Embed Size (px)
Citation preview

Abscesses of the
Periodontium

Dentoalveolar abscesses consist of two main types:
1. The endodontic (periapical) abscess
formed after necrosis of the dental pulp and subsequent
infection of the root canal.
2. The periodontal abscess
formed after infection of the periodontal tissues by bacteria

Periodontal abscess Periapical abscess
Associated with preexisting periodontal
pocket.
May have no periodontal pocket, or if
present, probes as a narrow defect.
Tests show vital pulp. Tests show non-vital pulp.
Swelling usually includes gingival tissue,
with occasional fistula.
- Offending tooth may have large
restoration
- Swelling often localized to apex, with a
fistulous tract.
Radiographs show periodontal angular
bone loss and furcation radiolucency.
Presence of a periapical radiolucency
Pain usually dull and localized. Pain often severe and difficult to
localize.
Sensitivity to percussion may or may not
be present.
Sensitivity to percussion.



Periodontal abscesses have been classified in different ways
depending on the main criteria of classification.
1. Depending on the location of the abscess, they have been divided
into periodontal and gingival abscesses
2. Depending on the course of the lesion, they have been divided
into acute and chronic periodontal abscesses.
3. Depending on the number, they have been divided into single
versus multiple periodontal abscesses.

Definition
Periodontal abscess: is a localized purulent
inflammation of the periodontal tissues.
Abscesses are one of the main causes for patients
to seek emergency care in the dental clinic.

Depending on the origin of the infection
the lesions can be classified:
Gingival abscess:involves the marginal gingival andinterdental tissues, caused by impaction of foreignbodies.
Periodontal abscess:is an infection locatedcontiguous to the periodontal pocket and may resultin destruction of the periodontal ligament andalveolar bone.
Pericoronal abscess: is associated with the crown of apartially erupted tooth.

Periodontal Abscess
Occurs :
In patients with untreated periodontitis and in
association with moderate-to-deep periodontal pockets.
With improper use of oral irrigating devices that
introduce bacteria into the tissues.
Subsequent to a scaling session when a piece of calculus
becomes dislodged and remains in the pocket.

The periodontal abscess lesion contains bacteria as:
- Gram negative, anaerobic species which include Porphyromonas
gingivalis, Prevotella intermedia, Prevotella melaninogenica,
Fusobacterium nucleatum, andTannerella forsythia.
- Gram-positive bacterial species in periodontal abscesses
include Micromonas micros, Actinomyces spp., and Bifidobacterium

Clinical features:
- Pain
- Swelling
- Teeth tender on chewing and sensitive to percussion.
- Tooth is mobile and may even extrude from the alveolar socket
and feel "high" to the occlusion.
- Purulent exudate can often be noted in the periodontal pocket
around the affected tooth.
- Lymphadenopathy
- Slight increase of body temperature

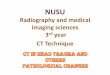
Periodontal abscess on the palatal aspect of a maxillary right first molar with a
periodontal probe in place demonstrating deep probing depth, with gingival
enlargement and discoloration

Gingival Abscess
It is a localized, acute inflammatory lesion that may arise
from a variety of sources, including:
- microbial plaque infection
- Trauma
- foreign body impaction.
- Clinical features: include a red, smooth, sometimes painful,
often fluctuant swelling.


Pericoronal Abscess
The pericoronal abscess results from inflammation of the
soft tissue operculum, which covers a partially erupted
tooth.
Inflammatory lesion may be caused by the retention of
microbial plaque, food impaction, or trauma.


Acute vs. Chronic Abscess

Acute Abscess
Mild to severe discomfort with pain
Localized red, ovoid swelling
Periodontal pocket
Mobility
Tooth elevation in socket
Tenderness to percussion or biting
Exudation
Elevated temperature
Regional lymphadenopathy
Chronic abscess
No pain or dull pain
Localized inflammatory lesion
Slight tooth elevation
Intermittent exudation
Fistulous tract often associated
with a deep pocket
Usually without systemic
involvement

Multiple abscess

Treatment
The treatment of the periodontal abscess usually includes
two stages:
(1) Management of the acute lesion
(2) Appropriate treatment of the original and/or residual
lesion, once the emergency situation has been controlled.

