Embed Size (px)
Citation preview
lnt~,rnational Jourmd 0/ Obstetric Anesthesia (2000) 9, 193-212 cO 2000 Harcourt Publishers Ltd
Abstracts of free papers
presented to the
Obstetric Anaesthetists' Association
meeting in Winchester, UK
on 11-12 May 2000
In order to avoid dual application, not all abstracts are included in the International Journal
of Obstetric Anesthesia
193

194 International Journal of Obstetric Anesthesia
001: Maternal heparin concentrations following a "prophylactic" subcutaneous dose
M Cox, DN Lucas, MR Nel, LJ Acton, C Costello, SM Yentis. Chelsea & Westminster Hospital, London.
Introduction: Venous thromboembolism (VTE) is a leading cause of maternal mortality, especially after caesarean section. Heparin requirements are increased in pregnancy, 1 but little information is available about appropriate doses in the puerperium. The Royal College of Obstetricians and Gynaecologists' guidelines on VTE prophylaxis, published in 1995, 2 are not evidence-based, but represent consensus. Our aims were (i) to survey current UK labour practice; (ii) to investigate whether our routine post-caesarean section dose of 5000 U s.c. unfractionated heparin (hep) produces therapeutic plasma levels; and (iii) to determine if there is a safe "window" after this dose for epidural catheter removal, in order to reduce the risk of epidural haematoma. 3
Methods: Phase I: 50 maternity units picked at random were telephoned and the anaesthetist on duty questioned about their VTE prophlaxis protocols. Phase II: After Ethics Committee approval and informed consent, blood was taken from 8 women following caesarean section, at 1, 2, 3, 4, 5, 6, 8, & 10 h after their first dose of 5000 U s.c. heparin. This was analysed using a single-stage anti factor-Xa activity assay (Coamatic Chromogenics) to determine plasma heparin levels.
Results: Phase I: In 32/50 units, heparin was used after all caesarean sections (13 hep; 19 low molecular weight heparin [LMWH]). Eight units used hep or LMWH in high-risk cases only. All these units used heparin at the standard doses for VTE prophylaxis in the non-pregnant population. Only one unit used increased doses (one dose ofhep 7500 U s.c. then enoxaparin 40 mg od). Phase H: None of the blood samples showed any evidence of an antithrombotic effect of heparin.
Conclusion: VTE prophlaxis varies among units in the UK; the majority administering hep or LMWH use the same postoperative doses as for the non-pregnant population. A dose of 5000 U heparin s.c. is inadequate following caesarean section; removing the epidural catheter after this dose therefore does not pose a risk. More work is needed to determine appropriate doses of these drugs in the post-natal population. This study was supported by the Special Trustees of Westminster & Roehampton. DN Lucas was funded by an OAA Fellowship.
References: 1. Barbour. LA, Smith JM, Marlar RA. Heparin levels to guide
thromboembolism prophylaxis during pregnancy. Am J Obstet Gynecol 1995; 173: 1869-73.
2 . Report o f a working party on prophylaxis against thromboembolism in gynaecology and obstetrics. London: Royal College of Obstetricians and Gynaecologists, 1995.
3. Horlocker TT, Wedel DJ. Anticoagulation and neuraxial block: historical perspective, anesthetic implications, and risk management. Reg Anes Pain Med 1998; 23 Suppl 2: 129-34.
002: Supplemental oxygenation for elective caesarean section under spinal anaesthesia
MS Cogliano, VA Clark, AC Graham Simpson Memorial Maternity Hospital, Edinburgh
Introduct ion: Many mothers undergoing elective caesarean section under regional anaesthesia will still routinely receive oxygen by mask. Although a direct proportionality between maternal PaO2 and fetal umbilical PO2 has been demonstrated 1 Kelly et al found no chan~e in cord blood gases, with maternal inspired 35% 02. Our study was designed to investigate if there is a real need to administer oxygen during elective caesarean section under spinal anaesthesia.
Methods: After ethical approval and informed consent, 69 patients were recruited. Standardised spinal anaes thes ia was instituted, and pat ients were randomised into one of three groups: 40% oxygen by mask (O), 4 L/min air by mask (A), and 2 L/min oxygen by nasal cannulae (NC). The study was double-blind with regards to groups O and A. Umbilical vein and artery samples were analysed, Apgar scores were noted, and a visual analogue score (VAS) was used to assess maternal satisfaction for the oxygen device.
Results: Patients' characteristics, spinal-delivery time and Apgar Scores were similar for the three groups. No statistical differences in the cord blood gases were found, most notably none were detected in the POz. Analysis of the VAS demonstrated that the mask both induced feelings of claustrophobia (O vs. NC p<0.0003, A vs. NC p<0.046) and impeded the mother's ability to communicate (O vs. NC p<0.004, A vs. NCp<0.014).
Cord Blood Ana lys i s
J BBuv 02 Air NO 02 A~r NO
Conclusion: Our study demonstrates that for elective caesarean section under spinal anaesthesia, there is no need to administer oxygen. I f compromised placental function is present or suspected, a more patient- acceptable nasal cannulae may be a useful alternative to a facemask. References: 1. Ramanathan S, Ghandi S, Arismendi J, Chalon J, Turndof H.
Oxygen transfer from mother to fetus during cesarean section under epidural anesthesia. Anesth Analg 1982; 61: 576-8 I.
2. Kelly MC, Fitzpatrick KT, Hill DA. Respiratory effects of spinal anaesthesia for caesarean section. Anaesthesia 1996; 51 : 1120- 1122.

Oral presentations 195
003: Evaluation of isotonic 'sport drinks' in labour M Kubli, M Serutton*, G O'Sullivan, P Seed. Departments of Anaesthesia, St.Thomas' Hospital, London & St Michaels Hospital Bristol Introduct ion: Aspiration of gastric contents is an important potential cause of matemal morbidity and mortality. As a result, many obstetric units restrict women to water only during labour. However, some argue that prolonged fasting during labour has never been proven to influence the incidence of pulmonary aspiration and that the metabolic consequences of fasting may be detrimental to the progress and outcome of labour. 1 Consuming a light diet during labour prevents the metabolic response to fasting but also increases gastric volumes. Isotonic drinks empty rapidly from the stomach and may provide a safer calorific altemative to solid food.
Methods : 60 women presenting in early labour (cervical dilatation <5cm) were randomised to receive
• either isotonic drinks (group 1) or water only (group 2) during labour. Plasma beta-hydroxybutyrate (BHB), non-esterified fatty acids (NEFAs) and glucose were measured in early labour (T 1) and at the end of the first stage (T2). Residual gastric volume was assessed within 45 minutes after delivery using an ultrasound scanner to measure gastric antral cross-sectional area. Incidence and volume of vomiting were recorded.
Results: There were no differences between the groups in any maternal or neonatal outcomes of labour. By the end of the first stage of labour (T2) plasma BHB (p<0.001) and NEFA (p<0.005) had increased and plasma glucose (p<0.01) had fallen significantly in the starved group (group 2). Gastric antral cross-sectional areas after delivery were similar in the 2 groups. The incidence of vomiting within the hour of delivery and the amount vomited was also similar. (Table 1)
Table 1: Mean plasma concentrations of BHB, NEFA and glucose (mmol/1) & antral cross-sectional a r e a (mean), percentage of women vomiting and volume vomited (mean).
Glucose BHB NEFA
TI T2 TI T2 T1 T2
gpl (n= 30) 5.33 5.59 0.19 0.11 . 0.65 0.63 gp2 (n = 29) 5.38 4.88 0.3 0.82 0.7 1.0
x-section %0 vomiting Volume area
gpl (n = 30) 4.37cm 2 23% (7/30) 280 ml gp2 ~n = 30) 4.59cm 2 17% (5/30) 215 ml
Conclusion: Isotonic drinks appear to reduce maternal ketosis in labour without increasing gastric volume. References: 1. Ludka L. Fasting during labour. Presented at International
Confederation of Midwives 21st Congress: 1987. 2. Scrutton M e t al. Eating in Labour: A randomised controlled
trial assessing the risks and benefits. Anaesthesia 1999; 54:329- 334.
005: Determining the density of bupivacaine and bupivacaine-opioid combinations at 37°C
SP Hallworth, R Fernando, GM Stocks, A England Dept of Anaesthesia, Royal Free Hospital, London Introduction: The addition of glucose to local anaesthetic solutions is known to increase their density.l Our laboratory-based study aimed to identify the relationship between the final glucose concentration of a solution and its measured density at 37 ° C.
Methods: A density meter (DMA 450, Paar Scientific Ltd) accurate to +0.00001 g ml -~ was used initially to measure the density of plain bupivacaine 0.5% (Antigen) at 37 ° C (+0.01 ° C). Eight ml of this solution was then added to 2 ml of several saline/glucose combinations, calculated to produce final glucose concentrations ranging from 0 to 10 mg ml -~, and their densities were measured. The experiment was then repeated with the 2 ml saline/glucose combinations containing either diamorphine 500 ~tg.ml -~ or fentanyl 10 ~g.ml ~. For each solution tested, a mean value was recorded from five density readings. Data were analysed using two-way ANOVA and linear regression analysis (P<0.05). Resul ts : Glucose produced solutions of predictable density in a linear fashion (figure), upon which opioids had a small but significant effect (P< 0.0001). Regression analysis defined this linear relationship as y = mx + c, where y = desired density of the solution, m = 0.00027 (slope), x = final glucose concentration of the solution and c = density of non-diluted (plain) bupivacaine (intercept on the x-axis).
1.00250 "
1.00200
~1~ 1.00150 -
..~ LOOt~- =
~ .00050
0.99950
~' O Bupivacaine
~ ] ~ 1 ( z~ Bupivacaine / diamolphine
v Bupiwcaine / fentanyl
2 4 6 8 10
Concentration of glucose (nag ml- 1 )
Conc lus ion: Using this formula, local anaesthetic solutions of predictable density can be produced by glucose addition if the initial density of the solution is known. Applications may include creation of solutions of known density and improvement in the interpretation of clinical study data.
Reference 1. Nicol ME, Holdcroft A. Density of intrathecal agents. Br J Anaesth 1992; 60: 60-63.

