Embed Size (px)
Citation preview

CANCER BIOTHERAPY & RADIOPHARMACEUTICALSVolume 18, Number 1, 2003© Mary Ann Liebert, Inc.
Accuracy of the Quantification of Organ Activityfrom Planar Gamma Camera Images
Kristina Norrgren Ph.D., Sigrid Leide Svegborn Ph.D., Johan Areberg Ph.D., Sören Mattsson Ph.D.Department of Radiation Physics, Malmö University Hospital, SE-205 02 Malmö, Sweden
ABSTRACT
The accuracy in determination of organ activity of 99mTc was investigated, with activity estimated from gammacamera images of phantoms, using the conjugate view method. The accuracy depends on several parameterssuch as the choice of background correction method, the accuracy in determination of the effective attenua-tion coefficient and the thickness of the body and organs and on the determination of the gamma camera sen-sitivity. The background correction method has a major influence on the quantification of the activity. Meth-ods which take the volume of the source organ into consideration are recommended. The discrepancy in thedetermined organ activity varied between an underestimation of 26% and an overestimation of 16% in theMIRD phantom, depending on which organ was studied and on the correction method used. To correct forabsorption and scattering, an effective attenuation coefficient was used. A theoretical analysis showed that achange in the effective attenuation coefficient of 0.01 cm21 resulted in a 15% change in the calculated ac-tivity. Also the thickness of the body and the organ of interest influences the calculated activity. A 2 cm de-viation in the body thickness causes a deviation of approximately 10% in the calculated activity. The quan-tification is improved if the attenuation coefficient is determined by transmission measurements.
125
INTRODUCTION
Radiation risk estimates and optimal use of var-ious radiodiagnostic techniques require accuratedosimetry for representative groups of patients.The increasing use of radiopharmaceuticals fortherapy requires even more detailed and patient-specific dosimetry, for both tumour and normaltissue. For estimation of the absorbed dose to pa-tients undergoing nuclear medicine investiga-tions, knowledge of biokinetics (e.g. cumulatedactivities in organs and tissues) as well as phys-ical data (e.g. decay properties of the radionu-clide, emitted radiation and source-target geom-etry) is required. The most common way toachieve information on the organ content of a ra-dionuclide is by means of whole body gammacamera measurement. The information can be ob-
tained from single planar gamma camera imagesor from two 180° opposed planar images (conju-gate view) using the geometric mean of the num-ber of counts in the two images.1–4
The various methods for quantification can befurther improved if patient-, organ- and phantom-specific attenuation corrections are introduced5–9. With correction for effective attenuation (ab-sorption and scattering) the conjugate countingtechnique can be used for absolute activity de-termination, provided that measurement of thesensitivity of the gamma camera is ascertainedbeforehand. In addition, the accuracy of the ac-tivity quantification depends to a considerable de-gree on the method to correct for background ac-tivity 10,11 and on correction methods to accountfor organ overlap12.
To overcome problems with background activ-ity and overlapping organs, Single-Photon Emis-sion Computed Tomography (SPECT) systems areuseful. SPECT has great potential for quantifica-tion of activity distributions in vivo due to its “three-
Address reprint requests to: Kristina Norrgren, Dept. ofRadiation, Physics Malmö, University Hospital, SE-205 02Malmö, Sweden

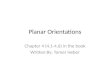
Figure 1. (a) MIRD phantom and (b) RSD Heart/thorax phantom and scanned images of the phantoms.
dimensional” imaging capability. There are, how-ever, several factors that must be considered inquantitative imaging. The two most significantnon-linear effects are the same as those for planarimaging, namely the photon attenuation in the sub-ject and the contribution from scattering in the sub-ject. Corrections to overcome these problems havebeen proposed using Monte Carlo techniques13.The major disadvantage using SPECT in internalwhole body dosimetry for radiation protection pur-poses is that it requires an unacceptable acquisitiontime. SPECT is, however, a valuable complementto planar conjugate counting imaging.
The aim of the study was to investigate the un-certainty in quantification due to attenuation pa-rameters, sensitivity and background correctionin a phantom study.
A theoretical analysis of the impact on the or-gan activity from reasonable deviation in the in-dividual parameters included in the equation ofFleming3, is presented.
MATERIAL AND METHODS
Phantom Measurements
Two different phantoms were used, a plastic torsophantom with plastic organ inserts constructed by
our group according to the phantom described inMIRD14, and a RSD Alderson Heart/thorax phan-tom (Elimpex Medizintechnik GesmbH, Austria).99mTc activity was filled in the, heart (10 MBq(160 ml)-, liver (42 MBq, 1800 ml)-, kidney in-serts (18 MBq, 155 ml each) and into the back-ground (66 MBq) of the MIRD phantom and inheart (Iowa heart phantom, 12 MBq, 110 ml),lungs (10 MBq in each lung) and background (76MBq) of the RSD phantom, figure 1.
The phantoms were scanned on a dual headedgamma camera (Siemens Multispect 2, Chicago,USA), with a low energy high resolution colli-mator. The scan speed was 15 cm/min for allmeasurements and the auto contour function wasused. No scatter correction was applied. A 15%energy window was centered over the 140 keVphoton peak. Scanning was also done on a sin-gle-headed gamma camera (Toshiba CGA901A, Tokyo) equipped with a low energy, gen-eral purpose collimator using a 20% energy win-dow.
The activity in the syringe was measured in adose calibrator (Capintec CRC-15, New Jersey,USA) before and after the administration to theorgans and the torso. Correction was made for ra-dioactive decay between the gamma camera mea-surement and the determination of the activity inthe syringe.
126
a b

