Embed Size (px)
Citation preview

CLINICAL ARTICLEJ Neurosurg 127:1181–1189, 2017
Publication has become a major criterion of success in the competitive academic environment of neuro-surgery. Research productivity has been linked with
the ability to rise to the upper echelons in the realm of academics. In fact, tenure-track appointment is directly
related to the number of scientific publications of an in-dividual.8,10,12 Citation analysis is a central tool of biblio-metric analysis, which is a statistical method used to quan-titatively analyze scholarly publications. An individual is the usual subject of a bibliometric analysis. However, the
ABBREVIATIONS ACGME = Accreditation Council for Graduate Medical Education; CAST = Committee on Advanced Subspecialty Training; DNV = Det Norske Veritas; h10 index = h index for publications in the last 10 years; h index-dept = departmental h index; h index-neuroendovascular = h index for the neuroendovascular fellowship; JC = Joint Commission; UCLA = University of California, Los Angeles; UCSF = University of California, San Francisco.SUBMITTED July 16, 2016. ACCEPTED September 15, 2016.INCLUDE WHEN CITING Published online January 13, 2017; DOI: 10.3171/2016.9.JNS161857.
Academic impact and rankings of neuroendovascular fellowship programs across the United StatesAshish Sonig, MD, MS, MCh,1,4 Hussain Shallwani, MD,1,4 Bennett R. Levy,4 Hakeem J. Shakir, MD,1,4 and Adnan H. Siddiqui, MD, PhD1–5
Departments of 1Neurosurgery and 2Radiology, Jacobs School of Medicine and Biomedical Sciences, and 3Toshiba Stroke and Vascular Research Center, University at Buffalo, State University of New York; 4Department of Neurosurgery, Gates Vascular Institute at Kaleida Health; and 5Jacobs Institute, Buffalo, New York
OBJECTIVE Publication has become a major criterion of success in the competitive academic environment of neuro-surgery. This is the first study that has used departmental h index– and e index–based matrices to assess the academic output of neuroendovascular, neurointerventional, and interventional radiology fellowship programs across the continen-tal US.METHODS Fellowship program listings were identified from academic and organization websites. Details for 37 pro-grams were available. Bibliometric data for these programs were gathered from the Thomson Reuters Web of Science database. Citations for each publication from the fellowship’s parent department were screened, and the h and e indices were calculated from non–open-surgical, central nervous system vascular publications. Variables including “high-pro-ductivity” centers, fellowship–comprehensive stroke center affiliation, fellowship accreditation status, neuroendovascular h index, e index (h index supplement), h10 index (publications during the last 10 years), and departmental faculty-based h indices were created and analyzed.RESULTS A positive correlation was seen between the neuroendovascular fellowship h index and corresponding h10 index (R = 0.885; p < 0.0001). The mean, median, and highest faculty-based h indices exhibited positive correlations with the neuroendovascular fellowship h index (R = 0.662, p < 0.0001; R = 0.617, p < 0.0001; and R = 0.649, p < 0.0001, respectively). There was no significant difference (p = 0.824) in the median values for the fellowship h index based on comprehensive stroke center affiliation (30 of 37 programs had such affiliations) or accreditation (18 of 37 programs had accreditation) (p = 0.223). Based on the quartile analysis of the fellowship h index, 10 of 37 departments had an neuro-endovascular h index of ≥ 54 (“high-productivity” centers); these centers had significantly more faculty (p = 0.013) and a significantly higher mean faculty h index (p = 0.0001).CONCLUSIONS The departmental h index and analysis of its publication topics can be used to calculate the h index of an associated subspecialty. The analysis was focused on the neuroendovascular specialty, and this methodology can be extended to other neurosurgical subspecialties. Individual faculty research interest is directly reflected in the research productivity of a department. High-productivity centers had significantly more faculty with significantly higher individual h indices. The current systems for neuroendovascular fellowship program accreditation do not have a meaningful impact on academic productivity.https://thejns.org/doi/abs/10.3171/2016.9.JNS161857KEY WORDS bibliometrics; cerebrovascular; citation analysis; e index; endovascular neurosurgery; endovascular surgical neuroradiology; fellowship program; h index; interventional neuroradiology; neuroendovascular surgery; neurointerventional; neurosurgery department; stroke; subspecialty
©AANS, 2017 J Neurosurg Volume 127 • November 2017 1181
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

