Embed Size (px)
Citation preview

Aberrant Coronary Artery Origin From the AortaReport of 18 Patients, Review of Literature andDelineation of Natural History and Management
RICHARD R. LIBERTHSON, M.D., ROBERT E. DINSMORE, M.D.,AND JOHN T. FALLON, M.D., PH.D.
SUMMARY To clarify the natural history and management of patients with aberrant origin of a coronaryartery from the aorta, we reviewed 18 patients whose right (RCA) or left (LCA) coronary artery aroseaberrantly and passed between the aorta and right ventricular infundibulum.
Nine patients had aberrant LCA. Three young males died suddenly after exertion, each with proximal focalLCA stenosis. None of the six adults with angina (ages 36-70 years) studied angiographically had proximalLCA stenosis. Unlike the young, "sudden death-prone" patients in whom coronary bypass of proximal stenosismay have prophylactic value, our older patients with aberrant LCA did not have proximal stenosis or suddendeath, and therefore LCA bypass for sudden death prophylaxis is not warranted.
Nine patients (ages 18-60 years) had aberrant origin and course of the RCA. Seven patients studied angio-graphically because of angina had no focal proximal RCA stenosis, but two patients had hypoplastic RCA os-tia. Although a potential concern in these latter patients, sudden death has not been reported with aberrantRCA, therefore in the absence of syncope, RCA bypass for sudden death prophylaxis is not indicated.
BECAUSE MANY PATIENTS undergo coronaryartery angiography and surgery, it is important to beaware of even the unusual morphologic variants ofcoronary artery anatomy, particularly those withclinical significance. Recent reports have identifiedtwo groups of patients with aberrant coronary arteryorigin from the aorta in which myocardial perfusionmay be subject to compromise because the anomalouscoronary artery passes between the aorta and the rightventricular infundibulum (RVinf).' 3 These studieshave linked sudden exertional death in young maleswith one of these variants.' '4 However, as experiencewith these anomalies increased, it became evident thatthey are not always associated with sudden death, andliving patients with these variants have beenreported.2 9 It is important for both prognosis andmanagement to differentiate those who are at risk forsudden death from those who are not.
In this report we review our experience with pa-tients in whom an aberrant coronary artery passesbetween the aorta and RVinf, describe their presenta-tion, pathophysiologic findings, management andfollow-up, review the literature and propose guidelinesfor patient management.
Methods
Between 1973 and 1977, 18 patients with aberrantcoronary artery origin from the aorta, in whom theleft coronary artery (LCA) or the right coronary
From the Departments of Medicine and Pediatrics (CardiacUnit), Radiology and Pathology, Massachusetts General Hospital,Boston, Massachusetts.
Supported in part by SCOR grant HL17665 from the NHLBI.Presented at the American College of Cardiology, 27th Annual
Scientific Sessions, Anaheim, California, March 1978.Address for reprints: Richard Liberthson, M.D., Cardiac Unit,
Massachusetts General Hospital, Boston, Massachusetts 02144.Received August 2, 1978; revision accepted November 8, 1978.Circulation 59, No. 4, 1979.
artery (RCA) passed between the aorta and theRVinf, were evaluated at the Massachusetts GeneralHospital. Incidence data concerning this entity is notdiscernible from our study since many of thesepatients were referred to this hospital after initialdiagnosis.
In five patients the aberrant coronary arteryanatomy was found at autopsy and in 13 the diagnosiswas established by selective coronary arteryangiography. The angiographic diagnosis of aberrantLCA with delineation of the exact course of theaberrant artery and its relationship to the aorta andRVinf was often difficult. This required selectiveangiography in multiple projections, in particular theright anterior oblique and lateral views, as outlined inearlier reports of this entity.", 2 A catheter positionedin the pulmonary artery was helpful in delineating theposition of the pulmonary outflow tract while per-forming selective LCA angiography.The pertinent clinical history and all available
pathophysiologic data, including electrocardiograms,treadmill stress tests, myocardial imaging and autopsyfindings, were reviewed for each patient.
