Embed Size (px)
Citation preview

604 AJR:191, August 2008
from these two echo lines undergo processing, and ultimately an elastographic image (elasto gram) appears on the monitor. There are two types of elastograms, grayscale and color. The hard and soft areas (i.e., areas of high and low elasticity, respectively) appear in the grayscale elastogram as dark and bright [5, 6]. In the color elastogram, increasing tissue hard ness appears in ascending order as red, yel low, green, and blue. These colors represent the relative hardness of the tissues in the elastogram.
Sonographic elastography has been used to examine several organs: the breast [7, 8], thyroid [5], prostate [9], cervix [10], liver [11], and so forth. Recently, an article relating their initial experience in the diagnosis of cervical lymph node metastasis us ing grayscale sonographic elastography was published by Lyshchik et al. [6]. To our knowledge, however, no Englishlanguage articles have documented the evaluation of cervical lymph nodes using color sonographic elastography.
Accuracy of Sonographic Elastography in the Differential Diagnosis of Enlarged Cervical Lymph Nodes: Comparison with Conventional B-Mode Sonography
Farzana Alam1
Kumiko Naito2,3
Jun Horiguchi2 Hiroshi Fukuda2
Toshihiro Tachikake1
Katsuhide Ito1
Alam F, Naito K, Horiguchi J, Fukuda H, Tachikake T, Ito K
1Department of Radiology, Division of Medical Intelligence and Informatics, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, Japan.
2Department of Clinical Radiology, Hiroshima University Hospital, 1-2-3, Kasumi-cho, Minami-ku, Hiroshima, 734-8551, Japan. Address correspondence to J. Horiguchi ([email protected]).
3Present address: Hiroshima Atomic Bomb Casualty Council, Hiroshima, Japan.
Head and Neck Imaging • Or ig ina l Research
AJR 2008; 191:604–610
0361–803X/08/1912–604
© American Roentgen Ray Society
Elasticity (hardness) is a mechanical tissue characteristic that prevents tissue displacement under pressure. It varies in different
types of tissue (fat, collagen, and so forth) and in the same tissue in different pathologic states (inflammatory, malignant). During the past few years, sonographic elastography, MR elastography [1, 2], and some other techniques have performed digital measurements of tissue hardness. In sonographic elastography, image represent ation of tissue hardness can be obtained using a conventional sonography machine with special software and a conventional ultrasound probe [3, 4].
In brief, sonographic elastography works in the following steps: first, elastography receives digitized radiofrequency echo lines from the tissue; second, it gives slight compression to the tissue by the transducer along the radiation axis to make some displacement; and third, it receives a second, postcompression digitized radiofrequency echo line from the same tissue [4]. Then the data
Keywords: elastography, lymph nodes, metastasis, sonography
DOI:10.2214/AJR.07.3401
Received November 9, 2007; accepted after revision February 17, 2008.
OBJECTIVE. The purpose of our study was to evaluate the diagnostic performance of sonographic elastography and Bmode sonography individually and combined in the differentiation of reactively and metastatically enlarged cervical lymph nodes.
SUBJECTS AND METHODS. Eightyfive lymph nodes (metastatic, n = 53; reactive, n = 32) from 37 patients were examined by both elastography and Bmode sonography in this prospective study. Elastographic patterns were determined on the distribution and percentage of the lymph node area with high elasticity (hard), with pattern 1 being an absent or very small hard area to pattern 5, a hard area occupying the entire lymph node. The cutoff line for reactive versus metastatic was set between patterns 2 and 3; patterns 3–5 were considered metastatic. Bmode sonographic diagnosis was based on the sum of scores for five criteria: shortaxis diameter, shape, border (regular or irregular), echogenicity (homogeneous or inhomo geneous), and hilum (present or absent). The cutoff line for reactive versus metastatic was set between scores 6 and 7; scores 5 and 6 were considered reactive, and scores 7–10, metastatic.
RESULTS. Sensitivity, specificity, and accuracy of Bmode sonography were 98%, 59%, and 84%, respectively; 83%, 100%, and 89% for elastography; and 92%, 94%, and 93% for the combined evaluation.
CONCLUSION. The combination of highly specific elastography with highly sensitive conventional Bmode sonography has the potential to further improve the diagnosis of metastatic enlarged cervical lymph nodes.