A. Sonig et al.
J Neurosurg Volume 127 • November 20171182
analysis can be extended to include a department, group, or journal. Several methods have been employed to evalu-ate the productivity of an individual or a department, the commonest of which is the h index.8,10,12 Proposed by a physicist from the University of California, San Diego, Jorge E. Hirsh, the h index is “the number of papers with citation number ≥ h as a useful index to characterize the scientific output of a researcher.”6 Another index that sup-plements the h index is the e index, which was proposed by Zhang.13 The e index accounts for not only all publica-tions that are part of the h index but also the cumulative ci-tations of these publication. Thus, it provides information on ignored citations. Other indices that have been used are the g index3 and the m quotient.8
The number of neuroendovascular and neurointer-ventional fellowship training programs in the US has in-creased in recent years.7 In this scenario, in which more than 50 neurosurgical programs offer these fellowships, it is of paramount importance to assess the academic pro-ductivity of such training programs and to know if ac-creditation with an authority or board has an impact on academic productivity. In the present study, our primary objective was to assess the academic output of neuroen-dovascular and neurointerventional programs across the continental US using h and e index–based matrices. To the best of our knowledge, this is the first study in which departmental academic productivity for this subspecialty has been assessed. An earlier study of pediatric neurosur-gery focused on the h indices of individual faculty mem-bers.9 This method may not be reliable, as faculty can move from one program to another, and thus the results of such an analysis may not reflect the true productivity of the fellowship program. Currently, few neurosurgical fel-lowships are accredited by a formal standardized system. Our secondary aim was to determine if a difference exists in terms of the academic productivity of fellowships with and without accreditation and with and without affiliation with a comprehensive stroke center.
MethodsListings for neuroendovascular, endovascular surgi-
cal neuroradiology, neuroendovascular surgery, and in-terventional neuroradiology fellowship programs were obtained from the websites of the fellowship directories of the American Association of Neurological Surgeons (http://www.aans.org/grants%20and%20fellowships/ fellowship%20directory.aspx), Accreditation Council for Graduate Medical Education (ACGME) (https://apps.acgme.org/ads/public/reports/report/1), and the Commit-tee on Advanced Subspecialty Training (CAST) of the Society of Neurological Surgeons (www.societyns.org/fellowships/NeuroEndovascularNeurosurgery.asp). Only those programs for which a description of a neuroendo-vascular, endovascular surgical neuroradiology, neuro-endovascular surgery, or interventional neuroradiology fellowship was available on the website of the parent de-partment or institution were included in the final analysis (Appendix 2). Thus, institutions offering only a noninter-ventional stroke fellowship were excluded. Additionally, information was gathered on the CAST or ACGME ac-
creditation status of the fellowship program and the af-filiation of the parent department or institution with com-prehensive stroke center certification (Det Norske Veri-tas [DNV; http://dnvglhealthcare.com/hospitals?search_ type=and&q=&c=20806&c=19200&prSubmit=Search] or the Joint Commission [JC; [http://www.strokecenter.org/trials/centers?utf8=L&search=14209]).
Bibliometric data for all years through May of 2016 were gathered from the Thomson Reuters Web of Science citation database (http://login.webofknowledge.com). Because neu-roendovascular training closely involves other departments and neurointerventionists can have a training background in radiology or neurology and neurosurgery, we used the fol-lowing search strings: neurol*surg*(neurological surgery), neurosurg*(neurosurgery), neurolog*(neurology), neuroendovasc*(neuroendovascular), neuroradiol*(neuroradiology), cerebrovasc*(cerebrovascular), and stroke*(stroke). These search strings were attached to the institute’s address strings (Appendix 1).10 Thus, a cumulative h index was generated, which is referred to as the departmental h index (h index-dept) (Table 1).
Calculation of the Neuroendovascular h and e IndicesEach publication citation included in h index-dept was
screened, and the h index for the neuroendovascular fel-lowship (referred to as h index-neuroendovascular) was calculated from citations in the CNS vascular domain, ex-cluding those that were limited to microneurosurgical nu-ances or microneurosurgical surgical anatomy. Similarly, the h index-neuroendovascular for citations during the last 10 years (referred to as h10 index) and the h index of indi-vidual neuroendovascular-trained faculty members at each parent department were calculated. Multiinstitutional data were equally distributed among all included institutes. For example, all institutions that were attributed to the authors of a publication received equal credit for that publication in the calculation of the h index for the department.
Next, h index-neuroendovascular was subjected to quartile analysis. Neuroendovascular fellowship programs falling in the ≥ 75th percentile were labeled as “high-pro-ductivity” centers in terms of academic works. Correlation analysis was done for these high-productivity centers with other parameters, including affiliation with a comprehen-sive stroke center, number of faculty members, accredita-tion status, and “highest” h index of neuroendovascular-trained faculty members from each department.
To calculate the e index, we used the formula13 below:
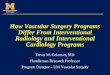
where citj are the citations received by the jth paper (j re-fers to the serial number when the citations are arranged in descending order of the number of times cited) and denotes excess citations within the h core (the h core comprises all articles within the h index).13 Figure 1 illustrates the calcu-lation of the neuroendovascular h, h10, and e indices.
Calculation of Faculty h IndexThe faculty h index was calculated from the Thomson
Reuters Web of Science citation database (http://login.
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

Academic impact and rankings of US neuroendovascular fellowship programs
J Neurosurg Volume 127 • November 2017 1183
TABL
E 1.