Sensitivity
The sensitivity of the gamma cameras (K) wasdetermined using a 10 cm diameter, 3 mm thicksource containing 32 MBq 99mTc placed 10 cmfrom the collimator surface. The number ofcounts per second was determined from a re-gion of interest (ROI) in the image, correctedfor background activity. The activity in thesource was determined using a dose calibrator.The sensitivity was calculated as (counts persecond)/MBq.
The Effective Attenuation Coefficient
The effective attenuation coefficient was mea-sured using a 57Co flood source. A transmissionscan was done, i.e. the phantom was scanned(scan speed 15 cm/min) with the flood source po-sitioned under the pallet of the gamma camera.A blank scan, i.e. a scan without the phantom,was performed using the same acquisition pa-rameters as for the phantom study. Regions of in-terest were drawn for all organs in the transmis-sion image and the blank scan image, and thetransmission factor (TF) for each organ was thencalculated as:
TF 5 (cts/pixel(transm))/(cts/pix(blank)) (1)
Background Correction
Regions of interest (ROI) were drawn around theorgans on the gamma camera images in the an-terior and posterior images. A background regionof the same size as the organ was defined adja-cent to the organ ROI. Background corrections
were carried out in two different ways. The firstmethod used the conventional background cor-rection method, in which the net counts in the re-gion, C was defined as:
C 5 C9 2 CB (2)
where C9 5 gross counts in region, CB 5 countsin background region (accounting for number ofpixels in the regions). The alternative method wasthe so-called organ volume background correctionmethod, which considers the organ thickness11.
C 5 C9 2 CB*F (3)
where F 5 1 2 (l / L), l 5 organ thickness, L 5body thickness.
127
Figure 2. Estimated relative activity vs. the effective at-tenuation coefficient, me (normalised to me 5 0.12 cm21). Land l are the body and organ thickness, respectively.
Figure 3. Estimated relative activity vs. deviation in body thickness (me 5 0.12 cm2).

Figure 4. The organ thickness correction term vs. the mean organ thickness (me 5 0.12 cm21).
Calculation of Activity
The activity was calculated as:
A 5 (Na ? Np)1/2
31e2me ? L/2 ? 2 K421
(4)
where Na and Np are the background correctedcount rates (cps) in the anterior and posterior im-age of the organ or tissue, respectively, L is thebody thickness (cm) at the region of interest, l isthe organ thickness (cm), me is the effective at-tenuation coefficient for the photon energy dis-tribution in question (cm21) and K is the sensi-tivity, count rate per unit activity, for themeasuring device (cps per MBq).
The relative activity was calculated to study theinfluence of the parameters effective attenuationcoefficient, body thickness and organ thickness.An effective attenuation coefficient of 0.12 cm21
sinh(me ? l/2}}
me ? l/2
or a measured coefficient was used in the calcu-lations.
For measured transmission, the activity wascalculated according to
A 5 (NaNp)1/2/TFl/2/K (5)
Calculation of Uncertainty
The total uncertainty is calculated using the er-ror propagation formula:
s2u 5 1 2 s2
x 1 1 22
s2y 1 . . . (6)
From the theoretical analysis of the activity cal-culation (eq. 4) the uncertainty was determinedusing an estimation of the uncertainty in deter-mination of each parameter in the formula. Forexample, it was estimated that the body thicknesscould be determined with an uncertainty of 61.5
u}y
u}x
128
Table 1. Sources Contributing to Overall Uncertainty in Organ ActivityAssessment
Sources contributing to overall uncertainty Uncertainty (%)
Effective linear attenuation coefficient, me 610.5Body thickness, L 610Source organ thickness, l 63Background correction 620Determination of sensitivity, K 65Count rate in the images, Na and Np 62Attenuation in gamma camera pallet 60.5Total 625

