Embed Size (px)
Citation preview
Breast MRI: What’s New in BI-RADS™, 5th Edition�
Orange County Radiological Society
September 13, 2014
Debra M. Ikeda, M.D. Director of Breast Imaging
Professor of Radiology Stanford University, Stanford, CA
Image courtesy of Bruce L. Daniel, M.D.
• Images courtesy of American College of Radiology ACR BI-RADS MRI, in American College of Radiology BI-RADS Imaging Atlas, Reston, VA, 2003, ACR Breast MRI Lexicon Committee, Elizabeth Morris, Constance Lehman and Bruce L. Daniel, M.D.
ACR Breast MRI Accreditation and
Breast MRI BI-RADS® 2013 Personnel Initial and Continuing
Qualifications Equipment Clinical Images QA and QC Progam MRI Safety Guidance
ACR MRI Accreditation ACR Breast MRI Accreditation Program - Background Medicare Improvement for Patients and Providers Act of 2008(MIPPA)(not hospitals) – requires all providers billing for the MRI, CT, NM,PET technical component of part B of the Medicare Physician Fee Schedule to be accredited by January 1, 2012 to bill for Medicare beneficiaries No reimbursement if no accreditation CMS approval for ACR, IAC, JCHO
ACR Breast MRI Accreditation
http://www.acr.org/Quality-Safety/Accreditation/BreastMRI
Phone 800-227-6440 Email: [email protected] http://www.acr.org Updated June 19, 2014 – New system
allows electonic image submission
BREAST MRI ACCREDITATION http://www.acr.org/Quality-Safety/
Accreditation/BreastMRI FAQs Accreditation takes 4-5 months No survey but MIPPA facilities must
pariticpate in unannounced validation surveys by accrediting organization and/or Cneters for Medicare and Medicai Services (CMS)
ACR Breast MRI Accreditation program Clinical Image Review Clinical Image Review
Examination identification Pulse sequence and image contrast
Positioning and anatomic coverage Artifacts Spatial resolution Temporal resolution
ACR Breast MRI Accreditation program Clinical Image Review- Examination identification Patient’s first and last names Patient age or date of birth Patient Identification number Facility name Examination date *Laterality, left or right of midline section If laterality is absent or is incorrect, the case will fail accreditation. -
ACR Breast MRI Accreditation program – 4 Sequences T2-weighted/bright fluid series Three Multi-phase T1-weighted series all with matching technical factors 1) Precontrast T1 2) Early phase post contrast T1 –
completed within 4 minutes of injection
3) Delayed phase post contrast T1
2014 BI-RADS™ Mammography, Ultrasound and MRI Lexicon Expert concensus on Terms New information from literature since 2004 incorporated
with hyperlinks to literature Terms harmonize between the Lexicons US Lexicon includes 3D images, doppler, elastography MRI new images and implant chapter
2014 BI-RADS™ 5th Edition MRI REPORT FORMAT 1) Clinical History and Indication 2) Comparison to Previous Examinations 3) Acquisition Reporting (see http://www.acr.org/-/
media/ACR/Documents/Accreditation/Breast MRI/Requirements.pdf)
4) Overall Breast Composition and Background Parenchymal Enhancement (BPE)
5) Clear description of Important Findings (Moprhology) 6) Kinetic Curve Assessment 7) Final Overall Assessment 8) Management
2014 ACR BI-RADS™ MRI Reporting
Size and Location Mass or NME type and modifiers (shape margin density) Associated Findings How changed; if previously present Summary and BI-RADS™ Code (0-6) Management Use combined reporting (MRI/Mammmo/US)