196 International Journal of Obstetric Anesthesia
006: Anaesthesia for caesarean section in pregnancy-induced hypertension - haemodynamic stability of spinal anaesthesia
VA Clark, G Sharwood-Smith, AVG Stewart Simpson Memorial Maternity Pavilion, Edinburgh
I n t r o d u c t i o n : Despi te con t roversy over the haemodynamically safest block for caesarean section in women with severe pregnancy-induced hypertension (PIH), an increasing number of anaesthetists are now opting for a spinal block. 1 In a previous study, we demonstrated that spinal anaesthesia, compared with epidural block, offers an equally safe and more efficacious option for women with severe PIH, undergoing caesarean section. 2 This study was designed to compare the induced hypotension, as measured by the amount of ephedrine needed, between normotensive women and those with PIH.
Methods: After ethical approval and informed consent, 20 normotensive, and 20 PIH women were recruited. Standardised spinal anaesthesia was instituted and ephedrine was given in boluses of 6 mg if the blood pressure fell more than 20% from the baseline, or the patient exhibited symptoms of hypotension.
,0
z 0 4
2 0 ~
. ,a
Ephedrine requirement during
spinal anaesthesia
[iii~i~i!iiiii~i~iii~iiiiiiiiii~ii~i~iii~iiiii~iiiiiiiiiiiiiii!i~i~iiiii~i~iii~ I
iiiiiiiiiiiiiiiii!ililililililiiiiiiii
Conclusion: Patients in the normotensive group required significantly more ephedrine, 28 (SD 15.0) mg, than did the PIH group, 16 (sd 11.6) mg (P<0.01). This suggests that the hypotension induced by spinal anaesthesia in women with PIH is less than that of normotensives. The past dictat that spinal anaesthesia in women with PIH would result in rapid and detrimental hypotension should now be abandoned. References: 1. Hood DD, Boese RN. Epidural and spinal anesthetics for elective Cesarean section in severely pre-eclamptie parturients. Reg Anesth 1992:17 (suppl): 35. 2. Sharwood-Smith G, Clark V, Watson E. Regional anaesthesia for caesarean section in severe preeclampsia. International Journal of Obstetric Anesthesia 1999; 8: 85-89.
009: Postnatal neurological deficit following regional blockade: a prospective case controlled study A Q Dar, A P C Robinson, G Lyons Obstetric Anaesthesia, St James' University Hospital, Leeds LS9 7TF, UK
Introduction: Up to 1 in 5 women experience postnatal neurological dysfunction.1 The aim of this study was to establish the incidence, nature and significance of postnatal neurological deficits in our unit and explore the role of regional blockade and obstetric intervention.
Methods: In a 12-month prospective case-controlled study with ethics committee approval, at a daily postnatal ward round women reporting motor and sensory disturbances were identified. Women with symptoms (group A) were matched with 2 case controls, one with similar regional blockade and obstetric intervention (group B) and another without intervention (group C). All groups answered structured questions and were examined in a standardised manner.
Results: 3991 women delivered in the study period. 21 women presented from 2618 having regional blockade, one woman presented from 1373 without. There was a significant association between postnatal neurological dysfunction and regional blockade (P=0.001). In group A (N=22) 6 reported combined sensory and motor dysfunction. Of these, 4 met criteria for femoral neuropathy and 2 had foot drop. 16 women complained of purely sensory disturbance: 8 had numbness over buttocks and/or heels (sacral dermatomes), and 3 had numbness in the distribution of the lateral cutaneous nerve of the thigh (meralgia paraesthetica). 3 had patchy numbness over the lower limbs, and one had numbness around a surgical wound. In one woman no deficit was detected. Motor deficits were associated with vaginal delivery (P=0.05). Sacral dermatome numbness was associated with caesarean delivery (P=0.02). In group B (n=21) 2 women had patchy sensory loss, and in group C (n=21) one had femoral neuropathy, 3 had numbness consistent with meralgia paraesthetica and 2 had patchy sensory loss. 17 women in group A completed a 6- month follow up, 14 had full recovery and 3 had only minor symptoms
Conelusions: Postnatal neurological deficits were identified in all groups but those with regional blockade were more likely to present with symptoms. Motor signs and specific sensory loss were readily diagnosed as recognised obstetric mononeuropathies and had a good prognosis. The significance of sacral dermatome numbness was not established but suggests attention should be given to pressure points during caesarean delivery with regional anaesthesia. Non-specific/patchy sensory loss is likely to be of little clinical significance.
References 1. Donnell DO et al. Incidence of maternal postpartum neurologic
dysfunction. Anesthesiology 1994; 81 :AI 127

Oral presentations 197
010: Aortocaval compression: The effect of changing the amount and direction of lateral tilt on maternal cardiodynamics
J Bamber Leeds General Infirmary, Leeds, UK Introduction: Standard anaesthetic references state that a 15 ° degrees lateral tilt is required to alleviate aortocaval compression and prevent its adverse effect on maternal cardiac output and blood pressure) In clinical practice a variety of methods and amounts of lateral tilt are used. 2 The optimal amount of tilt which is both effective but acceptable and tolerated is uncertain. The aim of the study was to determine whether varying the magnitude and direction of lateral tilt led to significant differences in maternal cardiac output.
Methods: Thirty-four women with singleton pregnancies were recruited. This sample size was sufficient to detect ___20% difference in cardiac output at a significance level of 0.05 and power of 0.8. Bioimpedance cardiography (BoMed NCCOM3-R7 monitor) measured cardiac output in each of seven randomly ordered positions: left and fight lateral; supine; left and right lateral tilt of 5 ° and 12.5 ° (the maximum possible lateral table tilt). Statistical analysis was by ANOVA and multiple comparison testing (Bonferroni).
Results: Compared to measurements in the left lateral position, cardiac output was significantly reduced in the right tilt positions (P<O.O1). No significant differences were found between the tilt positions but lower cardiac outputs were found with right tilt positions.
Percentage change in cardiac output w ith position
Ill Left lateral
5 • Left 12.5
° '0uI I -5 []] =Le f t 5
°/° -10 [] Supine
-15 B Right 5
-20 • Right 12.5
DI Right lateral
Conclusion: This study failed to demonstrate any beneficial effect on maternal cardiac output by increasing the magnitude of lateral tilt and questions the common recommendation of 15 ° tilt. Tilt to the left is preferable to tilt to the right. References: 1. Healy TE, Cohen PJ (eds). A Practice of Anaesthesia 6th ed.
London, Edward Arnold 1995; pp 1282-1297. 2. Marx GF. Aortocaval compression. International Journal of
Obstetric Anesthesia 1992; 1: 60-64.

198 • International Journal of Obstetric Anesthesia
P01: Failure of spinal anaesthesia for caesarean section
M Garry, S Davies. Department 'o f Anaesthesia, Singleton Hospital, Swansea, Wales
Introduction: Spinal anaesthesia is the technique of choice for caesarean section but pain is often experienced during the operation, in up to 17% of patients in some series.l The pain may be managed by supplementary analgesia but can be severe enough to warrant general anaesthesia (GA). We were interested to discover the supplementation and conversion rates in our unit over a prolonged period.
Methods: We conducted a 3-year retrospective review of case notes of patients in whom spinal anaesthesia failed. Case notes were identified by the obstetric anaesthetic database. We included anyone who was due to have caesarean section under spinal anaesthesia who subsequently went on to have GA, or anyone who received supplementary analgesia during the caesarean section.
Results: A total of 1114 patients due for spinal anaesthesia were reviewed; 121 patients needed supplementation. Most of these responded to Entonox and a short acting intravenous opioid. Other additional supplementat ion included ketamine, morphine, midazolam and propofol. A total of 39 patients required GA at some stage: data were available on 38. Of these patients 27 (71%) received GA pre-operatively, 15 due to inadequate height of the block, 11 for inability to locate the subarachnoid space and 1 who had paraesthesia on start of injection. Per-operatively only 2 (5%) received GA before delivery, one for pain and the other had a panic attack. After delivery 9 (24%) were received GA, 8 due to pain during caesarean section and one due to pain near the end of a 2.5 h operation involving a complex uterine tear.
Conclusion: This review shows the incidence of pain requiring supplementation during caesarean section under spinal anaesthesia to be 11.1% and intraoperative conversion to general anaesthesia to be 0.83%. These data enable the anaesthetist to give more accurate information to patients, so that better informed consent can be obtained. It also ensures that the patient is aware of the possibility of pain, which is relatively common, and the much smaller chance of conversion to GA. Inadequate consent and management of pain have important implications in the medico-legal environment in which we practice.
References: 1. Riley E T, Cohen SE, Macario A, Desai J B, Ratner E F. Spinal
verus epidural anesthesia for cesarean section: comparison of time efficiency, costs, charges and complications. Anesth Analg 1995; 80: 709-712.
P03: Anx ie ty , skin temperature & materna l h a e m o d y n a m i c s f o l l o w i n g spinal a n a e s t h e s i a for caesarean s e c t i o n
DN Lucas, K Ashworth, PK Barnes, SM Yentis. Chelsea & Westminster Hospital, London, UK. Introduct ion: Vasodilatation following spinal anaesthesia may cause hypotension. We aimed to study whether pre-operative anxiety is associated with severity of hypotension following spinal anaesthesia for caesarean section (CS), and also if skin temperature reflected pre-operative anxiety levels.
M e t h o d s : After local research ethics committee approval and informed consent, pre-operative anxiety was assessed in healthy women undergoing elective CS using the Hospital Anxiety & Depression Scale] Skin temperature (mean of two readings) was measured on the back of the hand with a Genius® infrared thermometer. Routine non-invasive monitoring was applied. After 12 ml/kg intravenous crystalloid preload, patients received 2.2-2.6 ml heavy bupivacaine 0.5% + 15-25 gg fentanyl intrathecally in the sitting'position, using a 27- gauge needle. Patients were placed supine with a 30 ° left lateral tilt using a wedge. Blood pressure (BP) was recorded every 3 min and 6 mg ephedrine given for systolic BP <100 mmHg or decrease in BP (dBP) >20%. Association between dBP or ephedrine/ fluid requirements and anxiety score, and between anxiety score, dBP or ephedrine/fluid requirements and skin temperature, was assessed using Kendall's rank correlation, P<0.05 denoting significance.
R e s u l t s : Values are mean+SD or median (IQR [range]). 77 women were studied, with age 32+5 yrs, weight 66+12 kg, height 164+7 cm and gestation 39+1 wks. Pre-operative anxiety score was 7 (5-9 [2-16]) and skin temperature 30.8+2.6°C. dBP was 31.8+10.6%; crystalloid & ephedrine requirements were 2.0 (1.7-2.0 [1.0-3.0]) 1 and 18 (12-24 [6-54]) mg respectively. There was no association between any of the variables assessed (tau<0.01; P>0.2 for all analyses).
C o n c l u s i o n : We found no association between pre- operative anxiety and severitY of hypotension and its required treatment. This suggests that either anxious patients do not have more vasoconstriction than non- anxious ones, or that the degree of pre-existing vasoconstriction does not affect the severity of hypotension after spinal anaesthesia. Either way, pre- operative assessment of anxiety is not a useful tool for distinguishing patients at risk of severe hypotension. Skin temperature is not a useful marker of pre-operative anxiety, nor does it predict severity of hypotension.
DN Lucas was funded by an OAA Fellowship References: 1. Zigmond AS, Snaith RP. The hospital anxiety and depression
scale. Acta psychiatr Scand 1983; 67: 361-70.

