Embed Size (px)
Citation preview

0099-2399/89,'1506-02491$02 00/0
CorpyrK:Jht C 1989 by The ~ C a ~ As~oo.aton o! E ~ t ~ s ~ s Pt~nlet'l ~n U S A
Vot 15 No 6 &,',~" 1989
Absorbed Radiation by Various Tissues during Simulated Endodontic Radiography
Mahmoud Torabinejad, DMD, MSD, Robert Dan|or|h, DDS, Kevin Andrews, DDS, and Charlene Chan, DDS
The amount of absorbed radiation by various organs was determined by placing lithium fluoride thermo- luminescent chip dosimeters at selected anatomical sites in and on a human-like X-ray phantom and exposing them to radiation at 70- and 90-kV X-ray peaks during simulated endodontic radiography. The mean exposure dose was determined for each anatomical site. The results show that endodontic X-ray doses received by patients are low when compared with other radiographic procedures.
( 'oncerns ha~ e t%'en expre',,,%'d alx)ut harmtid effects of radia- tion stm:e the initial use of X-rays for diagnostic inlaging. ,XccountabiliD t't~r usa: of radiation is expected from medicine and dcntistr3, b~, tile public, since the majorit.,, of rnan-naadc radiation ix in the form of medical and dental X-ra.~s. lX'ntal radiograph> constitutes the snlallcr lx`)rlion at.,, indicated b', .~veral studies ~hich Ila~.c compared the anlt`)unts ofradKltion asst~:iated ~ith medical and dental diagnostic radiograph', and ntdiation therap} {1-4). In spite of Iming tile smaller amount , it ix estimated that I{R} million dental X-rat.', exami- nations are Ix'rformed each ~ear m the t :n i tcd States, man.,, on patients prc~iousl} ex l x ~ ' d to medical X-ra.',s (5). "lhis ut i l i /a tmn has prompted nurr, erou,; studies m attl effort to quanti tale specific do~" amoun t s to denial patients ( 1. 2, 4.
Radiogn~phs are con l l l lon l} u~'d during cndt• pro- cedurcs. According It) at sur~e~ conducted by the American l.X.'ntal Association ('enstlS Bureau m It)79. more than 17 million endt~.h)ntic I realmenls v, erc pcrtormed in tile l.!nitcd States (10). Becau~ (if prcdictabilit', and tile high succt."ss rate of rt~`)t canal therap.,, and it public demand to ~ e teeth, a record numt%'r of teeth arc no~ Ix:ing cn&~lonticall~ treated. �9 Many patients are concerned a[~lut the numb, or of fihus that arc s.c)lTlelllllCs, required during treatment, anti direct data concerning doses during endt~hmttc treatment are lacking. I)OSC inforllaation al'umt sl• cndtxJontic prt~.'edures Would pro,,ide at basis for rcslxmding to patient concerns and allm~ a rational approach It`) tile us,.." of X-ra.~s in end(Kh)ntic thcraro. l h e purfx`),,,: of this m~estigation v, as It`) measure radiation &)sex it) selected organs atnd regions dur ing s, inltl- lated endt~lontic radiograph.~ using ~0- atnd tR)-k\'p extx`)st, rc h-'chniqucs.
MA' I ' I ' ~RI . 'd .% AND NIE'III()I)."i
Nlatcrials
I hc follov, ing v,r us,,:d: l . i thium lluoridc (l.iF) thcrmolurninc~ 'cnt dosimeters
( } larshav, ( 'heroical ( 'o.. (.'levcland. ( )! { )- -( "r'y 9.als ~ ere sup- plied in 2-mm: chips. l h e dosimeters absa)rb energ,, when cx lx~ 'd to rad ia t ion . .~xent , , -one do.simetcrs v, crc used for do~" nleasurenlcnts and lixc ~erc utilized as control for background radiation.
\"ictorccn mt~.lcl 2,R(R] ana lyzer - - | h i s ins t rument ,,~as u.~d to read tile exlx)~'d I iF dosimeters. Dosimeters ~verc indis id- uall', placed in tile anal',,,er and heat acti~ atted at 400~ ". The abs~rbcd radiation cnerg', within tile dosimeter ix rc lca~d it nd con ~ erred into c m it ted [igh t i tllpulse's s~,hich at rc nlcasu red b', a photomuhipl icr tribe and cxpms~-d as at numerical value.