Results
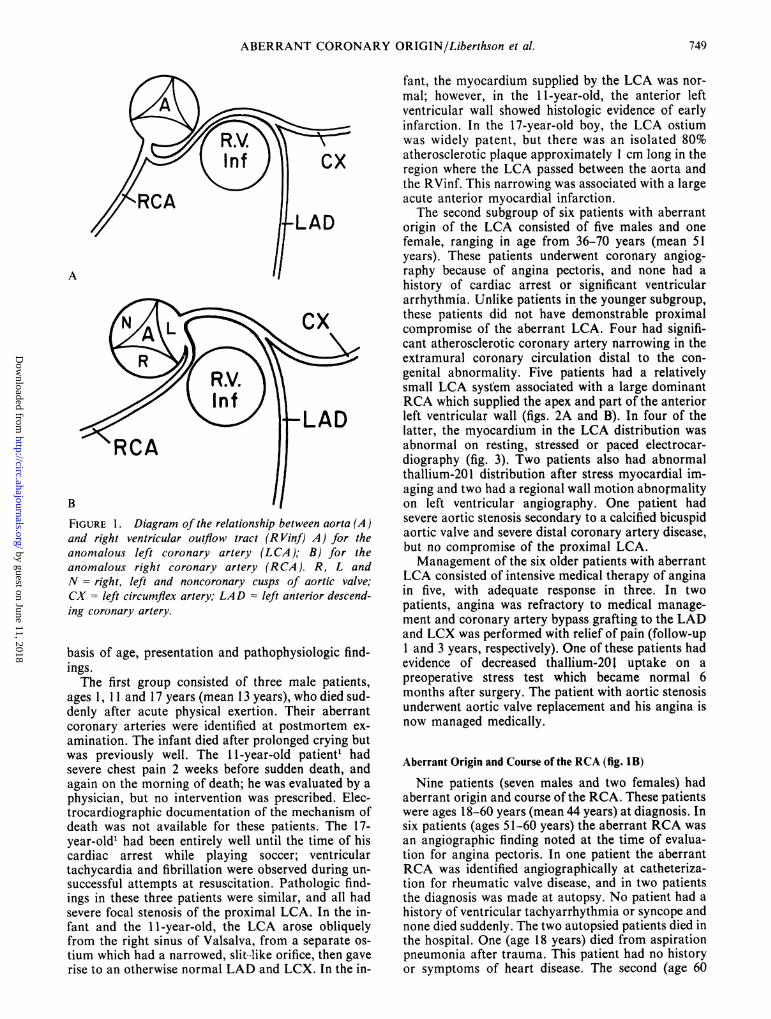
In nine patients (fig. IA) the LCA arose from theright sinus of Valsalva or the RCA, and passed to theleft and posteriorly between the aorta and the RVinfto reach the area of usual left anterior descending(LAD) and left circumflex (LCX) distribution. In ninepatients (fig. 1 B), the RCA arose from the left sinus ofValsalva or the LCA, and passed to the right andanteriorly, between the aorta and the RVinf, to reachthe usual RCA distribution. Fifteen patients weremale and three were female (overall age range 1-70years).
Aberrant Origin and Course of the LCA (fig. 1A)
We divided these patients into two subgroups on the748
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
ABERRANT CORONARY ORIGIN/Liberthson et al.