Poster presentat ions 199
P04: Accuracy of the Hewlett-Packard automated blood pressure monitor in pregnancy and pre- eclampsia
K Hunter,* DN Lucas,* N Anim, t P Steer, t SM Yentis* *Magill Dept. of Anaesthesia & tDept, of Obstetrics & Gynaecology, Imperial College School of Medicine, Chelsea and Westminister Hospital, London, UK.
Introduction: Automated blood pressure (BP) monitors may be inaccurate in p r e g n a n c y . ' _ Our aim was to assess the accuracy o f the Hewlett-Packard (HP) M1276A non-invasive BP monitor in pregnant women with and without pre-eclampsia.
M e t h o d s : After local research ethics committee approval and written consent, healthy women (controls) and pre-eclamptics (PE) had their BP taken in the third trimester with a sphygmomanometer/stethoscope (BP-S) and the HP monitor (BP-HP), using the same ann. Mean (SD) differences between BP-S and BP-HP for BP were calculated according to Bland and Altman._ Control and PE groups were compared using the unpaired t-test.
Results: These are shown in the Table: Control PE
n 53 23 Age (years) 29.8 + 4.6 31.5 (5.0) Gestation (weeks) 34.7 + 4.4 34.8 (3.7) Mean (SD) difference for -1.8 (8.8) -2.8 (11.8) systolic pressure (mmHg)* Mean (SD) difference for 8.5 (7.1) 11.3 (10.5) diastolic pressure (mmHg)*
*difference for BP-S minus BP-HP
Discuss ion: Associat ion for the Advancement o f Medical Ins t rumentat ion standards for assessing methods o f measuring BP require a mean (SD) difference o f less than 5 (8) mmHg when compared with a sphygrnomanometer. 4 Our results suggest the HP monitor falls short o f this, along with most other automated devices tested. 1'2 While the HP monitor over- reads systolic BP only slightly, the scatter of differences is large. Conversely, the considerable under-reading of diastolic BP by the HP monitor has implications for the diagnosis and monitoring o f PE, although we were unable to demonstrate its performance was any worse in PE than in healthy pregnant women. DN Lucas was funded by an OAA Fellowship References 1 Gupta M,Shennan AH, Halligan A, Taylor D J, de Swiet M
Accuracy of oscillometric blood pressure monitoring in pregnancy and pre-pregnancy. Br J Obstet Gynaeco11997; 104: 350-355.
2 Brown MA, Robinson A, Buddle ML. Accuracy of automated blood pressure recorders in pregnancy. Aust NZ J Obstet Gynaeco11998; 38: 262-265.
3 Bland JM, Airman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1 : 307- 310.
4. American National Standard. Electronic or automated sphygmomanometers. Arlington, Virginia: AAMI; 1992.
P05: Reducing the incidence of postoperative nausea & vomiting following elective caesarean section under spinal anaesthesia
C Hildyard, J .Freeman, M Dresner Obstetric Anaesthesia, Leeds General Infirmary, Leeds, UK
Introduction: Regional anaesthesia is now used for the majority of elective caesarean sections in the UK, and intrathecal opioids are administered to allow a reduction in the dose of local anaesthetic, whilst also providing post-operative analgesia.1 Audit has revealed a significant incidence of postoperative nausea and vomiting. This study compares the anti-emetic effectiveness of prochlorperazine, cyclizine, and placebo in women undergoing spinal anaesthesia with intrathecal diamorphine for elective caesarean section.
Methods: After ethics committee approval and informed consent, 90 patients were recruited. Patients were randomised to receive either cyclizine 50 mg, prochlorperazine 12.5 mg, or saline 1 ml. The women received our standard spinal anaesthetic technique for caesarean section, and at the end of the procedure patients received the study drug as an intramuscular injection into the anaesthetised thigh. The patients were questioned on the ward at 8 and 24 h about nausea, vomiting, and side effects. Results: There were 30 patients in each of the three groups. The incidence o f nausea and vomiting at 8 and 24 h in these groups is as follows:
Incidence of Nausea & Vomith g E
o4o "5 3O
2010 I ~ / I pr°chl°rperazJne 0 l ~ I [[2 saline
~. Nat8 Vat8 Nat Vat h h 24h 24h
Conclusions: Although not reaching statistical significance, early results indicate that cyclizine reduces the incidence of postoperative nausea and vomiting in comparison to both prochlorperazine and placebo. This effect seems to be greatest in the first 8 hours.
Reference I.Graham D, Russell IF. A double-blind assessment of the analgesic
sparing effect of intratheeal diamorphine (0.3mg) with spinal anaesthesia for elective caesarean section. International Journal of Obstetric Anesthesia 6:224-230 1997

200 International Journal of Obstetric Anesthesia
P06: Post caesarean section pain: a neglected and poorly managed problem.
P Cole, J Charlton, J Freeman, M Dresner Leeds General Infirmary, Leeds, UK
Introduction: Most anaesthetic research into post- caesarean section analgesia concerns itself with the first 4 8 hours after surgery. However , many women experience considerable pain or discomfort for more than a week. With this in mind, and acknowledging the failures of p.r.n, regimens, 1 our postoperative analgesia protocol includes a regular oral analgesic for the first week after caesarean section. Interested in compliance with this protocol, we decided to examine anaesthetists' and midwives' performance.
Methods: The case notes o f 100 women who had undergone elective caesarean section under spinal anaesthesia were reviewed. Each had received in t raopera t ive analgesia o f 300 ~tg intrathecal diamorphine and, when not contraindicated, 100 mg of rectal diclofenac. The written protocol dictated that either diclofenac 50 mg t.d.s, or paracetamol/codeine 1 g/60 mg q.d.s, be prescribed as appropriate. 2 The notes were assessed on the third postoperative day for: a) anaesthetists' compliance in prescribing the drug and b) midwives' compliance in giving it.
Results: Of the 100 women, 9 had no regular analgesia prescribed, despite the written protocol. Of those with a prescription, 2 did not receive all prescribed doses due to refusal or nausea. However, 45% of women with a formal prescription for regular analgesia had doses withheld by midwives, without medical approval. In total, therefore, 49% of our sample did not receive the desired analgesic therapy.
Discussion: Concerns about the quality o f postoperative analgesia were highlighted in a joint college report some l0 years ago. 1 Despite this, our survey suggests that some anaesthetists and many midwives remain to be conv inced about the value o f proac t ive pain management. Not only is this disappointing, but the d i scovery that doc tors ' written instruct ions are commonly ignored is cause for great concern. Obstetric anaesthetists have a responsibility to promote the importance o f good pain relief after caesarean section. It is clear that more research, audit, and education are required.
References 1. The Royal College of Surgeons of England and the College of
Anaesthetists Report of the Working Party on Pain. London: HMSO, 1990.
2. Quick Reference Guide: Guidelines for the use of NSAIDs in the postoperative period: Jan 1998, Royal College of Anaesthetists.
P08: A Comparison of patient controlled analgesia (PCA) using remifentani l with intramuscular pethidine for pain relief in labour
J A Thurlow, C H Laxton, A Dick, P Waterhouse. Department of Anaesthesia, Southmead Hospital, Westbury-on- Trym, Bristol.
Introduction: Pethidine is the most widely used systemic opioid for pain relief in labour; however, it is a poor analgesic and its main effect is sedation. ] Remifentani l is a new opioid with a rapid and predictable onset and offset o f effect 2'3 We compared the analgesic effect o f remifentanil given as PCA during labour with that o f intramuscular pethidine.
Methods: After Ethics Commit tee approval and informed consent 28 women of mixed parity at term were randomly assigned to receive either intramuscular pethidine 100 mg (P) or intravenous remifentanil via PCA (20 p.g bolus over 20 s with a lock-out o f 3 min) (R). Pain scores were assessed using visual analogue scores (0-100). The mother and fetus were monitored continuously.
Results: 14 patients were randomised to each group. Median pain scores before analgesia in groups P and R were comparable. After 60 min of allocated analgesia,
~ain scores were 71 in P, and 48 in R as shown median in Fig.
9 0
| ~ a J n s ~ o r ~
I J [ I
I 1 R e m i f e n t a n l l P e t h i d i n e
Fig.1 Pain scores 60 minutes after treatment given (median, interquartile range and range)
This difference was significant (Mann Whitney U test. P=0.0002). The majority o f mothers described their overall analgesia as 'poor-fair ' in group P and 'good ' in group R; those in group R also commented that they liked 'being in control of their analgesia'.
Conclusion: Our results have shown that remifentanil given via a PCA device can offer better pain relief to mothers in labour than can intramuscular pethidine.
References: 1. Olofsson Ch, Ekblom A, Ekman-Ordeberg G, Hjelm A,
Irestedt L. Lack of analgesic effect of systemically administered morphine or pethidine on labour pain. Br J Obstet Gynaecol 1996; 103:968-972
2. Glass PSA, Hardman D, Kamiyamay, et al. Preliminary pharmacokinetics and pharmacodynamies of an ultra-short- acting opioid: Remifentanil (G187084B) Anesth Analg 1993; 77:1031-1040
3. Selinger K, Nation RL, Smith GA. Enzymatic and chemical hydrolysis of remifentanil. Anesthesiology 1995; 83:A385

Poster presentat ions 201
P09: Patient Controlled Analgesia for Labour using Remifentanil: A feasibility study.
J M Blair, D A Hill, J P H Fee Department of Anaesthetics, Queen's University, Belfast, Northern lreland. Introduction: There is a need for a new alternative to epidural analgesia in labour as pethidine acts primarily as a sedative I and may result in fetal depression. Remifentanil has a rapid onset o f peak effect and a short duration of action independent o f duration of infusion 2 and may therefore be suitable for use in labour.
Methods: After local ethics committee approval and informed consent 21 women in established labour (6 nulliparous; 15 parous) were studied. All patients were aware that remifentanil had not been used in labour before. Blood pressure, heart rate, SaOz, respiratory rate and fetal heart rate were recorded at 5-min intervals. A baseline pain score and the smallest reduction in that score that each woman thought would be worthwhile were recorded using a visual analogue scale (VAS). Pain, nausea, anxiety, sedation and satisfaction were assessed using a VAS at 15-rain intervals. The remifentanil PCA dose increased in a stepwise manner every 15 min if desired unless an adverse event occurred. The bolus doses ranged from 0.25-1.0 ~tg kg -1 (B1-B4) and were given at three levels: level 1 (L1) no infusion, level 2 (L2!1 0.025 I.tg kg 1 min -1 and level 3 (L3) 0.05 ~tg kg -1 min-. Lock-out time was 2 min.
Results: 13 women (62%) used PCA until delivery (2 nulliparous; 1 lparous), 6 changed to regional analgesia (29%) and 2 required caesarean section for failure to progress (9%). 19 women (90%) achieved a reduction in pain score from baseline level (18/19 at L1Blor L1B2). The maximum reductions in pain scores were also achieved at L1Blo r L1B2. 10 women (48%) achieved the reduction in pain score that they had stated would be worthwhile, again occurring at L1Blo r L1B2. In 4 women the SaO2 fell to below 90% for more than 15 s and 2 women had sedation scores of more than 3. These adverse events were transient and occurred in the range L2B2-L3B3. Maternal blood pressure, heart rate and respiratory rate and fetal heart rate did not contravene protocol limits. The mean total dose of remifentanil was 2241 gg (range 340-6120). Apgar scores at 1 and 5 min were 8 (median) and 9 (median) respectively and the mean cord pH was 7.33.
Conclusion: Remifentanil PCA is able to provide safe analgesia for labour using bolus doses in the range o f 0,25-0.5 gg kg -1, without a background infusion. This will probably prove most useful in parous women.
References: 1. Olofsson C, Ekblom A, Ekman-Ordeberg G, et al. Lack of analgesic
effect of systemically administered morphine or pethidine on labour pain. Br J Obstet Gynaeco11996; 103: 968-972.
2. Michelsen LG, Hug CC Jr. The pharmacokinetics of remifentanil. J Clin Anesth 1996; 8: 679-682.
PIO: Does chronic backache cause epidurals for childbirth.
M Tewari, D Kamming, AJ England. Royal Free Hospital, London NW3 2QG
Introduction: Backache has been associated with epidural analgesia for childbirth) However, there is little work investigating the mode o f analgesia used for delivery in women with pre-existing backache.
Methods: We followed women with pre-existing backache that had been sufficiently severe to seek a medical opinion, who had been seen antenatally by a consultant anaesthetist. We compared the choice of analgesia and mode of delivery in this group with that of all the other women who delivered in our unit over a 20 month period from January 1998. Statistical analysis between groups was by ~2 test with Yates correction.
Results: More women with pre-existing backache received anaesthetic input at delivery than in the control group. Women with backache were more likely to deliver by elective caesarean section; their ventouse delivery rate was higher and their spontaneous vaginal delivery rate was lower than controls (table). General anaesthesia was given only to one patient (2%) in the backache group and to 141 (3%) o f the control group, preventing meaningful statistical analysis.
Backache Control P Total deliveries 50 4694 SVD without RA 10% 41.9% <0.00001 SVD + RA 26% 24.4% 0.92 Forceps + RA 2% 2.2% 0.69 Ventouse + RA 16% 5.7% <0.01 Elective CS 28% 10.8% <0.00001 Emergency CS 18% 15.0% 0.40
Discussion: Women with pre-existing backache were more likely to receive anaesthetic intervention for delivery than those without. Concerns of causing further back trauma during labour may have led to their higher elective caesarean section rate. For women in labour the desire to avoid a prolonged active second stage may have led to a lower threshold for recommending early ventouse delivery under epidural by obstetricians. The women with backache may also have had a lower pain threshold, or pathology that made pain more likely. They may also have had a better awareness o f what methods o f pain relief in labour were available following their discussion with an anaesthetist, making it more likely for them to request epidural analgesia.
Reference 1 MacArthur C, Lewis M, Knox EG, Crawford JS. Epidural
anaesthesia and long term backache after childbirth. BMJ 1990;301;9-12