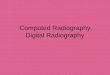
Radiat ion therap,, nmge cxlx)sure phan tom ( l t u m a n o i d Systems, Torrance, ( ' A ) - - T h i s consists of a hum an skull and cervical vertebrae ( ( '1-5) v,-ith a complete denti t ion which arc emtx'dded m a tis,sue..cquivalcnt material molded It') the shape of the h u m a n head. The phan tom could Ix- .~-paratcd into nine transverse .~ctions (Fig. I). l )osimcter site holes were prepared in tile phantom to correslxmd with the internal anatomical areas studied (Fig. 2). Exlx)surc of the phantom slmulatcxt patient eXlX~sure.
(;choral Electric I(RK) X-ray un t t - - ' I Lh i s unit ~ h i c h has a,
O.g-mm fov'al slx`)t, 2.5-ram a l u m i n u m filtration, and at 12- inch ofran-ended cone ,aas u~ 'd ;.Ix X-ra~ source. It ~as olx'ratcd at 70 and t)(I kVp. 15 ma ranges. ' lhe unit ',,~;ls calibrated fbr accurac3 prior to the stud,,.
Kcithlc.~ 960.15 ion chamlx.'r dos imete r - -This inst rument was used to measure tile 70- and ~')()-k~'p radiation output f'ronl tile X-KI~ .'~.)urcc during the calibnttion of tile l i t dosimeters.
Mcth(xl~
Prior to lilt." stud~, all of the dosimeters ~crc annealed ;.tl 4(R)~ and calibrated to a kn(`)~ n amoun t of radiation ill 70- and O0-kVp energ) ranges as measured b~ a Kcithlc~ ~/(~1)35 ion ctlanl|%'r. I l l , : dosimeters ~crc indi~iduall', read in a Victorecn mt~.lel 2,R(R) analy/er to determine lhe amount of absa`)rbcd radiation cncrg.~ ~ ithm the dosm/etcr, f h c anal~,/or ~aluc v, as di~ idcd b.', the kntlv, n amoun t of radiation and a calibration factor ~as established t'~r each I i l ' dosimeter.
249

250 Torabinejad et al.
FtG 1. A human-like X-ray phantom composed of human skull, cervical vertebrae, and complete dentition, embedded in tissue-equivalent material and supplied in nine separate 2.5-cm transverse sections.
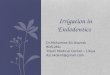
FIG 2. Internal profile of a section of the phantom showing holes for placement of dosimeters at a particular level (thyroid).
The phantom was prepared by placing three dosimeters at each anatomical site except for the calvarium which received only one per site. External dosimeters were placed into small gelatin capsules and taped to their respective anatomical locations or over the end of the X-ray cone in the center of the X-ray beam. The selected bone marrow sites were similar to those outlined~by White and Rose (7). Eight upper and lower internal sites were selected for the thyroid (Fig. 2). After the phantom was positioned in the dental chair upon the supporting stand, the dosimeters for the reproductive organ dose were positioned on the chair seat at the base of the stand.
The simulated endodontic X-ray procedure was performed using the long-cone paralleling technique. Cone alignment was facilitated by placing target spots over the selected expo-
Journal of Endodontics
sure regions and centering the cone over the spot 1 inch from the phantom's surface. The exposure regions corresponded to the maxillary and mandibular anterior, premolar, and molar teeth. The number of exposures for each region was deter- mined after a survey of 100 charts of endodontic patients who had been treated at Loma Linda Dental School. This revealed a minimum of four, six, and eight films were made for initial, working, and final procedures when treating anterior, pre- molar, and molar teeth, respectively. The clinical quality of the selected exposure techniques was ensured by prior test film exposures using step-wedge densities and dental X-ray teaching phantoms.
