Embed Size (px)
Citation preview

LYNN BAHTA , RN, PHNMINNESOTA DEPARTMENT OF HEALTH
SEPTEMBER 2011
ACIP Update: June 2011 Meeting

Recommendations Addressed
Zoster vaccine Meningococcal conjugate vaccine Pertussis Influenza
Zoster Vaccine
Expanded licensure for use in persons age 50 through 59 years
CDC workgroup made the decision to not provide a recommendation for vaccination Supply – No stable annual supply since licensure, competition with those at higher risk
Duration of immunity – unknown, concern of loss of protection at time most needed
Cost effectiveness issues – least cost effective at youngest (lower disease incidence) and oldest ages (lower VE)

Zoster FYI
Concomitant use of Zoster vaccine with PPSV Lower Zoster GMT when given together Clinical significance Kaiser Permanente studies – show no increased incidence of zoster disease when zoster vaccine given with PPSV
No change in recommendations If both are indicated, give both at the same visit
Meningococcal conjugate vaccine
Menactra (MCV4D) received FDA licensure to expand to ages 9 through 23 months
Licensed for a 2‐dose primary series ACIP focused on specific groups with medical conditions or exposure risks Keep it similar to the recommendations for 2 through 10 year‐olds at increased risk for meningococcal disease
This focus applies to less than 5000 persons annually
MCV4D Recommendation
At age 9 months, give a 2‐dose primary series of MCV4Dto: Infants with complement component deficiencies C3, C5‐C9, properdin, factor H, factor D
Infants who are in defined risk group for a community or institutional outbreak
Infants traveling to an area where meningococcal disease is epidemic or highly endemic
NOT included – infants with functional or anatomic asplenia – they should continue to receive MCV4 at age 2 years
MCV4D Recommendation
Separate doses by three months Children vaccinated for travel: give 2nd dose 2 months later
Children who remain at risk: Give a booster 3 years after primary series
Other consideration: Concomitant use with PCV7 showed reduced response to serotypes 4, 6b, and 18c (no data on PCV13)Clinical relevance unknown but workgroup concerned about impact to children with sickle cell anemia and asplenia
Proposal to separate these vaccines by 1 month is being considered

Pertussis Vaccination of Pregnant Women
Safety of Tdap on mother and fetus Td and TT used extensively in the past without adverse event Limited data should similar profile for Tdap Vaccination after 20 weeks gestation recommended to minimize perception of risk to fetus
Cost of maternal Tdap vaccination program Same cost as post natal vaccination program

Pertussis Vaccination of Pregnant Women
Effect of maternal vaccination on infant immune response to primary DTaP Concern that maternal vaccination may interfere with infant’s active antibody production following primary DTaPHowever, may be protective in first months of life – data not available to support this
Degree of interference to infant’s immune response not yet known but short lived
Clinical importance not clear When looking at pertussis mortality in infants, benefits of protection outweigh risk of less protection later in infancy

CDC, ACIP Meeting, June 2011
Tdap in Pregnancy Recommendation
Give Tdap to all women who have not previously received Tdap and all women who are due for a Td booster Preferably in late second* or third trimester
Reinforced need to give Tdap to all persons who have not previously received Tdap and that will have close contact to newborn Ideally, at least two weeks prior to first encounter
*After 20 weeks gestation

Pregnancy and Other Situations
Pregnancy and Wound Management: As part of standard wound management, if a Td booster is recommended for a pregnant woman who has previously not received Tdap, health care providers should administer Tdap
No history of primary series or unknown history: The recommended schedule is 0, 4 weeks, and 6‐12 months. Tdap should replace 1 dose of Td, preferably during the third or late second trimester* of pregnancy.
*After 20 weeks gestation

