Embed Size (px)
Citation preview

Acta Medica OkayamaVolume 25, Issue 5 1971 Article 4
OCTOBER 1971
Clinical and experimental studies on folic aciddeficiency due to anticonvulsants. I. Clinicaland nutritional study on megalobastic anemia
due to anticonvulsants
Hirokuni Taguchi∗
∗Okayama University,
Copyright c©1999 OKAYAMA UNIVERSITY MEDICAL SCHOOL. All rights reserved.

Clinical and experimental studies on folic aciddeficiency due to anticonvulsants. I. Clinicaland nutritional study on megalobastic anemia
due to anticonvulsants∗
Hirokuni Taguchi
Abstract
Two cases of megaloblastic anemia associated with anticonvulsant drugs were studied. Bothcases were inpatients of psychiatric hospitals and had quite inadequate intakes of food. The formerhad lung tuber. culosis and the second had febril illness before the manifestation of anemia. Multi-ple examinations including bone marrow smears, serum iron levels, vitamin B12 levels, estimationof urinary formiminoglutamic acid after histidine loading and folic acid tolerance test revealed thatthis anemia was due to folic acid deficiency. Complete hematological responses were ob3ervedwith injection of folic acid. Retrospective nutritional study on the second case was carried out.The study revealed that folic acid content of the diet of this hospital was 152 fl.g of free folateand 522 fl.g of total folate. The folic acid mtake of the patient was about 80 /1.g of free folateand 280 l1.g of total folate daily during a month before the manifestation of megaloblatic anemia.Importance of additional factors for the development of megaloblastic anemia in patients receiv-ing anticonvulsants was discussed and it was concluded that most important factor was nutritionaldeficiency of folic acid.
∗PMID: 4264432 [PubMed - indexed for MEDLINE] Copyright c©OKAYAMA UNIVERSITYMEDICAL SCHOOL

Acta Med. Okayama 25, 537-550 (1971)
CLINICAL AND EXPERIMENTAL STUDIES ON FOLICACID DEFICIENCY DUE TO ANTICONVULSANTS
1 CLINICAL AND NUTRITIONAL STUDY ONMEGALOBLASTIC ANEMIA DUE TO
ANTICONVULSANTS
Hirokuni T AGUCHI
Department of Internal Medicine, Okayama University Medical School,
Okayama, Japan (Director: Prof. K. Hiraki)
Received for publication, September 23, 1971
Megaloblastic anemia due to anticonvulsant drug therapy was firstreported by MANNHEIMER et al. (1) in 1952. Many case reports and in.vestigations on the anemia have hitherto been carried out. In Japan, thefirst case was reported by the author in 1967 (2). Three other cases havebeen recorded in Japan thereafter (3)(4)(5). The fifth case in Japan wasobserved by the author recently. Attention has been directed to rareoccurrence of the megaloblastic anemia in patients receiving anticon.vulsant drug therapy. Additional factors other than the ingestion ofanticonvulsant drugs appear to be operative in the development ofsufficient folate deficiency to produce a megaloblastic anemia. Inadequatediet was thought to be one of the most important factors for the aggrava.tion of folic acid deficiency in the two cases observed by the author.Therefore, case history of the two cases was briefly described and retrospective nutritional studies were carried out to show that malnutrition playsa role for the manifestation of severe anemia in these cases.
SPECIAL LABORATORY METHODS
Folic acid activity of serum, cerebrospinal fluid (CSF) and urine were assayedby the method described by WATERS and MaLLIN (6) using Lactobacillus casei (L.
casei ATCC 7469) as the test organism. Difco folic acid casei medium wasemployed. Normal value in this laboratory was 3.5-20ng/ml. Serum and CSFvitamin B12 (Ed activities were determined by the method of Japan Vitamin Society (7) using L. leichmannii (ATCC 7830). Normal value was 150-900pg/ml.
D-Xylose absorption test was performed by the technic described by BENSONet al. (8). Sideroblastogram was drawn by the way advocated by KIMURA (9).Urinary formiminoglutamic acid (FIGLU) secretion after oral histidine loadingwas estimated according to the technic described by CHANARIN and his associates
537
1
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

