Embed Size (px)
Citation preview

In this issue
Past Ponderingand Future Predicting inLiverpool
ALPS Testing atGreat OrmondStreet
Understandingthe Changes inPublic Sectorand NHS Pensions andWhat to DoNow
WorkingAcross the EU with Directive2005/36/EC
The Association for Clinical Biochemistry & Laboratory Medicine | Issue 611 | March 2014
ACBNews


About ACB NewsThe Editor is responsible for the finalcontent. Views expressed are not necessarily those of the ACB. EditorDr Jonathan BergDepartment of Clinical BiochemistryCity HospitalDudley RoadBirmingham B18 7QHTel: 07973-379050/0121-507-5353Fax: 0121-507-5290Email: [email protected]
Associate Editors Mrs Sophie BarnesDepartment of Clinical Biochemistry12th Floor, Lab BlockCharing Cross HospitalFulham Palace RoadLondon W6 8RFEmail: [email protected]
Mr Ian HanningDepartment of Clinical BiochemistryHull Royal InfirmaryAnlaby RoadHull HU3 2JZEmail: [email protected]
Dr Derren Ready Microbial DiseasesEastman Dental Hospital University College London Hospitals (UCLH) 256 Gray’s Inn Road London WC1X 8LD Email: [email protected]
Mrs Louise TilbrookDepartment of Clinical BiochemistryBroomfield HospitalChelmsfordEssex CM1 5ETEmail: [email protected]
Situations Vacant AdvertisingPlease contact the ACB Office:Tel: 0207-403-8001 Fax: 0207-403-8006Email: [email protected]
Display Advertising & InsertsPRC Associates Ltd1st Floor Offices115 Roebuck RoadChessingtonSurrey KT9 1JZTel: 0208-337-3749 Fax: 0208-337-7346Email: [email protected]
ACB Administrative OfficeAssociation for Clinical Biochemistry & Laboratory Medicine130-132 Tooley StreetLondon SE1 2TUTel: 0207-403-8001 Fax: 0207-403-8006Email: [email protected]
ACB PresidentProfessor Eric KilpatrickDepartment of Clinical BiochemistryHull Royal InfirmaryAnlaby RoadHull HU3 2JZTel: 01482-607-708Email: [email protected]: @ACBPresident
ACB Home Pagehttp://www.acb.org.uk
Printed by Swan Print Ltd, BedfordISSN 1461 0337© Association for Clinical Biochemistry &Laboratory Medicine 2014
ACBNews
General News page 4
Immunology News page 10
Practice FRCPath Style Calculations page 11
Federation News page 13
European Matters page 15
Meeting Reports page 17
ACB News Crossword page 22
Situations Vacant page 23
Issue 611 • March 2014
The monthly magazine for clinical science
Issue 611 |March 2014 | ACB News
Front cover: Ian Watson lines up with colleagues past and present inLiverpool
EuroLabFocus
The Patient &Laboratory MedicineLiverpool, UK • 7-10 October 2014
Pathology QA Review
A need for transparency, better safety checkson testing, consistency and standardisation ofprocesses and procedures are some of therecommendations made to NHS England in areview into pathology services.Professor Sir Bruce Keogh, Medical Director
of NHS England commissioned Dr Ian Barnes,chair of NHS England’s Pathology QualityAssurance Review Board, to strengthen andrefine the quality assurance process forpathology services in England and to make theprocess more transparent. His request for adetailed and thorough review was promptedby reports of inadequate assurance processesat Sherwood Forest Hospitals NHS FoundationTrust.The review runs to forty-two pages and can
be downloaded at: www.england.nhs.uk/publications/ind-rev �
Iain Percy-RobbACB News is sorry to announce the death of Iain Percy-Robb on 11th February 2014. Iain was one of the key laboratory Scottish
Clinical Biochemists through the 1980s and1990s. �
4 | General News
ACB News | Issue 611 |March 2014
Coming SoonIf you are organising a meeting, want to reportwhat was said at a recent event or havesomething on your mind, why not write anarticle for ACB News. Don’t leave it to theEditor to fill the pages! �
SudokuThis month’s puzzle
Lastmonth’ssolution