Alam et al.Sonographic Elastography of Cervical Lymph Nodes
Head and Neck ImagingOriginal Research
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:191, August 2008 605
Sonographic Elastography of Cervical Lymph Nodes
Of the 400–450 lymph nodes in the human body, the head and neck contain 60–70. These nodes show reactive enlargement due to infection (e.g., infection of upper aerodigestive tract). They also undergo enlargement when they are secondarily involved in head and neck cancer. Sometimes metastatic cervical lymphadenopathy appears as the first symptom in patients having malignancy in the head and neck, lung, breast, and so forth. Differentiation between reactive and metastatic lymph adenopathy is vital, and one of the differentiating criteria is hardness (elasticity) of the lymph node.
The purpose of this study was to investigate the accuracy of conventional sonography, sonographic elastography, and their combined evaluation for the differentiation between reactive and metastatic enlarged cervical lymph nodes.
Subjects and MethodsPatients
This was a prospective study. From January to November 2006, 109 lymph nodes of 59 con secutive patients who were referred for sonography of enlarged cervical lymph nodes were enrolled. Written informed consent was received from all pa tients for undergoing both conventional B mode sonography and elastography. The 85 lymph nodes (reactive, n = 32; metastatic, n = 53) from 37 patients (25 males, 12 females; mean age ± SD, 55 ± 22 years old; age range, 11–92 years) with (n = 25) and with out (n = 12) malignancy in which the final diag nosis was known, were used for evaluation.
Final DiagnosisLymph nodes were determined to be reactive
on the basis of histopathologic findings or on the basis of clinical findings such as enlarged tender lymph node, increased Creactive protein, leukocytosis, decreased size of the lymph node after antibiotic treatment, and the absence of known malignancy. The reference standard for the final diagnosis of metastatic lymph nodes was histopathologic findings or imaging findings suggesting central necrosis—that is, hypodensity on contrastenhanced CT [12] or hypointensity on contrastenhanced T1weighted MRI in patients with malignancy.
Equipment and ScanningOne radiologist who had 18 years’ experience
with conventional sonography and was a novice in elastography performed the sonography. The patients underwent both Bmode and elastographic sonography in the supine position with a digital sonography scanner (EUB 8500, Hitachi Medical) equipped with the Realtime Tissue Elastography software (Hitachi Medical); the probe was a conventional linear probe with a 13MHz transducer (EUPL65, Hitachi Medical).
For each lymph node, Bmode images were obtained first. Then, changing the system into the elastography mode, realtime freehand elastography was performed using the same probe for an additional 1–2 minutes. For elastography, compression with light pressure followed by decompression was repeated until a stable image was obtained—that is, nearly the same size and color distribution of the target area in several consecutive images. Direction of the compression
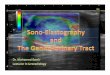
was upward and downward (along the radiation axis). Frequency of compression appeared on a scale on the monitor. Realtime elastographic and Bmode images simultaneously appeared as a twopanel image. Figure 1 shows a typical image displayed on the monitor during elastography, in which the elastogram appears in a regionofinterest (ROI) box. The size of the box was determined to be the target lymph node including surrounding tissue in almost the same proportion while avoiding tissues (bone, blood vessel) that might disturb the appropriate analysis of the relative hardness of the target lymph node. To maintain unbiased reading, 85 sets of elasto grams and corresponding Bmode images without any patient information were collected into two separate slide shows (Microsoft PowerPoint, 2003) in random order.
EvaluationTo minimize recall bias, 1 month after data
collection was completed, scorebased reevaluation of Bmode and elastographic images was done by one of the authors who was blinded to other information. Less than 1 minute was required for the evaluation of each image (elastography and Bmode).