Neur
oend
ovas
cula
r fell
owsh
ip ra
nkin
gs b
ased
on
the n
euro
endo
vasc
ular
fello
wshi
p h
inde
x
Institu
tion
Loca
tion
CAST
/AC
GME
Accr
edita
tion
Affili
ation
w/
Comp
rehe
nsive
St
roke
Cen
ter
(JC/D
NV)
Depa
rtmen
tal
h Ind
ex
Neur
oend
ovas
cular
Fe
llows
hip
h Ind
exh1
0 In
dex
e In
dex
No. o
f Ne
uroe
ndov
ascu
lar-
Train
ed
Facu
lty
High
est
h Ind
ex
of Fa
culty
Mea
n h
Inde
x of
Depa
rtmen
t Fa
culty
Med
ian
h Ind
ex
of Fa
culty
Stan
ford
Univ
ersit
ySt
anfo
rd, C
ANo
Yes
187
103
3912
1.35
453
27.5
024
UCSF
San F
ranc
isco,
CANo
No17
582
4011
5.24
674
37.5
036
UCLA
Los A
ngele
s, CA
NoYe
s14
277
4885
.715
5428
.60
22Un
ivers
ity at
Buf
falo
Buffa
lo, N
YYe
sYe
s72
7144
69.14
467
40.2
539
.5Jo
hns H
opkin
s Univ
ersit
yBa
ltimor
e, M
DYe
sYe
s17
764
3374
.215
3013
.80
14W
ashin
gton U
niver
sity
St Lo
uis, M
OYe
sNo
192
6323
89.0
33
4438
.00
40St
. Jos
eph’s
Hos
pital
(Bar
row)
Phoe
nix, A
ZYe
sNo
115
6234
80.01
238
38.0
038
Unive
rsity
of P
ittsbu
rgh
Pitts
burg
h, PA
NoYe
s11
159
3586
.26
427
19.0
017
.5Ne
wYor
k-Pr
esby
terian
/Cor
nell
Unive
rsity
New
York
, NY
NoYe
s14
857
2482
.46
344
21.0
011
Clev
eland
Clin
icCl
evela
nd, O
HYe
sYe
s11
554
2780
.973
2115
.6720
Duke
Univ
ersit
y Hos
pital
Durh
am, N
CNo
Yes
116
4720
49.31
226
17.0
017
Unive
rsity
of Te
xas–
Hous
tonHo
uston
, TX
NoYe
s12
347
2257
.713
2311
.33
6Em
ory U
niver
sity
Atlan
ta, G
AYe
sYe
s13
547
2561
.53
310
9.00
9Un
ivers
ity of
Minn
esot
aMi
nnea
polis
, MN
Yes
Yes
8543
2683
.45
311
9.00
9Un
ivers
ity of
Alab
ama
Birm
ingha
m, A
LNo
Yes
7338
2246
.762
2218
.50
18.5
Unive
rsity
of Ill
inois
at Ch
icago
Chica
go, I
LNo
Yes
5737
1340
.975
2717
.40
13Br
igham
& W
omen
’s Ho
spita
lBo
ston,
MA
NoNo
206
3420
43.0
62
2518
.00
18Ya
le Un
ivers
ityNe
w Ha
ven,
CTNo
Yes
169
328
40.3
23
8438
.33
20Th
omas
Jeffe
rson
Univ
ersit
yPh
ilade
lphia,
PA
Yes
Yes
8231
2652
.63
330
24.3
325
Roos
evelt
Hos
pital
(Mou
nt Si
nai)
New
York
, NY
NoYe
s10
731
1540
.00
436
18.5
017
New
York
Univ
ersit
yNe
w Yo
rk, N
YNo
Yes
109
305
49.0
02
1518
.00
18Un
ivers
ity of
Cali
forn
ia, S
an D
iego
San D
iego,
CANo
Yes
6128
1857
.65
419
9.00
7Un
ivers
ity of
Wisc
onsin
–Mad
ison
Mad
ison,
WI
Yes
Yes
5127
1734
.743
1511
.33
15In
diana
Univ
ersit
yIn
diana
polis
, IN
NoYe
s68
2712
41.51
315
12.3
314
Rush
Univ
ersit
yCh
icago
, IL
Yes
Yes
108
2613
36.19
321
16.3
320
Rutge
rs N
ew Je
rsey
Med
ical
Scho
olNe
wark
, NJ
Yes
Yes
7726
1932
.28
217
13.5
013
.5
Med
ical U
niver
sity o
f Sou
th Ca
rolin
aCh
arles
ton, S
CNo
Yes
5426
2036
.58
418
11.75
11
Unive
rsity
of Te
nnes
see/
Semm
es-
Mur
phey
Clin
icM
emph
is, T
NYe
sYe
s68
228
30.13
39
6.33
9
May
o Clin
ic Ja
ckso
nville
Jack
sonv
ille, F
LNo
Yes
4122
1522
.49
311
9.67
9Un
ivers
ity of
Flor
ida–G
aines
ville
Gaine
sville
, FL
Yes
Yes
3919
1324
.65
333
159
Ceda
rs-S
inai M
edica
l Cen
terLo
s Ang
eles,
CAYe
sYe
s63
1814
33.41
424
14.5
013
CONT
INUE
D ON
PAG
E 11
84 »
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

A. Sonig et al.
J Neurosurg Volume 127 • November 20171184
webofknowledge.com). This index was calculated using the author’s name, irrespective of his or her academic af-filiation.
