Embed Size (px)
Citation preview
5/2/17
1
AntibioticStewardship:“It’sAlsoAboutTheRightDiagnosis”
NeilGaffin,MDKimSimon,MSN,CIC,FAPIC
TheValleyHospitalRidgewood,NJ
Top7ThreatstotheHumanRace
2Source adapted from Science, Vol 325, September 2009Available at http://www.sciencemag.org/content/325/5948.cover-expansion
Remember These Days?WHO priority pathogens list for R&D of new antibiotic
February 27, 2017
Priority 1: CRITICAL
•Acinetobacter baumannii, carbapenem-resistant•Pseudomonas aeruginosa, carbapenem-resistant•Enterobacteriaceae, carbapenem-resistant, ESBL-producing
Priority 2: HIGH
•Enterococcus faecium, vancomycin-resistant•Staphylococcus aureus, methicillin-resistant, vancomycin-intermediate and resistant•Helicobacter pylori, clarithromycin-resistant•Campylobacter spp., fluoroquinolone-resistant•Salmonellae, fluoroquinolone-resistant•Neisseria gonorrhoeae, cephalosporin-resistant, fluoroquinolone-resistant
Priority 3: MEDIUM
•Streptococcus pneumoniae, penicillin-non-susceptible•Haemophilus influenzae, ampicillin-resistant•Shigella spp., fluoroquinolone-resistant
Background: Impact
• Hospital-acquired, hospital-onset: 165,000 cases, $1.3 billion in excess costs, and 9,000 deaths annually
• Hospital-acquired, post-discharge (up to 4 weeks): 50,000 cases, $0.3 billion in excess costs, and 3,000 deaths annually
• Nursing home-onset: 263,000 cases, $2.2 billion in excess costs, and 16,500 deaths annually
Campbell et al. Infect Control Hosp Epidemiol. 2009:30:523-33. Dubberke et al. Emerg Infect Dis. 2008;14:1031-8.
Dubberke et al. Clin Infect Dis. 2008;46:497-504. Elixhauser et al. HCUP Statistical Brief #50. 2008.

5/2/17
2
Background: EpidemiologyRisk Factors
• Antimicrobial exposure• Acquisition of C. difficile• Advanced age• Underlying illness• Immunosuppression• Tube feeds• ? Gastric acid suppression
Main modifiable risk factors
Date of download: 3/2/2017 © 2008 Infectious Diseases Society of America.
From: Antimicrobial-Associated Risk Factors for Clostridium difficile Infection
Clin Infect Dis. 2008;46(Supplement_1):S19-S31
BacterialCellsOutnumberUsBy10:1“Oral amoxicillin exposure caused marked shifts in microbiome composition that lasted approximately 30 days on average and were observed for more than 2 months in some of the treated individuals.
Large shifts were also reported during an oral course of ciprofloxacin, with the changes persisting for several weeks; the extent of restoration of the baseline composition of the microbiome was highly subject-dependent.”
Dethlefsen L, Relman DA. Incomplete recovery and individualized responses of the human distal gut microbiota to repeated antibiotic perturbation. Proc Natl Acad Sci U S A. 2011;108 Suppl 1:4554–61.
“Collateral Damage” From Antibiotics
PLoS Pathog. 2015 Oct; 11(10): e1005157.
Developmental life cycle of Clostridium difficile during infection.
PLoS Pathog. 2015 Oct; 11(10): e1005157.
Effect of bile acid metabolism on the developmental life cycle of C. difficile.
5/2/17
3
Genetic arrangement of the C. difficile pathogenicity locus and proposed protein domain structures of TcdA and TcdB.
