Embed Size (px)
Citation preview

iologicalsychiatry
Archival Report BP
Aberrant Cortical Morphometry in the 22q11.2Deletion SyndromeJ. Eric Schmitt, Simon Vandekar, James Yi, Monica E. Calkins, Kosha Ruparel, David R. Roalf,Daneen Whinna, Margaret C. Souders, Theodore D. Satterthwaite, Karthik Prabhakaran,Donna M. McDonald-McGinn, Elaine H. Zackai, Ruben C. Gur, Beverly S. Emanuel, andRaquel E. Gur
ABSTRACTBACKGROUND: There is increased risk of developing psychosis in 22q11.2 deletion syndrome (22q11DS). Althoughthis condition is associated with morphologic brain abnormalities, simultaneous examination of multiple high-resolution measures of cortical structure has not been performed.METHODS: Fifty-three patients with 22q11DS, 30 with psychotic symptoms, were compared with demographicallymatched nondeleted youths: 53 typically developing and 53 with psychotic symptoms. High-resolution magneticresonance imaging measures of cerebral volume, cortical thickness, surface area, and an index of local gyrificationwere obtained and compared between groups.RESULTS: Patients with 22q11DS demonstrated global increases in cortical thickness associated with reductions insurface area, reduced index of local gyrification, and lower cerebral volumes relative to typically developing controls.Findings were principally in the frontal lobe, superior parietal lobes, and in the paramedian cerebral cortex. Focallydecreased thickness was seen in the superior temporal gyrus and posterior cingulate cortex in 22q11DS relative tonondeleted groups. Patterns between nondeleted participants with psychotic symptoms and 22q11DS were similarbut with important differences in several regions implicated in schizophrenia. Post hoc analysis suggested that likethe 22q11DS group, cortical thickness in nondeleted individuals with psychotic symptoms differed from typicallydeveloping controls in the superior frontal gyrus and superior temporal gyrus, regions previously linked toschizophrenia.CONCLUSIONS: Simultaneous examination of multiple measures of cerebral architecture demonstrates thatdifferences in 22q11DS localize to regions of the frontal, superior parietal, superior temporal, and paramidlinecerebral cortex. The overlapping patterns between nondeleted participants with psychotic symptoms and 22q11DSsuggest partially shared neuroanatomic substrates.
Keywords: 22q11 Deletion syndrome, Cortical thickness, Genetics, Gyrification index, MRI, Psychosis
ISS
http://dx.doi.org/10.1016/j.biopsych.2014.10.025
The 22q11 deletion syndrome (22q11DS) is the most commonknown human genetic microdeletion, occurring in approxi-mately 1:2000 live births (1). This hemizygous deletion at22q11.2 spans �3 Mb, although other deletion sizes areobserved (2). The deletion results in a variable combination ofcraniofacial, cardiovascular, endocrine, and psychiatric abnor-malities (1). Congenital heart disease has been reported in upto 70% of individuals, including Tetralogy of Fallot, ventricularseptal defects, and truncus arteriosus (1,3). Cleft palate andother oropharyngeal abnormalities are common (4), as arepharyngeal and intracranial vascular abnormalities (1,5,6).Likewise, more prevalent are thymic aplasia and diminishedperipheral T cells (7), hypothyroidism, hypoparathyroidism,and hypocalcemia (4).
The 22q11DS also imparts a significantly increased risk ofintellectual disability and liability for several psychiatric dis-orders, most notably schizophrenia (8,9); the presence of the
N: 0006-3223 Bi
SEE COMMENTA
22q11DS is among the greatest known risk factors for psy-chosis (10,11). Neuroimaging studies have sought to character-ize functional neuroanatomy of 22q11DS as a geneticallydetermined subtype of schizophrenia. Volumetric magneticresonance imaging (MRI) studies have demonstrated globalreductions in cerebral volumes (CV) compared with typicallydeveloping (TD) control subjects, with some studies suggestingrelative sparing of the frontal lobes (12,13). More recent studieshave explored newer measures of cerebral morphometry suchas cortical thickness (14–17), cerebral surface area (16), andmeasures of gyral complexity (18,19). These reports havesuggested increased frontal and inferior parietal cortical thick-ness and decreased thickness in the parieto-occipital region,decreased surface area in frontal and occipital lobes, anddecreased gyral complexity in 22q11DS.
The current study represents a comprehensive high-resolution examination of the cerebral architecture of
& 2015 Society of Biological Psychiatry 135ological Psychiatry July 15, 2015; 78:135–143 www.sobp.org/journal
RY ON PAGE

Table 1. Demographic Characteristics of the Samples
22q11DS ND-TD ND-PS p Value
n 53 53 53
Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
22q11DS and nondeleted (ND) patients with psychotic symp-toms using anatomic MRI. It also represents one of the largeststudies of brain morphometry to date.
Age 20.3 (4.5) 18.6 (2.6) 18.5 (2.5) .01
14.6–29.7 13.3–21.9 13.3–21.8
Gender 27 M (51%) 27 M (51%) 27 M (51%) 1
26 F (49%) 26 F (49%) 26 F (49%)
Race 43 White (81%) 34 White (64%) 39 White (74%) .37
7 AA (13%) 15 AA (28%) 10 AA (19%)
3 Other (6%) 4 Other (8%) 4 Other (8%)
p values are based on analysis of variance for age and chi-squaretest for categorical variables.
22q11DS, 22q11 deletion syndrome; AA, African American; ND,nondeleted; PS, psychotic symptoms; TD, typically developing.
METHODS AND MATERIALS
Sample
The 22q11DS sample was drawn from a prospective study,Brain-Behavior and Genetic Studies of the 22q11DS, at theUniversity of Pennsylvania and Children’s Hospital of Phila-delphia (CHOP). Subjects were recruited from the 22q and YouCenter at CHOP and through social media. Inclusion criteriawere age $ 8, English proficiency, estimated IQ . 70 byclinical testing and the Wide Range Achievement Test 4 (20),and stable medical status. Exclusion criteria were pervasivedevelopmental disorder or IQ , 70 and medical disorders thatmay affect brain function (e.g., uncontrolled seizures, headtrauma, central nervous system tumor and infection) or visualperformance (e.g., blindness). Subjects 12 years or older wereeligible for MRI scanning.
