Embed Size (px)
Citation preview

Sleep Medicine 15 (2014) 476–479
Contents lists available at ScienceDirect
Sleep Medicine
journal homepage: www.elsevier .com/locate /s leep
Brief Communication
Accuracy of portable polygraphy for the diagnosis of sleep apneain multiple system atrophy
http://dx.doi.org/10.1016/j.sleep.2013.12.0131389-9457/� 2014 Elsevier B.V. All rights reserved.
⇑ Corresponding author at: Department of Neurology, University HospitalBordeaux, Avenue Magellan, 33604 Pessac cedex, France. Tel.: +33 5 57 65 64 61;fax: +33 5 57 65 66 97.
E-mail address: [email protected] (W.G. Meissner).
Wassilios G. Meissner a,b,c,d,⇑, Olivier Flabeau b, Paul Perez e, Jacques Taillard f,g, Fabienne Marquant e,Sandrine Dupouy a,b, François Tison a,b,c,d, Pierre Philip f,g, Imad Ghorayeb c,d,h
a Centre de référence atrophie multisystématisée, CHU de Bordeaux, Pessac, Franceb Service de Neurologie, CHU de Bordeaux, Pessac, Francec Université de Bordeaux, Institut des Maladies Neurodégénératives, UMR 5293, Bordeaux, Franced CNRS, Institut des Maladies Neurodégénératives, UMR 5293, Bordeaux, Francee CHU de Bordeaux, Unité de Soutien Méthodologique à la Recherche Clinique (USMR), Pôle de santé publique, Bordeaux, Francef Université Bordeaux, Sommeil, Attention et Neuropsychiatrie, USR 3413, Bordeaux, Franceg CNRS, Sommeil, Attention et Neuropsychiatrie, USR 3413, Bordeaux, Franceh Department of Clinical Neurophysiology, University Hospital Bordeaux, France
a r t i c l e i n f o a b s t r a c t
Article history:Received 7 September 2013Received in revised form 20 November 2013Accepted 8 December 2013Available online 21 February 2014
Keywords:Atypical parkinsonismStriatonigral degenerationOlivopontocerebellar atrophyAutonomicRespiratoryPolysomnography
Objective: To assess the diagnostic accuracy of portable polygraphy (PG) for the detection of sleep apnea(SA) in multiple system atrophy (MSA).Methods: Thirty consecutive patients with probable MSA underwent PG (overnight recording of nasalflow, thoracic/abdominal movements and pulse oximetry), followed 4 weeks later by full polysomnogra-phy (PSG) (reference standard). The accuracy of PG was first assessed using the same threshold as for PSG(apnea–hypopnea index [AHI] P 5), then for all possible AHI thresholds using the area under the receiveroperating characteristics (AUROC) curve. Inter-rater reliability of PG was assessed using the kappa coef-ficient.Results: Among 30 patients enrolled, seven were excluded for technical problems on PG or PSG and 23were included in the main analysis. Eight out of 23 had an AHI P 5 on PSG. With the same threshold,sensitivity, specificity, positive and negative predictive values of PG for the diagnosis of SA were 87.5%(95% confidence interval: 47–99), 80% (52–96), 70% (35–93) and 92.3% (64–99), respectively. The kappabetween PG raters was 0.75 (0.49–1.00) indicating good agreement. The AUROC was 0.93 (0.82–1.00). Noassociation was found between sleep and excessive daytime sleepiness questionnaires and SA.Conclusion: Portable PG seems to be valuable for ruling out SA in MSA.
� 2014 Elsevier B.V. All rights reserved.
1. Introduction
Multiple system atrophy (MSA) is a relentlessly progressiveneurodegenerative disorder leading to severe motor disabilityand death after nine years from symptom onset [1]. Autonomicfailure is a prominent feature of MSA and may present withbreathing disorders including sleep apnea (SA); the latter occursin 15–69% of patients (overall mean prevalence of previous studiesis 45% and 39% when considering those with unbiasedrecruitment) [2–8]. Breathing disorders may develop at any stageand the presence of nocturnal stridor is associated with a poor
prognosis in MSA [8]. Moreover, around 20% of MSA patients suc-cumb to nocturnal sudden death which may be related to stridor orother respiratory disturbances including sleep apnea [9]. SA ismostly obstructive, and is mixed or central in some MSA patients[2–8]. Continuous positive airway pressure has been suggested asan effective therapy for SA without distinguishing between central,obstructive or mixed origins [7,10,11].