ACB News | Issue 611 |March 2014
6 | General News
National Training Course No. 4University of South Wales, Pontypridd30th June – 1st July 2014 Aimed at all Clinical Scientist and Medical Trainees within Clinical Biochemistry to teach subjectsthat are not easily found within textbooks and preparation for FRCPath examination
Course itinerary includes the following key topics:
� Paediatric Metabolic Biochemistry� Biochemistry of Pregnancy� Biochemistry of Newborn� EQA Interpretation and Workshop� CPA/UKAS� Quality Management Systems� Clinical Cases� Essay Writing – Analytical Techniques
The Trainees evening will take place in the Mansell Hall at Llancaiach Fawr Manor on Monday30th June 2014, leading on to an historical tour around the Manor House followed by a threecourse evening meal in the conservatory area.
Costs for ACB Members are: £200 (Residential – 2 nights); £235 (Residential – 3 nights if requiredfor the Tuesday night); and £135 (non-residential).
For further information and to register please visit the ACB meetings page:
www.acb.org.uk
ACB NI Region & ACB in Ireland
Joint Scientific MeetingFriday 11th April 2014
Royal Hospitals Site, Belfast09.00-09.35 Registration and Welcome Refreshments09.35 Opening Remarks
Dr Peter Sharpe, Chair, ACB NI Region
Morning Session ChairDr Peter Sharpe, Southern HSCT09.45 Transforming Your Care
Mrs Pamela McCreedy, Director TYC, Health and Social Care Board10.30 Eating Disorders, Nutrition and the Laboratory
Dr Clodagh Loughrey, Consultant Chemical Pathologist, Belfast HSCT11.15-11.45 Coffee/Tea Break11.45 What is a Realistic and Safe Turnaround Time; Findings of a National Survey
Dr Derek McKillop, Consultant Clinical Scientist, Southern HSCT12.30 Endocrine Hypertension
Dr Una Graham, Specialist Registrar, Metabolic Unit, Belfast HSCT13.15-14.15 Lunch
Afternoon Session ChairProf Maurice O’Kane, Western HSCT14.15 Measuring the Value of Laboratory Medicine
Dr Mike Hallworth, Consultant Clinical Scientist, Shrewsbury15.00 Haemochromatosis: An Overview of Testing and Reporting
Dr Alan Balfe, Principal Clinical Scientist, St James Hospital, Dublin15.45 Stool Calprotectin: A Useful Tool in the Gastroenterologist’s Toolbox?
Dr Seamus Murphy, Consultant Gastroenterologist, Southern HSCT16.30 Closing Remarks
Dr Peter Sharpe, Chair ACB NI Region
Registration: The meeting is free to attend. To register please contact: Meetings Secretary: Dr Jenny Hamilton, Tel: 02890 633164, Email [email protected]
8 | General News
ACB News | Issue 611 |March 2014

General News | 9
Issue 611 |March 2014 | ACB News
Annual General MeetingsWednesday 21st May 2014
Thinktank Birmingham, Events Suite, Level 3, Curzon Street, Birmingham B4 7XG
12.00-13.15 ACB AGM 13.15-13.45 Lunch and refreshments13.45-14.30 Federation AGM
Thinktank Birmingham is a 10 minute walk from Birmingham city centre with closest railway stations being Moor Street on the Marylebone line and New Street.
National Clinical Biochemistry Audit GroupNational Audit MeetingThinktank, Birmingham, 21st May 2014Provisional Programme10.00 Registration and Coffee
Morning session Chair: Annette Thomas10.30 National Audit of Vitamin D Investigation
Ms Helen Verrill, University Hospital of North Tees, Stockton on Tees11.10 Vitamin D Measurement, Its Clinical Usefulness and Abuse
Professor Ian Young, Royal Victoria Hospital, Belfast11.50 Discussion 12.00 Lunch and AGM
Afternoon SessionChair: Teresa Teal14.30 Investigation of ACS, The Clinicians’ Perspective
Dr Richard Body, Consultant in Emergency Medicine, Manchester Royal Infirmary15.10 National Audit of Troponin
Dr Gareth McKeeman, Royal Victoria Hospital, Belfast15.50 A Selection of Local Audits within the UK – selected from Abstracts (3 x 10 mins)16.30 Summary and Proposals for Future National Audits16.45 Close
Full details and online registration will shortly be available at www.acb.org.uk

10 | Immunology News
ACB News | Issue 611 |March 2014
The Immunology Laboratory at Great OrmondStreet Hospital (GOSH) offers a regional servicefor the diagnosis of many rare primaryimmune deficiencies (PID). As a specialistlaboratory, we are always looking to expandour range of tests to reflect the constantidentification of novel proteins and causativemutations of primary immunedeficiency.A recent addition to our test repertoire is a
screening assay for the detection of functionalapoptosis. Defects in cellular apoptosis arelinked to a condition known as autoimmunelymphoproliferative syndrome (ALPS). This isan inherited disorder and patients with ALPShave a wide range of features includingchronic lymphadenopathy, splenomegaly,autoimmune cytopenias and an increased riskof B cell lymphoma.
Secondary Diagnostic Criteria
This assay uses peripheral blood mononuclearcells from the patient and a healthy unrelatedcontrol, which is stimulated for 6-7 days with
anti-CD3 and interleukin-2 (IL-2). The cells arethen stimulated with an anti-Fas antibody totrigger apoptosis. Apoptosis is detected bysurface staining of membrane proteins(Annexin V). Apoptosing cells are positive forAnnexin V but negative for DNA stains (e.g.propodium iodide or 7AAD).ALPS may be considered in patients with
lymphadenopathy and/or splenomegalypersistent for more than 6 months, and whereno malignant or infectious cause is found.Laboratory findings which may support thisinclude polyclonal hypergammaglobulinaemiaand expansion of a unique population ofdouble negative T cells (TCR�+CD4-CD8-). Abnormal lymphocyte apoptosis assay forms
part of the secondary diagnostic criteria forALPS. (Oliveira et al. Blood 2010; 116: 35-40)and is therefore useful in conjunction with theabove clinical and laboratory findings. GOSHImmunology are currently the only laboratoryroutinely offering functional apoptosis assaysfor a diagnostic purpose, although the testmay be offered by other laboratories on anR&D basis. If a diagnosis of ALPS is being queried then
5 mL Lithium heparin blood from the patientand the same from a healthy control should besent for the functional apoptosis assay. If double negative T cells have not alreadybeen investigated these should be measuredlocally or can be measured at GOSH but willalso require an additional 1 mL EDTA bloodfrom the patient. Samples should be receivedwithin 24 hours of being taken.
� The functional apoptosis assay costs£627.38 and results are available in 10 days.The double negative T cell measurementcosts £40.22 and takes 3 days. For moreinformation or to discuss sending samples,please contact the Immunology Laboratoryat Great Ormond Street Hospital on Tel: 020 7829 8835. �
Testing for ALPS at Great Ormond StreetNadia Shahid, Immunology Laboratory, Great Ormond Street Hospital
The screening assay uses a combination of cell culture,cell stimulation and flow cytometry