538 H. TAGUCHI
(10). Folic acid clearance study was performed by the method of CHANARIN et at.(11). Estimation of food folate contents was made by the technic of HERBERT(12). Slight modification was made as follows (13). One or two grams of foodswas homogenized with 0.1 M phosphate buffer (pH 6.0) containing 150 mg% ofascorbic acid in glass homogenizer. The homogenate was autoclaved at 121°Cfor 10 minutes. After centrifugation, a half of the clear supernatant was setaside for estimation of total folate. The another half of the supernatant wasdiluted with water adequately for assay of free folate. Total folic acid, whichimplies pteroylpolyglutamates conjugated by three to seven glutamic acids, wasestimated with the former half of the supernatant. After incubating them separately for 24 hours at 37°C by adding 3 mg/l0 ml of Difco dessicated chickenpancreas, they were autoclaved for 5 minutes at 121°C. Centrifigation was madeand clear supernatants were diluted adequately and assayed respectively forfree and total folic acid. The way how to calculate folic acid contents of thehospital diet will be shown in the part of special nutritional study of this paper.
CASE REPORTS
Case. 1. A 34.year-old male, who had been admitted in a psychi.atric hospital on a diagnosis of psychomotor epilepsy since 1955, hadsevere anemia in the end of September, 1965. He had not received anyanticonvulsant until May 6, 1965, when he was administered 100 mg ofdiphenylhydantoin and 100 mg of phenobarbital for the first time as aepileptic attack (grand mal type) recurred since April of that year.Hematological examination performed a month after initiation of theanticonvulsant therapy showed red cells 4, 300, 000 per cubic milliliter(cu. mm.), hemoglobin (Hb) 9796 and white cells 6, 200 per cu. mm.. Hisdietary history at the hospital was very capricious and he frequently refusedto take hospital diet. In September 1965, he complained of abdominalpain and anorexia. There were no vomiting and diarrhea. On 20th,September, fever of 38. 5°C occurred and continued every day. He becamepale and general weakness was aggravated. On 28th, September, preciseclinical examination was performed. The patient was an asthenic man,who appeared not to be malnourished. The skin was pale but edema,exanthema and petechiae were not detected. The tongue appeared normal.Pulse rate was 72 per minute and blood pressure, 100/56 mmHg. Slightdegree of systolic murmur was heared at the apex. Auscultation of thelung revealed moist rales at the right upper lobe. The liver and spleen werepalpable 1 em below the costal margin. The kidneys were also palpable.Neurological examinations did not disclose any abnormalities.
Initial laboratory study revealed Hb of 40 %, red cells 1, 770, 000 percu. mm., reticulocytes 1.2 % and a platelet count of 92, 000 per cu. mm.
2
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4

Folic Acid Deficiency due to Anticonvulsants 539
The count of white cells was 4, 600 per cu. mm. with a differential of 2.5% of promyelocytes, 1.5 96 myelocytes, 2.5 % metamyelocytes, 12.5 %band netrophils, 63.5% segmented neutrophils, 1.5% eosinophils, 1.5%monocytes, 14.5% lymphocytes. Microscopic examinations of peripheralblood smears revealed macrocytosis, anisocytosis, polychromatic erythro.cytes, Jolly bodies, Cabot rings in erythrocytes and hypersegmentedpolymorphonuclear cells. Serum iron level was 163 lJ.g / dl. Gastric juiceshowed normoacidity. Roentgenograms revealed normal upper gastro.intestinal and small bowel series. The chest film showed the presence oflung tuberculosis at the right upper lobe. Tubercle bacilli were negativein the sputum. Sternal marrow aspiration smears revealed a typicalmegaloblastic pattern. 39.4 % of the nucleated cells were megaloblastsand giant metamyelocytes were observed. Findings from the followingexaminations were all normal; relative to urinalysis, stool (parasite eggsand occult blood), liver function tests, serum cholesterol, serum protein,electrolytes, NPN, PSP, fasting blood sugar, glucose tolerance tests,amylase levels in serum and urine, electrocardiogram and ocular fundi.
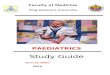
As assay of serum folic acid and Bj2 was impo~sible at that time, dia.gnosis ex juvantibus was employed (Fig. n Since 7, October, injection of2, OOOl-,g of hydroxocobalamin was made without subsequent reticulocytosiseven after one week. All the anticonvulsants were stopped since 12 Oct.Pteroylglutamic acid (15 mg) was injected intramuscularly since 14 Oct.Two days after the initiation of folic acid, bone marrow became normo.
Ph:~:~:;i~ital~ g::: ~;"N"'''4w,,,,!-,,,~,,:,'''t'<!'''''\:-:,,-,c':''':<l{"-.,'!!;\,-,,;:,,;-,,IV.B ,,1,0001'11 III I I II I II! III! 1 I II I IIII1I1!I!II!I!I!II1!U
Folic Acid I 5mg C:;:;:;:::::::::::::::::::::::;:;:;:;:;:~3~~~::::::::::::::::::::::::::::::::::::::;:.~
Fe 10mg 40mg ~V.C200mg l
~\ . '-'-"~,I " \
Hb 1'Ft\ \R-SC··-t,/! \. \
./ ! \ \,WB~ ! \ ~.- _.- -- - -.- -.-._._.- _.-.-.__':l_~_t .•/1 "" . ..._. __ ......_..._._...' • __...... ._••_.._._
Hb RBC ~;~:Nt, Eo. ~":Nt, Eo.
I. Ebl. Ebl
% X10' ::: Mgbl Mgbl80400
60300
40200
20100
1966 10.1 11.1
~"'N~: t, Eo.':~~
Ebl
// .........--
T.N. t Age 34~
/'-------
12.1
Ret WBC%" X 10'10010
505
Fig. 1 Blood changes and therapies in Case 1.
3
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