Limited availability and related cost restrict the systematic useof reference standard full polysomnography (PSG) for SA screeningin MSA. Whereas portable polygraphy (PG) can be easily performedat home, its diagnostic accuracy in MSA patients is unknown. Theprimary objective of this study was the estimation of the accuracyof PG compared with PSG in the diagnosis of SA. The secondary,exploratory objective was to assess the association between

W.G. Meissner et al. / Sleep Medicine 15 (2014) 476–479 477
excessive daytime sleepiness (EDS), nocturnal sleep complaints,Berlin questionnaire scores and the presence of SA in MSA patients.
Table 1Patient characteristics, scores of questionnaires and rating scales, and apnea–hypopnea indices (AHIs) for portable polygraphy (PG) and polysomnography (PSG).
All patients(n = 30 forclinical data,n = 25 for PGand n = 28for PSG)
Patients withPG and PSGdata availablefor mainanalysis(n = 23)
Age (years) 63.9 ± 7.3 64.1 ± 7.5Gender 55.2% male 59.1% maleDisease duration 5.0 ± 2.3 5.2 ± 2.4MSA type 51.7% MSA-P 50.0% MSA-PUMSARS
Activities of daily living (I) 20.0 ± 6.5 19.7 ± 6.7Motor examination (II) 25.7 ± 5.4 25.1 ± 5.9Disability (IV) 2.6 ± 1.2 2.5 ± 1.3
Berlin 0.5 ± 0.6 0.5 ± 0.6AHI P5 on PSG (mean) 0.5 ± 0.5 0.5 ± 0.7AHI <5 on PSG (mean) 0.5 ± 0.7 0.5 ± 0.7
ESS 6.6 ± 3.7 6.4 ± 3.6AHI P5 on PSG (mean) 5.5 ± 3.0 5.8 ± 3.5AHI <5 on PSG (mean) 7.4 ± 4.1 7.1 ± 3.8
PSQI 6.0 ± 3.7 6.8 ± 3.7AHI P5 on PSG (mean) 5.0 ± 3.8 6.0 ± 4.1AHI <5 on PSG (mean) 6.8 ± 3.6 7.3 ± 3.5
PSG (n = 28)a
AHI 15.5 ± 24.3 17.0 ± 26.5AHI if P5 37.9 ± 26.2 46.8 ± 25.5AHI if <5 1.0 ± 1.5 1.1 ± 1.6
Total sleep time (h) 5.3 ± 1.3 5.4 ± 1.2PG (n = 25)b
AHIRater 1 10.0 ± 15.4 10.5 ± 16.0Rater 2 9.5 ± 14.0 10.1 ± 14.4
AHI if P5Rater 1 20.1 ± 19.2 21.3 ± 19.8Rater 2 18.0 ± 15.9 19.1 ± 16.2
AHI if <5Rater 1 2.1 ± 1.3 2.1 ± 1.3Rater 2 1.3 ± 1.4 1.4 ± 1.4
Time (h) spent in bed(lights off to lights on)
8.4 ± 2.1 8.4 ± 2.2
MSA, multiple system atrophy (P, parkinsonism); UMSARS, Unified MSA RatingScale; ESS, Epworth Somnolence Scale; PSQI, Pittsburgh Sleep Quality Index.Data are shown as mean ± SD or percentage.
a PSG-AHI, number of apneas plus hypopneas per hour of sleep.b PG-AHI, number of apneas plus hypopneas per hour of recording (lights off to
light on).
2. Methods
The study received ethics approval (CPP Sud-Ouest et Outre-Mer III 2007-A00499-44, CCTIRS 07.389). All patients gave writteninformed consent before study enrolment. Thirty consecutive MSApatients were prospectively recruited at the French Reference Cen-tre for MSA in Bordeaux between 2008 and 2010. The diagnosis ofprobable MSA was based on established clinical criteria [12] andwas confirmed post mortem in four patients who have died sincethe end of the study.
