Embed Size (px)
Citation preview

J. Neurol. Neurosurg. Psychiat., 1963, 26, 528
Aberrant nerve fibres within the spinal cordJ. TREVOR HUGHES AND BETTY BROWNELL
From the Departments of Pathology and Neurology, The Radcliffe Infirmary, Oxford
Raymond (1893), in a necropsy account of a case ofsyringomyelia, described in the wall of the syrinxsmall bundles of fine nerve fibres ensheathed withSchwann cells. He traced the origin of these fibresfrom the posterior root entry zone and decided thatthey arose from axons of the cell bodies in theposterior root ganglia. Similar findings in syringo-myelia were subsequently recorded by Schlesinger(1902), Bischofswerder (1901), Jonesco-Sisesti (1929),and Druckman and Mair (1953). Similar bundles ofnerve fibres within and around the spinal cord havebeen described in other disease processes: in tabesdorsalis by Nageotte (1899), in Pott's paraplegia byFickler (1900), in malignant cord compression byBielschowsky (1901) and by Druckman and Mair(1953), in traumatic cord lesions by Henneberg(1907), by Roussy and Lhermitte (1918), and byKlaue (1949), in multiple sclerosis by Berchenko(1935), and in cervical spondylosis by Mair andDruckman (1953). These references do not exhaustthe world literature, and further instances are givenin a review of the subject undertaken by Druckman(1955) for a symposium on regeneration in the central
nervous system, held at Bethesda, Maryland, in1954. Most of these quoted references refer to singleinstances of this phenomenon which appears to berare although its exact incidence cannot be stated.In the present paper we record our own observationson the occurrence of these abnormal nerve fibres,illustrated by nine personally studied examples.The principal clinical features and neuropatho-
logical findings are given in the Table. In the accountthat follows we have confined our observations tothe detailed microscopical studies of the aberrantnerve fibres.
DESCRIPTION OF ABBERANT NERVE FIBRES STUDIED
EXAMPLE 1 The spinal cord contained a syrinx extendingfrom C4 to LI and placed asymmetrically transverselyacross the posterior half of the cord. At C6 (Fig. 1) thesyrinx, extending transversely across the cord, affectedthe left posterior horn and interrupted fibres from theleft C6 posterior nerve root. In this region, withinconnective tissue forming the posterior wall of thesynrinx, were small irregular bundles of fine nerve fibres,myelinated and ensheathed with Schwann cells (Fig. 2).
Case No. Sex and DiagnosisAge
TABLESUMMARY OF CLINICAL FEATURES
Duration of Neuropathological FindingsNeurologicalSymptoms
Position of AberrantAxons
1 C.G. M 60 Syringomyelia
2 D.G. M 37 Necrotizing myelitis
3 W.B. M 28 Necrotizing myelitis andmultiple sclerosis
4 W.S. M 59 Spinal injury with cordtransection
5 M.S. F 35 Neuromyelitis optica
6 G.H4. M 61 Acute anterior poliomyelitis
7 F.L. M 76 Secondary carcinoma ot spine
8 G.P. F 62 Cervical spondylosis
9 G.B. F 70 Diabetes mellitus andschizophrenia
Many yr. Syrinx from C4 to LI asym-metrically placed across posteriorhalf of cord
14 yr. Complete destruction of cord belowT7
10 yr. Multiple sclerosis plaques in brain;total destruction of cord below T8
16 yr. Connective tissue scar replacingdestroyed cord at T10, TI 1, andT12
11 yr. Atrophy with gliosis of opticnerves and spinal cord
40 yr. Atrophy of anterior horns andanterior roots
9 mth. Infarction of spinal cord fromTI to T7 due to tumour infiltra-tion of spine
8 yr. Spondylosis associated with C5-6and C6-7 discs, causing cordischaemia
Not known Atrophy of posterior nerve roots
528
C6 at left posterior rootentry zone in wall of syrinx
T8 to conus replacing cord
T8 to conus replacing cord
T10 to T12 in connectivetissue scar
Cervical and upper thoraciccord, in posterior columnsT7, in grey commissure
T6 in grey commissure
C6 in right anterior whitecolumn
T6 in grey commissureand anterior median sulcus
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from

<* ; 4
tf%
44>
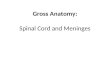
IG. 1I Case 1. Transverse section of C6 spinal cordegment showing an irregular syrinx cavity with aundle of abnormal nerve fibres in its posterior wall.ffaematoxylin and Van Gieson /x 7
FIG. 2
FIG. 3
$ft.
