation demonstrated that involvement in organized physical activity was
correlated with a fitness test?' Physical activity level. however. was not assessed in this
investigation.
Cornmon relationships seen between this study and the literature suggested that physical
activity participation in CF patients rnay be affected by factors common to the healthy
population. The significant relationships for the Activity Diary and the HAES with previously
documented correlates of physical activity participaiion implied M e r relevance for the use of
these two instruments in diis population.
5.1.6 Activity Cladicatioa
The classification system developcd for the activity types listeci by this CF study
population couid eventually allow for cornparisons m s s populations, and could help in the
detennination of which activities may k usehil for effecting change in health siatus in
intavation trials. Tm& in the classilïcation of activity type accordhg to category intensities
h m the Activity Diary suggcsced that the study population was assigning the suitable intensity
to theif activity types. Common sensc suggeated thaî persona1 care activitits, f a example, would

not be listed in caiegorics higher than intensity 4 or 5, the two categories of most miId intensity.
This was the case. Similarly, then were nlatively few activities in the sport classification listed
at lower intaisities, or for the most physically demanding category, indicating that most childrm
reporteci sport participation at a moderate hteasity. These results were also expecteà, as it is
unkly, for example, that many childnn would be involved in cornpetitive sport. The need for
an undefined category. bowevet. suggested that children do nquirc more explicit instructions on
detailing their activity so that they will be more specific in their activity descriptions.
5.1.7 Simple Comiation of Activity Score with FEVi
Trends in the data suggested a stronger association for FEVi with the HAES Activity
scores than with the Activity Diary Activity scores. Som of the potential diffennces between
the instruments that could have contributecl to these discrepmcies have a h d y been suggested.
Then was also stronger comlation between FEVl and the Weekday Activity scores than with
the Weekend Activity scores. These results may have been attributed to more variability in
weekend activity compand with weekday activity. Patterns of habitua1 physicai activity rnay be
more consistent during the school week as school routines are such that most children have an
opportunity to participate in at least some physicai activity. On the weekend, children may range
h m totally inactive to highly active.
Although these results may insinuate that a record of weekend activity is of littie value, it
is stiil important to measun physical activity for both wakdays and weekend âays. In a larger
sample, weeltaid activity may be indicated as important, especialiy if some chilârea perform the
majority of their physicai actinty on Saatrday and Sunday. This amount of physical activity may
be enough to demonstrate a positive und important nlationship with lung function.

For the cumnt study, a positive and significant correlation was demonsaated for the
HAES Activity score with lung hction and nutritional status, suggesting that those with
decreased lung function or inadequate kidyweight are less active. Similarly, in the healthy
population? a significant negative relationship ha9 ken demonstrated between physical activity
level and fatness. This association suggests that childnn who sn nutritionaily sound, neither too
fat nor too thin, are more k l y to be engaged in cegular physical activity. For the CF population
where many patients are nutritionaily compromised, these results suggest the importance of
longitudinal follow-up of this nlationship to determine whether changes in habitual physical
activity are related to change in nutritional status. Oniy pmperly designed intervention saidies
will be able to evaluate whether ppcticipation in habituel physical activity can effect change in
nutritional status.
Only two other studies have examinai the specific nlationship of lung huiction with
habituai physical activity in CF childnn and adolescents. The results from these two studies
diffend h m those of the cumnt investigation. In 36 CF patients:2 a significant relationship
was demonstrated between the Total Activity score of the HAES and nutritionai status in
children with clinicall y significant lung disease. However, thm was no relations hip between
activity level and lung function in these patients. In a study by Nixon et al:' activity level was
unreleted to both exercise tolerance and pulrnonary function in 30 CF patients.
Results of these two studies likely diffed from those of the cumnt study due to the use
of differcnt masurement tools, the cross-sectionai nature of the study designs, varying disease
statw, small numbers of patients, seasonal ciifferences in the periods of activity chta collection,
and differtnt activity intervals measured (wœkdPy versus wœkend). Rather than suggesting a
lack of consistent association betwan important sady vasiables in CF, these dimpant rwuits

further clarify the need for a longitudinal stuây in the CF population with repeated measunment
and follow-up of habitua1 physical activity, lung function, nutritional status, and exercise
capaci ty.
The results h m simple comlation suggested that luag functioa and the HAES Activity
score were nlated in a positive direction. Mthough more research is needed to determine the
direction of causality for these hvo variables, they may act upon one another within a positive
fcedback loop. For enample, relatively stable lung huictioning may promote participation in
ngular physical activity. In turn, physical activity participation may act to M e r maintain or
even improve lung function. Establishing causalit y, however, will nquire long-term follow-up of
CF patients into adulthood, and studies of specific activity interventions to alter physical activity
patterns.
5.18 Regretmion Anaïyses
These results h m multipIe regnssioa indicated a negative relationship between age and
FEVi in this study sample, and a positive nlationship for both percent of ideal weight and the
HAES Activity scores with FEVi. The choice of the HAES Activity score (Weekday Total or
Weighted Total) did not affect the amount of variability cxplained in FEVi by the three variable
model. These reaults indicated that either of these two HAES Activity scores could be considered
for inclusion in a model to explain variability in FEVl in CF patients.
5.2 Methodolonical Issues
5.2.1 swdy Limitriao~ls
This study indicated the importance of continuing to evaluate the nlationship between
habituai physical activity and lung fiinction in CF, such that the direction of cawality betwan
these two variables can be established Rior to fiirthcr investigation, however, it is important to

identiw study limitations, and to provide raommtndation~ for friture resexucb in this area. The
following sections outline some of the challenges and recommendations i n c d in conducting
this pilot study.
5.2.1.1 CompUPirc with, anà Return of, the 7-Day Acüvity D m
Experience h m this pilot study indicated that q p l a r phone contact during the week of
data collection was necessary to ensure pmpet completion and retwn of the Activity Diary. If the
Activity Diary was not retumed by mail, patients were asked to bring in their completed Activity
Diary to their next clinic visit. Clear instructions, detailed examples of a sarnple day, and
encouragement to tül out the Activity Di*ary as close as possible to the tirne of the chic visit
were also important.
Although the relatively high cornpliance rate with the Activity Diary suggested that a 7-
day Diary was a feasible methoci of collecting habituai physical activity data, a 3-day Activity
Diary may ensure even higher compüance. A 3-day ~ i a r ~ ' ~ would include s d f - ~ ~ p o ~ of two
weekdays and one weekend day, and could k especially useful as a study tool in longitudinal
followiip of W patients where more than one completion of the Activity Diary is necessary.
5.2.1.2 Ranàom and Systematic Emr in Sdl-Report of Activity
In any self-report of physical activity, thae is a risk of ranQm or systematic (bias)
emr? Although the assessrnent of habitual physical activity h m the HAES and the Activity
Diary was subject to this risk, specific design feanaes w a e intended to minimize the potential
for these types of mrs.
The potmtiai for ranâom emr dunng self-administration of the sumy instniments was
addressed in this sady. For the Activity Diary, thae was a risk for unintentional emrs during
the recording of activity inteasity. h part to minimizt this risk, subjects wae sslrcd to
specificaiiy describe the activity type next to their entry for activity inteasity. This enabled the
study coordinator to check one entry against the other to ensun that the intensity matched the
type. For the HAES, potential emrs in ncording were immdiately assessed upon the patient's
completion of it. If the assigned percentages for each time p e n d as provided by the patient, did
not add up to 10096, the study coordinator documented this discrepancy, and consuited with the
patient to nctify the inconsistency. If patients perceived dificulties in comctly assigning
percentage values to each activity level, the stuây coordinator completed a sampie entry with
hem, or invoked the assistance of the puent.
Both the Activity Diary and the HAES nquind self-report of activity for al1 levels of
intensity. This was intended to =duce a patient's tendency to over-estimate physical activity
participation or to engage in non-repnsentative activity patterns during the week of recording.
When patients were first introduced to the study pmtocol in clinic, the study coordinator
emphasized the importance of recording USMI activity patterns. Examples of many Merent
types and intensities of daily activities wen pfovided to patients, mging h m sleep and
television viewing to involvement in competitive sport* These guidelines were foiiowed with
each newly recmited patient io demase the chance of obtaining a biased estimate of habinial
physical activity.
5.2.1.3 Generriupbiiity of the Results
Due to the short-tem nature of this study, habituai physical activity was coliected for
only the s p ~ g season (March-June). Research has suggested that there is variation in the
physical activity participation according to the time of yeu. Whüe one study documented a
marked inmase in activity during the s u m m r months,I6 awtber study suggestd a ckciine in
activity kvds dwing the sumrn~r.~~ Therefort, as sctivity patterns poteatiaily vrry by season, the