Clinical assessment included the following scales and question-naires: Berlin Questionnaire, Beck Depression Inventory (BDI), Ep-worth Sleepiness Scale (ESS), Mini Mental State Examination(MMSE), MSA-Quality of Life questionnaire (MSA-QoL), PittsburghSleep Quality Index (PSQI), and Unified MSA Rating Scale (UM-SARS). UMSARS and MMSE were done at both study visits, whereasthe other scales and questionnaires were only assessed at the sec-ond study visit. The ClinicalTrials.gov Registration Identifier isNCT01223144.
2.1. Polygraphy and polysomnography
Patients underwent PG at the first study visit (overnight record-ing of nasal flow, thoracic/abdominal movements and finger pulseoximetry with an Embletta X100, Resmed, Lyon, France), followedfour weeks later by full PSG (reference standard) during an over-night stay in our sleep laboratory at the second study visit. ForPSG, EEG was recorded digitally on a Coherence polysomnograph(Natus Deltamed, Paris, France) and a Brainbox EEG-1042 amplifier(Braintronics, Almere, The Netherlands) using Ag–AgCl electrodeswith a sampling frequency of 250 Hz (0.1 Hz high-pass, 70 Hzlow-pass and 50 Hz notch filter). Electrodes were placed accordingto the 10–20-System with six channels referenced to linked mas-toids (F4–C4–O2–F3–C3–O1). Eye movements, submental andanterior tibialis muscle electromyography, nasal airflow, respira-tory effort (thorax and abdomen) and oximetry were also recorded.
PSGs were interpreted and scored by one (I.G.) and PGs by two(I.G., J.T.) independent investigators. Investigators were blind tothe other test results and clinical data. PG and PSG were scoredaccording to alternative (PSG) and recommended (PG) methodsdescribed in the American Academy of Sleep Medicine manualfor the scoring of sleep and associated events [13]. Accordingly,hypopnea on PSG was considered only when there was a P4% oxy-gen desaturation from pre-event baseline, independently of theassociation with an arousal. We applied the same recommenda-tions for the identification of hypopneas on PG. As the primaryobjective of the study was the estimation of the diagnosis accuracyof PG, we only considered SA as a whole regardless of its central orobstructive nature. Patients with an apnea–hypopnea index(AHI) P 5 on PSG were classified as having SA. Sleep positionwas not specifically adjudicated for PG and PSG. Given their severemotor disability, patients with MSA usually sleep in supineposition.
2.2. Statistics
The primary objective was the estimation of the diagnosticaccuracy of PG (as interpreted by the first rater), when the samethreshold as for PSG was used (PG classified positive when AHI P 5on PG). Ninety-five percent confidence intervals (95% CI) ofsensitivity, specificity, and predictive values were calculated usingthe exact binomial distribution. Inter-rater agreement of PG
interpretation was assessed by calculating the kappa coefficientfor the presence versus absence of SA and the intraclass correlationcoefficient for the quantitative value of AHI, and their confidenceintervals [14,15]. The overall accuracy of PG for all possible AHIthresholds used the area under the receiver operating characteris-tics (ROC) curve and its 95% CI [16].
The association between the presence of SA and scores on Berlinquestionnaires, ESS and PSQI was assessed by Wilcoxon tests forcontinuous variables and by Fisher’s exact tests for categoricalvariables.
All statistical analyses used the SAS� statistical software(v. 9.1.3, SAS Institute, Inc., Cary, NC, USA).
3. Results
Patient characteristics, scale and questionnaire scores are sum-marized in Table 1 for all enrolled patients (n = 30) and for thosewho had both PG and PSG and were therefore included in the mainanalysis (n = 23). Mean disease duration and mean UMSARS sub-scores indicate moderate disease severity for the enrolledpopulation.

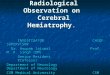
Fig. 1. Receiver operating characteristics curve of the diagnostic accuracy ofpolygraphy in comparison with polysomnography (reference standard) in patientswith multiple system atrophy.
478 W.G. Meissner et al. / Sleep Medicine 15 (2014) 476–479
3.1. Polygraphy and polysomnography
Five PGs and two PSGs could not be interpreted because of tech-nical issues (no recording despite programming in one, dislocationof the nasal cannula in two, and battery failure in two PGs), i.e. 23patients were included in the main analysis. The median time-interval between the two tests was 30 days (1st quartile, 30; 3rdquartile, 35).