RCA
cx
LAD
A
RCA
B
FIGURE 1. Diagram of the relationship between aorta (A)and right ventricular outflow tract (R Vinf) A) for theanomalous left coronary artery (LCA); B) for theanomalous right coronary artery (RCA). R, L andN= right, left and noncoronary cusps of aortic valve;CX = left circumflex artery; LAD = left anterior descend-ing coronary artery.
basis of age, presentation and pathophysiologic find-ings.The first group consisted of three male patients,
ages 1, 11 and 17 years (mean 13 years), who died sud-denly after acute physical exertion. Their aberrantcoronary arteries were identified at postmortem ex-amination. The infant died after prolonged crying butwas previously well. The 11-year-old patient' hadsevere chest pain 2 weeks before sudden death, andagain on the morning of death; he was evaluated by a
physician, but no intervention was prescribed. Elec-trocardiographic documentation of the mechanism ofdeath was not available for these patients. The 17-year-old' had been entirely well until the time of hiscardiac arrest while playing soccer; ventriculartachycardia and fibrillation were observed during un-successful attempts at resuscitation. Pathologic find-ings in these three patients were similar, and all hadsevere focal stenosis of the proximal LCA. In the in-fant and the 11-year-old, the LCA arose obliquelyfrom the right sinus of Valsalva, from a separate os-
tium which had a narrowed, slit like orifice, then gaverise to an otherwise normal LAD and LCX. In the in-
fant, the myocardium supplied by the LCA was nor-mal; however, in the 1 1-year-old, the anterior leftventricular wall showed histologic evidence of earlyinfarction. In the 17-year-old boy, the LCA ostiumwas widely patent, but there was an isolated 80%atherosclerotic plaque approximately I cm long in theregion where the LCA passed between the aorta andthe RVinf. This narrowing was associated with a largeacute anterior myocardial infarction.The second subgroup of six patients with aberrant
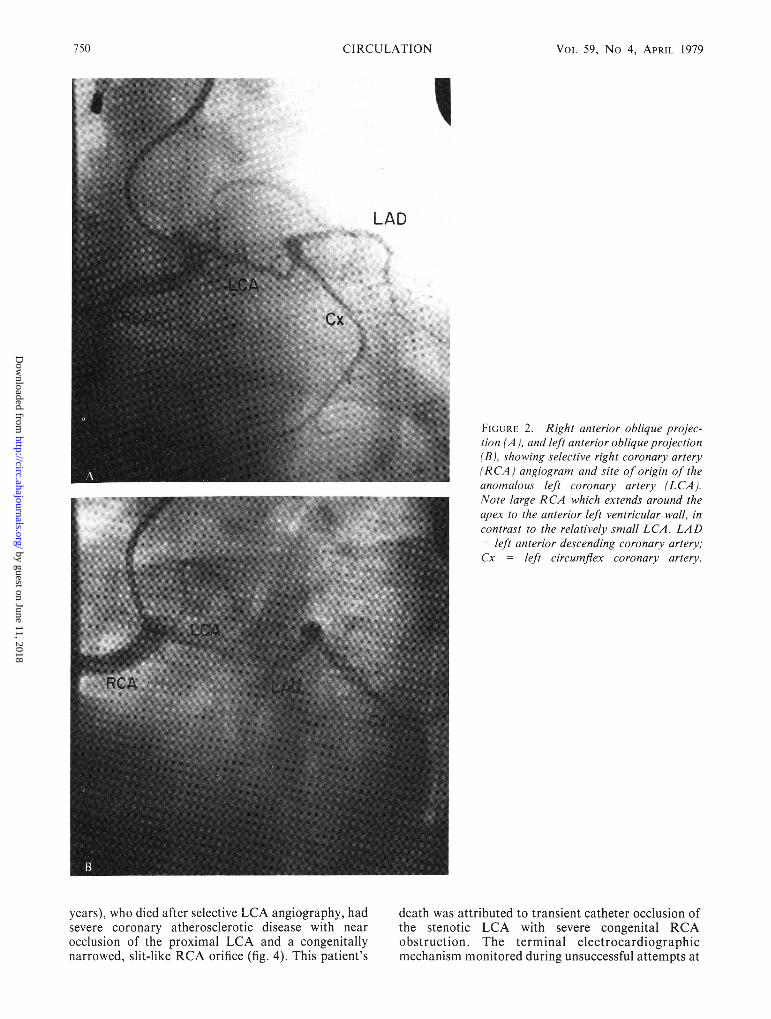
origin of the LCA consisted of five males and onefemale, ranging in age from 36-70 years (mean 51years). These patients underwent coronary angiog-raphy because of angina pectoris, and none had ahistory of cardiac arrest or significant ventriculararrhythmia. Unlike patients in the younger subgroup,these patients did not have demonstrable proximalcompromise of the aberrant LCA. Four had signifi-cant atherosclerotic coronary artery narrowing in theextramural coronary circulation distal to the con-genital abnormality. Five patients had a relativelysmall LCA system associated with a large dominantRCA which supplied the apex and part of the anteriorleft ventricular wall (figs. 2A and B). In four of thelatter, the myocardium in the LCA distribution wasabnormal on resting, stressed or paced electrocar-diography (fig. 3). Two patients also had abnormalthallium-201 distribution after stress myocardial im-aging and two had a regional wall motion abnormalityon left ventricular angiography. One patient hadsevere aortic stenosis secondary to a calcified bicuspidaortic valve and severe distal coronary artery disease,but no compromise of the proximal LCA.Management of the six older patients with aberrant