Daniel E. Voth, and Jimmy D. Ballard Clin. Microbiol. Rev. 2005;18:247-263
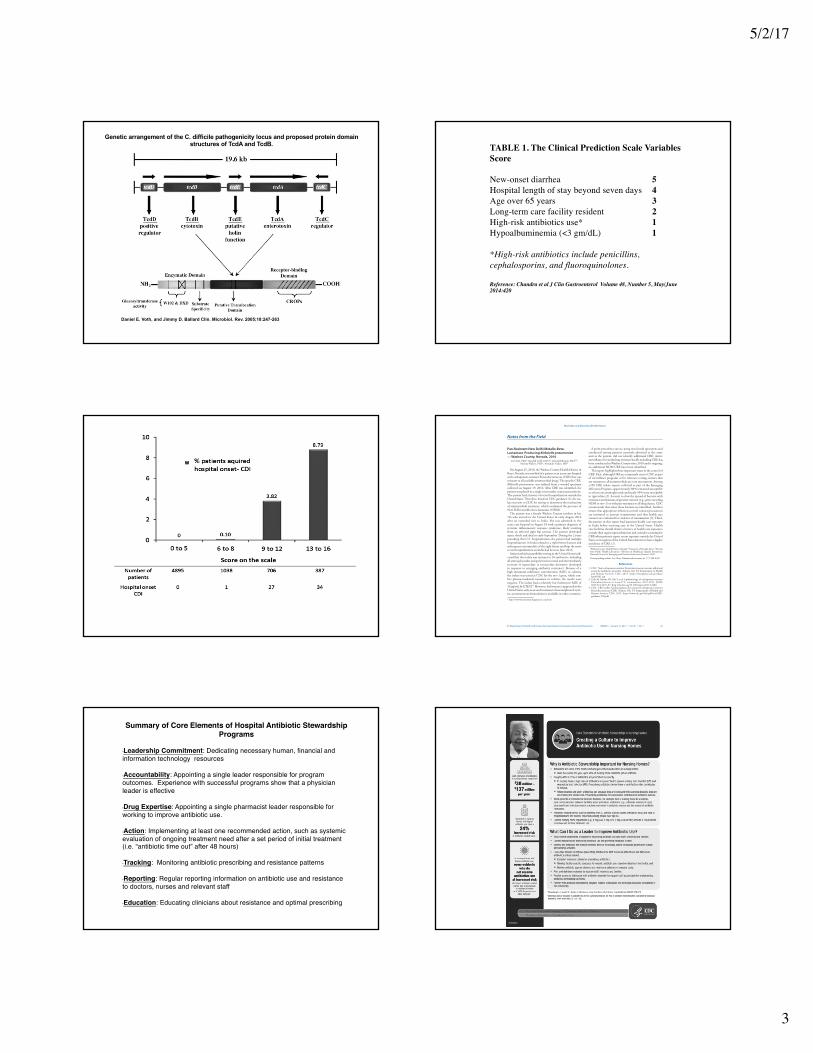
TABLE 1. The Clinical Prediction Scale Variables Score
New-onset diarrhea 5Hospital length of stay beyond seven days 4Age over 65 years 3Long-term care facility resident 2High-risk antibiotics use* 1Hypoalbuminemia (<3 gm/dL) 1
*High-risk antibiotics include penicillins, cephalosporins, and fluoroquinolones.
Reference: Chandra et al J Clin Gastroenterol Volume 48, Number 5, May/June2014:420
Morbidity and Mortality Weekly Report
MMWR / January 13, 2017 / Vol. 66 / No. 1 33US Department of Health and Human Services/Centers for Disease Control and Prevention
Pan-Resistant New Delhi Metallo-Beta-Lactamase-Producing Klebsiella pneumoniae — Washoe County, Nevada, 2016
Lei Chen, PhD1; Randall Todd, DrPH1; Julia Kiehlbauch, PhD2,3; Maroya Walters, PhD4; Alexander Kallen, MD4
On August 25, 2016, the Washoe County Health District in Reno, Nevada, was notified of a patient at an acute care hospital with carbapenem-resistant Enterobacteriaceae (CRE) that was resistant to all available antimicrobial drugs. The specific CRE, Klebsiella pneumoniae, was isolated from a wound specimen collected on August 19, 2016. After CRE was identified, the patient was placed in a single room under contact precautions. The patient had a history of recent hospitalization outside the United States. Therefore, based on CDC guidance (1), the iso-late was sent to CDC for testing to determine the mechanism of antimicrobial resistance, which confirmed the presence of New Delhi metallo-beta-lactamase (NDM).