The exposed dosimeters were individually read in the ana- lyzer in the same manner as described for calibration. The analyzer numerical value was multiplied by the dosimeter calibration factor to calculate the absorbed radiation from the endodontic exposures. The bone marrow dose was calculated according to the method of White and Rose (7) to reflect the head and neck marrow contributions toward the whole-body bone marrow dose. The surveys were conducted three times at both 70- and 90-kVp energy ranges, The mean absorbed dose and standard deviations per tissue/organ site were cal- culated from the total dose recorded by the dosimeters from the three patient-equivalent surveys for each dental region. The resultant dose was expressed in microGrays (gGy) (Gy = 100 rads, 1 rad = 0.01 Gy, 1 mrad = 10 uGy, Scientific International Units) (11).
Comparative Data
Dose data reflecting estimated biological effects, medical, therapeutic, and diagnostic radiation were obtained from the literature for direct comparison with the study dose measure- ments. These data are included in the dose (Tables 1 to 3).
RESULTS
Mean dose data for each site with comparative data are listed in Tables 1 to 3. Table 1 shows the surface dose for the skin and reproductive organs. The skin surface dose was the largest dose measured by the study and increased with the expostlre time and the number of exposures from anterior to posterior sites. It also was greater for the mandibular expo- sures, although the exposure factors were the same for the maxilla. These doses can be compared with radiation-induced mucosal changes associated with head and neck radiation cancer therapy which reportedly occurs at ranges of 10 to 600 X 10 5 uGy (12, 13).
The unshielded reproductive organs received the smallest dose, with the mandibular dose approximately two to three times greater than the maxilla dose. The mandibular dose was three to four times greater than the comparative estimated daily background radiation dose to the reproductive organs of 2.5 to 5.0 #Gy (14, 15). This increase resulted from not using a lead apron and because the plywood stand supporting the phantom does not absorb scatter radiation in a manner similar to the human body. Study doses were nominal when compared with those of 200 • l0 s uGy reported to be asso- ciated with congenital anomalies and death in animal studies (14).

Vol. 15, No. 6, June 1989
Table 2 indicates that the eyes received a variable dose depending upon the survey site being radiographed. The greatest dose was to the right eye when exposing the maxillary premolar. The fight eye was located on the tube side for the exposure and was positioned more directly in the X-ray beam. Mandibular surveys exposed the eyes to lesser doses compared with those during maxillary examination. These doses, re- gardless of the exposure site, are considerably less than the comparative dose of 20 x 105 ~Gy associated with cataract formation (14).
Internal dose for the thyroid and bone marrow and the thyroid surface dose are shown in Table 3. As previously
Absorbed Radiation 251
observed, dose increased with the exposure time, number of exposures, and for the mandibular sites. The internal thyroid dose from the mandibular molar exposure was the greatest dose to the thyroid. This is to be compared with the dose estimates for development of thyroid neoplasia from absorbed radiation which have been on the order of 6 x 104 ~Gy (14).
The whole-body bone marrow was the highest from the mandibular molar exposures and most likely reflects the greater concentration of bone marrow in the posterior man- dible. Comparative data indicate acute radiation bone marrow effects occur at 20 • l0 s uGy (13). A 21-film full-mouth dental X-ray series has been reported to give 160 #Gy (7).
TABLE 1. Skin and reproductive organs/mean dose per survey (expressed in microGrays)*
Survey
70 kVp, 15 ma 90 kVp, 15 ma
No. of Time Skin Reproductive Time Skin Reproductive Exposures (Unshielded) (Unshielded)
Maxillary Central 4 24/60 4,608 4- 269 5.4 _+ 1 12/60 3,976 4- 68 6.1 _+ 0.6 Premolar 6 36/60 8,070 _+ 791 7.3 4- 1 18/60 8,324 4- 329 4.2 4- 1.8 Molar 8 36/60 12,359 4- 2476 5.4 _+ 1 18/60 10,788 4- 1652 3.6 _+ 0.9
Mandibular Central 4 24/60 5,010 4- 104 13.0 4- 4 12/60 4,468 4- 111 17.0 ___ 1.9 Premolar 6 36/60 11,708 + 633 15.6 _+ 7 18/60 9,837 4- 237 17.0 4- 7.0 Molar 8 36/60 14,862 4- 685 18.0 4- 8 18/60 12,572 4- 862 22.3 _+ 3.0
* Medical comparisons (estimated dose in microGrays): erythema--acute dose, 100 • 105 (12); oral mucositis/ulceration, 10 to 600 x 105 (13) . . . accumulated fractionated dose; atrophy/ cancer, over 600 x 105 (12) . . . chronic accumulated; estimated background radiation, 2.5 daily, 900.0 annual (14, 15); genetic dose estimates dental X-rays--with lead apron, 0.1 to 0.3; without lead apron, 5.0 (16); congenital anomalies/neonatal death (animal studies), 200 x 105 (14).