Mean AHIs are shown for PG and PSG in Table 1. Eight patientsout of 23 (34.8%) had an AHI P 5 on PSG recordings versus 10(43.5%, rater 1) and 11 (47.7%, rater 2) on PG. When applying anAHI threshold P5 sensitivity, specificity, positive and negativepredictive values of PG for the diagnosis of SA were 87.5% (95%CI: 47–99), 80% (52–96), 70% (35–93) and 92.3% (64–99) for rater1, and 87.5% (47–99), 71.4% (41–91), 63.6% (30–89) and 90.9%(58–99) for rater 2. ROC curve analysis yielded an area under thecurve of 0.93 (0.82–1.00) for rater 1 and 0.90 (0.82–1.00) for rater2 (Fig. 1).
3.2. Inter-rater reliability
The kappa coefficient between both PG raters for the diagnosisof SA was 0.75 (0.49–1.00) indicating good inter-rater agreement.The intraclass correlation coefficient (ICC) for the quantitativevalue of AHI was 0.97 (0.93–0.99) indicating good concordance be-tween both raters. The median range of absolute differences of AHIbetween raters for the same subjects was 1.4 (1st quartile: 1.0; 3rdquartile: 3.5).
3.3. Relationship between SA, sleep quality, EDS and Berlinquestionnaire scores
The results of all patients with available AHI on PSG (n = 28)were included in this analysis.
PSQI scores were not significantly different between patientswith and without SA (P = 0.14). When applying a PSQI cut-off score>5 [17], 27.3% (3/11) with SA and 70.6% (12/17) without had poor
sleep quality. When applying a PSQI cut-off score >8 [18], only18.2% (2/11) with and 23.5% (4/17) without SA had poor sleepquality.
ESS scores were not significantly different between patientswith and without SA (P = 0.11). When applying an ESS cut-off score>10 [19], one patient with SA and 35.3% (6/17) without had EDS.
Berlin questionnaire scores were not significantly different be-tween patients with and without SA (P = 0.72). When applying aBerlin questionnaire cut-off score P2, no patient had a high riskfor SA.
The presence of SA was not different between patients withhigh risk for SA according to the combination of either ESS score>10 or Berlin questionnaire score P2, compared to those with low-er risk (P = 0.19).
4. Discussion
The main result of the present study was that PG had good accu-racy for ruling out a diagnosis of SA when applying an AHI thresh-old of P5 with PSG as reference standard. The results furtherindicate (i) good inter-rater agreement for the diagnosis of SA onPG and (ii) the limited usefulness of clinical measures such asthe ESS and the Berlin questionnaire for identifying MSA patientsat risk for SA. The general characteristics of our cohort in termsof age, gender, disease duration and MSA type were similar com-pared to previous studies [1] and the overall cohort followed atthe French Reference Centre for MSA.
In patients with SA, the analysis of PSG recordings yielded high-er AHIs compared with PG. This may be related to the fact that totalsleep time and nocturnal wake episodes are not quantified on PG.
Around 20% of all patients had poor sleep quality according toPSQI scores when applying a cut-off >8 [18], whereas EDS (ESSscore >10) was observed in four patients. Scores evaluating sleepquality and EDS were not different between groups, suggestingthat SA has only little impact on these symptoms in MSA patients.
Technical failure of PG occurred in five patients. Whereas bat-tery failure is avoidable, the loss of the nasal cannula signal, as oc-curred in two patients, may be more difficult to control. Despitethese technical limitations, portable PG could be easily repeatedfor another night at the patient’s home without adding a majorfinancial burden. The study also has some methodological limita-tions. The estimate of the ICC was high because of the wide rangeof AHI values, whereas the assessment of PG recordings yieldeddifferences in AHI values up to 11.4 between raters. However,these differences were not clinically relevant for the diagnosis ofSA since they mainly occurred in patients with higher AHI. Itshould also be mentioned that PG does not detect or may underde-tect any other forms of sleep-related respiratory breathing abnor-malities such as nocturnal alveolar hypoventilation and nocturnalstridor in patients with MSA, and therefore a subsequent labora-tory study should be recommended when these disturbances aresuspected.
In conclusion, portable PG seems to be a valuable tool for rulingout SA in MSA but improved applicability is needed.