.*A.,
FIG. 2. Case 1. High-power magnificationof Fig. I showing the abnormal bundleto consist of irregular, intertwined axons.(Holmes x 255.)
FIG. 3. Case 2. Transverse section at LIstained for myelin. No normal spinal cordremains, instead there are bundles ofinterlacing myelinated fibres cut intransverse section. Note the plumpposterior nerve roots in contrast to theatrophied anterior nerve roots. (Weil x 12.)
FIG. 4. Case 2. Transverse section at LIstained for myelin and showing aposterior root from which fibres areentering the spinal cord and joiting theabnormal bundles. (Weil x 35.)
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from

J. Trevor Hughes and Betty Brownell
1~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~i4
>'t <,f,,tk:
-..e 0,
p
I
,1Si }m-}{'*j:8 itv '< 'bi.i4 QJ'gtR 1' 't
FIG. 5 FIG. 6
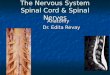
FIG. 5. Case 4. Longitudinal section of spinal cord showing fibres ofa posterior root arrested by gliosis. (Haematoxylinland Van Gieson x 102.)FIG. 6. Case 4. View from same section as Fig. S but showing fibres ofa posterior root growing into adjacent connectivetissue scar. (Haematoxylin and Van Gieson x 102.)
Serial sections demonstrated their close association withthe posterior root entry zone. Every spinal cord segmentwas sectioned but no further abnormal fibres were found.
EXAMPLE 2 This case and case 3 have been described indetail elsewhere (Hughes, 1961).The spinal cord was normal down to T6 segment
below which normal nervous tissue was totally de-stroyed.The spinal cord below T7 was completely replaced by
interlacing bundles of peripheral type nerve fibres mainlyarranged parallel to the longitudinal axis of the spinalcord (Fig. 3). In a detailed microscopic study the originof these nerve fibres from the posterior nerve roots wasdemonstrated (Fig. 4). Analysis of this and other casesshowed that in this necrotic form of myelitis, neurones,nerve fibres, and glia were completely destroyed. The finalsequel was invasion of the region of cord necrosis bynerve fibres regenerating from neurones in the posteriorroot ganglia.
EXAMPLE 3 The spinal cord was atrophied below T8having suffered almost total destruction of normal
nervous tissue. The destroyed region of the spinal cordwas replaced by large numbers of peripheral type nervefibres in the form of irregular bundles. As in case 2,their origin from the intact posterior nerve roots couldbe demonstrated.
EXAMPLE 4 The spinal cord at segments T1O, TlI, andT12 was severely damaged, being replaced by a thickconnective tissue scar enveloping the meninges. Longi-tudinal sections through cord segments TIO, TI 1, andT12 showed a scar of connective tissue merging aboveand below into gliosis. Throughout the connective tissuescar were tangled nerve fibres of peripheral type, ramify-ing widely but never entering a region of gliosis. Theorigin of these abnormal fibres from the posterior nerveroots could frequently be demonstrated (Fig. 6).
EXAMPLE 5 The spinal cord showed extensive atrophywith gliosis suggestive of an antecedent destructive pro-cess destroying grey and white matter. Bundles ofperipheral type nerve fibres were present in the posteriorcolumns on the right side near the posterior root entryzone. These were seen in many sections from the cervical
530
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from

Aberrant nerve fibres within the spinal cord
FIG. 8.
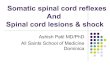
FIG. 7. Case 6. Transverse section of spinal cord at T7segment showing position of abnormal fibres in the greycommissure. The anterior horns show atrophy withneuronal loss. (Haematoxylin and Van Gieson x 27.)
FIG. 8. Case 6. High-power view of Fig. 7 showing theappearance of the bundle when stained for nerve axons.(Holmes x 255.)
and upper thoracic cord segments where they formed anabnormal bundle seen in the posterior columns. In somesections fibres were demonstrated joining the bundlefrom nearby posterior nerve roots.