Psychopathology was assessed with the Kiddie-Schedulefor Affective Disorders and Schizophrenia (21), StructuredInterview for Prodromal Syndromes (22), and the psychoticand mood differential diagnoses modules of the StructuredClinical Interview for DSM-IV (modules C and D) (23). Asdetailed previously (20), positive, negative, and disorganizedsymptoms were rated on the 7-point Scale of ProdromalSymptoms from the Structured Interview for Prodromal Syn-dromes (22) (0 5 absent, 1 5 questionably present, 2 5 mild,3 5 moderate, 4 5 moderately severe, 5 5 severe but notpsychotic, and 6 5 severe and psychotic). A prodromediagnosis was given if a patient had one positive symptomrated $3 or at least two negative and/or disorganized symp-toms rated $3 within the past 6 months. The 22q11DSpsychosis spectrum group included those with the prodromediagnoses and psychiatric disorders with psychotic symptoms(schizophrenia, psychosis not otherwise specified, majordepression with psychotic features, schizoaffective disorder,and delusional disorder).
Deletion status was confirmed using multiplex ligation-dependent probe amplification (24). University of Pennsylvaniaand CHOP institutional review boards approved all proce-dures. Informed consent/assent was obtained from eachparticipant and accompanying parent for those younger than18 at the time of initial evaluation.
Control groups were obtained from the Philadelphia Neuro-developmental Cohort (PNC), a prospective neuroimagingsample of 1400 youths aged 8 to 21 years (25–27). Anautomated optimal matching algorithm developed by Kosankeand Bergstralh (28) (GREEDY) written in SAS (SAS Institute,Cary, North Carolina) generated a 1:1 typically developing(ND–TD) subsample from this population matched to the22q11DS sample based on age, race, and gender (28). Asecond subsample of subjects from the PNC with psychosisspectrum symptoms (PS) (ND–PS) was obtained and similarlymatched using an automated algorithm. Psychosis spectrumsymptoms were assessed using an abbreviated Kiddie-Schedule for Affective Disorders and Schizophrenia andscales for measuring subthreshold psychotic symptoms,
136 Biological Psychiatry July 15, 2015; 78:135–143 www.sobp.org/jo
including the PRIME Screen-Revised and selected Scale ofProdromal Symptoms scales (21,26,27). Summary groupstatistics are provided in Table 1.
Image Acquisition
High-resolution axial T1-weighted magnetization prepared rapidacquisition gradient-echo was acquired, with the followingparameters; repetition time/echo time 1810/3.51 milliseconds;inversion time 1100 milliseconds; field of view 180 3 240 mm;effective resolution 1 mm3. Subjects were scanned by a boardcertified technologist on the same 3T MRI scanner (TIM Trio;Siemens, Erlangen, Germany) using a 32-channel head coil.
Image Processing
Digital imaging and communications in medicine images wereimported into FreeSurfer version 5.0, a freeware image-processing program (MGH, Harvard, Cambridge, Massachu-setts; http://surfer.mgh.harvard.edu). FreeSurfer’s surface-basedimage processing pipeline has been described (29–32). Briefly,for each subject, image intensity was normalized to account formagnetic field inhomogeneity. The skull and other nonbraintissues were removed (33). Preliminary segmentation was thenperformed using a connected components algorithm. The sur-face boundary was then covered with a polygonal tessellationand smoothed, resulting in high-resolution vertices over bothcerebral hemispheres. A deformable surface algorithm wasthen employed to identify the pial surface. For all subjects, thecortical surface model was manually reviewed and edited ifnecessary.
CV, cortical thickness (CT), surface area (SA), and localgyrification index (lGI) were subsequently calculated at highresolution. Cortical thickness is estimated as the distancebetween the pial surface and the gray-white matter junction(31). Surface area was calculated by measuring the averagetriangular size surrounding the tessellated cortical vertices,following deformation of individual subject vertices (32,34).Maps of CV could then be generated by calculating theproduct of SA and CT at each vertex.
Gyrification index was determined using a method originallydescribed by Schaer et al. (19) for evaluating gyral complexityin 22q11DS and subsequently integrated into FreeSurfer.Briefly, this method creates a smoothed outer surface sur-rounding the more convoluted pial surface at every vertex. The
urnal

Table 2. Mean (SD) Global Measures by Group
CorticalVolume (mm3)
CorticalThickness (mm)
SurfaceArea (mm2) lGI
ND–TD 525788(68511)
2.69 (.09) 176346(19263)
3.01(.13)
ND–PS 543620(60455)
2.68 (.11) 171569(19535)
3.01(.21)
22q11DS 495180(56334)
2.75 (.10) 157533(19192)
2.88(.17)
p Value .0009 .0004 ,.0001 .0001
22q11DS, 22q11 deletion syndrome; lGI, local gyrification index;ND, nondeleted; PS, psychotic symptoms; TD, typically developing.
Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
algorithm then calculates the ratio of the inner and outersurfaces for j faces in the three-dimensional mesh
GIj3D 5∑MP
j 5 1AjP
∑MOj 5 1A
jO
where AjP and Aj
Orepresent the pial and outer (smoothed)surfaces, respectively, and MP and MO represent the totalnumber of faces in the pial and outer mesh.
Statistical Analyses
Measures of total cortical volume, total surface area, meancortical thickness, and mean lGI were calculated to identifyglobal group differences in cerebral morphology. Analysis ofvariance (ANOVA) was performed with diagnostic group as anindependent factor controlling for linear and nonlinear effectsof age, sex, and race. Post hoc Tukey-Kramer tests wereemployed to identify which groups drove global differences.
Three group ANOVAs were then performed at each vertex forCT to identify significant group differences, controlling for linearand nonlinear effects of age, sex, and race. Control for multipletesting was performed using false discovery rate (FDR), with athreshold of q 5 .05 (35). Univariate ANOVA probability mapswere similarly constructed for measures of SA, CV, and lGI.Post hoc pairwise t tests were performed to identify whichgroup contrasts were driving the observed differences in brainmeasures. Control of multiple testing was performed via FDR.