202 International Journal of Obstetric Anesthesia
P12: Knee bend to assess suitability for walking after epidural analgesia in labour
Z Sheikh, G Lyons, APC Robinson Obstetric Anaesthesia, St James's University Hospital, Leeds LS9 7TF. UK.
Introduction: Women with motor sparing after epidural analgesia in labour may be capable o f walking unaided. While accidents are rare, unsteadiness does occur. Breen et al have suggested that a knee bend test would identify women who do not have complete control of their legs) We wanted to evaluate the usefulness of the knee bend test in assessing ability to walk after epidural pain relief in labour.
Methods: After ethics committee approval and patients' consent, 90 women requiring epidural pain relief in labour were recruited in a randomised double blind prospective study to measure the local anaesthetic spar ing e f fec t add ing ep idura l fen tany l to levobupivacaine. Motor block was assessed 30 min after epidural injection using the modified Bromage scale as follows: 0 = no paralysis, full flexion of the knees and ankles 1 = inability to raise extended leg, able to move knees 2 = inability to flex knees able to flex ankle 3 = inability to move lower limb Motor block was recorded for both left and right sides. If the total score was zero, patients were assessed for their ability to stand unaided, perform a knee bend and walk unaided.
Results: The mean (SD) for age (years), height (cm) weight (kg) were 28 (5.7), 164 (5.8) and 77.8 (15.4) respectively. The median value for cervical dilatation was 3 cm [range 2-5] and the median gestational age was 39 weeks [range 37-42]. The table shows the breakdown of motor assessment.
Total no Bromage Stand Able to Walk score zero unaided knee bend unaided
90 38 37 34 33
Five out o f 38 patients were unable to walk having scored zero on the Bromage scale. Out o f these five patients one patient could not stand unaided and three could not perform the knee bend test. One patient able to perform knee bend was still unable to walk.
Conclusion: Walking itself appears to be the only satisfactory test o f ability to walk after epidural pain relief in labour.
References" 1. Breen TW Shapiro T, Glass B, Foster-Payne D, Oriol NE..
Epidural anesthesia for labor in an ambulatory patient. Anesth Analg. 1993; 77: 919-924.
2. Robinson, APC Lyons G, Wilson RC, Sabrine A, Columb MO. Levobupivacaine for extradural analgesia in labour; the sparing effect of extradural fentanyl. Br J Anaesth 1999; 82:Supp.1 A536.
P13: The role of motor block in patient satisfaction with epidural analgesia
J S Charlton, M Dresner and JM Freeman Leeds General Infirmary, Leeds, UK
Introduction: It has become accepted wisdom that mobility is a prerequisite for maternal satisfaction with epidural analgesia. The aim of this study was to test the validity of this assumption.
Methods: With ethics committee approval, 200 women who had received epidural analgesia were interviewed 24 hours after delivery. All had received 0.1% bupivacaine with 2 gg fentanyl. Satisfaction was scored on a 4 point scale, and patients' perception o f motor block on a 6 point scale, as previously described] Those with optimal satisfaction and mobil i ty were not questioned further. Satisfied women with significant motor block were asked: "Although your epidural worked well, it did cause weakness in your legs? Would you have preferred less leg weakness, even if this reduced your pain relief?." Women dissatisfied by excess motor block were asked the same question. Women dissatisfied by poor analgesia were asked: "Using a stronger epidural your pain control might have been better. However, this might have caused more leg weakness. Would you have preferred this?"
Resul t s : 63 women had optimal satisfaction but significant motor block (31.5%). Of these, 95% said they would not exchange analgesia for mobility. Only 6 o f the 200 women (3%) were less satisfied due to significant motor block. Only 1 o f these would have swapped analgesia for mobility. Of the 26 women less satisfied due to poor analgesia, 76% said they would have accepted the price o f motor block for better pain relief.
Discussion: These results suggest that the majority of women in our unit are more concerned with analgesia than mobility. It is clear that for the women studied, mobil i ty is not a prerequisite for satisfaction with epidural analgesia.
References 1. Dresner M, Bamber J, Calow C, Freeman J, Charlton P.
Comparison of low-dose epidural with combined spinal-epidural analagesia for labour. Br J Anaesth 1999; 83:756-760