nsults fiom thie pilot study cannot be generaüzed to otha seasonal periods duriag the year. In
future long-term stuàies. the collection of habituai physical activity data shodd be appmpriately
timd to capture physicai activity data during al1 four semons so that a seasonai effect can be
eshateci.
5.2.1.4 Direction of Causaüty
The mss-sectional design and smail sample size of this study limi ted an y efforts to
evaiuate the direction of causality between habitual physical activity and pulmonary function.
Instead, the presence of a positive, statistical association between Activity scores &rived h m
the HAES and FEVl suggested the need for longitudinal follow-up of habitual physical activity
patterns in CF patients. Routine assessrnent of habitual physical activity, in addition to the
collection of pulmonary huiction. nutritionai status and exercise data already available through
reguiar clinical foiiow-up, would be instrumental in beginning to addrrss the issue of causality.
5.2.2 Suggested Modifications of the Cumnt Rotocol
Results h m the cumnt study an equivocal regardng the use of the 7-Day Activity
Diary in quantifying habituai physical in CF. The Activity Diary did not demonsmte a
significant or smng relationship with the primsry outcome variable. FEVI, and this finding
warrants m e r investigation. The Activity Diary and the HAES may have been capturing
different dimensions of habituai physical activity in the CF patients. Altemately, the iim
consuming nature of accurate completion of the 7&y Activity Diary may mder it impractical
for longitudinal usage. Future reseacch rnay indicate the importance of quantifjing habituai
physical activity by mwis of a single instniment that woulà fimction to collect infomraton on
ail dimensions of activity at one time period This type of instnmient muid potentially combine
featuns fiom both the HAES and ihe Activity Disry.

A s w e y instrument of this design rnay entaiI ha* patients complete the HAES in
clinic, while comspondingly listing the usual activity types. In addition to providing data on
activity type, patients would also be accountable for the percentage estimatar that they ncorded
This option, however. needs M e r consideration with regards to its feasibiiity and accmy.
5.3 Future Directions
53.1 Proposai lor a bngitudinai Study
Survival regression studies in CF have demonstratecl how pulmonary function and
nutritional status affect sumival. It has been pnviously established that FEVi is the best
predictor of s~rvival?~ and consequently, this variable is widely accepted as a surrogate for
mortality risk in CF. Research has examinecl faftors that &termine the severity of lung disease in
order to clarify the survival model: which is essentid for the timing of procedures such as lung
transplant. In addition to FEVi and nuhitional statua, other important predictors of sumival are
age, gender and specific gene mutations.
A masure of habitua1 physical activity may further explain some of the variance in
Wi, and thus enhance the CF survival model. Habituai physical activity, however, has neither
been followed longitudinaliy in the CF population, nor considend for inclusion in the survival
model. Rior to the inception of a longitudinal study, a quantifiable measun of habituai physical
activity that could be incorporated into the clinical follow-up of patients was neeâeà. The cumnt
pilot study was designeci to invcstigate this issue.
This pilot study examincd the fcasibility and cornpliance rates for the collection of
quantifiable data on habituai physical activity. This shidy also explod the â h t i o n and strength
of the relationship betwem Mitual physicai activity and =VI, while taking into collsideration
.otha variables that may influence thïs nlationship. Resdts implied a positive nlationship

between FEVl and habituai physicd activity. On the b&s of these encoumghg nsults, a
longitudinal study has been proposed, and the project protoc01 submitted for fimding in October
1999 to the Canadian Cystic Fibmsis Foundation.
The purpose of the pmposeâ pmject is to estubiish ifhabiturrl pkysical uctivity is a
significmt predictor of the change in m. Patients will be recniited from the CF clinics at two
study centers, HSC and Montreal Children's Hospital, between which there is a long history of
collaboration. The inclusion of two study centers will inmase the sample size and ailow for
smnger conclusions to be Qawn h m the &ta. Data collected over a two-year W o d h m both
the HAES and a 3day Activity Diary wili pennit the creation of a comprehensive profile of
habitua1 physical activity in a large study population. The 3day Diary, a modification of the 7-
day Activity Diary used in the pilot study, has been proposeci to encourage cornpliance over the
two-year study pend. Exercise capacity, nueitional status, and puhonary function data will
also be mutinely collected h m clinic records in keeping with the protocol of the pilot study.
However, this longitudinal study will aliow for more complete collection of data on exercise
capacity, and pmnit the inclusion of this data in regnssion analyses. A power calculation,
conducted for the grant application, has b a n included in Appmdtr G.
The short-term goals of this pmposed project include the integration of the HAES into
regular clinic proceâures for aU CF patients, and inclusion of this measun into the Toronto CF
database. F m the combined mdts of the 3-day Activity Diary and the HAES. a
compnhmsive CF activity profile wili be crcakâ, which wi l l enable bctter understandi11g of
activity behaviors in the C F population. A quantification of activity level wil i aüow us to
evaluate the rclaticmship of pulmonary function with habituai physicd activity, nutritional status
mi exefcisc capacity in a large study population. Capturing activity on a rcguiar bads win d o w

for the assessrnent of the effecis of seasonal variability on activity patterns, and subscquently on
lung huiction.
There are no hown longitudinal sadies that have examincd and monitored habitual
activity patterns and the relationship to diseass progression in CF. This pmposed project will
encourage the foîiow-up of CF activity pattems into aduithood, such that the causal relationship
between activity level and disease progression cm be eddressed. As demonstrateci by the pilot
study, the activity measures employed in Uiis investigation are well suited for clhic use, and the
HAES may allow for longitudinal tracking of activity patterns. Long-term goals include the
development of recommendations for exetcise prescription, and future coilaboration with the
Clinical Studies Netwotk (CSN) to &velop a plan for longitudinal, multi-center intervention
studies throughout Canadian CF clinics. An understanding of the inter-nlationship of pulmonary
function with habitual physical activity level, nutritional status, and exercise capacity, will allow
for improvements to our mode1 of survival in CE
5.4 Conclusions
This pilot study met its primary objectives. The results suggested a positive association of
weekday activity level (HAES) with both nutritional statw and pulmonary function, and
supportecl the hypothesis that CF patients would be receptive to providing data on theu activity
patterns. While this study has begun to demonstrate the practicaiity of using the HAES and the
Activity Diary in CF patients to quantify habituai physicai activity, preliminuy cross-sectional
trends indiate the need for longitudinal followiip.
Exercise training pmgrams are difncult to foster in the CF population wherc &mancihg
trament regimens can consume much of the CF patient's spare time. The promotion of
increcwd habituai physicai activity, howevcr, is hypothaized to effect change in the clinid

status of these patients, and is iikely casier to foster than cornpliance with an exercise training
program. The cuennt study was intendeci to gather supportive evidence necessary to warrant a
longitudinal study of the nlationship berneen FEVl and habitual physical activity. A
longitudinal study, bas& on the nsults of this pilot study, may eventually establish whether
habituai physical activity can help to explain variability in the suniival of CF patients. If the
answer is yes, the importance of encouraging regular ph ysical activi ty participation in CF
patients wili be confirmed.