cm, giving an uncertainty in the activity deter-mination of 610%.
RESULTS
The accuracy of the organ activity estimations ishighly dependent on the accuracy of the effectiveattenuation coefficient used in the calculation. Arange of values for the effective attenuation co-efficient has been reported in the literature, from0.11 to 0.15 cm21 for 140 keV photons from99mTc 15–18. From eq. 4 follows that a deviationof 0.01 cm21 from a fixed value for mewill resultin a deviation of up to 15% in the calculated ac-tivity (Figure 2). To improve the accuracy of the
attenuation correction and to reduce the effect ofdifferent effective body thickness, the attenuationin various parts of the body can be determinedusing transmission measurements.
A theoretical analysis of the “conjugate-viewequation” (eq. 4) showed that the accuracy of theactivity assessment was predominantly influ-enced by uncertainties in the determination of theeffective attenuation coefficient and in the bodythickness. A deviation in the body thickness of 2cm resulted in a deviation of 12% in activity(me 5 0.12 cm21) (Figure 3).
An uncertainty in the estimation of the organthickness yielded only a minor effect on the accu-racy, and omitting the organ attenuation correctionterm resulted in an overestimation of the activity
129
Table 2. Differences between Calculated 99mTc-Activity and True Activity for Organs in the MIRD Phantom
Background correction Liver region Kidney region Heart region
Conventional method 224% 226% 221%Organ volume method 24% 221% 21%Organ volume method including 9% 25% 216%
correction for organ attenuation
Figure 5. The deviation in measured activity from true activity for heart and lungs in the thorax phantom. The activity was cal-culated using both a theoretical attenuation coefficient and a measured coefficient. 1. No background correction, no attenuationcorrection. 2. No background correction, transmission measurement. 3. Conventional background correction, abdominal back-ground region. 4. Conventional background correction, background ROI in thorax. 5. Conventional background correction, back-ground in thorax region, attenuation correction using transmission measurement. 6. Organ volume background correction, ab-dominal background region. 7. Organ volume background correction, background ROI in thorax region. 8. Organ volumebackground correction, background ROI in thorax region, transmission measurement.

of 1–6% for most organs in the body (organ thick-ness: 3–10 cm), e.g. the kidneys and the spleen.Disregarding the organ attenuation correction termfor thicker organs such as the liver (thickness: 20cm) resulted, however, in an overestimation ofabout 20% (me 5 0.12 cm21) (Figure 4).
The major contribution to the overall uncertaintyin the organ activity assessment thus comes fromfactors including the effective attenuation coeffi-cient, body thickness, background correctionmethod, source organ thickness and determinationof the sensitivity for the measuring device (Table1). The uncertainty for each contributing parame-ter was estimated from the theoretical analysis.
Next, the effect of background correctionmethod in quantification of organ activity in thephantoms was studied. In the MIRD phantom, us-ing the conventional background correctionmethod, the use of this method resulted in an un-derestimation of the activity by 21 to 26% in theorgans (Table 2). If the organ volume method11
was used, the values were underestimated in theliver- and heart-phantom by 4% and 1%, respec-tively, and in the kidney phantom by about 21%in the MIRD phantom. However, when the atten-uation in the organs was taken into account in theorgan-phantom measurements, the activity in theliver-phantom was overestimated by 9% and inthe heart phantom by 16%, whereas the activityin the kidney phantom was underestimated by 5%.
Similar results were obtained in the thorax phan-tom for lungs and heart for different activity con-centrations in the organs and background, Figure 5.
The influence on the choice of background re-gion, background correction method and on thechoice of attenuation correction method is shownin Figure 5. An effective attenuation coefficientof 0.12 cm21 was used except in cases wheretransmission measurement is stated in the figurelegend.
The choice of background region is a very im-portant factor for the quantification. The organvolume method is recommended for small organsand the use of transmission measurement im-proves the accuracy in the quantification com-pared with the use of an effective attenuation co-efficient in the calculation of activity.
DISCUSSION
In order to make accurate absorbed dose estima-tions knowledge of the activity content and re-tention in organs and tissues is needed. The ac-
curacy of the activity assessment is influenced byfactors such as correction of background activity,absorption and scattering of the photons withinthe body. Another factor to consider in quantifi-cation of the activity based on planar scintigra-phy is the effect of overlapping tissues. This ap-plies particularly to kidneys and liver; a methodto correct for this is to use the count per pixel ra-tios of the nonoverlapping regions of the organs.Another method is to double the number ofcounts from one kidney which does not haveoverlapping regions, assuming equal activity dis-tribution between the two kidneys. Redistributionof activity during scanning is yet another sourceof uncertainty that has to be considered in quan-tification. This factor is very difficult to assessquantitatively.
CONCLUSIONS
In order to limit the uncertainties in quantifica-tion of organ activity, special effort should be fo-cused on the choice of correction methods, ofwhich the background correction is perhaps themost important. In this study, the discrepancy inthe determined organ activity varied between anunderestimation of 26% and an overestimation of16% in the MIRD phantom, depending on whichorgan was studied and on the correction methodused. A change in the effective attenuation coef-ficient of 0.01 cm21 resulted in a 15% change inthe calculated activity. The thickness of the bodyand the organ of interest influences the calculatedactivity. A 2 cm deviation in the body thicknesscauses a deviation of approximately 10% in thecalculated activity. The quantification is im-proved if the attenuation coefficient is determinedby transmission measurements.
REFERENCES
1. Sorensson JA. Quantitative measurement of radioactiv-ity in vivo by whole-body counting. In: Hine GJ andSorenson JA. Instrumentation in nuclear medicine.Academic Press Inc. New York. 1974. pp. 311–348.
2. Thomas SR, Maxon HR and Kereiakes JG. In vivoquantitation of lesion radioactivity using external count-ing methods. Med Phys 1976;3:253–255.
3. Fleming JS. A technique for the absolute measurementof activity using a gamma camera and computer. PhysMed Biol 1979;24:176–180.
4. Sharp PF, Dendy PP, Keyes WI. Radionuclide imagingtechniques. Academic Press 1985.
130