Practice FRCPath Style Calculations | 11
Issue 611 |March 2014 | ACB News
An adult male (body weight 60 kg) volunteered to donate one of his kidneys to his brother. The pre-opinvestigations included a carefully conducted creatinine clearance with the following results: plasmacreatinine 80 µmol/L, 24h volume 1.45 L and urine creatinine 8.0 mmol/L. The donor operation proceededwithout any problems but a routine blood 24h showed a plasma creatinine concentration of 162 µmol/L.A worried on-call SHO reviewing his result that evening queried whether a creatinine concentration thishigh would be expected so soon after the operation. In order to answer this question calculate:
a) The expected new steady state plasma creatinine concentration.
b) The time taken to achieve 95% of the new steady-state value.
A number of assumptions are necessary:
� Creatinine is cleared predominantly by glomerular filtration, following first order kinetics.� Both kidneys function equally.� Creatinine production by the body remains constant.� Creatinine is confined to the ECF.� Total body water is 60% of body weight and a third of this is located in the ECF.
a) Creatinine clearance = UV P
Since UV is constant it follows that if the clearance is halved then the plasma concentration mustdouble. Therefore the new steady state plasma creatinine concentration is 2 x 80 = 160 µmol/L.
b) Applying the above assumptions, the plasma creatinine concentration will behave exactly as a druginfused at a constant rate and whose clearance follows first order kinetics. The only difference is thatcreatinine arises endogenously within the body rather than being added by infusion. Therefore wecan use the same integrated form of the rate equation as in question 153.
Cp = Vi (1 - e-kd.t)kd
It is important to use the correct units for each term.
Calculation of the elimination rate constant, kd (h-1):
kd = Cl Vd
Where Cl = clearance (L/h) and Vd = volume of distribution (L).
The pre-op clearance can be calculated from the data given:
Cl (L/h) = U(mmol/L) x 1000 x V(L) = 8.0 x 1000 x 1.45 = 6.04 L/hP(µmol/L) x 24 80 x 24
Assuming removal of one kidney halves the clearance the post-op clearance is 6.04/2 = 3.02 L/h
Vd = Body wt (kg) x 60 x 1 = 60 x 60 x 1 = 12 L100 3 100 3
Substituting for Cl and Vd to calculate kd:
kd = Cl = 3.02 = 0.252 h-1
Vd 12
Deacon’s Challenge No 154 – Answer
12 | Practice FRCPath Style Calculations
ACB News | Issue 611 |March 2014
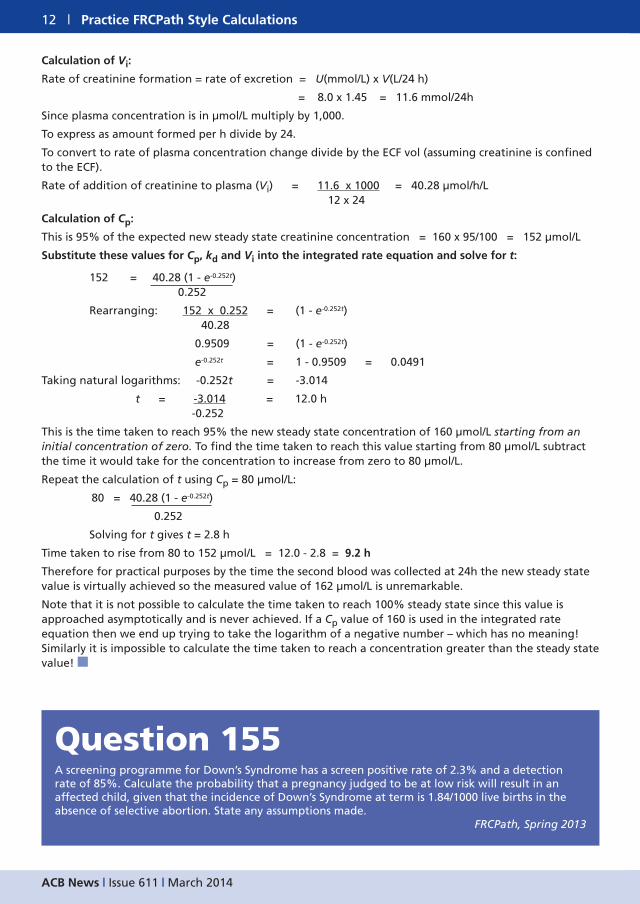
Calculation of Vi:
Rate of creatinine formation = rate of excretion = U(mmol/L) x V(L/24 h)
= 8.0 x 1.45 = 11.6 mmol/24h
Since plasma concentration is in µmol/L multiply by 1,000.
To express as amount formed per h divide by 24.
To convert to rate of plasma concentration change divide by the ECF vol (assuming creatinine is confinedto the ECF).
Rate of addition of creatinine to plasma (Vi) = 11.6 x 1000 = 40.28 µmol/h/L12 x 24
Calculation of Cp:
This is 95% of the expected new steady state creatinine concentration = 160 x 95/100 = 152 µmol/L
Substitute these values for Cp, kd and Vi into the integrated rate equation and solve for t:
152 = 40.28 (1 - e-0.252t)0.252
Rearranging: 152 x 0.252 = (1 - e-0.252t)40.28
0.9509 = (1 - e-0.252t)
e-0.252t = 1 - 0.9509 = 0.0491
Taking natural logarithms: -0.252t = -3.014
t = -3.014 = 12.0 h-0.252
This is the time taken to reach 95% the new steady state concentration of 160 µmol/L starting from aninitial concentration of zero. To find the time taken to reach this value starting from 80 µmol/L subtractthe time it would take for the concentration to increase from zero to 80 µmol/L.
Repeat the calculation of t using Cp = 80 µmol/L:
80 = 40.28 (1 - e-0.252t)
0.252
Solving for t gives t = 2.8 h
Time taken to rise from 80 to 152 µmol/L = 12.0 - 2.8 = 9.2 h
Therefore for practical purposes by the time the second blood was collected at 24h the new steady statevalue is virtually achieved so the measured value of 162 µmol/L is unremarkable.
Note that it is not possible to calculate the time taken to reach 100% steady state since this value isapproached asymptotically and is never achieved. If a Cp value of 160 is used in the integrated rateequation then we end up trying to take the logarithm of a negative number – which has no meaning!Similarly it is impossible to calculate the time taken to reach a concentration greater than the steady statevalue! �
Question 155A screening programme for Down’s Syndrome has a screen positive rate of 2.3% and a detectionrate of 85%. Calculate the probability that a pregnancy judged to be at low risk will result in anaffected child, given that the incidence of Down’s Syndrome at term is 1.84/1000 live births in theabsence of selective abortion. State any assumptions made.
FRCPath, Spring 2013