Breast Lesion Locations Right or Left Breast Quadrant Clock position Depth in the breast - anterior, middle or posterior third Distance in cm from the nipple, skin, chest wall
*2013 ACR Breast Imaging Reporting and Data System, Reston, VA.
Combined Reporting Make a final BIRADS Assessment 0 - Incomplete Additional Imaging Needed 1 - Negative (routine f/u) 2 - Benign (routine f/u) 3 - Probably Benign - Short Interval Follow-up
( <2% cancer)
1 month f/u for hormones 6 month f/u NOT background enhancement
ACR MRI Lexicon 2nd Edition
Combined Reporting BIRADS Assessment 4 - Suspicious Tissue diagnosis “Biopsy should be performed in
the absence of clinical contraindication” Recommend Bx and How Guided, by US, Mammo, MRI
5 - Highly Suggestive of Malignancy - Tissue diagnosis “Biopsy should be performed in
the absence of clinical contraindication” 6 - Known Biopsy Proven Malignancy - Surgical excision when clinically appropriate MRI Lexicon 2nd Edition, ACR MRI Accreditation
Program
Important
Assessment is based on imaging findings OK to add additional sentence suggesting
biopsy based on clinical findings even if exam is BI-RADS® 1 or 2
16�
Slide courtesy ACR www.acr.org �
2014 BIRADS Reporting Cut-offs for BIRADS 4 4a = 2%-10% 4b = 11%-50%
4c = 51-95%) BIRADS Assessment and Management
are separated to treat the patient, not the BIRADS code
ACR BI-RADS™ MRI LEXICON ACR Subcommittee on BI-RADS MRI American College of Radiology 1891 Preston White Drive Reston, VA 20191 FAX: 703-648-9176 Email: [email protected] Elizabeth A. Morris, M.D., Chair, Subcomimittee on BI-
RADS MRI