5. Forge NI, Mountford PJ, O’Doherty MJ. Quantificationof technetium-99m lung radioactivity from planar im-ages. Eur J Nucl Med 1993;20:10–15.
6. van Rensburg AJ, Lötter MG, Heyns AP, and MinnaarPh C. An evolution of four methods of 111In planarquantification. Med Phys 1988;15:853–861.
7. Miller C, Filipow L and Jackson S. A review of activ-ity quantification by planar imaging methods. J NuclMed Technol 1995;23:3–9.
8. Smith T. Comparison of two methods of quantitation inhuman studies of biodistribution and radiation dosime-try. Phys Med Biol 1992;37(5):1065–1076.
9. Rowell NP, Glaholm J, Flower MA, Cronin B, and Mc-Cready VR. Anatomically derived attenuation coeffi-cients for use in quantitative single photon emission to-mography studies of the thorax. Eur J Nucl Med 1992;19:36–40.
10. Kojima M, Takaki Y, Matsumoto M, Tomiguchi S, HaraM, Shimomura O, Koga Y, and Takahashi M. A pre-liminary phantom study on a proposed model for quan-tification of renal planar scintigraphy. Med Phys 1993;20:33–37.
11. Buijs WCAM, Siegel JA, Boerman OC and CorstensFHM. Absolute organ activity estimated by five differ-ent methods of background correction. J Nucl Med1998;32:2167–2172.
12. Goris ML, Knox SA, Nielsen KR, Bouillant O. Organmodelling in the quantitation of planar images for dis-
tribution studies. Cancer Supplement 1994;73:919–922.
13. Ljungberg M. Development and evaluation of attenuationand scatter correction techniques for SPECT using theMonte Carlo method. [PhD Thesis] Department of Radi-ation Physics, Lund University, Lund, Sweden. 1990.
14. Snyder WS, Ford MR, Warner GG. Estimates of spe-cific absorbed fractions for photon sources uniformlydistributed in various organs of a heterogenous phan-tom. MIRD Pamphlet No. 5, Revised. 1978.
15. Seddon DJ and Snashall PD. Thoracic tissue thicknessmeasured by transmission scintigraphy with 99mTc.Nucl Med Comm 1990;11:135–141.
16. Harris CC, Greer KL, Jaszczak RJ, Floyd CE, Jr.,Fearnow EC and Coleman RE. Tc-99m attenuation co-efficients in water-filled phantoms determined withgamma cameras. Med Phys 1984;11:681–685.
17. Starck SA and Carlsson S. The determination of the ef-fective attenuation coefficient from effective organdepth and modulation transfer function in gamma cam-era imaging. Phys Med Biol 1997;42:1957–1964.
18. Vestergren E, Jacobsson L, Mattsson S, Johansson L,Bjure J, Sixt R and Uvebrandt P. Biokinetics anddosimetry of 99mTc-HM-PAO in children. In: Schlafke-Stelson AT and Watson EE, eds. Proceedings of theFifth International Radiopharmaceutical DosimetrySymposium. -910529. Oak Ridge Associated Universi-ties, Oak Ridge, Tennessee, USA, 1992;444–455.
131