The patient was a female Washoe County resident in her 70s who arrived in the United States in early August 2016 after an extended visit to India. She was admitted to the acute care hospital on August 18 with a primary diagnosis of systemic inflammatory response syndrome, likely resulting from an infected right hip seroma. The patient developed septic shock and died in early September. During the 2 years preceding this U.S. hospitalization, the patient had multiple hospitalizations in India related to a right femur fracture and subsequent osteomyelitis of the right femur and hip; the most recent hospitalization in India had been in June 2016.
Antimicrobial susceptibility testing in the United States indi-cated that the isolate was resistant to 26 antibiotics, including all aminoglycosides and polymyxins tested, and intermediately resistant to tigecycline (a tetracycline derivative developed in response to emerging antibiotic resistance). Because of a high minimum inhibitory concentration (MIC) to colistin, the isolate was tested at CDC for the mcr-1 gene, which con-fers plasma-mediated resistance to colistin; the results were negative. The isolate had a relatively low fosfomycin MIC of 16 µg/mL by ETEST.* However, fosfomycin is approved in the United States only as an oral treatment of uncomplicated cysti-tis; an intravenous formulation is available in other countries.
A point prevalence survey, using rectal swab specimens and conducted among patients currently admitted to the same unit as the patient, did not identify additional CRE. Active surveillance for multidrug-resistant bacilli including CRE has been conducted in Washoe County since 2010 and is ongoing; no additional NDM CRE have been identified.
This report highlights three important issues in the control of CRE. First, although CRE are commonly sent to CDC as part of surveillance programs or for reference testing, isolates that are resistant to all antimicrobials are very uncommon. Among >250 CRE isolate reports collected as part of the Emerging Infections Program, approximately 80% remained susceptible to at least one aminoglycoside and nearly 90% were susceptible to tigecycline (2). Second, to slow the spread of bacteria with resistance mechanisms of greatest concern (e.g., gene encoding NDM or mcr-1) or with pan-resistance to all drug classes, CDC recommends that when these bacteria are identified, facilities ensure that appropriate infection control contact precautions are instituted to prevent transmission and that health care contacts are evaluated for evidence of transmission (3). Third, the patient in this report had inpatient health care exposure in India before receiving care in the United States. Health care facilities should obtain a history of health care exposures outside their region upon admission and consider screening for CRE when patients report recent exposure outside the United States or in regions of the United States known to have a higher incidence of CRE (1).
1Washoe County Health District, Nevada; 2University of Nevada, Reno, 3Nevada State Public Health Laboratory, 4Division of Healthcare Quality Promotion, National Center for Emerging and Zoonotic Infectious Diseases, CDC.Corresponding author: Lei Chen, [email protected], 775-328-2447.
References1. CDC. New carbapenem-resistant Enterobacteriaceae warrant additional
action by healthcare providers. Atlanta, GA: US Department of Health and Human Services, CDC; 2013. https://emergency.cdc.gov/han/han00341.asp
2. Guh AY, Bulens SN, Mu Y, et al. Epidemiology of carbapenem-resistant Enterobacteriaceae in seven U.S. communities, 2012–2013. JAMA 2015;314:1479–87. http://dx.doi.org/10.1001/jama.2015.12480
3. CDC. CRE toolkit: facility guidance for control of carbapenem-resistant Enterobacteriaceae (CRE). Atlanta, GA: US Department of Health and Human Services, CDC; 2015. https://www.cdc.gov/hai/pdfs/cre/CRE-guidance-508.pdf
Notes from the Field
* http://www.biomerieux-diagnostics.com/etest.
Summary of Core Elements of Hospital Antibiotic Stewardship Programs
•Leadership Commitment: Dedicating necessary human, financial and information technology resources
•Accountability: Appointing a single leader responsible for program outcomes. Experience with successful programs show that a physician leader is effective
•Drug Expertise: Appointing a single pharmacist leader responsible for working to improve antibiotic use.