American College of Radiology (ACR) ACR BI-RADS™ MRI LEXICON
New Web-based format (hardcopy on demand) Mammo/US/MRI compatibility Evidence based information with hyperlinks to
references
BI-RADS™ MRI Lexicon Changes New Quality Assessment Section Includes
Technical Parameters and Kinetic/Functional Considerations – influence images; standardization results in consistent architecture & kinetic reporting
BI-RADS™ MRI Lexicon Changes Morphology and kinetics are still both
important, add T2 weighted non-con Terms added (BPE) or deleted as better
terms identified, other terms clarified New Section on Non-enhancing Findings New Implant Section Clarify BIRADS 0 and BIRADS 3 Need for Combined Reporting
Kinetic Description (Unchanged)
Initial slope within 2 minutes or when curve starts to change. Delayed slope after 2 minutes or after curve starts to change
SI
Initial Delayed persistent
plateau
washout
fast
medium
slow
Kinetic Description: Signal Intensity/Time Intensity Curve
Persistent - 6% cancer Plateau - 64% cancer
Washout - 87% cancer Sensitivity 91% Specificity 83%
PPV 77% Kuhl et al. Radiology 1999
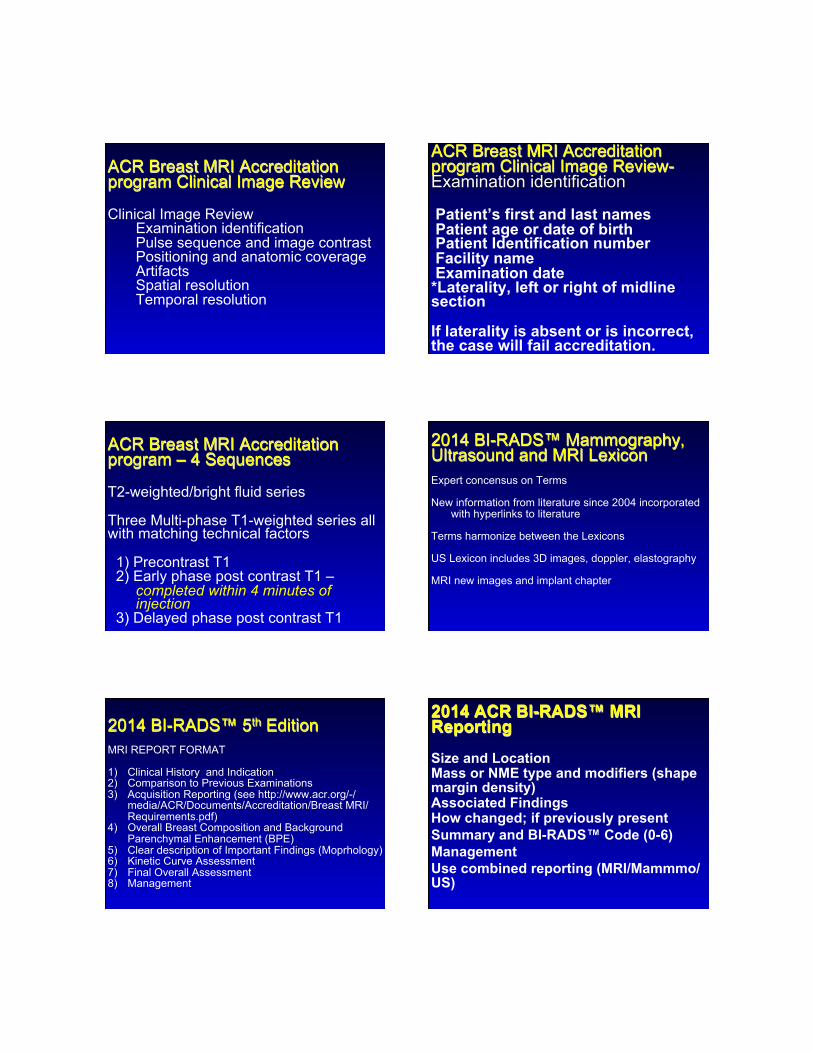
BI-RADS™ MRI Lexicon- Kinetics Initial phase – enhancement pattern in the first 2 minutes or when the curve starts to change Initial Slow – increase of <50% Initial Medium – increase of 50-100% Initial Fast/rapid - >100% increase
BI-RADS™ MRI Lexicon- Kinetics Delayed phase – enhancement pattern after 2 minutes or when the curve starts to change Persistent – continued > 10% increase Plateau – SI does not change after initial
rise, flat Washout – SI decreases >10% after rise
Breast MRI BI-RADS® 2013 Contrast Bolus w saline flush Contrast dose based on weight (Use a power injector) Timing so first post contrast scan is at 90
seconds to 2 minutes after injection, center of scan is ½ way through peak contrast
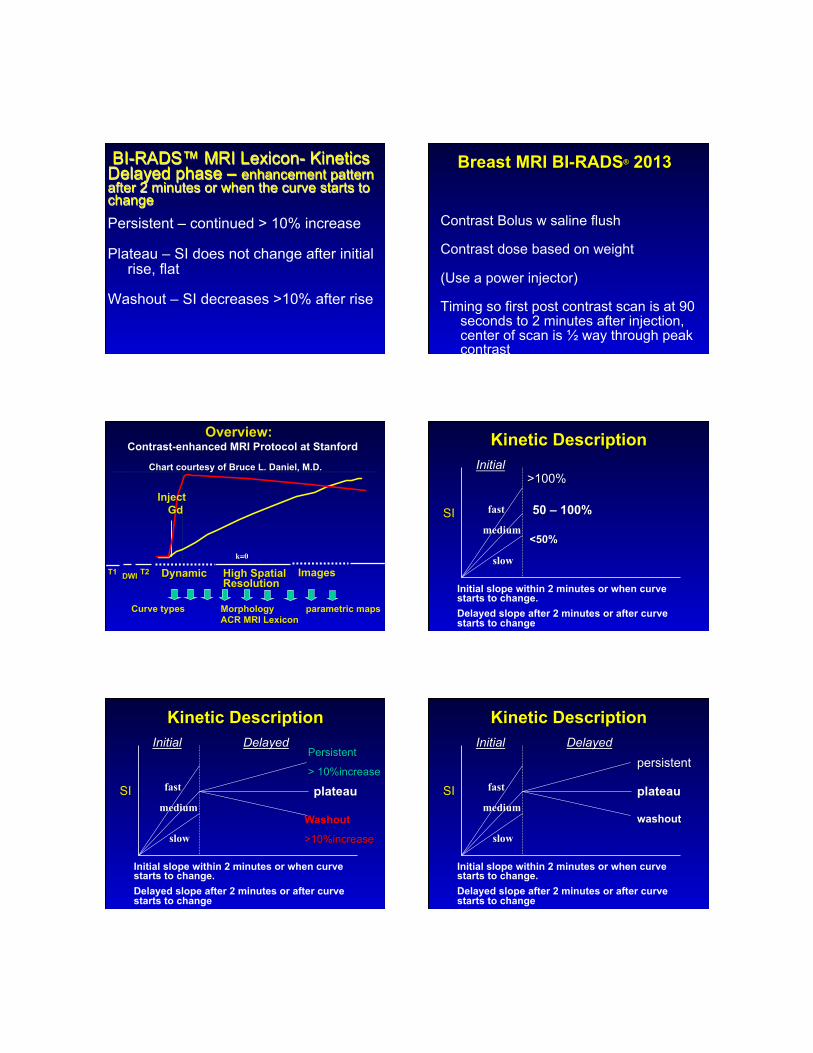
Dynamic Images High Spatial Resolution
k=0
Overview: Contrast-enhanced MRI Protocol at Stanford
T1 DWI
Inject Gd
T2
Curve types Morphology ACR MRI Lexicon
parametric maps
Chart courtesy of Bruce L. Daniel, M.D.
Kinetic Description
Initial slope within 2 minutes or when curve starts to change. Delayed slope after 2 minutes or after curve starts to change
SI
Initial >100%
50 – 100%
<50%
fast
medium
slow
Kinetic Description
Initial slope within 2 minutes or when curve starts to change. Delayed slope after 2 minutes or after curve starts to change
SI
Initial Delayed Persistent
> 10%increase
plateau
Washout
>10%increase
fast
medium
slow
Kinetic Description
Initial slope within 2 minutes or when curve starts to change. Delayed slope after 2 minutes or after curve starts to change
SI
Initial Delayed persistent
plateau
washout
fast
medium
slow