Statistical AnalysisThe Shapiro-Wilk test was performed to determine
if each of the continuous variables in our study was nor-mally distributed. The continuous variables were h index-neuroendovascular, h10 index-neuroendovascular, number of faculty members, mean h index of faculty, median h index of faculty, and highest h index of faculty. Correla-tions between these variables were evaluated using the Spearman’s rank correlation coefficient. The Wilcoxon-Mann-Whitney test was used to compare the distributions of the continuous variables by group. The chi-square test or Fisher’s exact test was used to evaluate the relationship between categorical variables (i.e., affiliation with a com-prehensive stroke center, accreditation status, and higher productivity center). When the p value was < 0.05, the 2 variables under evaluation were considered to be signifi-cantly related. SAS (version 9.4, SAS Institute) was used for the statistical analysis.
ResultsRankings of Neuroendovascular Fellowships Based on the h Indices
The search revealed a total of 54 fellowship programs, of which details for 37 fellowships were available on the parent institute or department websites. These 37 pro-grams were included in our analysis (Table 1).
The median h index-neuroendovascular was 31 (mean 38.86 ± 22.04; range 12–103). The median of the h10 in-dex-neuroendovascular was 19 (mean 20.32 ± 10.92; range 4–48). The mean number of neuroendovascular faculty members in each department was 3.27 ± 0.962 (range 2–6). Stanford University, University of California, San Francisco (UCSF), University of California, Los Angeles (UCLA), University at Buffalo, and Johns Hopkins Uni-versity had the top 5 rankings based on h index-neuro-endovascular. The h index-neuroendovascular indices for these institutions were 103, 82, 77, 71, and 64, respectively.
Correlation Analysis of Neuroendovascular Fellowship h Indices With Faculty h Indices
Correlation analysis (Table 2) showed a strong positive correlation between the neuroendovascular fellowship h index and its h10 index (rs = 0.885; p < 0.0001). Similarly, the mean, median, and highest h indices of the neuroen-dovascular departmental faculty were positively corre-lated with the neuroendovascular fellowship h index (rs = 0.662, p < 0.0001; rs = 0.617, p < 0.0001; and rs = 0.649, p < 0.0001 respectively). There was a significant correlation between the number of faculty members and the neuroen-dovascular h index (rs = 0.408; p = 0.006) and h10 index (rs = 0.441; p = 0.003). The mean, median, and highest h indices of neuroendovascular departmental faculty were also correlated with the h10 index of the fellowship (rs = 0.568, p < 0.0001; rs = 0.569, p < 0.0001; and rs = 0.541, p < 0.0001, respectively).TA
BLE
1. Ne
uroe
ndov
ascu
lar f
ellow
ship
rank
ings
bas
ed o
n th
e neu
roen
dova
scul
ar fe
llows
hip
h in
dex
Institu
tion
Loca
tion
CAST
/AC
GME
Accr
edita
tion
Affili
ation
w/
Comp
rehe
nsive
St
roke
Cen
ter
(JC/D
NV)
Depa
rtmen
tal
h Ind
ex
Neur
oend
ovas
cular
Fe
llows
hip
h Ind
exh1
0 In
dex
e In
dex
No. o
f Ne
uroe
ndov
ascu
lar-
Train
ed
Facu
lty
High
est
h Ind
ex
of Fa
culty
Mea
n h
Inde
x of
Depa
rtmen
t Fa
culty
Med
ian
h Ind
ex
of Fa
culty
Unive
rsity
of M
iami
Miam
i, FL
Yes
No51
169
32.9
82
1211
.00
11Ha
rtfor
d Hos
pital
Hartf
ord,
CTNo
Yes
2416
1523
.123
75.
336
Alba
ny M
edica
l Cen
terAl
bany
, NY
NoNo
6015
923
.973
2517
.6723
Unive
rsity
of U
tah
Salt L
ake C
ity, U
TYe
sYe
s64
1510
19.18
48
3.25
2.5
The O
hio S
tate
Unive
rsity
Colum
bus,
OHYe
sYe
s73
147
14.97
314
11.0
011
Penn
Sta
te He
rshe
y Med
ical
Cente
rHe
rshe
y, PA
Yes
No57
124
24.91
39
4.33
3
» CON
TINU
ED F
ROM
PAGE
1183
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

Academic impact and rankings of US neuroendovascular fellowship programs
J Neurosurg Volume 127 • November 2017 1185
Comparison of Neuroendovascular Fellowship h Indices With CAST/ACGME Accreditation and With Affiliation to a JC/DNV Stroke Center
Of the 37 fellowships, 18 (48.6%) were accredited by CAST or ACGME, and 30 (81.1%) were affiliated with a JC- or DNV-accredited stroke center. There was no sig-nificant association between the neuroendovascular fel-lowship h indices and CAST/ACGME accreditation or JC/DNV-accredited stroke center affiliation (Table 3).