•Action: Implementing at least one recommended action, such as systemic evaluation of ongoing treatment need after a set period of initial treatment (i.e. “antibiotic time out” after 48 hours)
•Tracking: Monitoring antibiotic prescribing and resistance patterns
•Reporting: Regular reporting information on antibiotic use and resistance to doctors, nurses and relevant staff
•Education: Educating clinicians about resistance and optimal prescribing

5/2/17
4
Source: CDC Vital Signs, August 2015
EmpiricAntibioticOrders
PositiveCultures/Definite
Infection
CulturesNegative/DefiniteInfection
CulturesNegative/NoObviousInfectionRequiringIVRx
IDMDSupervisedAutomaticNarrowing
ofAntimicrobialTherapy
DailyAssessmentofContinuedNeedforIVRxandAutomatic
ChangetoPOWhenAppropriate
DiscontinueTherapy
48HoursLater
TheValleyHospitalAntimicrobialStewardshipProcess.
ApprovedbyMedicalBoardDecember2013
Right drug, dose, time and duration, but it’s also about the right diagnosis.
Nursing Facility Stewardship

5/2/17
5
2012AvgMonthly 1stQtr.2016AvgMonthly 2ndQtr.2016AvgMonthly 3rdQtr.2016AvgMonthly 9Months2016AvgMonthly Avg%ChangeinAntibiotic DaysofABXTherapy DaysofABXTherapy DaysofABXTherapy DaysofABXTherapy DaysofABXTherapy DaysofABXTherapy
CEFTRIAXONESODIUM(ROCEPHIN) 2387 725 732 758 738 -69.08%CEFAZOLINSODIUM(KEFZOL) 257 309 304 300 304 18.29%METRONIDAZOLE/SODIUMCHLORIDE(FLAGYLIVPB) 670 325 372 394 364 -45.67%VANCOMYCINHCL(VANCOCIN) 640 229 244 297 257 -59.84%AMPICILLINSODIUM/SULBACTAMNA(UNASYN) 109 151 178 178 169 55.30%AZITHROMYCIN(ZITHROMAXINJ) 468 144 127 86 119 -74.57%PIPERACILLINSODIUM/TAZOBACTAM(ZOSYNVIAL) 279 79 89 80 83 -70.25%LEVOFLOXACIN/D5W(LEVAQUINIVPB) 165 71 62 62 65 -60.61%AZTREONAM(AZACTAM) 260 86 69 81 79 -69.62%
Avg%ChangeAveragePatientDays 10,458 9,477 8,378 9,053 8,969 -9.40%
AverageTotalDaysofAntibioticTherapy 5,235 2,119 2,177 2,236 2,177 -58.41%
AntibioticDaysofTherapy/1000PatientDays 501 232 260 247 243 -51.50%
AntibioticCostperPatientDay2012 $14.20 $5.26 $5.20
DaysofAntibioticTherapy
“Things are not always what they seem; the first appearance deceives many; the intelligence of a few perceives what has
been carefully hidden”
Phaedrus
The Major Culprits Contributing To Overuse Pneumonia is a Clinical Diagnosis-A Chest X-Ray alone Can’t Diagnose It
AntibioticsDiscontinued
IsolatedFever-NoPulm Sx’s Post- Seizure&MI
TransitionsofCare-TheDoortoUnnecessaryDOT
• First,wehavetoensurethattheoriginaldiagnosiswascorrect-don’tjusttakethediagnosisonfacevalue!Manyinfectiousdiagnosesareincorrect,inparticular“pneumonia”,“UTI”,and“cellulitis”.
• Second,wehavetorealizethatmosttypicalinfectionscanbetreatedeffectivelywith5-7daysoftherapy,orwhenclinicalsignsandsymptomshaveresolved(couldbesooner!!).
• Third,sincetheaverageLOSatacutecarefacilityis4daysroughly,thenwe’repotentiallytalkingaboutonly0-3moredaysoftherapyuponarrivalattheSNF!
5/2/17
6
Beware!The“UTI”Problem
“Insanityisdoingthesamethingoverandoverandexpectingdifferentresults.”AlbertEinstein
The Urine Problem
Under normal conditions…
the skin surface is not sterile…
the mouth is not sterile…
the colon is not sterile…
and in many patients,
the bladder is not sterile.