BI-RADS™ MRI Lexicon Changes Literature on morphology and dynamic curve
interpretation for benign and malignant lesions advanced (2004)
Variations on MRI technique influence what is observed and reported
New Quality Assessment Section Includes Technical Parameters and Kinetic/Functional Considerations – influence images; standardization results in consistent architecture & kinetic reporting
BI-RADS™ MRI Lexicon Changes Morphology and kinetics are still both
important, add T2 weighted non-con Terms added (BPE) or deleted as better
terms identified, other terms clarified New Section on Non-enhancing Findings New Implant Section Clarify BIRADS 0 and BIRADS 3 Need for Combined Reporting
ALMOST ENTIRELY FAT SCATTERED FIBROGLANDULAR TISSUE HETEROGENEOUS FIBROGLANDULAR TISSUE EXTREME FIBROGLANDULAR TISSUE
*2013 ACR BIRADS Breast Imaging Reporting and Data System, Reston, VA. Released 2/2014 .
A) Amount of Fibroglandular Tissue (FGT)– ON MRI -
B) Normal “background” parenchymal enhancement (BPE)
percentage of normal enhancing fibroglandular tissue
background dependent on breast density (% fibroglandular tissue by volume)
Background Parenchymal Enhancement (BPE)
ENHANCEMENT SYMMETRIC None ASYMMETRIC
Minimal Mild Moderate*
Marked* *Moderate and Marked Background Enhancement can hide invasive cancer noninvasive cancer
*2013 ACR BIRADS Breast Imaging Reporting and Data System, Reston, VA. Released 2/2014
C. NON-MASS LIKE ENHANCEMENT: now NME Diffuse enhancement: Now marked BPE
Image # NH5
DIFFUSE enhancement.

C. NON-MASS LIKE ENHANCEMENT: now NME Multiple Regions: Now moderate BPE
Image # 012
MULTIPLE REGIONS of heterogeneous enhancement. Fibrocystic change.
C. NON-MASS LIKE ENHANCEMENT: now NME Diffuse enhancement: Now mild BPE
Image # 005
DIFFUSE stippled enhancement. Fibrocystic changes.
Normal Background Parenchymal Enhancement (BPE) Previously all enhancement was thought
to be abnormal Normal breast parenchyma enhances
and fluctuates with hormonal cycles or exogenous hormones
2003 2001
2005 2004
Image courtesy Aya Kamaya, M.D.
None/Minimal BPE
Minimal BPE (in scattered breast )