B-mode evaluation—Bmode images were evaluated on the criteria of size, shape, border, echogenicity, and hilum. Size and shape were evaluated per region. Regional distribution was determined according to the 1997 American Joint Committee on Cancer (AJCC) criteria for lymph nodes [13], in which neck lymph nodes are divided into seven levels. Lymph nodes in level 7 were excluded because scanning them was not possible with sonography. For the criterion of size, the shortaxis diameter (in mm) of the lymph nodes was evaluated. For shape, the ratio of the shortaxis diameter to the longaxis diameter (S/L axis ratio) was used. For each lymph node, we determined the cutoff values of shortaxis diameter and S/L axis ratio that gave the best accuracy. In cases of level 4 (AJCC classification) lymph nodes in which two cutoff values had the highest accuracy, we used receiver operating characteristic (ROC) curve analysis to select one for our purposes. Scores were determined for five criteria: the shortaxis diameter (diameter ≤ cutoff value, score of 1; diameter > cutoff value, score of 2), the S/L axis
Fig. 1—Appearance of monitor during elastography examination of 52-year-old man. Elastogram appears on left side of box and is superimposed on corresponding B-mode image. Corresponding B-mode image is displayed on right side of monitor. Color scale of tissue elasticity and frequency scale appear in center (upper and lower, respectively). Final diagnosis was metastasis.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

606 AJR:191, August 2008
Alam et al.
ratio (ratio ≤ 0.6, score of 1; > 0.6, score of 2), the border (regular, 1; irregular, 2), echogenicity (homo geneous, 1; inhomogeneous, 2), and hilum (present, 1; absent, 2) [6, 12–21]. The score for each lymph node was determined by summing scores for all criteria. A statistically supported cutoff line between reactive and metastatic was set between scores 6 and 7, depending on the best accuracy. Scores 5 and 6 were determined to be reactive, and scores 7–10, metastatic.
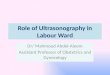
Elastogram evaluation—After observing all the elastograms, two authors together subjectively decided five patterns for the elastograms depending on the distribution of the blue (i.e., hard) area in the lymph node. Elastographic patterns were deter mined on the distribution and percentage of the lymph node area with high elasticity (hard): pattern 1, an absent or a very small hard (i.e., blue) area; pattern 2, hard area < 45% of the lymph node; pattern 3, hard area ≥ 45%; pattern 4, peripheral hard and central soft areas; pattern 5, hard area occupying entire lymph node with or without a soft rim. The patterns 1, 2, 3, 4, and 5 were assigned scores of 2, 4, 6, 8, and 10, respectively. The outline of the lymph node was drawn, and the percentage of blue area was measured on an offline computer using image analysis software “Image J” developed by the National Institutes of Health [22]. On average, approximately 1–2 min utes was required for the measurement of the blue area of each lymph node. A statistically sup ported cutoff line at 45% blue between patterns 2 and 3 was obtained from the ROC (Table 1 and Figs. 2–7).
Combined evaluation—The combined score for each lymph node was the sum of the Bmode
and elastographic scores. A statistically supported cutoff line between metastatic and reactive was set between scores 12 and 13, depending on the best accuracy. Scores 7–12 were determined to be reactive, and scores 13–20, metastatic.
For Bmode, elastography, and the combined evaluations, the precision of the diagnostic parameters (sensitivity, specificity, accuracy, and positive and negative predictive values) was expressed using 95% CI. The areas under the ROC curves were calculated.
ResultsFinal Diagnosis
The prevalence of lymph node metastasis was 62% (53/85). Among the metastatic lymph nodes, 36 had primary squamous cell car ci
noma (SCC), 13 had primary thyroid carcinoma, two had their primary site in the breast, one was in the lung, and one was unknown. The lymph nodes were finally diagnosed as reactive histopathologically (n = 2) and clinically (n = 30). The lymph nodes were diagnosed as metastatic by histo pathology (n = 26), CT (n = 24), and MRI (n = 3). By AJCC levels, 17 nodes were in level 1, 26 in level 2, 21 in level 3, nine in level 4, and 12 in level 5.
B-Mode SonographyCutoff shortaxis diameters according to
AJCC levels were 11 mm in level 1, 13 mm in level 2, 5 mm in level 3, 9 mm in level 4, and 7 mm in level 5. The cutoff S/L axis ratio was 0.6; ≤ 0.6 was reactive and > 0.6 was metastatic. The accuracy for individual B mode criteria was 84% for size, 56% for S/L axis ratio, 67% for border, 86% for hilum, and 78% for echogenicity (Table 2).