These five examples may be conveniently con-sidered together, for they are similar in that in eachcase the spinal cord was invaded by abnormal fibresarising from the posterior or nerve roots.The common factor was long survival after a
destructive process involving the region of posteriornerve root entry (in cases 1 and 5) or the wholecross-section of the cord (in cases 2, 3, and 4). Incase 1 the position of the abnormal fibres suggestedstrongly that they arose from posterior nerve roots.This origin was quite certain in cases 2, 3, 4, and 5since nerve fibres could be followed in serial histo-logical sections from the plump healthy posteriornerve roots into the spinal cord to join the inter-lacing bundles of abnormal fibres. In cases 2, 3, and4 there was no possibility of proliferation from othercell bodies or axons, for these had perished in thesevere and total spinal cord necrosis.
In the next three instances the pathology wasdifferent as was the location of the aberrant fibres.
EXAMPLE 6 The spinal cord showed in its thoracic andlumbar regions atrophy of the anterior nerve roots andneuronal depletion with gliosis in the anterior horns.In the T7 spinal cord segment a small spherical bundleof intertwined fine myelinated nerve fibres was situatedin a perivascular space in the grey commissure on theright side (Figs. 7 and 8). Serial sections demonstratedthe shape, size, and extent of these abnormal nervefibres but failed to show their origin. From theirposition they were presumed to arise from cell bodiesin the right anterior horn.
EXAMPLE 7 The spinal cord from TI to T7 had sufferedinfarction from extensive infiltration of the spine bytumour. Tumour was present in the extradural space buthad not invaded the spinal canal or its leptomeninges.
In T6 spinal cord segment a small bundle of peripheraltype nerve fibres (myelinated and associated withSchwann-cell nuclei) was present in the grey commissureon the right side. The bundle, composed of intertwinedfine axons, was surrounded by a thin layer of spongyconnective tissue, the whole structure being within aperivascular space. Serial sections demonstrated theextent and the spherical shape of the bundle but failedto show its origin. The neighbouring anterior and lateralgrey horns were severely depleted of neurones by theneoplastic process.
lmFh
FIG. 7
531
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from

J. Trevor Hughes and Betty Brownell
FIG. 9. Case 8. Low-powerview of right anterior part oftransverse section throughC6 spinal cord segment.The abnormal fibres aresituated in a perivascular spacein the right anterior whitecolumn.(Haematoxylin and VanGieson x 27.)
*."A-;L-*~.EXAMPLE 8 Severe spondylosis affected the cervical spinewith protrusions associated with C5 to C6 and C6 to C7discs bulging backwards into the spinal canal and indent-ing the spinal cord. The spinal cord showed myelin andneuronal loss from C6 to C8 with vascular proliferationsuggestive of ischaemia. Wallerian degeneration was
evident above and below the affected segments. A fusi-form bundle of fine myelinated peripheral type nerve
fibres was present in C6 spinal cord segment within a
radially situated perivascular space in the right anteriorwhite column (Figs. 9 and 10). Serial sections demon-strated their extent and suggested, but did not prove,
their origin from cell bodies in the right anterior horn.
FIG. Case 8. High-
power view of abnormal"t* :4 vT i fibres seen in Figure 9.
(Haematoxylin and VanGieson x 255.)
4*,28 ; v
The three cases just described were alike in having
a disease affecting the anterior horn cells. In each a
small bundle of abnormal nerve fibres was found in a
perivascular space: in cases 6 and 7 in the grey
commissure and in case 8 in the anterior white
column. In none could the precise origin of the
fibres be established but from their position the
likeliest explanation was that they arose from cell
bodies in the anterior horn.
EXAMPLE 9 In T6 cord section small bundles of inter-
twined axons surrounded the vessels in the anterior
0 ~~~~~~~~~~~~~~~~~~~~......~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~....::........ . ....*: ^ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......I~~~~~~~~~~~~~~~~~
532
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from

Aberrant nerve fibres within the spinal cord
DISCUSSIONts ..
