Embed Size (px)
Citation preview

www.aana.com/aanajournalonline AANA Journal June 2019 Vol. 87, No. 3 243
AANA Journal CourseClarifying the Confusion of Adult Emergence Delirium
Col Shawna Greiner, PhD, CRNA, USAF, NCMichael J. Kremer, PhD, CRNA, CHSE, FNAP, FAAN
ObjectivesAt the completion of this activity, the learner will be able to:
1. Identify the populations most at risk of emergenceand postoperative delirium.
2. Classify emergence delirium.3. Identify other phenomenon that can present similar
to emergence delirium.4. Select factors that may increase risk or exacerbate
emergence delirium.5. Differentiate between common anesthesia related
toxicities, postoperative delirium, and emergencedelirium.
IntroductionAlthough emergence delirium (ED) is well studied and understood in children, research findings pertaining to adults are contradictory, with an inadequate amount of evidence to guide practice. The definition of ED is unclear in the literature,1 and the reported incidence of ED is widely variable, ranging from 1.8% to 75%.2,3
Emergence delirium is a dangerous and costly occurrence in patients of all ages, and it is most prevalent in healthy pediatric patients and in younger adults.3-5 Postoperative delirium (POD) is typically noted in older patients with multiple comorbidities.6,7 Emergence delirium and POD
share some risk factors; both can be triggered by noxious stimuli encountered during the perioperative period, in-cluding surgery, medications, noise, and light, but they are distinctly different phenomena. There is a continuum of delirium that surgical patients may experience starting with ED that may progress to POD and postoperative cognitive decline.8,9 The distinction between ED and POD is important since prevention and treatments differ, yet the 2 phenomena are often referred to synonymously in the literature.
There is an increasing awareness of ED in adults, especially in military members who have been involved in combat or conflicts.3,10 Current literature does not adequately discriminate between ED, other deliria, or similarly presenting drug toxicities and medical condi-tions. Without an accurate differential diagnosis, the potential treatment choices for ED are unclear, and some options can exacerbate delirium. This course will discuss the similarities and differences of other phenomena that present similarly to ED, and describe evidence-based treatment options from an integrative literature review and a Delphi study.
Delphi Study Methods The authors obtained institutional review board approval
To date, researchers studying emergence delirium in adults have not adopted a consensus on the terminol-ogy for the phenomenon, a formalized definition, a measurement tool or standardized differential diag-nosis to distinguish emergence delirium from postop-erative delirium, anticholinergic or serotonergic toxici-ties, and other physiologic issues that may present on emergence from anesthesia. This lack of a consensus in emergence delirium research and differential diag-nostic tools is confounding findings and preventing
improved patient outcomes. Information from an integrative review of the literature in conjunction with a Delphi study was used to develop a standardized dif-ferential of similarly presenting phenomena to assist clinicians in determining appropriate interventions for patients who appear to have emergence delirium.
Keywords: Adult, differential diagnosis, emergence delirium.
The AANA Journal Course is published in each issue of the AANA Journal. Each article includes objectives for the reader and sources for additional reading. A 5-question open-book exam for each course is published on www.AANALearn.com and will remain live on the site for a period of 3 years. One continuing education (CE) credit can be earned by successfully completing the examination and evaluation. Each exam is priced at $35 for members and $21 for students but can be taken at no cost by using one of the six free CEs available annually to AANA members as a benefit of membership. For details, go to www.AANALearn.com. This educational activity is being presented with the understanding that any conflict of interest has been reported by the author(s). Also, there is no mention of off-label use for drugs or products.

244 AANA Journal June 2019 Vol. 87, No. 3 www.aana.com/aanajournalonline
and conducted a Delphi study to determine the definition of ED, to identify an appropriate assessment tool, and to highlight key concepts that could be used for future development of an adult ED assessment tool. A 3-round Delphi study composed of (1) automated telephone open-ended questions, (2) online relevance rating with com-ments, and (3) online relevance ranking with comments was conducted. The wording of the instructions, survey layout, confidence ratings, and scaling of the items were developed from themes identified during the integrative review per Delphi and survey development methods. Because of gaps identified during the literature review, the surveys were framed to determine the definition, appro-priate terminology, and key concepts of adult ED.
The 12 open-ended questions and survey items were developed using standard survey development methods. Perioperative clinicians including 2 anesthesiologists, 2 Certified Registered Nurse Anesthetists (CRNAs), 2 operating room nurses, and 2 postanesthesia care unit nurses reviewed each survey used for the 3 rounds of the Delphi for clarity, readability, and relevance. The first round of open-ended questions was formulated based on information gleaned through a integrative literature review. The second and third rounds of the Delphi study were generated from participant responses during the study and audited by associate investigators for clarity and readability. The surveys were created in Qualtrics software (SAP). As each round of the Delphi was com-pleted, open-ended responses were thematically coded, and quantitative data were analyzed using descriptive statistics and Cronbach α in SPSS version 22 (IBM Corp).
Nineteen purposively sampled perioperative profes-sionals were recruited, including 6 anesthesiologists, 7 CRNAs, 3 operating room nurses, and 3 recovery room nurses. By the end of the study, 13 (68%) of the par-ticipants remained. All participants met the criteria to be considered ED experts. For each round of the Delphi, all participants received feedback on their individual responses and the group responses. The participants were encouraged to provide rationale when they were in disagreement with the group or changed their mind regarding their individual responses.
Confusion About Emergence DeliriumIssues that confound our understanding of ED in the adult population include a lack of agreement on the fol-lowing items:
• a name• a definition• an assessment tool• a differential diagnosis• prevention and treatmentAmbiguous terminology and the absence of a set ED
definition limit our understanding of ED, resulting in the use of various terms to identify what may be ED. Other
terms used to describe delirium occurring during emer-gence from anesthesia are emergence agitation (primar-ily for pediatric patients), recovery room delirium, and POD. These terms are often used interchangeably but may not be synonymous with ED. Postoperative delirium is an example; it is likely that this is a related but differ-ent phenomenon.
A variety of ED measurement tools that were not identified, created without a validation process, devel-oped for use with pediatric patients, or used to monitor patient sedation and agitation in intensive care units were noted in current literature.1,11-16 To date, only the Pediatric Anesthesia Emergence Delirium tool has undergone construct and content validation for ED. Studies that validated the use of the Pediatric Anesthesia Emergence Delirium for adults involved participants who were military nurse anesthetists caring for military service members who were combat veterans.10 Many of these patients had preexisting mental health issues, such as anxiety, depression, and posttraumatic stress disorder (PTSD). It is possible that ED is being misidentified in practice and research, leading to inappropriate treatment and conflicting evidence without consistent use of a vali-dated adult assessment tool.
Lack of use of an adult-specific ED assessment tool hinders clear discernment between ED and similar phe-nomena. A clinical differential diagnosis that includes ED and does not consider other similar phenomena has led to imprecise ED prevention and treatment strategies. Some descriptions of ED based on the literature review and Delphi study follow.