Federation News | 13
Issue 611 |March 2014 | ACB News
It is very clear that in 2014 we will be forced tothink about our NHS pensions. These remain ahighly valued and valuable part of our rewardspackages but there will be significant changescoming into effect during 2014 and even moreso in 2015 when all public sector pensions willchange to Career Averaged ReadjustedEarnings (CARE) basis. Some of us will havesignificant decisions to make soon and therewill be deadlines that individual schememembers should not miss.As well as changes for individuals there are
major changes in pension scheme governancewhich will involve your FCS representatives.Key elements of legislation enshrined in thePublic Services Pensions Act 2013 will comeinto force in 2014 and 2015. The PSPA2013 put into law for England and Wales (there will be parallel legislation for the Scotland and N Ireland schemes) the recommendationsof the Hutton Public Sector Pensions Review.This is the first, introductory article in a
series FCS will produce this year to give somedetail on what is happening and importantlythe areas you need to consider. The key issuescentrally, currently addressed by the jointPensions Governance Group which is itself asubgroup of NHS Staff Council, are:
� A statutory requirement (formally on theSecretary of State) to set up a PensionsBoard to oversee the operation of thescheme.
� A statutory requirement to set up a SchemeAdvisory Board which will be responsiblefor advising on future changes to thescheme.
� A revaluation of the current liabilities ofthe scheme under a set of regulations setby HM Revenue & Customs (HMRC).
� Finalisation of the regulations andoperational rules for the future 2015 CARE
scheme including protection arrangementsfor those approaching retirement.
� Further work by the joint “Working LongerReview” which has recognised the need tocommission further research into theimpact specifically in the health sector onthose working up to the new retirementages.
� Access to the NHS Pension Scheme byIndependent Providers (non-NHSemployers) primarily providing clinicalservices to the NHS. This directly affects FCSmembers whose employment is transferredinto new developing pathologyarrangements whether or not they involvecommercial sector partners. This is the so-called “New Deal” provision.
Individuals will need to get to grips with:
� Whether and how your existing NHSpensions arrangements are protected forthose approaching (within 10 years or so)retirement.
� For those who will be transferred into the2015 Scheme on 1st April 2015 revisingyour retirement expectations, includingwhen you might retire, and how the twoparts of your pension (the years you havealready accrued and those you accrue inthe 2015 scheme) might work.
� During 2014 those who used their PensionsChoice exercise when the 2008 scheme wasintroduced to stay in the 1995 scheme willbe offered the opportunity for a secondchoice to transfer to the 2008 scheme. This arises because of changes they willexperience to their final retirement agethat had not been suggested when theoriginal choice was made.
� The third year of employee pensionscontributions increases which come into
Public Sector & NHS Pensions. . . Understanding theChanges and What to Do NowGeoff Lester, NHS Staff Council and Pensions Governance Group Representative