Poster presentations 203
P14: Comparison of five epidural regimens for labour pain
M Dresner, J Bamber Leeds General Infirmary, Leeds, UK
Introduction: We have compared 5 epidural drug regimens used in 3800 epidurals, all sited with a standard technique. The outcomes were derived from our audit database. Without randomisation and blinding, these data are of limited scientific value, but have helped shape clinical protocols and plan research.
Methods: The five epidural drug regimens were: A: 0.1% bupivacaine with 2 ~tg/ml fentanyl in a 20-ml
loading dose, an infusion of 12 ml/h, with 20-ml top- ups (20/12/20).
B: as regimen A, but initial analgesia with a spinal of 2.5 mg plain bupivacaine with 25 ~tg fentanyl rather than an epidural loading dose (CSE/12/20).
C: as A but smaller drug volumes (15/8/10 ml). D: as B but with smaller volumes (CSE/8/10 ml). E: as C but using 0.2% plain ropivacaine. The regimens were compared using scores from a four point maternal analgesia satisfaction scale (see chart). Statistical analysis was by X 2 test for trend.
Results: Data was available on 1064 women in group A, 738 in group B, 1158 in group C, 318 in group D, and 102 in group E. The ~2 test for trend was highly significant (P<0.001), suggesting a relationship between satisfaction and epidural regimen. Further analysis revealed a significant difference only between the best (group B) and the worst (group C). The figure shows the percentage of women in each satisfaction category for the 5 regimens.
6 0 B E x c e l l e n t
4 0 I I S a t i s f a c t o r y
2 [] < Sa t i s fac to ry
. . . . . ~ ~ E] Unsa t i s fac to ry
C E A D B
Discussion: The ranking of the groups is identical to that seen by combining the results of 2 randomised studies. 1'2 We therefore suggest that audit data have some value in evidence-based practice and feel justified in rejecting the worst regimen (C). Of the four remaining groups, E (ropivacaine) achieved its results without the risks, side effects, and complications of opioids or intrathecal injections. References 1. Dresner M, Bamber J, Calow C, Freeman J, Charlton P.
Comparison of low-dose epidural with combined spinal-epidural analagesia for labour. Br J Anaesth 1999; 83: 756-760.
2. Dresner M, Morris J, Freeman J, Calow C. Is ropivacaine a useful drug for obstetric epidural analgesia? Br J Anaesth 1999; 82:162 (A.540).
P15: No difference in pain and no gain? Analgesic and motor sequelae of ropivacaine 0.2% versus bupivacaine 0.1% plus fentanyl 2 ~tg/ml for epidural analgesia in labour
JD Morrison, J Candy, A Simpson, F Bryden, EM McGrady Royal Maternity Hospital, Rottenrow, Glasgow, UK
Introduction: Ropivacaine may have advantages over bupivacaine in epidural pain relief in labour with a greater dissociation of sensory and motor effects. ] We report a prospective, double-blind, randomised study to compare the analgesic and motor effects of ropivacaine 0.2% with the standard epidural preparation of bupivacaine 0.1% plus fentanyl 2 ~tg/ml which is used in labouring parturients at our institution.
Methods: After ethics committee approval and with written informed consent, 67 women were recruited and randomised to receive one of the following initial bolus preparations: group A (33 women)- 15 ml of ropivacaine 0.2%, group B (34 women)- 15 ml of bupivacaine 0.1% plus fentanyl 2 ~g/ml. Patients received 10-ml top-ups of respective preparations on request. Analgesia was measured on a 100-mm visual analogue scale (VAS). Motor power was assessed using a modified Bromage score. Data are expressed as mean + SEM and the Mann-Whitney U tests is applied.
Results: Time between VAS Bromage top-ups (min) (mm) Score
Group A 73.3+5.30 32.2+2.31 0.37+0.08 Group B 55.8+4.54 36.9+2.93 0.1+0.05 P 0.0045 0.25 0.0019
Conclusion: These data show that there are no appreciable differences in the analgesic effects of ropivacaine 0.2% when compared with the standard preparation of bupivacaine 0.1% plus fentanyl 2 ~g/ml in use at our institution. While 0.2% ropivaeaine provided longer lasting analgesia surprisingly it produced significantly more motor blockade than bupivacaine 0.1% plus fentanyl 2 ~tg/ml. This may have important clinical implications.
Reference
1. Cederholm I. Preliminary risk-benefit analysis of ropivacaine in labour and following surgery. Drug Safety 1997; 16:391-402
204 International Journal of Obstetric Anesthesia
P16: Response time for regional analgesia in labour: comparison of teaching and district general hospitals
S Rutter, C Skinner, S Comara*, R Russell. Nuffield Department of Anaesthetics, Oxford Radcliffe Hospitasl NHS Trust, Oxford, OX3 9DU, UK. *Department of Anaesthetics, Milton Keynes General Hospital NHS Trust, Milton Keynes, MK5 6LD, UK Introduction: 90% of UK hospitals currently provide 24-hour epidural service with an average epidural rate of 24%. 1 It has been recommended that time from informing the anaesthetist of the mother's request until
• • 2 attendmg the woman should not exceed 30 mm. In a prospective study we assessed the difference between a teaching (TH) and a district general hospital (DGH) in response times for regional analgesia in labour.
Methods: In each hospital 100 consecutive blocks in labour were studied. Anaesthetists recorded time of maternal request (TR), being informed (Ti), attending the woman (TA) and time of loading dose (TL).
Results: Both hospitals provide 24-hour pain relief service in labour. Delivery rate per year in TH is 6500, compared with 3200 in DGH. Dedicated anaesthetic cover is available in TH, b u t is shared in DGH. The rate of regional blocks in labour in TH group was 5.9 per day and 1.6 per day in DGH. In TH 91% of women were attended within 30 min of the anaesthetist being informed, (median T~-TA interval 5 min, interquartile range 5-14 min). Findings in DH were almost identical: 91% (median 10 min, interquartile range 5-15 min). Causes for delays included waiting for blood results, shortage of trained midwives, anaesthetist being busy (3 occasions in TH and 9 in DGH). 74% of women were attended within 30 min of the mother's requesting epidural analgesia in TH and 66% in DGH. Other time intervals are summarised in the table: Time, min median (interquartile range)
TH re'nun DGH arouo TR-T~ (min) 5 (5-15) 5 (5-20) TR-TA(min) 15 (10-30) 20 (10-40) TA-TL (min) 20 (15-30) 24 (15-30) TR-TL (min) 40 (28-55) 45 (30-60)
Discussion: Despite different workload and manpower between hospitals, OAA standards on response times for regional blocks in labour were achievable in most cases. Time from mother's request to administration of the loading dose may be a better marker of quality of anaesthetic service. Optimising this time requires effort from both midwives and anaesthetists. References: 1. Bumstein R, Buckland R, Pickett JA. A survey of epidural
analgesia for labour in the United Kingdom• Anaesthesia 1999;7:634-640•
2. Guidelines for obstetric anaesthesia services. Association of Anaesthetists of Great Britain and Ireland and Obstetric Anaesthetists Association. London 1998.
PI7: Evaluation of a spinal needle locking device for use with the combined spinal epidural (CSE) technique
GM Stocks, SP Hallworth, R Fernando Dept of Anaesehesia, Royal Free Hospital, London. Introduction: The needle through needle technique is a popular method of performing a CSE. The detection of CSF in the spinal needle hub and immobilisation of the spinal needle during injection are essential. A failure rate of 10% has been quoted using this technique and this may partly be due to accidental spinal needle movement. ~ A new spinal needle locking device has become available (CSEcure®, sIMS Portex) which allows the spinal needle to be locked within the epidural needle to prevent movement after dural puncture. The aim of this study was to compare this new locking needle system with the conventional (non-locking) CSE technique.
Methods: Following ethics committee approval, 200 labouring women requesting regional analgesia were randomly allocated into one of two groups, with a CSE performed using either a standard technique or using the new locking device. Anaesthetists of varying experience performed the CSE using bupivacaine 2.5 mg with fentanyl 5 g g for the intrathecal injection. Data collection included the analgesic success of the spinal injection, ease of use (5 point scale; 5=excellent, l=poor), presence of"dural click" and detection of CSF in the spinal needle hub. Statistical analysis included t- test, Mann Whitney and X 2 (P<0.05).
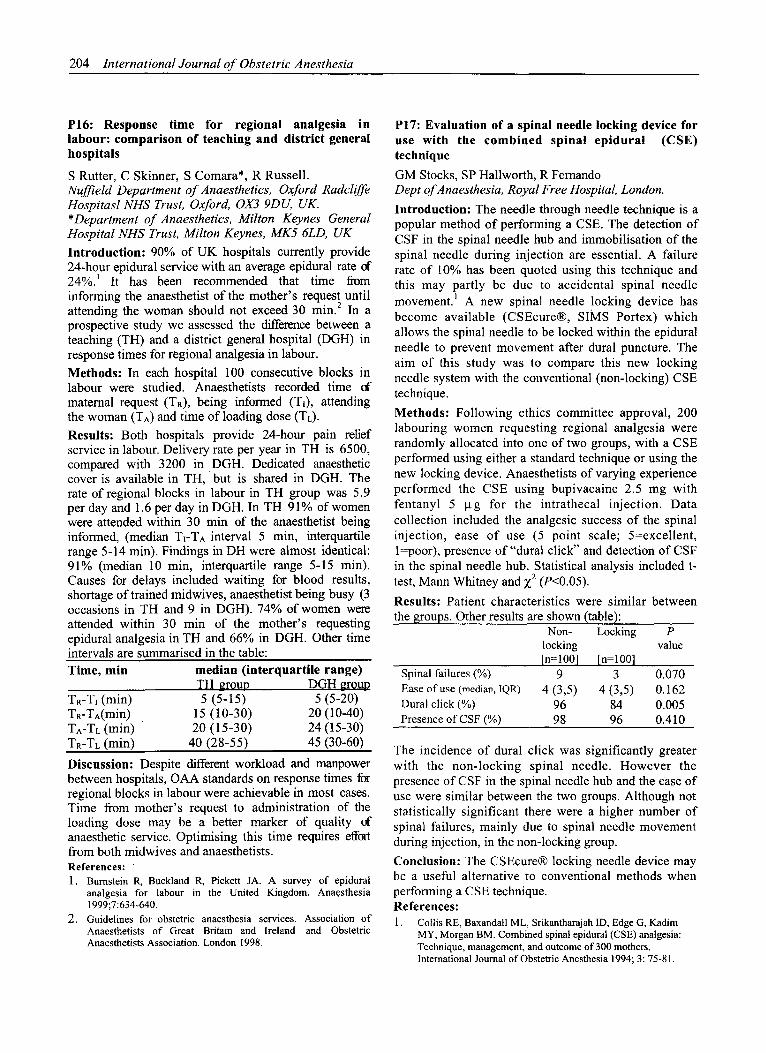
Results: Patient characteristics were similar between the groups. Other results are shown (table):
Spinal failures (%) Ease of use (median, IQR) Dural click (%) Presence of CSF (%)
Non- Locking P locking value [n=100] [n=100 l
9 3 0.070 4 (3,5) 4 (3,5) 0.162
96 84 0.005 98 96 0.410
The incidence of dural click was significantly greater with the non-locking spinal needle. However the presence of CSF in the spinal needle hub and the ease of use were similar between the two groups. Although not statistically significant there were a higher number of spinal failures, mainly due to spinal needle movement during injection, in the non-locking group.
Conclusion: The CSEcure® locking needle device may be a useful alternative to conventional methods when performing a CSE technique• References: 1. Collis RE, Baxandall ML, Srikantharajah ID, Edge G, Kadim
MY. Morgan BM. Combined spinal epidural (CSE) analgesia: Technique, management, and outcome of 300 mothers• International Journal of Obstetric Anesthesia 1994; 3:75-81.

Poster presentations 205
P18: Dural taps: has Caiman opened the flood- gates?
G Sommerville, JJS Ruston, R Femando, A England. Royal Free Hospital, London NW3 2QG.
Introduction: Our computerised audit reveals a progressive fall in inadvertent dural puncture rate (IDPR) since 1990. In 1998 the first 'Calman' trainees were allocated to the labour ward and the IDPR increased considerably. We devised a plan to identify the cause and to correct this increase in morbidity.
Methods: From 1990 to 1994 the highest IDPR was by locums (2.2%) and the lowest by senior registrars (SR) (0.4%) and consultants (0.7%). But between January and May 1998 Calman trainees achieved an IDPR of 2.6%. Because those with the highest IDPR were usually new to the labour ward, we postulated that these results reflected a lack of familiarity with equipment and organisation rather than deterioration in the ability of trainees, w e therefore standardised epidural packs and local anaesthetic solutions for labour, reinforced the existing protocols and introduced a program of intensive, consultant-supervised training and assessment for SHOs with 9-15 months of training. When competent they were introduced to the labour ward on- call rota, with SR supervision. This increased the pool of competent in house trainees and removed the need for external locum anaesthetists.
Results: The IDPR fell from 1.7% in 1990 to 0.5% in 1997 (data from 1996 were incomplete). From January to May 1998 the IDPR was 2.5%, with peaks in March and May associated with large variations in anaesthetic personnel. After the changes introduced in June 1998 the IDPR fell significantly, from 2.5% to 0.5% [Fishers exact test, P = 0.00004].
2 5
2
=~15
05
0
Inadxettcnt Dtnal Puncture Rates From 1990 ~o 1999
. . . . . i i i n 1990 1991 1992 1 1994 1995 1997 Jan Jun
May 1998 1998 199.
Discuss ion: Our results support the hypothesis that a high turnover may result in increased morbidity. We suspect the high turnover of trainee anaesthetists associated with the introduction of Calman training in early 1998 caused the increase in IDPR. By providing greater emphasis on training, supervision and regulation of equipment, protocols and staffing we have reversed this unwanted increase in anaesthetic morbidity.
P19: Survey of epidural technique and accidental dural puncture rates among obstetric anaesthetists.
EW Moore, CM Cowan. University Department of Anaesthesia, Duncan Building, Liverpool L69 3GA. Introduction: Inadvertent dural puncture has been attributed to various aspects of epidural insertion technique] A survey was designed to examine the association between components of catheter insertion technique and personal accidental dural puncture rates.
Methods: 500 members of the Obstetric Anaesthetists' Association were asked to complete a questionnaire comparing: experience of the anaesthetist; frequency of performing the technique; rotation of the epidural needle within the epidural space and the agent used to detect loss of resistance (e.g. air or saline) against accidental dural puncture rate. Data were analysed using Z 2 and Analysis of Variance where appropriate. P<0.05 was considered significant.
Results: Responses were received from 390 (78%) of those surveyed. These comprised anaesthetists with varying experience ofepidural anaesthesia: 0-5 years, 32 (8.2%); 5-15 years, 191 (49.1%); 15 or more years, 166 (42.7%). The mean accidental dural puncture rate was 0.37%. Lower inadvertent dural puncture rates were found to be associated with increased experience (P=0.001), increased frequency of performing the procedure (P=0.002) and non-rotation of the epidural needle (P=0.012). Anaesthetists with <15 years' experience were more likely to perform an epidural with the patient sitting (P<0.001); use saline for loss of resistance (P<0.001) and not rotate the epidural needle (P<0.001).
Discussion: Accidental dural puncture rates are significantly influenced by experience, frequency of performing the procedure and rotation of the needle. The continued increase in the use of saline to detect loss of resistance 3 is demonstrated. Even advocates of the rotating technique acknowledge that rotation may tear dural fibres and increase dural puncture rates. 2
Conclusion: As the incidence of inadvertent dural puncture has remained unchanged over the past decade, Z efforts to improve this should include abandoning the practice of needle rotation within the epidural space. R e f e r e n c e s 1. Reynolds F. Dural Puncture and Headache: Avoid the first but treat
the second. BMJ 1993; 306:874-6 2. Norris MC, Leighton DL, De Simone CA. Needle bevel direction
and headache after inadvertent dural puncture. Anesthesiology 1989; 70:729-31
3.Howell TK, Prosser DP, Harmer M. A change in resistance? A survey of epidural practice amongst obstetric anaesthetists. Anaesthesia 1998; 53:238-43