Emergence Delirium Emergence delirium is in a subset of delirium catego-rized as substance/medication-induced delirium.9,17 It is described as an altered level of consciousness, disorien-tation, agitation, hyperactivity and/or hypoactivity, and thrashing and violent behavior with the potential to harm self or others, and it is prevalent in pediatric patients or adults under 40 years of age.3,10,14,16 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), delirium is a neurocognitive disor-der characterized by a deficit in cognitive function that is acquired.17 There are 5 diagnostic criteria, 4 elements, and 5 characteristics used for the differential diagnosis of the different types of delirium found in the DSM-5 under neurocognitive disorders, specifically the subcategories of substance intoxication delirium, medication-induced delirium, delirium due to medical conditions, and de-lirium due to multiple other causes.
Distinctions between ED, delirium resulting from drug toxicities, delirium due to another medical condi-tion (hypoxia, metabolic derangements, and dehydra-tion), and POD characterize prevention and helpful vs harmful interventions. Medications delivered during

www.aana.com/aanajournalonline AANA Journal June 2019 Vol. 87, No. 3 245
anesthesia can cause ED as seen in pediatric patients. Drugs that are commonly taken by adult patients interact with perioperative medications and can exacerbate other phenomena such as toxicities and POD that are under-diagnosed and misdiagnosed as ED. One example is the 400% rise in antidepressant prescriptions from 1988 to 2011, and polypharmacy involving psychoactive drugs, which can exacerbate these similar diagnoses such as drug toxicities.18 The clinical presentation of these deliria is similar to ED, but when the differential diagnosis does not result in an ED diagnosis, treatment specific to the identified delirium is required.
In addition to the physical ramifications of ED, there is an increased cost to patients, their families, and surgi-cal facilities. Patients who experience ED may remove in-dwelling catheters or tubes, injure themselves, or dehisce wounds or disrupt sutures, resulting in hemorrhage ne-cessitating surgical repair.1,16 Adult patients with ED re-quired up to 6 times more nursing resources than typical patients recovering from anesthesia.1 Those patients who experienced the hypoactive form of ED, in which the patient is sedate and unresponsive or mute, averaged 2 more days of hospitalization than their peers.15,19 This form of ED was likely to result in POD and ongoing com-plications, specifically cognitive and physical deteriora-tion that eventually required long-term care.9,20
• Defining Factors. There is no consistent definition of adult ED. Delphi study participants suggested this adult ED definition: “behavior after exposure to anesthe-sia in which a patient demonstrates or exhibits anxiety, restlessness, confusion, and combativeness.” The types of anesthetics most commonly associated with ED that were identified by study participants were any general anesthetic and inhaled anesthetics. Inhaled anesthetics were also indicated in several studies,21-24 specifically sevoflurane.11,12,25
Most clinicians assert that the onset of ED occurs as the patient awakens from anesthesia, although the exact time of onset varies. The literature review and the Delphi study described ED onset as occurring during either emergence or recovery from anesthesia. The literature review and the Delphi study results described ED as a short-lived reaction to perioperative events.
• Risk Factors. Identified ED risk factors included du-ration of anesthesia more than 1.5 hours, type of surgery, medical conditions, psychological issues, smoking, social alcohol use, and medications. Cases that required greater than 1 hour to complete increased the potential for ED. The types of surgery in which ED was more likely to occur included surgeries of the abdomen; breast; and ear, nose, and throat. The literature described other factors for ED as irritants (external and indwelling medical equipment), hypoxia, or a sense of suffocation and pain.
There was agreement between the literature and the Delphi study participants that fear, depression, anxiety
state and/or trait, PTSD, or trauma3,10,22,26 were more likely to exist in patients who experienced ED. The Delphi study participants added the risk factors of a history of sexual trauma or abuse and a prior history of ED. A prospective correlational study of ED in military members found ED rates of 20% in patients with combat experience and 17.5% in patients without psychological issues, and the authors noted that 50% of patients had anxiety, depression, and/or PTSD.10
The incidence of ED in military members and veterans is higher than in their civilian counterparts of the same age, ranging from 20% to 75%3,10 and 1.8% to 54%,2,4 respectively. Possible contributors to these higher rates include deployment to a combat area, underlying psychi-atric issues, psychotropic medications, and the formerly prescribed antimalarial, mefloquine.27,28
Drugs and drug interactions were cited as exacerbat-ing factors in both the literature and the Delphi study. Findings included perioperative medications adminis-tered, drug interactions, individual responses to anesthe-sia, and longer exposure times to anesthetics, but there was no consensus regarding specific triggering agents for ED. Many of the medications identified in the literature can be related to medical conditions and drug toxicities. Serotonin toxicity is exacerbated by a variety of anti-depressants, cocaine, and fentanyl.29,30 Anticholinergic toxicity can be related to risk of postoperative nausea and vomiting, anxiety, or scopolamine and benzodiaz-epines.13,14 Guidelines for diagnosing delirium recom-mend ruling out these 2 drug toxicities; both toxicities are common yet underdiagnosed because of provider unawareness.30,31 Neuromuscular relaxants1,15 and me-floquine were also identified as exacerbating factors and likely reflect other medical issues such as hypoxia secondary to inadequate oxygenation and ventilation and neurologic and/or psychological issues related to meflo-quine damage.
Mefloquine chemoprophylaxis was standard practice for personnel who served in conflicts where malaria is common, such as the Middle East, until 2009, when permanent neurologic sequelae were noted.32 Six years of mefloquine prescription statistics indicate that at least 150,000 veterans32,33 received this drug for 5 to 20 months. The neurologic and psychiatric side effects of mefloquine are very similar to ED and include abnormal dreams, anxiety, paranoia, agitation, confusion, memory impairment, and hallucinations.32 There is also a correla-tion between PTSD and mefloquine.32 The likely influ-ence of mefloquine in the military and veterans is a vari-able that has not been accounted for in most ED research.
• Diagnosis and Treatment. Treatment suggestions are limited by conflicting information regarding ED and by the probable misdiagnosis of ED. Currently, there is a lack of evidence for the prevention and treatment of ED, and the Food and Drug Administration (FDA) has not

246 AANA Journal June 2019 Vol. 87, No. 3 www.aana.com/aanajournalonline
approved any medications for its treatment. The correct diagnosis, determined by differential diag-
nosis, can be guided by information from the literature review and Delphi study. Predictive factors for adult ED include male gender, a younger age (< 40 years of age), history of smoking or social alcohol consumption, long-term use of benzodiazepines or antidepressants, preexisting mefloquine treatment, combat or deployment experience, depression, anxiety state and/or trait, PTSD, intraoperative inhaled anesthesia, fracture repairs, otolar-yngologic surgery, urologic surgery, gastric tubes, Foley catheters, endotracheal tubes, severe pain, and longer duration of surgery.4,5,16,22,24,26,34,35
The Pediatric Anesthesia Emergence Delirium tool is used to assess ED in pediatric patients and may have some limitations for the adult population, but it has been validated for use in adults.10 The Richmond Agitation-Sedation tool and the Confusion Assessment Method for the ICU (Intensive Care Unit; CAM-ICU) have the limita-tion of not being validated for use in ED, but were used to assess ED in most of the studies conducted within the past 5 years.4,5,16,24,25 Emergence delirium is the appropri-ate diagnosis if the patient has the identified predictive factors, POD and drug toxicities have been ruled out, and the Pediatric Anesthesia Emergence Delirium criteria have been met or findings from the combined Richmond Agitation-Sedation and CAM-ICU are consistent with ED.