Influenza: Egg Allergy
Most persons with an egg allergy may be able to receive influenza vaccination In particular, persons who can eat lightly cooked eggs (e.g., scrambled) can be vaccinated
Studies show that when the ovalbumin content of the vaccine was known, up to 0.7 µg per dose was tolerated without serious reactions; however, the upper level in which no anaphylaxis would occur is unknown. Ovalbumin concentration can vary from season to season and from lot to lot for a given vaccine.
Vaccine with an ovalbumin content ≤0.6 mcg/dose should be used
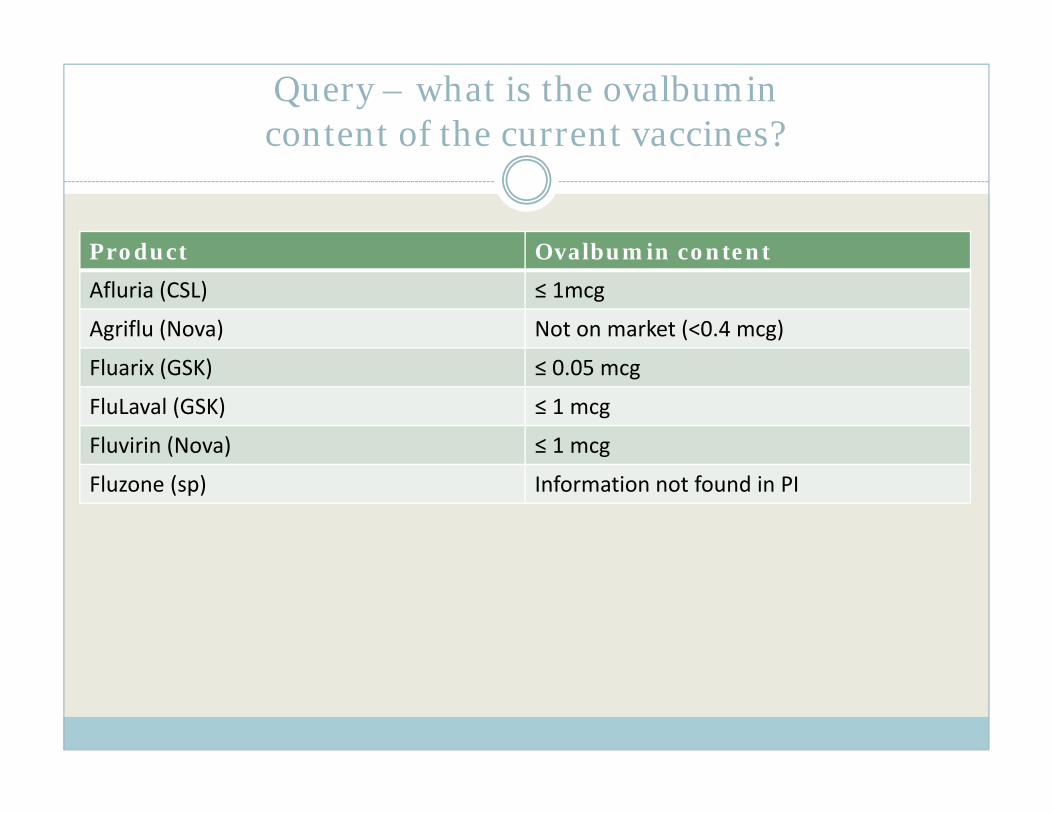
Query – what is the ovalbumin content of the current vaccines?
Product Ovalbumin content
Afluria (CSL) ≤ 1mcg
Agriflu (Nova) Not on market (<0.4 mcg)
Fluarix (GSK) ≤ 0.05 mcg
FluLaval (GSK) ≤ 1 mcg
Fluvirin (Nova) ≤ 1 mcg
Fluzone (sp) Information not found in PI

Algorithm for evaluating egg allergy
Table 2. CDC. Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR, August 26, 2011; 60[33].

Recommendations Regarding Persons with Egg Allergy: CAVEATS
Each of the following recommendations applies when considering influenza vaccination of persons who have or report a history of egg allergy.
1. Persons who have experienced only hives following exposure to egg should receive influenza vaccine with the following additional measures (Figure 2):
a) Because studies published to date involved use of TIV, TIV rather than LAIV should be used. b) Vaccine should be administered by a health‐care provider who is familiar with the potential manifestations of egg allergy. c) Vaccine recipients should be observed for at least 30 minutes for signs of a reaction following administration of each vaccine
dose. Other measures, such as dividing and administering the vaccine by a two‐step approach and skin testing with vaccine, are not
necessary. 2. Persons who report having had reactions to egg involving angioedema, respiratory distress, lightheadedness, or recurrent
emesis, or persons who required epinephrine or other emergency medical intervention, particularly those that occurred immediately or within minutes to hours after egg exposure are more likely to have a serious systemic or anaphylactic reactionupon reexposure to egg proteins. Before receipt of vaccine, such persons should be referred to a physician with expertise in the management of allergic conditions for further risk assessment (Figure 2).
3. All vaccines should be administered in settings in which personnel and equipment for rapid recognition and treatment of anaphylaxis are available. ACIP recommends that all vaccination providers be familiar with the office emergency plan (18).
4. Some persons who report allergy to egg might not be egg allergic. Those who are able to eat lightly cooked egg (e.g., scrambled eggs) without reaction are unlikely to be allergic. Conversely, egg‐allergic persons might tolerate egg in baked products (e.g.,bread or cake); tolerance to egg‐containing foods does not exclude the possibility of egg allergy (35). Egg allergy can be confirmed by a consistent medical history of adverse reactions to eggs and egg‐containing foods, plus skin and/or blood testing for immunoglobulin E antibodies to egg proteins.
5. A previous severe allergic reaction to influenza vaccine, regardless of the component suspected to be responsible for the reaction, is a contraindication to receipt of influenza vaccine.
CDC. Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR, August 26, 2011; 60[33].