MILD BPE (in scattered breast) Moderate BPE (in hetero/dense breast)
Marked BPE (in dense breast) Findings that are NOT “background enhancement”
DCIS - in appropriate clinical setting focal area linear linear branching (historic ductal) segmental asymmetric
- especially if in setting of known cancer
or if “clumped”
MRI Enhancement in Stromal Tissue Surrounding Breast Tumors: Association with Recurrence Free Survival following
Neoadjuvant Chemotherapy
Jones, E.F., et al. PLoS One, 2013. 8(5): p. e61969.
Fifty patients with locally-advanced breast cancer were imaged with dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) before (V1) and after one cycle (V2) of adriamycin-cytoxan therapy.�
Results: The mixed effects model displayed a decreasing radial trend in PE at both V1 and V2. An increasing trend was less pronounced in SER. Survival analysis showed that the hazard ratio estimates for each unit decrease in global SER was statistically significant at V1 [estimated hazard ratio = 0.058, 95% Wald CI (0.003, 1.01), likelihood ratio p = 0.03]; but was not so for V2.�
MRI Enhancement in Stromal Tissue Surrounding Breast Tumors�
Jones, E.F., et al. PLoS One, 2013. �

Conclusions: stromal tissue outside the tumor can be quantitatively characterized by DCE-MRI, and stromal enhancement measurements may be further developed for use as a potential predictor of recurrence/disease-free survival following therapy.�
MRI Enhancement in Stromal Tissue Surrounding Breast Tumors�
Jones, E.F., et al. PLoS One, 2013. �
MRI Findings (> BPE) Focus
Mass Shape – Oval/Round/Irregular Margin – Circumscribed Not circumscribed : Irregular/Spiculated Internal Enhancement Homogeneous/Heterogeneous Rim
Dark Internal Septations ACR BIRADS Breast MRI Lexicon Update
MASS DESCRIPTORS MARGIN SHAPE
Circumscribed
Not Circumscribed
Irregular
Spiculated
Homogeneous
Heterogeneous
Rim
Dark septations
Oval Round
Irregular
INTERNAL ENHANCEMENT
MRI Findings (> BPE) Non-mass Enhancement (NME)
Distribution Internal Enhancement Focus Focal NME Homogeneous Linear Heterogeneous
Segmental Clumped Regional Clustered Ring
Multiple Regions Diffuse ACR BIRADS Breast MRI Lexicon Update
Breast MRI Lexicon
Non-Mass Enhancement NME
Focus Focal NME
Linear
Segmental
Clustered Ring Ducts vs Microcysts

DCIS Clumped non-masslike enhancement in a
ductal, linear, segmental, or regional distribution
14% show no enhancement! Kinetics not helpful
Usually rapid uptake, but can demonstrate persistent, plateau, or washout
Mimics normal breast parenchyma on T1 and T2
Kuhl CK et al. Lancet 2007 Aug 11:370(9586):485-92
DCIS Characteristics
MORPHOLOGY IMPORTANT SEGMENTAL {DUCTAL ENHANCEMENT} LINEAR (FOCAL AREA} FOCAL NME LINEAR CLUMPED (COBBLESTONE)
(BIRADS 2013 think Clustered Ring) PROXIMITY TO IDC KINETICS LESS IMPORTANT- MAY INDICATE
HIGH GRADE DCIS IF PRESENT Kuhl CK et al. Lancet 2007 Aug 11:370(9586):
485-92
Anatomy and Pathology Explain DCIS Appearances Segmental,Regional, Linear
Focal NME
Breast MRI Non-Mass Enhancement Distribution
REGIONAL Enhancement not confined to single duct; may be in multiple ducts
MULTIPLE REGIONS Multiple areas of regional enhancement
DIFFUSE Scattered enhancement throughout the breast
Asymmetric
(Septal -thickened trabeculae)
Associated Features Nipple retraction
Nipple invasion Skin retraction Skin thickening Skin invasion –a) Direct invasion b) Inflammatory cancer Axillary adenopathy Pectoralis muscle invasion Chest wall invasion Architectural distortion *2013 ACR BIRADS Breast Imaging Reporting and Data System, Reston, VA.
Released 2/2014
Fat Containing Lesions Lymph nodes – a) Normal b) Abnormal
Fat necrosis Hamartoma Postoperative seroma/hematoma with fat *2013 ACR BIRADS Breast Imaging Reporting and Data
System, Reston, VA. Released 2/2014