LCA consisted of intensive medical therapy of anginain five, with adequate response in three. In twopatients, angina was refractory to medical manage-ment and coronary artery bypass grafting to the LADand LCX was performed with relief of pain (follow-up1 and 3 years, respectively). One of these patients hadevidence of decreased thallium-201 uptake on apreoperative stress test which became normal 6months after surgery. The patient with aortic stenosisunderwent aortic valve replacement and his angina isnow managed medically.
Aberrant Origin and Course of the RCA (fig. 1B)
Nine patients (seven males and two females) hadaberrant origin and course of the RCA. These patientswere ages 18-60 years (mean 44 years) at diagnosis. Insix patients (ages 51-60 years) the aberrant RCA wasan angiographic finding noted at the time of evalua-tion for angina pectoris. In one patient the aberrantRCA was identified angiographically at catheteriza-tion for rheumatic valve disease, and in two patientsthe diagnosis was made at autopsy. No patient had ahistory of ventricular tachyarrhythmia or syncope andnone died suddenly. The two autopsied patients died inthe hospital. One (age 18 years) died from aspirationpneumonia after trauma. This patient had no historyor symptoms of heart disease. The second (age 60
749
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from
VOL 59, No 4, APRIL 1979
FIGURE 2. Right anterior oblique projec-tion (A ), and left anterior oblique projection(B), showing selective right coronary artery(RCA) angiogram and site of origin of theanomalous left coronary artery (LCA).Note large RCA which extends around theapex to the anterior left ventricular wall, incontrast to the relatively small LCA. LAD
left anterior descending coronary artery;Cx = left circumflex coronary artery.
years), who died after selective LCA angiography, hadsevere coronary atherosclerotic disease with nearocclusion of the proximal LCA and a congenitallynarrowed, slit-like RCA orifice (fig. 4). This patient's
death was attributed to transient catheter occlusion ofthe stenotic LCA with severe congenital RCAobstruction. The terminal electrocardiographicmechanism monitored during unsuccessful attempts at
750 CIRCULATION
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

ABERRANT CORONARY ORIGIN/Liberthson et al.-. S -1--- r---1.... fi . . ... . .... .... . .Z.... . " . _ . .. . ... . . . .; i :1 ; . . :1. .............. j . .. - . 5 a_m .. 1 _, .-. H. . . . . . X . . . z - ._ S _ 4 _. _ , <
} \ l X \ 1
' iK / . . J f o .S.... . . ... . ... .... ... .... ... ... . . .... ............ ..... ... .... ... .,, , .. , . . .. _ , ........... ,i I . .
.. ! . : ..-.:.. = . 1 .- _.
...1. .. ..............
