Embed Size (px)
Citation preview

ACROMEGALY CASE ACROMEGALY CASE STUDIESSTUDIES
Margaret E Roberts
Acromegaly Specialist Nurse
Christie Hospital Manchester
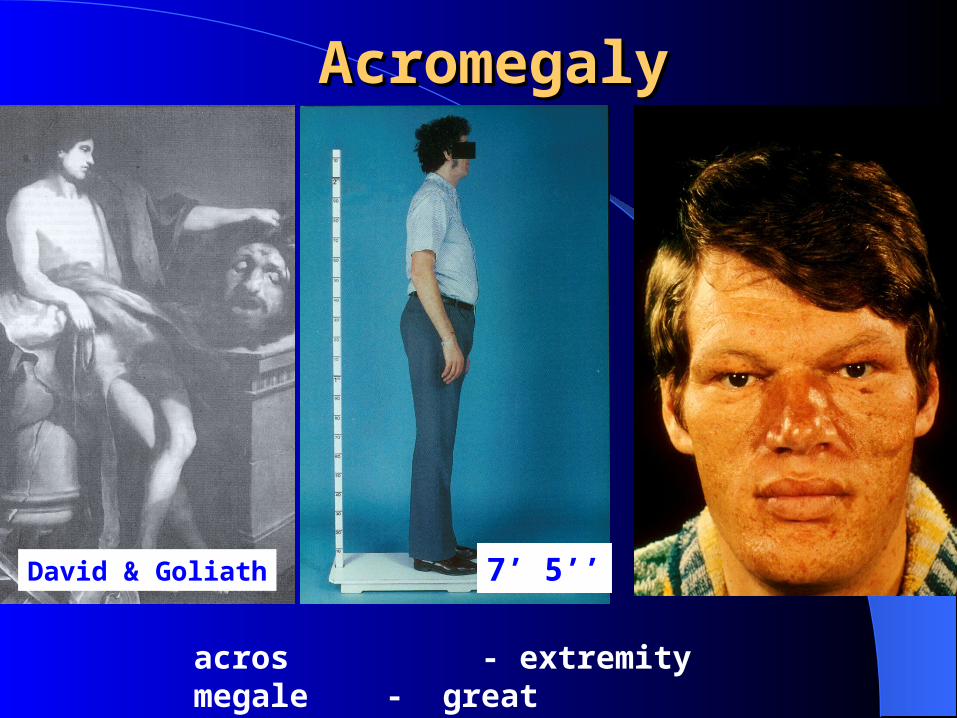
AcromegalyAcromegaly
acros - extremitymegale - great
David & Goliath 7’ 5’’
AcromegalyAcromegaly
Acromegaly is Rare (3 per million per year)
Can be disfiguringLife shortening (average 10 Years)Equally prevalent in both ♂ and ♀ Average age 44 years at diagnosisDelay in diagnosis (8 to 10 years)
CauseCause
Excess of growth hormone Slow growing pituitary tumour (99%) Post puberty Overgrowth soft bone tissue Bone thickening Pre-puberty- gigantism ↑ GH
Hypopituitarism
↓ Testosterone and Oestrogen
Ectopic GHRH McCune-Albright Syndrome
Signs and SymptomsSigns and Symptoms
Enlargement of hands and feetInsidious changes in the faceDeepening of the voiceCoarsening of the skinExcess sweatingHypopituitarism

Signs and SymptomsSigns and Symptoms
Severe headacheSnoringSleep ApnoeaLethargyAches and painsMenstrual cycle disturbance/impotence

Acromegaly Acromegaly “spade-like”“spade-like” hands hands


AcromegalyAcromegalyCo-morbiditiesCo-morbidities
Hypertensionand heart disease
Cerebrovascular eventsand headache
Sleep apnea 50%
Arthritisirreversible
Insulin-resistantdiabetes
40% DM or Glucose
in tolerance

AcromegalyAcromegalyCo-morbiditiesCo-morbidities
Hypertensionand heart disease
Cerebrovascular eventsand headache
Sleep apnea
Arthritis
Insulin-resistantdiabetes
Direct tumour effects
visual problems
compression
hypopituitarism
TreatmentTreatment
SurgeryRadiotherapy (not widely used)Stereotactic Gamma KnifeDopamine Agonists ( Cabergoline)Somatastatin Analogue (Octreotide LAR,
Lanreotide Autogel)GH receptor Antagonist (Pegvisomant)

Objectives of treatmentObjectives of treatment
Reverse the symptoms and signs of acromegaly
Restore circulating GH (<2.5 µg/l) and Insulin-like growth factor (IGF-1) levels to normal
Restore normal life expectancy
Remove the pituitary tumour and preserve residual pituitary function
Prevent recurrence
Case StudyCase Study
Summary18 year old Iady Height 180.5cm (5ft 11½in)diagnosed 2006Acromegaly with hyperprolactinemia

History History
From 6 years age taller than friendsSlept for long periods up to 20hrs at a
time.Headaches and tirednessPins and Needles in arms and handsMum thought depressed and alcoholic
16 years went to GP referred to local hospital
Diagnosed acromegaly commenced cabergoline.
Commenced Menstrual Periods

12 months later referred to Hope Hospital.
Endocrine blood screenBasal pituitary functionIGF-IGHDCOGTT
MRIscan

Assessment (on cabergoline)Assessment (on cabergoline)
GHDC mean 14.92mU/LIGF-I 109 nmol/L (ref range 21.2-
75.9nmol/L) Prolactin 129 mU/L (ref range 50-400)Non-suppression of GH during OGTTMRI scan macroadenomaComfirmed
Acromegaly with Hyperprolactinemia
.2006 referred for surgery had 2
transsphenoidal operations not cured.
Had octreotide LAR injections not controlled.
2007 referred to Christie Hospital for further opinion.
Assessment (off cabergoline)Assessment (off cabergoline)
Prolactin 1810mU/L (ref range 50-400)IGF-I 790 mg/l (ref range 151-528)
Persistent AcromegalyThyroid and Cortisol DeficientDiabetes insipidusMenstrual Periods stopped

MedicationMedication
Thyroxine 75mcgs dailyHydrocortisone 10/5/5mgsOmeprazoleDesmopressin sprayCabergoline

Cabergoline effective in 30% patients Prolactin and GH co-secreting
tumours respond well to dopamine agonist
─ biochemical response
─ tumour shrinkage Non responsive to somatostatin
analogues

Prolactin responds, better than Growth hormone to dopamine agonists.
Cabergoline effect on heart no evidence in Acromegaly patients
Dopamine agonist → ORAL → CHEAP
In this patient Cabergoline had a much more dramatic effect.
She now feels very well on 3.5mgs Cabergoline weekly

I would like to thank
Dr Claire Higham for all her help.