Key Considerations
Recommendations only apply to TIV Person who report only hives: Vaccination should be conducted in a setting in which the provider is familiar with egg allergy reactions
Observe for 30 minutes following vaccination Skin testing and partial doses are not necessary Personnel should be trained and equipment available in the event of an anaphylactic reaction
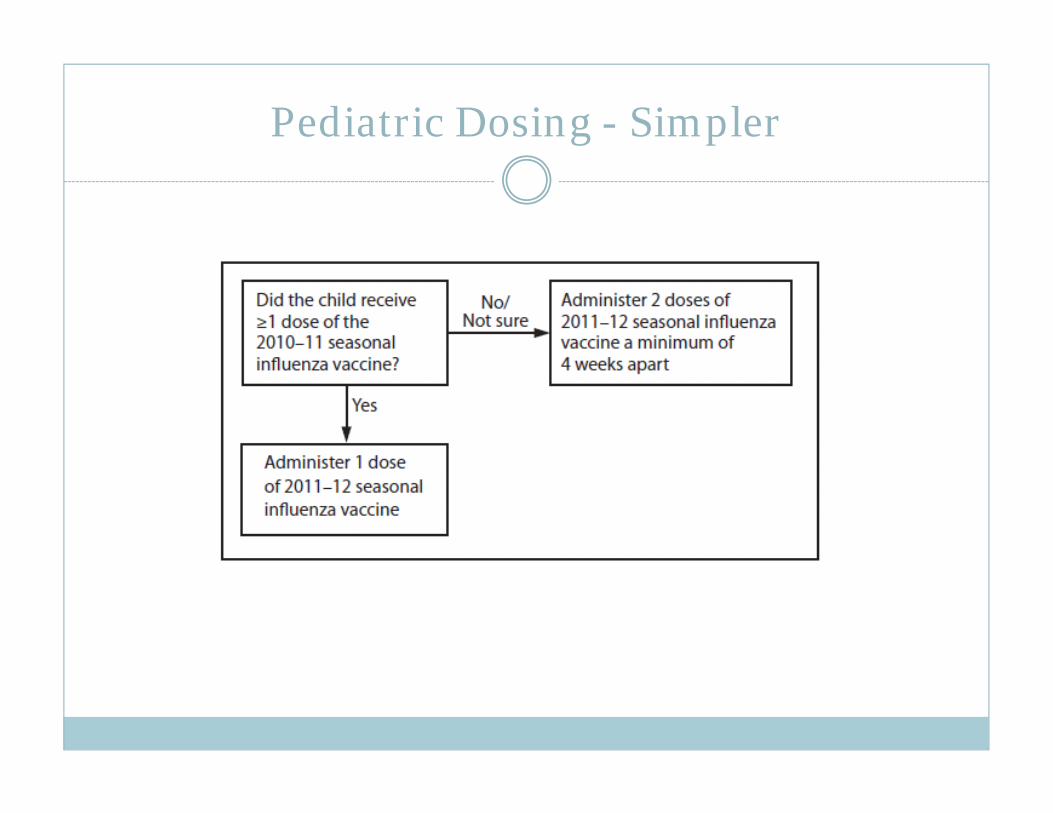
Pediatric Dosing - Simpler

Influenza and Febrile Seizures: Update
Increased risk of febrile seizures on days 0‐1 post‐vaccination among 6‐59 month old children who received 1st dose TIV plus PCV13 Highest incidence in 12‐23 month old infants DTaP often also co‐administered, however febrile seizure with TIV/DTaP‐only co‐administration not previously identified
2010 was first season for PCV13, pattern not detected for PCV7 Attributable risk:
42 (95% CI 3,81) per 100,000* (original assessment was 61/100,000)
1 per 2,375 vaccinees

Issues considered
Children with influenza also risk febrile seizures Burden of influenza in young children great Burden of invasive pneumococcal disease in young children increased
Delay of vaccination to prevent a febrile seizure must be weighed against the risk of disease due to non vaccination
No decision to delay vaccination of either vaccine Providers should discuss this with parents Talking points now up on web
New Influenza Product
Fluzone Intradermal, licensed May 2011 Distribution somewhat limited for 2011‐12 season Indicated for persons age 18 through 64 years Pre‐filled microinjection syringe Efficacy data not available
No preference given by ACIP










![Approved aCIP FFC 13 April 2018[1] - Florence City Schools · Report Summary 21 2018-2019 ACIP Assurances. Introduction 23 ACIP Assurances 24 ... FFC has several safety nets directed](https://img.dokumen.tips/doc/110x75/5f11b173c1f6c83e44789be8/approved-acip-ffc-13-april-20181-florence-city-schools-report-summary-21-2018-2019.jpg)


