TABLE 2. Eye/mean dose per survey (expressed in microGrays)*
Survey
70 kVp, 15 ma 90 kVp, 15 ma
No. of Time Right Left Time Right Left
Exposures
Maxillary Central 4 24/60 238 _ 48 84 _4- 19 12/60 187 4- 17 154 _+ 25 Premolar 6 36/60 955 _+ 193 164 + 84 18/60 718 4- 35 140 _+ 18 Molar 8 36/60 277 _+ 117 98 4- 47 18/60 462 _+ 33 115 -+ 9
Mandibular Central 4 24/60 45 4- 22 46 4- 14 12/60 51 4- 2 42 _+ 5 Premolar 6 36/60 82 4- 26 63 4- 43 18/60 87 4- 34 82 4- 23 Molar 8 36/60 62 4- 10 79 4- 19 18/60 90 + 38 75 4- 13
* Medical comparisons (estimated dose in microGrays): risk of cataract formation, single exposure, 20 x 105; fractionated dose over 40 x 105 (14); lens. . , full-mouth series (16 films), 400 + 45.0 (19); eye . . , panoramic, 60 to 70 #Gy (adapted from. ref. (20)).
TABLE 3. Thyroid and bone marrow/mean dose per survey (expressed in microGrays)*
70 kVp, 15 ma 90 kVp, 15 ma
Survey No. of Thyroid Bone Thyroid Bone Time Time
Exposures Surface Internal Marrow Surface Internal Marrow
Maxillary Central 4 24/60 23 + 2 26 + 6 8 + 3 12/60 36 4- 2 45 _ 0.9 23 __- 0.7 Premolar 6 36/60 32 4- 10 51 _ 17 31 4- 8 18/60 38 + 3 66 + 15 49 ___ 17 Molar 8 36/60 42 _+ 9 86 + 44 63 _+ 28 18/60 58 -+ 16 159 + 83 80 + 28
Mandibular Central 4 24/60 92 + 14 73 + 24 32 4- 2 12/60 81 + 16 78 4- 19 41 + 4 Premolar 6 36/60 121 + 38 159 + 93 75 + 29 18/60 169 _ 67 164 + 58 84 _+ 10 Molar 8 36/60 207 + 30 341 _+ 96 121 + 13 18/60 260 _+ 66 409 + 109 127 4- 6
* Comparisons (estimated dose in microGrays): thyroid--development of tumors (therapy dose range), 6 x 104 (14); thyroid scan (whole-body dose range) over 2000 (14); panoramic X-ray, 80 (13); chest X-ray, 10 (13); lateral skull, cephalometry, 160 (13); full-mouth dental series... 600 (2) and 730 (18). Bone marrow--estimated annual background radiation dose to marrow, 870 (7); whole-body acute bone marrow syndrome, over 20 • 105 (13); full-mouth dental series (21 films), 160 (7); panoramic X-ray, 24 (7).

252 Torabinejad et al.
Comparing 70- with 90-kVp energy X-rays indicates that the surface entrance dose (Table 1) is greater for 70 kVp than for 90 kVp. Results also indicate that the dose to specific anatomical sites can vary with the kVp used and the site distance from the area under the X-ray cone. The majority of the data show measured 90-kVp doses to internal and distant surface anatomical sites are slightly greater or very similar to those recorded for 70 kVp. Examples are higher surface doses for the reproductive organs (Table 1), thyroid (Table 3), and the internal doses for the thyroid and bone marrow (Table 3).
