-
8/13/2019 ACS Pearl and Pitfall_handout
1/27
21/05
W. Wiwatworapan MD.
Cardiologist, Maharat Nakorn Ratchasima Hospital
Acute Coronary syndromePearl & Pitfall
Outline STEMI ACC guideline 2013
Management algorithm
Pitfall in STEMI
NSTE-ACS Management algorithm
Pitfall in NSTE-ACS
-
8/13/2019 ACS Pearl and Pitfall_handout
2/27
21/05
STEMI
-
8/13/2019 ACS Pearl and Pitfall_handout
3/27
21/05
SymptomRecognition Call toMedical System ED
Cath LabPreHospital
Delay in Initiation of Reperfusion TherapyIncreasing Loss of
Myocytes
Treatment Delayed is Treatment Denied
Management Guideline
-
8/13/2019 ACS Pearl and Pitfall_handout
4/27
21/05
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
In PCI-capable
center
In non-PCI-capable
center
Primary PCI
FMC-device time
90 min
Transfer for primary PCI
if FMC-device time 120 min
Fibrinolyticwithin 30 minutes
if FMC-device time > 120 min
Urgent transferfor PCI
If fail reperfusion
or reocclusion
Transferfor CAGwithin 3-24 hr
(pharmacoinvasive
strategy)PCI
or CABG
or Medication
DIDO 30 minutes
2013 ACCF/AHA Guideline for the Management of ST-Elevation
Myocardial Infarction
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
-
8/13/2019 ACS Pearl and Pitfall_handout
5/27
21/05
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
In PCI-capable
center
Primary PCI
FMC-device time
90 min
PCI
or CABG
or Medication
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
In non-PCI-capable
center
Fibrinolyticwithin 30 minutesif FMC-device time > 120 min
DIDO 30 minutes
Transfer for primary PCIif FMC-device time 120 min
PCI
or CABG
or Medication
-
8/13/2019 ACS Pearl and Pitfall_handout
6/27
21/05
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
In non-PCI-capable
center
Fibrinolyticwithin 30 minutes
if FMC-device time > 120 min
DIDO 30 minutes
Except
Posterior wall MI
Suspected acute Leftmain stenosis
Fibrinolytic Agents
Anaphylaxis
Should repeat dosewithin 6 months
Need adjunctiveanticoagulant Higher patency rate More
complication
-
8/13/2019 ACS Pearl and Pitfall_handout
7/27
21/05
Fibrinolytic Agents - Contraindications
Adjunctive Antiplatelet to SupportReperfusion With Fibrinolytic
Therapy
!
-
8/13/2019 ACS Pearl and Pitfall_handout
8/27
21/05
Adjunctive Anticoagulant to SupportReperfusion With Fibrinolytic
Therapy
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
In non-PCI-capable
center
Fibrinolyticwithin 30 minutesif FMC-device time > 120 min
Urgent transfer
for PCI
If fail reperfusion
or reocclusion
Transferfor CAG
within 3-24 hr
(pharmacoinvasive
strategy)PCI
or CABG
or Medication
DIDO 30 minutes
-
8/13/2019 ACS Pearl and Pitfall_handout
9/27
21/05
Reperfusion Therapy for STEMI Patients
STEMI who candidate for reperfusion
In PCI-capable
center
In non-PCI-capable
center
Primary PCI
FMC-device time
90 min
Transfer for primary PCI
if FMC-device time 120 min
Fibrinolyticwithin 30 minutes
if FMC-device time > 120 min
Urgent transferfor PCI
If fail reperfusion
or reocclusion
Transferfor CAGwithin 3-24 hr
(pharmacoinvasive
strategy)PCI
or CABG
or Medication
DIDO 30 minutes
< 12-24 hr
Cardiogenic shock
Contraindication for
fibrinolytic
Inconclusive
Loading 2
antiplatelet
Loading 2
antiplatelet
Loading 2
antiplatelet
anticoagulant
Pitfall in STEMI
-
8/13/2019 ACS Pearl and Pitfall_handout
10/27
21/05
Female 50 y, chest pain 1 h
A. Repeat ECGB. Refer for primary PCI
C. Fibrinolytic agent
D. Work up other cause of chest pain
F/U ECG 10 min later
A. Repeat ECG
B. Refer for primary PCI
C. Fibrinolytic agent
D. Work up other cause of chest pain
-
8/13/2019 ACS Pearl and Pitfall_handout