ElastographyDuring elastography, compression at a fre
quency of 3 or 4 on the frequency scale was needed to obtain stable elastographic features. In elastogram evaluation, all 32 reactive lymph nodes showed patterns 1 and 2 (re active). Among 53 metastatic lymph nodes,
TABLE 1: Patterns and Scoring System on Elastographic Findings
Pattern Score Description Elastographic Diagnosis Figure
1 2 Absent or very small blue area(s) Reactive 2, 3
2 4 Small scattered blue areas, total blue area < 45%
Reactive 2, 4
3 6 Large blue area(s), total blue area ≥ 45% Malignant 2, 5
4 8 Peripheral blue area and central green area, suggesting central necrosis
Malignant 2, 6
5 10 Blue area with or without a green rim Malignant 2, 7
Fig. 2—Drawings show typical diagrammatic appearance of five patterns of lymph nodes. Elastographic patterns were determined on distribution and percentage of lymph node area having high elasticity (hard): pattern 1, absent or small hard area; pattern 2, hard area < 45% of lymph node; pattern 3, hard area ≥ 45%; pattern 4, peripheral hard and central soft areas; pattern 5, hard area occupying entire lymph node. Increasing tissue hardness appears in ascending order as red, yellow, green, and blue.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:191, August 2008 607
Sonographic Elastography of Cervical Lymph Nodes
44 (83%) had patterns 3, 4, and 5 (metastatic). Two (4%) and seven (13%) metastatic lymph nodes showed patterns 1 and 2, respectively. Con cerning elasticity pattern 4 (i.e., suggestive of central necrosis), 12 of 13 (92%) lymph nodes were metastasized from SCC and one (8%) from an unknown origin.
Diagnostic PerformanceThe diagnostic performances of Bmode
sonography, elastography, and the combined test are shown in Table 3. Bmode sonography showed sensitivity of 98% (95% CI, 94–100%), specificity of 59% (42–76%), and accuracy of 84% (76–91%). Elasto graphy
showed sensitivity of 83% (73–93%), specificity of 100% (100–100%), and accu racy of 89% (83–96%). The combined evaluation showed sensitivity of 92% (85–100%), specificity of 94% (85–100%), and accuracy of 93% (88–98%). The ROC curves for B mode, elastography, and the combined evalu
Fig. 3—Transverse sonogram of level 1 lymph node in 30-year-old man with left submandibular lymphadenopathy. Elastography image on left shows pattern 1, absent or small hard area. B-mode sonographic image on right shows score of 5, reactive. Final diagnosis from clinical and serologic findings was reactive lymph node.
Fig. 4—Longitudinal sonogram of level 2 lymph node in 33-year-old woman with left posterior auricular lymphadenopathy. Elastography image on left shows pattern 2, hard area < 45% of node. B-mode sonographic image on right shows score 5, reactive. Final diagnosis from clinical and serologic findings was reactive lymph node.
Fig. 6—Longitudinal sonogram of level 5 lymph node in 52-year-old man with nasopharyngeal carcinoma. Elastography image on left shows pattern 4, peripheral hard and central soft areas. B-mode sonographic image on right shows score 7, metastatic. Final diagnosis by CT was metastatic lymph node.
Fig. 5—Transverse sonogram of level 2 lymph node in 79-year-old man with laryngeal carcinoma. Elastography image on left shows pattern 3, hard area ≥ 45%. B-mode sonographic image on right shows score 7, metastatic. Final diagnosis by histopathology was metastatic lymph node.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

608 AJR:191, August 2008
Alam et al.
ation in the differentiation of reactive and metastatic lymph nodes are shown in Figure 8. The areas under the curves for Bmode sonography, elastography, and the combined evaluation were 0.901, 0.873, and 0.970, respectively.
DiscussionTo our knowledge, this is the first English
language study documenting the accuracy of color sonographic elastography individually and combined with Bmode sonography in the differential diagnosis of reactive versus metastatic cervical lymph nodes. Elasto graphy provides high specificity; especially when combined with Bmode sonography, elas tography increases the accuracy of sono graphy for enlarged cervical lymph nodes.