On the basis of accreditation status, there was no sta-tistically significant difference in the mean or median of the neuroendovascular fellowship h index and h10 index (Table 3). Similarly, on the basis of an affiliation with a JC- or DNV-accredited comprehensive stroke center, there was no statistically significant difference in the mean or median values of those indices.
Comparison of Neuroendovascular Fellowships Based on Productivity
On the basis of the quartile analysis, the 75th percen-
tile of the neuroendovascular fellowship h index was 54. Departments with an h index-neuroendovascular of ≥ 54 were labeled as “high-productivity” centers. Ten (27.0%) centers formed this cohort: Stanford University, UCSF, UCLA, University at Buffalo, Johns Hopkins University, Washington University, St. Joseph’s Hospital (Barrow), University of Pittsburgh, NewYork-Presbyterian/Cornell University, and Cleveland Clinic. In addition, Stanford University had the highest e index (121.35) (Table 1).
The mean number of neuroendovascular faculty mem-bers in the department was significantly higher in neuroen-dovascular fellowship programs with higher productivity (p = 0.013) (Table 4). Moreover, higher productivity fellow-ship programs had significantly higher mean and median neuroendovascular faculty h indices (p ≤ 0.0001 and p ≤ 0.0001). Also, significantly higher productivity was seen in the last 10 years (p < 0.0001). However, higher productivity was not associated with the CAST/ACGME accreditation of the fellowship or its affiliation with a JC/DNV-accred-ited stroke center (p = 0.7140 and p = 0.295, respectively).
FIG. 1. Steps involved in the computation of the departmental h index, neuroendovascular fellowship h index, and e index.
TABLE 2. Correlation coefficients between neuroendovascular fellowship program–related bibliometric variables
VariableFellowship
h Indexh Index From Previous
10 Yrs (p value)No. of Faculty
Members (p value)Highest h Index of Faculty (p value)
Mean h Index of Faculty (p value)
Median h Index of Faculty (p value)
Neuroendovascular fellowship h index
1.00000 0.885 (<0.0001)* 0.408 (0.006)* 0.649 (<0.0001)* 0.662 (<0.0001)* 0.617 (<0.0001)*
Neuroendovascular h index from last 10 yrs
1.00000 0.441 (0.003)* 0.541 (<0.0001)* 0.568 (<0.0001)* 0.569 (<0.0001)*
No. of faculty 1.00000 0.409 (0.006)* 0.188 (0.132) 0.117 (0.246)Highest h index of faculty 1.00000 0.894 (<0.0001)* 0.685 (<0.0001)*Mean h index of faculty 1.000 0.910 (<0.0001)*Median h index of faculty 1.000
* Significant p value.
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

A. Sonig et al.
J Neurosurg Volume 127 • November 20171186
DiscussionTo the best of our knowledge, we have performed the
most detailed bibliometric evaluation to date on the neu-roendovascular subspecialty. Our study is unique for sev-eral reasons. First and foremost, department productivity was analyzed by specifically looking at the subspecialty of interest and using address and subject matter search strings (Appendix 1) to extract publication citations. By screening the citations for publications (Fig. 1) that com-prised the parent department’s h index, we created a new h index (i.e., h index-neuroendovascular) that was based on relevant neuroendovascular publications. This method-ology can be used to study and analyze most fellowship programs in neurosurgery or other specialties across the US. Ponce and Lozano10 compared the academic produc-tivity of American and Canadian neurosurgical training programs using departmental address search strings and concluded that h indices can be useful for comparing aca-demic output across neurosurgery departments. However, their study was limited to neurosurgery and did not in-clude any subspecialty.
Klimo et al.9 used the Scopus (https://www.scopus.com/) and Google Scholar (http://scholar.google.com/) bibliometric databases to profile the academic productiv-ity of individual pediatric neurosurgeons. Their study was mainly an individual authorship–based study in which the h index of a pediatric neurosurgeon was calculated according to his or her name. Those authors also evalu-ated pediatric department productivity for a period of 5 years. The study did not focus on publications pertaining to pediatric neurosurgery alone. For example, a pediatric neurosurgeon might have coauthored several manuscripts
on different topics of interest, but those citations would still be part of his or her h index. Each department was ranked based on the cumulative h and e indices of its cur-rent faculty members; thus, the method may not reflect the department’s productivity. Additionally, faculty members may change from one department to another, which is an-other aspect that was not into taken into account during the ranking of the program.