REFERENCE LIST
Thompson K. Cystic fibrosis-update on exercise. Phys Sports Med 1990; 18:103-106.
Keens TG, Krastius IRB, WannamaLa EM, Levison H, Crozier DN, Bryan C. Ventilatory muscle endurance training in normal subjects and patients with cystic fibrosis. Am Rev Respir Dis 1977; 116:853-860.
Schneideman-Waiker J, Pollock SL, Corey ML, Wiikes DD, Cmny GJ, Pedder L, et al. A mdomized cotrolied trial of a thne year home exercise p m g m in cystic fibrosis. In Press-Jn of Pediatr, 1999.
Jackson ADM, Dodge JA, Cuthbert AW, Van Heyningen V, Porteous DJ. Cystic Fibrosis. Oxford: Oxford University Press, 1989.
Meams M. Cystic Fibrosis: the First 50 Years-A Review of the CLinical Roblems and their Management. In: Dodge JA. Bmck DJH, Widdicombe IH, editors. Cystic Fibrosis-Cumnt Topics. Chichester: John Wiley & Sons, 1993:217-250.
Corey M, Farewell V. Detenninants of mortality h m cystic fibrosis in Canada, 1970- 1989. Am J Epiâemiol 19%; 143:10(n-1017.
Cystic Fibrosis Foundation. Patient registry annuai report 1996.1997; Bethesda, MD.
Kerem B, Rommens J, Buchanan J, Markiewicz D, Cox T, Chakravarti A, et al. Identification of the cystic fibrosis gene: genetic analysis. Science 1989; 245:1073- 1080.
Kerem E, Reisman JJ, Corey ML, Canny GJ, Levison H. Rediction of mortality in patients with cystic fibrosis. N Engl J Med 1992; 326: 1 187-1 191.
Nixon PA, Onnstcin DM, Kelsey SF, Doerschuk CF. The prognostic value of exercise testing in patient with cystic fibrosis. N Engl J Med 1992; 327: 1785-1788.
ûrenstein DM, Henke KG, Cemy FJ. Exmise and cystic fibrosis. The Physician and Sportsrnedicine 1983; 9 (2 Suppl):6-18.
Cystic Fibrosis Team: The Hospital for Sick Childnn. Cystic fibmsis: a teaching manual for parents and patients. 1992; 3rd ed Toronto, ON.
Lai H-C, Cony M, FtzSimmons S, Kosorok MR. Fameil P. Cornparison of growth status of patients with cystic fibmsis betwen the United States and Canada, Am J Clin Nutr 1999; 69:S 1-538,
Sallis J, Patrick K Physical activity guidelines for adolescents: consensus statemtnt. Pecl Ex Sci 1994; 6:3O%3 14,

Sallis J. Epiûemiology of physical ectivity and fitness in childrcn and adolescents. Crit Rev Food Sci Nutr 1993; 33:40348.
Pate RR, Long BJ, Heath O. Descriptive epidemiology of physical activity in adolescents. Ped Ex Sci 1994; 6:434-447.
hutzenhiser JK, Clark R. Physical activity and exercise in children with cystic fihsis. Jomal of Pedatric Nming 1993; 8: 1 12-1 19.
Singsen B. Physical fitness in children with juvenilie cheumatoid arthntis and other chronic pediatnc illnesses. Pediatric Rheumatology 1995; 42:1035-1050.
Boas SR. Exercise ncommendations for individuals with cystic fibmsis. Sports Medicine 1997; 24: 17-37.
Coates AL. Exercise in CF: Does in help? Does it tell us anything? Pediatr Puhonol 1987; 3 Suppl:7 1-72.
Orenstein DM. Exercise testing in cystic fibmsis. Pediatr Pulmonol 1998; 25:223-225.
Pegues DA, Carson LA, Tablan OC, FitzSimrnons S. Roman SB, Miller JM, et al. Acquisition of Pseudomonas cepacia at summer camps for patients with cystic fibrosis. Summer Camp Study Group. J Pediatr 1994; 124:694-702.
Zach M, Oberwaldner B. Hausler F. Cystic fibrosis: physical exercise versus chest physiotherapy. Arch Dis Child 1982; 57:587-589.
Zach MS, Purnr B, Oberwaldner B. Effect of swimming on forced expiration and sputum clearance in cystic fibrosis. Lancet 198 1; 2: 1201- 1203.
Heijerman HG, Bakker W, Sterk PJ, Diflanan H. Oxygen-assisted exercise training in adult cystic fibrosis patients with pulmonary limitation to exercise. Int J Rehab Res 1991; 14: 101-1 15.
Cemy FI. Relative effects of branchial drainage and exercise for in-hospital c a n of patients with cystic fibrosis. PhysicaI Therapy 1989; 69:633639.
Edlund LD, French RW, Herbst JJ, Ruttenbag HD, Ruhling RO, Adams TD. Eff- of a swimming pgcam on children with cystic fibrosis. Sports Medicine 1986; 140:80- 83.
Orenstcin DM. Exercise conditioning and cudiopulmonary fitness in cystic fibmsis: the effects of a 3 month supervisai e d n g program. Chest 1981; 80392.
Stanghelle TI(, Hjeltncs N, Bangmi H. Michalsen EL Effécts of daily short bouts of trampoline wdse àuring 8 w& on the puimonary fiinction and the mPximal oxygen uptake of cbildiai with cystic fibmsis, ht J Sparts hkd 1988; 9 Suppl:32-36.