To explore the relationships between 22q11DS and psycho-sis, we performed subgroup analyses comparing the 3022q11DS subjects with psychosis spectrum symptoms withtheir matches from the ND–TD and ND–PS groups (Table S1 inSupplement 1). Post hoc pairwise tests were similarly performedon the full group models. We similarly contrasted cerebralmeasures between the 22q11DS subjects with and withoutpsychosis spectrum symptoms (Table S2 in Supplement 1).
To increase sensitivity for subtle group differences (parti-cularly between the two nondeleted groups), we reanalyzedthe data using cluster threshold permutation methods ratherthan FDR to control for multiple testing (33–35). Thesemethods, adapted for surface-based anatomical analysis frommethods originally designed for functional MRI data, are builtinto the FreeSurfer environment. They use permutation toestimate maximum cluster size assuming that false-positivevertices are less likely to be near each other; thus, unlike FDR,cluster thresholding takes advantage of spatial informationinherent to imaging data. The cluster thresholding approachdoes sacrifice spatial specificity relative to FDR in return for anincreased sensitivity for small but more regional group differ-ences. For these analyses, a full-width at half maximum of 20with 5000 permutations and global p value threshold of .05were used to identify significant clusters. Post hoc statisticaltesting of pairwise group differences was then performed, withcontrol of multiple testing via the Tukey-Kramer test.
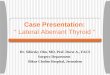
Figure 1. Probability maps from four-group analysis of variance showingregional differences in cerebral volume, cortical thickness, surface area, andlocal gyrification index. Statistical maps for each hemisphere are firstmasked at pFDR 5 .05 and then displayed at an uncorrected threshold of1.3 , 2log(p) , 4 for consistency. FDR, false discovery rate.
RESULTS
Global Measures
Patients with 22q11DS had significantly reduced total corticalvolumes relative to nondeleted control subjects (Table 2).
Biological
These reductions were driven by global reductions in totalbrain area rather than reductions in cortical thickness. Indeed,global measures of thickness were significantly increased in22q11DS relative to control subjects. Mean lGI was decreasedin the 22q11DS group. Statistically significant group differ-ences were identified for all four global measures, withp values , .0009. Global differences were primarily driven bydifferences in deletion status; there were no significant differ-ences between the TD and PS groups. Vertex level ANOVAdemonstrated that significant differences in all measures wereheterogeneous throughout the cerebrum (Figure 1), with themidline cortex and frontal and superior parietal lobes parti-cularly affected.
Cerebral Volume
Subjects with 22q11DS had multiple foci of significantly lowerCV relative to ND–TD (Figure 2); differences were centered onthe rostral lateral frontal lobe, superior parietal lobe, medialoccipital lobe, and temporal pole. Relative volumetricincreases were observed in the insular cortex bilaterally in22q11DS relative to ND–TD. Similar but less extensive differ-ences were seen when comparing 22q11DS and ND–PSgroups. An exception was a focal region of bilaterallydecreased volume in the caudal frontal lobe in ND–PS relativeto 22q11DS. There were no significant differences between22q11DS subjects with and without psychosis spectrum
Psychiatry July 15, 2015; 78:135–143 www.sobp.org/journal 137

Figure 2. Group differences driving significantchanges in cortical thickness. Pairwise probabilitymaps depicting significant increases (blue) anddecreases (red/yellow) in several morphological mea-sures as compared with typically developing (ND–TD)and idiopathic psychotic symptom (ND–PS) groups.Statistical maps for each hemisphere are first maskedat pFDR 5 .05 and then displayed at an uncorrectedthreshold of 1.3 , 2log(p) , 4 for consistency.22q11DS, 22q11 deletion syndrome; FDR, false dis-covery rate; ND, nondeleted; PS, psychosis symp-toms; TD, typically developing.
Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
symptoms or between the ND–TD and ND–PS groups afteradjusting for multiple testing.
Cortical Thickness
Thicker cortex was seen in 22q11DS relative to the ND–TDgroup in frontal lobes bilaterally, orbitofrontal cortex bilaterallyextending into anterior insula and operculum, inferior parietallobe and paracentral lobule, fusiform gyrus, cuneus, andparacalcarine cortex (Figure 2). In contrast, significantly lowercortical thickness in 22q11DS was observed in anterior andmiddle superior temporal gyrus and mid to posterior cingulategyrus bilaterally. Similar patterns were seen for the 22q11DScompared with ND–PS. However, we observed additional fociof significantly greater thickness in 22q11DS in left dorso-lateral prefrontal cortex and right insula and less pronounceddecreases in superior temporal cortex and medial frontallobes. Direct comparison between ND–TD and ND–PS groupsdid not demonstrate significant findings at vertex level.Similarly, no significant differences in cortical thickness wereseen between 22q11DS subjects with and without psychosisspectrum after controlling for multiple testing with FDR.
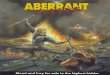
Clusterwise correction identified 10 significant clusters(Figure 3). For clusters in the parietal and occipital lobes, groupdifferences were driven by significantly thicker cortex in22q11DS compared with the two control groups. In contrast, acluster including portions of the left superior frontal gyrus,anterior cingulate, and medial orbitofrontal cortex was morecomplex, with significant differences between all groups and
138 Biological Psychiatry July 15, 2015; 78:135–143 www.sobp.org/jo
with the ND–PS intermediate in thickness between the other twogroups. A similar pattern was seen in left superior temporal lobe(STG). In right STG, there were significant group decreases inthe ND–PS group relative to ND–TD (p 5 .001). The results fromcluster analyses for CV, surface area, and local gyrification indexare presented in Figure 2S in Supplement 1.