Despite the lack of consensus and research findings regarding ED in adults, there are a few evidence-sup-ported recommendations for prevention and treatment. However, it is important to note that many of the current double-blind, randomized controlled studies excluded patients with a history of alcohol use or any psychologi-cal illness, although these patients typically are consid-ered to be at risk of ED.
The incidence of ED in adults is lower in institutions that provide extensive preoperative education and offer emotional support in lieu of benzodiazepine premedica-tion24,34 and avoid administration of inhaled anesthet-ics.5,21-24 When inhaled anesthetics were used instead of total intravenous anesthesia, patients who received a con-tinuous infusion of dexmedetomidine or remifentanil or a bolus of dexmedetomidine (0.5-1 μg/kg) or an N-methyl-d-aspartate (NMDA) agonist such as ketamine (0.5 mg/kg) at induction or 5 to 10 minutes before emergence were less likely to experience ED.4,25,36-38 The dosing for the con-tinuous infusion was 0.4 to 1 μg/kg/h and 0.25 to 1 μg/kg/min, respectively.11,39-41 Patients who received dexmedeto-midine had less postoperative pain, nausea, and vomiting. Newer case reports describe reversal of ED with dexme-detomidine, 0.5 to 1 μg/kg, when midazolam treatment, reassurance, and the presence of a family member failed.42 There is no current evidence that supports physostigmine as a treatment; it is likely that agitation that is reversed by this drug is unidentified anticholinergic toxicity.31,43
Similar PhenomenaPostoperative delirium and serotonergic and anticho-linergic toxicities can have signs that mimic ED. Other physiologic issues commonly experienced by patients during the perioperative period that can present as ED include hypoxia, inadequate reversal of neuromuscular blockade, pain, and metabolic derangements. An accu-rate differential diagnosis is essential because inappropri-ate treatments will exacerbate the presenting condition.
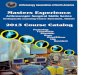
Postoperative delirium and anticholinergic and se-rotonin toxicities share the signs of agitation, rest-lessness, anxiety, confusion, and disorientation with ED.10,29,35,44,45 There are other distinguishing signs that can be used to identify ED in adults and to assist in ap-propriate clinical interventions. The Figure compares phenomena that can present as ED.
• Postoperative Delirium. Postoperative delirium is both costly and dangerous. The average cost of postopera-tive delirium is $2,947 per affected patient, annualized to $2 billion each year.19 Patients with POD have the poten-tial for up to 3 times higher morbidity and mortality within 6 months, related to ensuing progressive cognitive decline and other medical issues such as stroke and sepsis.8,14
In contrast to ED, POD primarily affects older adults and occurs after initial recovery from anesthesia up to 24 hours or even days after surgery.9,20,45,49 Inouye50 de-scribed delirium in older adults as resulting from triggers that are a combination of preexisting vulnerabilities and noxious stimuli in the Multifactorial Model of Delirium of Older Persons. This theoretical model is the primary theoretical framework for POD literature. There are some studies that identified older adults with ED,1 but the as-sessment tools used were developed and validated for intensive care sedation and agitation. Established POD risk factors include a lack of acetylcholine, excessive do-pamine, proinflammatory cytokines, γ-aminobutyric acid deficiency (linked to substance abuse), sensory impair-ments, sleep deficits, lack of familiarity with the environ-ment, social isolation, loss of cognitive reserve associated with aging, constipation, indwelling catheters, smoking, anesthetic neurotoxicity, coexisting comorbidities (eg, hypertension, diabetes), dehydration, metabolic derange-ments, infection, inflammation, hypoxia, hypercapnia or hypocapnia, inadequate perfusion, and pharmacologic interactions.7,46,47,49
Because pharmacologic treatments of POD can lead to poorer long-term outcomes and can exacerbate and prolong adverse outcomes, current POD clinical practice guidelines by the American Geriatrics Society (AGS) Expert Panel on Postoperative Delirium in Older Adults recommend first employing prevention.47 Prophylaxis of POD includes orienting the patient to the perioperative area, allowing the use of hearing aids and glasses before surgery and on emergence reorienting the patient to his or her environment after surgery, presence of family or

www.aana.com/aanajournalonline AANA Journal June 2019 Vol. 87, No. 3 247
a friend during recovery from anesthesia, adjusting the environment, encouraging fluid and nutritional intake, avoiding constipation, promoting early activity, cognitive stimulation, nonpharmacologic sleep hygiene before and after surgery, and providing oxygenation. Avoid anes-thetic neurotoxicity by using age-appropriate (chrono-logic or physiologic age) anesthetic doses, maintaining a mean arterial pressure close to the patient’s awake levels, and considering avoiding a deep anesthetic. Also impor-tant is adequate pain control,6,46,47 preferably nonopioid options such as acetaminophen doses of 650 mg if the patient is older than 65 years and 1,000 mg if younger, or use of dexmedetomidine, 0.1 μg/kg/h. If narcotics must be used, avoid meperidine.48 The analgesic and antiinflammatory properties of ketamine decrease the incidence of POD; the recommendation is to give a single dose of 0.5 to 1 mg/kg before the incision. Gabapentin and celecoxib may also have a role,47,49 but more research is needed. In older adults, several medications potentiate POD. Whenever possible, avoid all tricyclic antidepres-sants, anticholinergics (using only glycopyrrolate), an-tihistamines, benzodiazepines (especially midazolam), chlorpromazine, corticosteroids, histamine H2 receptor antagonists, meperidine,46 minimizing sedative hypnot-ics, and medications that increase serotonin (to avoid serotonin toxicity),47 in addition to following the current AGS Beers Criteria Update Expert Panel as a guide of medications to avoid.49 When POD occurs, determina-tion of the underlying causes, including dehydration, infection, hypoxemia, and alcohol or drug withdrawal should be considered. As a last resort for a patient with POD who is in jeopardy of harming self or others, re-straints or pharmacologic treatment can be employed, such as haloperidol dosed in 0.5- to 1-mg increments every 30 minutes for a maximum of 20 mg/24 h, but this may result in worse patient outcomes.47,49 Other drugs that may be effective in treating POD are chlorpromazine and benzodiazepines, which have yielded inconsistent outcomes. Another possible pharmacologic interven-tion is the benzodiazepine lorazepam, 0.5 mg, every 30 minutes for a maximum dose of 6 mg in 24 hours, which also may worsen the delirium and impair full recovery.49
• Anticholinergic Toxicity. Anticholinergic toxicity shares similar characteristics with ED. In fact, delirium is caused by anticholinergic drugs in healthy adults.31 Therefore, it is useful to rule out this diagnosis in pa-tients who have received antiemetics, antihistamines, antiparkinsonian agents, benzodiazepines, opioids, sco-polamine, atropine, promethazine, droperidol, halo-peridol, halothane, etomidate, propofol, or ketamine.43,44 However, there are no current user-friendly diagnostic criteria and many presentations, a difficulty that compli-cates identifying anticholinergic toxicity.