540 H. TAGUCHI
blastic. On the fifth day of the treatment, reticulocytes' peak of 11.6 %was observed. Appetite improved within three days. Epigastralgia, nauseaalso disappeared rapidly after administration of folic acid.
Streptomycin, isonicotinic acid, sulphonamide were administered forthe lung tuberculosis. On 20 Oct., eighth day after the cessation of anti.convulsants, a severe attack of epilepsy occurred. Anticonvulsants wereadministered again since that time. No increase in fit frequency wasobserved since then despite the administration of folic acid. Parenteraliron supplements were employed for the relative iron deficiency by a rapidrecovery of the anemia. These procedures gave rise to complete hemato.logical and clinical remission within two months. This case was the firstreport of megalo blastic anemia due to anticovulsant in Japan.
Case 2. A twenty.year old male, who had been admitted to FuchuHospital since January of 1967 as psychomotor epilepsy, was referred to ainternist of the hospital for his severe anemia on 14 Oct. 1970. He hadbeen taking60mg of phenobar bital since February of 1968, then ComitalL (containing 50 mg of diphenylhydantoin, 50mg of prominal and 50 mgof phenobarbital in a tablet) two tablets a day since May, 1968. ComitalL was increased up to 3 tablets a day since September 1969. The attack ofepilepsy had been infrequent but he had shown explosive disposition andautistic proneness. He had been irascible and violent to other patientsfrequently. His dietary habits had been very fluctuating. He had not eatenvegetables at all. Occasionally he refused to eat anything all day long.In March 1970, hematological examinations revealed red cells 4, 150, 000per cu. mm., Hb 15.9g/ dl, and white cells 4, 400 per cu. mm. In June,slight degree of anemia (red cells 3, 580, 000 per cu. mm.) was detected.No attention was paid to this fact by his doctor at that time. In Septern ber, he had fever, cough and sore throat. His appetite was lostmarkedly. Nausea, vomiting and sore tongue made him not to takehospital diet sufficiently. At the end of September, the nurses notedpaleness of his face. In October. 1970, nausea, vomiting, dizziness andgeneral weakness were aggravated. So examinations on the cause of theanemia were asked of the author.
Physical examination showed a well nourished, middle statured man.No edema and petechiae were observed in the skin. No palpable lymphnodes were detected. Conjunctiva was anemic but not icteric. Tonguewas not atrophic but had slight hyperemic appearance. Gingiva showedno hypertrophy. Body temperature was 36.7°C. Pulse rate was 76 perminute and blood pressure 120/70 mmHg. Evidence of cardiomegaly waspot observed. A grade II systolic cardiac murmur was heard best at the
4
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4

Folic Acid Deficiency due to Anticonvulsants 541
apex. Lungs were clear. No abnormalities was found in the abdomenand at no time was there any subjective or objective evidence of anyneurological abnormalities.
Examination of his blood showed red cells 1, 430, 000 per cu. mm.,Hb 5.3 g/dl, packed cell volume 16 %, mean corpuscular volume (MCV)112 cu. p.., mean corpuscular Hb concentration 34%, reticulocytes 0.4%,platelets 180, 000 per cu. mm., leucocytes 2, 150 per cu. mm. (polymorphs62%, eosinophils 1%, lymphocytes 37%)
Stained blood film showed macrocytosis, anisocytosis and hypersegmented neutrophils. Erythrocyte sedimentation rate was 45mm/hour.Urinalysis and stool examination were normal. Serum iron level was 500/J.g/dl. Serum LDH showed a high level of 1130 unit. Examinations ofserum revealed cholesterol 186 mg/dl, bilirubin 0.50 mg/dl, SGOT 19,SGPT 14 Karmen Unit, Alkaline phosphatase 6.9 King.Armstrong units,and serum protein 7.3 g/dl with A/G ratio of 2.09. The chest roengenogram, gastrointestinal series with small bowel study were within normallimits.
Free hydrochloric acid was present in the gastric juice. Bone marrowaspiration was not performed at the time of the first examination. Totalof seven units (1, 400 m!) of blood transfusion, parentheral iron and B12
were given on the following seven consecutive days. To this treatmentthere were no reticulocyte response. Marrow aspiration was carried outon 24, October. The stained film revealed the presence of 30.8 % ofmegaloblasts. Giant metamyelocytes were also present. Sideroblastogramdisclosed a type of pernicious anemia. Serum folic acid level was 0.5 ng/ml. Serum B12 level was 2,375 pg/ml. FIGLU excretion was 110.5 mg(normal 0-17 mg). CSF folic acid level was 8 ng/ml (normal 5-50) andCSF BJ2 level was 60.7 pg/ml (normal 0-30), Folic acid clearance test wasmade by intravenous injection of 15 ,ag/kg of folic acid. The peak ofserum folic acid level obtained after injection of folic acid was lower inthe patient than in control. Urinary excretion of folic acid was alsoreduced in the patient. These results showed that there was folic aciddeficiency in the patient (Table 1). The course and therapy are shown in
TABLE 1. FOLIC ACID CLEARANCE STUDY
Time (min.)Serum Folate Levels after 15pg/kg
of Folic Acid (ng/ml)5 15 30 60 120
UrinaryExcretion(pg/day)
Patient
Control
50
110
20
92
12.5
58.5
8.7
447.5
4087.5
210
5
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