Accreditation and ProductivityThe accreditation of neurosurgical fellowships is a
“hot” topic in view of a recent increase in the number of programs that offer neuroendovascular or neurointerven-tional fellowships.4 An argument was made to halt fel-lowship training because of a decrease in the volume of procedures and the saturation of larger centers with neu-rointerventionists.4 It was feared that graduating fellows would accept appointments at community hospitals with lower procedure volumes and untrained support staff.
Unlike other specialties (such as obstetrics and gyne-cology, cardiology, vascular surgery, and surgical oncol-ogy) where almost all fellowships are accredited by the ACGME, fellowships in neurosurgery mostly are either unaccredited or accredited by the Accreditation Council for Pediatric Neurosurgical Fellowships (for pediatric neu-rosurgery fellowships) or CAST, which offers accreditation of fellowship programs in the subspecialties of neurocriti-cal care, cerebrovascular neurosurgery, neuroendovascular surgery, spinal neurosurgery, neurosurgical oncology, pe-diatric neurosurgery, peripheral nerve neurosurgery, and stereotactic and functional neurosurgery. Few fellowships in neurosurgery are ACGME accredited.
TABLE 3. Neuroendovascular fellowship and faculty h indices compared by accreditation and stroke center affiliation status and p values (Wilcoxon-Mann-Whitney test)
Affiliation Status No. of Neuroendovascular Fellowship Programs Mean SD Median Min Max p Value
CAST/ACGME Accreditation Status Fellowship h index No 19 42.53 23.64 34.00 15.00 103.00
0.2238 Yes 18 35.00 20.16 26.50 12.00 71.00 h index from last 10 yrs No 19 21.05 11.68 20.00 5.00 48.00
0.7726 Yes 18 19.56 10.92 18.00 4.00 44.00 No. of faculty No 19 3.42 1.12 3.00 2.00 6.00
0.3340 Yes 18 3.11 0.76 3.00 2.00 5.00JC/DNV Stroke Center Affiliation Status Fellowship h index No 7 40.57 28.27 34.00 12.00 82.00
0.824 Yes 30 38.47 20.89 31.00 14.00 103.00 h index from last 10 yrs No 7 19.85 13.55 20.00 4.00 40.00
0.904 Yes 30 20.43 10.82 18.50 5.00 48.00 No. of faculty No 7 3.00 1.41 3.00 2.00 6.00 0.417 Yes 30 3.33 0.84 3.00 2.00 5.00
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

Academic impact and rankings of US neuroendovascular fellowship programs
J Neurosurg Volume 127 • November 2017 1187
In the present study on neurosurgical departments with a neuroendovascular fellowship program, we analyzed if academic productivity correlates with accreditation status (ACGME/CAST). Fourteen fellowships were accredited by CAST, 4 by ACGME, and 2 by both. There was no significant difference in the academic productivity of un-accredited versus accredited programs (p = 0.70). In fact, only 5 of 10 programs in the higher productivity cohort are accredited (Table 1). At present, the accreditation system for endovascular training is fragmented, in part because it is a field populated by 3 different specialties: neurosurgery, neurology, and neuroradiology. Further-more, there is no mandate for academic productivity by any of the participating societies, which stands in contrast to the standard for residency training programs that have research criteria that need to be met prior to the gradua-tion of their residents. To meet the needs of this rapidly evolving field, including the evaluation of indications, techniques, and devices, in addition to expanding hori-zons to new paradigms, research should be embraced as a foundational element of accredited programs. This would serve both to advance and justify the field, as well as to further raise the bar for those who wish to enter it. Our study is a step in that direction. The methods can be used by accreditation bodies to extract the research productiv-ity of endovascular fellowship programs and monitor pre-established goals.
Affiliation With a Stroke CenterThe year 2015 saw the publication of 5 randomized
controlled trials that favored mechanical thrombectomy plus intravenous tissue plasminogen activator over medi-cal management with intravenous tissue plasminogen ac-tivator alone for large-vessel occlusion in the setting of anterior circulation stroke.1,2,5–7 These trials endorsed the superiority of endovascular treatment over medical man-agement alone. As a result, endorsement by the DNV or JC
for comprehensive stroke center status became important for an institution. A recent study has shown that the direct admission of patients to a comprehensive stroke center (as opposed to the transfer of patients from another facility to such a center) is associated with better outcomes and lower hospitalization costs.11
The present study showed that departments affiliated with a JC- or DNV-certified stroke center did not have a significantly higher number of neuroendovascular faculty members (p = 0.417). The small number of nonaffiliated centers (7 of 37 centers) may explain the lack of signifi-cance. Moreover, there is a requirement for a minimum of 2 trained neurointerventionists to staff a certified com-prehensive stroke center, which was met by all affiliated and nonaffiliated centers (Table 1). However, association with a JC- or DNV-certified stroke center did not increase the academic productivity of the department. Even though certification as a primary stroke center started in the year 2003 (https://www.jointcommission.org/certification_for_comprehensive_stroke_centers/), comprehensive stroke center certification is a recent phenomenon. The DNV an-nounced its first comprehensive stroke center in the year 2012 (http://dnvglhealthcare.com/releases/dnv-healthcare-introduces-comprehensive-stroke-center-certification). Because the h index depends on the number of times a paper is cited, it will take some time before the impact of faculty volume is reflected in academic productivity at these comprehensive stroke centers.
h Index-Neuroendovascular and its h10 and e IndicesIn our study, we were able to extract publications spe-
cific to the subspecialty of interest and compute the h10 index. The h index-neuroendovascular correlated sig-nificantly with the number of neuroendovascular faculty members (p = 0.04), the highest h index of the faculty (p < 0.0001), and its mean (p < 0.0001).