DISCUSSION
The practice of radiology can be viewed from two broad viewpoints: (a) adverse effects upon living tissues with accom- panying risks and (b) benefits to patient from obtained diag- nostic information. These viewpoints are affected by public opinion, which can influence how diagnostic information is obtained. Because of this influence, much of the research data obtained for radiology has been directed toward accountabil- ity by quanitating dose, determining biological effects, and developing techniques to obtain quality images with mini- mum exposure. Unfortunately, in some instances, there is a trade off between image and dose.
Major concerns arising from the use of ionizing radiation in dentistry are the carcinogenic potential and the adverse effect upon the lens of the eyes. Two critical organs at risk for a radiation-induced carcinoma and leukemia are the thyroid gland and bone marrow. Exposure to the thyroid is a concern because of previous reports suggesting tumor formation from therapeutic doses as low as 6 • 104 #Gy (17). The bone marrow is a significant site for evaluation of radiation dose because leukemia carries a greater chance of patient mortality than does a tumor of the thyroid (17). The eye is important because patients are aware of eye damage associated with radiation exposure.
It is apparent when evaluating Tables 2 and 3 that the dosages which cause biological effects and the dosage from medical related radiology are much higher than our measured endodontic dose to these organs.
Comparative dental data indicate a full-mouth series ex- poses the thyroid to 600 uGy (2) or 730 ~Gy (18) while the bone marrow receives 160 #Gy (7) and the lens of the eye receives approximately 400 #Gy (19). Panoramic techniques are less: thyroid, 80#Gy (13); bone marrow, 24 uGy (7); and eyelid, 60 to 70 #Gy (20).
Except for the right maxillary premolar eye dose, the ab- sorbed doses in this study are much lower than those for a full-mouth series and reflect the reduced number of films required for endodontic therapy. The higher eye dose is the result of repeated and virtually direct exposure. The study doses were genenally higher when compared with those re- ported for panoramic X-rays and are associated with the close proximity of the X-ray cone to the target organs and the use of direct exposure dental film instead of the faster film-screen combinations used with panoramic techniques.
The 70- and 90-kVp data indicate that the 90-kVp dose is generally similar or greater for every anatomical site except when that site is positioned directly under the X-ray cone. Thus, it seems that greater penetrating 90-kVp energy X-rays are able to travel further through tissue and deposit doses to
Journal of Endodontics
organs remote from the primary X-ray site more readily than are those of the 70-kVp techniques. This suggests that 90-kVp techniques do not spare the patient any tissue dose except at the surface exposure site. This conclusion supports the study by Price (21) who investigated the quality of images produced by 70- and 90-kVp techniques. He found a clinical preference for images made at 70 kVp and cited other studies reporting a greater depth dose with increased X-ray energy. These combined data suggest it is a misconception that preferred image contrast, obtained with lower kVp exposures, must be sacrificed for lower patient dose generally associated with higher kVp techniques.
The surface and reproductive doses have minimal impor- tance when evaluating patient dose from dental X-rays. In one study, surface exposure varied from 1% to about 30% of the total X-ray beam exposure depending upon location (20). The discrepancy between surface and internal doses is best seen with the generally increased internal thyroid dose. Re- productive data have been eliminated from some governmen- tal dental X-ray reports (13) due to reported low reproductive doses (22). The unshielded reproductive dose, while greater than the comparative background dose, reflects the manner in which the dose was measured. In a clinical setting, with a real patient and proper lead shielding, reproductive dose would be more comparable to background levels.
In a subsequent paper, these data will be used to calculate estimates of patient risk associated with endodontic radiog- raphy.
CONCLUSIONS
Our study shows that endodontic X-ray doses are variable, depending on anatomical sites. The doses are relatively low to the critical organs at risk when compared with biological effects of medical therapeutic and diagnostic radiation. There is not a significant dose difference to internal organs from 70- or 90-kVp energy ranges. Despite the low dosages to endo- dontic patients determined by this study, the number of radiographs should be kept to a minimum. Further protective measures such as lead aprons, thyroid collars, and faster E speed films (Kodak Ektaspeed) are recommended.
We would like to thank Dr. Helene Engstrom, Lars M. Bakland, and Lance Gorton for their technical assistance.