20 100
542 H. TAGUCHI
DPHf2????Z222Z?222222ZZ2222222ZZZZ2222ZZZ22d( Aleviatin)
Folic Acid15"'f I:;··:·· ... ,.'.:.""."",,', ,.. ,...,.:.,.:.,:.....::",,:,.... :......]
VB. 0.5"'f ImIIIDBlood _200m!
Fe4O"'f_
Hb RBC T N ~ Age20% 10
80 400 "RBC'" f-..
\ : 'J \ /'.60 300 \ ./•••••':'.... // ""'___..-...........\--
40 200 WBC "'-:::':\ i............... :;;-.f
'.Ret··········.: ••••••••••••
Ret WBC.0/00 10
30 6
20 4
10 2
1970 3.106.159.3 10.1 11.1 12.1
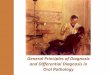
FiZ. 2 Blood changes and treatments in Case 2.
Fig. 2. 720 Jl1g of folic acid was injected on 31, Oct. for the folic acidclearance test. Then 15 mg of folic acid was injected twice a week.Reticulocytes reached its peak of 3.4 % three days after the injection offolic acid. A week later, bone marrow became normoblastic. A goodhematologic response was obtained without discontinuing the anticonvulsants. The administration of folic acid had no effect on fit frequency.The blood picture improved rapidly and on December 4, it showed: redcells, 4,460, 000 per cu. mm., Hb., 14.6 gjdl, white cells, 6, 100 per cu.mm.
NUTRITIONAL STUDY
The anemia III the second case was severe from July to September,1970, that is before folic acid therapy. A retrospective nutritional studyon this period on the patient was carried out to ascertain the cause of thisanemia.
Dietar)l histOly :Amounts of foods he had taken daily during these period were obtained
by the clinical records of that hospital. The rate of food intake of allthe given hospital diet is shown in Fig. 3. During the period of August 20to 31, he had taken all given diet in six of twelve days. In September hetook full diet only two days. For fifteen days he took less than a half ofthe daily diet. His food intake was less than 80% for other eleven days.
2 folic acid contents of each food:Folic acid contents of various food were assayed by the method des.
cribed in the chapter of special laboratory methods of this paper. The
6
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4

Folic Acid Deficiency due to Anticonvulsants 543
Folic Acid Intake of the Patient
600
500
400
300
200
,00
Date
~ Total Folate~ Free Folate
~E::~t" E::v ~~~~~~ ~ ~~ ~1;1 1;1 17 ~[;' l)- I-
~,p'1"t7. ~~I" u
I)- r;-I"
50 50% %
% intake of diets
Fig. 3 Intake of diets and folic acid in Case 2.
TABLE 2. FOLIC ACID CONTENTS OF MAIN FOODS.
(ftg/g)
THE TERM "FREE" INDICATES FOLIC ACID CONTENT OF FOOD ASSAYED BEFORE
TREATMENT OF CONJUGASE. "TOTAL" MEANS FOLIC ACID ASSAYED AFTER CONJUGASE.
IN PARENTHESIS THE WAY OF COOKING WAS SHOWN.
Free Total Free Total
Rice (boiled) 0.024 0.200 Tuna, sliced 0.040 0.243l l Whale (boiled) 0.008 1.1550.070 0.345
Bread 0.035 0.750 Spinach 1.280 2.105
Potatoes (boiled) 0.027 1.692 Lettuce 0.750 1.340
Eggs, white 0.007 0.066 Cabbage 0.483 1.270
yolk 1.300 1.800 Leak, green 0.704 2.006
Beef (steak) 0.105 0.991 Radish 0.450 0.770
Fork (steak) 0.011 0.912 Cucumbers 0.290 1.017
Chicken (boiled) 0.140 0.408 Carrot 0.235 0.456
Lobster (broiled) 0.855 1.710 Onions 0.020 0.062
Mackerel (boiled) 0.166 0.788 Apples 0.040 0.100
horse Mackerel (boiled) 0.144 0.344 Tomatoes 0.500 0.840
~ a1mon (salted) 0.024 0.440 Bananas 0.350 0.966
Facific ~aury (broiled) 0.090 0.410 Mandarin Oranges 0.260 0.294
Octopus (boiled) 0.035 0.180
results have been reported previously (13). Some of them are quoted mTable 2.
3 Calculation of the folic acid intake of the patient.An example of the way of how to calculate the folic acid intake is
shown in Table 3. Materials of each meal are presented at the first column.
7
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