14 | Federation News
ACB News | Issue 611 |March 2014
force on 1st April 2014.� Keeping an eye on any deadlines set by HMRC. It is not in your interest to ignore these. You do not get a secondchance.
Where Can I Get Information?
During the year FCS will be producing articleswith more details on these items. You an alsoapproach FCS officers but it is important tonote that we cannot give personal financialadvice which includes decisions about yourpension. Your personal financial advisor oraccountant should be able to help.The NHS Pension Scheme will be producing
lots of literature on paper and on its website.This will start with a pay slip note in January or February. Keep a regular watch on webpages: http://www.nhsbsa.nhs.uk/4017.aspxand the NHS Employers pensions pages:http://www.nhsemployers.org/PayAndContracts/NHSPensionSchemeReview/Pages/NHSPensionScheme.aspx
Important Action Now
The HMRC is reducing the limit of the“Lifetime Pensions Contribution Allowance”.
This is a calculation based on your expectedretirement benefit multiplied by a factor toturn the pension sum into the equivalentcapital you would need to invest to get it plusany other pensions investments you may have.It is the limit of the sum on which you can gettax relief. HMRC are reducing it over a numberof years. For tax year 2012-13 it was £1.8m,2013-14 £1.5m and is reducing to £1.25m in2014-15. If your calculated total lifetimecontribution exceeds the limit then you willhave to pay a levy on the excess.The reduced limit may affect some of the
highest earners. Under certain circumstancesyou qualify to protect yourself at the current£1.5m limit but this must be applied for before 6th April 2014. This is referred to as“Fixed Protection 2014”. Information and links to HMRC are available at:http://www.nhsbsa.nhs.uk/4415.aspx We would strongly recommend that thosewho think they may be affected contact theirfinancial advisors now.
Next time: How does CARE work? What is Pensions Choice 2 about? �

European Matters | 15
Issue 611 |March 2014 | ACB News
After many years gestation EU Directive2005/36/EC (the recognition of professionalqualifications) saw the light of day inDecember 2013 with its passage through theEU’s Parliament, Council and Commission. It will allow professionals to move freely acrossEU member states’ borders in pursuit of newjobs and comes at a time when demand forhighly qualified professionals across the EU isincreasing whilst the labour force is declining.It is key to ensuring a more equitabledistribution of knowledge and skills across theCommunity.For specialists in laboratory medicine in the
UK, the impact is probably more significant onscientific than medical staff. Medical staff(along with groups like architects and dentists)already enjoy the benefits of free professionalmovement through automatic, mutualrecognition of their qualifications. The samecannot be said for scientific staff wishing towork in Europe (or vice versa) where theexperience is often of imposed ‘compensationmeasures’ such as additional degrees, furthertraining and competency tests before access tothe employment market is granted.
Transposition into National Law
With effect from December 2015, the Directivewill be transposed into national law under theSingle Markets Act. Under this act Europeanlaw supersedes national law. The two yeartransposition period allows a minimum of 9 EU member states to work together to shapea common training framework for theirprofession on behalf of all 28 EU memberstates. Linked to individual achievement of the
requirements of a common trainingframework will be the issue of a Europeanprofessional card – effectively a passport foraccessing the EU jobs market. The 2 yeartransposition period is vital to ensuringprofessional ownership of the components ofa framework. Failure to present a commontraining framework may result in one beingimposed by the Commission.
Establishing a Common TrainingFramework for Laboratory MedicineAcross the EU Community
The shape of a framework is the safeguard toensuring high quality, safe laboratorymedicine services for people and patientsacross the Community. The ACB has workedclosely for many years with colleagues in EC4* to develop such a framework inanticipation of the Directive’s passage.Consultant level practice is recognised throughaward of the title Specialist in LaboratoryMedicine when an individual reaches‘equivalence of standards’ with his/her EUcounterparts (the post nominal EuSpLMreplaces EurClinChem with effect from 1st January 2014 – see headline article aboutthis in February’s edition). Approximately 400ACB Members currently hold this title and joinover 3500 colleagues on the EC4 Register. An updated syllabus for education andtraining to include competencies waspublished in 2012 with UK authors being keycontributors. Many of the components of acommon training framework are therealready, a fact recognised by the EUCommission who keenly await specialists in
EU Directive 2005/36/EC: A New Horizon to WorkingAcross the EuropeanCommunity Nuthar Jassam, ACB European Officer & Gilbert Wieringa, EC4 FoundationBoard Chair