206 International Journal of Obstetric Anesthesia
~ 8 - ©
"~ 6 - >
") 4 []
[]
P20: Assessment of S1 motor block for the rapid detection of accidental intrathecal injection of bupivacaine
R Collis and Z Daoud, University Hospital of Wales, Cardiff Introduction: Accidental intrathecal injection of bupivacaine during epidural analgesia remains a hazard. This study is designed to determine the dose of bupivacaine that, if given intrathecally, will not cause total spinal anaesthesia, hut will give a reliable and reproducible clinical sign to differentiate intrathecal from epidural injection.
Methods: A CSE technique with sequential allocation of a varying intrathecal dose was used for elective caesarean section. Bupivacaine 0.25% with fentanyl were given in a fixed ratio of lmg bupivacaine to 2~tg fentanyl. A study response was motor block of ankle dorsiflexion 10 min after spinal injection. The next patient after a responder received lmg bupivacaine less, the next patient after a non-responder received lmg bupivacaine more. Having determined the ED50 for S 1 motor block, 30 patients all received 13mg plain bupivacaine with 26~tg fentanyl.
Results: The ED50 for S1 motor block after intrathecal bupivacaine with fentanyl is 7.0 mg (95% CI 6.2-7.8).
10- []
[] [] [] [] UCl Eos0 [] [] [] [] [] Oh LCI i"i Fi ~ - I ~ - F~
[]
I I I I
5 10 15 20 Sequence
All 30 patients hadS1 motor block 10 min after 13mg bupivacaine. This gives a CI 89-100% of patients as being responders at this dose. A dose response curve can now be drawn to establish the ED95 for S 1 block.
Discussion: Although analgesia may occur rapidly with small doses of bupivacaine and fentanyl in the epidural space, I motor block especially S1 block occurs slowly. 2 This study describes an easy and reproducible clinical sign to help differentiate between spinal and epidural injection, 10 min after a top-up intended for the epidural space. The results confirm clinical practice of using 10- 15mg of bupivacaine per epidural top-up. This study design can now be used to test safe top-up practice for newer local anaesthetics coming into clinical practice.
References 1. James KS, McGrady E, Quasim I, Patrick A. Comparison of
epidural bolus administration of 0.25°//0 bupivacaine and 0.1% bupivacaine with 0.0002% fentanyl for analgesia during labour. Br J Anaesth 1998;81:507-10
2. Yarnell RW, Ewing DA, Tierney E, Smith MH. Sacralization of epidural block with repeated doses of 0.25% bupivacaine during labor. Reg Anesth 1990; 15:275-9
P22: Inadequate prophylaxis against thromboembolism in caesarean sections: which women are at higher risk?
S Rutter, R Orme, J Burry, C Grange, R Russell. Nuffield Department of Anaesthetics, Oxford Radcliffe Hospitals NHS Trust, Oxford, OX3 9DU, UK. Introduction: Thromboembolism (TE) remains the most common cause of death in pregnant women in the UK. 1 Caesarean section (CS) substantially increases the risk of TE. 2 Despite awareness amongst clinicians and Royal College of Obstetricians and Gynaecologists (RCOG) guidelines, 3 the latest CEMD report stated that inadequate TE prophylaxis was a common cause of substandard care. 1 The aim of this prospective study was to assess adequacy of prophylaxis, as recommended by RCOG, in our obstetric unit.
Methods: Thromboembolic risk was assessed in 108 consecutive women undergoing CS. Women were divided into low (LR), moderate (MR) or high risk (HR) groups according to RCOG guidelines. In addition, mobilisation whichtook longer than 12 h following surgery was considered to be delayed and, subsequently, a risk factor. TE prophylaxis measures were recorded and adequacy assessed according t o RCOG standards. Complete data were available on 101 women: 41 elective and 60 emergency CS.
Results: Postoperative mobilisation was delayed for more than 12 h in 36 parturients (36%). Of 101 women, 13 (13%) were group LR, 66 (65%) MR and 22 (22%) HR. Prophylactic measures included elastic stockings, standard heparin and combination of both. Overall, TE prophylaxis was inadequate in 55 women (54%). Most (62.5%) of 88 moderate and high-risk women received inadequate TE prophylaxis, emergency cases being at higher risk. Distribution of women with inadequate TE prophylaxis is summarised in the table.
Table: Inadequate thromboprophylaxis ModRisk HighRisk Total
EICS 11/25(44%) 1/3 (33%) 12/28(43%) EmCS 31/41(76%) 12/19(63%) 43/60(72%)
Discussion: 36% of women failed to mobilise early, necessitating consideration of TE prophylaxis in some low risk parturients. Moderate risk women were at higher risk of inadequate TE prophylaxis than those at high risk. All clinicians should be made aware of RCOG guidelines and assess parturients for TE risk perioperatively.
References : 1. Why mothers die. Report on Confidential Enquiries into
Maternal Deaths in the United Kingdom 1994- 1996.London:HMSO, 1998.
2. Greer IA. Epidemiology, risk factors and prophylaxis of venous thrombo-embolism in obstetrics and gynaecology. Bailliere's Clinical Obstetrics and Gynaecology 1997; 11: 403- 430.
3. Royal College of Obstetrician and Gynaecologists. Report of a Working Party on Prophylaxis against Thromboembolism in Gynaecology and Obstetrics. London: RCOG, 1995.
Poster presentations 207
P23: Coagulat ion failure and caesarean section. A role for desmopress in (DDAVP).
H Gorton, G Lyons. Obstetric Anaesthesia, St James's University Hospital Leeds LS9 7TF, UK
Introduct ion: Major haemorrhage is the second major cause of maternal mortality and is a serious risk when performing caesarean section. Coagulation failure should be treated aggressively before surgery. DDAVP causes transient improvement of coagulation because it stimulates platelet adhesiveness. It has been used clinically in cardiac and hepatic surgery/ Its use has not been previously recorded in obstetric practice. DDAVP shortens bleeding time, but thromboelastography (TEG) is a more pragmatic monitor of coagulation in the obstetric unit. 2 TEG is a ward-based, in vitro monitor of coagulation, which gives results of whole blood coagulation within 30 minutes.
M e t h o d s : T h r e e w o m e n wi th deteriorating coagulopathy requiring emergency caesarean section were treated with DDAVP and monitored using TEG. We recorded TEG variables before and after i.v. DDAVP 20 ktg prior to administration of blood products.
Results: Two patients had haemolysis, elevated liver enzymes and low platelets (HELLP), the other severe proteinuric hypertension (PH). All proceeded to emergency caesarean section, two with general and one with spinal anaesthesia. In all cases, TEG showed improvement in coagulation allowing uneventful surgery to start.
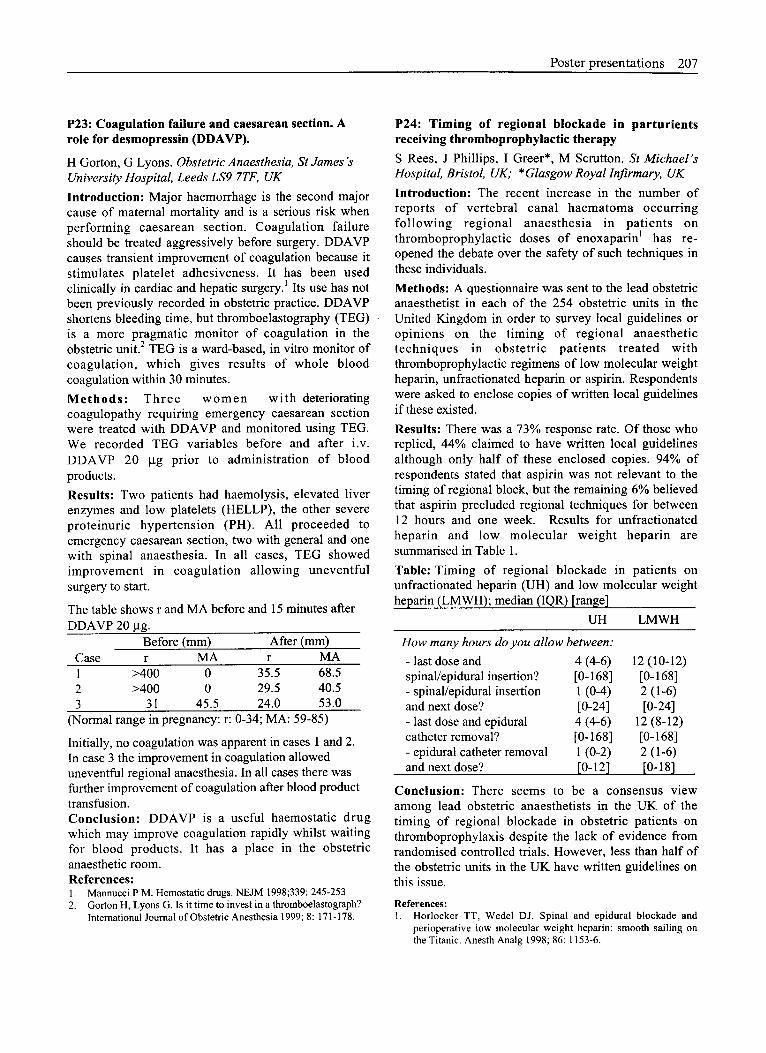
The table shows r and MA before and 15 minutes after DDAVP 20 ~tg.
Before (mm) After (mm) Case r MA r MA 1 >400 0 35.5 68.5 2 >400 0 29.5 40.5 3 31 45.5 24.0 53.0
(Normal range in pregnancy: r: 0-34; MA: 59-85)
Initially, no coagulation was apparent in cases 1 and 2. In case 3 the improvement in coagulation allowed uneventful regional anaesthesia. In all cases there was further improvement of coagulation after blood product transfusion. C o n c l u s i o n : DDAVP is a useful haemostatic drug which may improve coagulation rapidly whilst waiting for blood products. It has a place in the obstetric anaesthetic room. References: 1. Mannucci P M. Hemostafic drugs. NEJM 1998;339:245-253 2. Gorton H, Lyons G. Is it time to invest in a thromboelastograph?
International Journal of Obstetric Anesthesia 1999; 8:171 - 178.
P24: T i m i n g of reg iona l b lockade in partur ients receiving thromboprophylact ic therapy
S Rees, J Phillips, I Greer*, M Scrutton. St Michael's Hospital Bristol UK; *Glasgow Royal lnfirmary, UK
Introduction: The recent increase in the number of reports of vertebral canal haematoma occurring fol lowing regional anaesthesia in patients on thromboprophylactic doses of enoxaparin I has re- opened the debate over the safety of such techniques in these individuals.
Methods: A questionnaire was sent to the lead obstetric anaesthetist in each of the 254 obstetric units in the United Kingdom in order to survey local guidelines or opinions on the timing of regional anaesthetic techniques in obstetric patients treated with thromboprophylactic regimens of low molecular weight heparin, unfractionated heparin or aspirin. Respondents were asked to enclose copies of written local guidelines if these existed.
Results: There was a 73% response rate. Of those who replied, 44% claimed to have written local guidelines although only half of these enclosed copies. 94% of respondents stated that aspirin was not relevant to the timing of regional block, but the remaining 6% believed that aspirin precluded regional techniques for between 12 hours and one week. Results for unfractionated heparin and low molecular weight heparin are summarised in Table 1.
Table: Timing of regional blockade in patients on unfractionated heparin (UH) and low molecular weight heparin (LMWH); median (IQR) [ran~e]
UH LMWH
How many hours do you allow between:
- last dose and 4 (4-6) 12 (10-12) spinal/epidural insertion? [0-168] [0-168] - spinal/epidural insertion 1 (0-4) 2 (1-6) and next dose? [0-24] [0-24] - last dose and epidural 4 (4-6) 12 (8-12) catheter removal? [0-168] [0-168] - epidural catheter removal 1 (0-2) 2 (1-6) and next dose? [0-12] [0-18]
Conclus ion: There seems to be a consensus view among lead obstetric anaesthetists in the UK of the timing of regional blockade in obstetric patients on thromboprophylaxis despite the lack of evidence from randomised controlled trials. However, less than half of the obstetric units in the UK have written guidelines on this issue.
References: 1. Horlocker TT, Wedel DJ. Spinal and epidural blockade and
perioperative low molecular weight heparin: smooth sailing on the Titanic. Anesth Analg 1998; 86:1153-6.