544 H. TAGUCHI
TABLE 3. AN EXAMPLE OF THE WAY OF CALCULATION OF FOLICACID INTAKE OF THE PATIENT.
Unit folate Food folate Intake of Folate inta1,eMenu Amount content ( ) diet by of the patient
(I-lg/g) content I-lg patient (fIg)
Break fast rice 250 0.047 11.8 7 8.310
17 5 8.5soy soup 10
Lunch rice 250 0.047 11.8 7 3.5-TOOm1et egg 50 0.47 23
onion 40 0.02 0.8
5 0.1 0.53
15.6carrot -10-
pea 3 0 0
minched chicken 20 0.14 2.8
Cabcage 30 0.48 14.5
Salted greens
cucumber 50 0.2 10
carrot 5 0.1 0.5
Supper rice 250 0.047 11.8
octopus 70 0.082 5.7
radish 20 0.45 9.0
cucumber 10 0.29 2.9 0 0
potato 80 0.027 2.2
pork 10 0.02 0.2
green pepper 10 0.02 0.2
Total 124.7 35.9
The second column shows amount of each materials. The third one isfolic acid content of the foods. The next column, folic acid contents ofeach food, is obtained by multiplying the value of the second column bythat of the third one. The fifth column is the ratio of his food taking.The final column indicates the amount of folic acid taken by the patientfrom each materials. According to this table, he took 35.9 .'tg of freefolate of 124.7 ,'l.g of given foods on Septem ber 6. Calculations of folateintake of the other days were carried out in the same way. Results werepresented in Table 4. Mean folic acid supply by diets of this hospital was152 IJ.g of free folate and 522 IJ.g of total folate. From August 30, meanfree folate intake of the patient was 123 jag of 151 /l.g of given folate ofthe hospital diet and mean total folate 412 Itg of 509 IJ.g, and the patienttook about 80 IJ.g of free folic acid and 280 IJ.g of total folic acid during
8
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4

Folic Acid Deficiency due to Anticonvulsants
TABLE 4. FOLIC ACID INTAKE OF THE PATIENT. THE AMOUNTS SHOWN IN
PAREI\THESES ARE THAT OF FOLIC ACID GIVEN AT THIS HOSPITAL.
545
Date
20,Aug.
21
22
-23
24
25
26
27
28
29
30
Free Folate
125 (171)
119
169
131 (152)
193
189
116
64 (102)
29 (122)
79 (164)
142 (169)
Total Folate
371 (552)
452
600426 (520)
554
740
373
254 (282)
98 (458)
195 (525)
471 (539)
rate
31
1, ~e;.
23
4
5
6
7
8
9
10
Free Folate
154
182
169
85 (141)
54 (112)
41 (204)
36 (12.5)
8 (I05)
51 (165)
24 (139)
32 (86)
Total Folate
539
522
636
327 (553)
215 (430)
166 (625)
123 (597)
48 (463)
108 (504)
136 (504)
189 (613)
Mean 123 (151) 412 (509) I Mean 76 (153)
free folate
274 (544)
Total Folate
II,Sep.
12
13
14
15
16
17
18
19
20
Mean
84 (I34)
72 (47)
50 (172)
74 (149)
56 (156)
97 (l80)
93 (137)
69 (l32)
123 (165)
82 (170)
80 (154)
354 (504)
330 (544)
210 (566)
247 (494)
200 (488)
271 (523)
378 (533)
257 (473)
329 (531)
269 (507)
284 (516)
21,Sep.
2223
24
25
26
27
23
29
30
Mean
iO (140)
106 (129)
65 (167)
32 (198)
70 (139)
82 (l09)
117 (150)
76 (168)
117 (126)
82 (78)
82 (I50)
270 (540)
357 (537)
194 (537)
133 (585)
225 (550)
264 (421)
382 (484)
270 (582)
352 (441)
279 (515)
273 (519)
September, when his anemia might be aggravated.
DISCUSSION
Megaloblastic anemia due to anticonvulsants is very rare. In Japan,only five cases have been reported. In this paper the first and fifth casesare recorded. Anemia was detected in psychiatric hospitals. They hadsevere megaloblastic anemias during the course of anticonvulsant therapy.Differences from the classic type of pernicious anemia was the presenceof free hydrochloric acid in gastric juice and absence of neurologicaldisturbances. The nature of the anemia was clearly by folic acid defi.ciency. In the first case, therapy by BI2 was not effective. Administra-
9
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