Surface Area
Analysis of cerebral surface area identified multiple areas thatwere significantly smaller in 22q11DS relative to TD (Figure 2). Onthe lateral surface, rostral frontal lobes, superior parietal lobe, andlingual gyrus were particularly affected bilaterally. Midline arealdifferences were more extensive than those of cortical thickness,with large portions of the medial superior frontal gyrus, anteriorcingulate cortex, and midline occipital lobe affected bilaterally.Similar findings were seen comparing 22q11DS with the ND–PSgroup at the vertex level, with less extensive differences inthe lateral temporal lobe relative to the 22q11DS compared withND–TD contrast. There were no significant differences betweenND–TD and ND–PS groups or between 22q11DS subjects withand without psychosis spectrum. Cluster models producedsimilar patterns; group differences were entirely driven by arealdecreases in 22q11DS relative to ND-TD; there were nosignificant differences between ND–PS and 22q11DS.
Local Gyrification Index
Analysis of lGI demonstrated group differences in gyral com-plexity (Figure 2). Smaller lGIs were noted in 22q11DS
urnal

Figure 3. Regional group differences in cortical thickness. Brain maps at center show significant vertices (global p , .05) as determined via clusterthreshold analysis. Plots along the periphery demonstrate group differences in mean cortical thickness for each significant cluster. Vertical lines represent95% confidence intervals for mean cortical thickness for each group. Significant two-way group differences are displayed with brackets (adjusted p values;***p , .0001; **p , .01, *p , .05). 22q11DS, 22q11 deletion syndrome; ND, nondeleted; PS, psychosis symptoms; TD, typically developing.
Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
throughout anterior and posterior midline cerebral cortex, inorbitofrontal cortex and frontal pole, centered over angulargyrus and extending into the remainder of the inferior parietallobe, and mid precentral and postcentral gyrus. Similar tosurface area, group differences were principally explained bydeletion status. Cluster threshold models produced similarfindings, with significant decreases in mean lGI (p , .0001)between 22q11DS and other groups in all cases.
DISCUSSION
Although schizophrenia is a devastating condition with sig-nificant morbidity and mortality, the underlying biologicalmanifestations remain elusive. Twin and family studies havedemonstrated a strong genetic influence on liability to developschizophrenia (10) and large-scale genetic studies have begunto identify putative genes, most with very small effect sizes(36). Understanding the neural substrates of this geneticvariation remains an area of active research. 22q11DS repre-sents the genetic variant of the largest effect on liability toschizophrenia and thus warrants investigation.
Our study provides a comprehensive examination of mor-phological characteristics of 22q11DS in a relatively largesample at high resolution and high field strength. Our findingsreplicate observed patterns of volumetric reductions inparieto-occipital cortex, dorsolateral prefrontal cortex, andmidline structures, with relative increases in insular volumescompared with the ND–TD (12,15,16,37,38). In 22q11DS, we
Biological
additionally identified significantly thicker cortex in the frontallobes, inferior parietal lobes, lingual gyrus, and medial occipitallobes. Higher cortical thickness in these regions was associ-ated with corresponding smaller mean surface area. Theobserved patterns of areal reduction in 22q11DS were similarto, but more extensive than, the observed increases in corticalthickness. We also observed extensive midline, frontal, andparietal reductions in cortical gyral complexity relative toND–TD control subjects.
A similar approach by Jalbrzikowski et al. (16) simultane-ously examined differences in cortical thickness, surface area,and volume in a sample of 31 individuals with 22q11DS (meanage 16.4 years) and 34 matched ND–TD control subjects, alsoat 3T. FreeSurfer analysis of 60 cortical regions of interestidentified volumetric reductions in frontal lobes, anteriorcingulate, cuneus, precuneus, superior parietal, and temporalcortex. Like the current study, the volumetric differences wereprimarily driven by decreases in cortical surface area. Alsosimilar to the current study, they observed relatively thickenedcortex in 22q11DS, most pronounced in frontal lobes. Thus,higher cortical thickness may explain why early volumetricstudies observed relative preservation of the frontal lobe (12)despite the observed large reductions in area. Schaer et al.(14) similarly reported increased cortical thickness in frontalregions in a large sample of children and adolescents with22q11DS. However, in this longitudinal study, deviant trajec-tories of cortical thickness were observed in 22q11DS com-pared with ND–TD; while dorsal frontal regions were thicker in
Psychiatry July 15, 2015; 78:135–143 www.sobp.org/journal 139

Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
22q11DS during late childhood and adolescence, thickness inthese regions by adulthood was comparable with ND–TD(group by age interaction). Schaer et al. (14) also observedthis interaction in left superior temporal gyrus; although therewere no significant group differences in younger subjects,relative decreases in this region manifested by adulthood in22q11DS.
Unlike elsewhere in the brain, we also observed significantreductions in cortical thickness within superior temporal lobesand in mid cingulate gyrus bilaterally in 22q11DS. Several priorstudies on 22q11DS suggested morphological deficits insuperior temporal gyrus. Jalbrzikowski et al. (16) observedreductions in superior temporal lobes in their region of interestanalysis, although the findings did not reach statistical sig-nificance. Eliez et al. (39) identified significant reductions inhand-drawn superior temporal gyrus volumes in 23 childrenand adolescents with 22q11DS compared with matchedND–TD; these differences were not significant after adjustingfor global brain volume. Aberrant morphology of STG has longbeen associated with schizophrenia (40), with recent studiesshowing reductions in both gray matter density and corticalthickness (41,42). A large study by Chow et al. (43) on subjectswith 22q11DS demonstrated significant reductions in STGgray matter density in the group with schizophrenia, a findingparticularly interesting given that STG morphological abnor-malities have been associated with idiopathic schizophrenia.
To further characterize the neurodevelopmental patterns in22q11DS, we examined differences in gyral complexity usingthe local gyrification index. We identified smaller lGI in22q11DS, primarily in the paramidline cerebral cortex andextending to the superior and lateral parietal cortices.Decreases in gyrification in frontal and parietal lobes havebeen reported in several studies at lower levels of resolution(18,44). Prior studies of gyral complexity at vertex level arelimited. For example, Schaer et al. (45) examined lGI in 44young individuals with 22q11DS (mean age 9.1 years) and alsoidentified significantly smaller lGIs in orbitofrontal cortex,superior parietal lobes extending into the angular gyri, andmidline structure including the cingulate cortex and midlineparietal and occipital lobes. Likewise, Srivastra et al. (46)examined lGI in 49 children with 22qDS (mean age 10.74years) and found lower measures of gyral complexity in midlinestructures and within the parietal lobes and orbitofrontalcortices. Although our findings suggest more extensivechanges in the midline frontal lobes, the overall pattern offindings is strikingly similar to these prior reports.