Asymptomatic Bacteriuria
• Positive urine culture, but no need for antibiotic treatmentExceptions:
- Pregnancy
- Prior to urologic surgery
Nicolle LA, et al. IDSA Guidelines for Asymptomatic Bacteriuria. CID 2005: 40( March 1); 643-654
Prevalence-Asymptomatic Bacteriuria
Population Prevalence
Long-term care facility, age ≥70Women 25-50%Men 15-40%
Community, age ≥70Women 11-16%Men 4-19%
Healthy pre-menopausal women 1-5%
10
Nicolle LA, et al. IDSA Guidelines for Asymptomatic Bacteriuria. CID 2005: 40( March 1); 643-654
Population Percentage(%)
YoungWomen 32
PregnantWomen 30-70
DiabeticWomen 70
ElderlyInstitutionalized 90
Hemodialysis 90
Bacteriuric Short–TermCatheters 30-75
Bacteriuric Long-TermindwellingCatheters 50-100
Nicolle LA, et al. IDSA Guidelines for Asymptomatic Bacteriuria. CID 2005: 40( March 1); 643-654

5/2/17
7
ASBIsA MarkerForVulnerability
• 318womenwithASBolder,sickerandhadgreatermortalitythan1173womenwithoutASB.
• Multivariateanalysis-ASBunrelatedtomortality.• TreatmentofASBhadnoeffectonmortality.
Abrutyn, Ann Int Med 1994
Beware!“ThePneumoniaConundrum”• Thestandardfordiagnosingpneumoniathathasdevelopedoverthepast
severaldecadesinvolvesrecognitionofasyndromeofclinical,laboratoryandradiographicfeaturescompatiblewithpulmonaryinfection.
• PatientswithnonspecificCXRopacitiesbutwithoutclinicalfeaturessuggestiveofpulmonaryinfectionshouldnotbereflexivelydiagnosedwithpneumoniaandtreatedwithantibiotics.
• InthisstudyofadultEDpatientspresentingwithacutecardiopulmonarysymptoms,6.6%ofpatientshadpulmonaryopacitiesinterpretedonCXRthatwerenotreproducedonCT.Consideringthe12.4millionEDvisitsannuallyintheUSduetoshortnessofbreath,chestpainorcough,an“opacityequalsantibiotics”reflexivemanagementstrategyislikelytoleadtofrequentoveruseofantibioticsandunnecessarypressureforthedevelopmentofantibioticresistance.
1. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007; 44(Suppl 2):S27–S72.
2. Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 1997; 278:1440–1445.
3.High Discordance of Chest X-ray and CT for Detection of Pulmonary Opacities in ED Patients: Implications for Diagnosing Pneumonia Wesley H. Self, MD MPHa Am J Emerg Med. 2013 February ; 31(2): 401–405
Procalcitonin-CouldPotentiallyHelpUsGetPatientsOffAntibioticsSooner
• TheUSFoodandDrugAdministration(FDA)hasclearedtheexpandeduseoftheVidas Brahmsprocalcitonin (PCT)testtohelpcliniciansdeterminewhetherantibiotictreatmentshouldbeinitiatedorstoppedinpatientswithlowerrespiratorytractinfectionsandstoppedinpatientswithsepsis.
Beware!“TheCellulitisProblem”
• It'spurelyaclinicaldiagnosis,almostalwaysofacuteonsetandunilateral.
• Inflammatorydermatosesofthelowerextremityareoftenmisdiagnosedascellulitis(aka“pseudocellulitis”)andtreatedwithantibioticsand/orhospitalization.Thereislimiteddataonthecostandcomplicationsfrommisdiagnosedcellulitis.
• Inthiscross-sectionalstudythatincluded259patients,30%weremisdiagnosedwithcellulitis,ofwhich85%didnotrequirehospitalizationand92%receivedunnecessaryantibiotics.Combiningthesefindingswithpreviouslypublisheddata,costestimates,andandprojectionsindicatethatcellulitismisdiagnosisleadsto50 000to130 000unnecessaryhospitalizationsintheUnitedStatesand$195millionto$515millioninavoidablehealthcarespendingannually.
JAMA Dermatol. 2017;153(2):141-146.

5/2/17
8





