.- _ -, I. -1_ -:
4
I ..*"-.A _-_FIGURE 3. Lead V4 electrocardiogram recorded before (left), and during (right), atrialpacing. Note ST-T-wave changes suggesting myocardial ischemia in the region supplied by the anomalous left coronary artery.
resuscitation was electromechanical dissociation.Six patients with aberrant RCA (including five
patients with angina) had significant atheroscleroticnarrowing in portions of their coronary circulationdistal to the congenitally aberrant origin. No patientwith angina had demonstrable proximal RCAobstruction (figs. 5A and B). One patient had nodemonstrable cause for his atypical angina, andresponded to minimal medical regimen. Angina in theother five patients responded well to medical treat-
FIGURE 4. Pathologic specimen ofan anomalous right cor-
onary artery (RCA) which has been strippedfrom the heart.Note hypoplastic origin of the RCA which traverses the aor-
tic wall (bracket). RC - right coronary ostium; RM = rightmarginal; PDS = posterior descending coronary.
ment. One patient had severe rheumatic aortic, mitraland tricuspid valve disease and underwent successfultriple valve replacement.
Discussion
Because the occurrence of exertional sudden deathin patients with aberrant LCA is well-established,' 4
questions arise concerning the natural history andmanagement of these patients. Awareness of this en-tity is paramount in making this diagnosis during life.It must be considered in young patients, particularlymales, presenting with exertional chest pain or syn-cope, or in those successfully resuscitated. However,not all patients with these anomalies die suddenly, andthis diagnosis is being made with increasing frequencyin patients who have already demonstrated significantlongevity free of syncope. Thus, awareness of theclinical spectrum and natural history of theseanomalies is essential for appropriate patient manage-ment.
Aberrant Origin and Course of the LCA
As demonstrated by our aberrant LCA patients andreported by others,2' 9 there are two subgroups, bothwith the same morphological pattern shown in figureIA which, however, differ markedly in their clinicalpresentation, age at recognition, and pathophysiologicfindings.Our three young patients with aberrant LCA, and
17 similar patients previously reported,2' '- make up a
homogenous subgroup. The mean age of these 20patients was 16 years (range 1-36 years). All weremale, and all died suddenly after physical exertion.Two of the 20 patients reported severe chest painwithin days or weeks before death1 7and three hadsyncope.2' 7 The terminal electrocardiographicmechanism in three patients who were monitored dur-ing their acute event was ventricular fibrillation." 2
Four patients had histologic evidence of acutemyocardial infarction, and a fifth had changessuggestive of early infarction in the distribution of theanomalous LCA.' 2 7 Focal proximal LCA obstruc-tion was present in our three young patients and men-tioned in the remaining, 1,2, 4-7 although the proposedetiology for this proximal obstruction varied. In somepatients the obstruction had an anatomic basis, in
Lead ¼4
11T- I.... .1- ..I. .- .- .1 I..::l
. I. ..I -..T--.II-- ' '!t'- i
. ' ' ' t t ' ' ' ' ' ' t ' ' ' t -'i''''* ' 4.-
I-,-I....F- ,IIIIIIII -1
751
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

CIRCULATION VOL 59, No 4, APRII 1979752
s-! l - l by guest on June 11, 2018
http://circ.ahajournals.org/D
ownloaded from

ABERRANT CORONARY ORIGIN/Liberthson et al.