30. Kaens TG. Ventilatory muscle endurance training in normal subjects and patients with cystic fibmsis. Am Rev Respir Dis 1977; 1 l6:853.
3 1. Braggion C, Coniacchia M, Miano A, Schena F, Verlato G, Masteiia GD Exercise tolerance and effects of training in young patients with cystic fibrosis and mild aiiway obstruction. Pediatr Pulmonol1989; 7: 145-152.
32. Stanghelle JK, Winnem M, Roaldsen K. de Wit S. Notgewitch JH, Nilsen BR. Young patients with cystic fibrosis: attituâe toward phyeicai activity and influence on physical fitness and spimmetric values of a 2-week training course. Int J Spom Med 1988; 9 Suppl:25-3 1.
33. & Jong W, Grevink R, Roda RJ, Kaptein A, van der Schans CP. Enect of a home exercise training program in patients with cystic nbroais. Chest 1994; 105:463-468.
34. O'Neill PA, Dodd MA, Phillips B. Poole J, Webb AK. Regular exercise and reduction of breathiessness in patients with cystic fibmsis. Br J Dis Chest 1987; 8162-69.
35. Ancireasson B. Jonson B. Komfalt R, Nordmark E, Sanâstrom S. Long-term effects of physical exercise on working capacity and pulmonary function in cystic fibrosis. Acta Paediatr Scand 1987; 76:70-75.
36. Blomquist M. Freyschuss U, Wiman CO, Strandvik B. Physical activity and self treatment in cystic fibrosis. Arch Dis Child 1986; 61:362-367.
37. Hoizer FJ, Schnall R, Landau U The effect of a home exercise porgramme in childscn with cystic fibrosis aud asthma. Aust Psediah J 1984; 20:297-302.
38. Salh W. Bilton D, Dodd M, Webb AK. Enect of exercise and physiothecapy in aiding spuaim expectoration in ad& with cystic fibrosis. Thorax 1989; 44:1006-1008.
39. Heijerman HG, B a k r W, Sterk PJ, Dijkman Et lang-term effccts of exercise training and hyperaümentation in adult cystic fibrosis patients with severe pulmonary dysfunction. Int J Rehab Res 1992; 15:252-257.
40. KoIIberg H. Cystic fibmsis and physical activiw an introduction. Int J Sports Med 1988; 9:2-5.
41. Nixon PA, bnstein DM, Keisey SF. Habitua1 physical activity in childrcn and ado1cscents with cystic fibrosis. Peû Ex Sci 1999; 11: 18 1 (Abstract).
42. ouc cher GP, Lands LC, Hay JA, Homby L. Activity Ievels and the relationship to lung function and nutritional status in childrcn wîth cystic fibrosis. Am J Phys Med Rehabil 1997; 7633 1 1-3 15.
43. Marcotte JE, Gfisble R Lenson H, Coaes AL, Canny GJ* Multiple factors M t txcrcise capacity in cystic fi'brosis. Pediatr PiiImonoI 1986; 23274-28 1.

44. Lands LC, Heigenhauser GIP, Jones NL. Analysis of factors limiting maximal exeinse performance in cystic ûbmsis. Clinicd Science 1992; 83:391-397.
45. Marcotte JE, Canny GJ, Grisdale R, DuMond KJ, Corey ML, Zinman R. et al. Effects of nutritional status on exacise performance in advanced cystic fibrosis. Chest 1986; 90:375-379.
46. Hay J. Development of a 24 hour ncall measure. Canadian Association of Sport Sciences Annual Confertnce 199 1.
47. Montoye HJ, Kemper HCG, Saris WHM, Washburn RA. Measuring ph ysical activity and energy expenditure. 1st cd Windsor, ON: Human Kinetics, 19%.
48. Freedson P, Melanson E. Measuring physicd activity. In: Docherty D, editor. Measment in Pediaüic Exercise Science. 1st ed. Victoria, B.C.: Hman Kinetics, 1996:261-283.
49. Bouchard Cl Tremblay A, Leblanc C. Lortie G, Savard R, Thenault G. A method to assess energy expenditun in chilnn and adults. Am J Clin Nutr 1983; 37:461-467.
50. Bratteby L-E. Sandhagen B. Lotborn M, Samuelson O. Daily energy expenditure and physical activity assessed by an activity diary in 374 randomly selectd 15-year-old adolescents. Eur J Clin Nutr 1997; 51:592-600.
51. Bratteby L-E, Sandhagen B. Fan Hs Samuelson O. A 7day activity diary for the assessrnent of daily energy expenditure validateci by the doubly labeiled water methocl in adolescents. Eur I Clin Nutr 1997; 5 1:58S-S9l.
52. Hendemn CJ, Love11 DJ, Specker BL. Campaigne BN. Physical activity in children with juvenille rheumatoid arthritis: quantification and evduation. Arthritis Care and Research 1995; 8: 114-1 19.
53. Eisenmann JC, Katzmarzyk PT, Theriault G, Song TMK, Malina RM, Bouchard C. Physical activity and pulmonary huiction in youth: the Quebec family study. Ped Ex Sci 1999; 11:208-217.
54. Weston AT, Petosa R, Patc RR. Validation of an instrument for rneasurement of physical activity in youth. Med Sci Spom Exerc 1997; 29:138-143.
55. Crocker PRE, Baiky DA. Faulkner RA. Kowallcsi KC, McOrath R. Measuring generai levels of physical activity: pnliminary evidenct for the Physical Activity Qucsti0mai.e for Oldcr Children. Mcd Sci Sports Exerc 1997; 29: 1344-1349.
56. Oodin 0. Shephard RI. A simpIe mcthod to assess exercisc behavior in the community. Can J Appl Sport Sci 198% 10141-146.

Sallis JI& Buono MJ, Roby JI, Micale FG, Nelson JA. Seveaday recall and other physical activity self-teports in childm and adolescents. Msd Sci Sports Exerc 1993; 2S:gg- 108.
Hay JA. Development and testing of the habituai aclinty estimation scde. Proceedings of the XIXth International Symposium of the European Orwp of Pediatnc Work Physiology 1997; 2: 125-129.
Halton JM, Atkinson SA, Hay J, Webber CE. Mntin RF, Barr RD. Ostopenia in children with acute lyrnphoblastic leukernia &hop Tms 1995; 18:684 (Abstract).
Hay J, Shephard RI. Perceptions and patterns of physicd activity: a cornparison of MohawkKayuga and non-native adolescents. American Journal of Human Biology 1998; 10:629-635.
Atkinson SA, Halton J, Hay J, Gordon C, Webber C. Nonnative values for lumbar spine bone mass in children in relation to age, gender, and physical activity. Jn Bone Min Res 1991; 6:S132 (Abstract).
Moelgaard C. Bone mineraiization during growth; the influence of growth, puberty, and calcium intake. 19%; University of Copmhagen. Denmark.
DiLorenzo TM, Stucky-Ropp RC, Vander Wal JS, Ootham W. Detenninants of exescise among chiidren. II. a longitudinal anaysis. Reventive Medicine 1998; 27:470-477.
Sallis JK, Simons-Morton BG, Stone EJ, Corbin CB, Epstein LH, Faucette N, et al. Detemiinants of physical activity and interventions in youdi. Med Sci Sports Exerc 1992; 24:S248-S257.
Sallis JK, Johnson MF, Calfas KJ, Caparosa S, Nichols JF. Assessing perceived physical environmental variables that may influence physical activity. Reseaich Quarterly for Exercise and Sport 1997; 68:345-351.
Pate RR, Tmst SG, Felton GM, Ward DS, Dowda M, Saunders Re Cornlates of physical activity behavior in nual youth. Rescarch QuarterIy for Exerciae and Sport 1997; 68:241-248.
Robinson TN, Hammer LD, Külen JD. Kraemtr HC, Wilson DM, Hayward C, et al. Does television viewîng increasc obesity and rcâuce physical pctivity? Cross-sectional and longitudinal analyses among aàolescmt girls. Pediatrics 1993; 9 1:273-280.
F ' n P, Evenson S. Familiai aggregation in physicd activity. Reseprch Quarterly for Exercise and Sport 1991; 62:384-389.
Dishman RK, Sallis JK, ûrcnstein DR The detaminuits of physicd activity and exCrci=. Public Hialth R w 1985; 100:158-171.