TABLE 4. Neuroendovascular fellowship and faculty h indices compared by productivity group (Wilcoxon-Mann-Whitney test)
High Productivity No. of Neuroendovascular Fellowship Programs Mean SD Median Min Max p Value
h index from previous 10 yrs No 27 15.00 6.34 15.00 4.00 26.00
<0.0001* Yes 10 34.70 8.33 34.50 23.00 48.00No. of faculty No 27 3.04 0.76 3.00 2.00 5.00
0.013* Yes 10 3.90 1.20 4.00 2.00 6.00Highest h index of faculty No 27 20.96 14.89 18.00 7.00 84.00
<0.0001* Yes 10 45.20 17.15 44.00 21.00 74.00Mean h index of faculty No 27 13.76 7.03 12.33 3.25 38.33
<0.0001* Yes 10 27.93 10.13 28.05 13.80 40.25Median h index of faculty No 27 12.87 5.86 13.00 2.50 25.00
<0.0001* Yes 10 26.20 11.15 23.00 11.00 40.00
* Significant p value.
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

A. Sonig et al.
J Neurosurg Volume 127 • November 20171188
If one looks at the subgroup analysis of high-produc-tivity centers (Table 4), these centers had a significantly higher h10 index and number of neuroendovascular facul-ty members. The highest and mean faculty h indices were significantly greater at these centers, suggesting more re-sources for research are provided at these centers or that these centers attract faculty members with better research profiles. Further, larger programs have more faculty mem-bers and can spread call and case responsibilities. This might facilitate more “protected time” for research and academic endeavors.
The h10 index depicts academic productivity regardless of the longevity of the program, and thus it negates the natural advantage of older fellowship programs. Our study showed that h10 correlated significantly with h index-neuro endovascular (p < 0.0001) and the mean, median, and highest h index of neuroendovascular faculty mem-bers (Table 2).
The h index bibliometric has been criticized for its in-ability to truly reflect the citation prowess of an individual or an institution. For example, 2 institutions can have the same h index, yet one of these may have manuscripts that have been cited much more often than its h index indicates. These unaccounted for or excess citations can be calcu-lated in the e index. Thus, if 2 institutions have the same h index and one of them has a higher e index, it would mean that the institution with the higher e index had more citations.
The e index needs to be interpreted along with the h in-dex; hence, we did not perform a separate statistical analy-sis of the e index. In our study, Stanford University had the highest neuroendovascular h and e indices, and UCLA had the highest h10 index.
Study LimitationsThis is the first attempt to rank fellowship programs on
the basis of the h indices that specifically pertained to spe-cialty of interest: in this instance, the neuroendovascular subspecialty. Such an analysis is prone to errors, as the de-nominator was based on the address strings of the parent institution or department. It is possible that a completely different abbreviated address could be used by the depart-ment for publication purposes. It is also possible that the Thomson Reuters Web of Science portal may not harbor all of the articles published by the department.
The h index considers overall citations rather than the importance of single contributions, neglects the quality of the content of the publications, and does not consider the context of the citation. It is also influenced by the accuracy of the citation database used for its calculation.
Future PerspectivesThis study included neuroendovascular fellowship pro-
grams in the continental US. The pattern of research pro-ductivity at centers across the globe is different because each country has its own process for accreditation and af-filiation. Moreover, information for fellowships outside the scope of our study is lacking at present. Once more infor-mation is available on websites, the methods enumerated in this manuscript can be used to analyze neuroendovas-cular fellowship programs across the globe.
In addition, the methods applied here can be used as a benchmark for future academic productivity by deter-mining if a correlation exists between the individual pro-ductivity of the graduates of the fellowship program and that of the parent department. The data can be extrapo-lated into various subsets of publication types: clinically oriented (patient outcomes and technology advancement) and basic science oriented (bench research and preclinical in vivo and in vitro work).
ConclusionsOn the basis of the institution’s address and subject
matter strings, a departmental h index can be calculated. Further analysis of the publications that make up the h in-dex could reveal the inclination of a department toward one particular subspecialty and can be used to accurately calculate the h index of a particular specialty. Our analysis was restricted to the neuroendovascular subspecialty, but the methodology can be extended to other neurosurgical subspecialties. The research interests of individual faculty members are directly reflected in the research productivity of a department. The current systems for the accreditation of neuroendovascular fellowship programs do not have a meaningful impact on academic productivity. Publication prowess based on the above-mentioned methods could be given consideration during the process of the accreditation of neuroendovascular fellowships in the future.