Considered together, the overlapping patterns of generallythicker cortex, smaller surface area, and reduced gyral com-plexity are suggestive of aberrant neural organization andmigration in 22q11DS, most pronounced in the frontal andparietal lobes and midline occipital lobe. Thickened cortexcompared with ND–TD control subjects is an unusual findingin the literature, although it has been reported with otherneurodevelopmental conditions including Williams syndrome(47), autism (48,49), and both idiopathic polymicrogyria andlissencephaly (50,51). Notably, neuropathologic correlation in22q11DS is limited, with a single case series demonstratingextensive microscopic gray matter heterotopia in one of threespecimens (52). Qualitative MRI studies have reported pachy-gyria and polymicrogyria (abnormalities of migrational and
140 Biological Psychiatry July 15, 2015; 78:135–143 www.sobp.org/jo
postmigrational neuronal development, respectively) in22q11DS (53,54), findings that may relate to the quantitativereductions in lGI found in the current study. Although qual-itative reports of polymicrogyria have not noted as extensiveor consistent findings compared with newer quantitativemeasures, differences are likely due to increased sensitivityof these new measures to detect more subtle abnormalities.
The potential etiologies of polymicrogyria are myriad andinclude genetic, metabolic, infectious, and traumatic causes(55). However, it is hypothesized that most are ultimatelycaused by vascular injury resulting in disruption of cellularinteractions at the glial-pial barrier (51). A putative vascularcause of neuromigrational abnormalities is a particularlyintriguing hypothesis in 22q11DS, given the spectrum ofcardiovascular features associated with the condition (1).Schaer et al. (56) have described an association betweencongenital heart disease and gyrification at the parieto-temporal-occipital junction, although the reason for this asso-ciation is incompletely understood. Ongoing genetically medi-ated cerebrovascular insult could potentially explain both theobserved congenital neuroanatomic abnormalities and theaberrant neurodevelopmental trajectories observed later in life(14,16,46). 22q11DS is associated with diffuse white matterabnormalities reminiscent of small vessel ischemic changes,findings often seen in healthy people following middle age(57–59). Limited pathological examination of individuals with22q11DS has demonstrated astrocytic gliosis and hemo-siderin-laden macrophages in cerebral white matter, sugges-tive of diffuse cerebrovascular injury consistent withsmall vessel ischemia (52) in two out of three specimensexamined.
Morphometric Relationships to Psychosis SpectrumSymptoms
Our purely vertex-level analysis did not identify any directdifferences between subgroups with and without psychosisspectrum symptoms after controlling for multiple testing. Thismay be due to our relatively small sample and possibly therelatively broad definition of the psychosis spectrum in ourND–PS group. The broad definition permitted power toestablish differences between individuals with psychoticsymptoms and those without psychotic symptoms acrossdeletion groups. As our 22q11DS sample grows, we will beable to examine whether individuals with more severe psy-chotic symptoms have more specific patterns of abnormal-ities. It is important to note that in our efforts to control for typeI error, we are at risk for committing a type II error andtherefore should await the availability of larger samples beforeconcluding that such differences do not exist.
We did observe indirect vertex-level differences betweenour ND–TD and ND–PS groups, as there were significantdifferences in their probability maps when each was comparedwith the 22q11DS group. In particular, the ND–PS group hadmore extensive cortical thickness reductions in the dorso-lateral prefrontal cortex relative to 22q11DS but less extensivethickness differences elsewhere in the brain including thesuperior temporal gyrus and superior frontal lobe. Post hoccluster threshold models did identify significant reductions inright STG in ND–TD relative to ND–PS and superior frontal
urnal

Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
gyrus thickness intermediate between 22q11DS and ND–TDgroups, suggesting a partially shared neural etiology forpsychosis. The ND–PS group also tended toward less exten-sive differences in area compared with 22q11DS, particularlyin the temporal lobes.
The literature on anatomic differences in schizophrenia isvariable, but volume and cortical thickness reductions indorsolateral prefrontal cortex, limbic and midline structures,and mesial temporal structures are most commonly reported(42,60–65). Unlike the prior literature on schizophrenia, thecurrent study focuses on subthreshold psychotic symptoms,which may explain the more subtle findings we observedrelative to the schizophrenia literature. There is mountingevidence that neurodegeneration during late childhood andadolescence is evident at the onset of schizophrenia insusceptible individuals; patients with schizophrenia experi-ence loss of cortical thickness and volume over time whenexamined longitudinally (66). It is possible that our ND–PSsubjects represent individuals experiencing early neurodege-nerative changes that are difficult to detect when comparedwith typically developing control subjects directly. Subtledifferences in ND–PS groups (for example in dorsolateralprefrontal cortex and superior temporal gyrus) may becomemore apparent when the 22q11DS contrast is added. Althoughour findings are preliminary, the approach of group triangu-lation may ultimately help to disentangle what portions of the22q11DS endophenotype are shared with idiopathic schizo-phrenia. Longitudinal studies using this multiple groupapproach may prove particularly fruitful for identifying putativebiomarkers present before the manifestation of floridpsychosis.
Although the current study supports several prior findingson 22q11DS in a relatively large sample, there are severallimitations of the study that must be noted. First, our subjectascertainment procedures selected for higher functioningpatients. Thus, the study may underestimate morphologicaldifferences between the 22q11DS and the nondeleted groups.Similarly, our study excluded patients with neurological diag-noses, including seizure disorders. Considering that seizuresare associated with neurodevelopmental abnormalities, thisselection criteria again may underestimate true group differ-ences as compared with an unselected sample (55). Second,although ND–TD and 22q11DS were matched for age, gender,and race, the 22q11DS groups were still significantly older.Age, along with race and gender, was partially controlledstatistically in our analyses. Third, our PNC screening proce-dure for psychotic symptomology is less comprehensive ascompared with the 22q11DS group. Finally, there were differ-ences in the prevalence of mood disorders between 22q11DSsubjects with and without psychosis spectrum symptoms,which could potentially affect the contrast between thesesubgroups.