11/27
21/05
Post SK 30 min
Post SK 60 min
At ER
-
8/13/2019 ACS Pearl and Pitfall_handout
12/27
21/05
Post SK 70 min
A. Urgency refer for PCI
B. Refer for CAG in 3-24 hr
C. Optimize medication &
refer next few days
D. Medication only
Pearl & Pitfall In inconclusive ECG
Look for reciprocal change
Serial ECG
Or.. Echocardiogram if you can
-
8/13/2019 ACS Pearl and Pitfall_handout
13/27
-
8/13/2019 ACS Pearl and Pitfall_handout
14/27
21/05
Pearl & Pitfall In Acute inferior wall MI (esp. RV
infarct)
Carefully exam pulse 4 extremities
Consider CXR
Wide mediastinum
Calcium sign
Female 50 y, chest pain 1 hA. Repeat ECG in 10 minutes
B. Repeat ECG with V3R, V4R
C. Repeat ECG with V7-V9
D. Rx as UA/NSTEMI
-
8/13/2019 ACS Pearl and Pitfall_handout
15/27
21/05
Pearl & Pitfall In ACS with suspected Posterior wall MI
Tall R in V1-2 with ST depression
ECG V7-9
EKG .Male 70 y, chest pain 1 h
A. Prinzmetalsangina
B. Acute RV infarct
C. Tako tsubo cardiomyopathy
D. Left main stenosis
-
8/13/2019 ACS Pearl and Pitfall_handout
16/27
21/05
EKG 2
ST elevation in aVR ST elevation greater 0.5 mm in aVR in
NSTEMI with often very significant ST
depression in many leads (8)favors the
diagnosis of occlusion of left main trunk.
The 12 lead ECG in ST elevation myocardial infarction :a
practical approach for clinicians
-
8/13/2019 ACS Pearl and Pitfall_handout
17/27
21/05
Female 50 y, chest pain 1 h
A. Anterior wall MIB. Inferior wall MI
C. Lateral wall MI
D. Not MI
Pearl & Pitfall In other causes of ST elevation (Not MI)
No Dynamic change
No progression to Q wave
Involve > 1 coronary territories
-
8/13/2019 ACS Pearl and Pitfall_handout
18/27
21/05
NSTE-ACS
What should you know aboutNSTE-ACS
Assessment of Likelihood of ACS
Early Hospital care
Early Risk Stratification
Invasive vs. Conservative Strategy
Pharmacotherapy
Long-term secondary prevention
-
8/13/2019 ACS Pearl and Pitfall_handout
19/27
21/05
Likelihood of ACS
ACC/AHA UA/NSTEMI Guideline 2007
High Intermediate Low
Symptoms Chest or left arm
discomfort
reproducing prior
documented angina
Chest or left arm
discomfort
Symptom in absence
of any intermediate
likelihood character
History Know history of CAD > 70 years
Male, DM
Recent Cocaine use
Physical
Examination
Transient MR
Hypotension
Rales
Manifestation of
extracardiac vascular
disease
Chest pain
reproduced by
palpation
ECG ST deviation 1 mm
T wave inversion in
multiple lead
Q wave
ST depression 0.5
1 mm
Normal
Cardiac Biomarkers Positive Normal Normal
Early Hospital CareClass I
Bed rest & Telemetry
Oxygen (maintain saturation > 90%)
Nitrate
Oral Beta-blockers in 1st
24-hours if nocontraindications (IV Beta-blockers class IIa)
ACE-I in 1st24-hours for heart failure ofLVEF < 40% (Class
IIa for all other patients)
Statin
-
8/13/2019 ACS Pearl and Pitfall_handout
20/27
21/05
Early Hospital CareClass III
Nitrates if SBP < 90 mmHg or RV infarction
Nitrates within 24-hrs of Sildenafil or 48-hrs of
Tadalafil use
IR-CCB in absence of Beta-blockers
NSAIDs & COX-2 inhibitors
Early Risk Stratification Rapid clinical determination
Troponin is the preferred biomarker
If normal, repeat biomarker at 6-12 hours
after onset of symptoms
-
8/13/2019 ACS Pearl and Pitfall_handout
21/27
21/05
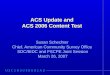
Antman EM, et al. N Engl J Med. 1996;335:1342-1349.
TIMI III B Trial
N=1,404
Troponin I Levels to Predict the Riskof Mortality in ACS
4.78.3
13.2
19.926.2
40.9
0
1020
30
40
50
0/1 2 3 4 5 6/7Number of Risk Factors
14-d Death, MI, or UrgentRevascularization (%) 10 times
Antman EM, et al. JAMA.2000;284:835-842.