B-Mode SonographySeveral studies have been published on the
diagnosis of metastatic cervical lymph node by Bmode sonography [12, 14–21]; however, specific criteria for distinguishing reactive from metastatic cervical lymph nodes are not yet clear. The cutoff shortaxis diameter for level 2 lymph nodes was two times higher than that for level 3. This suggests that, for the evaluation of cervical lymph nodes, a common cutoff diameter should not be set for all levels. In a study by Lyshchik et al. [6] using the fixed cutoff diameter of 8 mm, the accuracy of the shortaxis diameter was 65%, whereas in our study it was 84%. With respect to shape, our calculation gave the best accuracy at S/L axis ratio ≤ 0.6 for reactive and > 0.6 for metastatic nodes, which supports the findings of round shape for metastatic nodes in previous studies [6, 14, 15]. Very few studies have evaluated lymph node borders. Ying et al. [16], Ahuja and Ying [17], and Ying et al. [21] evaluated lymph node borders as sharp and unsharp. In this study, we evaluated regular and irregular lymph node borders as a criterion of reactive and metastatic lymph nodes, respectively, that showed 67% accuracy. The presence or absence of a hilum has been reported to be an important criterion for lymph node diagnosis [6, 18]. In our study also, this showed the best accuracy (86%).
Fig. 7—Longitudinal sonogram of level 3 lymph node in 59-year-old man with thyroid carcinoma. Elastography image on left shows pattern 5, hard area occupying entire node. B-mode sonographic image on right shows score 8, metastatic. Final diagnosis by histopathology was metastatic lymph node.
TABLE 3: Diagnostic Performance of Elastography, B-Mode Sonography, and Combined Evaluation
Performance Measure B-Mode Sonography Elastography Combined
Sensitivity (%) 98 (94–100) 83 (73–93) 92 (85–100)
Specificity (%) 59 (42–76) 100 (100–100) 94 (85–100)
Accuracy (%) 84 (76–91) 89 (83–96) 93 (88–98)
Positive predictive value (%) 80 (70–89) 100 (100–100) 96 (91–100)
Negative predictive value (%) 95 (85–100) 78 (65–91) 88 (77–99)
Note—Values in parentheses are 95% CIs (in percentages).
TABLE 2: Results According to Criteria for Reactive and Metastatic Lymph Nodes
Sonography Criteria
Lymph Nodes
Accuracy (%)Reactive Metastatic
B-mode
Size of short-axis diameter 84
≤ Cutoff value 28 (88) 10 (19)
> Cutoff value 4 (12) 43 (81)
S/L axis ratio 56
≤ 0.6 18 (56) 23 (43)
> 0.6 14 (44) 30 (57)
Border 67
Regular 24 (75) 20 (38)
Irregular 8 (25) 33 (62)
Hilum 86
Present 26 (81) 6 (11)
Absent 6 (19) 47 (89)
Echogenicity 78
Homo geneous 21 (66) 8 (15)
Inhomo geneous 11 (34) 45 (85)
Elastography pattern 89
1 19 (59) 2 (4)
2 13 (41) 7 (13)
3 0 21 (40)
4 0 13 (24)
5 0 10 (19)
Note—Numbers in parentheses are percentages. S/L axis ratio = ratio of short-axis diameter to long-axis diameter.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:191, August 2008 609
Sonographic Elastography of Cervical Lymph Nodes
ElastographyStiffness of cervical lymph nodes was
independently assessed both quantitatively and qualitatively by Lyshchik et al. [6] using external sonographic grayscale elastography. Those authors assessed the diag nostic potential of qualitative criteria—lymph node visibility, relative brightness, margin regularity, and margin definition—as well as the quantitative criterion strain index, which was obtained by comparing the absolute values of lymph node strain with the absolute values of surrounding muscle strain. Among these criteria, strain index greater than 1.5 was the most useful in metastatic lymph node classification, having 98% specificity, 85% sensitivity, and 92% accuracy. We obtained a similar level of results (100% specificity, 83% sensitivity, and 89% accuracy) using the combination of both qualitative and quantitative criteria. However, we propose the combined criteria, for the following reasons: The presence of a central green area in pattern 4 was considered to be central necrosis. Our result showing 12 of the 13 pattern 4 lymph nodes had primary SCC supports this consideration. Furthermore, we considered a large blue area in a scattered distribution to suggest the manifestation of focal cortical metastatic invasion and there fore categorized this appearance as pattern 3. This criterion did not show any falsepositive results.