X
w...... . .. . ..* :.Y
* .. -: ; .._ Pt
q0:' i ': .4.
; > X,.4* -.<.'S #85 o# _ ' # '.w ... ; v.
e . v4
0:,- S ^
*-+t. < *, *t..:t,+.. tPw . P..- ^ > e.w . ... *> ,,e, w w
.4, ;,- g 9 f....: ..; *% ...
-. * w.'A ,; N r r:,^3S ;:: .:s x:
it . jz>j, Pw n X asX r M- $ } ^ '§S JS*v._ §*_vA..-- B.|s .s: 'S
*§-y ag t} -# ^R S gWi-;
.8e tW y v
,4Z'j3f.: *, .:
t-<
4. e vZ Yi:o:
*s 4
FIG. 11. Case 9. Transverse section of T6 spinal cordsegment showing anterior median sulcus with manyabnormal fibres around a siulcal artery. (Haematoxylinand Van Gieson x 102.)
median sulcus (Fig. 11) and were present in severalperivascular spaces in the grey commissure on the leftand in two spaces on the right. The appearances sug-gest ramifying nerve fibres entering the spinal cordalongside a sulcal branch of the anterior spinal artery.Similar bundles of abnormal fibres were seen in theleptomeninges on the lateral aspect of the cord and nearone posterior nerve root.
In this last instance the findings differed from allthe other cases in that the abnormal fibres werepresent in greatest numbers in the anterior mediansulcus around a sulcal artery. Within the spinalcord they were present in much smaller numbers intwo perivascular spaces in the grey commissure,one on either side of the central canal, these vesselsbeing branches of the sulcal artery. These abnormalfibres had probably entered the spinal cord centri-petally along the spinal vessels. Their exact origincould not be determined but the presence of similarfibres near one posterior nerve root and the clinicalevidence of diabetes mellitus suggested the possi-bility of their arising from nerve roots damaged bya diabetic neuropathy.
The nature and origin of these abnormal nerve fibreshas been the subject of recurrent speculation whichis reviewed by Druckman and Mair (1953) withwhose conclusions we are mainly in agreement. Thesuggestion that the fibres concerned are abnormallyplaced spinal nerve roots can be discounted, astheir interlacing pattern is quite unlike the parallelfibres of a normal spinal nerve root. They are notnormal perivascular nerves (as described and illu-strated by Clark in 1929), for the aberrant fibres arepresent in much greater numbers and differ in al-ways possessing myelin sheaths. That these bundlesmight be neurofibromata does not require extensiveconsideration, for the resemblance is quite superficial,and all the structures we have described in this papercan be demonstrated with silver stains to be com-posed of interwoven axons. We arrive at the mostprobable explanation that these aberrant nervetangles are the result of proliferation of severedaxons.From our analysis of the cases it can be seen that
we favour in six cases showing these abnormalfibres (cases 1, 2, 3, 4, 5, and 9) an origin in the cellbodies of the posterior spinal ganglia. In the otherthree cases we have suggested an origin in theanterior horn neurones. In none of our cases wasthere evidence for regeneration from long intra-spinal nerve fibres, and so our findings do notsupport the contention (held by an importantminority) that regeneration of this type of injuredaxon occurs within the spinal cord.The nerve fibre bundles we have described are
more akin to neuromata occurring after peripheralnerve or spinal root section. That they occur withinthe spinal cord seems to us less important than theobservation that in other respects they are similar totraumatic neuromata. Severed posterior root axonshave a propensity to regenerate as we have recentlyobserved in necropsy studies in a case of posteriorrhizotomy for intractable pain. The regeneratingnerve fibres were identical histologically with thosewe describe here though ramifying only in the lepto-meninges and not entering the intact spinal cord.One pertinent observation common to all our casesis that the immediate environment of the abnormalnerve fibres, even though technically within thespinal cord, is not central nervous tissue but meso-dermal connective tissue. This relationship was mostevident in case 4 where a traumatic connective tissuescar replaced large areas of the spinal cord. Themesodermal scar was everywhere invaded by peri-pheral type fibres which never entered nearby areasof normal or gliosed central nervous tissue. Itseems that these fibres, for some interesting and
533
ir
V.