Although some treatments for ED are useful for an-ticholinergic toxicity, others can further exacerbate the
problem if anticholinergic toxicity is misdiagnosed as ED. One treatment, physostigmine, is useful because it can reverse anticholinergic crisis. But, if a patient has anticho-linergic toxicity and is treated for ED with some recom-mended drugs, such as propofol, ketamine, or droperidol, then anticholinergic toxicity could be amplified.31,43 Signs and symptoms specific to anticholinergic toxicity that can be used for diagnostic differentiation and directing treat-ment are anhidrosis, mydriasis, constipation, an urge to urinate, and a sense of bladder fullness. A confounding factor is that many patients emerging from anesthesia cannot coherently verbalize the last 3 symptoms.
Patients with anticholinergic toxicity usually respond to treatment with physostigmine. It is important to note there is a high incidence of nausea and vomiting with this treatment. Appropriate adult intravenous dosing is 0.5 to 2 mg given over 5 minutes not to exceed 1 mg/min and may be repeated in 20 to 30 minutes if symptoms resurge.44 It is important to have atropine ready to treat cholinergic responses. Benzodiazepines can be used to relieve some of the signs and symptoms of anticholinergic toxicity, but they do not treat the underlying pathology.
• Serotonergic Toxicity. Like anticholinergic toxic-ity, serotonin toxicity can present similarly to ED. Some medications that can trigger or potentiate serotonergic toxicity are synthetic phenylpiperidine opioids (fentanyl, alfentanil, sufentanil, meperidine, methadone, dextro-methorphan, and tramadol), amphetamines, monoamine oxidase inhibitors, tricyclic antidepressants, serotonin or serotonin-norepinephrine reuptake inhibitors, lithium, buspirone, and L-tryptophan; other potential triggers are cocaine, MDMA (Ecstasy), and bath salts.29,30 A thor-ough preoperative examination and history can provide clinicians with useful diagnostic information.
Serotonin toxicity is a physiologic reaction to an excess of serotonin in synaptic clefts that presents as motor and mental excitability with altered levels of consciousness that resembles ED. The clinical features of serotonin toxicity are demonstrated in the Figure. Some of the motor and autonomic effects, specifically myoclonus, hyperthermia, flushing, diaphoresis, and mydriasis29 are not present in adults with ED. This toxicity is reliably diagnosed using the Hunter Serotonin Toxicity Criteria29 (see Figure). The primary treatments of serotonin toxicity are avoiding further administration of triggering agents, supportive care, sedation with benzodiazepines (eg, lorazepam, 2-4 mg, or diazepam, 5 to 10 mg, IV repeated every 8 to 10 minutes as needed), cyproheptadine in a 12-mg loading dose fol-lowed by 2 mg by mouth or gastric tube every 2 hours for a maximum of 32 mg/d if the patient is hemodynamically labile, and providing neuromuscular relaxation and intuba-tion for hyperthermic or critically ill patients.29,30
ConclusionInformation regarding adult ED is not conclusive with

248 AANA Journal June 2019 Vol. 87, No. 3 www.aana.com/aanajournalonline
PREDICTIVE FACTORS
■ Male, younger age ■ History of smoking or social alcohol drinking ■ Long-term use of benzodiazepines or antidepressants■ Pre-existing mefloquine regimen, combat or deployment experience,
depression, anxiety state and/or trait, PTSD Intraoperative inhaled anesthesia ■ Longer surgical durations (greater than 1.5 hours)■ Types of surgery: Fracture repairs, otolaryngological surgery, urological
surgery ■ Presence of gastric tubes, foley catheters, endotracheal tubes ■ Severe pain, previous experienced ED
■ Lack of acetylcholine, excessive dopamine, proinflammatory cytokines ■ Gamma-aminobutyric acid deficiency (linked to substance abuse), smoking■ Sensory impairments, sleep deficits, lack of familiarity with the environment,
social isolation■ Anesthetic neurotoxicity (too much anesthetic for age), inadequate
perfusion from hypotension■ Loss of cognitive reserve associated with aging or substance abuse ■ Coexisting comorbidities: Hypertension, diabetes, dehydration, metabolic
derangements, infection, inflammation, hypoxia, hyper or hypocapnia ■ Irritants: Constipation, full bladder, indwelling catheters■ Pharmacological interactions
High risk medications: Parkinson's medications; trihexyphenidyl (Artane), benztropine mesylate (Cogentin), biperiden (Akineton); antipsychotics and antidepressants such as clomipramine (Anafranil), chlorpromazine (Thorazine), clozapine (Clozaril), fluphenazine (Prolixin), loxapine (Loxitane), olanzapine (Zyprexa), perphenazine (Trilafon), pimozide (Orap), quetiapine (Seroquel), thioridazine (Mellaril), thiothixene (Navane), trifluoperazine (Stelazine), chloridiazepoxide (Librium), amitriptyline (Elavil, Endep), amoxapine (Asendin), clomipramine (Anafranil,) desipramine (Norpramin), doxepin (Silenor), imipramine (Tofranil), nortriptyline (Pamelor), protriptyline (Vivactil), trimipramine (Surmontil); antispasmodics belladonna, dicyclomine (Bentyl), hyoscyamine (Levsin); overactive bladder medications oxybutynin (Ditropan), darifenacin (Enablex), solifenacin (Vesicare), fesoterodine (Toviaz), tolterodine (Detrol), trospium (Sanctura); muscle relaxants such as cyclobenzaprine (Flexeril), dantrolene (Dantrium), carisoprodol (Soma), methocarbamol (Robaxin), orphenadrine (Norflex), tizanidine (Zanaflex); motion sickness medications such as meclizine (Antivert); belladonna; dicyclomine (Bentyl); hyoscyamine (Levsin); loperamide (Imodium); scopolamine, diphenhydramine (Benadryl), or promethazine (Phenergan).
A person taking monoamine oxidase inhibitors (furazolidone, isocarboxazid, linezolid, phenelzine, selegiline, Syrian rue, tranylcypromine), tricyclic antidepressants (amitriptyline, amoxapine, clomipramine, desipramine, doxepin, imipramine, maprotiline, nortriptyline, protriptyline, trimipramine), serotonin or serotonin-norepinephrine reuptake inhibitors (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, desvenlafaxine, duloxetine, venlafaxine), triptans (almotriptan, dihydroergotamine, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan), levomethorphan, levorphanol, pentazocine, pethidine, tapentadol, the antiparkinsonian L-dopa, mirtazapine, trazadone, lithium, buspirone, phentermine, bupropion, risperidone, nefazodone, trazodone, granisetron, ondansetron, chlorpheniramine, ciprofloxacin, ritonavir, fluconazole, citalopram, methadone, oxycodone, tramadol, metoclopramide, amphetamines, bath salts, cocaine, dextromethorphan, ecstasy, LSD, L-tryptophan, St. John’s wort (Hypericum perforatum).