Conclusions
Comprehensive analysis of multiple complementary measuresof cerebral architecture in 22q11DS demonstrate overlappingabnormalities in cortical thickness, surface area, and localgyrification, most notably in the frontal, superior parietal,and paramidline cerebral cortex. Findings suggest a
Biological
neurodevelopmental origin of many of the neuroanatomicmanifestations of 22q11DS. Several affected regions areassociated with idiopathic schizophrenia in the literature, moststrikingly in the superior temporal gyrus and prefrontal cortex,with our study providing preliminary evidence that subjectswith idiopathic psychotic symptoms may have somewhatdifferent morphological patterns than ND–TD control subjectswhen compared with 22q11DS. By identifying the neuro-anatomic fingerprint of a deletion, we can elucidate thecontribution of specific genetic effects to the phenotypicmanifestations of psychosis. This paradigm can extend toother populations with genetic alterations associated withincreased risk for psychosis, thereby establishing both sharedand unique biomarkers for at-risk populations.
ACKNOWLEDGMENTS AND DISCLOSURESThis study was supported by National Institutes of Health (NIH) GrantsMH087626 and MH087636, and T32 Grants MH019112 (JY), EB004311(JES), and a Radiological Society of North America Fellow Grant (JES).The Philadelphia Neurodevelopmental Cohort is supported by NIH grantsMH089983 and MH089924. Additional support was provided by K23MH098130 (TDS), K08MH079364 (MEC), and the Marc Rapport FamilyInvestigator Grant through the Brain and Behavior Foundation (TDS).
REG disclosed consulting to Otsuka America Pharmaceutical. RCGdisclosed expert testimony. All other authors declare no biomedicalfinancial interests or potential conflicts of interest.
ARTICLE INFORMATIONFrom the Brain Behavior Laboratory (JES, SV, JY, MEC, KR, DRR, DW, TDS,KP, RCG, REG), Department of Psychiatry, Neuropsychiatry Section, Uni-versity of Pennsylvania; Department of Radiology (JES, RCG, REG), Hospitalof the University of Pennsylvania; Department of Child and AdolescentPsychiatry (JY) and Division of Human Genetics (MCS, DMM-M, EHZ, BSE),Children’s Hospital of Philadelphia; and Department of Pediatrics (DMM-M,EHZ, BSE), Perelman School of Medicine, University of Pennsylvania,Philadelphia, Pennsylvania.
Authors JES and SV contributed equally to this work.Address correspondence to Raquel E. Gur, M.D., Ph.D., Hospital of the
University of Pennsylvania, Brain Behavior Laboratory, Philadelphia, PA19104; E-mail: [email protected]; [email protected].
Received Mar 25, 2014; revised Oct 23, 2014; accepted Oct 24, 2014.
Supplementary material cited in this article is available online at http://dx.doi.org/10.1016/j.biopsych.2014.10.025.
REFERENCES1. Shprintzen RJ (2008): Velo-cardio-facial syndrome: 30 years of study.
Dev Disabil Res Rev 14:3–10.2. Shaikh TH, Kurahashi H, Saitta SC, O’Hare AM, Hu P, Roe BA, et al.
(2000): Chromosome 22-specific low copy repeats and the 22q11.2deletion syndrome: Genomic organization and deletion endpointanalysis. Hum Mol Genet 9:489–501.
3. Ryan AK, Goodship JA, Wilson DI, Philip N, Levy A, Seidel H, et al.(1997): Spectrum of clinical features associated with interstitialchromosome 22q11 deletions: A European collaborative study.J Med Genet 34:798–804.
4. Bassett AS, Chow EWC, Husted J, Weksberg R, Caluseriu O, WebbGD, Gatzoulis MA (2005): Clinical features of 78 adults with 22q11Deletion Syndrome. Am J Med Genet A 138:307–313.
5. MacKenzie-Stepner K, Witzel M, Stringer D, Lindsay W, Munro I,Hughes H (1987): Abnormal carotid arteries in the velocardiofacialsyndrome: A report of three cases. Plast Reconstr Surg 80:347–351.
6. Mitnick R, Bello J, Golding-Kushner K, Argamaso R, Shprintzen R(1996): The use of magnetic resonance angiography prior to
Psychiatry July 15, 2015; 78:135–143 www.sobp.org/journal 141

Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
pharyngeal flap surgery in patients with velocardiofacial syndrome.Plast Reconstr Surg 97:908–919.
7. Jawad F, McDonald-Mcginn DM, Zackai E, Sullivan KE (2001):Immunologic features of chromosome 22q11.2 deletion syndrome(DiGeorge syndrome/velocardiofacial syndrome). J Pediatr 139:715–723.
8. Murphy KC, Jones LA, Owen MJ (1999): High rates of schizophrenia inadults with velo-cardio-facial syndrome. Arch Gen Psychiatry 56:940–945.
9. Bassett A, Chow E (1999): 22Q11 deletion syndrome: A geneticsubtype of schizophrenia. Biol Psychiatry 46:882–891.
10. Sullivan PF, Kendler KS, Neale MC (2014): Schizophrenia as acomplex trait. Arch Gen Psychiatry 60:1187–1192.
11. Giusti-rodríguez P, Sullivan PF (2013): The genomics of schizophrenia:Update and implications. J Clin Invest 123:4557–4563.
12. Eliez S, Schmitt JE, White CD, Reiss AL (2000): Children andadolescents with velocardiofacial syndrome: A volumetric MRI study.Am J Psychiatry 157:409–415.
13. Tan GM, Arnone D, McIntosh AM, Ebmeier KP (2009): Meta-analysisof magnetic resonance imaging studies in chromosome 22q11.2deletion syndrome (velocardiofacial syndrome). Schizophr Res 115:173–181.
14. Schaer M, Debbané M, Bach Cuadra M, Ottet M-C, Glaser B, ThiranJ-P, Eliez S (2009): Deviant trajectories of cortical maturation in22q11.2 deletion syndrome (22q11DS): A cross-sectional and longi-tudinal study. Schizophr Res 115:182–190.