In endoscopic sonographic elastography of lymph nodes, Giovannini et al. [23] reported 100% sensitivity and 50% specificity without using any qualitative pattern analysis, whereas Saftoiu et al. [24] reported 91.7% sensitivity and 94.4% specificity using a pattern analysis. These facts also indicate the importance of qualitative pattern analysis. However, another pattern of elastographic lymph node analysis has been reported in which only the percentage of blue area was used as a criterion [25].
The greatest advantage of elastography is its high specificity, which has been found not only in our study but also in other studies [6, 24]. Because of this, elastography may re duce unnecessary invasive procedures for the diagnosis of cervical lymph node metastasis.
Combined EvaluationAccuracy and area under the ROC curve
showed that the diagnostic power of the combined evaluation was higher than that of the individual evaluations. This suggests that the examination can be best performed when Bmode sonography, with its high sensitivity, and elastography, with its high specificity, are complementary. The scope of our study was to test the performance of elastography and the combined test compared with Bmode sonography alone. In clinical practice, however, sonography practitioners should use both methods in real time.
Gray-Scale and Color ElastographyIn the grayscale elastography study by
Lyshchik et al. [6], postprocessing of radiofrequency images was done on an offline computer. In our color elastogram study, postprocessing was done in real time, which made the process quicker. Although our study was performed on an offline computer, in clinical practice realtime color elastog raphy seems to have an advantage over grayscale. Realtime diagnosis needs further investigation.
LimitationsThis study had some limitations. First, our
data sample was small; we used the lymph node as our unit, not the patient. Second, we included only enlarged lymph nodes, whereas elastographic findings of normalsized lymph nodes should also be explored. Most metastatic lymph nodes in our study were in patients who had either primary SCC or
thyroid cancer. Lymph nodes with primary malignancy or metastases from other primary malignancies such as melanoma or breast cancer were not included. Third, the final diagnosis of almost all reactive lymph nodes was done based on followup findings instead of histopathologic findings. Fourth, evaluation was done on an offline computer from single images, which would not be practical for realtime evaluation.
Although elastography is a good improvement in the field of sonography, we still need to address one limitation for the future. Our evaluation had to be done in only one section of the lymph node. Assessment of the stiffness of the whole lymph node, by volu metric measurement, may increase the diag nostic performance of elastography.
In conclusion, elastography, with its high specificity, can improve the performance of sonography for the diagnosis of enlarged metastatic cervical lymph nodes. The combined evaluation of elastography and B mode sonography offers the strongest diagnostic power, and we recommend it in clinical practice.
AcknowledgmentsWe thank professors Megu Ohtaki and
Keiko Otani, from the Department of Environmetrics and BioMedical Informatics, Research Institute for Radiation Biology and Medicine, for their contribution in statistical analysis.
References 1. Glaser KJ, Felmlee JP, Manduca A, Kannan Mar
iappan Y, Ehman RL. Stiffnessweighted mag
netic resonance imaging. Magn Reson Med 2006;
55:59–67
2. Huwart L, Peeters F, Sinkus R, et al. Liver fibro
sis: noninvasive assessment with MR elastogra
phy. NMR Biomed 2006; 19:173–179
3. Ophir J, Cespedes I, Ponnekanti H, Yazdi Y, Li X.
Elastography: a quantitative method for imaging
the elasticity of biological tissues. Ultrason Imag-
ing 1991; 13:111–134
4. Ophir J, Garra B, Kallel F, et al. Elastographic
imaging. Ultrasound Med Biol 2000; 26[suppl
1]:S23–S29
5. Lyshchik A, Higashi T, Asato R, et al. Thyroid
gland tumor diagnosis at US elastography. Radi-
ology 2005; 237:202–211
6. Lyshchik A, Higashi T, Asato R, et al. Cervical
lymph node metastases: diagnosis at sonoelastog
raphy—initial experience. Radiology 2007; 243:
258–267
7. Itoh A, Ueno E, Tohno E, et al. Breast disease:
1
0.8
0 0.2 0.4
1 – Specificity
Sen
siti
vity
0.6 0.8 1
0.6
0.4
0.2
0
Fig. 8—Receiver operating characteristic curve for elastography (), B-mode sonography (), and combined evaluation (). Area under the curve for combined evaluation (0.970) is higher than that for B-mode sonography (0.901) or elastography (0.873).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

610 AJR:191, August 2008
Alam et al.
clinical application of US elastography for diag
nosis. Radiology 2006; 239:341–350
8. Thomas A, Fischer T, Frey H, et al. Realtime
elastography: an advanced method of ultrasound—
first results in 108 patients with breast lesions.