546 H. TAGUCHI
tion of folic acid alone could induce a clinical and hematological response.In the second case various examinations on folic acid metabolism werecarried out. Serum folic acid level was extremely low. FIGLU excretionafter histidine loading was increased. Folic acid tolerance test revealedlow peak serum level of folic acid and less urinary folate excretion. Thereis no doubt that megaloblastic anemia during anticonvulsant therapy isdue to folic acid deficiency. Though the mechanism by which anticon.vulsants cause folic acid deficiency is yet unknown (4), evidence suggest.ing frequent occurrence (as high as 75%) of subclinical folic acid deficiencyamong patients receiving anticonvulsant drugs was known (5)06). Manyother observations in non.anemic patients receiving anticonvalsants (7)
(8) (9) (20) (21) (22) showed a high incidence of macrocytosis and lowserum folate levels. These 0 bservations suggest that folic acid deficiencycaused by anticonvul~antsis not so severe in its degree. Some additionalfactors may be required for the initiation of severe megaloblastic anemia.Two cases presented in this paper were inpatients of psychiatric hospitals.Many other reports (23)(24)(25) noted high incidence of this anemia amongmentally defective or psychotic patients. The dietary intake of mentallydefective patients is frequently inadequate as was the case in the twopatients reported in this paper. Therefore the importance of nutritionalfactors for the occurrence of megaloblastic anemia due to anticonvulsantswas suggested. NEWMAN et ai. (26) and KIDD et ai. (25) reported cases inwhom malnutrition were observed. FLEXNER et ai. (27) were the fir~t thatperformed nutritional studies on the case of megaloblastic anemia due toanticonvulsant~. Their studies were composed of taking dietary history,folic acid tolerance tests, estimations of serum vitamin C level, vitamin Alevel, carotene level and iron level. Absorption test on Bj~, glucose andtriolein were also included. These analysis disclosed poor intake of folicacid, vitamin C and of some of vitamin B complexes. Amounts of folicacid taken by the patient was not studied.
The pre~ent study may be the first that investigated the amount offolic acid which the patient had taken before the onset of megaloblasticanemia. The second patient received diphenylhydantoin, phenobarbitaland prominal since May, 1968. He was not anemic in March 1970.Anemia was dicovered in Octo ber 1970. Folic acid deficiency was rapidlyaggravated in these period. The clinical record of this hospital showedthat his dietary intake was extremely diminished in August and Septemberof that year. Even the half of the given diets were not taken by thepatient in September, that was a month before his anemia was detected.Accordingly folic acid intake from diets was diminished. Mean folate
10
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4

Folic Acid Deficiency due to Anticonvulsants 547
content of the hospital in these period was calculated as 152 /J.g of freefolate and 522 p.g of total folate. Folic acid content of hospital diets inJapan was reported by IWASAKI and SANADA (28). According to theirwork assay was made in two hospitals. Free folate of 108 /J.g/day andtotal folate of 422 ,ag/day were the mean daily folic acid content of thehospital A. In hospital B in their work, mean free folate per day was138 lJ.g and total 351 /J.g. The values obtained in the present study werecomparable to these value~.
BUTTERWORTH et al. (29) showed that American diet contained 157 ,fI.gof free folate and 688 lJ.g of total folate per day. CHANARIN et al. (30)reported that healthy pregnant women in England took 160 /J.g of freefolate and 676 lJ.g of total folate daily from their diets. These values areessentially in agreement with the values found in the present study. Availability of food folate is different by its form. Monoglutamate form offolate are readily absorbed than polyglutamate. About 80 % of monoglutamate form of folate in foods is absorbed (31). Most of the folate infoods is present in the form of polyglutamate. PERRY and CHANARIN (32)described that some 27 % of polyglutamate forms of folate was absorbed.Calculated amount of folate by applying the values was about 263 lJ.g inthis hospital.
Minimal daily requirement of folic acid has been considered to be 50/J.g (33) to 100 /-~g (34). Therefore, folic acid was adequately supplied in thishospital. As was demonstrated in Table 3 and Fig. 3, folic acid intake ofthe patient studied in this paper was very poor in September. Mean wasabout 80 lJ.g of free folate and 280 ,ag of total folate during this period.These amounts were about half of the given folate. Considering theabsorption rate, some 140 /J.g of folate could be absorbed if inhibition offolate absorption was not present.
At present a hypothesis that anticonvulsants interfere with absorptionof folic acid is almost proved (35) (36) (37). Therefore, folic acid absorbedby the patient in the present study was much less. Folic acid deficiencyof the patient was aggravated and megaloblastic anemia became manifestduring this period. Though coincident occurrence of infection in thesepatients may playa role for the development of the anemia by increasingfolic acid requirement (38) (39) (40), it is concluded that inadequate intakeof folic acid from foods is the most important factor for the manifestationof megaloblastic anemia due to anticonvulsants. This fact suggest~ thatmegaloblastic anemia will not be seen in patients receiving anticonvulsantsif their diet intake is adequate. This conclusion explains well the questionwhy megaloblastic anemia is so rare among patients receiving anticonvul-
11
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