15. Bearden CE, van Erp TGM, Dutton RA, Tran H, Zimmermann L, Sun D,et al. (2007): Mapping cortical thickness in children with 22q11.2deletions. Cereb Cortex 17:1889–1898.
16. Jalbrzikowski M, Jonas R, Senturk D, Patel A, Chow C, Green MF,Bearden CE (2013): Structural abnormalities in cortical volume, thick-ness, and surface area in 22q11.2 microdeletion syndrome: Relation-ship with psychotic symptoms. Neuroimage Clin 3:405–415.
17. Bearden CE, van Erp TGM, Dutton RA, Lee AD, Simon TJ, Cannon TD,et al. (2009): Alterations in midline cortical thickness and gyrificationpatterns mapped in children with 22q11.2 deletions. Cereb Cortex 19:115–126.
18. Schaer M, Schmitt JE, Glaser B, Lazeyras F, Delavelle J, Eliez S(2006): Abnormal patterns of cortical gyrification in velo-cardio-facialsyndrome (deletion 22q11.2): An MRI study. Psychiatry Res 146:1–11.
19. Schaer M, Cuadra MB, Tamarit L, Lazeyras F, Eliez S, Thiran J (2008):A surface-based approach to quantify local cortical gyrification. IEEETrans Med Imaging 27:161–170.
20. Wilkinson G, Robertson G (2006): Wide Range Achievement Test.Fourth Edition. Lutz, FL: Psychological Assessment Resources.
21. Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, et al.(1997): Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliabilityand validity data. J Am Acad Child Adolesc Psychiatry 36:980–988.
22. Miller TJ, McGlashan TH, Rosen JL, Cadenhead K, Cannon T, VenturaJ, et al. (2003): Prodromal assessment with the structured interview forprodromal syndromes and the scale of prodromal symptoms: Pre-dictive validity, interrater reliability, and training to reliability. SchizophrBull 29:703–715.
23. First M, Gibbon M (2004): The Structured Clinical Interview for DSM-IVAxis I Disorders (SCID-I) and the Structured Clinical Interview forDSM-IV Axis II Disorders (SCID-II). In: Hilsenroth M, Segal D, editors.Comprehensive Handbook of Psychological Assessment, Volume 2:Personality Assessment. Hoboken, NJ, 134–143.
24. Jalali GR, Vorstman JAS, Errami A, Vijzelaar R, Biegel J, Shaikh T,Emanuel BS (2008): Detailed analysis of 22q11.2 with a high densityMLPA probe set. Hum Mutat 29:433–440.
25. Satterthwaite TD, Elliott MA, Ruparel K, Loughead J, Prabhakaran K,Calkins ME, et al. (2013): Neuroimaging of the Philadelphia neuro-developmental cohort. Neuroimage 86:544–553.
26. Calkins M, Moore T, Merikangas K, Berstein M, Satterthwaite T, BilkerW, et al. (2014): The psychosis spectrum in a young U.S. communitysample: Findings from the Philadelphia neurodevelopmental cohort.World Psychiatry 13:296–305.
142 Biological Psychiatry July 15, 2015; 78:135–143 www.sobp.org/jo
27. Gur RC, Calkins ME, Satterthwaite TD, Ruparel K, Bilker WB, MooreTM, et al. (2014): Neurocognitive growth charting in psychosisspectrum youths. JAMA Psychiatry 71:366–374.
28. Kosanke J, Bergstralh E (2004): Match One or More Controls to CasesUsing the GREEDY Algorithm. Rochester, MN: Mayo Clinic College ofMedicine.
29. Dale AM, Fischl B, Sereno MI (1999): Cortical surface-based analysis.Neuroimage 194:179–194.
30. Fischl B (2012): FreeSurfer. Neuroimage 62:774–781.31. Fischl B, Dale A (2000): Measuring the thickness of the human
cerebral cortex from magnetic resonance images. Proc Natl AcadSci U S A 97:11050–11055.
32. Fischl B, Sereno MI, Dale AM (1999): Cortical surface-based analysisII: Inflation, flattening, and a surface-based coordinate system. Neuro-image 207:195–207.
33. Ségonne F, Dale AM, Busa E, Glessner M, Salat D, Hahn HK, Fischl B(2004): A hybrid approach to the skull stripping problem in MRI.Neuroimage 22:1060–1075.
34. Joyner AH, J CR, Bloss CS, Bakken TE, Rimol LM, Melle I, et al.(2009): A common MECP2 haplotype associates with reduced corticalsurface area in humans in two independent populations. Proc NatlAcad Sci U S A 106:15483–15488.
35. Genovese CR, Lazar NA, Nichols T (2002): Thresholding of statisticalmaps in functional neuroimaging using the false discovery rate 1.Neuroimage 15:870–878.
36. Ripke S, O’Dushlaine C, Chambert K, Moran JL, Kähler AK, Akterin S,et al. (2013): Genome-wide association analysis identifies 13 new riskloci for schizophrenia. Nat Genet 45:1150–1159.
37. Simon T, Ding L, Bish J, McDonald-McGinn, Zackai E, Gee J (2005):Volumetric, connective, and morphologic changes in the brains ofchildren with chromosome 22q11. 2 deletion syndrome: An integrativestudy. Neuroimage 25:169–180.
38. Campbell LE, Daly E, Toal F, Stevens A, Azuma R, Catani M, et al.(2006): Brain and behaviour in children with 22q11.2 deletion syn-drome: A volumetric and voxel-based morphometry MRI study. Brain129:1218–1228.
39. Eliez S, Blasey CM, Schmitt EJ, White CD, Hu D, Reiss AL (2001):Velocardiofacial syndrome: Are structural changes in the temporal andmesial temporal regions related to schizophrenia? Am J Psychiatry158:447–453.
40. Pearlson GD, Marsh L (1999): Structural brain imaging in schizophre-nia: A selective review. Biol Psychiatry 46:627–649.
41. Kubicki M (2002): Voxel-based morphometric analysis of gray matterin first episode schizophrenia. Neuroimage 17:1711–1719.