208 International Journal of Obstetric Anesthesia
P25: Audit o f use of a latex sensitivity protocol in a maternity hospital setting
S Smith, S Young Department of Anaesthesia, Glasgow Royal Maternity Hospital, Glasgow Aim: To identify the outcome and frequency of use of a latex sensitivity protocol in an isolated site maternity unit with 4300 deliveries per year.
Methods: Retrospective review of theatre records and personal anaesthetic logbooks with casenote review at" patients identified over a 10-month period.
Results: 4 patients with a history of latex sensitivity had been identified and safely treated according to the hospital latex protocol. A 5 th patient, a community nurse, who did not volunteer a history of latex sensitivity developed severe bronchospasm after insertion of a latex urinary catheter. Subsequent questioning revealed that she avoided latex gloves due to skin reactions and triggering of asthma and that she developed swollen lips after blowing up balloons.
Previous exposure
1 Nurse in a paediatric haematology ward
2 Surgical nurse
3 General practitioner
4 Nurse in a medical ward
Type of allergy
mild skin reaction to latex gloves
previous local reaction to a latex urinary catheter. Avoids latex gloves
mild skin reaction to latex gloves
skin reaction and possibly bronchospasm associated with wearing latex 8loves
The audit identified 5 cases out of a total number of 990 theatre cases in the 10 month study period giving an estimated incidence of 1:200. All patients were health care workers.
Conclusion: Latex allergy is an increasing problem • 1 - • pamcularly amongst health care workers. We beheve it
is an important potential problem in maternity hospitals although only one previous case report could be found. 2 All such units should have a latex allergy protocol and be able to provide a latex free theatre. There should be reliable protocols for identifying high risk patient groups at an early stage. Eliminating latex- containing products and equipment from our environment will protect both ourselves and patients.
References: 1. Sinha A, Harrison PV. Latex glove allergy among hospital
employees: a study in the north-west of England. Occupational Medicine 1998;48:405-411
2._~. Takamatsu I, Karasawa F, Kamei M, OzakiK, Fukada I. A case of emergency caesarian section as result of anaphylaxis to latex. Masui - Japanese Journal of Anaesthesiology Jan 1999, 48:83-85
P26: Anaesthetic input at childbirth preparation classes. Self-indulgent hobby or professional role?
AF Davies, MJ Richards Department of Anaesthesia, Cheltenham General Hospital, Glos. Introduction: Providing advice at antenatal classes is not viewed as a core activity by many obstetric anaesthetists. The Changing Childbirth Reform Report j however, emphasises the need for informed maternal choice, based primarily on information imparted by relevant professional groups. We have examined the perceived usefulness and effectiveness of an antenatal talk on pain relief by an experienced anaesthetist.
M e t h o d s : l l 0 pregnant women completed a pre- and post-talk questionnaire. Three point verbal rating scales were used to explore maternal satisfaction with information provided, anxiety related to labour and likelihood of requesting epidural analgesia. 10cm Visual Analogue Scales (VAS) were used to assess changes in anxiety level, confidence in ability to control pain and expectation of severity of pain. VAS scores pre- and post-questionnaire were analysed using Wilcoxon Signed rank statistics.
Results: 72% rated the talk very useful and 28% useful. 96% stated that they were better equipped to make an informed choice. 58% felt less anxious after the talk whilst anxiety levels increased in only 4%. 25% were more likely to request epidural analgesia in labour, and 18% less likely to do so. Anxiety levels decreased from median 4.7 to 4.4 cm [P<0.05]. Confidence in controlling pain increased from a median of 4.5 to 5.5 cm [P<0.001]. Expectation of degree of pain decreased from 8.2 to 7.1 cm [P<0.001].
Conclusion: Maternal satisfaction with information imparted was high. A decrease in anxiety was seen particularly amongst the more anxious women. An improvement in self confidence and lowering of pain expectation was apparent without having increased anticipated uptake of epidural analgesia. This may indicate a shift in the mothers locus of control relating to pain relief in labour. A high internal locus of control (or belief in personal control) is usually associated with indicators of good mental health as well as increased childbirth " • 2 satisfaction. Overall, the antenatal talk, which adopted a systematic framework on pain relief methods, promoted several factors predictive of a positive childbirth experience.
References: 1 Department of Health. Changing childbirth. London: HMSO, 1993. 2 Crowe K, Von Baeyer C. Predictors of a Positive Childbirth Experience. Birth 1989;16:59-63

Poster presentations 209
P27: Can we improve our service ? Midwives' knowledge, training and attitudes towards epidural analgesia
D Uzeirbegovic, M Albin Guy's - St. Thomas' N H S t-Iospital Trust - London
Introduction: It is widely accepted that midwives assist in the monitoring and management of epidural analgesia in labour] "2 Their training in this field varies from hospital to hospital. Auditing of midwives' performance within an epidural service will help to identify deficiencies and issues that might be addressed by further education and retraining. A structured input from the anaesthetic department will help achieve and maintain a high standard of practice. 2
Methods: A survey was conducted amongst labour ward midwives in two hospitals: one teaching and one district general hospital. The questionnaire contained 18 questions in total. The first section obtained information about demographics. The second section aimed to evaluate knowledge about both pharmacological methods of labour analgesia and practical aspects of management of epidural analgesia in labour and its complications. The final section investigated midwives' training in epidural analgesia before and after qualification and their attitudes towards it.
Results: 62 out of 72 forms were returned giving >83% response rate. 38% of responders had >10 y e a r s ' midwifery experience. Though most (87%) had received formal education about epidural analgesia, nearly 20% had no postgraduate education on the subject. 50% of all responders ranked Entonox as most effect ive pharmacological pain relief method in uncomplicated labour. Only 25% of midwives would discuss epidural analgesia with their patient and nearly 30% would offer it only on patient's request. 30-40% of responders did not answer the question about complications of epidural analgesia and 33% regarded hypotension associated with epidural analgesia as a minor problem. There were significant differences between the two hospitals regarding postgraduate education on epidurals and numbers of midwives certified to do epidural top-ups.
Conclusion: Our audit shows that there is a clear requirement for ongoing education and training of labour ward midwives in management and monitoring of epidural analgesia in labour with input from the anaesthetic department.
References: 1. Department of Health and others. Report on Confidential
Enquiries into Maternal Deaths in the United Kingdom 1994 - 1996. London : TSO, 1998.
2. Vandendriesen N M, Lira W, Peach M J. Labour ward midwifery staff epidural knowledge and practice. Anaesth Intensive Care 1998; 26:411-419
P28: Now, where did I put that epidural?
AR Moye, F Plaat Queen Charlotte "s Hospital, London, UK
Introduction: When anaesthetists insert neuraxial blocks, the interspace entered is an important feature of the medical record. There may be reasons to avoid a particular interspace. Post-partum, identification of the interspace is required if blood patching is performed, or when assess ing a pat ient with neurological complications. Identification may be difficult because a line joining the iliac crests (Tuffier's line) does not consistently coincide with the L4 spinous process or the L4-L5 interspace] Anatomical variation is common; posture and the degree of spinal flexion affect landmarks. 2 This audit was designed to assess the reproducibility of the lumbar interspaces as they are recorded in our routine practice.
Method: Data was collected for 167 parturients who received CSEs for labour or operative delivery (150 inserted by SpRs, 17 by consultants). Anaesthetists were instructed not to change their standard practice; the site of insertion was recorded. At the routine post-partum follow-up ward round, a second anaesthetist, blinded to the recorded site, made their own assessment of where the CSE had been inserted.
Results: In 59.9% of patients there was agreement between assessor and insertor as to the insertion site. Agreement was more likely if the CSE had been inserted in the left lateral position (74.5%), compared to the sitting position (54.2%; P<0.05, ~a). The grade of anaesthetist, time of day, and lumbar interspace used had no significant effect on the rate of agreement. Similarly, the parity of the patient, whether in labour, the stage of labour and the urgency of operative delivery showed no significant effects on the rate of agreement.
Conclusion: Whilst imaging would be required to determine the true site of insertion of each lumbar CSE, the lack of agreement found in this audit demonstrates the low level of reproducibility when Tuffier's line is used to identify lumbar interspaces. Alternative methods, such as counting the interspaces from C7 or palpation of the 12th rib 2 might improve accuracy. The higher level of agreement in the lateral position may be a further reason for agreeing with Kinsella that the lateral position may be optimal in terms of safety, and that trainees should be encouraged to use it. 3
References: 1. Render CA: The reproducibility of the iliac crest as a marker of
lumbar spine level. Anaesthesia 1996; 51 : 1070-1071 2. Thavasothy M: The reproducibility of the iliac crest as a marker
of lumbar spinal level. Anaesthesia 1997; 52:811. 3. Kinsella SM: Lateral positioning for regional analgesia during
labour. Br J Anaesth 1997; 79: 260-261.