Serotonergic ToxicityEmergence Delirium Postoperative Delirium Anticholinergic Toxicity
■ Provide extensive preoperative education and emotional support ■ Minimize or avoid benzodiazepines through reassurance and preoperative
education■ Avoid inhaled anesthetics or combine with
• Continuous infusion of dexmedetomidine 0.4-1 μg/kg/hr or remifentanil 0.25-1 μg/kg/min or
• Bolus of dexmedetomidine (0.5-1 mcg/kg) or ketamine (0.5 mg/kg) on induction or 5-10 minutes before emergence
■ Orient and educate the patient to the perioperative area ■ Instruct the patient on non-pharmacological sleep hygiene before surgery
and promote after surgery■ Encouraging fluid and nutritional intake per the enhanced recovery protocol
before and after surgery■ Allow the use of hearing aids and glasses before surgery and on
emergence■ Consider using ketamine 0.5-1 mg/kg before incision for the
antiinflammatory properties ■ Avoid anesthetic neurotoxicity by using age (chronologic or physiologic)
appropriate anesthetic doses■ Maintain a mean arterial pressure near the patients’ awake levels■ Ensure adequate pain control using non-opioid options whenever possible
• Acetaminophen 1000 mg unless >65 years old then 650 mg or dexmedetomidine 0.1mcg/kg/hr
■ Provide oxygen during recovery from anesthesia■ Reorienting the patient to their environment after surgery■ Allow the presence of family or a friend during recovery from anesthesia■ Adjust the environment (e.g. quiet with mid-level lighting)■ Avoiding constipation■ Promoting early activity■ Provide cognitive stimulation■ Avoid all tricyclic antidepressants, anticholinergics (use only glypyrrolate),
antihistamines, benzodiazepines (especially midazolam), chlorpromazine, corticosteroids, H2 receptors antagonists, meperidine, minimizing sedative hypnotics, and medications that increase serotonin, follow current AGS Beers Criteria
PREVENTIVE STRATEGIES
COMMON PRESENTING S/S Disoriented, RestlessAgitated, Anxious, Confused, Delusions, Hallucinations, Calling Out, Amnesia, Hypoactivity
DIFFERENTIATING S/S young, healthy, violent, thrashing, traumatic past or military deployment history. older age, altered sleep and sensory perception or after recovery within 24 hours of surgery, possible continuation from ED
Anhidrosis, mydriasis, constipation, an urge to urinate and a sense of bladder fullness.
If the patient is on any of the medications above avoid administering atropine, scopolamine, diphenhydramine (Benadryl), or promethazine (Phenergan) during the perioperative period.
ASSESSMENT TOOLS
Pediatric Anesthesia Emergence Delirium scale or Richmond Agitation Sedation Scale with Confusion Assessment Method for Intensive Care Patients. A score of 10 or greater on this PAED indicates ED.
TREATMENT
■ Address triggers such as anxiety, pain, hypoxia and catheters
■ Provide reassurance ■ Allow the presence of a loved one ■ Bolus with dexmedetomide 0.5–1 mcg/kg
Mini-Mental State Exam and the Confusion Assessment Method
Treat underlying causes to include dehydration, infection, hypoxemia, and alcohol or drug withdrawal. Haldoperidol dosed in 0.5-1 mg increments every 30 minutes for a maximum of 20 mg per 24 hours if the patient is harming self or others and treating the underlying cause has failed.
1)
2) Avoid or stop the triggering agentsProvide supportive care (hydration, cooling, neuromuscular relaxation and intubation) and sedate with benzodiazepines (e.g. lorazepam 2-4 mg or diazepam 5-10 mg IV repeated every 8-10 minutes as needed)
3) Load with cyproheptadine 12 mg then 2 mg by mouth or gastric tube every 2 hours up
to 32 mg/day
None
Physostigmine 0.5-2 mg over 5 minutes or 1mg/minute, repeat every 20-30 minutes as needed.Benzodiazepines can be used, but do not relieve the underlying cause.
Hunter Serotonin Toxicity Criteria
This algorithm was created using these sources4,6,7,9-11,14,16,20-31,34-46,48-50
*Boolean terms or and and
Figure. Algorithm for Differential Diagnosis of Emergence Delirium (ED)aAbbreviations: AGS, American Geriatrics Society; L, levo; LSD, lysergic acid diethylamide; PAED, Pediatric Anesthesia Emergence Delirium tool; POD, postoperative delirium; PTSD, posttraumatic stress disorder; S/D, signs and symptoms.

www.aana.com/aanajournalonline AANA Journal June 2019 Vol. 87, No. 3 249
PREDICTIVE FACTORS
■ Male, younger age ■ History of smoking or social alcohol drinking ■ Long-term use of benzodiazepines or antidepressants■ Pre-existing mefloquine regimen, combat or deployment experience,
depression, anxiety state and/or trait, PTSD Intraoperative inhaled anesthesia ■ Longer surgical durations (greater than 1.5 hours)■ Types of surgery: Fracture repairs, otolaryngological surgery, urological
surgery ■ Presence of gastric tubes, foley catheters, endotracheal tubes ■ Severe pain, previous experienced ED
■ Lack of acetylcholine, excessive dopamine, proinflammatory cytokines ■ Gamma-aminobutyric acid deficiency (linked to substance abuse), smoking■ Sensory impairments, sleep deficits, lack of familiarity with the environment,
social isolation■ Anesthetic neurotoxicity (too much anesthetic for age), inadequate
perfusion from hypotension■ Loss of cognitive reserve associated with aging or substance abuse ■ Coexisting comorbidities: Hypertension, diabetes, dehydration, metabolic
derangements, infection, inflammation, hypoxia, hyper or hypocapnia ■ Irritants: Constipation, full bladder, indwelling catheters■ Pharmacological interactions
High risk medications: Parkinson's medications; trihexyphenidyl (Artane), benztropine mesylate (Cogentin), biperiden (Akineton); antipsychotics and antidepressants such as clomipramine (Anafranil), chlorpromazine (Thorazine), clozapine (Clozaril), fluphenazine (Prolixin), loxapine (Loxitane), olanzapine (Zyprexa), perphenazine (Trilafon), pimozide (Orap), quetiapine (Seroquel), thioridazine (Mellaril), thiothixene (Navane), trifluoperazine (Stelazine), chloridiazepoxide (Librium), amitriptyline (Elavil, Endep), amoxapine (Asendin), clomipramine (Anafranil,) desipramine (Norpramin), doxepin (Silenor), imipramine (Tofranil), nortriptyline (Pamelor), protriptyline (Vivactil), trimipramine (Surmontil); antispasmodics belladonna, dicyclomine (Bentyl), hyoscyamine (Levsin); overactive bladder medications oxybutynin (Ditropan), darifenacin (Enablex), solifenacin (Vesicare), fesoterodine (Toviaz), tolterodine (Detrol), trospium (Sanctura); muscle relaxants such as cyclobenzaprine (Flexeril), dantrolene (Dantrium), carisoprodol (Soma), methocarbamol (Robaxin), orphenadrine (Norflex), tizanidine (Zanaflex); motion sickness medications such as meclizine (Antivert); belladonna; dicyclomine (Bentyl); hyoscyamine (Levsin); loperamide (Imodium); scopolamine, diphenhydramine (Benadryl), or promethazine (Phenergan).