70. Anonymous Inteptation of pulmonq fiinction tests: a practical guide. Philadelphia: Lippincott-Raven, 1997.
7 1. American 'ïhoracic Society. Standardization of sphmetry - 1994 Update. Am J Respir Crit Care Med 1995; lS2:llO7-1136.
72. Corey M, Levison H, Crozier DN. Eve- to seven-year course of pulmonary function in cystic fibmsis. Am Rev Respir Dis 1976; 1 14: lO8SlO92.
73. Rosenfeld M. Davis R, FiaSinunoas S, Pepe M, Ramsey B. Gender gap in cystic fibmsis moaality. Am J Epidemiol 1997; 145794-803.
74. Tanner JM, Whitehouse RH, Takashima S. Standards h m birth to manuity for height, weight, height velacity and weight velocity. British childmi, 1%5. Arch Dis Child 1966; 41:613-635.
FitzSimmons SC. Changing epidemiology of cystic fibrosis. J Pediatr 1993; 122:l-9.
Moore BJ, Durie PR, Forstner 00, Penchan P. The assessment of nutritional status in chiidren. Nutr Res 1985; 57:9749.
Szeinberg A, England S. Mindorff C, Fraser IM, Levison H. Maximal inspiratory and expiratory pressures are nduced in hyperinfiated, malnourished young adult male cystic fibrosis patients. Am Rev Rmpù Dis 1985; 132:766-769.
American Thoracic Society. Lung function testing: Selection of reference values and interpretative strategies. Am Rev Respu Dis 1991; 144: 1202-1218.
Godfny S, Davies CM, Wozniak ER, Barnes C. Cardio-respiratory nsponse to exercise in normai children. Clin Sc Mol Bi01 1971; 40:419-442.
Reisman JJ, Rivington-Law B. Corey ML, Marcotte JE, Wannamaker E, Harcourt D, et al. Role of conventional physiothcrapy in cystic fibrosis. J Pediatr 1988; 1 13:632- 636.
Dumin M A , Rahaman MM. The assessment of the amount of fat in the humsn h m meastuement of skinfold thickness. Br J Nutr 1967; 21:681-689.
Coates AL, Boyce P, Shaw DG, Godftzy S, Meams M. The relationship b e ~ e c n the chest radiograph, regional lung act ion studies asing 13N2, exacise tolerance and clinicai condition in children with cystic naOeis. Arch Dis Child 1981; 56:106-1ll.
Passero M. Remor B, Salomon I. Patient nportcd cornpliance with cystic fibrosis therapy. Clin M m 1981; 20:264-266.
McArdle WD, Katch FI. Kaîch VL. Exercisc Physiology. 3rd cd. Philaddphi$: Lea & Ftbiger, 1991.

Pate RR, Dow& M. Rose JG. Associations between physical activity and physicai fi mess in American children. AJDC 1990; 144: 1 123- 1 129.
Cody RP, Smith JK. Applied Statistics and the SAS Programming Language. 4th ed. New Jersey: Pnntice-Hall, Inc., 1997.
Kelsey JL, Whittemore AS, Evans AS, Thompson WD. Methods in Observational Epidemiology. 2nd ed. New York: Oxford University Press, 1999.
Cony ML, Edwards L, Lenson H, Knowles MR. Longitudinal analysis of pulmonary function decline in patients with c ystic fibrosis. J Pediatr 1997; 13 1 :809-8 14.
Reisman, I. J., Schneidennan-Waiker, Je, Canny, O. J., Wilkes, D. D., Mappa, L., Levison, He, Lu, W-Y., and Cony, P. Normal responses to progressive and steady state exedse in chilâren 11 to 18 years. Unpublished Work, 19%.
Washington RL, van Gundy JC, Cohen C, Sondheimer HM, Wolfe RR. Normal aerobic and anaerobic exercise data for North American schwl-age children. J Pediatr 1988; 1 12:223-233.
Cale LA, Almond L. Children's activity levels: a review of studies conducted on Bxitish chiidren. Phys Ed Rev 1992; 15: 1 1 1-1 18.
Koo MM, Rohan TE. Cornparison of four habituai physical activity questionnaires in girls aged 7-15 yr. Med Sci Sports Exerc 1999; 3 1:421-427.
Snedecor GW, Cochrane WG. Statistical Methods. 6th ed. Iowa: The Iowa State University Press, 1967.
Selvin S. Ptactical Biostatistical Methoàs. Caiifomia: Wadsworih Publishing Company, 1995.
Glantz SA. Slinka BK. Rimer of Applied Regmision and Analysis of Variance. 1st ed. New York: McGraw-Hill, hc., 1990.
Rowlandp AV, Eston RG. Ingledcw DK Relationship ktween activity levels. aembic fitncss, and body fat in 8- to 10-yr-old chilhn. J Appl Physiol1999; 86: 1428-1435.
Saüis JF, McKenzie TL, Alcaraz JE. Habituai physical activity and healthielateà physicai fitness in fourth-grede cMdren. AJDC 1993; 147:8%.
Pate RR, Ross JG. Factors associateci with health-rtlated fitness. JOPERD 1987; Novemk-Decemk.93-95.
Dotson CO, Ross JG. Relationship betwan activity patterns and fimess. JOPERD 1985; January:86-89.

100. Hyan RE, S c d m PD. Nalumm M. hterpretation of Pulmonary Function Tests. Philadelphia. Lippincott-Raven, 1997.

APPENDIX A
A SUMMARY OF EXERCISE INTERVENTION STUDIES IN CF



- a
go: œ

Table A.2: Unsurxrvised el
Patient motivation, inmesî, clinicai stability and panllnity to hospital
kontinued) Study Duradon
Phase A: 6 rnonths
Phssc:B:6months
Basdine vermis PbriseAvasus Pbasc B
Coatrol patients, askdiom -ge u ! d sctivity .
Conclusions


APPENDIX B
CONSENT AND ASSENT FORMS
Consent Fonn
HABITUAI, PHYSICAL ACTIVrrY AND THE ASSOCIATION WiTH DISEASE SEVERXTY AND EXERCISE CAPACEY IN CYSTIC FIBROSE: A PILOT STUDY
Sue PoUock, BPE Master of Science Candidate in Epidemiology, Department of Public Health Sciences, The University of Toronto (supe~sed by Dr. Mary Corey) Research Assistant, Division of Gmtmenterology and Nutrition, The Hospital for Sick Childnn Phone: (416) 8 13-5751
Dr. Mary Corey, PhD E~iderniolos!ist and Scientist. Division of Gastroeniaology and Numon, The Hospital for Sick Childrcn Associate Professor, Departments of Paediaüics and niblic Health Sciences, The University of Toronto Phone: (416) 8 13-5750
Jane Schneidennan-Waiker, MSc Exercise Physiologist, Division of Respiratory Medicine, The Hospital for Sick Childm Phone: (4L6) 813-7654 (extension: 4407)
Dr. Ja Reisman, MD, FRCP(C), MBA irologi&Division of Respiratory Medicine,
The Hospital fot Sick Children clsonate Rof«sot, The Facuity of Medicine,
The University of Toronto Phone: (416) 8 13-6167

Furpœe of the Researcb
We are conducting this study to document the M y activity patterns of cystic fibrosis patients. One of our aims is to evaluate the rclationship of different amounts, intensities, and types of activity with puimonary function and exercise performance. Knowleâge gained h m this study may help us benet understand the unique role of other therapies, such as exercise, in the treatment of cystic fibrosis. Additionally, we plan to invcstigate household and family-related fsctors that may pmmote participation in specific activities. This will help us make recommendations towards improving cornpliance to specific therapy pmgrams.
Description of the Reseoreh
If you choose to participate, the tim we nqUe h m you, as outlined below, will be minimal.
i)
ii)
iii)
iv)
During your c h i c visit, one of the study investigaton, will be avaiiable to answer any questions you may have, and to m e r explain this nsearch project. Your participation in this study mil not interfm with your standard treatment.
If you agree to s i p the consent form, you will be givm a questionnaire to complete while at the chic. This questionnaire asks you about your usual activity, and should take approximately 15 minutes to complete. There are also a few questions for parents to answer nlated to their own activity levels and other household factors.
Next, we will provide you with an activity diary to take home. We wiU ask you to fil1 out this diary for the 7 days folîowing your clinic visit, & M n g al1 your activities (sleep includeâ!). Upon completion of your activity record, you will need to send it back to us at the hospital. We may telephone you during the study period to offer support.
For children l a s than 12 years of age, parents will need to help with both the questionnaire and the activity diary. Investigato~ wiU need access to patient health mords to obtain information on pulmonary hnction. exercise testing, and chical statu. We may rtquire furthet input, by phone, to clPrify intonnation a h the saidy.
Then are no known harms associateci with participation in this study. However, you may find completion of the 7&y activity diary to be a minor time inconvenicnce.
Although you (or your child) wi i i not ducctiy benefit h m this study, we h o p tbat the uifonnation we collcct on your activity Ievels wiIi heIp us better undenitaad the d e that otha therapics, such as exacise therspy, couid play in the management of cystic l%msis. At the end of the study, we wiU m d you a summary of your o v d activity Ievel.