TIMI risk score
Age 65 years
3 risk factors for CAD
Prior stenosis > 50%
ST-segment deviation
2 anginal in 24 hours
Use of aspirin in 7 days
cardiac biomarkers
-
8/13/2019 ACS Pearl and Pitfall_handout
22/27
21/05
JAMA 2004;291:2727-33
Management Strategies forNon ST elevation ACS
Definite/Possible ACSInitiate ASA, Beta-blockers, Nitrates, ECG
monitor
Early Invasive Strategy
TIMI Risk Score 3
New ST segment deviation
Positive biomarkersHemodynamic instability
Refractory angina
PCI in past 6 months
CABG
LVEF < 40%
Conservative
TIMI Risk Score < 3
No ST segment deviation
Negative biomarkers
Recurrent symptoms
Heart failure
Serious arrhythmia
Stable
Assessment of EF
Stress TestCoronary angiography
LVEF < 40%Stress test +ve
-
8/13/2019 ACS Pearl and Pitfall_handout
23/27
21/05
Antithrombotic in ACSAt least
2 Antiplatelet
1 Anticoagulant
Antiplatelet (At least 2)Clopidogrel Prasugrel Ticagrelor
Conservative X PCI Thrombolytic X XDose OD OD b.i.dVariability
of
Response
++ + +Risk of Bleeding + ++ +Genotyping CYP 2C19 Not establish
Not establishTransition toelective Sx 5 d 7 d 3-5 dAntiplatelet
effect Slowwer Faster Faster
ASA +
-
8/13/2019 ACS Pearl and Pitfall_handout
24/27
21/05
Anticoagulant (Indirect)Heparin LMWH Fondaparinux
Molecular Wt 15,000 5,000 1,728Target Xa and IIa Xa > IIa
XaBioavailability 30% 90% 100%(hr) 1 4 17Renal excretion No Yes
YesAntidote Complete Partial NoHIT
-
8/13/2019 ACS Pearl and Pitfall_handout
25/27
21/05
Early Invasive Strategy
Initiate Anticoagulant (I A)
UFH (I A)
Enoxaparin (I A)
Bivalirudin (I B)
Fondaparinux* (I B)
Clopidrogrel (I A)
Prasugrel (I B)
Ticagrelor (I B)
IV GP IIb/IIIa inh (I A)
ASA (I A)
Clopidogrel if ASA intolerant (I B)
UFH if CAG
Bleeding ?
Should not switch from
UFH
Clopidogrel + GP IIb/IIIa
inh (IIa) : Favor if
Delay CAG
High risk feature
MACEBleeding
Use in PCI case only
NSTE-ACS
ASA intolerantClopidogrel 75 mg OD
Indefinite Therapy (IIa B)
ASA 75-162 mg OD
Indefinite Therapy (I A)
Medication
Clopidogrel 75 mg OD(I A) or
Ticagrelor 90 mg BID (I B)
At least 1 mo (I A) & up to 12 mo in
the absence of risk of bleeding (I B)
PCI
Clopidogrel 75 mg OD (I A) or
Ticagrelor 90 mg BID(I B) for 12 mo
Continuation > 12 months may be
considered in pt with a high risk of
thrombosis and a low risk of bleeding (IIb C)
Prasugrel 10 mg daily may be
Considered (12 mo) in the absence of :
Increased bleeding risk
Likely to undergo CABG within 7 days
History of stroke or TIA
Age > 75 years
Weight < 60 kg
(Class IIa, Level B) (I B for ACC)
Risk of stent
thrombosis
Canadian Journal of Cardiology 27 (2011) S1S59
ASA 162-325 mg LD(I A)
Clopidogrel 300-
600 mg LD before
or at time of PCI(I B)
Plasugrel at timeof PCI (I B)
-
8/13/2019 ACS Pearl and Pitfall_handout
26/27
21/05
Secondary PreventionClass I Indications
Aspirin
Beta-blockers
ACE-I : CHF, LVEF
-
8/13/2019 ACS Pearl and Pitfall_handout
27/27
21/05
Likelihood of ACS
2 antiplatelet +
1 anticoagulant +
Other medication
Reperfusion
Risk stratification Revascularization
1
2
3
4
5
W. Wiwatworapan MD.
Cardiologist, Maharat Nakorn Ratchasima Hospital
Acute Coronary syndromePearl & Pitfall