A person taking monoamine oxidase inhibitors (furazolidone, isocarboxazid, linezolid, phenelzine, selegiline, Syrian rue, tranylcypromine), tricyclic antidepressants (amitriptyline, amoxapine, clomipramine, desipramine, doxepin, imipramine, maprotiline, nortriptyline, protriptyline, trimipramine), serotonin or serotonin-norepinephrine reuptake inhibitors (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, desvenlafaxine, duloxetine, venlafaxine), triptans (almotriptan, dihydroergotamine, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan), levomethorphan, levorphanol, pentazocine, pethidine, tapentadol, the antiparkinsonian L-dopa, mirtazapine, trazadone, lithium, buspirone, phentermine, bupropion, risperidone, nefazodone, trazodone, granisetron, ondansetron, chlorpheniramine, ciprofloxacin, ritonavir, fluconazole, citalopram, methadone, oxycodone, tramadol, metoclopramide, amphetamines, bath salts, cocaine, dextromethorphan, ecstasy, LSD, L-tryptophan, St. John’s wort (Hypericum perforatum).
Serotonergic ToxicityEmergence Delirium Postoperative Delirium Anticholinergic Toxicity
■ Provide extensive preoperative education and emotional support ■ Minimize or avoid benzodiazepines through reassurance and preoperative
education■ Avoid inhaled anesthetics or combine with
• Continuous infusion of dexmedetomidine 0.4-1 μg/kg/hr or remifentanil 0.25-1 μg/kg/min or
• Bolus of dexmedetomidine (0.5-1 mcg/kg) or ketamine (0.5 mg/kg) on induction or 5-10 minutes before emergence
■ Orient and educate the patient to the perioperative area ■ Instruct the patient on non-pharmacological sleep hygiene before surgery
and promote after surgery■ Encouraging fluid and nutritional intake per the enhanced recovery protocol
before and after surgery■ Allow the use of hearing aids and glasses before surgery and on
emergence■ Consider using ketamine 0.5-1 mg/kg before incision for the
antiinflammatory properties ■ Avoid anesthetic neurotoxicity by using age (chronologic or physiologic)
appropriate anesthetic doses■ Maintain a mean arterial pressure near the patients’ awake levels■ Ensure adequate pain control using non-opioid options whenever possible
• Acetaminophen 1000 mg unless >65 years old then 650 mg or dexmedetomidine 0.1mcg/kg/hr
■ Provide oxygen during recovery from anesthesia■ Reorienting the patient to their environment after surgery■ Allow the presence of family or a friend during recovery from anesthesia■ Adjust the environment (e.g. quiet with mid-level lighting)■ Avoiding constipation■ Promoting early activity■ Provide cognitive stimulation■ Avoid all tricyclic antidepressants, anticholinergics (use only glypyrrolate),
antihistamines, benzodiazepines (especially midazolam), chlorpromazine, corticosteroids, H2 receptors antagonists, meperidine, minimizing sedative hypnotics, and medications that increase serotonin, follow current AGS Beers Criteria
PREVENTIVE STRATEGIES
COMMON PRESENTING S/S Disoriented, RestlessAgitated, Anxious, Confused, Delusions, Hallucinations, Calling Out, Amnesia, Hypoactivity
DIFFERENTIATING S/S young, healthy, violent, thrashing, traumatic past or military deployment history. older age, altered sleep and sensory perception or after recovery within 24 hours of surgery, possible continuation from ED
Anhidrosis, mydriasis, constipation, an urge to urinate and a sense of bladder fullness.
If the patient is on any of the medications above avoid administering atropine, scopolamine, diphenhydramine (Benadryl), or promethazine (Phenergan) during the perioperative period.
ASSESSMENT TOOLS
Pediatric Anesthesia Emergence Delirium scale or Richmond Agitation Sedation Scale with Confusion Assessment Method for Intensive Care Patients. A score of 10 or greater on this PAED indicates ED.
TREATMENT
■ Address triggers such as anxiety, pain, hypoxia and catheters
■ Provide reassurance ■ Allow the presence of a loved one ■ Bolus with dexmedetomide 0.5–1 mcg/kg
Mini-Mental State Exam and the Confusion Assessment Method
Treat underlying causes to include dehydration, infection, hypoxemia, and alcohol or drug withdrawal. Haldoperidol dosed in 0.5-1 mg increments every 30 minutes for a maximum of 20 mg per 24 hours if the patient is harming self or others and treating the underlying cause has failed.
1)
2) Avoid or stop the triggering agentsProvide supportive care (hydration, cooling, neuromuscular relaxation and intubation) and sedate with benzodiazepines (e.g. lorazepam 2-4 mg or diazepam 5-10 mg IV repeated every 8-10 minutes as needed)
3) Load with cyproheptadine 12 mg then 2 mg by mouth or gastric tube every 2 hours up
to 32 mg/day
None
Physostigmine 0.5-2 mg over 5 minutes or 1mg/minute, repeat every 20-30 minutes as needed.Benzodiazepines can be used, but do not relieve the underlying cause.
Hunter Serotonin Toxicity Criteria
This algorithm was created using these sources4,6,7,9-11,14,16,20-31,34-46,48-50
*Boolean terms or and and
aThis algorithm was created using references 4, 6, 7, 9-11, 14, 16, 20-31, and 34-48.

250 AANA Journal June 2019 Vol. 87, No. 3 www.aana.com/aanajournalonline
regard to its definition, applicable assessment tools, ter-minology, differential diagnosis for similar phenomena, and treatment. Some of these concerns were clarified by a review of the literature and a Delphi study, whereas other questions need further study. In the Delphi study, the definition most agreed on by the experts was “be-havior after an exposure to anesthesia in which a patient demonstrates or exhibits anxiety, restlessness, confusion, and combativeness.” Prevention through the actions pre-viously discussed is the most beneficial for the patient.
It is still unclear which assessment tool is most appro-priate for differentiating ED, but until there is a reliable and valid adult tool, the Pediatric Anesthesia Emergence Delirium scale is supported in both the literature review and the Delphi. An alternative presented in the literature is the Richmond Agitation-Sedation Scale combined with the CAM-ICU. Additionally, it is important to consider other phenomena that can appear to be adult ED through the use of more standardized differential diagnostic tools such as the one provided in the Figure.
Physiologic issues, POD, and anticholinergic and serotonergic toxicities must be carefully ruled out by differentiating signs that are unique to each diagnosis. If a patient presents as experiencing ED, the practitioner should evaluate for the presence of common adult ED predictors. When ED is ruled in, address the triggering physical issue (eg, hypoxia, pain, anxiety, catheters), provide reassurance, or allow a loved one to be present. If ED continues, treat with a bolus of dexmedetomidine.
For POD, if the patient is physiologically or chrono-logically older than 65 years of age or has other comor-bidities such as hypertension, diabetes, sensory depriva-tion, substance abuse, or diseases that cause metabolic derangements or dehydration, these conditions must be considered in the differential diagnosis. Prevention is the most effective strategy to limit the occurrence of POD and results in improved patient outcomes. Note that POD can be delirium that persists beyond the usual timeframe for recovery from anesthesia and responds to treatment with antipsychotics.