others it was attributed to a physiologic mechanism,and still others may have had elements of both. Two ofour patients had a hypoplastic LCA orifice in the rightsinus of Valsalva which was functionally narrowedfurther by the abrupt angle which the LCA made as itpassed to the left, between the aorta and RVinf. It hasbeen postulated that these patients die during exertionbecause of proximal LCA obstruction secondary tokinking at the LCA orifice caused by the dilatation ofthe aorta and RVinf associated with an increased car-diac output.2' 5' 7 Our 17-year-old patient differed fromthe others described. He had a widely patent LCAorifice but had severe atherosclerotic stenosis localizedto the segment between the aorta and RVinf. In thispatient, focal narrowing may have been caused bychronic LCA compression between the aorta and theRVinf. This has been proposed by some as an ad-ditional explanation for LCA obstruction in thesepatients.6 7 However, significant LCA compressionbetween the aorta and RVinf in the presence of nor-mal right ventricular pressure seems unlikely.'5
In most young patients with aberrant LCA, thediagnosis was made at autopsy. In one, it was made byangiography after successful resuscitation from twoepisodes of ventricular flbrillation.2 Thus, diagnosis ofthis anomaly in life was possible in approximately 20%of the young patients in whom exertional chest pain,syncope, or ventricular tachyarrhythmia precededsudden death. Thus, appropriate use of noninvasivestudies, including stress electrocardiography andmyocardial imaging, are indicated if the diagnosis issuspected in a young patient after exertional chestpain, syncope or significant ventricular arrythmia. Ifthese studies are abnormal, coronary angiographyshould then be performed. If an aberrant LCA isdemonstrated in these young patients, surgical bypassgrafts to the LAD and LCX for sudden deathprophylaxis is appropriate. One such patient has beenpreviously reported.2The second subgroup of older patients with aberrant
LCA is, to our knowledge, the only such group of pa-tients in whom an aberrant LCA was identified in life.All were identified by coronary angiography performedfor evaluation of angina pectoris. None had a historyof syncope, ventricular tachyarrhythmia or cardiacarrest. Twenty-nine similar patients (mean age 56years) with this anatomy who did not have syncope or
sudden death but were identified at autopsy examina-tion have been reported.2' 10-14 Not surprisingly, inview of the age of these patients, those with angina hadsignificant coronary artery disease not related to theircongenital abnormality.'2' 14 The follow-up of ourolder patients is 1-4 years, therefore, definitive state-ments concerning overall longevity cannot be madeyet.The most obvious differences between patients with
aberrant LCA who die suddenly and those who do not
are the acute clinical presentation, youth and thepresence of proximal anatomical or physiologicalLCA obstruction in the former group in contrast tothe latter. Unlike the young patients, the olderpatients do not seem to be at risk for sudden death anddo not have demonstrable proximal LCA obstruc-tion.2' 12-14 Therefore, we feel that management ofolder patients should be directed at their presentingproblem, e.g., angina pectoris, and not specifically atsudden death prophylaxis. In four of our patients, ini-tial medical treatment of angina was successful.However, angina was refractory to medical treatmentin two others and necessitated aortocoronary arterybypass surgery to which each responded well.The etiology for angina in our older patients with
aberrant LCA appeared to be related to their abnor-mal left ventricular myocardium. Although the exactnature of these abnormalities is unclear, ischemia was
probably present in some, as demonstrated in one ofour patients by ischemic ST-T-wave changes whichwere inducible at an increased heart rate (fig. 3), andby a thallium-201 stress imaging abnormality whichwas present preoperatively and disappeared after cor-
onary bypass surgery. A relatively small LCA systemwas noted in four of our patients and has also beendescribed by others.4 6, 10-12 We do not know whetherthe relatively small size of the LCA is related to theaberrant origin of the LCA, as suggested by its fre-quent occurrence in this entity, or is merely secondaryto the presence of a large, dominant RCA supplyingthe left circumflex coronary artery territory.
Aberrant Origin of the RCA
Our nine patients with aberrant RCA, combinedwith 18 previously reported autopsied patients,2 had a
mean age of 54 years, and none had been known tohave syncope, related ventricular tachyarrhythmia orsudden death. Therefore, it would seem that aberrantRCA usually has a benign clinical course.
Considering the ages of these patients (mean 54years) it is not surprising that coronary artery diseasewas common. Because sudden death in patients withanomalous RCA is rare, coronary artery bypass asprophylaxis for sudden death does not seem indicated.Management of these patients should be directed atcontrolling angina, when present, which we ac-complished successfully with standard medicalregimens in all of our patients. However, as shown byour two patients with hypoplasia of the RCA orifice(fig. 4), proximal RCA stenosis may be severe andcould have dire consequences, particularly if associ-ated with a dominant RCA.
Acknowledgments
The authors express their appreciation to the members of theCardiac Unit and Cardiac Surgical Service at the Massachusetts
FIGURE 5. Right anterior oblique (A) and left anterior oblique (B) projections showing selective left cor-onary artery (LCA) angiogram in a patient with anomalous origin ofthe right coronary artery (RCA). Noteabsence of proximal RCA compromise (arrows).
753
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 59, No 4, APRIL 1979
General Hospital, to Dr. Robert Kiger, Columbia Hospital, Colum-bia, South Carolina, and Dr. Joel Cannilla, Morristown MemorialHospital, Morristown, New Jersey for allowing us to includepatients followed by them in this study; to Drs. William Strauss andGerald Pohost for their assistance in the thallium-201 imaging; andto Deborah Scharf for her help in preparing this manuscript.
References
1. Liberthson RR, Dinsmore RC, Bharati S, Rubenstein JJ,Caulfield J, Wheeler EO, Hawthorne JW, Lev M: Aberrantcoronary origin from the aorta: diagnosis and clinicalsignificance. Circulation 50: 774, 1974
2. Cheitlin MD, DeCastro CM, McAllister HA: Sudden death asa complication of anomalous left coronary origin from theanterior sinus of Valsalva. A not so minor congenital anomaly.Circulation 50: 780, 1974
3. Odgen JA: Congenital anomalies of the coronary arteries. Am JCardiol 25: 474, 1970
4. Nicod JL: Anomalie coronaire et mort subsite. Cardiologia 20:172, 1952
5. Jokl E, McClellan JT, Williams WC, Gouze FS, BartholomewRD: Congenital anomaly of the left coronary artery in youngathletes. Cardiologia 49: 253, 1966
6. Benson PA, Lack AR: Anomalous aortic origin of the left cor-
onary artery: Report of two cases. Arch Pathol 86: 214, 19687. Cohen LS, Shaw LD: Fatal myocardial infarction in an 11-
year-old boy associated with a unique coronary artery anomaly.Am J Cardiol 19: 420, 1967
8. McClellan JT, Jokl E: Congenital anomalies of coronaryarteries: a cause of sudden death associated with physical exer-tion. Am J Clin Pathol 50: 229, 1968
9. Liberthson RR, Dinsmore RD, Block PC, Pohost GM, StraussHW: Myocardial compromise and sudden death in aberrantcoronary artery origin from the aorta. Am J Cardiol 41: 358,1978
10. Gallavardin L, Ravault P: Anomalie d'origine de la coronarieauterieure. Lyon Med 136: 270, 1920
11. Born E: Uber Missbuildungen der Kranzarterien und ihreBeziehungen und plotzlichem. Virchows Archiv (Cell Pathol)290: 688, 1933
12. Roberts JT, Loube SD: The congenitally single coronaryartery. Anat Rec 94: 81, 1946
13. Kinter AR: Anomalous origin and course of the left coronaryartery. Arch Pathol 12: 586, 1931
14. Allen GL, Snider TH: Myocardial infarction with a single cor-onary artery. Arch Intern Med 117: 261, 1966
15. Schaffer Al, Bonaccorsi B, Tchertkoff V: Compressibility ofthe coronary artery by pulmonary artery distention. Am J Car-diol 12: 406, 1963
754 CIRCULATION
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from

R R Liberthson, R E Dinsmore and J T Fallonliterature and delineation of natural history and management.
Aberrant coronary artery origin from the aorta. Report of 18 patients, review of
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1979 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.59.4.748
1979;59:748-754Circulation.
http://circ.ahajournals.org/content/59/4/748the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 11, 2018http://circ.ahajournals.org/
Dow
nloaded from





