Confidentiality WU be respectai, and no information that discloses the identity of the subject will be nlcased or published without consent unless required by law. For your information, the nsearch consent form will be insemi in the patient heaith mord.
Participation in nseacch is voluntsry. If you choose not to participate, you and your family will continue to have access to quaiity c m at HSC. If you choose on behalf of your child to participate in this stuây, you can withdraw your child fiom the study at any t h e . Again, you and your family wiiî continue to have access to quality can at HSC.

For participants 16 y- otage a d o k r :
"1 acknowledge that the research procedm dehbed &ove have ban explained to me and that any questions that 1 have asked have been answed to my satisfhction. 1 have ban informeci of the alternatives to participation in this study, including the right not to participate and the right to withdraw without compmising the quality of medical c m at The Hospital for Sick Children for me and for other members of my family. As well, the potential harms and discornforts have been explained to me and I also understand the benefits (if any) of participating in the research study. 1 how that 1 may ask now, or in the future, any questions I have about the study or the restarch pmceduns. 1 have ban assured that recorcîs relating to me and my care wili be kept confidential and that no intorrnation will be released or printed that would disclose personal identity without my pemission unless required by law."
1 hereby consent to participate.
The Person who may be contacteci Nam of Patient and Age about the research is:
who may be reached at telephone #k Signature (if 16 p. or over)
Name of person who obtained consent
Date

For parene of participants leai tb.n 16 y t u r of age:
'1 acknowledge that the nsearch procedures describeci above have been explained to me and that any questions that I have askcd have k e n answmd to my satisfaction. 1 have been idormeci of the aitematives to participation in this study, includhg the right not to participate and the right to withdraw without compromising the quality of mcdicai can at The Hospital for Sick Chiidren for my child and for other members of my famiiy. As well, the potential hanns and discornforts have been explained to me and I also understand the benefits (if any) of participatiag in the nsearch stuây. 1 know that 1 may ask now, or in the future, any questions 1 have about the study or the research procedures. 1 have k e n assured that records rclating to my child and my child's care wiiî be kept confidentid and that no information will be nleased or printed that would disclose personal identity without my permission unless nquind by law."
1 hemby consent for my child to participate.
The Person who may be contacted Name of Patent about the research is:
who may be reached at telephone #: Signature
Name of person who obtained consent.
Date
Signature

Titie of Sbdy
HABITVAL PHYSICAL ACï IV ï ïY AND THE ASSOCIATION WITH DISEASE SEVERlTY AND EXERCISE CAPACIT'Y IN CYSTIC FiBROSIS: A PILXlT STUDY
1) Sue Pollock, BPE -Research Assistant, The Hospital for Sick Children -Graduate Student, The University of Toronto
2) Dr. Mary C o q PhD Scientist and Epidcmiologist, The Hospital for Sick Children -Associate Professor, The University of Toronto
3) Jane Schneidennan-Waiker, MSc -Exercise Ph ysiologist, The Hospiital for Sick Children
4) Dr. Joe Reisman, MD, FRCP(C), MBA -Pediatric Respirologist, The Hospital for Sick Children -Associate Rofessor, The University of Toronto
Questions vou mav have about the stumt:
Why are ne doing tbis study?
At the cystic fibrosis chic, doctors, nurses and physiotherapists ns intmsted in your activity patterns. Remarchers at the hoapital also want to know how you spend your time, including how much TV you watch, how often you go shopping with Ken&, end how many sports you play. This study wiii aiïow us to describe your activity levels, and compare them with other childm and other CF ciinics. Wc would aiso Lik to know why you choosc the activities that you do. For example, why Q some kids s p d thcir summers at the local pool. while others prefer to play on the cornputsr? This information will help us encourage aiî CF lads to make good choices about thcir chosen activities.

what rrUi happen d* thir study?
At your clinic visit, you wil l meet one of the study investigators. She wii i explain the study to you. If you and your parents agnt to participate. we wiii give you a short questio~maire to n11 out, esking you about the amount of time that you spend each day at high and low activity levels. If you are las than 13 years old, your parents will help you to fiii out this questiomain. Parents WU also have their own questions to answer about thcmselves and your neighbo&d We will also give you an activity diary to tak home. This is a record of your daily activities over a one week t h period After 7 days of filling out the diary, you will need to smd it back to the hospitai. We wiil provide you with a stamped, addresseci envelope to send it in.
A n the= good things and baà things about the ihdy?
We don't think that there is anything bad about this study. In fact, we think it will be fin for you to describe yow activity panmis, and to find out how you spend your time each day. At the end of the study, we wiil send you a summary of your o v e d activity level.
Who rvill know about what 1 did la the study?
Any information that we collect about you during this study wiil only be shared with the other study investigatonr. If we need to i&ntiQ you. we wiii only use your hospital identification number.
Yes. If you do not want to join ihis study, or decide halfway through that you no longer want to participate, notify the hospitai or your parents. We wiil respect any decision you make about your own participation.
For participants lem than 16 years of age:
"1 was pment when read this fom and gave hislher verbal assent."
Name of person who obtained assent
Date

GLOSSARY OF TERMS and ABBREVIATIONS
Forced Ex~Vstory Fiow Rate (FEF3-7s): The average forced expiratory flow rate over the middle b
50% of the forced vital capacity test.lm
Forced Ex~iratory Volume in one second (FEVI): The volume of air exhaleci in the first second
of the forced vital capacity test.Im
Forced Vital Ca~acitv WC): A maneuver in which the subjects exhales as rapidly and
completely as possible following a maximal in~~iration. '~
Maximal heart rate (HRmax): A measun of the number of times the heart bats per minute at
maximal exercise."
Maximal minute ventilation (vEmax): The amount of air that a subject inspires or expins in one
minute at maximal e~ercise.~
Maximal oxygen saturation (Sa02 at mm): An assessrnent of pulmonary p exchange at
maximal exercise."
Peak ex~iratorv flow rate (PEF): The maximal expiratory fiow rate that occurs shortly afkr the
onset of expiration in the WC test?"
Maximal oxvgen conswn~tion ( 9 0 ~ ~ ) : The maximal rate et which oxygen can be consumed
per minute. It is considmd to be the kst physiologie indicator of an individuai's aality to
transport and utiiize oxygen, and is a masure of an individuai's aerobic capacity."
1mai work caywity (wmax): The maximal workld a subject achi~ves during exercise
testingU
Ventüatorv ceserve (vE/MVV): The ratio of maximal ventiiation to maximum voluntary
ventüation. The test involveci fm mpxunal volrmtary ventilation requires the subjoct ta bmthe
138

hard and fat for 15 seconds. These nsults are extrapolated to 60 seconds, and repoaed in
minute?'