AcknowledgmentsThe authors thank Tingting Zhuang, MA, from the University
at Buffalo Department of Biostatistics for statistical analysis, Adri-enne R. Doepp, BA, MLS, from the A. H. Aaron Health Sciences Library at Buffalo General Medical Center for assistance with the search strategy, and Debra J. Zimmer from the University at Buf-falo Department of Neurosurgery for editorial assistance.
References 1. Berkhemer OA, Fransen PS, Beumer D, van den Berg LA,
Lingsma HF, Yoo AJ, et al: A randomized trial of intraar-terial treatment for acute ischemic stroke. N Engl J Med 372:11–20, 2015
2. Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al: Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 372:1009–1018, 2015
3. Egghe L: Theory and practice of the g-index. Scientometrics 69:131–152, 2006
4. Fiorella D, Hirsch JA, Woo HH, Rasmussen PA, Shazam Hussain M, Hui FK, et al: Should neurointerventional fellow-ship training be suspended indefinitely? J Neurointerv Surg 4:315–318, 2012
5. Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al: Randomized assessment of rapid endovas-cular treatment of ischemic stroke. N Engl J Med 372:1019–1030, 2015
6. Hirsch JE: An index to quantify an individual’s scientific re-search output. Proc Natl Acad Sci U S A 102:16569–16572, 2005
7. Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al: Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 372:2296–2306, 2015
8. Khan NR, Thompson CJ, Taylor DR, Venable GT, Wham
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC

Academic impact and rankings of US neuroendovascular fellowship programs
J Neurosurg Volume 127 • November 2017 1189
RM, Michael LM II, et al: An analysis of publication produc-tivity for 1225 academic neurosurgeons and 99 departments in the United States. J Neurosurg 120:746–755, 2014
9. Klimo P Jr, Venable GT, Khan NR, Taylor DR, Shepherd BA, Thompson CJ, et al: Bibliometric evaluation of pediat-ric neurosurgery in North America. J Neurosurg Pediatr 14:695–703, 2014
10. Ponce FA, Lozano AM: Academic impact and rankings of American and Canadian neurosurgical departments as as-sessed using the h index. J Neurosurg 113:447–457, 2010
11. Sonig A, Lin N, Krishna C, Natarajan SK, Mokin M, Hop-kins LN, et al: Impact of transfer status on hospitalization cost and discharge disposition for acute ischemic stroke across the US. J Neurosurg 124:1228–1237, 2016
12. Spearman CM, Quigley MJ, Quigley MR, Wilberger JE: Sur-vey of the h index for all of academic neurosurgery: another power-law phenomenon? J Neurosurg 113:929–933, 2010
13. Zhang CT: The e-index, complementing the h-index for ex-cess citations. PLoS One 4:e5429, 2009
DisclosuresThe authors report the following. Dr. Siddiqui has financial inter-ests in Buffalo Technology Partners Inc., Cardinal Health, Inter-national Medical Distribution Partners, Medina Medical Systems, Neuro Technology Investors, StimSox, and Valor Medical. He serves as a consultant to Amnis Therapeutics Ltd., Cerebrotech Medical Systems Inc., CereVasc LLC, Codman & Shurtleff Inc., Corindus Inc., Covidien (acquired by Medtronic), GuidePoint Global Consulting, Lazarus (acquired by Medtronic), Medina
Medical (acquired by Medtronic), Medtronic, MicroVention, Neuravi, Penumbra, Pulsar Vascular, Rapid Medical, Rebound Medical, Reverse Medical (acquired by Medtronic), Silk Road Medical Inc., Stryker, The Stroke Project Inc., Three Rivers Med-ical Inc., Cerebrotech Medical Systems Inc., and W. L. Gore & Associates. He is a principal investigator or serves on the National Steering Committee for the following trials: Covidien SWIFT PRIME, LARGE, Medtronic SWIFT DIRECT, MicroVention CONFIDENCE trial, MicroVention FRED trial, Penumbra 3D Separator, Penumbra COMPASS, Penumbra INVEST, and POSI-TIVE Trial. He is a member of the board of the Intersocietal Accreditation Committee.
Author ContributionsConception and design: Sonig. Acquisition of data: Siddiqui, Sonig, Shallwani. Analysis and interpretation of data: all authors. Drafting the article: Sonig. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors.
Supplemental Information Online-Only ContentSupplemental material is available with the online version of the article.
Appendices 1 and 2. https://thejns.org/doi/suppl/10.3171/2016. 9.JNS161857.
CorrespondenceAdnan H. Siddqui, Department of Neurosurgery, University at Buffalo, 100 High St., Ste. B4, Buffalo, NY 14203. email: [email protected].
Unauthenticated | Downloaded 06/22/20 12:44 PM UTC