16 | European Matters
ACB News | Issue 611 |March 2014
laboratory medicine to be pioneers amongstthe over 600 EU ‘ liberal’ professions.
Where Next?
The task of shaping a common training workhas fallen on EFLM*, in particular its ProfessionCommittee which has established 2 workinggroups – the first to shape a common trainingframework (chaired by NJ), the second tolobby and then present the framework to theEU Commission. Progress is rapid with one EU member state already signed up to shapingthe 2015 version and 15 countries engagingwith their governments. ACB Members in
EFLM and EC4 are playing a key role inpreparing the necessary syllabi acrosslaboratory medicine (not just clinicalchemistry), learning outcomes, competencies,and refining the equivalence of standardscriteria. Update articles on progress withidentifying the 9 member states and how acommon training framework is shaping willfollow in ACB News. EFLM* - the EuropeanFederation of Clinical Chemistry andLaboratory Medicine.EC4* - the European Communities
Confederation of Clinical Chemistry andLaboratory Medicine. �

Meeting Reports | 17
Issue 611 |March 2014 | ACB News
An exciting scientific meeting looking at where we have come from andwhere we are going markedthe retirement of Ian Watson
An interesting mix of the eminent, mainlyretired and close to same, those gallantlytrying to take things forward and the up andcoming, met one fine Friday in late Novemberto celebrate the retirement of Ian Watson. David Holt opened proceedings by looking
at the inception and maturation oftherapeutic drug monitoring (TDM) over theforty years he has worked in the area. The 1960s saw early work on anticonvulsant,antibiotic and antidepressant measurement.GLC gave us technique which was of use inoverdose situations while the introduction ofradioimmunoassay was also harnessed for
drug analysis. Work on digoxin TDMdemonstrated a drug which was very difficultto dose correctly. Even though WilliamWithering had given the use of foxgloveextract digitalis in 1785, still in the 1970s thestrength of digoxin preparations was oftennot always correct. Digoxin dosing graduallyincreased to effective therapeutic levels asdrug measurement helped provide saferadministration.At the New Cross Poison’s Unit in London
new methods were developed and applied todifferent clinical scenarios such as paediatrics,drug interactions, modified releaseformulations and, of course, overdose. Cardiac arrhythmia drugs were given in largeamounts but with the exception ofamiodarone many were stopped when dataanalysis showed that these drugs were notworking as intended. David looked at hisstudies on pharmacokinetics of amiodaronewhere, based on studies of just six volunteers,
Past and Future of ClinicalToxicology and MoreJonathan Berg, Editor
The Glasgow team of Mike Stewart, Ian Watson and Graham Beastall were a powerhouse of the ProfessorGemmell Morgan stable

18 | Meeting Reports
ACB News | Issue 611 |March 2014
they demonstrated the exceptionally longhalf-life and metabolites. Amiodarone toxicitycases led to tissue measurements and helpedto increase understanding but this was intissue samples that certainly would not be soeasy to collect today. In the 1980s the use of mass spectrometry
helped with measurement of drugs such asSirolimus with the enormous variation inexposure in individuals making the TDM useabsolutely clear. With Everolimus in transplantpatients there was a clear 3 ng/mL cut-offabove which the dose must be kept to keepthe likelihood of rejection low. LC-MS/MS sawthe ability to measure much lower levels andenabled lower dose and combination dosedrug concentrations to be properly controlled.The key treatment aim is to arrive at thelowest dose that gives effectiveimmunosuppression. Standardisation of assaysfor drugs such as Tacrolimus has been thecentre of recent work.David pointed to web-based
self-administration as new issues looking aton-line drugs as of great interest and the socalled “generic” drugs generate much work inlooking at what is actually in the tablets.Herbal treatments often contain real drugsrelevant to their treatment claim. Fake drugsare an increasing concern with anti-cancerdrugs containing no active drug. For examplefake arsunate for treating malaria with littleor no active drug.
KIMMS Liverpool Style
Jenny Glaysher looked at pre-analytical qualitystudies. The testing process starts well beforethe sample enters the laboratory. We mustconsider the time of patient review onthrough ordering, phlebotomy, transport andthen into the analytical phase. Jenny pointedout that only 15% of errors occur in theanalytical phase and yet the pre-analysis areahas very little QC oversight. The whole processis important to control and if we are notrecording errors and incidents it is not possibleto act upon pre-analytical errors. Key Incident Monitoring and Management
Systems (KIMMS) is a way of classifying errorsoutside the analytical phase developed in
Australia (www.rcpaqap.com.au/kimms/). At Aintree the approach has been to producea similar approach to KIMMS to report errorsalongside existing reporting systems. Theapproach is aligned to KIMMS and feedbackreports give an overall error rate and thendivide into the different types of error. Jenny compared the Aintree approach withlaboratories that she had visited in Australia.Haemolysis rates varied between KIMMS andthe Aintree system but some of this is due tothe way we actually measure and definehaemolysis. Indeed there are a large numberof variables in the way pre-analysis error ratesare defined and measured and standardisationis required to enable different error ratesystems to be compared.In Australia Jenny observed very different
elements of control over the pre-analyticalprocess. Some organisations had total controlof the pre-analytical approach and also a verystrong attitude to phlebotomy errors with a“three strikes and you’re out” attitude tomistakes. Certainly much more emphasis onthe transport systems for pathology sampleswas also seen. Jenny sees laboratories takingmuch more responsibility for the pre-analyticalprocess with much greater emphasis on acting on data that are collected.Sally Hanton presented her work on an
enzymatic method for ethylene glycolpoisoning undertaken while a trainee at
Jenny Glayser looks at preanalytical error rates