4p.0%
qp
IN-
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from

J. Trevor Hughes and Betty Brownell
hitherto unexplained reason, are not usually able togrow into central nervous tissue. This observationhas a parallel in animal experiments, such as thoseof Windle, Clemente, and Chambers (1952). Theseworkers embedded the cut proximal end of the facialnerve of cats, rabbits, and rats into the animal'sown brain. The interesting result was a connectivetissue scar containing a large neuroma whose fibresfailed to invade the neighbouring brain. The barrierto such invasion is not seemingly insuperable, forWindle et al., by treating their animals with piromen,A.C.T.H., or desoxycorticosterone, could persuadethe proliferating fibre of the implanted nerve tospread into the adjacent brain tissue.
Concerning the function of these abnormal nervefibres, it is clear that they serve no useful purpose.Cases 2, 3, and 4 had suffered a complete paraplegiawith total interruption of all motor and sensorypathways. The invasion of the spinal cord byabnormal fibres of peripheral nerve type was veryextensive, yet there was no evidence of any clinicalimprovement in their many years of paraplegic life.
SUMMARY
Nine instances are reported in which at necropsyirregular bundles of fine myelinated axons associatedwith Schwann-cell nuclei were found inside thespinal cord.
In six cases the nerve bundles appeared to arisefrom posterior nerve roots, this origin being clearlydemonstrable in five cases. In three cases the spinalcord was replaced to a remarkable extent by theseabnormal fibres, which could only have arisen fromthe posterior nerve roots, for all other cell bodiesand axons had perished in the severe and totalspinal cord necrosis. In three cases the position of
the nerve bundles suggested their origin from cellbodies of anterior horn neurones.The abnormal nerve fibres were always surround-
ed by mesodermal connective tissue, never by gliosisor normal central nervous tissue.
All the instances followed some destructive pro-cess, suggesting that the origin of the fibres was theproliferation of severed axons.None of these cases provided evidence for re-
generation from long intraspinal nerve fibres, forthe nerve fibre bundles described could never betraced to this type of injured axon.
The observations recorded in this paper were made pos-sible by the courtesy of the many people from whom wereceive material for neuropathological examination.For clinical details we thank Dr. W. Ritchie Russell
(cases 1, 5, and 8), Dr. Ludwig Gutman (cases 2, 3, and4), Dr. J. D. Kidd (case 6), Mr. J. Pennybacker (case 7),and Dr. Sabina Strich (case 9).
REFERENCES
Berchenko, F. (1935). Schweiz. Arch. Neurol. Psychiat.. 37, 3.Bielschowsky, M. (1901). Neurol. Zbl., 20, 242.Bischofswerder, L. (1901). Rev. neurol., 9, 178.Clark, S. L. (1929). J. comp. Neurol., 48, 247.Druckman, R. (1955). In Regeneration in the Central Nervous Svstem,
edited by W. F. Windle, p. 241. Thomas, Springfield, Illinois.and Mair, W. G. P. (1953). Brain, 76, 448.
Fickler, A. (1900). Dtsch. Z. Nervenheilk., 16, 1.Henneberg, R. (1907). Charite-Ann., 31, 161.Hughes, J. T. (1961). M.D. Thesis, University of Manchester.Jonesco-Sisesti, N. (1929). Tumeurs Medullaires Associees Li un
Processus Syringomyelique. Masson, Paris.Klaue, R. (1949). Wien. Z Nervenheilk., 2, 488.Mair, W. G. P., and Druckman, R. (1953). Brain, 76, 70.Nageotte, J. (1899). C.R. Soc. Biol. (Paris), 51, 738.Raymond (1893). Arch. Neurol. (Paris), 26, 97.Roussy, G., and Lhermitte, J. (1918). Les Blessures de la Moelle et de
la Quete de Cheval. Masson, Paris.Schlesinger, H. (1902). Die Syringomyelie, 2nd ed. Deuticke, Leipzig
and Vienna.Windle, W. F., Clemente, C. D., and Chambers, W. W. (1952).
J. comp. Neurol., 96, 359.
534
Protected by copyright.
on April 18, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.26.6.528 on 1 Decem
ber 1963. Dow
nloaded from