210 International Journal of Obstetric Anesthesia
P29: Accuracy of obstetric anaesthes ia data recording: a comparison of two systems
M J Oldman, F L Roberts Department of Anaesthesia, Royal Devon & Exeter Hospitals, Exeter, UK
Introduction: Whilst the minimum data set for obstetric anaesthesia has been agreed, no specification has been made as to how and by whom it should be recorded. A computerized record-keeping system for materni ty data (SWif tSTORK version 3.0) was introduced in Exeter in 1995 with data entry by midwives, including basic information about peripartum anaesthesia and analgesia. This has subsequently run in parallel with our obstetric anaesthetic register, a "pen and paper" system completed by anaesthetists. We have compared the accuracy of the data recorded in each system.
Methods: Records for the 12 month period starting 1 April 1997 were analyzed. All entries relating to anaesthetic intervention (GA, epidural, spinal or CSE) were retrieved from SWiftSTORK and compared with the data recorded in the anaesthetic register. Where a discrepancy occurred the patient's case-notes were used to determine the correct information.
Resu l t s : Combining the data from both systems produced a total of 1245 anaesthetic interventions on 1169 patients. 23 interventions (1.8%) had been omitted from SWiftSTORK and 20 (1.6%) from the anaesthetic register. Errors in the type of anaesthetic intervention recorded occurred in 41 cases (3.3%), 39 in SWiftSTORK and 2 in the anaesthetic register. The most common error (22/41) was a CSE entered as an epidural, though in 7 cases a GA had been erroneously recorded.
Conclusion: The rates of data omission were similar in the two systems and at <2% compare very favourably with those reported in other settings. 13 Although our analysis will not have identified interventions omitted from both systems, with these low rates this should be less than 0.05% of cases. The number of errors in the data entered by midwives (39), however, was far higher than that recorded by anaesthetists (2). We conclude, therefore, that anaesthetists rather than midwives should record obstetric anaesthetic data to ensure maximum accuracy.
References: 1. Lyons C, Gumpert R. Medica| audit data: counting is not
enough. BMJ 1990; 300: 1563-1566. 2. Barrie J, March D. Quality of data in the Manchester orthopaedic
database. BMJ 1992; 304: 159-162. 3. Cleary R, Beard RW, Coles J, et al. The quality of routinely
collected maternity data. Br J Obstet Gynaecol 1994; 101 : 1042- 1047.
P30: An audit into documentation and case note keeping in obstetric anaesthesia.
K D Rooney, R J Chestnut, M Shaw Department of Anaesthesia, Crosshouse and Ayrshire Central Maternity Hospital, Ayrshire, Scotland
Introduction: Medical negligence claims against obstetr ic anaesthet is ts have been increasing dramatically over the last ten years. This is probably due to increased patient expectation and the better availability of legal aid. Substandard record and note keeping can make many medical negligence claims very difficult to defend. The Obstetric Anaesthetists' Association has published guidelines on note keeping, which are "by no means comprehensive but represent a minimum record of a procedure". As a result, failure to follow these guidelines may make us easy targets for litigation. The aims of the study were to compare and contrast what is recorded in everyday practice in a busy district general teaching hospital, with what is recommended by the OAA as a "minimum record of a procedure". In addition, we hoped to design a new obstetric anaesthetic chart, which incorporates the guidelines recommended by the OAA.
Methods: After local ethics committee approval, we performed a retrospective audit of 100 consecutive deliveries between 1 April and 12 April 1999. Thirteen anaesthetists of varying grades were involved and all were blind to the fact that their documentation was being audited. We searched for the specific issues that the OAA recommend as a "minimum record of a procedure" in the case notes.
Results: Fifty of the 100 deliveries received some degree of anaesthetic involvement. Of these 50 deliveries, the standard of documentation varied dramatically from being excellent with a close correlation to the OAA guidelines, to baring no resemblance to the above guidelines at all.
Conclusion: Good note keeping and documentation is a very time consuming but necessary practice in a busy obstetric unit, where time can be of the essence. At times our current practice does not meet up with the "minimum record of a procedure", as recommended by the OAA. Perhaps a more user-friendly obstetric anaesthetic chart would make it easier for'us to follow the recommendations of the OAA.
Reference: 1. OAA Training Module:
http://www.,gaa-anaes.ac.uk/guidelines/train005.htm

Poster presentations 211
P31: Major obstetric haemorrhage audit
MD Esler, DJA Vaughan, B Loughnan, PN Robinson. Northwick Park Hospital, Harrow, Middlesex HA1 3UJ.
Introduction: Peripartum haemorrhage is a major cause of preventable maternal mortality. We analysed 17 cases of major obstetric haemorrhage (MOH), and used these data to assess and augment our protocol.
Methods: Notes were analysed retrospectively for all cases over a three year period. Haematology records were cross-checked to ensure no cases were missed.
Results: Ethnic mix was normal for our unit. Patients were older than our standard obstetric population (median 35 years, interquartile range 29-39) and had lower body mass index scores (mean 24.5, standard deviation SD=3.4). Mean gestational age was low (36 weeks, SD=4.5). 70% were multiparous, and 30% had a previous history of haemorrhage. Factors contributing to MOH were varied (uterine atony, placenta accreta/ abruption/praevia/retention, DIC, genital trauma). All patients had full antenatal care. Only 1 MOH was predictable (grade 4 praevia). 53% of deliveries were by caesarean section of which half were elective. A consultant attended in 76% of cases (obstetrician 47%, anaesthetist 53%). Invasive monitoring was often used (77%, arterial line 59%, CVP line 71%, only 1/17 peripheral long line). Where a dedicated porter was used, sample and blood product transfer was subjectively much faster. 59% received ITU care. No patients died.
Haematological Analysis." Mean (SD)
Blood loss 5.3 litres (2) Total blood 10.3 units (5.2) Blood first 2 h 4.6 units (2.5)
Total FFP 4.8 units (3.5) FFP first 4 h 3 units (2.8)
Platelets 1.8 pools (1.1) Cryoprecipitate 10.9 units (4.2)
Comments
0% no blood 18% no blood in this period 18% no FFP 53% no FFP in this period 76% no platelets 88% no cryo. Normal Range
Lowest Hb 6. lg dl -l (1.5) 13.5-17.5g dl 1 Lowest Platelets 74 x 109/L (30) 150-400 x 109/L Highest PT 23 s (7) 11.5-16 s Highest APTT 68 s (20) 26-38 s Lowest 106 mg dl 1 (81) 150-400mg dl 1 Fibrinogen
Recommendations: Criteria for MOH declaration must be clinically based and allow for pre-emptive preparation where possible. An automatic sequence should occur on declaration of MOH: blood and product preparation, senior staff contacted and a dedicated porter provided.
Conclusions: Ongoing audit of MOH allows fine- tuning of protocols to reduce the risk of maternal morbidity and mortality, and more effective use of limited haematological, staff and equipment resources.
P32: UK Registry of high-risk obstetric anaesthesia: the first three years
D.P. Dob and S.M. Yentis on behalf of OAA members Magill Dept. of Anaesthesia, Intensive care & Pain Management, Chelsea & Westminster Hospital, London, UK
Introduction: Information about uncommon conditions in pregnancy is obtained from (i) published case reports and series; (ii) textbooks; and (iii) personal anecdotes. However, the first two sources are highly selective and frequent ly out of date, whilst few individual anaesthetists have adequate exposure to rare conditions to have gained much experience. To remedy this a voluntary registry was started in late 1996 whereby individual experiences across the UK could be pooled into a central database
Methods: A standard data collection form was sent to all members of the OAA, requesting information on all cases of cardiorespiratory disease passing through maternity units throughout the UK. Information was requested about the hospital involved, the history of the complaint and the antepar tum and postpar tum management (planned and actual), as well as maternal and fetal outcome. An interim bulletin describing the main results of the Registry was sent out to all OAA members in 1998.
Results: Over the last 3 years OAA members have sent in 229 reports from all over the UK. The reports are divided into four main categories.
Complex congenital heart disease 45
Valvular heart disease 73
Miscellaneous cardiac conditions 89
22 Respiratory disease
Conclusion: There has been an overwhelming response from OAA members who have taken the time and trouble to record cases, many of which might not otherwise be published. The Registry is becoming a valuable collection, and we hope that members will continue to send reports. We feel it is important that details of cases collected should be made available to all OAA members. Currently a more detailed report is in preparation The purpose of this abstract is to thank all those anaesthetists who have contributed to the project and to publicise it further. It is presented by the authors on behalf of the members of the OAA.

212 International Journal of Obstetric Anesthesia
P33: Cont inuous intrathecal anaesthesia for caesarean section in a patient with Ehlers-Danlos syndrome.
D Guerin, B Moore, K McKeating Department of Anaesthesia and Intensive Care Medicine, St. Vincent's University Hospital, Elm Park, Dublin 4, Ireland
Introduction: Ehlers-Danlos syndrome (EDS) is a heterogenous group of connective tissue disorders characterised by articular hyperlaxity, cutaneous hyperelasticity, and vascular and cutaneous fragility. EDS-type 4 is the most severe form and in pregnancy is associated with a mortality of up to 25%. Complications of anaesthetic significance include difficult intubation, rupture of viscus aorta, vena cava or uterus, intractable haemorrhage and increased risk ofpneumothorax. These risks are compounded by pregnancy. This is the first reported case of continuous intrathecal anaesthesia for Caesarean section in a patient with EDS.
Case report: A 35-year-old primigravid woman with a known diagnosis of EDS-type IV, presented for elective caesarean section at 36 weeks' gestation. Her history included hypothyroidism, easy bruising, fragile skin and recurrent toe dislocation. Her antenatal course was otherwise unremarkable. An ejection systolic murmur was shown by echocardiography to be flow-related and cardiac function was otherwise normal. Perioperative monitoring included ECG, pulse oximetry, continuous invasive blood pressure and central venous pressure monitoring. Anaesthesia was established and maintained with intermittent intrathecal boluses of 0.5% bupivacaine plus fentanyl via a 22-gauge Braun Spinocath continuous intrathecal anaesthetic system.
Results: Perioperative haemodynamics were stable with an estimated intraoperative blood loss of 500 ml. A healthy female infant of 2300 g was delivered. There were no anaesthetic complications and post- operative analgesia was adequate.
Conclusion: A continuous intrathecal anaesthetic technique provided optimal anaesthetic and surgical conditions for caesarean section.
P34: Combined spinal-epidural anaesthesia for caesarean section in a patient with cavernous spinal haemangioma.
J Onslow Southampton University Hospitals NHS Trust Southampton General Hospital, Southampton S016 6FD
Introduction: A primigravida with a known spinal cord arter io-venous malformation (AVM) at T9-T10 presented for elective caesarean section (LSCS). She had presented to the neurosurgeons two years before her pregnancy with an acute haemorrhage from a spinal cord AVM. The successful use of combined spinal-epidural anaesthesia (CSE) for LSCS is described, and the risks and benefits of regional anaesthesia in women with neurological deficit will be discussed.
Case Report: A healthy woman presented t o the neurosurgeons in 1995 with acute onset of bilateral lower limb weakness and altered sensation. Examination revealed neurological deficit below T9/T10. Magnetic resonance imaging and myelography demonstrated a bleed from a cavernous haemangioma of the spinal cord situated at T9/T10. Surgical intervention was not considered indicated. The patient presented to the neurosurgeons early in her pregnancy. Delivery by elective caesarean section was advised to reduce the risk of haemorrhage from the AVM during labour and to avoid risk of neurological damage from difficult vaginal delivery. After full discussion of the potential risks and benefits combined spinal epidural (needle-through- needle) anaesthesia was planned. An anaesthetic block to T4 was obtained, and surgery was uneventful. The patient made a full neurological recovery.
Discussion: Use of a regional anaesthetic technique in the face of existing neurological disease is controversial. There are few reports in the literature of the anaesthetic management of patients with spinal AVM presenting for caesarean section. 1"2 Traditionally neurological disease has been considered a relative contraindication to regional anaesthesia. The risk benefit ratio for a chosen anaesthetic technique in a patient with neurological disease must be considered on an individual basis. A multidisciplinary approach to management, including full documentation and discussion with the patient is essential.
References 1. Ong BY, Littleford J, Segstro R, Paetkau D, Sutton I. Spinal
anaesthesia for caesarean section in a patient with a cervical arterio-venous malformation. Can J Anaesth 1996; 42: 1052- 1058.
2. Eldridge AJ, Kipling M, Watt-Smith J. Anaesthetic management of a woman who became paraplegic at 22 weeks gestation after a spontaneous spinal cord haemorrhage secondary to a presumed arterio-venous malformation. Br J Anaesth 1998; 81: 976-978.





