Treatment options
1- Drainage through pocket retraction or incision
2- Scaling and root planing
3- Periodontal surgery
4- Systemic antibiotics
5- Tooth removal

Acute Periodontal Abscess- The acute abscess is treated to alleviate symptoms, control the
spread of infection, and establish drainage.
1. Drainage through Periodontal Pocket
- The peripheral area around the abscess is anesthetized with
sufficient topical and local anesthetic to ensure comfort.
- The pocket wall is gently retracted with a periodontal probe or
curette in an attempt to initiate drainage through the pocket
entrance.
- Gentle digital pressure and irrigation to clear the pocket.
- If the lesion is small and access uncomplicated, debridement in
the form of scaling and root planing may be undertaken.

- If the lesion is large and drainage cannot be established, root
debridement by scaling and root planing or surgical access should
be delayed until the major clinical signs have abated.
- In these patients, use of adjunctive systemic antibiotics with short-
term high-dose regimens is recommended.
Antibiotic therapy alone without subsequent drainage
and subgingival scaling is contraindicated

Antibiotic option Amoxicillin, 500 mg
- 1.0-g loading dose, then 500 mg 3 times a day for 3 days.
- Reevaluation after 3 days to determine need for continued or
adjusted antibiotic therapy.
* If there is Penicillin Allergy use:
Clindamycin
- 600 mg loading dose, then 300 mg 4 times a day for 3 days.
- Azithromycin (or clarithromycin) 1.0-g loading dose, then 500
mg 4 times a day for 3 days.

2. Drainage through External Incision
- The abscess is dried and isolated with gauze sponges.
- Topical anesthetic is applied, followed by local anesthetic
injected peripheral to the lesion.
- Vertical incision through the most fluctuant center of the
abscess is made with a surgical blade.
- The tissue lateral to the incision can be separated with a
curette or periosteal elevator.
- Pus is expressed, and the wound edges approximated under
light digital pressure with a moist gauze pad.

- Post-treatment instructions include frequent rinsing with warm
salt water (1 tbsp/8-oz glass) and periodic application of
chlorhexidine gluconate either by rinsing or locally with a
cotton-tipped applicator.
- Analgesics may be prescribed for comfort.
- By the following day, the signs and symptoms will usually subside
and the lesion can be treated as a chronic abscess.

Chronic Periodontal abscess
- As with a periodontal pocket, the chronic abscess is usually
treated with scaling and root planing or surgical therapy.
- Surgical treatment is suggested when deep vertical or
furcation defects are encountered that are beyond the
therapeutic capabilities of nonsurgical instrumentation.
- As with the acute abscess, antibiotic therapy may be
indicated.

Gingival Abscess- Treatment of the gingival abscess is aimed at reversal of the
acute phase and when applicable, immediate removal of thecause.
- Topical or local anesthesia by infiltration is administered.
- When possible, scaling and root planing are completed toestablish drainage and remove microbial deposits.
- In more acute situations the fluctuant area is incised with a#15 scalpel blade, and exudate may be expressed by gentledigital pressure.
- Any foreign material (e.g., dental floss, impression material)is removed.

- The area is irrigated with warm water and covered with moist
gauze under light pressure.
- Once bleeding has stopped, the patient is dismissed with
instructions to rinse with warm salt water every 2 hours for
the remainder of the day.
- After 24 hours the area is reassessed, and if resolution is
sufficient, scaling not previously completed is undertaken.

Pericoronal Abscess- The treatment of the pericoronal abscess is aimed at management
of the acute phase, followed by resolution of the chronic
condition.
- The acute pericoronal abscess is properly anesthetized for
comfort.
- Drainage is established by gently lifting the soft tissue operculum
with a periodontal probe or curette. If the underlying debris is
easily accessible, it may be removed, followed by gentle irrigation
with sterile saline.
- If there is regional swelling, lymphadenopathy, systemic
antibiotics may be prescribed.

- The patient is dismissed with instructions to rinse with warm
salt water every 2 hours, and the area is reassessed after 24
hours.
- If discomfort was one of the original complaints, appropriate
analgesics should be employed.
- Once the acute phase has been controlled, the partially
erupted tooth may be definitively treated with either surgical
excision of the overlying tissue or removal of the offending
tooth.

Thank you