Meeting Reports | 19
Issue 611 |March 2014 | ACB News
Aintree. Ethylene glycol itself is actually notthat toxic but is metabolised to more toxicmetabolites with renal failure being a seriousside effect. Traditional ethylene glycolmeasurement is not easy. The non-directmarkers such as the osmolar and anion gap areoften used along with ruling out other reasonsfor presenting with a high gap. The enzymicassay was developed on the reaction ofglycolate oxidase and a key problem was theinstability of the enzyme which was thencompounded by commercial supplies notbeing available. Not to be thwarted Sally setabout extracting the enzyme from spinach andSally’s home brew enzyme extract worked fine.
Differential Spectrometry is the Future
Bob Flanagan commented on the way IanWatson had managed to take on a careerstraddling both toxicology and biochemistry.Bob also looked at the issues with toxicalcohols and presented differential mobilityspectrometry following membrane extractionas a future way to measure methanol, ethanoland ethylene glycol. This could enable a POCTtest for a preliminary result but what isneeded is a membrane which separates the
alcohols. Bob went on to look at variousaspects of problematic toxicology. ClozapineTDM is of interest as it has become central totreatment. Current innovations in thecalibration of clozapine include internalcalibration on LC-MS/MS used multiple-pointinternal calibration. This innovation has beendriven by the training scheme which hasmeant we have had the investment in traineetime to look at novel ways of applying modernanalytical systems in a clinical toxicologysetting. Bob concluded by pointing out thatquantitative results in toxicology need verycareful interpretation and showed with anumber of examples that results withoutfurther information can be a fool’s paradise.
Into the Future
Graham Beastall, IFCC President, looked at theinternational perspective with future trends inlaboratory medicine. It is never easy to predictthe future but Graham suggested we shouldlook at what the business world think aboutand most directions of travel include asignificant dependence on the clinicallaboratory in many areas of medicine. In IFCC a debate on the global future of

20 | Meeting Reports
ACB News | Issue 611 |March 2014
laboratory medicine is being stimulated with“Shaping the future of Laboratory Medicine”. The concept includes some broad drivers:Globalisation: Instant global communication
with impact on quality standards, laboratorypractice and clinical applications.Technological Advance: Lots of areas impact
on us with robotics, POCT, genomics,proteomics, bioinformatics and massspectrometry all being significant.Economies of Scale: Increased efficiency is
clearly a big driver and is already impacting the UK in particular.Integrated Diagnostics: Laboratory medicine
as part of an integrated approach across thediagnostic field to challenge our silos.Adding value of laboratory medicine:
Aspects such as education, and effectiveness.Patient Centred Care: The informed patient
and the increasing role of personalised careand patient focussed care. Companiondiagnostics will require that you cannot give adrug unless the appropriate tests have beenperformed first. Patients will own their ownpatient care plan and this can include someself-monitoring. These are all huge changes inthe “mindset”.Harmonisation: Another key area on the
world stage. Drivers for harmonisation includepatient safety and empowerment.Accreditation and governance also drive usalong the harmonisation route as do the ITissues and the electronic patient record.Harmonisation is for every phase of theprocess and at local, national andinternational levels. Many of us of course arealready working at local level to harmoniseusing appropriate national advice. A role forharmonised quality indicators is beingconsidered by the IFCC.Innovation: Here is another key future
proof. There are plenty of barriers toinnovation that need to be overcome. Successrequires a business approach where evidencefor change is important. New markers beingapplied in ever more clinical settings are many,but the laboratory also needs to input to howwe deliver new types of service. Embracing change is important and we need
a positive strategy; just like we have when we
move from paper to electronic in our personallives. In Pathology we even have barriers inour names. Some years ago we showed wehad twenty or so names for our disciplines.Within the Pathology department there areproblems with different grades of staff withinthe laboratory and across the world grade-specific societies are set up as barriersbetween staff. Clinical chemistry is sometimesits own entity and sometimes linked withhaematology and transfusion. LaboratoryMedicine seems to be the preferred term butreally not easy to get to. Graham sees changeaplenty ahead in laboratory medicine andsuggests inclusivity is the key. In the questionsthe name issue clearly demonstrated theproblems of harmonised change with a lack ofconsensus quickly surfacing even within thismeeting.
Shaping the Future
Closing the day Mike Hallworth looked at thevalue of tests in different settings. The metricsof value are important. One we all know is thesupposed 70% claim – this being the amountof medical decisions that involve pathology.However, this 70% claim is ill-defined andclearly problematic based perhaps more onwhimsical grabbing of numbers out of the airthan a clear scientific basis. George Lundberg
Mike Hallworth in typical poise