Location of Lesion
Location Depth *2013 ACR BIRADS Breast Imaging Reporting and Data
System, Reston, VA. Released 2/2014
MRI Findings (> BPE) Intramammary Lymph Node
Skin Lesion *2013 ACR BIRADS Breast Imaging Reporting and
Data System, Reston, VA. Released 2/2014
BI-RADS™ MRI Lexicon Changes Morphology and kinetics are still both
important, add T2 weighted non-con Terms added (BPE) or deleted as better
terms identified, other terms clarified New Section on Non-enhancing Findings New Implant Section Clarify BIRADS 0 and BIRADS 3 Need for Combined Reporting
Non-enhancing Findings Ductal high signal on T1W
Cyst –simple and complicated Post-operative fluid collections (Hematoma/seroma) Post-therapy skin thickening and trabecular thickening (w
skin thickening, post XRT, edema) Non-enhancing mass Architectural distortion Signal void from clips, foreign bodies *2013 ACR BIRADS Breast Imaging Reporting and Data
System, Reston, VA. Released 2/2014
BI-RADS™ MRI Lexicon Changes Morphology and kinetics are still both
important, add T2 weighted non-con Terms added (BPE) or deleted as better
terms identified, other terms clarified New Section on Non-enhancing Findings New Implant Section Clarify BIRADS 0 and BIRADS 3 Need for Combined Reporting
IMPLANTS IMPLANT TYPE – Saline, silicone, other LOCATION – subpectoral, subglandular INTACT – radial folds INTRACAPSULAR FINDINGS –
keyhole (teardrop, noose) subcapsular line linguine
EXTRACAPSULAR RUPTURE Abnormal Implant Contour – focal bulge, Globular Water Droplets, Peri-implant fluid

IMPLANTS Implant Material and Type– Saline, silicone (intact or
ruptured), other material, lumen type Implant Location – Retroglandular, Retropectoral Abnormal Implant Contour – Focal Bulge Intracapsular Silicone Findings– Radial folds,
subcapsular line, keyhole sign (teardrop, noose), linguine sign
Extracapsular silicone – Breast, Lymph Nodes Water Droplets Peri-implant fluid
BI-RADS™ MRI Lexicon Changes Morphology and kinetics are still both
important, add T2 weighted non-con Terms added (BPE) or deleted as better
terms identified, other terms clarified New Section on Non-enhancing Findings New Implant Section Clarify BIRADS 0 and BIRADS 3 Need for Combined Reporting
BIRADS 0 - Additional Imaging Needed
USED ONLY TO STOP A BIOPSY - mammo or US to confirm a benign lymph node that would otherwise undergo MRI biopsy
- US for fibroadenoma
ACR BIRADS Breast MRI Lexicon 2nd Edition, 2013
BIRADS 3
BACKGROUND PARENCHYMAL ENHANCEMENT
Should NOT fall into this category except for 1 month follow-up for hormones
Usually 6-month follow up for benign findings
Few studies on BIRADS 3 for follow up or showing < 2% malignancy (Marshall et al 2012)
Descriptors adapted from Mammography BI-RADS for
uniformity ACR BIRADS Breast MRI Lexicon 2nd Edition 2013
BI-RADS™ MRI Lexicon Changes Morphology and kinetics are still both
important, add T2 weighted non-con Terms added (BPE) or deleted as better
terms identified, other terms clarified New Section on Non-enhancing Findings New Implant Section Clarify BIRADS 0 and BIRADS 3 Need for Combined Reporting
Multifocal Disease (2)
calcs 4 cm from nipple 1.4 cm from nipple
3 cm from nipple

Thank You!













![QuantifyingTumorVascularHeterogeneitywithDynamic Contrast ... · 2015. 7. 29. · ACR Breast Imaging-Reporting and Data System (BI-RADS) MRI lexicon [18]. In cancer treatment, tumor](https://img.dokumen.tips/doc/110x75/5fc9df59a8ef470c23133cae/quantifyingtumorvascularheterogeneitywithdynamic-contrast-2015-7-29-acr.jpg)