548 H. TAGUCHI
sants and why the anemia is relatively frequent in mentally defective menwho seem to have peculiar diet habits.
CONCLUSION
Two cases of megaloblastic anemia associated with anticonvulsantdrugs were studied. Both cases were inpatients of psychiatric hospitalsand had quite inadequate intakes of food. The former had lung tuber.culosis and the second had febril illness before the manifestation of anemia.Multiple examinations including bone marrow smears, serum iron levels,vitamin B12 levels, estimation of urinary formiminoglutamic acid afterhistidine loading and folic acid tolerance test revealed that this anemiawas due to folic acid deficiency.
Complete hematological responses were ob3erved with injection offolic acid. Retrospective nutritional study on the second case was carriedout. The study revealed that folic acid content of the diet of this hospitalwas 152 fl.g of free folate and 522 fl.g of total folate. The folic acid mtakeof the patient was about 80 /1.g of free folate and 280 l1.g of total folatedaily during a month before the manifestation of megaloblatic anemia.Importance of additional factors for the development of megaloblasticanemia in patients receiving anticonvulsants was discussed and it was con.cluded that most important factor was nutritional deficiency of folic acid.
ACKNOWLECGEMENT
Grateful ac' nowledgement is made to frofessor KIYOSHI HIRAKI, Director, Departmentof Internal Medicine, OJ ayama University Medical School, for his constant interest andguidance; to Assistant Frofessor ICHIRO IWASAKI and to Dr. HIROSHI SANADA for theirdirections; to Elara Se'izen Hospital and Fuchu Hospital for their kind supports forstudying the cases.
REFERENCES
1. MANNHEIMER, R., PAKESCH, F., REIMER, E. F. and VETTER, R.: Die hamatologischenKompli' ationen der Epilepsie Eehandlung mit Hydantoin-Korpern. Med. Klin. 47,1397, 1952
2. TAGUCHI, H.: Megalo'lastic anemia due to anticonvulsant drug therapy. jap. j. Clin.Hemal. 8, 549, 1967 (in japanese)
3. SHIMIZU, H.: Megaloblastic anemia due to anticonvulsants. j. jap. Soc. Int. Med. 59,
90, 19iO (in japanese)4. HIKA, H., SAKURAGAWA, N., FUKUHARA, N. and YAMADA, K.: Megaloblastic anemia
during diphenylhydantoin therapy. j. jap. Soc. Int. Med. 59, 72, 1970 (in japanese)5. TAKAHASHI, R. and HIROSE, H.: Megaloblastic anemia due to anticonvulsant drug the
rapy. jap. j. Clin. Hemal. 11, 259, 1970 (in japanese)
12
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4