Funding sources
This study was supported by a grant from the French Ministry ofHealth (PHRC, CHUBX 2007/04).
Conflict of interest
The ICMJE Uniform Disclosure Form for Potential Conflicts ofInterest associated with this article can be viewed by clicking onthe following link: http://dx.doi.org/10.1016/j.sleep.2013.12.013.

W.G. Meissner et al. / Sleep Medicine 15 (2014) 476–479 479
Acknowledgement
We are grateful to Aline Maillard for conducting parts of the sta-tistical analysis.
References
[1] Wenning GK, Geser F, Krismer F, Seppi K, Duerr S, Boesch S, et al. The naturalhistory of multiple system atrophy: a prospective European cohort study.Lancet Neurol 2013;12:264–74.
[2] Vetrugno R, Provini F, Cortelli P, Plazzi G, Lotti EM, Pierangeli G, et al. Sleepdisorders in multiple system atrophy: a correlative video-polysomnographicstudy. Sleep Med 2004;5:21–30.
[3] Shimohata T, Shinoda H, Nakayama H, Ozawa T, Terajima K, Yoshizawa H, et al.Daytime hypoxemia, sleep-disordered breathing, and laryngopharyngealfindings in multiple system atrophy. Arch Neurol 2007;64:856–61.
[4] Ghorayeb I, Bioulac B, Tison F. Sleep disorders in multiple system atrophy. JNeural Transm 2005;112:1669–75.
[5] Manni R, Morini R, Martignoni E, Pacchetti C, Micieli G, Tartara A. Nocturnalsleep in multisystem atrophy with autonomic failure: polygraphic findings inten patients. J Neurol 1993;240:249–50.
[6] Plazzi G, Corsini R, Provini F, Pierangeli G, Martinelli P, Montagna P, et al. REMsleep behavior disorders in multiple system atrophy. Neurology1997;48:1094–7.
[7] Iranzo A, Santamaria J, Tolosa E. Continuous positive air pressure eliminatesnocturnal stridor in multiple system atrophy. Barcelona Multiple SystemAtrophy Study Group. Lancet 2000;356:1329–30.
[8] Silber MH, Levine S. Stridor and death in multiple system atrophy. Mov Disord2000;15:699–704.
[9] Shimohata T, Ozawa T, Nakayama H, Tomita M, Shinoda H, Nishizawa M.Frequency of nocturnal sudden death in patients with multiple systematrophy. J Neurol 2008;255:1483–5.
[10] Iranzo A, Santamaria J, Tolosa E, Vilaseca I, Valldeoriola F, Marti MJ, et al. Long-term effect of CPAP in the treatment of nocturnal stridor in multiple systematrophy. Neurology 2004;63:930–2.
[11] Ghorayeb I, Yekhlef F, Bioulac B, Tison F. Continuous positive airway pressurefor sleep-related breathing disorders in multiple system atrophy: long-termacceptance. Sleep Med 2005;6:359–62.
[12] Gilman S, Low PA, Quinn N, Albanese A, Ben Shlomo Y, Fowler CJ, et al.Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci1999;163:94–8.
[13] Iber C, Ancoli-Israel S, Chesson A, Quan S. The AASM manual for the scoring ofsleep and associated events: rules, terminology and technical specifications.1st ed. Westchester (IL): American Academy of Sleep Medicine; 2007.
[14] Blackman NJ, Koval JJ. Interval estimation for Cohen’s kappa as a measure ofagreement. Stat Med 2000;19:723–41.
[15] Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability.Psychol Bull 1979;86:420–8.
[16] DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two ormore correlated receiver operating characteristic curves: a nonparametricapproach. Biometrics 1988;44:837–45.
[17] Buysse DJ, Reynolds 3rd CF, Monk TH, Berman SR, Kupfer DJ. The PittsburghSleep Quality Index: a new instrument for psychiatric practice and research.Psychiatry Res 1989;28:193–213.
[18] Carpenter JS, Andrykowski MA. Psychometric evaluation of the PittsburghSleep Quality Index. J Psychosom Res 1998;45:5–13.
[19] Johns MW. Sensitivity and specificity of the multiple sleep latency test (MSLT),the maintenance of wakefulness test and the Epworth Sleepiness Scale: failureof the MSLT as a gold standard. J Sleep Res 2000;9:5–11.