42. Narr KL, Bilder RM, Toga AW, Woods RP, Rex DE, Szeszko PR, et al.(2005): Mapping cortical thickness and gray matter concentration infirst episode schizophrenia. Cereb Cortex 15:708–719.
43. Chow E, Ho A, Wei C, Voormolen E, Crawley A, Bassett A (2011):Association of schizophrenia in 22q11.2 deletion syndrome and graymatter volumetric deficits in the super temporal gyrus. Am J Psychia-try 168:522–529.
44. Kunwar A, Ramanathan S, Nelson J, Antshel KM, Fremont W, HigginsAM, et al. (2012): Cortical gyrification in velo-cardio-facial (22q11.2deletion) syndrome: A longitudinal study. Schizophr Res 137:20–25.
45. Schaer M, Glaser B, Cuadra MB, Debbane M, Thiran J-P, Eliez S(2009): Congenital heart disease affects local gyrification in 22q11.2deletion syndrome. Dev Med Child Neurol 51:746–753.
46. Srivastava S, Buonocore MH, Simon TJ (2012): Atypical developmen-tal trajectory of functionally significant cortical areas in children withchromosome 22q11.2 deletion syndrome. Hum Brain Mapp 33:213–223.
47. Thompson PM, Lee AD, Dutton RA, Geaga JA, Hayashi KM, EckertMA, et al. (2005): Abnormal cortical complexity and thickness profilesmapped in Williams syndrome. J Neurosci 25:4146–4158.
48. Hardan AY, Muddasani S, Vemulapalli M, Keshavan MS, Minshew NJ(2006): An MRI study of increased cortical thickness in autism. Am JPsychiatry 163:1290–1292.
urnal

Cortical Morphometry in 22q11.2DSBiologicalPsychiatry
49. Bauman ML, Kemper TL (2005): Neuroanatomic observations of thebrain in autism: A review and future directions. Int J Dev Neurosci 23:183–187.
50. Barkovich AJ, Chuang SH, Norman D (1988): MR of neuronalmigration anomalies. AJR Am J Roentgenol 150:179–187.
51. Barkovich AJ, Rowley H, Bollen A (1995): Correlation of prenatalevents with the development of polymicrogyria. AJNR Am J Neuro-radiol 16:822–827.
52. Kiehl TR, Chow EWC, Mikulis DJ, George SR, Bassett AS (2009):Neuropathologic features in adults with 22q11.2 deletion syndrome.Cereb Cortex 19:153–164.
53. Robin NH, Taylor CJ, Mcdonald-McGinn DM, Zackai EH, Bingham P,Collins KJ, et al. (2006): Polymicrogyria and deletion 22q11.2 syn-drome: Window to the etiology of a common cortical malformation.Am J Med Genet A 140:2416–2425.
54. Gerkes EH, Hordijk R, Dijkhuizen T, Sival DA, Meiners LC, Sikkema-Raddatz B, van Ravenswaaij-Arts CM (2010): Bilateral polymicrogyriaas the indicative feature in a child with a 22q11.2 deletion. Euro J MedGenet 53:344–346.
55. Barkovich AJ, Guerrini R, Kuzniecky RI, Jackson GD, Dobyns WB(2012): A developmental and genetic classification for malformationsof cortical development: Update 2012. Brain 135:1348–1369.
56. Schaer M, Glaser B, Ottet M-C, Schneider M, Bach Cuadra M,Debbané M, et al. (2010): Regional cortical volumes and congenitalheart disease: A MRI study in 22q11.2 deletion syndrome. J NeurodevDisord 2:224–234.
57. Altman D, Altman N (1995): Further delineation of brain anomalies invelo‐cardio‐facial syndrome. Am J Med Genet 175:174–175.
58. Kates WR, Burnette CP, Jabs EW, Rutberg J, Murphy AM, Grados M,et al. (2001): Regional cortical white matter reductions in
Biological
velocardiofacial syndrome: A volumetric MRI analysis. Biol Psychiatry49:677–684.
59. Amelsvoort TV (2001): Structural brain abnormalities associated withdeletion at chromosome 22q11: Quantitative neuroimaging study ofadults with velo-cardio-facial syndrome. Br J Psychiatry 178:412–419.
60. Steen RG, Mull C, McClure R, Hamer RM, Lieberman JA (2006): Brainvolume in first-episode schizophrenia: Systematic review and meta-analysis of magnetic resonance imaging studies. Br J Psychiatry 188:510–518.
61. Vita A, De Peri L, Silenzi C, Dieci M (2006): Brain morphology in first-episode schizophrenia: A meta-analysis of quantitative magneticresonance imaging studies. Schizophr Res 82:75–88.
62. van Erp TG, Guella I, Vawter MP, Turner J, Brown GG, McCarthy G,et al. (2014): Schizophrenia miR-137 locus risk genotype is associatedwith dorsolateral prefrontal cortex hyperactivation. Biol Psychiatry 75:398–405.
63. Callicott JH, Bertolino A, Mattay VS, Langheim FJ, Duyn J, Coppola R,et al. (2000): Physiological dysfunction of the dorsolateral prefrontalcortex in schizophrenia revisited. Cereb Cortex 10:1078–1092.
64. Hashimoto T, Arion D, Unger T, Maldonado-Avilés JG, Morris HM,Volk DW, et al. (2008): Alterations in GABA-related transcriptome inthe dorsolateral prefrontal cortex of subjects with schizophrenia. MolPsychiatry 13:147–161.
65. Gur RE, Cowell PE, Latshaw A, Turetsky BI, Grossman RI, Arnold SE,et al. (2000): Reduced dorsal and orbital prefrontal gray mattervolumes in schizophrenia. Arch Gen Psychiatry 57:761–768.
66. Thompson PM, Vidal C, Giedd JN, Gochman P, Blumenthal J,Nicolson R, et al. (2001): Mapping adolescent brain change revealsdynamic wave of accelerated gray matter loss in very early-onsetschizophrenia. Proc Natl Acad Sci U S A 98:11650–11655.
Psychiatry July 15, 2015; 78:135–143 www.sobp.org/journal 143