Folic Acid Deficiency due to Anticonvulsants 549
6. WATERS, A. H. and MOLLIN, D. L.: Studies on the folic acid activity of human serum.J. Glin. Path. 14, 335, 1961
7. Japan Vitamin Society: Method for assay of blood vitamin BIz. Vitamin 19, 438, 1960(in Japanese)
8. BENSON, J. A.Jr., CULVER, P.J., RAGLAND, S., JONES, C. M., DRUNMERY, G. D. andBOUGAS, E.: The D-Xylose absorption test in malabsorption syndromes. New Engl. J.A1el 256, 335, 1957
9. KIMURA, I.: ~tudies on sideroblasts. Okayama Igakkai Zasshi 69, 1773, 1957 (in Japanese)10. CHANARIN, I. and BENNETT, M. C.: A spectrophotometric method for estimating formi
minoglutamic and urocanic acid. Brit. A1ed. J. 1, 27, 196211. CHANARIN, I., MOLLIN, D. L. and ANDERSON, B. B.: The clearance from the plasma of
folic acid injected intravenously in normal subjects and patients with megaloblasticanaemia. Brit. J. Haemat. 4, 435, 1958
12. HERBERT, V.: A palatable diet for producing experimental folate deficiency in man.Amer. J. Glin. Nutr. 12, 17, 1963
13. TAGUCHI, H., HARA, K. and SANADA, H.: Folic acid contents of various foods. Vitamin
42, 338, 1970 (In Japanese)14. WAXMAN, S., CNRCINO,J.J. and HERBERT, V.: Drugs toxins and dietary amino acids
affecting vitamin BIz or folic acid absorption or utilization. Amer. J. A1ed. 48, 599,1970
15. REYNOLDS, E. H.: Mental effects of anticonvulsants and folic acid metabolism. Brain 91,
197, 196816. SANADA, H. and TAGUCHI, H.: Folic acid deficiency due to anticonvulsant drugs. Vitamin
40, 76, 1969 (In Japanese)17. HAWKINS,C. F. and MEYNELL,M.J.: Macrocytosis and macrocytic anaemia caused by
anticonvulsant drugs. Quart. J. A1ed. N. S. 27, 45, 195818. KLIPSTEIN, F. A.: Subnormal serum folate and macrocytosis associated with anticon
vulsant therapy. Blood 23, 68, 196419. MULPAS,J. S., SPRAY, G. H. and WITTS, L.].: Serum folic acid levels in anticonvulsant
therapy. Brit. A1ed. J. ~, 955, 196620. REYNOLDS, E. H., MILNER, G., MATTHEWS, D. M. and CHANARIN, I.: Anticonvulsant
therapy, megaloblastic haemopoiesis and folic acid metabolism. Quart. J. A1ed. N. S.35, 521, 1966
21. IBBOTSON, R. N., DILENA, B. A. and HORWOOD,]. M.: Studies on deficiency and absorption of folates in patients on anticonvulsant drugs. Australas Ann. A1ed. 16, 144, 1967
22. MILLER, D. R.: Serum folate deficiency in children receiving anticonvulsant therapy.Pediatrics 41, 630, 1968
23. BERLYNE, N., LEVENE, M. and Me GLASHAM, A.: Megaloblastic anaemia following anticonvulsants. Brit. A1ed. J. 1, 1247, 1955
24. HOBSON, Q.J. G., SELWYN, J. G. and MaLLIN, D. L.: Megaloblastic anaemia due tobarbiturates. Lancet 1I 1079, 1956
25. KIDD, P. and MOLLIN, D. L.: Megaloblastic anaemia and vitamin BI2 deficiency afteranticonvulsant therapy. Brit. A1ed. J. 2, 974, 1957
26. NEWMAN, M.J. D. and SUMNER, D. W.: Megaloblastic anemia following the use of primidone. Blood 12, 183, 1957
27. FLEXNER,J. M. and HARTMANN, R. C.: Megaloblastic anemia associated with anticonvulsant drugs. Amer. J. A1ed. 28, 386, 1960
28. IWASAKI,1. and SANADA, H.: Folic acid deficiency. Jap. J. Haemat. 33, 27, 1970 (In
Japanese)29. BUTTERWORTH, C. W.Jr., SANTINI, R.Jr. and FROMMEYER, W. B.Jr.: The pteroylglutamate
13
Taguchi: Clinical and experimental studies on folic acid deficiency due to
Produced by The Berkeley Electronic Press, 1971

550 H. TAGUCHI
components of American diets as determined by chromatographic fractionation. j. Clin.Invest. 42, 1929, 1963
30. CHANARIN,1., ROTHMAN, D., PERRY,j. and STRATFULL, D.: Normal dietary folate, ironand protein intake, with particular reference to pregnancy. Brit. Med. j. 2, 394, 1968
31. ANDERSON, B., BELCHER, E. H., CHA!\ARIN, I. and MOLLlN, D. L: The urinary andfoecal excr.etion of radioactivity after oral doses of 3H-folic acid. Brit. j. Haemat. 6,439, 1960
32. PERRY,j. and CHANARIN,1.: Absorption and utilization of polyglutamyl forms of folatein man. Brit. Med. j. 4, 546, 1968
33. HERBERT, V.: Minimal daily adult folate requirement. Arch. Intern. Med. 110, 649,1962
34. SHEEHY, T. W.: How much folic acid is safe in pernicious anemia? Amer. j. Clin. Nutr.9, 708, 1961
35. HEPNER, G. W.: The absorption of pteroylglutamic (folic) acid in rats. Brit. j. Haemat.16, 241, 1969
36. MEYNELL, M.j.: Megaloblastic anemia in anticonvulsant therapy. Lancet I, 487, 196637. DAHLKE, M. B. and MSRTEN~-RoESLER,E.: Malabsorption of folic acid due to dipheny
lhydantoin. Blood 30, 341, 196738. HARA, K.,TAGUCHI, H., KANBARA, K., YOSHIOKA, H., ARIMORI, S., SANADA, H. and
IWASAKI,1.: A case of megaloblastic anemia induced by pregnancy. jap. j. Clin. Hemat.12, 398, 1971 (In japanese)
39. PANDERS,j. T. and RUPERT, M. S. E.: The effect of temperature on folic acid metabolism.Brit. j. Haemat. 11, 518, 1965
40. ROBERTS, P. D., HOFFBRAND, A. V. and MOLLlN, D. L.: Iron and folate metabolism intuberculosis. Brit. Med. j. 2, 198, 1966
14
Acta Medica Okayama, Vol. 25 [1971], Iss. 5, Art. 4
http://escholarship.lib.okayama-u.ac.jp/amo/vol25/iss5/4