APPENDIX D
THE HABITUAL ACTIVITY ESTIMATION SCALE (HAES)

THE HABITVAL ACTMTY ESTIMAION SCALE (HAES)
Date :
This questionnaire contains specific questions about your activities of daily living. Try to answer each question as best as you possibly can.
Please nad the al i the directions canfully before completing the questiomaire. This wili make the task easier for you.
Instructions
This fom asks you to estimate your level of activity during different time pefiods throughout an average weekday (Monday to Fhday) and weekend (Saturday or Sunday). Please mal1 the activities of one typical dry within the past several weeks. For each t h e period, please estimate the percentage of time that you spent in each of 4 different activity levels. The different activity levels are deecribeâ below. For each of the time paiods, the totai time spent in all activity levels must add up to 100 96. Following is a sample question and answer senes. When completing the fom, only give the percentage of time in each category. You do not need to write in what you were actually doing!
Sample:
From when you finished breakfiut until you started lunch, please estimate the percentage of time
that you spent in each of the following activity levels:
a) inactive (i.e.. having a nap)
b) sornewhat inactive 60aD (i.e., watching TV)
C) somcwhat active 25% (i.e., shopping)
d) active JO% (i.e., riding a bicycle)
e) totai
Thene an ais0 a series of questions asking about the timing and length of meals and sleeping
habits. Plcase answer ail of these qutstims completely.

AC- LE= DESCRIPTIONS
These descriptions give you examples of activities that are hlpical of each activity level. You
should refer back to these descriptions as often as you need when completing your estimates.
a) inactive - sleeping, lying Qwn, resting, napping
b) somewhat inactive - Sitting, reading, watching television, playing vide0 gams, time in front
of the cornputet, playing games or activities which an mostly done sitthg down
c) sonwwhat active - walking, shopping, light household chores
d) active - ninning, jumping, skipping, bicycling, skating, swirnming, games that require lots of
movernent and make you breathdsweat hard

WeeWv Acn'vin,: For an average weekday (Le., Monday, Tuesday, Wednesday, Thursday or M y ) , please
estimate the percentage of tirne that you spent in each activity level.
1) After getting out of bed until starting breakfast:
a) inactive
b) somewhat inactive
C) somewhat active
d) active
e) totai
2) After finishing breakfiut until staxting lunch:
a) inactive
b) somewhat inactive
c) somewhat active
d) active
e) total
3) Afkr finishing lunch until starting supper:
a) inactive
b) somewhat inactive
c) somewhat active
d) active
e) total
4) A f h finishing supper until kâtime:
a) inactive
b) somewhat inactive
C) somewhat active
d) active
e) totai

For the average weekday that you are refedng to, please answer the following questions as
accurately as possible in the spaces pmvided.
s) At what time did you get out of bed in the moming?
6) At what time did you start eaîing breakfast?
7) How long did you spend eating breakfast? minutes
8) At what time did you start eating lunch?
9) How long did you spend eating lunch? minutes
10) At what time did you star& eating supper?
11) How long did you spend eating supper? minutes
12) At what time did you go to bed that evening?
13) For the average weekday that this questionnaire has asked you about, would
you rate your ovedl level of activity as being: (please chle)
a) very inactive
b) inactive
C) somewhat inactive
d) somewhat active
e) active
f) veryactive
14) Compand to other ment weekâays, would you rate yowlf on this
chosen &y as being: (please circle)
a) much less active than usud
b) a Little less active than usual
c) about the same as usual
d) a littie more active
e) much more active than usual

. ActtviLv:
For an average weekend day (i.e., Saturday or Sunday), please estin.uk the percentage of time
that you spent in each activity level.
15) After getting out of bed untii staiting breakfast:
a) inactive
b) somewhat inactive
C) somewhat active
d) active
e) totai
16) Mer finishing breakfast until starting lunch:
a) inactive
b) somewhat inactive
c) somewhat active
d) active
e) total
17) After finishing lunch until starting supper:
a) inactive
b) somewhat inactive
C) somewhat active
d) active
e) totai
18) After finishing suppei until bcdtimt:
a) inactive
b) somewhat inactive
C) soxnewhat active
d) active
e) totai

For the average weekend day that you are refenhg to, please answer the foilowing questions as
accuraîely as possible in the spaces providcd
19) At what time did you get out of bed in the moming?
20) At what fime did you start eating breakfast?
21) How long did you spend eating breakfast? minutes
22) ~t what time did you start eating lunch?
23) How long did you spend eating lunch? minutes
24) At what time did you start eating supper?
25) How long did you spend eating supper? minutes
26) At what time did you go to bed that evening?
27) For the average weekend day that this questionnaire has asked you about,
wouid you rate your ovedl level of activity as being: (please circle)
a) very inactive
b) inactive
c) somewhat inactive
d) somewhat active
e) active
f ) very active
2û) Compared to other recent weekend days, wouid you rate yourseif on this
chosni day as being: (please circle)
a) much less activethan wual
b) a iittie less active than usual
c) about the saute as usual
d) a iittie more active
e) much more active than usual
29) if you have any commcnts about your activity patterns that you tbink are
important, pl- mention them in the s p m below.