Anticholinergic toxicity may manifest for patients who have received the medications discussed earlier. Evaluate for the presence of the signs and symptoms unique to this diagnosis, which are anhidrosis, mydriasis, constipation, and bladder fullness (if possible to assess). The treatment is administration of physostigmine following the guide-lines provided.
Finally, serotonergic toxicity is triggered by many of the medications we administer during an anesthetic. Follow the Hunter Serotonin Toxicity Criteria if a patient is displaying any of the signs specific to this toxicity, to include diaphoresis, muscle rigidity, clonus, ocular clonus, hyperreflexivity, tremors, shivering, vomiting, or diarrhea. In the event that serotonergic toxicity is ruled in, remove the offending drug and provide supportive
care, benzodiazepines, and cyproheptadine. Awareness of how to differentiate these similar phe-
nomena and incorporating an algorithm, such as the one provided in this article, for a thorough and consistent differential diagnosis can lead to improved patient out-comes and interventions for adults with ED. There is a need for research to develop an adult ED assessment tool that investigates patient outcomes when an algorithm like the one provided in this article is implemented.
REFERENCES 1. Lepouse C, Lautner CA, Liu L, Gomis P, Leon A. Emergence
delirium in adults in the post-anaesthesia care unit. Br J Anaesth. 2006;96(6):747-753. doi:10.1093/bja/ael094
2. Hung WT, Chen CC, Liou CM, Tsai WY. The effects of low-dose fentanyl on emergence agitation and quality of life in patients with moderate developmental disabilities. J Clin Anaesth. 2005;17(7):494-498. doi:10.1016/j.jclinane.2004.09.014
3. Wilson JT, Pokorny ME. Experiences of military CRNAs with ser-vice personnel who are emerging from general anesthesia. AANA J. 2012;80(4):260-265.
4. Demir CY, Yuzkat N. Prevention of emergence agitation with ketamine in rhinoplasty. Aesthetic Plast Surg. 2018;2(3):847-853. doi:10.1007/s00266-018-1103-4
5. Kim HJ, Kim DK, Kim HY, Kim JK, Choi SW. Risk factors of emer-gence agitation in adults undergoing general anesthesia for nasal surgery. Clin Exp Otorhinolaryngol. 2015;8(1):46-51. doi:10.3342/ceo.2015.8.1.46
6. Oh ES, Fong TG, Hshieh TT, Inouye SK. Delirium in older persons: advances in diagnosis and treatment. JAMA. 2017;318(12):1161-1174. doi:10.1001/jama.2017.12067
7. Cascella M, Muzio MR, Bimonte S, Cuomo A, Jakobsson JG. Postoperative delirium and postoperative cognitive dysfunction: updates in pathophysiology, potential translational approaches to clinical practice and further research perspectives. Minerva Anestesiol. 2018;84(2):246-260. doi:10.23736/S0375-9393.17.12146-2
8. Guenther U, Radtke FM. Delirium in the postanaesthesia period. Curr Opin Anaesthesiol. 2011;24(6):670-675. doi:10.1097/ACO.0b013e32834c7b44
9. Silverstein JH, Timberger M, Reich DL, Uysal S. Central nervous system dysfunction after noncardiac surgery and anesthesia in the elderly. Anesthesiology. 2007;106(3):622-628.
10. McGuire JM. The incidence of and risk factors for emergence delirium in U.S. military combat veterans. J Perianesth Nurs. 2012;27(4):236-245. doi:10.1016/j.jopan.2012.05.004
11. Kavalci G, Ethemoglu FB, Durukan P, Batuman A, Emre C. Com-parison of the effects of dexmedetomidine and remiphentanyl on emergence agitation after sevoflurane anesthesia in adults undergoing septoplasty operation: a randomized double-blind trial. Eur Rev Med Pharm Sci. 2013;17(22):3019-3023.
12. Kim YS, Chae YK, Choi YS, et al. A comparative study of emergence agitation between sevoflurane and propofol anesthesia in adults after closed reduction of nasal bone fracture. Korean J Anesthesiol. 2012;63(1):48-53. doi:10.4097/kjae.2012.63.1.48
13. Kim SY, Kim JM, Lee JH, Song BM, Koo BN. Efficacy of intraopera-tive dexmedetomidine infusion on emergence agitation and quality of recovery after nasal surgery. Br J Anaesth. 2013;111(2):222-228. doi:10.1093/bja/aet056
14. Radtke FM, Franck M, Hagemann L, Seeling M, Wernecke KD, Spies CD. Risk factors for inadequate emergence after anesthesia: emergence delirium and hypoactive emergence. Minerva Anestesiol. 2010;76(6):394-404.
15. Xara D, Silva A, Mendonca J, Abelha F. Inadequate emergence after anesthesia: emergence delirium and hypoactive emergence in the Postanesthesia Care Unit. J Clin Anesth. 2013;25(6):439-446.
16. Yu D, Chai W, Sun X, Yao L. Emergence agitation in adults: risk fac-tors in 2,000 patients. Can J Anaesth. 2010;57(9):843-848.

www.aana.com/aanajournalonline AANA Journal June 2019 Vol. 87, No. 3 251
17. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition: DSM-5. Washington, DC: American Psychiatric Association; 2013.
18. Szalavitz M. What does a 400% increase in antidepressant use really mean? Time. October 20, 2011. http://healthland.time.com/2011/10/20/what-does-a-400-increase-in-antidepressant-pre-scribing-really-mean/ Accessed April 5, 2019.
19. Radtke FM, Franck M, Lorenz M, et al. Remifentanil reduces the incidence of post-operative delirium. J Int Med Res. 2010;38(4):1225-1232. doi:10.1177/147323001003800403
20. Whitlock EL, Vannuccie A, Avidan MS. Postoperative delirium. Minerva Anestesiol. 2011;77(4):448-456.
21. Cotoia A, Mirabella L, Beck R, et al. Effects of closed-loop intravenous anesthesia guided by the Bispectral index in adult patients on emer-gence delirium. A randomized controlled study. Minerva Anestesiol. 2018;84(4):437-446. doi:10.23736/S0375-9393.17.11915-2
22. Chen L, Xu M, Li GY, Cai WX, Zhou JX. Incidence, risk factors and consequences of emergence agitation in adult patients after elective craniotomy for brain tumor: a prospective cohort study. PloS One. 2014;9(12):e114239. doi:10.1371/journal.pone.0114239
23. Liu GY, Chen ZQ, Zhang ZW. Comparative study of emergence agita-tion between isoflurane and propofol anesthesia in adults after closed reduction of distal radius fracture. Genet Mol Res. 2014;13(4):9285-9291. doi:10.4238/2014.January.24.9
24. Munk L, Andersen G, Moller AM. Post-anaesthetic emergence delirium in adults: incidence, predictors and consequences. Acta Anaesthesiol Scand. 2016;60(8):1059-1066. doi:10.1111/aas.12717
25. Jung J-W, Kim YH, Lee KH, et al. Effect of dexmedetomidine on emergence agitation in male patients undergoing closed reduction of a nasal bone fracture. Rawal Med J. 2015;40(2):191-196.