Meeting Reports | 21
Issue 611 |March 2014 | ACB News
has pointed out that clinical outcomes are thekey to the roles of laboratory medicine. Valuemust also equate to the misapplication oflaboratory tests as actually causing harm.Certainly evidence is there for the role of
laboratory medicine. Screening clearly has agood evidential base with, for example, thefaecal occult blood service being clearly shownto be cost effective. In diagnosis a number ofsituations are only decided by the laboratoryresult and this applies to diabetes, cancer anda whole range of other situations. However,we also need to capture what happens withour results which are not diagnostic but at anindividual level make a difference totreatment. In monitoring guidelines thelaboratory is clearly central to many situationsfor example in cardiology out of thirty-four
guidelines all but five have laboratory resultsas part of the process.Mike also pointed to increasingly sensitive
tests actually increasing disease prevalencewith less severe forms of disease and sensitiveTroponin is a good example of this. Mikefinished by running through the huge costsaving of lipid testing to optimise statintreatment. This was a stimulating day with much to
take home and apply locally. Clearly thepioneers of toxicology in the clinicallaboratory were present in numbers but theymust now make way for the next generationto build on their foundations. If this meetingis a forerunner to next year’s EuroLabFocus,then Liverpool is certainly the place to be inOctober 2014. �
Association for Quality Management in Laboratory Medicine
AQMLM is a not-for-profit, mutual support organisation for all those engaged
in the quality management of laboratory medicine.
AQMLM serves the needs of its members; it does not accredit laboratories.
Its aims are to:
� Enhance the status of quality management as a speciality
� Focus equally on analytical as well as process quality
Forthcoming Meetings at the University Research Park, Birmingham
� Tuesday, 13th May 2014: “ISO 15189 - Evidence-based Accreditation”
� Tuesday, 8th July 2014: “Verification and Validation”
Please go to our website at www.aqmlm.org.uk for further information
22 | Crossword
ACB News | Issue 611 |March 2014
Last month’s solutionAcross 6 They display wide ranges of
exceptional carpets (7)7 A neatly altered component
we measure (7)9 More complex traumas
admitted (5)10 Doctor is caustic and intellectually
dishonest (9)11 Abnormal actomyosin fails to
maintain any kind of pressure (7)13 Indicated poor design (6)15 Retraces silly unreliable task in
chemical purification (13)19 Female organ specialist operated,
lost case (6)20 Unbeatable opponent seems in
disarray (7)
23 Dry? Order our shandy! (9)24 Plot of initial growth rate
against plant hormone (5)26 Drunken colleagues want ale
as a source of energy (7)27 Rather superior sort of duct (7)
Down1 Qualifying competition in
theatre (4)2 Sound said to be unmixed (6)3 Metal container for minute
mechanism used to monitorpatient? (5,4)
4 Having a high relative frequency (8)
5 Sits in cosy curious 4 state (10)
6 Holy man brought up populartradition about alcohol (6)
7 Constituent of material used to seal sole to boot (4)
8 Digitise data posted with poem (6)
12 Claylike 14 mineral worked each summer (10)
14 Metal puzzle amusing menwithout number (9)
16 Preordain ingredients lacking a bearing on condensationproduct (8)
17 Got up quickly from secondaccident (6)
18 Model pharmacists reject scrip for a common medical condition (6)
21 Some back horses often;gambling exerts a greatattraction (6)
22 Spot spy (4)25 Cachectic patient admits
discomfort (4)
ACB News CrosswordSet by RugosaWalking Holiday in Austrian Alps Summer 2014The prize this month is an amazing tip for a walking holiday in Austria. Ski companies, in a bid to help summer tourism, offer brilliant holidays using their winter infrastructure. A hot tip is to book late and get remarkable value. For example, www.inghams.co.uk offer the Alpine Palace resort hotel in Hinterglemm.When booked about 6 weeks out this can be had for around £500 per personincluding plane, transfers and full board (breakfast, evening meal and packed walkers lunch) and even a free pass for the mountain lifts and local transport.
H E R A P E U T I C D R U GT
M O N I T O R I N G

Situations Vacant | 23
Issue 611 |March 2014 | ACB News