Ultrasound Obstet Gynecol 2006; 28: 335–340
9. Taylor LS, Rubens DJ, Porter BC, et al. Prostate
cancer: threedimensional sonoelastography for
in vitro detection. Radiology 2005; 237:981–985
10. Thomas A, Kummel S, Gemeinhardt O, Fischer T.
Realtime sonoelastography of the cervix: tissue
elasticity of the normal and abnormal cervix.
Acad Radiol 2007; 14:193–200
11. FriedrichRust M, Ong MF, Herrmann E, et al.
Realtime elastography for noninvasive assess
ment of liver fibrosis in chronic viral hepatitis.
AJR 2007; 188:758–764
12. van den Brekel MW, Stel HV, Castelijns JA, et al.
Cervical lymph node metastasis: assessment of
radiologic criteria. Radiology 1990; 177:379–384
13. Castelins JA, van den Brekel MW, Mukherji SK,
Lameris JS. Ultrasound of the neck. In: Som PM,
Curtin HD, eds. Head and neck imaging. Boston,
MA: Mosby, 2003:1935–1953
14. Vassallo P, Wernecke K, Roos N, Peters PE. Dif
ferentiation of benign from malignant superficial
lymphadenopathy: the role of highresolution US.
Radiology 1992; 183:215–220
15. Takashima S, Sone S, Nomura N, Tomiyama N,
Kobayashi T, Nakamura H. Nonpalpable lymph
nodes of the neck: assessment with US and US
guided fineneedle aspiration biopsy. J Clin Ul-
trasound 1997; 25:283–292
16. Ying M, Ahuja A, Metreweli C. Diagnostic accu
racy of sonographic criteria for evaluation of cer
vical lymphadenopathy. J Ultrasound Med 1998;
17:437–445
17. Ahuja A, Ying M. An overview of neck node
sonography. Invest Radiol 2002; 37:333–342
18. Leboulleux S, Girard E, Rose M, et al. Ultrasound
criteria of malignancy for cervical lymph nodes in
patients followed up for differentiated thyroid
cancer. J Clin Endocrinol Metab 2007; 92: 3590–
3594
19. Jank S, Robatscher P, Emshoff R, Strobl H, Gojer
G, Norer B. The diagnostic value of ultrasonogra
phy to detect occult lymph node involvement at
different levels in patients with squamous cell car
cinoma in the maxillofacial region. Int J Oral
Maxillofac Surg 2003; 32:39–42
20. van den Brekel MW, Castelijns JA, Snow GB. The
size of lymph nodes in the neck on sonograms as
a radiologic criterion for metastasis: how reliable
is it? Am J Neuroradiol 1998; 19:695–700
21. Ying M, Ahuja A, Brook F. Sonographic appear
ances of cervical lymph nodes: variations by age
and sex. J Clin Ultrasound 2002; 30:1–11
22. Image J: image processing and analysis in Java.
rsb.info.nih.gov/ij/. Accessed January 11, 2008
23. Giovannini M, Hookey LC, Bories E, Pesenti C,
Monges G, Delpero JR. Endoscopic ultrasound
elastography: the first step towards virtual biopsy?
Preliminary results in 49 patients. Endoscopy
2006; 38:344–348
24. Saftoiu A, Vilmann P, Hassan H, Gorunescu F.
Analysis of endoscopic ultrasound elastography
used for characterisation and differentiation of
benign and malignant lymph nodes. Ultraschall
Med 2006; 27:535–542
25. Furukawa MK, Kubota A, Hanamura H, Furuka
wa M. Clinical application of realtime tissue
elastography to head and neck cancer: evaluation
of cervical lymph node metastasis with realtime
tissue elastography. Nippon Jibiinkoka Gakkai
Kaiho 2007; 110:503–505
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
nive
rsity
of
Was
hing
ton-
Inte
rnet
on
08/2
5/14
fro
m I
P ad
dres
s 12
8.95
.104
.66.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved