Embed Size (px)
Citation preview

Abdominal Trauma
Oleh :
Dr. A. Aziz, Sp.B-KBD
Disajikan pada Pelatihan Penanggulangan Penderita Gawat
Darurat (PPGD) RSD Raden Mattaher Jambi tanggal 28 November
2005 s/d 04 Desember 2005
Objectives
Describe external and internal anatomy
Recognize blunt vs penetrating injury Patterns
Indentify signs different types of injuries
Apply diagnostic and therapeuti
Procedures
Demonstrate and discuss DPL

Abdominal Trauma
Unrecognized injury : Cause of
preventable death
Exam compromised by
• Alcohol, illicit drugs
• Injury to brain, spinal cord
• Injury to ribs, spine, pelvis
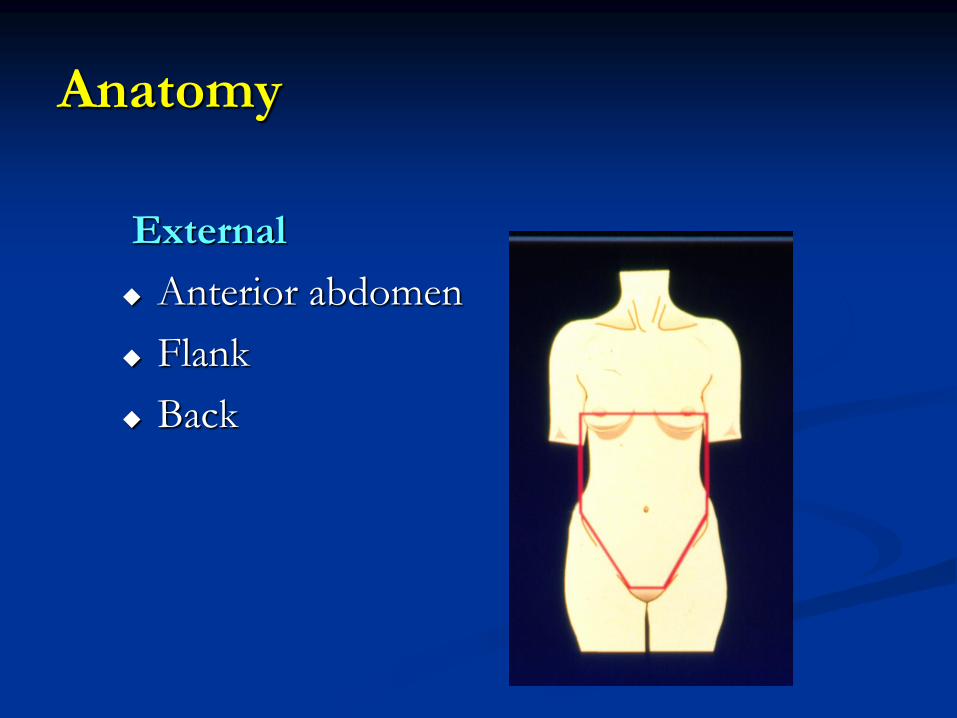
Anatomy
External
Anterior abdomen
Flank
Back

Anatomy

Mechanism of injury
Blunt
Spleen, liver, and Hollow viscus
Compression
Crushing
Shearing
Deceleration (fixed organs)

Mechanism of injury
Penetrating
Liver , small bowel, and colon
Laceration / low energy
Kinetic energy / high energy
Assessment : History
Blunt
Speed
Point of impact
Intrusion
Safety devices
Position
Ejection
Penetrating
Weapon
Distance

Assessment : Physical Exam
Inspection
Percussion
Palpation
Auscultation

Assessment : Physical Exam
Local wound exploration by surgeon
Pain over bony pelvis
Genitourinary, perineal, rectal,vaginal
and gluteal

Adjuncts : Intubation
Gastric Tube
Relieves dilatation
Decompresses stomach before DPL
Basilar skull/facial fractures
My induce vomiting/ aspiration

Adjuncts : Intubation
Urinary Catheter
Monitors urinary output
Decompresses bladder before DPL
Diagnostic
Urethral injury

Adjuncts : x – ray Studies
Routine
Blunt : AP chest, pelvis
Penetrating : AP chest, abdomen with
markers (if hemodynamically normal)
Contrast
Urethrogram
Cystogram
GI
IVP

Special Studies in Blunt Trauma
DPL US* CT
Time Rapid Rapid Delayed
Transport No No Required
Sensitivity High High? High
Specificity Low Intermediate High
Eligibility All
patients
All patients Hemodyna
mically normal
Indications for Celiotomy
Blunt
+ DPL or ultrasound
↓BP suspected
visceral injury
Peritonitis
Penetrating
+ DPL or ultrasound
Peritoneal/
retroperitoneal injury
Peritonitis
Hypotension
Evisceration
Indications for Celiotomy
Plain X – ray
Free air
Retroperitoneal air
Ruptured diaphragm
Indications for Celiotomy
Special Studies
CT scan : Free air, visceral injury ? Fluid?
Cystogram : Bladder rupture, intraperitoneal
injury
Arteriogram: Renal pedicle occlusion
Upper GI : Duodenal rupture

Special Problems : Blunt Trauma
Diaphragm :
Duodenum/
small bowel :
Pancreas :
GU :
Abnormal chest x –ray
Retroperitoneal air, contrast
seat belt sign, chance
fracture ,free air
Amylase ?, CT ?
Extravasation of contras
nonfunctioning renal

Pelvic Fractures
Significant force
applied
Associated injuries
Pelvic bleeding
• Ends of bones
• Pelvic muscles
• Veins/arteries

Pelvic Fractures
Mechanism
Ap compression
Lateral
compression
Vertical shear
Classification
Open
Closed
Pelvic Fractures
Assessment
Inspection
Palpate prostate
Pelpiv ring
• Leg-length disrepancy , external rotation
• Pain on palpation of bony pelvic ring
• AP x - ray

Pelvic Fractures : Management
Resuscitate
Transfer as needed with PASG
Determine if intraperitoneal hermorrhage
Operation
Control hemorrhage Fixation device
Possible angiography

Questions

Summary
ABCDEs
Delineate mechanism
Repeated exams
Diagnostics as needed
High index of suspicion
Early recognition /prompt celiotomy