26. Umholtz M, Cilnyk J, Wang CK, Porhomayon J, Pourafkari L, Nader ND. Postanesthesia emergence in patients with post-trau-matic stress disorder. J Clin Anesth. 2016;34:3-10. doi:10.1016/j.jclinane.2016.02.047
27. Gullahorn GM, Bohman HR, Wallace MR. Anaesthesia emergence delirium after mefloquine prophylaxis. Lancet. 1993;341(8845):632. doi:10.1016/0140-6736(93)90392-T
28. Nevin RL. Re: McGuire JM. The inicidence of and risk factors for emergence delirium in U.S. military combat veterans [letter]. J Peri-anesth Nurs. 2013;28(6):334-335. doi:10.1016/j.jopan.2013.09.003
29. Buckley NA, Dawson AH, Isbister GK. Serotonin syndrome. BMJ. 2014;348:g1626. doi:10.1136/bmj.g1626
30. Volpi-Abadie J, Kaye AM, Kaye AD. Serotonin syndrome. Ochsner J. 2013;13(4):553-540.
31. Gopinathan V. Central anticholinergic syndrome—a forgotten entity. Br J Anaesth. 2008;101(eLetters suppl). doi:10.1093/bja/el_2684
32. Nevin RL. Mefloquine and post traumatic stress disorder. In: Ritchie EC, ed. Forensic and Ethical Issues in Military Behavioral Health. Wash-ington, DC: Borden Institute; 2015:278-296. Textbooks of Military Medicine series.
33. Kersgard CM, Hickey PW. Adult malaria chemoprophylaxis prescrib-ing patterns in the military health system from 2007-2011. Am J Trop Health Med Hyg. 2013;89(2):317-325. doi:10.4269/ajtmh.13-0013
34. Card E, Pandharipande P, Tomes C, et al. Emergence from general anaesthesia and evolution of delirium signs in the post-anaesthesia care unit. Br J Anaesth. 2015;115(3):411-417. doi:10.1093/bja/aeu442
35. Wilson JT. Pharmacologic, physiologic, and psychological character-istics associated with emergence delirium in combat veterans. AANA J. 2014;82(5):355-362.
36. Ham SY, Kim JE, Park C, Shin MJ, Shim YH. Dexmedetomidine does not reduce emergence agitation in adults following orthognathic surgery. Acta Anaesthesiol Scand. 2014;58(8):955-960. doi:10.1111/aas.12379
37. Lee SH, Lee CY, Lee JG, Kim N, Lee HM, Oh YJ. Intraoperative dexmedetomidine improves the quality of recovery and postop-erative pulmonary function in patients undergoing video-assisted thoracoscopic surgery: a CONSORT-prospective, randomized, con-trolled trial. Medicine (Baltimore). 2016;95(7):e2854. doi:10.1097/MD.0000000000002854
38. Xu K, Pan Y, Zhu M. Effects of dexmedetomidine on the recovery profiles from general anesthesia in patients undergoing endoscopic
sinus surgery. Int J Clin Exp Med. 2016;9(5):8405-8410.39. Kurhekar P, Vinod K, Rajarathinam B, Dhiviya Krishna JS, Raghura-
man MS. Randomized comparison between dexmedetomidine and midazolam for prevention of emergence agitation after nasal surger-ies. Saudi J Anaesth. 2018;12(1):61-66. doi:10.4103/sja.SJA_419_17
40. Kwon S-Y, Joo J-D, Cheon G-Y, Oh H-S, In J-H. Effects of dexme-detomidine infusion on the recovery profiles of patients undergo-ing transurethral resection. J Korean Med Sci. 2016;31(1):125-130. doi:10.3346/jkms.2016.31.1.125
41. Polat R, Peker K, Baran I, Bumin Aydın G, Topçu Gülöksüz Ç, Dön-mez A. Comparison between dexmedetomidine and remifentanil infusion in emergence agitation during recovery after nasal surgery: a randomized double-blind trial. Anaesthesist. 2015;64(10):740-746. doi:10.1007/s00101-015-0077-8
42. Read MD, Maani CV, Blackwell S. Dexmedetomidine as a rescue therapy for emergence delirium in adults: a case series. A A Case Rep. 2017;9(1):20-23.
43. Brown DV, Heller F, Barkin R. Anticholinergic syndrome after anes-thesia: a case report and review. Am J Ther. 2004;11(2):144-153.
44. Su M, Goldman M. Anticholinergic poisoning. UpToDate. 2015. Updated March 2019. https://www.uptodate.com/contents/anticholinergic-poisoning?search=Anticholinergic%20poisoning&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 Accessed April 5, 2019.
45. Wofford K, Vacchiano C. Sorting through the confusion: adverse cog-nitive change after surgery in adults. AANA J. 2011;74(4):335-342.
46. Fu H, Fan L, Wang T. Perioperative neurocognition in elderly patients. Curr Opin Anaesthesiol. 2018;31(1):24-29. doi:10.1097/ACO.0000000000000536
47. AGS Expert Panel on Postoperative Delirium in Older Adults. Ameri-can Geriatrics Society abstracted clinical practice guideline for post-operative delirium in older adults. J Am Geriatr Soc. 2015;63(1):142-150. doi:10.1111/jgs.13281
48. Drummond JC. Are you confused about delirium (and its causa-tion, prevention and treatment)? Paper presented at: Anesthesiology Review Course 2017: A Thorough Review and Update in the Practice of Anesthesiology; April 9-13, 2016; San Antonio, TX.
49. Hamrick I, Meyer F. Perioperative management of delirium and dementia in the geriatric surgical patient. Langenbecks Arch Surg. 2013;398(7):947-955. doi:10.1007/s00423-013-1102-5
50. Inouye SK. Predisposing and precipitating factors for delirium in hos-pitalized older patients. Dement Geriatr Cogn Disord. 1999;10(5):393-400. doi:10.1159/000017177
AUTHORSCol Shawna Greiner, PhD, CRNA, USAF, NC, practices at 60th Medical Group at Travis Air Force Base and was an assistant professor who has taught for military nurse anesthesia programs. For 25 years, she has served in the US Navy and now the Air Force. Dr Greiner has authored and coau-thored peer-reviewed publications focused on ethics, deployment experi-ences of mothers, military mental health stigma, and emergence delirium.
Michael J. Kremer, PhD, CRNA, CHSE, FNAP, FAAN, received undergraduate degrees in psychology and nursing from Northern Illinois University in DeKalb, Illinois; his anesthesia education was at St John’s Hospital/University of Illinois-Springfield in Springfield, Illinois. Dr Kre-mer is a Certified Healthcare Simulation Educator and is a fellow in the National Academies of Practice, the Institute of Medicine of Chicago, and the American Academy of Nursing.
DISCLOSURESThe authors have declared no financial relationships with any commercial entity related to the content of this article. The authors did discuss off-label use within the article. Disclosure statements are available for viewing upon request.
MILITARY DISCLAIMERThe views presented here are those of the authors and are not to be con-strued as official or reflecting the views of the Department of Defense, Air Force, or the Uniformed Services University of the Health Sciences.