APPENDME
THE 7-DAY ACTnrlTY DIARY b

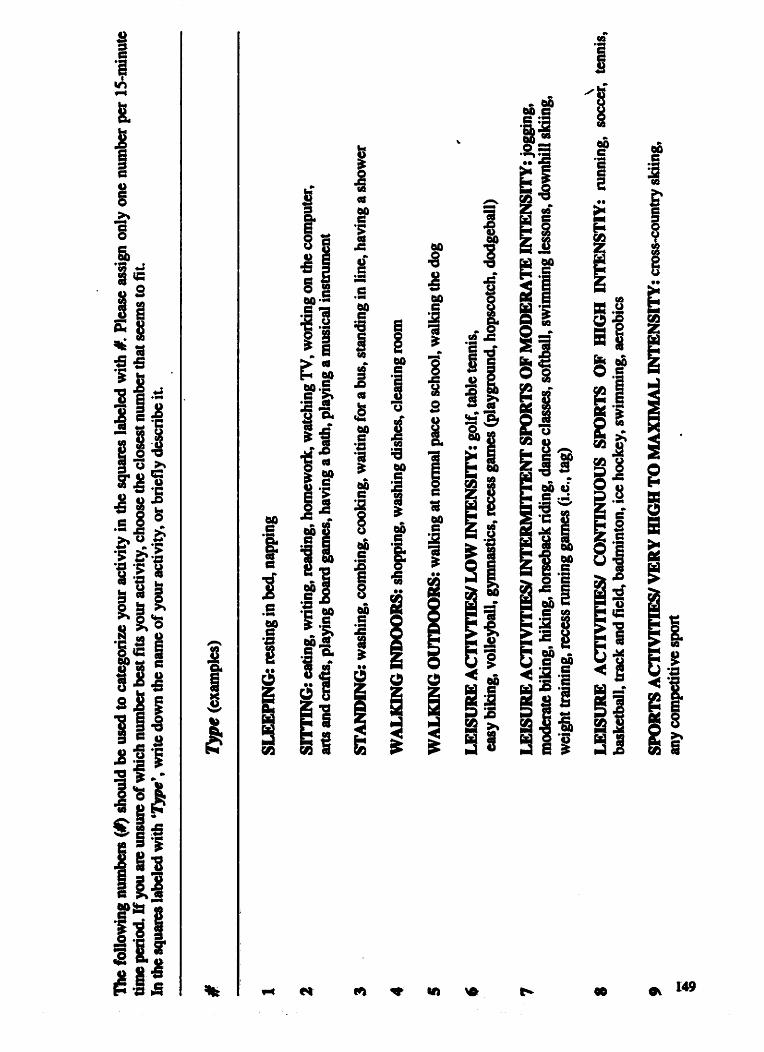




APPENDIX F
PARENT QUESTIONNAIRE

PARENT OUESTIONNAIRE
Dear pamts,
In order to complete our study on pediaûic activity patterns in cystic fibmsis, we also need to ask you a few questions about your own habits, household, and your child's involvement in activities. PIease answer as accurately as possible.
Child's name
Name of person completing this questiomain
Relationship to child
Date
Place an K next to the orie section which b a t describes YOUR current Ievel of daüy physicai activity:
You have a sit-down job and no regular physical activity.
Tlme to four hours of accumulated waking or standing in your working day are usual. You have no ngular organized physical activity dhng kisure time.
You are sporadically involved in mreational activities, such as weekend golf or tennis, occasional jogging, swimming, or cycling.
Usuai job activities might include lifting or srair climbing, or you participa& ngularly in ~ationaüfitncss activities such as jogging, swimming or cycling at least three buncs per week for 30 to 60 minutes each time.
You participate in txtcnsivt physical activity for60 minutes or mon at least four days pa
2. Now we WIN ask you abut YûUR CHILDsS participation in mmmudty baseâ phydcai acüvitime Please &le either YES or NO.
At the present tim, is YOUR CBILD involved in:
a public park or recreation department activities YES
b. physical activities within a church group YES
c. sports team or league YES
d. YMCA, YWCA or similar organization YES
e. health club, or pnvate sports lessons YES
f. Brownies, Cub Scouts, or other scouting group YES
g. 4-H or other farm club YES
h. another organization that promotes physical activity YES
If "Yes", please specify type/narne organization(s)

3. For each of these places where you an execcîse, p h ladicate CIit is on a h q d y trPvcleü route, andhot easiîy accessible to you (i.e., withtn a 5-minute àrîve h m your chiid's scbool or home).
a, aerobic dance studio
b. basketball court
6 bike lane or trails
e. golf course
f. health spdgym
g. mareialartsstudio
h. playing field (soccer, football, softbail)
i. public park
j. pubüc recreation center
k. racquetbalVsquash court
m. skating rink
n, sports store
O. swimming pool
p. walkinghüring trail
q. tennis court
r dance studio
A How d e do you tcd wPlWng la your neighborhood durjbg the &y? Pleacc chle ontv ong numbet fiom 1 - 5, whae 1= very unsefe and 5 = very safe.

5. Piara indicate which of the foiiowing apply Q your ndghborhoad
sidewatks
heavy trafnc
hilis
stnet lights
dogs that are unattended
enjoyable scenery
fnquently see people walkinglexercising
high crime
Herne indlfste which items you have in your home, yarà, or spartment complex
stationary aerobic equipment
bicycle
h g trampoline
running shoes
swirnming pool
weightlifting equipment, i.e., f ke weights, Universal gym, Nautilus equipment
toning devices, i.e., ankle weights, Dynabands, Thighmaster
aerobic workout vide0 or audiotapes
step aerobics, siide aembics
skates ( d e r blades. ice skates)
sports quipment (baiis, racquets)
surf board, boogie board, windsurf board
Cam, row boat, kayak
skis (water skis, domihiil skis, crosssountry skis)

APPENDM G
POWER CALCULATION
Given 188 eligible patients and an estimated 75% nsponse rate, we expect 140 patients
to participate in a longitudinal study. An estimate (bmed on objective monitoring) of the overall
percentage of adolescents in the healthy population engaged in regular moderate to vigorous
activity is 50%,16 therefore, we pmject approximattly 70 patients in each of the active and
inactive groups. The primary outcorne variable for our study, percent predicted FEVl. was found
to have a standard deviation of 18.6 in a similerly aged sample of cystic fibrosis childmi? At a
5% significance level. this sample of 140 patients has 89% power to detect a clinically
significant difference in mean FEVi of 10% pdcted betwem high and low activity groups of
qual numbers.
za
where: q3 =unbiown d = 10% predicted (the magnitude of diffmnce we an interested
in detecting between mean FEVl percent predicted for the active vems inactive groups
a = 18.6 n = the estimated numbcr of exposecl individuals=70 r = the ratio of umxposed to exposeci individuals=l/l za12 =1.%

APPENDIX H
SUMMARY OF ACTMTY TYPES
CF treatmen t crying Getting Dressed Getting Redy for Bed Gening Ready for Schaol Getting Ready for Sports Searching for Something
Domestic Work
Cleaning Cleaning (mm) Cooking Dusting Taking out the Garbage Making Bed Mowing Lam Packing up Supplies Putthg Away Omccnes Raking Lami Shopping Shopping for Grocenes Watering PlanWGrass
Acting Classes Drama Classes cornputer work Hdping Teacher Homework
A€tcr-schwl I wakend job

Hicle and Seek Playing Playing with F d l y Singing and Clapping Recess
Going to Lunch Socializing WaMng Around Walking h g Walking Indoors Work Break
Gym Class
CATEGORY S
Drying Self Off Searching for Something
Domestic Work
Outside Chorts Cleaning B k Mowing the L a w Packing up Stuff Ralsng the Lawn Shopping S weeping the S tain Washing the Car Watmog the GrasdPlants
CIssses School Field Trip Homcwodc

Ball Playing Sidewak Chaik h * g Party Games Amusement Park Carnival Oioup Gams Hide and Seek Hopscotc h Outside Play Playing Video Gama Play gmund Recess Swinging
Socializing Walking Dog Walking Outdoors Walking to Bus Walk To/Fmrn Schwl Walking to Work Work Break
Bike Hocda Hoop Hopping Running Yoga
CATEGORY 6
CrIrying Stuff aeaning Cicaning (mm) Hou8twork Wmhing Car wateriag Plmt!3 Yard Work

Drama Classes
Emlo~ment
AfierSchoo1/FYeekend Work
Hopscotch Game: 4-square Piaying in the Gym Playground Playing Playing in the School Yard Playing with Sister Recess S winging
Baii Playing Baseball Basketball Bike Bowling Playing Catch PE Class Cool-Down, Post-Soccer Dancing Dht Biking Dodgeball Fighting Fishing Tag Golf Gym GymnPstcs Hockey Roilerblade Rdg/JopgUig SkatcboBtding SItipping soccei: S=-B=M

RunningStairs Swim T-Bal1 Traick & Field Tmpoline
After-School and Weekend Work
Ultstructured Play
Chasing Someone Playing Recess
Walking
Badminton Bal1 Playing Baseball Basketball Bike Dancing DodgebaU Football Tag Gym Class Gymnastics Hockey Hado Hoop Lactosse Running Squash Running Stairs Soccer Soccef-Baseball Swim Tat-Bo TnickdField Trampoline Warsn-Up, Pre-Soccc~

CATEGORY 8
Rayground Playing Recess
Aerobics Badminton Bail Playing Bike Dancing DodgebaU Tag Gym Class Gym Class (Capture the Hag,) Gym Class (Scooters) Hockey Lacrosse Ksrate Rollerblading Roller-skating Running So~~er-Drills SoccerScnmmage Running S tain Track and Field
CATEGORY 9
red Pla\!
Reccss
Basketbal1 Bike Dance RoUctblding Soccer Track andField