Dr. Torabinejad is professor of endodontics, School of Dentistry, Loma Linda University, Loma Linda, CA. Dr. Danforth is associate professor, Depart- ment of Diagnostic Sciences, School of Dentistry, University of Southern California, Los Angeles, CA. Drs. Andrews and Chan are former predoctoral dental students and are currently in private practice.
References
1. Bankvall G, Hakanssnon HAR. Radiation-absorbed doses and energy imparted from panoramic tomography, cephalometric radiography, and occlusal film radiography in children. Oral Surg 1982;53:532.
2. Bengtsson G. Maxillo-facial aspects of radiation protection focused on recent research regarding critical organs. Dentomaxillofac Radio11978;7:5-14.
3. Shope TB, Morgan TJ, Showalter CK, et al. Radiation dosimetry survey of computed tomography from ten manufacturers. Br J Radio11982;55:60.
4. 8ankvall G, Engstrom H, Engstrom C, Hotlender L. Absorbed doses in the craniofacial region during various radiographic and radiotherapeutic Droce- dures. J Dento=Maxillofac Radiol 1985;14:19-24.
5. Lurie A. Journal of Clinical Orthodontics/interview; Risk/benefit consid-

Vol. 15, No. 6, June 1989
eration in orthodontic radiation. JCO 1981 ;15:469-84. 6. Wall BF, Kendall GM. Collective doses and risks from dental radiology
n Great Britain. Br J Radio11983;56:511. 7. White SC, Rose TC. Absorbed bone marrow dose in certain dental
radiographic techniques. J Am Dent Assoc 1979;98:553. 8. Wall BF, Fisher ES, Paynter R, Hudson A, Bird FD. Doses to patients
from pantomographic and conventional dental radiography. Br J Radiol 1979;52:727.
9. Greer DF. Determination and analysis of absorbed doses resulting from various intraoral radiographic techniques. Oral Surg 1972;34:146.
10. American Dental Association, Bureau of Economic and Behavior Re- search, 1979 Survey of dental services rendered. Chicago, ADA Bureau of Economic and Behavior Research.
11. International Commission on Radiation Units and Measurements. Ra- diation quantities and units, ICRP Report 33. ICRP Publications, Washington, DC, 1979.
12. Travis EL. Primer of medical radiobiology. Chicago Year Book Medical Publisher Inc., Chicago, IL, 1975.
13. Goaz PW, White SC. Oral radiology, principles and interpretation. St. Louis: CV Mosby, 1982.
Absorbed Radiation 253
14. Hall EJ. Radiology for the radiologist. 2nd ed. Philadelphia: Harper & Row, 1978.
15. United Nations Scientific Committee on the Effects of Atomic Radiation. 1977 Report to the General Assembly, with Annexes. New York: United Nations, pp. 308,309, 311.
16. Langland OE, Sippy FA, Langlais RP. Textbook of dental radiology. 2nd ed. Springfield, IL: Charles C Thomas, 1984.
17. Modan B, Baidatz D, Mart H, Steinitz R, Levin SG. Radiation induced head and neck tumors. Lancet 1974;1:277.
18. Danforth R, Gibbs SJ. Diagnostic dental radiation: what is the risk? J Calif Dent Assoc 1980;8:28-35.
19. Kircos LT, Lorton L, Angin LL. Order of magnitude dose reduction in intraoral radiography. ADA 1987;114:344-7.
20. Alcox RW, Jameson WR. Patient exposures from intraoral examina- tions. J Am Dent Assoc 1974;88:558-79.
21. Price C. The effects of beam quality and optical density on image quality in dental radiography. Oral Surg 1986;62:580-8.
22. Gonad doses and genetically significant dose from diagnostic radiology: U.S., 1964 and 1970. Washington, DC: DNEW publication no. (FDA) 76-8034, 1976.
NOTICE TO MEMBERS
AAE Members are requested to send any change of address to the American Association of Endodontists, 211 E. Chicago Avenue, Suite 1501, Chicago, IL 60611 and not to the Publisher. In this way, changes can be handled more expeditiously since the mailing lists are generated in the Chicago office.
253